Embed Size (px)
Citation preview

Pneumothorax spontané :
Stratégie de prise en charge aux urgences
1
Thibaut DESMETTRE MD, PhD
Pôle Urgences/Réanima2on Médicale/SAMU
CHRONO ENVIRONNEMENT UMR 6249
Toulouse, 28 septembre 2018

Pas de liens ni conflits d’intérêt
en rapport avec la présentaCon
2

Médecine d’urgence et pneumothorax
⇒ Services d’Urgences : mode d’arrivée des paCents
⇒ UrgenCstes impliqués :
§ dans le diagnos<c et ses méthodes
§ dans la stratégie thérapeuCque
§ dans les gestes thérapeuCques
§ Dans la filière de prise en charge
3

Enjeux et problémaCques posés par les pneumothorax spontanés ?
• Epidémiologie : mal connue
• Nosologique : évoluCf
• Diagnos<que : plusieurs classificaCons
• Thérapeu<que : plusieurs écoles – Absence de consensus naConal et internaConal
– Caractère mul<disciplinaire de la prise en charge
4

Travaux sur la thémaCque du pneumothorax spontané UMR 6249 CNRS/Université de Franche Comté
EXPRED
Etude prospec<ve randomisée mul<centrique de non infériorité dans 28 centres en France De 2009 à 2015 Critère d’inclusion: 1er épisode de PSP de grande taille Objec<f principal: comparer l’efficacité immédiate (H24) d’une exsuffla<on simple par rapport au drainage thoracique
EXP-‐PI
Etude transversale rétrospec<ve mul<centrique dans 14 centres en France De 2009 à 2013 Critère d’inclusion: PSP et PSS Objec<f principal: décrire l’épidémiologie des PS
EXP-‐PO et EXP-‐PAT
Etude cas croisé dans 14 centres en France De 2009 à 2013 Critère d’inclusion: 1er épisode de PSP Objec<f principal: déterminer le lien entre la survenue de PSP et -‐ les varia<ons de pression atmosphérique -‐ La pollu<on
Etude des FDR de récidives de PSP
Prise en charge thérapeuCque du PS aux urgences
EvaluaCon médicoéconomique de 2 stratégies thérapeuCques du PSP
5

Conséquences de l’irrup2on d’air dans l’espace pleural ?
Plusieurs facteurs déterminants sur la tolérance : • mécanisme du PNO • taille du PNO (minime, parCel, complet) • terrain sous jacent (pathologie respiratoire) • lésions associées traumaCques
Conséquences = variables ! • De l’absence de retenCssement respiratoire ... • À un tableau d’insuffisance aiguë ou de détresse Hyperpression intra-‐thoracique = pneumothorax suffocant, par :
⇒ compression des cavités cardiaques droites ⇒ gène au retour veineux ⇒ signes de cœur pulmonaire aigu avec retenCssement hémodynamique et
hypotension artérielle.
6

Pneumothorax (PNO) = présence d’air dans l’espace pleural PNO spontanés (non trauma2ques)
PNO spontané primaire idiopathique bénin du sujet jeune PNO spontané secondaire survenant sur un poumon pathologique
PNO trauma2ques classés selon le mécanisme :
-‐ trauma<sme thoracique direct ou indirect
-‐ PNO iatrogène, conséquence d’une procédure ou d’un geste médical :
Défini<on/classement
7

• trois registres naConaux du Royaume-‐Uni • tous les cas de pneumothorax avec ou sans admission à
l'hôpital entre 1991 et 1995 • taux annuels combinés de pneumothorax (primaire et
secondaire) : Ø 24 pour 100 000 chez les hommes Ø 9,8 pour 100 000 chez les femmes
Epidémiologie
8

Epidémiologie
c
Gupta et al. Thorax 2000
9
En France, données PMSI
• 2008 à 2011 (via PMSI) • Âge ≥ 14 ans + hospitalisés + diagnosCc de PNO non-‐traumaCque
• 59 637 séjours à l'hôpital = 42 595 paCents, • 28% ré-‐hospitalisés au moins une fois au cours des 4 ans • Taux annuel de pneumothorax : 22,7 pour 100 000 • raCo femmes/hommes de 1/3,3
Thorax 2015. doi:10.1136/thoraxjnl-‐2014-‐206577
10
Epidémiologie

Facteurs de risque
Tabagisme
Etude rétrospecCve de Stockholm :
=> tabagisme chez 138 paCents fumeurs hospitalisés sur durée 10 ans
=> comparaison avec échanCllon aléatoire contemporain de la même région
• Par rapport aux non fumeurs, risque relaCf d'un premier PNO spontané :
X 9 chez les femmes
X 22 fois chez les hommes
Bense et al. Chest. 1987;92:1009-‐12.
11

• grandes bulles périphériques
mulCples au sommet du poumon
• sans dommages parenchymateux
importants par ailleurs
Fumée de cannabis ? associée à maladie bulleuse +++
12

Facteurs environnementaux ?
Etude de Gupta et Bobbio : pas de variaCon saisonnière Pour certains : survenue en cluster hypothèse des changements de pression atmosphérique (Alifano) ? Hypothèse des niveaux de polluCon de l'air (Bertolaccini) ?
Alifano et al. Chest 2007; 131: 1877–1882. Bertolaccini et al. J Thorac Dis 2010; 2: 9–15.
Taille : faible indice de masse corporelle (IMC)
Withers et al.. Am J Surg 1964; 108: 772–776 Marque^e et al.. Eur Respir J 2006; 27: 470–476.
13
Facteurs de risque

Nosologie
14

pneumothorax primaire,
pneumothorax secondaire,
pneumothorax traumaCque ,
pneumothorax iatrogène
Pneumothorax spontané
absence de toute cause extrinsèque iden<fiée :
§ PSP : absence de maladie cliniquement apparente pulmonaire sous-‐jacente
§ PSS : complicaCon d'une maladie pulmonaire pré-‐existante.
des stratégies de traitement différentes
Enjeux ?
15
Nosologie

16

(3. Nosologie ) MAIS :
… les connaissances évoluent
… dis<nc<on entre PSP et PSS de plus en plus floue….
… possibilité d’anomalies pulmonaires non diagnos<quées en cas de PSP …
=> système de classifica<on différent dans l'avenir ??
Pneumothorax récurrent ou récidivant : PNO survenant après un
pneumothorax homolatéral ou controlatéral. Pneumothorax sous tension : pression intrapleurale > pression atmosphérique AtenCon ! ⇒ paCents sous venClaCon mécanique ⇒ après un traumaCsme ⇒ au décours d’une réanimaCon cardiorespiratoire
Dans le PSP ?? très rare ++ 17

Physiopathologie • Pathogenèse exacte du PSP ? non complètement élucidée • Bulles ipsi ou bilatérales, visualisées :
• Imagerie • Lors de la chirurgie, thoracoscopie
18
Aspects diagnos<ques
Condi<ons survenue du PSP : § au repos (80%) § douleur thoracique (81%) § avec dyspnée (39%)
douleur thoracique pleuré2que brutale, avec ou sans dyspnée, Parfois douleur de l’épaule ou de la pointe de l’omoplate
Incidence des récidives de PSP : entre 17% et 54% dans la première année suivant le pneumothorax Distribu<on d'âge : bimodale PSP : symptômes minimes PSS : dyspnée prédomine Aggrava<on des symptômes très rare : suggère complicaCons ou autre éCologie. 19

Aspects diagnosCques Radiographie thoracique De face, en inspiraCon + radiographie de profil dans les cas difficiles § déplacement de la ligne pleurale § absence de trame vasculaire du poumon entre plèvre viscérale et paroi thoracique
20

21

616 paCents with 807 episodes of PSP :
incidence of BPSP : 1.6% (13 paCents). Lee. Respirology 2008;13:145-‐8
In mul2ple regression analysis : BMI and the presence of bilateral blebs/bullae retained sta@s@cally significant importance lower BMI and smoking were significantly associated with the forma2on of BPSP. Propor2on of bilateral blebs/bullae seen in HRCT was higher in the BPSP group (P = 0.724)
Huang. Thorac Cardiovasc Surg 2007;55:310-‐2
PNO spontané bilatéral
22

Aspects diagnosCques
Tomodensitométrie
• plus sensible que la radio de thorax
• non systémaCque
• cas complexes
• visualisaCon malposiCon de drain
• Intérêt si suspicion de maladie pulmonaire
sous-‐jacente ou cas de chirurgie
A distance : pronosCc récidive ?
ClassificaCon ?
23

24

Aspects diagnosCques
Ultrasons
u Rôle bien établi pour diagnosCc de PNO en traumatologie grave :
-‐ sensibilité 98%, -‐ VPN 82% et VPP de 100%
§ Rendement diagnosCque significaCvement plus élevé avec des US versus Radio Thx, quand scanner uClisé comme examen de référence.
u UClisaCon systémaCque de l'échographie dans le PSP ? pas encore bien établie.
25
• Modes 2D et TM avec une sonde de 5 MHz ( de type cardiologique)
Ø Absence de lignes B + absence de glissement pleural

ACCP : distance apex > 3cm
BTS : distance > 2cm sur Toute hauteur
BSP: de haut en bas
EsCmaCon de la taille du PNO selon ACCP et BTS
26

Prise en charge aux urgences d’un pneumothorax spontané
Consensus NaConal ?
InternaConal ?
Preuves dans la
litérature ?
Chirurgien ? Filière pnemologique ?
Des recommandaCons Françaises ?
27
Aspects thérapeuCques

Aspects thérapeu<ques
Traitement des premiers épisodes de PSP : deux objecCfs 1) évacuaCon de l'air (si nécessaire) 2) prévenCon de la récidive.
1966
586 www.thelancet.com/respiratory Vol 3 July 2015
Series
framework that would provide early triage to patients who can be treated conservatively, those who are suitable for ambulatory management as outpatients, and those who require early intervention. Such a framework would allow availability of a tailored spectrum of options and ensure that invasive treatments are off ered promptly to those at high risk of recurrence.ContributorsOJB and RJH contributed equally to the search and appraisal of relevant studies for inclusion and the initial drafting of the manuscript. AE, DF-K, YCGL, CHM, J-MT, DW, NMR, and NAM reviewed the manuscript and proposed amendments, corrections, and clarifi cations. All authors approved the fi nal version for submission.
Declaration of interestsDF-K reports personal fees from Spiration, outside of the submitted work. DW reports grants from Covidien, outside of the submitted work. NAM reports grants from CareFusion to run the IPC plus study and personal fees to attend a CareFusion advisory board meeting, outside of the submitted work. NMR reports grants and personal fees from Rocket Medical UK, outside of the submitted work. All other authors declare no competing interests.
References1 Kjæergaard H. Spontaneous pneumothorax in the apparently
healthy. Acta Med Scand Suppl 1932; 43: 1–159.2 Hyde B, Hyde L. Spontaneous pneumothorax—contrast of the
benign idiopathic and the tuberculous types. Ann Intern Med 1950; 33: 1373–77.
3 Bense L, Lewander R, Eklund G, et al. Nonsmoking, non-alpha 1-antitrypsin defi ciency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identifi ed by computed tomography of the lungs. Chest 1993; 103: 433–38.
4 Mitlehner W, Friedrich M, Dissmann W. Value of computer tomography in the detection of bullae and blebs in patients with primary spontaneous pneumothorax. Respiration 1992; 59: 221–27.
5 Gupta D, Hansell A, Nichols T, et al. Epidemiology of pneumothorax in England. Thorax 2000; 55: 666–71.
6 Guo Y, Xie C, Rodriguez RM, et al. Factors related to recurrence of spontaneous pneumothorax. Respirology 2005; 10: 378–84.
7 Cottin V, Streichenberger N, Gamondès JP, et al. Respiratory bronchiolitis in smokers with spontaneous pneumothorax. Eur Respir J 1998; 12: 702–04.
8 Cheng YL, Huang TW, Lin CK, et al. The impact of smoking in primary spontaneous pneumothorax. J Thorac Cardiovasc Surg 2009; 138: 192–95.
9 Melton LJ 3rd, Hepper NG, Off ord KP. Infl uence of height on the risk of spontaneous pneumothorax. Mayo Clin Proc 1981; 56: 678–82.
10 Bense L, Eklund G, Wiman LG. Smoking and the increased risk of contracting spontaneous pneumothorax. Chest 1987; 92: 1009–12.
11 Sadikot RT, Greene T, Meadows K, et al. Recurrence of primary spontaneous pneumothorax. Thorax 1997; 52: 805–09.
12 Johnson MK, Smith RP, Morrison D, et al. Large lung bullae in marijuana smokers. Thorax 2000; 55: 340–42.
13 Gill A. Bong lung: regular smokers of cannabis show relatively distinctive histologic changes that predispose to pneumothorax. Am J Surg Pathol 2005; 29: 980–82.
14 Feldman AL, Sullivan JT, Passero MA, et al. Pneumothorax in polysubstance-abusing marijuana and tobacco smokers: three cases. J Subst Abuse 1993; 5: 183–86.
15 Dyhdalo K, Farver C. Pulmonary histologic changes in Marfan syndrome: a case series and literature review. Am J Clin Pathol 2011; 136: 857–63.
16 Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007; 175: 1044.
17 Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax Clin Genet 2008; 74: 178–83.
18 Daniel R, Teba L. Spontaneous pneumothorax and alpha 1-antitrypsin defi ciency. Respir Care 2000; 45: 327–29.
19 Bass HN, LaGrave D, Mardach R, et al. Spontaneous pneumothorax in association with pyridoxine-responsive homocystinuria. J Inherit Metab Dis 1999; 20: 831–32.
20 Johannesma PC, Reinhard R, Kon Y, et al. Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. Eur Respir J 2015; 45: 1191–94.
21 Biffl WL, Narayanan V, Gaudiani JL, et al. The management of pneumothorax in patients with anorexia nervosa: a case report and review of the literature. Patient Saf Surg 2010; 4: 1.
22 Huang TW, Lee SC, Cheng YL, et al. Contralateral recurrence of primary spontaneous pneumothorax. Chest 2007; 132: 1146–50.
23 Alifano M, Roth T, Broët SC, et al. Catamenial pneumothorax: a prospective study. Chest 2003; 124: 1004–08.
24 Joseph J, Sahn SA. Thoracic endometriosis syndrome: new observations from an analysis of 110 cases. Am J Med 1996; 100: 164–70.
25 Bagan P, Berna P, Assouad J, Hupertan V, Le Pimpec Barthes F, Riquet M. Value of cancer antigen 125 for diagnosis of pleural endometriosis in females with recurrent pneumothorax. Eur Respir J 2008; 31: 140–42.
26 Weissberg D, Refaely Y. Pneumothorax: experience with 1,199 patients. Chest 2000; 117: 1279–85.
27 Shamaei M, Tabarsi P, Pojhan, et al. Tuberculosis-associated secondary pneumothorax: a retrospective study of 53 patients. Respir Care 2011; 56: 298–302.
28 Ruckley CV, McCormack RJ. The management of spontaneous pneumothorax. Thorax 1966; 21: 139–44.
29 Stradling P, Poole G. Conservative management of spontaneous pneumothorax. Thorax 1966; 21: 145–49.
30 Baumann MH, Strange C, Heff ner JE, et al, and the AACP Pneumothorax Consensus Group. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest 2001; 119: 590–602.
31 MacDuff A, Arnold A, Harvey J, and the BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65 (suppl 2): ii18–31.
32 Henry M, Arnold T, Harvey J, and the Pleural Diseases Group, Standards of Care Committee, British Thoracic Society. BTS guidelines for the management of spontaneous pneumothorax. Thorax 2003; 58 (suppl 2): ii39–52.
33 Kelly AM, Weldon D, Tsang AY, et al. Comparison between two methods for estimating pneumothorax size from chest x-rays. Respir Med 2006; 100: 1356–59.
34 Northfi eld TC. Oxygen therapy for spontaneous pneumothorax. BMJ 1971; 4: 86–88.
35 De Leyn P, Lismonde M, Ninane V, et al. Belgian Society of Pneumology. Guidelines on the management of spontaneous pneumothorax. Acta Chir Belg 2005; 105: 265–67.
36 Kelly A-M, Druda D. Comparison of size classifi cation of primary spontaneous pneumothorax by three international guidelines: a case for international consensus? Respir Med 2008; 102: 1830–32.
37 Noppen M, Alexander P, Driesen P, et al. Manual aspiration versus chest tube drainage in fi rst episodes of primary spontaneous pneumothorax: a multicenter, prospective, randomized pilot study. Am J Respir Crit Care Med 2002; 165: 1240–44.
38 Wakai A, O’Sullivan RG, McCabe G. Simple aspiration versus intercostal tube drainage for primary spontaneous pneumothorax in adults. Cochrane Database Syst Rev 2007; 1: CD004479.
39 Vedam H, Barnes DJ. Comparison of large- and small-bore intercostal catheters in the management of spontaneous pneumothorax. Intern Med J 2003; 33: 495–99.
40 Clementsen P, Evald T, Grode G, et al. Treatment of malignant pleural eff usion: pleurodesis using a small percutaneous catheter. A prospective randomized study. Respir Med 1998; 92: 593–96.
41 Spector ML, Stern RC. Pneumothorax in cystic fi brosis: a 26-year experience. Ann Thorac Surg 1989; 47: 204–07.
42 Wait MA, Estrera A. Changing clinical spectrum of spontaneous pneumothorax. Am J Surg 1992; 164: 528–31.
586 www.thelancet.com/respiratory Vol 3 July 2015
Series
framework that would provide early triage to patients who can be treated conservatively, those who are suitable for ambulatory management as outpatients, and those who require early intervention. Such a framework would allow availability of a tailored spectrum of options and ensure that invasive treatments are off ered promptly to those at high risk of recurrence.ContributorsOJB and RJH contributed equally to the search and appraisal of relevant studies for inclusion and the initial drafting of the manuscript. AE, DF-K, YCGL, CHM, J-MT, DW, NMR, and NAM reviewed the manuscript and proposed amendments, corrections, and clarifi cations. All authors approved the fi nal version for submission.
Declaration of interestsDF-K reports personal fees from Spiration, outside of the submitted work. DW reports grants from Covidien, outside of the submitted work. NAM reports grants from CareFusion to run the IPC plus study and personal fees to attend a CareFusion advisory board meeting, outside of the submitted work. NMR reports grants and personal fees from Rocket Medical UK, outside of the submitted work. All other authors declare no competing interests.
References1 Kjæergaard H. Spontaneous pneumothorax in the apparently
healthy. Acta Med Scand Suppl 1932; 43: 1–159.2 Hyde B, Hyde L. Spontaneous pneumothorax—contrast of the
benign idiopathic and the tuberculous types. Ann Intern Med 1950; 33: 1373–77.
3 Bense L, Lewander R, Eklund G, et al. Nonsmoking, non-alpha 1-antitrypsin defi ciency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identifi ed by computed tomography of the lungs. Chest 1993; 103: 433–38.
4 Mitlehner W, Friedrich M, Dissmann W. Value of computer tomography in the detection of bullae and blebs in patients with primary spontaneous pneumothorax. Respiration 1992; 59: 221–27.
5 Gupta D, Hansell A, Nichols T, et al. Epidemiology of pneumothorax in England. Thorax 2000; 55: 666–71.
6 Guo Y, Xie C, Rodriguez RM, et al. Factors related to recurrence of spontaneous pneumothorax. Respirology 2005; 10: 378–84.
7 Cottin V, Streichenberger N, Gamondès JP, et al. Respiratory bronchiolitis in smokers with spontaneous pneumothorax. Eur Respir J 1998; 12: 702–04.
8 Cheng YL, Huang TW, Lin CK, et al. The impact of smoking in primary spontaneous pneumothorax. J Thorac Cardiovasc Surg 2009; 138: 192–95.
9 Melton LJ 3rd, Hepper NG, Off ord KP. Infl uence of height on the risk of spontaneous pneumothorax. Mayo Clin Proc 1981; 56: 678–82.
10 Bense L, Eklund G, Wiman LG. Smoking and the increased risk of contracting spontaneous pneumothorax. Chest 1987; 92: 1009–12.
11 Sadikot RT, Greene T, Meadows K, et al. Recurrence of primary spontaneous pneumothorax. Thorax 1997; 52: 805–09.
12 Johnson MK, Smith RP, Morrison D, et al. Large lung bullae in marijuana smokers. Thorax 2000; 55: 340–42.
13 Gill A. Bong lung: regular smokers of cannabis show relatively distinctive histologic changes that predispose to pneumothorax. Am J Surg Pathol 2005; 29: 980–82.
14 Feldman AL, Sullivan JT, Passero MA, et al. Pneumothorax in polysubstance-abusing marijuana and tobacco smokers: three cases. J Subst Abuse 1993; 5: 183–86.
15 Dyhdalo K, Farver C. Pulmonary histologic changes in Marfan syndrome: a case series and literature review. Am J Clin Pathol 2011; 136: 857–63.
16 Toro JR, Pautler SE, Stewart L, et al. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 families with Birt-Hogg-Dubé syndrome. Am J Respir Crit Care Med 2007; 175: 1044.
17 Ren HZ, Zhu CC, Yang C, et al. Mutation analysis of the FLCN gene in Chinese patients with sporadic and familial isolated primary spontaneous pneumothorax Clin Genet 2008; 74: 178–83.
18 Daniel R, Teba L. Spontaneous pneumothorax and alpha 1-antitrypsin defi ciency. Respir Care 2000; 45: 327–29.
19 Bass HN, LaGrave D, Mardach R, et al. Spontaneous pneumothorax in association with pyridoxine-responsive homocystinuria. J Inherit Metab Dis 1999; 20: 831–32.
20 Johannesma PC, Reinhard R, Kon Y, et al. Prevalence of Birt-Hogg-Dubé syndrome in patients with apparently primary spontaneous pneumothorax. Eur Respir J 2015; 45: 1191–94.
21 Biffl WL, Narayanan V, Gaudiani JL, et al. The management of pneumothorax in patients with anorexia nervosa: a case report and review of the literature. Patient Saf Surg 2010; 4: 1.
22 Huang TW, Lee SC, Cheng YL, et al. Contralateral recurrence of primary spontaneous pneumothorax. Chest 2007; 132: 1146–50.
23 Alifano M, Roth T, Broët SC, et al. Catamenial pneumothorax: a prospective study. Chest 2003; 124: 1004–08.
24 Joseph J, Sahn SA. Thoracic endometriosis syndrome: new observations from an analysis of 110 cases. Am J Med 1996; 100: 164–70.
25 Bagan P, Berna P, Assouad J, Hupertan V, Le Pimpec Barthes F, Riquet M. Value of cancer antigen 125 for diagnosis of pleural endometriosis in females with recurrent pneumothorax. Eur Respir J 2008; 31: 140–42.
26 Weissberg D, Refaely Y. Pneumothorax: experience with 1,199 patients. Chest 2000; 117: 1279–85.
27 Shamaei M, Tabarsi P, Pojhan, et al. Tuberculosis-associated secondary pneumothorax: a retrospective study of 53 patients. Respir Care 2011; 56: 298–302.
28 Ruckley CV, McCormack RJ. The management of spontaneous pneumothorax. Thorax 1966; 21: 139–44.
29 Stradling P, Poole G. Conservative management of spontaneous pneumothorax. Thorax 1966; 21: 145–49.
30 Baumann MH, Strange C, Heff ner JE, et al, and the AACP Pneumothorax Consensus Group. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. Chest 2001; 119: 590–602.
31 MacDuff A, Arnold A, Harvey J, and the BTS Pleural Disease Guideline Group. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65 (suppl 2): ii18–31.
32 Henry M, Arnold T, Harvey J, and the Pleural Diseases Group, Standards of Care Committee, British Thoracic Society. BTS guidelines for the management of spontaneous pneumothorax. Thorax 2003; 58 (suppl 2): ii39–52.
33 Kelly AM, Weldon D, Tsang AY, et al. Comparison between two methods for estimating pneumothorax size from chest x-rays. Respir Med 2006; 100: 1356–59.
34 Northfi eld TC. Oxygen therapy for spontaneous pneumothorax. BMJ 1971; 4: 86–88.
35 De Leyn P, Lismonde M, Ninane V, et al. Belgian Society of Pneumology. Guidelines on the management of spontaneous pneumothorax. Acta Chir Belg 2005; 105: 265–67.
36 Kelly A-M, Druda D. Comparison of size classifi cation of primary spontaneous pneumothorax by three international guidelines: a case for international consensus? Respir Med 2008; 102: 1830–32.
37 Noppen M, Alexander P, Driesen P, et al. Manual aspiration versus chest tube drainage in fi rst episodes of primary spontaneous pneumothorax: a multicenter, prospective, randomized pilot study. Am J Respir Crit Care Med 2002; 165: 1240–44.
38 Wakai A, O’Sullivan RG, McCabe G. Simple aspiration versus intercostal tube drainage for primary spontaneous pneumothorax in adults. Cochrane Database Syst Rev 2007; 1: CD004479.
39 Vedam H, Barnes DJ. Comparison of large- and small-bore intercostal catheters in the management of spontaneous pneumothorax. Intern Med J 2003; 33: 495–99.
40 Clementsen P, Evald T, Grode G, et al. Treatment of malignant pleural eff usion: pleurodesis using a small percutaneous catheter. A prospective randomized study. Respir Med 1998; 92: 593–96.
41 Spector ML, Stern RC. Pneumothorax in cystic fi brosis: a 26-year experience. Ann Thorac Surg 1989; 47: 204–07.
42 Wait MA, Estrera A. Changing clinical spectrum of spontaneous pneumothorax. Am J Surg 1992; 164: 528–31.
Approche chirurgicale Approche conservatrice
28

ACCP
(consensus Delphi de 2001) : approche plus agressive ⇒ drainage thoracique intercostal si taille PNO > 20% de l'hémithorax quels que soient les symptômes
Aspects thérapeuCques
BTS
Depuis recos de 2010 : approche basée principalement sur les symptômes cliniques
29
2016

L’exsufflaCon en urgence
• Pneumothorax sous tension pression intrapleurale > pression atm
• Pneumothorax compressif = détresse respiratoire et/ou hémodynamique
⇒ paCents sous venClaCon mécanique ⇒ après un traumaCsme ⇒ au décours d’une réanimaCon cardiorespiratoire
=> Impose un geste de sauvetage immédiat => objecCf :
-‐ supprimer l’hyperpression intra – thoracique -‐ amener la pression pleurale à la pression atmosphérique
30

31

32
Exsuffla<on en urgence
32

ExsufflaCon avec un Kit dédié
Trousse pour Thoracentèse Permet l’évacuation d’épanchements liquidiens (au moyen de la poche de recueil) ou gazeux, soit par aspiration simple, soit avec aspiration murale
diamètre CH 8 , soit 2,7 mm
33

Aiguille et cathéter de thoracentèse avec témoin coloré
A
B
C
34
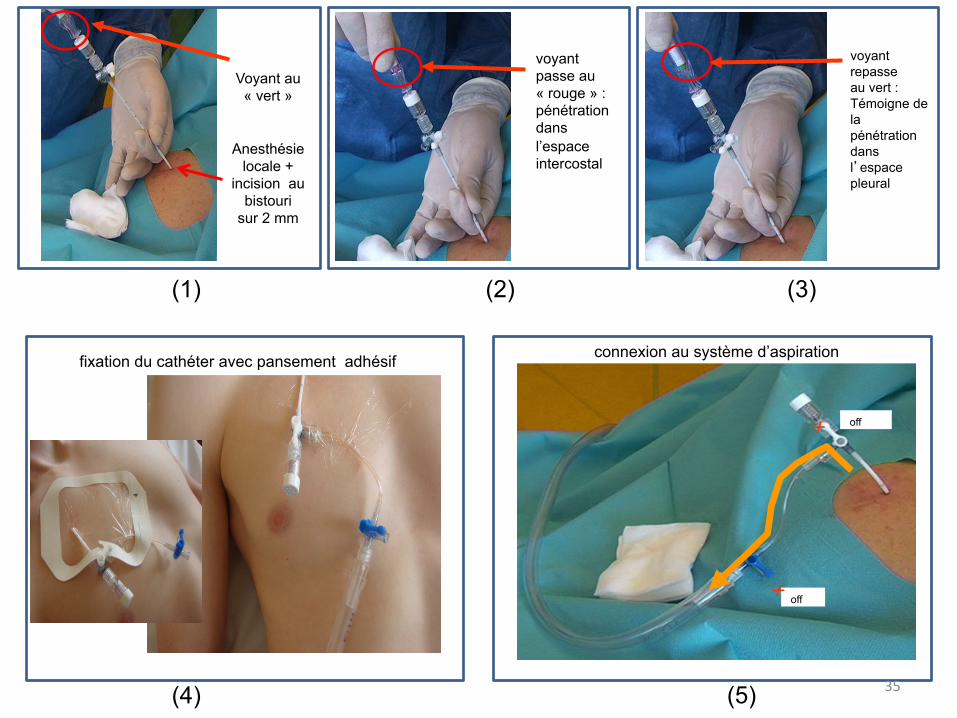
Voyant au « vert »
Anesthésie locale +
incision au bistouri
sur 2 mm
voyant passe au « rouge » : pénétration dans l’espace intercostal
voyant repasse au vert : Témoigne de la pénétration dans l’espace pleural
fixation du cathéter avec pansement adhésif
off
off
connexion au système d’aspiration
(1) (2) (3)
(4) (5) 35

“mini” valve de Heimlich
Taux de succès immédiats et à un an de 69 et 51%
Needle aspiration as first line management of primary spontaneous pneumothorax Camuset j, Laganier J, Brugière O, Dauriat G, Jebrak G, Thabut G. Presse Med 2006;35:765-8 Simplified stepwise management of primary spontaneous pneumothorax : a pilot study Marquette CH, Marx A, Leroy S, Vaniet F, Ramon P, Caussade S, Smaiti N, Bonfils C. Eur Respir J 2006;27:470-76
Prise en charge ambulatoire
36
37
without and with the 11 patients lost to follow-up (worst case).Statistical significance was considered when P<.05. Statisticalsoftware used was R (version 2.15.2; R Core Team, Vienna,Austria).
RESULTSCharacteristics of Study Subjects
We included all 132 consecutive large spontaneouspneumothoraces, detailed in Figure 2. No pneumothoraces weremissed because pulmonologists were on call and could becontacted day and night if a patient presented with a largespontaneous pneumothorax. The clinical characteristics of thepatients are detailed in Table 1. The mean age of our patients was32 years (SD 15; range 16 to 82 years). The mean duration ofpigtail drainage was 3.4 days (SD 1.8; range 1 to 12 days).
Main ResultsThe 22 secondary spontaneous pneumothoraces concerning 18
patients (4 patients with a first episode of secondary spontaneous
pneumothorax displayed 1 recurrence during the study period)managed in our center were divided as follows: 16 patients withemphysema (including only 1 patient who had received a diagnosisbefore the pneumothorax), 1 patient with bilateral community-acquired pneumonia and positive pneumococcal urinary antigen,and 1 patient with breast cancer and pulmonary metastases.
Of the 132 patients managed with a pigtail catheter, 103 weremanaged exclusively as outpatients, with full resolution of thepneumothorax by day 2 or 4, which represents an ambulatorysuccess rate of 78% (95% CI 71% to 85%) (Figure 3).
A total of 121 patients with spontaneous pneumothoraceswere initially managed as outpatients and the other 11 withpneumothoraces were hospitalized (Figure 3). Seven of thehospitalized patients were discharged at day 2, with fullresolution by day 2 or 4, which represents a total success rateof pigtail catheter with 1-way valve at day 4 of 83% (95% CI77% to 89%; Table 2).
Of these 7 patients, 2 were observed for 48 hours because theywere the first patients to be treated with a pigtail catheter inour center. The treatment was successful, and they were
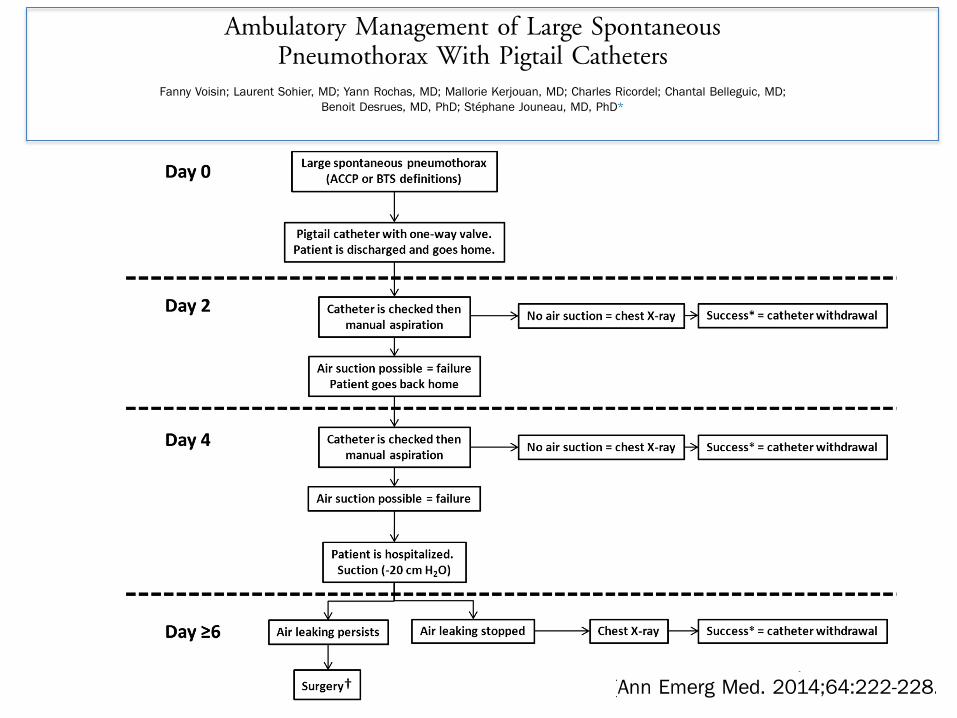
Figure 1. Therapeutic algorithm used in our study for ambulatory management of spontaneous pneumothorax. The catheter’scheckup consisted of the absence of tube torsion, the right position of the 3-way stopcock, and the permeability of the 1-way valve.*Success was defined as previously reported5: complete lung expansion or nearly complete lung expansion (only a very small rim ofapical air). †Surgery was the first option, depending on the patient’s health status (able to undergo surgery) and agreement to theprocedure. ACCP, American College of Chest Physicians; BTS, British Thoracic Society.
Ambulatory Management of Large Spontaneous Pneumothorax Voisin et al
224 Annals of Emergency Medicine Volume 64, no. 3 : September 2014
Ambulatory Management of Large SpontaneousPneumothorax With Pigtail Catheters
Fanny Voisin; Laurent Sohier, MD; Yann Rochas, MD; Mallorie Kerjouan, MD; Charles Ricordel; Chantal Belleguic, MD;Benoit Desrues, MD, PhD; Stéphane Jouneau, MD, PhD*
*Corresponding Author. E-mail: [email protected].
Study objective: There is no consensus about the management of large spontaneous pneumothoraces. Guidelinesrecommend either needle aspiration or chest tube drainage and most patients are hospitalized. We assess theefficiency of ambulatory management of large spontaneous pneumothoraces with pigtail catheters.
Methods: From February 2007 to January 2011, all primary and secondary large spontaneous pneumothoraces fromLorient’s hospital (France) were managed with pigtail catheters with a 1-way valve. The patients were dischargedimmediately and then evaluated every 2 days according to a specific algorithm.
Results: Of the 132 consecutive patients (110 primary, 22 secondary), 103 were exclusively managed as outpatients,with full resolution of the pneumothorax by day 2 or 4, which represents an ambulatory success rate of 78%. Mean time(SD) of drainage was 3.4 days (1.8). Seven patients were initially hospitalized but quickly discharged and had fullresolution by day 2 or 4, leading to a total success rate of 83%. The use of analgesics was low. The 1-year recurrencerate was 26%. If successful, this outpatient management is potentially cost saving, with a mean cost of $926, assumingup to 2 outpatient visits and 1 chest radiograph, compared with $4,276 if a chest tube was placed and the patient wasadmitted to the hospital for 4 days.
Conclusion: Ambulatory management with pigtail catheters with 1-way valves could be a reasonable first-line oftreatment for large spontaneous pneumothoraces. Compared with that of other studies, our protocol does not requirehospitalization and is cost saving. [Ann Emerg Med. 2014;64:222-228.]
Please see page 223 for the Editor’s Capsule Summary of this article.
A feedback survey is available with each research article published on the Web at www.annemergmed.com.A podcast for this article is available at www.annemergmed.com.
0196-0644/$-see front matterCopyright © 2014 by the American College of Emergency Physicians.http://dx.doi.org/10.1016/j.annemergmed.2013.12.017
SEE EDITORIAL, P. 229.
INTRODUCTIONBackground
Spontaneous pneumothoraces are common1; however, thereis no consensus about their management. Three major articlescontain guidelines for the management of spontaneouspneumothoraces, but they differ both in definition andmanagement of large spontaneous pneumothoraces.2-4 Althoughthe American College of Chest Physicians recommends theuse of small-bore catheters, the British Thoracic Society andBelgian Society of Pulmonary Diseases recommend needleaspiration as the first step, followed by chest tube drainage in caseof at least 1 unsuccessful needle aspiration attempt.
ImportancePigtail catheters are worth investigating as a treatment
procedure for managing pneumothoraces because of their
limited invasiveness. Marquette et al5 published a pilot studyin 2006 with a simplified management of primary spontaneouspneumothoraces in hospitalized patients, using a small-caliberindwelling catheter connected to a 1-way Heimlich valve. Thesame group recently published a study of a series of 48 patientswith a first episode of large primary spontaneous pneumothoracestreated with pigtail catheter and 1-way valve, in which 18 (37%)were treated as outpatients, with good efficiency and safety.6 Otherstudies with approximately 50 patients each have shown thatambulatory management of primary spontaneous pneumothoracesusing small catheters connected to a 1-way valve is possible.7-10
Goals of This InvestigationWe report here a series of 132 patients with both primary and
secondary spontaneous pneumothoraces treated in an ambulatorysetting with pigtail catheters. Our aims were to assess thesuccess rate of exclusive outpatient management of spontaneouspneumothoraces (primary outcome) and evaluate 1-year
222 Annals of Emergency Medicine Volume 64, no. 3 : September 2014
PULMONARY/ORIGINAL RESEARCH
Ambulatory Management of Large SpontaneousPneumothorax With Pigtail Catheters
Fanny Voisin; Laurent Sohier, MD; Yann Rochas, MD; Mallorie Kerjouan, MD; Charles Ricordel; Chantal Belleguic, MD;Benoit Desrues, MD, PhD; Stéphane Jouneau, MD, PhD*
*Corresponding Author. E-mail: [email protected].
Study objective: There is no consensus about the management of large spontaneous pneumothoraces. Guidelinesrecommend either needle aspiration or chest tube drainage and most patients are hospitalized. We assess theefficiency of ambulatory management of large spontaneous pneumothoraces with pigtail catheters.
Methods: From February 2007 to January 2011, all primary and secondary large spontaneous pneumothoraces fromLorient’s hospital (France) were managed with pigtail catheters with a 1-way valve. The patients were dischargedimmediately and then evaluated every 2 days according to a specific algorithm.
Results: Of the 132 consecutive patients (110 primary, 22 secondary), 103 were exclusively managed as outpatients,with full resolution of the pneumothorax by day 2 or 4, which represents an ambulatory success rate of 78%. Mean time(SD) of drainage was 3.4 days (1.8). Seven patients were initially hospitalized but quickly discharged and had fullresolution by day 2 or 4, leading to a total success rate of 83%. The use of analgesics was low. The 1-year recurrencerate was 26%. If successful, this outpatient management is potentially cost saving, with a mean cost of $926, assumingup to 2 outpatient visits and 1 chest radiograph, compared with $4,276 if a chest tube was placed and the patient wasadmitted to the hospital for 4 days.
Conclusion: Ambulatory management with pigtail catheters with 1-way valves could be a reasonable first-line oftreatment for large spontaneous pneumothoraces. Compared with that of other studies, our protocol does not requirehospitalization and is cost saving. [Ann Emerg Med. 2014;64:222-228.]
Please see page 223 for the Editor’s Capsule Summary of this article.
A feedback survey is available with each research article published on the Web at www.annemergmed.com.A podcast for this article is available at www.annemergmed.com.
0196-0644/$-see front matterCopyright © 2014 by the American College of Emergency Physicians.http://dx.doi.org/10.1016/j.annemergmed.2013.12.017
SEE EDITORIAL, P. 229.
INTRODUCTIONBackground
Spontaneous pneumothoraces are common1; however, thereis no consensus about their management. Three major articlescontain guidelines for the management of spontaneouspneumothoraces, but they differ both in definition andmanagement of large spontaneous pneumothoraces.2-4 Althoughthe American College of Chest Physicians recommends theuse of small-bore catheters, the British Thoracic Society andBelgian Society of Pulmonary Diseases recommend needleaspiration as the first step, followed by chest tube drainage in caseof at least 1 unsuccessful needle aspiration attempt.
ImportancePigtail catheters are worth investigating as a treatment
procedure for managing pneumothoraces because of their
limited invasiveness. Marquette et al5 published a pilot studyin 2006 with a simplified management of primary spontaneouspneumothoraces in hospitalized patients, using a small-caliberindwelling catheter connected to a 1-way Heimlich valve. Thesame group recently published a study of a series of 48 patientswith a first episode of large primary spontaneous pneumothoracestreated with pigtail catheter and 1-way valve, in which 18 (37%)were treated as outpatients, with good efficiency and safety.6 Otherstudies with approximately 50 patients each have shown thatambulatory management of primary spontaneous pneumothoracesusing small catheters connected to a 1-way valve is possible.7-10
Goals of This InvestigationWe report here a series of 132 patients with both primary and
secondary spontaneous pneumothoraces treated in an ambulatorysetting with pigtail catheters. Our aims were to assess thesuccess rate of exclusive outpatient management of spontaneouspneumothoraces (primary outcome) and evaluate 1-year
222 Annals of Emergency Medicine Volume 64, no. 3 : September 2014
PULMONARY/ORIGINAL RESEARCH

Prise en charge ambulatoire du PNO spontané. Voisin F et al. Université de Rennes, CH Lorient
132 pts – 110 PSP – 22 PSS.
103 pts (78%) exclusivement en ambulatoire avec succès taux de succès à J+4
– 85,4% PSP – 72,7% PSS
38

1) Recommandations de la British Thoracic Society
= approche la moins invasive possible
Exsufflation :
- Tous les PSP symptomatiques
- PSS mesurés à moins de 2 cm / dyspnée minime/ âge inférieur à 50ans ( +
hospitalisation 24h)
Drain thoracique :
- Non régression des symptômes après exsufflation
- PSS sauf si absence de dyspnée et décollement < 1 cm.
Avis chirurgical :
- bullage persistant ou non ré expansion pulmonaire dans les 3 à 5 jours.
39
RecommandaCons ?

2) Recommandations American College of Chest Physicians
en fonction du caractère primitif (PSP) ou secondaire (PSS)
PSP :
PNO de grande taille :
Cliniquement stable : Drainage (Pleurocath – Heimlich - Dispositif d’aspiration)
Cliniquement instable : Drainage (Drains - Dispositif d’aspiration) Persistance d’un bullage : avis chirurgical J4
PSS :
PNO de grande talle : Drainage + VATS après ré expansion
40

ProposiCon d’algorithme de prise en charge du PSP complet
41

freins à la prise en charge ambulatoire ??
1. Le docteurs ne savent pas 2. Les docteurs n’aiment pas le changement 3. Les docteurs ont peur 4. Les docteurs n’aiment pas l’échec 5. Les docteurs n’ont pas le matériel 6. Les données manquent …. 42
Pr CH Marque^e CHU de Nice

Prise en charge aux urgences d’un pneumothorax spontané
Consensus NaConal ?
InternaConal ?
Preuves dans la
litérature ?
Chirurgien ? Filière pneumologique ?
Des recommandaCons Françaises ?
freins à l’exsuffla<on et à la prise en charge
ambulatoire ?
43

Méthodologie
• Etude rétrospec<ve observa<onnelle de 2009 à 2013 dans les services d’urgence de 14 centres hospitaliers en France
• Objec<f principal: décrire le traitement de première inten<on réalisé aux urgences des SP, notamment la part du traitement ambulatoire
En pra2que, sur le terrain, en France ?
EXP-‐PI : épidémiologie et prise en charge du PNO spontané aux urgences
44

Principaux résultats CaractérisCques des paCents présentant un pneumothorax spontané
Caractéristiques
Tous les SP
PSP
PSS
p
N (%) N (%) N (%)
Sexe 0.65
Femme 399 (21.8) 351 (21.6) 48 (23)
Homme 1435 (78.2) 1274 (78.4) 161(77)
Age (années). moyenne (écart type) 33.2 (15.6) 30.4 (12.6) 54.4 (19.9) <0.0001
Tabagisme <0.0001
Fumeur 885 (67.2) 787 (68.3) 98 (60.1)
Ancien fumeur 143 (10.9) 89 (7.7) 54 (33.13)
Non fumeur 288 (21.9) 277 (24) 11 (6.75)
Consommation de cannabis 81 (4.4) 77 (4.7) 4 (1.9) 0.07
Antécédents de pneumothorax 708 (38.5) 619 (37.9) 89 (43) 0.15
45

Signes de gravité: douleur, dyspnée et hypoxémie des SP
Signes de gravité
Tous les PS
N (%)
PSP
N(%)
PSS
N (%)
P
Score de douleur <0,0001
>0 1014 (85,9) 938 (12,7) 76 (28,3)
0 167 (14,1) 137 (87,3) 30 (71,7)
Dyspnée <0,0001
Oui 787 (45,4) 644 (41,9) 143 (27,4)
Non 948 (54,6) 894 (58,1) 54 (27,4)
SpO2 (%) <0,0001
≤90% 52 (3,5) 28 (2,1) 24 (16,7)
>90% 1449 (96,5) 1329 (97,9) 120 (83,3)
46

PSP n=1491
Drainage ou chirurgie ?
ExsufflaCon ?
HospitalisaCon ?
n=915 (61,4%)
ObservaCon n=774 (51,9%)
n =201 (13,5%)
Drainage n=551 (37%) Chirurgie
n=25 (1,6%) HospitalisaCon ?
n = 141 (9,5%)
n = 573 (38,5%) HospitalisaCon ?
n =30 (2%)
n =111 (7,4%)
n=576 (38,6%)
Oui
Oui
Oui Oui
Oui No
Non
Non Non
-‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐-‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐-‐ -‐
Hospitalisa<on
Prise en charge
ambulatoire
Prise en charge des PSP aux urgences
47

PSS n=358
Drainage ou chirurgie ?
ExsufflaCon ?
n=147 (41,1%)
ObservaCon n=93 (15,1%)
n =9 (2,5%)
Drainage n=210 (58,6%)
Chirurgie n=1 (0,3%)
HospitalisaCon ?
n = 54 (15,1%)
n=84 (23,5%)
HospitalisaCon ?
n =54 (15,1%)
n=211 (58,9%)
Oui
Oui
Oui Oui
Oui Non
Non
Non
HospitalisaCon ?
Hospitalisa<on
Prise en charge
ambulatoire
-‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐-‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐-‐ -‐
-‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐-‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐ -‐-‐ -‐
Prise en charge des PSS aux urgences
48

Discussion
Ø Parmi les 1849 PS, le traitement ambulatoire est retenu pour 30 paCents (1,6%)
Ø Limites : caractère rétrospecCf = > pas de données concernant la taille, mais critère non consensuel
Ø Traitement ambulatoire – Un moyen de réduire « l’overcrowding » aux urgences – Bon taux de succès environ 70%
Ø Peu de recours à UHCD malgré les indicaCons (8%)
Ø Place encore prépondérante du drainage thoracique malgré préconisaCon de traitement moins invasif
49
Aspects thérapeuCques Pleurodèse :
Objec<f : réaliser une symphyse pleurale et prévenir la récidive
Méthodes :
§ InsCllaCon d’un irritant chimique (pleurodèse chimique)
§ Abrasion mécanique (pleurodèse mécanique)
§ Abrasion pariétale (pleurectomie)
En Europe : talcage par thoracoscopie
§ Procédure très ancienne, simple et peu couteuse,
§ Effectuée par thoracoscopie et anesthésie locale, ou par VATS § Taux de réussite à long terme après simple talcage thoracoscopique : 93-‐97%
50
Aspects thérapeuCques
Indica<ons d’un traitement défini<f du PSP (pleurodèse) :
§ deuxième épisode de PSP (première récidive)
§ bullage persistant après 3 à 5 jours
§ hémopneumothorax
§ pneumothorax bilatéral
§ professions à risque
51

• Période : juin 2009 -‐ fevrier 2015
• Déroulement étude : – Financement PHRC 2008 – Debut inclusions juin 2009 – Fin des inclusions (n=400) février 2014 – Fin du suivi à un an : février 2015
• Equipes impliquées : – CMC, DRCI, UMR chrono-‐environnement – 30 centres en France (CHU et CHG)
Etude EXPRED Etude mul<centrique, prospec<ve, randomisée, conduite en ouvert et u<lisant un schéma de deux
groupes parallèles Besançon, Dijon, Belfort, Mulhouse, Reims, Nancy,Boulogne/mer, Béthune, Liévin, Hénin-‐Beaumont, Lomme, Roubaix, Tours, PoiCers, Angers, Rouen, Mon�ermeil, Clermont-‐
Ferrand, Saint-‐ECenne, Grenoble, Nîmes, Perpignan, Marseille, Aurillac, Toulouse, Vesoul
Impossible d'afficher l'image. Votre ordinateur manque peut-être de mémoire pour ouvrir l'image ou l'image est endommagée. Redémarrez l'ordinateur, puis ouvrez à nouveau le fichier. Si le x rouge est toujours affiché, vous devrez peut-être supprimer l'image avant de la réinsérer.
52
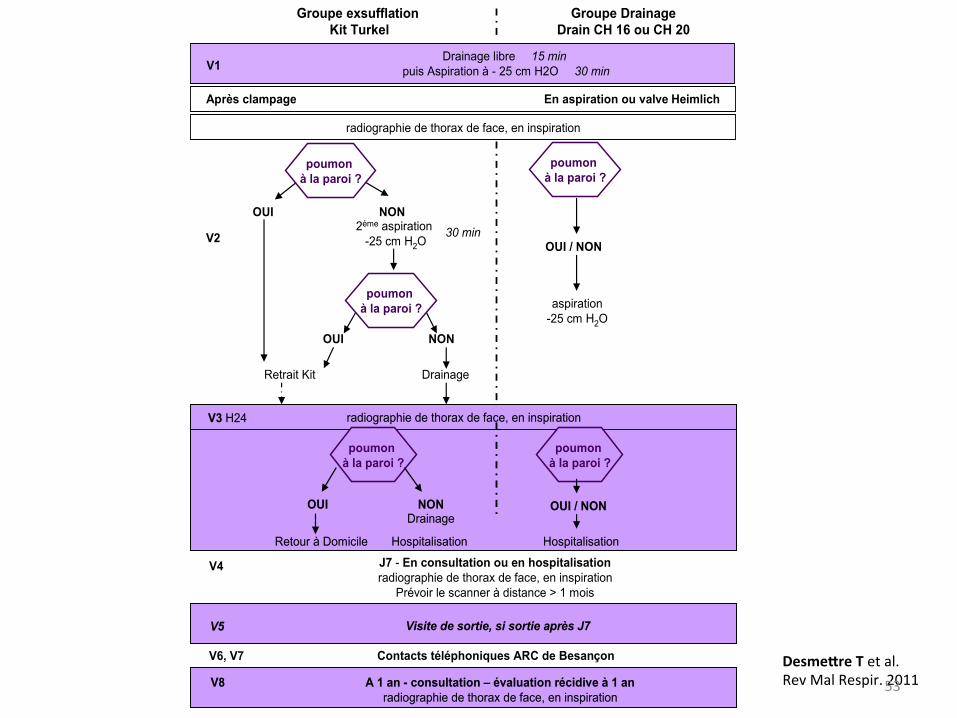
V2
V4
V6, V7
Groupe DrainageDrain CH 16 ou CH 20
Groupe exsufflation Kit Turkel
2éme aspiration -25 cm H2O
NON
DrainageRetrait Kit
NON
OUI
OUI
J7 - En consultation ou en hospitalisationradiographie de thorax de face, en inspiration
Prévoir le scanner à distance > 1 mois
Drainage libre 15 minpuis Aspiration à - 25 cm H2O 30 minV1
Après clampage En aspiration ou valve Heimlich
radiographie de thorax de face, en inspiration
OUI / NON
poumon à la paroi ?
poumon à la paroi ?
poumon à la paroi ?
Contacts téléphoniques ARC de Besançon
aspiration -25 cm H2O
30 min
Visite de sortie, si sortie après J7V5 Visite de sortie, si sortie après J7V5
A 1 an - consultation – évaluation récidive à 1 anradiographie de thorax de face, en inspiration
V8 A 1 an - consultation – évaluation récidive à 1 anradiographie de thorax de face, en inspiration
V8
radiographie de thorax de face, en inspiration
Retour à Domicile Hospitalisation
OUI NON
V3 H24
poumon à la paroi ?
poumon à la paroi ?
Drainage
Hospitalisation
OUI / NON
radiographie de thorax de face, en inspiration
Retour à Domicile Hospitalisation
OUI NON
V3 H24
poumon à la paroi ?
poumon à la paroi ?
Drainage
Hospitalisation
OUI / NON
Desmesre T et al. Rev Mal Respir. 2011 53

1 1 1 3 3 3 3 4 4 5
7 8 8 10 11
13 13 15 15 16
21 21
26
53
65
72
0
10
20
30
40
50
60
70
80
Inclusions par centre
54
29 centres, 402 paCents

Nombre de sujets randomisés : n=402
Bras exsufflaCon: n=200
Bras drainage: n=202
Exclusion (inclus à tort, retrait
consentement, …) : n=12
Exclusion (inclus à tort, retrait
consentement, …) : n=10
Analysables en ITT
Per Protocol
Exclusion pour non respect du bras alloué : n=4
Exclusion pour non respect du bras alloué : n=1
Exclusion pour non respect des
caractérisCques du matériel : n=4
Exclusion pour non respect du bras alloué : n=11
PP strict
N=190 (95%)
N=186 (93%)
N=182 (91%)
n=190 (94,1%)
n=189 (93,6%)
n=178 (88,1%)
Analyse du recollement pulmonaire
à 24h du geste
N=172 (90,5%) N=172 (90,5%) Analyse de la récidive à
1 an
55

Données démographiques et cliniques
Bras Exsuffla<on
Bras Drainage
P value
Age -‐ moyenne (SD) 28,1 (7,3) 27,9 (7,2) 0,79 Hommes/Femmes 153/35 159/31 0,64 IMC (n=351) -‐ n (%) 0,59
Famine et maigreur 33 (18,8%) 26 (14,9%) Corpulence normale 132 (75%) 136 (77,7%)
Surpoids 11 (6,2%) 13 (7,4%) Condi<on survenue -‐ n (%) 0,95
Repos (n=305) 151 (81,2%) 154 (81,5%) Effort (n=70) 35 (18,8%) 35 (18,5%)
Douleur thoracique -‐ n (%) 0,27 Non 6 (3,2%) 2 (1,1%) Oui 181 (96,8%) 187 (98,9%)
Essoufflement -‐ n (%) 0,77 Non 41 (21,9%) 45 (23,7%) Oui 146 (78,1%) 145 (76,3%) 56

Résultats EXPRED • Critère de jugement principal :
Ø Non infériorité a 24h, en ITT et en PP Ø bras exsufflaCon : 66 recollements à 24h avec exsufflaCon seule
• Récidive pneumothorax à un an : Ø pas de différence entre les 2 bras
• Chirurgie à un an : Ø pas de différence entre les 2 bras
57

PerspecCves (1/2)
v Incidence exacte du PSP inconnue v Litérature semble en faveur d’une aspira<on simple iniCalement si 1er PSP
symptomaCque
v Valves de Heimlich :
§ méthode prometeuse
§ permet de proposer alternaCve ambulatoire
§ sous réserve des résultats d’essais contrôlés randomisés
v Le traitement définiCf avec thoracoscopie talcage / pleurectomie :
§ souvent réalisé dans les groupes à risque
§ n’est pas indiqué pour la plupart des paCents en cas de premier épisode
v Arrêt du tabac = seul facteur de risque réversible connu ; le rôle délétère cannabis. 58

• Etude EXPRED : ExsuflaCon en première intenCon : lui donner sa chance ?
• Nécessité de recommanda<ons françaises qui devront s’appuyer sur les résultats de récentes études publiées concernant la stratégie thérapeuCque et les études de terrain
• Impact médico-‐économique des stratégies est un élément clé en l’absence de supériorité d’efficacité des techniques
• Points clés de ces recommanda<ons – indicaCons d’intervenCon en cas de PS – choix de la stratégie thérapeuCque en cas d’intervenCon – condiCons de prise en charge hospitalière ou ambulatoire
59
PerspecCves (2/2)



![Pneumothorax spontané primitifLe pneumothorax est 151 Pneumothorax spontané primitif rarement asymptomatique et de découverte fortuite (47) [niveau de preuve 3] . • Signes de](https://img.dokumen.tips/doc/110x75/607aefc477b78a72dc7e4ffc/pneumothorax-spontan-primitif-le-pneumothorax-est-151-pneumothorax-spontan-primitif.jpg)

























