Embed Size (px)
Citation preview

Potential Role of Neuroprotective Agents in the Treatment of Patients with Acute Ischemic StrokeBruce Ovbiagele, MD*
Chelsea S. Kidwell, MDSidney Starkman, MDJeffrey L. Saver, MD
Address*Stroke Center and Department of Neurology, University of California at Los Angeles, 710 Westwood Plaza, Los Angeles, CA 90095, USA.E-mail: [email protected]
Current Treatment Options in Cardiovascular Medicine 2003, 5:441–449Current Science Inc. ISSN 1092-8464Copyright © 2003 by Current Science Inc.
IntroductionStroke is the third leading cause of death and theleading cause of serious long-term disability in the
United States. Intravenous tissue plasminogen activatoris the only US Food and Drug Administration–
Opinion statementCurrently, intravenous recombinant tissue plasminogen activator is the only US Food and Drug Administration–approved therapy for acute ischemic stroke. Although effica-cious, its usefulness is limited, mainly because of the very limited time window for its administration. Neuroprotective treatments are therapies that block the cellular, biochemical, and metabolic elaboration of injury during or after exposure to ischemia, and have a potential role in ameliorating brain injury in patients with acute ischemic stroke. More than 50 neuroprotective agents have reached randomized human clinical trials in focal ischemic stroke, but none have been unequivocally proven efficacious, despite successful preceding animal studies. The failed neuroprotective trials of the past have greatly increased understanding of the fundamental biology of ischemic brain injury and have laid a strong foundation for future advance. Moreover, the recent favorable results of human clinical trials of hypothermia in human cardiac arrest and global brain ischemia have validated the general concept of neuroprotec-tion for ischemic brain injury. Recent innovations in strategies of preclinical drug development and clinical trial design that rectify past defects hold great promise for neuroprotective investigation, including novel approaches to accelerating time to initiation of experimental treatment, use of outcome measures sensitive to treatment effects, and trial testing of combination therapies rather than single agents alone. Although no neuroprotective agent is of proven benefit for focal ischemic stroke, several currently available interventions have shown promising results in preliminary trials and may be considered for cautious, off-label use in acute stroke, including hypothermia, magnesium sulfate, citicoline, albumin, and erythropoietin. Overall, the prospects for safe and effective neuroprotective therapies to improve stroke outcome remain promising.

442 Valvular, Myocardial, Pericardial, and Cardiopulmonary Disease
approved treatment for acute ischemic stroke, but mustbe used within 3 hours of symptom onset, and carries asubstantial risk of hemorrhagic transformation [1]. As aconsequence, less than 3% of patients with acutestroke in the United States currently receive tissueplasminogen activator [2]. Additional therapies areurgently needed to reduce the devastating consequencesof stroke.
Neuroprotection is a promising acute stroke treat-ment strategy. Therapy in acute ischemic stroke may bedivided into the following broad approaches: 1) restor-ing blood flow (reperfusion), and 2) enabling brain cellsto endure reduced blood flow (neuroprotection). Neuro-protective treatments are therapies that interrupt thecellular, biochemical, and metabolic processes that leadto brain injury during or after exposure to ischemia andencompass a wide, and continually expanding, array ofpharmacologic interventions [3–5].
Within the field of cerebrovascular disease, thegrowth of neuroprotective intervention strategies overthe past two decades has increased understandingof the pathophysiologic complexity of focal ischemicbrain injury and the ischemic cascade. Early formu-lated strategies included suppression of neuronalmetabolism and blockade of calcium entry. Morerecently developed approaches include blockade ofexcitotoxic neurotransmission, free radical scavenge,nitric oxide–related intervention, inhibition of apop-tosis, hyperpolarization to inhibit peri-infarct depolar-ization, anti-inflammatory and anticytokine strategies,and neurotrophic agents [6].
Although these and additional neuroprotectiveclasses have been effective in reducing infarct size inanimal stroke models, the record of neuroprotectiveagents in human clinical trials has been remarkablydisappointing. More than 50 neuroprotective agentshave been tested in randomized controlled clinicaltrials in acute ischemic stroke [6], but none have beenshown unequivocally beneficial in definitive phase IIItrials. These results have led many investigators to ask,“Why do neuroprotective drugs work in animals butnot in humans [7,8]?”
Fortunately, the past has been instructive. Valuablelessons learned from previous trials have yieldedunique insights into fundamental mechanisms ofischemic brain injury, novel classes of pharmacologictherapies, more appropriate designs for neuroprotectiveclinical trials, and novel treatment delivery strategies.
CASCADES MEDIATING INJURY IN CEREBRAL ISCHEMIAThe ischemic cascade When focal occlusions disruptcerebral blood flow, a cascade of molecular eventsproducing cell injury ensues [9]. Cell death proceedsrapidly in the infarct core, where blood flow is mostdrastically curtailed, but more slowly in the surround-ing ischemic penumbra, where blood flow is variably
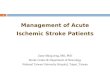
reduced and molecular elaboration of neuronalinjury may proceed over 12 hours or more. Apoptosis(programmed cell death), as well as necrosis, contrib-utes to cel l death in penumbral regions. Eachstep along the ischemic cascade is a potential targetfor therapeutic intervention (Fig. 1). The mechanismsby which anoxia-tolerant and hibernation-capablespecies regulate controlled metabolic suppression, pre-serve their cell structure, and maintain membraneintegrity in the face of reduced energy supplies haveprovided important clues to potentially effective phar-macologic interventions.
The reperfusion cascade Prompt reperfusion of ischemicbrain tissue is critical for restoring normal function.However, the return of blood flow may produce destruc-tion of preserved or recovered cells. “Reperfusion injury”has a multifactorial etiology, but appears stronglyassociated with inflammatory processes potentiatingischemic injury [10].
Leukocytes potentiate central nervous systemreperfusion injury by clogging the microcirculation andinfiltrating the brain. The initial step is leukocyte-to-endothelial cell adhesion. Leukocyte capillary pluggingmay be the major mechanism of the “no-reflow”phenomenon, which is incomplete restoration ofnormal blood flow despite full recanalization of themacrocirculation [9]. Proinflammatory cytokinesalso probably exert influences on leukocyte adhesion.Modulation of the “cytokine cascade” is a pertinent goalfor future neuroprotective investigation.
GENERAL ADVANCES IN THE DEVELOPMENT AND TESTING OF NEUROPROTECTIVE AGENTSPreclinical development Numerous general designdefects of the preclinical development process contrib-uted to the plenitude of failed human neuroprotectiveclinical trials [4]. Recently, several groups have sug-gested revisions in experimental animal model systemsto avoid selecting for human trials with neuroprotectiveagents of misleading promise. Most influential havebeen the recommendations of the Stroke TherapyAcademic Industry Roundtable, which recommendedminimal and ideal requirements that a purportedneuroprotective agent should meet in preclinical testingbefore proceeding to clinical trials [11••]. The idealcriteria require the agent to 1) demonstrate efficacy inat least two species; 2) demonstrate efficacy in at leasttwo different laboratories that use different models;3) demonstrate efficacy in permanent and transientfocal ischemia models; 4) improve short- and long-termhistologic and functional outcomes; 5) demonstrateefficacy when administered several hours after ischemiaonset; 6) achieve brain concentrations that rapidlyequilibrate with the plasma, when the drug site ofaction is beyond the the blood-brain barrier; 7) show a

Potential Role of Neuroprotective Agents Ovbiagele et al. 443
consistent minimal concentration that provides neuro-protection across different species, allowing predictionof likely minimum neuroprotective concentration inhumans; 8) demonstrate a sigmoid-shaped rather thanbell-shaped dose-response curve; and 9) have data to
guide duration of treatment based on pharmacokineticprofile and hypothesized mechanism of action.
HUMAN CLINICAL TRIAL DESIGNRecent authoritative reviews have identified key designdefects of past human clinical trials of neuroprotectiveclinical trials [12••]. The deficiencies and remedies thatprevent them from being implemented in currentgeneration trials are summarized in Tables 1 and 2.
Delayed time to initiation of study treatment may bethe most critical defect of past trials. Although neuro-protective agents are generally beneficial in focal animalstroke models primarily in the first 2 hours postonset,no human clinical neuroprotective agent trial hasenrolled any substantial cohort of patients in thistime window [6]. Among 5370 enrolled patients in sixrecent neuroprotective trials, only 0.2% were treatedwithin 60 minutes of onset and 1.2% between 61 to 120minutes of onset [21].
Paramedic start of study treatment in the field is aparticularly promising approach to the challenge oftesting neuroprotective agents in hyperacute timeepochs. The FAST-MAG (Field Administration of StrokeTherapy–Magnesium) pilot trial recently demonstratedthe feasibility of paramedic field initiation of neuro-protective agents in acute stroke trials [22•]. Paramedicsused the Los Angeles Prehospital Stroke Screen toidentify patients with stroke in the field, and initiatedmagnesium sulfate study agent in 20 acute patients.The field enrollment strategy reduced the interval fromparamedic arrival on the scene to the start of the neuro-protective trial agent to 23 minutes, accelerating thestudy agent start by nearly 2 hours compared withhistorical control individuals.
SELECTED PROMISING NEUROPROTECTIVE THERAPIESNo neuroprotective therapy is of proven benefit in acuteischemic stroke. Several agents of great promise arecurrently in the mid to late stages of clinical trial testingand may emerge in routine practice within the nextfew years. For this review of current treatment options,in the absence of approved neuroprotective strokeagents, the authors highlight select therapies that areunapproved for stroke, but currently available for use,because they are approved for other indications in theUnited States and are available for off-label use forstroke at individual physician discretion, or becausethey are approved for the indication of stroke in coun-tries outside the United States. The authors occasionallyuse these agents in practice, but only very sparingly, inhighly select patients, and only after eliciting detailedinformed consent from patients and family members.
Hypothermia Hypothermia exerts pleiotropic neuro-protective effects, including decreasing cerebral meta-bolic rate, preserving the blood-brain barrier, inhibitingexcitotoxic neurotransmitter release, diminishing
Figure 1. Ischemic cascade in patients with acute ischemic stroke. AMPA—�-amino-3-hydroxy-5-methyl-4-isoxazolepropi-onate; NMDA—N-methyl-D-aspartate.

444 Valvular, Myocardial, Pericardial, and Cardiopulmonary Disease
activity of protein kinases, promoting resynthesis ofcellular repair proteins, inhibiting apoptosis, andattenuating postischemic inflammation [23]. Low bodytemperature on admission in the setting of an acuteischemic stroke has been an independent predictorof good short-term outcome [24]. Two randomizedclinical trials have demonstrated that induced moderatehypothermia (32ºC to 34ºC) improves outcomefrom global hypoxia-ischemia in patients with out-of-hospital cardiac arrest. In an Australian trial enrolling77 patients, survival to hospital discharge to home orrehabilitation occurred in 49% of patients treated withhypothermia versus 26% of control individuals [25].In the Hypothermia after Cardiac Arrest Study Grouptrial, good 6-month functional outcome was achievedin 55% of patients treated with hypothermia versus39% of patients with normothermia (n = 273) [13••].
Initial studies of hypothermia in patients with focalstroke focused on large infarctions, aiming to preventfatal cerebral herniation by limiting cytotoxic edema.Among 25 patients with severe middle cerebral arterystroke, induced hypothermia to 33ºC within 14 ±
7 hours after symptom onset reduced mortality to 44%compared with approximately 80% in historical controlindividuals [14].
More recent studies have focused on early neuro-protection with hypothermia. Prophylactic adminis-tration of acetaminophen has yielded mild reductionin average temperatures in phase II stroke trials [15].In the past, induction of moderate hypothermia(to 33ºC) required muscular paralysis to avert shiver-ing, mandating intubation, and limiting applicationto only severe strokes. However, recent studies havedemonstrated that aggressive antishivering regimenswith meperidine, buspirone, and surface warming(while cooling internal structures) permits patientsto tolerate moderate hypothermia while awake andbreathing normally, without shivering [16]. Endo-vascular cooling devices to accelerate the induction ofmoderate hypothermia are being tested in phase IIstroke trials, given the suboptimal 3- to 6-hour orgreater delay from treatment start to achievementof target body temperature using standard surfacecooling techniques [17–19].
Table 1. Evolving improvements in neuroprotective clinical trial design
Trial design feature Problem Emerging solutions
Sample size Too small Larger sample sizesTypically 100 to 1000 patients 1000 to 10,000 patientsAble to detect only major effects Able to detect 2% to 5% absolute benefitTypically 3 to 12 hours
Time window Too long Shorter time window strategiesTypically 3 to 12 hours Shorter trial-wide enrollment window
(3 to 4 hours)Drug arrives after infarct completion Prehospital initiation
Prespecified short treatment window cellsIncreased reimbursement of shorter enrollments
Patient severity Too broad Typical lower bound of NIHSS [4–8]Enrolling all patients confounds detection
of treatment effectTypical upper bound of NIHSS [13••,14–20]
Mild patients do well, even on placeboSeveral patients do poorly, even on treatment
Stroke location Too wide Enroll only patients with stroke at the site of putative agent action
Certain neuroprotective agent mechanisms benefit only specific stroke locations
Clinical and diffusion MR localization and exclusion
EAA blockers active only in cortexTrial end point Too insensitive Employ novel end points sensitive to small,
but clinically relevant impairmentsSimple function scale rating scales have
substantial ceiling effectsStroke-specific quality-of-life scales
Many patients will score well on Barthel, Rankin, NIHSS at 3 months
Generic health-related quality-of-life scales
Quantifiable performance outcomes (eg, walking speed)
EAA—excitatory amino acid; MR—magnetic resonance; NIHSS—National Institutes of Health Stroke Scale.

Potential Role of Neuroprotective Agents Ovbiagele et al. 445
Magnesium Magnesium exerts several potentially neuro-protective effects, including noncompetitive blockade ofthe N-methyl-D-aspartate receptor, inhibition of presyn-aptic release of excitatory neurotransmitters, presynapticpotentiation of adenosine, blockade of voltage-gatedcalcium channels, suppression of cortical-spreadingdepression and anoxic depolarization, and relaxation ofvascular smooth muscle and antagonism of endothelin-1and other vasoconstrictors, resulting in vasodilation oflarge and small vascular beds and increased cerebralblood flow [4]. Magnesium sulfate demonstrated neuro-protective effects in temporary and permanent middlecerebral artery occlusion models, and has shown promisein seven randomized phase II human clinical trialsenrolling a total of 744 patients [20].
Magnesium sulfate is currently being tested in twophase III trials: the 2800 patient, 12 hour or less post-onset Intravenous Magnesium Efficacy in Acute Stroketrial and the 1298 patient, 2 hour or less postonsetFAST-MAG trial [26]. Its well-established safety profilemakes magnesium sulfate an attractive agent for pre-hospital administration in the ambulance. In the FAST-MAG pilot trial, no adverse effects related to fieldadministration were observed [22•].
Citicoline Citicoline is a choline precursor that ismetabolized after administration to form phosphatidyl-choline, a major neuronal membrane lipid. Citicolinemay reduce acute ischemic injury by stabilizing cellmembranes, decreasing free radical formation, and
Table 2. Evolving improvements in neuroprotective clinical trial design
Trial design feature Problem Emerging solutions
Statistical analysis of primary end point
Too coarse Use entire range of rating scale in primary analysis
End point frequently dichotomized (eg, disabled vs nondisabled), failing to use all information available from rating scale
Apply different "win" criteria adjusted to patient status to stroke subtype at entry
Same "win" criteria applied to all patients, whether mild, moderate, or severe at entry
Surrogate outcome Too variable Measure salvage of initially treated tissue measured in each patient at entry (low variance, high statis-tical power)
Final infarct size on CT or MR has high variance, limiting statistical power
MR diffusion-perfusion penumbra characterization
CT perfusion-collapsed blood volume penumbra characterization
Number of agents under the study Too limitedSingle agents unlikely to exert dramatic
effects given multiple branches in ischemic cascade of injury
Combination therapy trials
Add-on neuroprotective to standard TPA
Combination of neuroprotectivesFactorial designAcademic consortia to facilitate
industrial collaborationInferring best pivotal trial end point
from phase II trialsToo subjective to chance positive results Select pivotal trial end point using
general principles, not pilot dataMeasure outcomes of clinical
relevance to patientsMinimal floor and ceiling effectsEasily administered, highly
reproducibleYields results easily, interpretable
by physicians and patients
CT—computerized tomography; MR—magnetic resonance; TPA—tissue plasminogen activator.

446 Valvular, Myocardial, Pericardial, and Cardiopulmonary Disease
alleviating free fatty acid–induced toxicity, and mayfacilitate functional recovery by fostering synapticoutgrowth and increased neuroplasticity [4].
Eight randomized clinical trials have investigatedciticoline in acute human stroke. Although individualtrials were not definitively positive, two recent meta-analyses suggested potential beneficial treatment effects[27]. The most comprehensive meta-analysis identifiedeight randomized clinical trials of citicoline enrolling2063 patients [27]. Across all trials, treatment withciticoline was associated with absolute reductions of10% to 12% in rates of long-term death and disability,although no individual trial has demonstrated treat-ment benefit unequivocally. Pooled analysis of twociticoline trials collecting serial diffusion magneticresonance imaging data similarly suggested a dose-dependent reduction in infarct growth [28].
Citicoline is currently approved in Spain, Mexico,Japan, and many other countries for use in stroke, headtrauma, and other neurologic disorders. A definitivelarge trial of citicoline in acute stroke in the UnitedStates to confirm or refute signals of efficacy from meta-analysis and imaging studies is being organized.
Albumin Albumin is the major protein of bloodplasma and has numerous potential neuroprotectiveproperties when administered as a therapeutic agent.Human albumin is a potent antioxidant, stabilizesblood-brain barrier function, exerts anti-edema effectsas an osmotic agent, may increase export of pyruvatefrom glial to neuronal cells, sustaining neuronal mito-chondrial metabolism, acts as a blood volume expand-ing hemodilution agent, and reverses stagnation andthrombosis in the cerebral microvasculature [29].
In animal focal stroke models, administration ofhuman serum albumin exerts a marked neuroprotectiveeffect [30,31]. On the basis of scant trial evidence, albuminhas long been used empirically as an osmotic agent fordeteriorating patients with stroke who need blood volumeexpansion. Formal, systematic phase II human clinicaltrials of albumin in acute stroke are now under way.
Erythropoietin Erythropoietin stimulates erythropoiesis.In addition, erythropoietin has shown potent neuro-protective effects in vitro and in vivo, potentially throughantiapoptotic anti-inflammatory, neuronal excitabilitymodulatory, and neurotrophic mechanisms [4].
Recombinant human erythropoietin administeredup to 3 hours after a cerebral arterial occlusion in ratsprevents apoptosis of neurons in the ischemic penum-bra and reduces infarction volume by 75% [32]. Aclinical trial using recombinant human erythropoietinas an acute treatment of cerebral ischemia showed thatthe agent was well tolerated and promising [33].
COMBINATION THERAPIESNeuroprotective agents active at only a single branchpoint in the highly ramified ischemic cascade can beexpected to exert only a modest treatment effect atbest [4]. The hypothesis that combinations of neuro-protective agents with complementary modes ofaction will exert additive or multiplicative beneficialeffects has been repeatedly confirmed in animalstroke models [34]. Likewise, combined neuroprotec-tive and thrombolytic therapies confer increasedbenefit in animal models, probably because of, inpart, greater access of the neuroprotective agent toinjured tissue. Thrombolytic reperfusion also shortensthe duration of ischemia that neuroprotective agentsmust counter.
Combination therapies raise a variety of designissues in human clinical trials [4]. Drug regulatoryagencies discourage combinations of novel agents intrials, so that the efficacy and safety profiles of each newdrug are delineated unambiguously. Eliciting collabora-tion from competing pharmaceutical companies toundertake combination agent trials is difficult. Preclini-cal and phase II pharmacokinetic and dose-rangingstudies may be made more complex by metabolicinteractions of study agents.
These pertinent issues, however, can be addressed.Factorial trial designs allow gathering of monotherapyand combination therapy data concurrently, with only amodest increase in trial sample size. Academic consortiacan act as independent, honest brokers to negotiate thecontributions of competing sponsors to a trial combin-ing agents from different companies. Add-on therapytrials, when a novel agent is tested in combination withan already accepted treatment, pose little difficulty, andseveral combined neuroprotective tissue plasminogenactivator human stroke trials or substudies have alreadybeen performed [35•,36]. Combination therapyregimens undoubtedly constitute the future of neuro-protective stroke therapy.
Treatment
• No neuroprotective therapy is of proven benefit in acute ischemic stroke. In the absence of approved neuroprotective stroke agents, this section high-lights select therapies that are unapproved for stroke, but are currently avail-able for use because they are approved for other indications in the United

Potential Role of Neuroprotective Agents Ovbiagele et al. 447
States and are available for off-label use for stroke at individual physician discretion, or because they are approved for the indication of stroke in countries outside the United States. The authors occasionally use these agents in practice, but only very sparingly, in highly select patients, and only after eliciting detailed informed consent from patients and family members.
• The aim of neuroprotective stroke therapy is to improve functional outcome from acute stroke.
Magnesium sulfate
Standard dosage 4-g intravenous bolus over 15 minutes, then 16-g intravenous bolus over 24 hours. In a dose-ranging trial in acute stroke patients, this regimen yielded rapid and sustained doubling of the serum magnesium level. Several phase II clinical trials suggest magnesium sulfate may be safe and efficacious in acute stroke, but no definitive phase III trial has yet been reported.
Contraindications Second- or third-degree heart block (magnesium may exacerbate). Renal failure (magnesium is cleared renally; risk of magnesium toxicity increased by renal failure).
Main drug interactions Calcium neutralizes effects of magnesium. In digitalis, magnesium may potentiate heart block effects. Magnesium may potentiate neuromuscular blocking agents, central nervous system depressants, and hypotensive response in nifedipine.
Main side effects At therapeutic levels, flushing and diaphoresis. At overdose levels, loss of deep tendon reflexes, respiratory paralysis, cardiac conduction block, and cardiac arrest.
Special points Magnesium sulfate injection 50% must be diluted to concentration of 20% or less before intravenous infusion. Rate of intravenous infusion should generally not exceed 150 mg/min.
Cost/cost-effectiveness For loading dose and 24-hour maintenance regimen, cost is $94.00.
Citicoline
Standard dosage Regimens tested in large acute stroke clinical trials have been 500 mg orally once daily for 6 weeks, 1000 mg orally once daily for 6 weeks, and 2000 mg orally once daily for 6 weeks. The 2000-mg daily regimen appears most promising. Several phase III trials individually have not proven benefit, but meta-analyses have suggested potential advantageous effects.
Contraindications None known.Main drug interactions Adverse interaction with meclofenoxate. Potentiates the effects of levodopa.
Main side effects Gastrointestinal upset.Special points When administered orally, citicoline is absorbed almost completely, and its
bioavailability approximates that when administered intravenously. Safety for use in human pregnancy has not yet been established. The agent is commercially available in Spain, Mexico, Japan, and several additional countries in Europe, South America, and Asia.
Cost/cost-effectiveness Approximately $1052 for a 6-week course of 2000 mg/d.
Albumin
Standard dosage No standard stroke dosing established. The regimen the authors use is 50 cm3 of 25% albumin over 15 to 30 minutes intravenously four times daily. Rate of admin-istration should not exceed 2 mL/min to minimize circulatory overload and pulmo-nary edema. Animal studies suggest benefits in stroke but no phase II or phase III human clinical trials have been reported.
Contraindications Uncompensated heart failure, esophageal varices, pulmonary edema, hemorrhagic diathesis, aluminum overload, anuresis, severe anemia, and history of allergic reaction to albumin.
Main drug interactions Increased frequency of atypical reactions with angiotensin-converting enzyme inhibitors (eg, hypotension and flushing).

448 Valvular, Myocardial, Pericardial, and Cardiopulmonary Disease
Main side effects Pulmonary edema, cardiac failure, and rare infusion rate–related events including flushing, urticaria, fever, chills, and nausea.
Special points Albumin normally constitutes 50% to 60% of plasma proteins and, because of its relatively low molecular weight, exerts 80% to 85% of the colloidal oncotic pressure of the blood. Intravenous administration of concentrated albumin human solutions causes a shift of fluid from the interstitial spaces into the circulation and a slight increase in the concentration of plasma proteins. When administered intra-venous to a well-hydrated patient, each volume of 25% albumin human solution draws about 3.5 Vol of additional fluid into the circulation within 15 minutes, reducing hemoconcentration and blood viscosity.
Cost/cost-effectiveness $712 per day when used four times daily.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Tissue plasminogen activator for acute ischemic stroke: the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995, 333:1581–1587.
2. Nilasena D, Kresowik TF, Wiblin RT, et al.: Assessing patterns of t-PA use in acute stroke. Stroke 2002, 33:354.
3. Fisher M, Ratan R: New perspectives on developing acute stroke therapy. Ann Neurol 2003, 53:10–20.
4. Ovbiagele B, Kidwell CS, Starkman S, Saver JL: Neuro-protective agents for the treatment of acute ischemic stroke. Curr Neurol Neurosci Rep 2003, 3:9–20.
5. Lutsep HL, Clark WM: Neuroprotection in acute ischaemic stroke: current status and future potential. Drugs R D 1999, 1:3–8.
6. Kidwell CS: Trends in acute ischemic stroke trials through the 20th century. Stroke 2001, 32:1349–1359.
7. DeGraba TJ, Pettigrew LC: Why do neuroprotective drugs work in animals but not humans? Neurol Clin 2000, 18:475–493.
8. Grotta J: Why do all drugs work in animals but none in stroke patients? 2. Neuroprotective therapy. J Intern Med 1995, 237:89–94.
9. Felberg RBW, Grotta JC: Neuroprotection and the ischemic cascade. CNS Spectr 2000, 5:52–58.
10. Clark W: Reperfusion injury in stroke. Emedicine Journal 2001, 2:12. http://www.emedicine.com.
11.•• Recommendations for standards regarding preclinical neuroprotective and restorative drug development. Stroke 1999, 30:2752–2758.
First joint recommendations of this academic and industry panel of experts, offering guidelines for preclinical assess-ments of potential neuroprotective therapies for the treatment of acute stroke.12.••STAIR Roundtable: Recommendations for clinical trial
evaluation of acute stroke therapies. Stroke 2001, 32:1598–1606.
Second meeting of the STAIR ad hoc expert panelists provid-ing guidelines for the design of pilot and pivotal human clinical trials of neuroprotective and other therapies for acute ischemic stroke.
13.••Mild therapeutic hypothermia to improve the neuro-logic outcome after cardiac arrest. The Hypothermia after Cardiac Arrest Study Group [no authors listed]. N Engl J Med 2002, 34:549–556.
A landmark multicenter trial that revealed that therapeutic mild hypothermia increased the rate of a favorable neurologic outcome and reduced mortality in patients who have been successfully resuscitated after cardiac arrest caused by ventricu-lar fibrillation, thus buttressing the neuroprotective principle.14. Schwab SSS, Spranger M, Keller E, et al.: Moderate hypo-
thermia in the treatment of patients with severe middle cerebral artery infarction. Stroke 1998, 29:2461–2466.
15. Kasner SE: Acetaminophen for altering body tempera-ture in acute stroke: a randomized clinical trial. Stroke 2002, 33:130–134.
16. Kammersgaard LRB, Jorgensen HS, Reith J, et al.: Feasibility and safety of inducing modest hypo-thermia in awake patients with acute stroke through surface cooling: a case-control study. The Copenhagen Stroke Study. Stroke 2000, 31:2251–2256.
17. Georgiadis DSS, Kollmar R, Schwab S: Endovascular cooling for moderate hypothermia in patients with acute stroke: first results of a novel approach. Stroke 2001, 32:2550–2553.
18. Krieger DW: Cooling acute ischemic brain damage: a randomized pilot trial of endovascular cooling for patients with acute ischemic stroke. Stroke 2003, 34:248A.
19. Lyden P: Phase I study of endovascular-induced hypothermia in patients with acute ischemic stroke. Stroke 2003, 34:249A.
20. Muir KW: Magnesium for neuroprotection in ischaemic stroke: rationale for use and evidence of effectiveness. CNS Drugs 2001, 15:921–930.
21. Ferguson KKC, Starkman S, Saver JL: Hyperacute treatment initiation in neuroprotective stroke trials. Neurology 2002, 58(suppl):A387.

Potential Role of Neuroprotective Agents Ovbiagele et al. 449
22.• Saver JKC, Leary MC, Ovbiagele B, et al.: Results of the Field Administration of Stroke Treatment-Magnesium (FAST-MAG) pilot trial: a study of pre-hospital neuro-protective therapy. Stroke 2002, 33:353.
First of its kind study of prehospital application of neuroprotec-tive therapy for acute ischemic stroke, demonstrating feasibility and significant acceleration of treatment start when compared with in-hospital initiation of neuroprotective therapy.23. Kollmar R: Neuroprotective effect of delayed moderate
hypothermia after focal cerebral ischemia: an MRI study. Stroke 2002, 33:1899–1904.
24. Kammersgaard LP: Admission body temperature predicts long-term mortality after acute stroke: the Copenhagen Stroke Study. Stroke 2002, 33:1759–1762.
25. Bernard SGT, Buist MD, Jones BM, et al.: Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002, 346:557–563.
26. Bradford A, Lees K: Design of the intravenous magnesium efficacy in acute stroke trial (IMAGES). Curr Control Trials Cardiovasc Med 2000, 1:184–190.
27. Saver JWJ: Choline precursors in acute and subacute human stroke: a meta-analysis. Stroke 2002, 33:353.
28. Warach SHK: Dose dependent reduction in infarct growth with citicholine treatment: evidence of neuro-protection in human stroke? Stroke 2002, 33:354.
29. Belayev L: Albumin therapy of transient focal cerebral ischemia: in vivo analysis of dynamic microvascular responses. Stroke 2002, 33:1077–1084.
30. Belayev L: Human albumin therapy of acute ischemic stroke: marked neuroprotective efficacy at moderate doses and with a broad therapeutic window. Stroke 2001, 32:553–560.
31. Ginsberg MD: Adventures in the pathophysiology of brain ischemia: penumbra, gene expression, neuro-protection: the 2002 Thomas Willis lecture. Stroke 2003, 34:214–223.
32. Brines M: What evidence supports use of erythro-poietin as a novel neurotherapeutic? Oncology 2002, 16(suppl):79–89.
33. Ehrenreich HHM, Piotr L, Dembowski C, et al.: Erythro-poietin treatment for acute stroke: a randomized double blind proof of concept trial in man. Stroke 2002, 33:354.
34. Grotta JSR, Aronowski JA: Tx ethanol plus caffeine (caffeinol) neuroprotection for ischemic stroke: further studies in preparation for human trials. Stroke 2002, 33:402.
35.• Lyden P: The Clomethiazole Acute Stroke Study in tissue-type plasminogen activator-treated stroke (CLASS-T): final results. Neurology 2001, 57:1199–1205.
This study is an example of the first generation of combina-tion tissue-type plasminogen activator plus add-on neuro-protective agent trials. Demonstrated the feasibility and safety of adding the neuroprotectant clomethiazole to under 3-hour fibrinolytic therapy in patients with acute ischemic stroke.36. Grotta J: Combination Therapy Stroke Trial: recombi-
nant tissue-type plasminogen activator with/without lubeluzole. Cerebrovasc Dis 2001, 12:258–263.