Embed Size (px)
Citation preview

Address for correspondence:
COHEN-LEVY,255 rue Saint-Honore,75001 Paris,[email protected]
DOI: 10.1051/odfen/2010402 J Dentofacial Anom Orthod 2010;13:317-333� RODF / EDP Sciences
317
Article received: 06-2010Accepted for publication: 07-2010
Posterior mandibular rotations
Julia COHEN-LEVY, Sophie ROZENCWEIG
With the gracious participation
of Professor Jean DELAIRE
RESUME
The morphological particularities of the posteriorly rotated mandible, firstdescribed by A. Bjork, may correspond to extremely variable clinical situations.We can derive important information by analyzing the forms and proportions ofdifferent mandibular entities. This article proposes to illustrate the mostfrequently encountered situations by describing a number of cases ofposterior rotation and by explaining how Delaire’s architectural analysis can beused in clinical practice.
KEYWORDS
Mandible
Condyle
Posterior rotation
Growth.
INTRODUCTION
Mandibular rotations are widely known andfrequently used in determining the prognosisof both vertical and posterior skeletal devia-tions. The typological characteristics of ‘‘pos-terior rotation,’’ considering the 7 points thatBjork2,3,4 initially described, orientation andshape of the mandibular condyles, shape ofthe mandibular symphysis, shape of the loweroccipital border, orientation of the mandibularcanal, and the proportion of the lower third ofthe face, can, nevertheless, refer to verydifferent clinical situations.
In Class II division 1 malocclusions, signsof posterior rotation may reflect weakmandibular growth and, because of it, makethe prognosis for effective functional ther-apy dim. But for certain types of Class IIImalocclusion similar signs may, on the otherhand, accompany a strong growth potentialand minimize the ‘‘real’’ interarch discre-pancy.
According to Moss’s 1968 work, cited byLatrou9, the anatomic mandible is formedfrom the juxtaposition of several functional
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2010402

entities, a systematic analysis ofwhich such as the one proposed byDelaire and Salagnac, makes it possi-ble for practitioners to create moreprecise diagnoses5,6,7,13. These im-proved formulations will be based onthe size of the condyles, which de-pends on genetic influences and adap-tive growth, the size of the coronoidprocesses, a function of the temporalperiosteal matrix, the form and theshape of the gonial region, a function ofthe masseter and the medial ptyergoidmatrix, with respect to the spinalcolumn11,12 and, finally, the orientationof the alveolar processes.
This article will review differentclinical situations described by a mor-phological analysis of the mandible andthen by an orthognathic architecturalconstruction using Delaire’s digitizedanalysis (TridimTM). The results of thesimplified analysis are presented in
graph form with the maxillary arearepresented in the naso-maxillary stagein red, the dento-alveolar area in blackand the mandible in blue. All areconstructed with an ideal relationshipto each subject’s cranial and cervicalmorphology.
For the first case of a severemandibular hyperdivergence, Profes-sor Delaire, the eponymous creator ofthe analysis, himself has prepared acomplete morphological study of theskeletal and pharyngeal structuresthat delineates the deformations andinsufficiencies in the development ofthe different entities as well as thenotion of auxological potential.
We discuss the repercussions suchstudies of the different types ofposterior rotation of the mandible canhave on orthodontic, orthopedic, andsurgical therapy,
PRESENTATION OF CASE NUMBER ONE
This 30 year-old patient suffers froma rare systemic disease, related toskin sclerosis, or scleroderma, calledthe stiff skin syndrome. Small in size,with deformed fingers she walked andseated herself with difficulty. Althoughthe effort was not painful, she couldopen her mouth only to a limitedextent making taking pictures of herteeth (fig. 1 a to g) a troublesomeprocedure.
The stiff skin syndrome is a geneti-cally transmitted disorder that affectsskin and connective tissue throughoutthe body that leads to progressivedecrease in joint mobility, caused,an international team of researchersdiscovered last year, by excessive
production of the protein fibrillin-1and possibly transmitted by a domi-nant autosomic gene1,10.• An oral examination revealed:
– lack of lip closure at rest– a strongly convex facial profile– a ‘‘gummy’’ smile– and a reduced chin to neck
distance
• The patient had a Class I molar
occlusion, almost normal overjetas a result of orthodontic treatmentaccompanied by the extraction ofboth maxillary canines and twolower bicuspids and germectomyof all four third molars that she hadundergone as a teenager.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
318 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations

Analysis of the profilecephalometric X-ray
• The head of the condyle is small,shorter than the coronoid process,and oriented obliquely backward.The posterior border of the ramusis concave and the angle of themandible is positioned higher than
C2-C3 intervertebral disc, open to anexaggerated extent, and with amarked antegonial notch. The sym-physis is high and extremely narrowin it upper sector.
• The apices of the molars are veryclose to the mandibular canal whilethe apices of the incisors are at aconsiderable distance from the border
Figures 1 a to gFacial and intraoral photographs of patient 1, who suffers from the stiff skin syndrome. Note her facial convexity andher inability to close her lips at rest. Her dental occlusion, however, was relatively well balanced.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 319

of the mandible. The occlusal plane istilted vertically, which makes thepatient’s smile almost gummy
• In addition, one can note, a
narrowing of the caliber of the
airways that appear to be shrunkenbehind the base of the tongue. Apartial calcification of the stylo-hyoid ligaments can also be seen.
• An architectural orthognathic
analysis (shown in simplified formin fig. 1 i, and in complete form infig. 1 j) gives a clear picture of theforward position of the condyle,posterior vertical insufficiency,anterior vertical excess, bi-maxillaryretrusion with a short mandible aswell as a Class II skeletal pattern.The analysis presented in figure 1 kquantifies the developmental short-comings of the skeletal compo-nents of the mandible, showinghow it can be a formidable toolfor planning surgical procedures.The tracing depicted in figure 1l focuses on the pharyngeal airway.
What diagnosis has beendelineated?
The shortness of the condyles wascaused by an organic assault on thecondylar blastema that provoked in-sufficient posterior vertical develop-ment, a posterior rotation of the bodyof the mandible, and, finally, repercus-sions affecting the teeth and thealveolar process. In addition to mal-formation syndromes like hemi-facialmicrosomia, the Treacher Collins orGoldenhar syndromes as well asinflammatory, infectious, and trau-matic assaults on the condyles maybe at the root of the problem.
While moderate cases that havelittle clinical effect do exist, other,more serious disorders may, in theirdevelopment, express themselves in
Figure 1 hProfile cephalometric film. Note the signs of markedposterior rotation, thin symphysis and pronouncedantegonial notch.
Figure 1 iSimplified analysis with the ten most important traitsportrayed. The ideal maxillary configuration is shown inblack, and the ideal mandibular in blue in contrast to theactual cranial and cervical morphology of the patient. Themaxillary and mandibular structures are clearly seen intheir retro position in relation to the ideal framework. Theensemble of this patient’s facial complex has rotated in adistinct counter-clockwise fashion.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
320 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations

Figure 1 jHere is the complete architectural and orthog-nathic analysis that Professor Jean Delairehas made of this case.
Figure 1 kProfessor Delaire’s analysis ofthe surfaces of the mandible:interestingly the naso-maxillaryand dento-alveolar regionsshow normal values indicatingthat they have not suffered anydevelopmental insufficiency incontrast to the body and ramiof the mandible.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 321

temporo-mandibular joint ankylosis,intra-articular hemorrhage, condylarfractures, prolonged immobilization ofthe mandible, systemic and localinfections, scleroderma, and spondy-larthritic ankylosis.
What procedures should thepractitioner initiate and whateventual influence will this typeof posterior mandibular rotationhave on orthodontictreatment?
In cases of short rami, traditionalorthognathic surgery could givedisappointing results. The usual treat-ment consists of a sagittal osteotomythat corrects the antero-posterior dis-crepancy but perpetuates the intrinsicmandibular imbalance and gives the
body of the mandible a relative excessof length from the work of ProfessorFerri8).
In this particular case, because ofthe patient’s serious systemic diseaseand in spite of the negative estheticeffects of the malocclusion, we didnot plan any surgical intervention, noteven a genioplasty, because, in thesurgeon ‘s opinion, the difficulties ofintubation and the risk of poor oss-eous consolidation would be toogreat.
On further examination we deter-mined the patient was suffering froma moderate case of obstructive sleepapnea syndrome for which she haddemonstrated no daytime symptoms.She was successfully treated for thisdisorder with non-invasive positivepressure ventilation.
Figure 1 lProfessor Jean Delaire’s analysis of the oro-pharyngeal soft tissues above the hyoid bone.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
322 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations
PRESENTATION OF CASE NUMBER TWO
Here are the basic diagnostic featuresof this case of a 12 year-old femalepatient suffering from Still’s disease,juvenile rheumatoid polyarthritis.• Occlusion:
– asymmetric Class II division 1malocclusion,
– a narrow maxillary arch with across bite of the right buccalteeth,
– all four first molars had beenextracted because of rampant car-ies,
– anterior overjet of 5 mm. Inanterior propulsion patient slidher mandible 2 mm away fromcentric relation.
• Basal bone was in a Class IIrelationship with a retruded mand-ible and hyperdivergent face.
• Treatment
Because of condylar resorption weconsulted Professor Couly’s maxillo-facial surgery service at the NeckerSick Children University Hospital Cen-tre, which graciously agreed to takecare of the patient’s medical needs.
With the approval of our consultants,we began a phase of orthopedic treat-ment with a monobloc activator. Weconcluded with a full banded and bonded30 month treatment, accompanied byhigh pull head gear, to close spaces,coordinate the arches, and to obtain aClass I occlusion (see fig. 2 a to h, beforetreatment, and fig. 2 I to p, aftertreatment).• At a check-up visit ten years after
the end of treatment we found thatthe occlusionhad relapsed to aClass IIrelation, the patient’s profile wasretrusive, and that a molar-to-molaropen bite had appeared. (fig. q to x).
• An architectural analysis beforetreatment delineated the inade-quate vertical development of therami before treatment (fig. 2 y), themaxillary retrusion, and the conti-nuation of the posterior rotation ofthe mandible, with a marked ascen-sion of the mandibular angle duringthe course of treatment that con-tinued until the end of the growthperiod (fig 2 z to z’).
What diagnosis has beendelineated?
Rheumatoid polyarthritis is a chronicinflammatory disease that causes pro-gressive destruction of joints andimposes multiple and, sometimes,profound functional, psychological, so-cial, and, later, professional problemson patients it strikes. It is the mostfrequently occurring and the mostsevere of the inflammatory rheuma-toid diseases, affecting 0.3 to 0.5% ofthe French population. The diseasedevelops in spurts separated by peri-ods of remission. During the acutephases, joints become swollen andpainful and patients suffer frommoderate fever and asthenia. Whenattacks by the disease on both left andright temporo-mandibular joints be-come aggravated they can causedeformities and a crippling destructionof the heads of the condyles.
In this young patient’s case, theearly destructive effect on the headsof the condyles diminished the heightof the rami so that gonion rises inrelation to the lower border of theodontoid process. This also generatesan imbalance of the maxillo-facial
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 323

complex within its framework, mark-edly verticalizing the occlusal plane.
What procedures should thepractitioner initiate and whateventual influence will this typeof posterior mandibular rotationhave on orthodontic treatment?
This kind of severe relapse canbewilder the orthodontist, especially
after such a therapeutic success,which, even more gratifyingly, hadbeen achieved after the end of thepubertal growth spurt.
The brutal appearance of the anterioropen bite reflected a progression of therheumatoid polyarthritis’s disintegrat-ing action on the heads of the condyles,although the persistence of juvenileswallowing may have made a func-tional contribution to the onset of thisunwelcome occlusal development.
Figures 2 a to hFacial and intraoral photographs of patient 2, who is afflicted with rheumatoid polyarthritis before treatment.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
324 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations
As a component of our plan totreat this problem symptomatically,we do not plan to grind the poster-ior inter-arch contacts that protectthe joints, but, instead to constructa thin oral splint that would increase
vertical dimension only slightly butwould have the effect of augment-ing the distribution of the inter-archcontacts.
The increasing severity of the pa-tient’s arthritic disease would make it
Figure 2 i to pThe same patient after treatment. Note the harmonious smile, the well-balanced profile, with overjet and overbitewithin normal limits.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 325

difficult to justify correcting the newClass II relationship and the open bitewith a mandibular osteotomy but wemay consider a genioplasty at some
future time to bring the maxilla tomandible relationship and the unaes-thetic ‘‘chinless’’ profile closer tonormal limits.
Figures 2 q to xFacial and, especially, intraoral photos of the same patient ten years after the end of treatment show the brutalappearance of an open bite that extends from molar to molar associated with a retrusion of menton.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
326 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations

Figure 2 z’Profile cephalometric X-ray taken at the end of growthperiod recall visit.
Figure 2 zProfile cephalometric X-ray at the end of treatment andsimplified architectural analysis.
Figure 2 yProfile cephalometric X-ray and architecturalanalysis before treatment.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 327

PRESENTATION OF CASE NUMBER THREE
This 8 year-old girl consulted usbecause of the delayed eruption of herupper lateral incisors as well as theupper first molars that were blockedunder the second temporary molars.
(fig. 3 a to g). Even though her tonsillartissues were hypertrophied she dis-played no symptoms of otolaryngolo-gical infection or serious otitis.
Figure 3 a to gFacial and intraoral photos of patient 3 who suffers from juvenile obstructive sleep apnea syndrome. She had a Class IImalocclusion, a narrow and retruded maxilla, with bilateral buccal cross bites, and an anterior open bite.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
328 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations
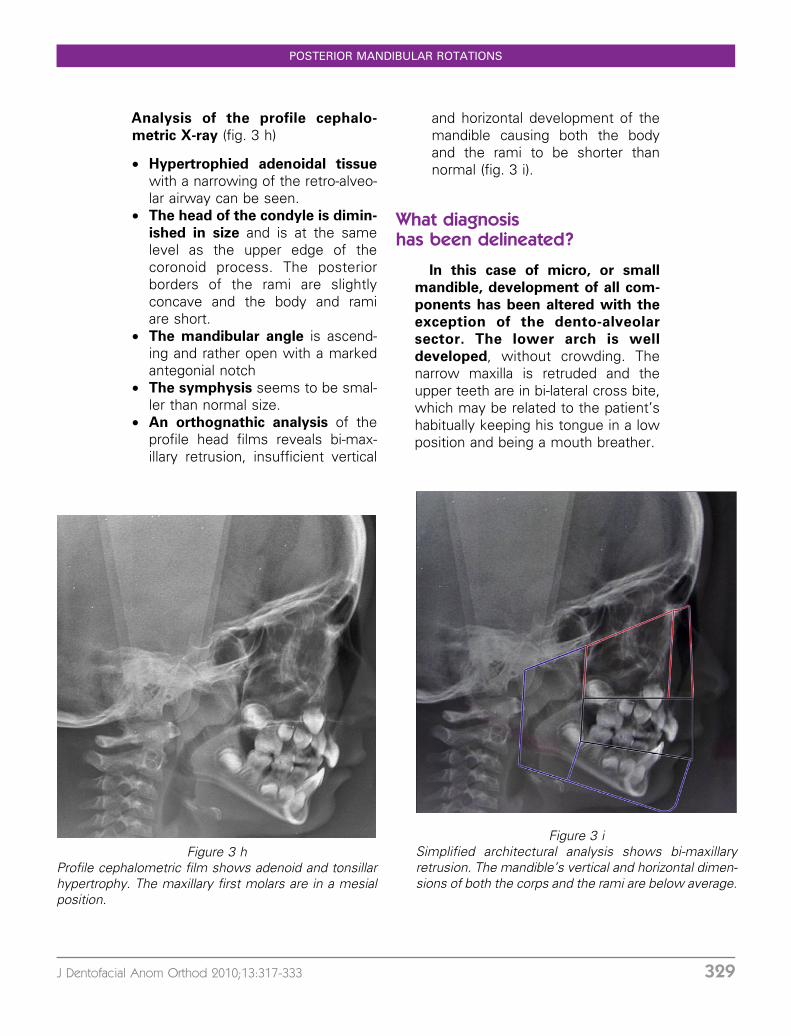
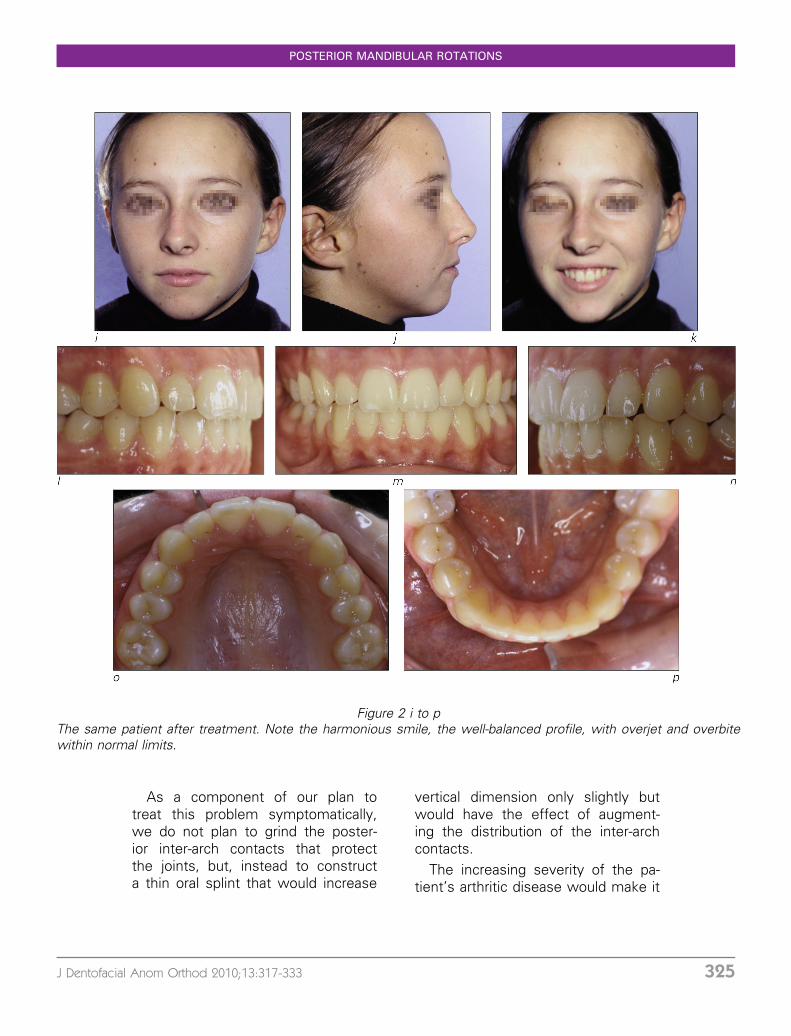
Analysis of the profile cephalo-
metric X-ray (fig. 3 h)
• Hypertrophied adenoidal tissue
with a narrowing of the retro-alveo-lar airway can be seen.
• The head of the condyle is dimin-
ished in size and is at the samelevel as the upper edge of thecoronoid process. The posteriorborders of the rami are slightlyconcave and the body and ramiare short.
• The mandibular angle is ascend-ing and rather open with a markedantegonial notch
• The symphysis seems to be smal-ler than normal size.
• An orthognathic analysis of theprofile head films reveals bi-max-illary retrusion, insufficient vertical
and horizontal development of themandible causing both the bodyand the rami to be shorter thannormal (fig. 3 i).
What diagnosishas been delineated?
In this case of micro, or small
mandible, development of all com-
ponents has been altered with the
exception of the dento-alveolar
sector. The lower arch is well
developed, without crowding. Thenarrow maxilla is retruded and theupper teeth are in bi-lateral cross bite,which may be related to the patient’shabitually keeping his tongue in a lowposition and being a mouth breather.
Figure 3 hProfile cephalometric film shows adenoid and tonsillarhypertrophy. The maxillary first molars are in a mesialposition.
Figure 3 iSimplified architectural analysis shows bi-maxillaryretrusion. The mandible’s vertical and horizontal dimen-sions of both the corps and the rami are below average.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 329

What procedures should thepractitioner initiate and whateventual influence will this typeof posterior mandibular rotationhave on orthodontic treatment?
Because of the patient’s facialretrusion and young age, we decidedto attempt to stimulate growth withorthopedic procedures and to avoidextractions.
After an orthodontic evaluation, werequested a polysomnographic exam-ination. It confirmed what our assess-ment had indicated, that the patient
suffered from a severe case of ob-structive sleep apnea syndrome with
peaks of oxygen desaturation. Afterwe began to treat her with rapidpalatal expansion, the index of ap-nea-hypopnea spontaneously im-proved making a tonsillectomy andadenoidectomy less urgent.
Later, treatment with an activatormay be indicated to stimulate growthof the mandible, whose verticalgrowth, despite the anterior open bite,was inadequate, probably because ofthe tongue’s habitual low and forwardpositioning.
PRESENTATION OF CASE NUMBER FOUR
Surgeons had operated on thisseventeen year-old boy numeroustimes to correct his left labio-alveolar-palatal cleft by closing the oro-nasalopening, performing a uni-lateral Zlabioplasty, and bringing the upper leftcuspid into its place in the arch withsurgico-orthodontic means. His upperleft lateral incisor was congenitallyabsent.
The esthetic repercussions of hisdeformity, which were profound, werecaused by lack of support for his noseand insufficient lateral growth of themaxilla (fig. 4 a to g).
Because of the narrow and retrudedupper arch, there was a bilateral crossbite of the buccal teeth. A severeanterior open bite was present to-gether with asymmetry caused jointlyby the maxillary midline’s drifting tothe left toward the space of themissing lateral incisor and by thelateral deviation of the mandible.
Analysis of the profilecephalometric X-ray (fig. 4 h)
• The head of the condyle is quitelarge with a long and thick neckresembling the coronoid process,which is also over-developed.
• The angle of the mandible is split,lowered on one side, and extremelyopen, with a well-chiseled antego-nial notch.
• The mandibular symphysis israther delicate, with the lowerdental arch seemingly retruded asa compensation for the Class IIImalocclusion.
• Paralleling these features tongue
posture is low, maxillary structureseems to have collapsed with thepre-maxilla rising as a component ofan exaggerated compensatorycurve.
• An orthognathic analysis reveals
a skeletal Class III conformation
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
330 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations

Figures 4 a to gFacial and intraoral photographs of patient 4 who had received treatment for a naso-labio-alveolar-palatal cleft. He hada Class III malocclusion with insufficient lateral growth of the maxilla.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 331

with a retruded maxilla, a custom-ary finding in patients with labio-alveolar clefts, a large mandible,antecondylia, and excess anteriorheight (fi. 4 i).
What diagnosis has beendelineated?
Macro-mandibles, which show in-crease of substance in all threedimensions of space, are rare anoma-lies, notably found in cases of acro-megaly. They exhibit very strongcondylar growth, a phenomenon thatoften generates a Class III mal-occlu-sion that is likely to be asymmetrical.The lowering of the mandibular angletoward the second cervical vertebra (C2) reflects excess of posterior verticalheight, a finding that does not seem toobtain in this particular case.
The architectural analysis revealsthat this patient does not have a truemacro-mandible but, instead, ante-riorly placed condyles in addition toan excessively long mandibular bodyor dolicho mandible.
What procedures should thepractitioner initiate and whateventual influence will this typeof posterior mandibular rotationhave on orthodontic treatment?
In cases of true hypercondylia, asingle or bilateral condylectomy isstrongly indicated. On the other hand,when the mandibular angle is locatedabove the C 2 vertebra, this is usuallya sign of vertical posterior insuffi-ciency.
Figure 4 iThis simplified architectural analysis shows the exces-sively long body of this mandible that extends verticallybeyond the ‘‘ideal’’ framework but whose rami seem toconform better to the standard dimensions. The under-developed maxilla has an ascending anterior portion.
Figure 4 hThe mandible is long and massive and shows markedsigns of posterior rotation.
JULIA COHEN-LEVY, SOPHIE ROZENCWEIG, JEAN DELAIRE
332 Cohen-Levy J, Rozencweig S, Delaire J. Posterior mandibular rotations
CONCLUSION
Like cats, all images of posteriorrotation may look gray in the dark, butafter a careful morphological analysis,effectively completed by an architec-tural construction, mandibles all havetheir own specific characteristics andthe orthodontic, orthopedic, and surgi-cal therapeutics for treating posteriorrotation are numerous.
We invite our readers to intensifytheir understanding of the subject byreading the principal works of Profes-sors Jean Delaire, Mercier, and Salag-nac, whose studies have been theprimary inspiration for these lines.
REFERENCES
1. Azevedo VF, Serafini SZ, Werner B, Muller CS, Franchini CF, Morais RL. Stiff skinsyndrome versus scleroderma: a report of two cases. Clin Rheumatol. 2009Sep;28(9):1107–1111. Epub 2009 May 5.
2. Bjork A. Variation in the growth pattern of the human mandible. A longitudinalradiograph study by the implant method. J Dent Res 1963;42:400–411.
3. Bjork A. Prediction of mandibular growth rotation. Am J Orthod 1969;55:585–599.4. Bjork A. Croissance mandibulaire normale et pathologique. Synthese d’etudes
cephalometriques longitudinales a l’aide d’implants sur une periode de 25 ans. RevOrthop Dento Faciale 1981;18:9–63.
5. Delaire J. L’analyse architecturale et structurale craniofaciale. Principes theoriques.Quelques exemples d’emploi en chirurgie maxillo-faciale. Rev Stomatol 1978;79:1–33.
6. Delaire J. L’equilibre architectural craniofacial en ODF et en chirurgie orthognathique.Orthod Fr 1985;85:353–364.
7. Delaire J. Le role du condyle dans la croissance de la machoire inferieure et dansl’equilibre de la face. Rev Chir Maxillofac 1990;91:179–192.
8. Ferri J, Movaghar R, Movaghar AS. Les insuffisances verticales posterieures de lamandibule : presentation d’une nouvelle technique de correction et etude retro-spective de 15 cas. Int Orthod 2007;5:98–110.
9. Lautrou A. Croissance faciale : theories explicatives et clinique orthodontique. RevOrthop Dento Faciale 1994;28:433–453.
10. Liu T, McCalmont TH, Frieden IJ, Williams ML, Connolly MK, Gilliam AE. The stiff skinsyndrome: case series, differential diagnosis of the stiff skin phenotype, and review ofthe literature. Arch Dermatol 2008 Oct;144(10):1351–1359.
11. Mercier J. L’interet de l’etude des rapports mandibulo-rachidiens dans l’indicationoperatoire en chirurgie orthognathique. Rev Orthop Dento Faciale 2007;41:461–477.
12. Mercier J, Gordeeff A, Delaire J. Les alterations de la dimension verticale posterieurede la face. Facteurs etiopathogeniques, criteres architecturaux et aspects therapeu-tiques. Orthod Fr 1989;60 Pt 2:575–582.
13. Salagnac JM, Delaire J, Mercier J. Developpement vertical de la face et du rachiscervical. Interets diagnostique et therapeutique en ODF et en chirurgie maxillo-faciale.Rev Stomatol Chir Maxillofac 1999;100:13–26.
POSTERIOR MANDIBULAR ROTATIONS
J Dentofacial Anom Orthod 2010;13:317-333 333