Embed Size (px)
Citation preview

PLEURAL DISEASEPLEURAL DISEASE
Sevda Özdoğan MD, Sevda Özdoğan MD,
Chest DiseasesChest Diseases

Pleural effusionsPleural effusions EmphyemaEmphyema Pleural malignancyPleural malignancy HemothoraxHemothorax PneumothoraxPneumothorax

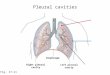
Pleural Anatomy and PhysiologyPleural Anatomy and Physiology
Pleura is a serous membrane formed from Pleura is a serous membrane formed from mesenchyme that separates the lung mesenchyme that separates the lung paranchym, mediastinum, diaphragm and paranchym, mediastinum, diaphragm and thoracic cagethoracic cage
It is composed of 2 layers as:It is composed of 2 layers as: Parietal pleuraParietal pleura Visceral pleuraVisceral pleura

Pleural CavityPleural Cavity
It is the space between the visseral and It is the space between the visseral and parietal pleuraparietal pleura
Normally contains a small amount of fluid Normally contains a small amount of fluid (10-20 ml in each pleural cavity)(10-20 ml in each pleural cavity)
This pleural fluid is mainly produced by the This pleural fluid is mainly produced by the parietal pleural surface and reabsorbed by parietal pleural surface and reabsorbed by the two layers (Mainly parietal pleura)the two layers (Mainly parietal pleura)

The production and reabsorbtion of the pleural fluid is normaly in an equilibrium accounted primarily by the forces employed in Starling equation:
F=k[(Pcap-Ppl)-δ(πcap- πpl)]
F: The rate of fluid movement
P, π: Hydrostatic and oncotic pressures
k: The filtration coefficient
δ: Osmotic reflection coefficient

Pleural EffusionPleural Effusion
If the physiologic balance between the If the physiologic balance between the filtration and the drainage of the pleural filtration and the drainage of the pleural fluid is disturbed, pleural effusion fluid is disturbed, pleural effusion accumulate.accumulate.
Fluid may accumulate in the pleural space Fluid may accumulate in the pleural space in response to the disease of the pleural in response to the disease of the pleural membranes or as a manifestation of a membranes or as a manifestation of a systemic illnesssystemic illness

The Mechanisms of Pleural The Mechanisms of Pleural EffusionEffusion
Increased hydrostatic pressure (Cardiac failure, Increased hydrostatic pressure (Cardiac failure, increased atrial pressure)increased atrial pressure)
Decreased oncotic pressure (Protein deficiency)Decreased oncotic pressure (Protein deficiency) Decreased pleural cavity negative pressure Decreased pleural cavity negative pressure
(Atelectasis)(Atelectasis) Increased permeability in microvascular Increased permeability in microvascular
circulation (İnfections, inflammation)circulation (İnfections, inflammation) Impaired lymphatic drainage of pleural space Impaired lymphatic drainage of pleural space
(Tumor, fibrosis)(Tumor, fibrosis) Transperitoneal route (Congenital defects, Transperitoneal route (Congenital defects,
ascite)ascite)

SymptomsSymptoms
Chest pain (inspiratory)Chest pain (inspiratory) Decreases when the fluid increasesDecreases when the fluid increases
DyspneaDyspnea CoughCough Symptoms of the underlying diseaseSymptoms of the underlying disease
FeverFever HemoptysisHemoptysis Weight lossWeight loss ......

Physical ExaminationPhysical Examination
No physical signs can be detected when No physical signs can be detected when the fluid is less than 300 mlthe fluid is less than 300 ml
İnspectionİnspection İncreased size of the affected hemithoraxİncreased size of the affected hemithorax Trachea is deviated away from the diseased Trachea is deviated away from the diseased
sideside

PalpationPalpation İpsilateral restriction of İpsilateral restriction of
chest wall motion chest wall motion VT absentVT absent
PercussionPercussion Dullness (>300-400 ml)Dullness (>300-400 ml)
OscultationOscultation Diminished breath sounds Diminished breath sounds
or inaudibleor inaudible Pleural friction rubPleural friction rub Bronchial sound over the Bronchial sound over the
fluid levelfluid level

RadiologyRadiology The fluid initially accumulates in the more The fluid initially accumulates in the more
dependent recesses of the thoracic cavity dependent recesses of the thoracic cavity forming a forming a Damoiseau LineDamoiseau Line
200-300 ml of pleural effusion can be detected 200-300 ml of pleural effusion can be detected on standard chest radiograph as blunting of the on standard chest radiograph as blunting of the costophrenic anglecostophrenic angle



Massive pleural fluid Massive pleural fluid often shifts the often shifts the mediastinum to the mediastinum to the opposite sideopposite side
Unusual localized Unusual localized pleural effusions can pleural effusions can be seen due to the be seen due to the localized obliteration localized obliteration of the pleural space of the pleural space often by inflammatory often by inflammatory conditions conditions (adherence)(adherence)

Smaller amounts of pleural fluid can be Smaller amounts of pleural fluid can be detected on lateral decubitus radiography detected on lateral decubitus radiography as the free intrapleural fluid moves from as the free intrapleural fluid moves from top of the diaphragm to the dependent top of the diaphragm to the dependent chest wallchest wall
Pleural effusion in a lateral decubitus radiograph

Ultrasound is able to demonstrate smaller Ultrasound is able to demonstrate smaller amounts of fluid as 100 mlamounts of fluid as 100 ml
CT has similar sensitivity to ultrasound, CT has similar sensitivity to ultrasound, not routine but can be performed to not routine but can be performed to evaluate concomitant paranchymal lesionsevaluate concomitant paranchymal lesions
CT is sensitive in identifying pleural CT is sensitive in identifying pleural thickening and calcificationthickening and calcification


Thoracenthesis and Pleural Fluid analysisThoracenthesis and Pleural Fluid analysis
AppereanceAppereance Serous (light to dark yellow, clear)Serous (light to dark yellow, clear) Serosangineous (Blood tinged can be due to Serosangineous (Blood tinged can be due to
thoracentesis itself)thoracentesis itself) Hemorrhagic (hemothorax if hct>50% of blood Hemorrhagic (hemothorax if hct>50% of blood
hct)hct) Purulent (fetid odor in unaerobic infections)Purulent (fetid odor in unaerobic infections) Chylous (milky)Chylous (milky)

Biochemical evaluationBiochemical evaluation ExudativeExudative TransudativeTransudative Some special hintsSome special hints
Microbiological evaluationMicrobiological evaluation Cellular structureCellular structure Special stains and cultureSpecial stains and culture
Cytologic evaluationCytologic evaluation

Biochemical EvaluationBiochemical Evaluation
RoutineRoutine pHpH GlucoseGlucose Lactate Lactate
dehydrogenasedehydrogenase Total proteinTotal protein AlbumineAlbumine
OptionalOptional HtcHtc CholesterolCholesterol TrigliseridTrigliserid BilirubineBilirubine Adenosin deaminaseAdenosin deaminase AmylaseAmylase RFRF LE cellLE cell ANAANA Hyaluronic asciteHyaluronic ascite

Biochemical EvaluationBiochemical Evaluation
ExudateExudate Dark yellow colorDark yellow color Total protein >3 gr/dlTotal protein >3 gr/dl Density >1016Density >1016 Light Criteria:Light Criteria:
• Protein pl/sProtein pl/s >0.5>0.5• LDH pl/sLDH pl/s >0.6>0.6• LDH >200 or >2/3 of LDH >200 or >2/3 of
normal upper value of normal upper value of serumserum
TransudateTransudate Light yellow colorLight yellow color Total protein <3 gr/dlTotal protein <3 gr/dl Density <1016Density <1016 Light Criteria:Light Criteria:
• Protein pl/sProtein pl/s <0.5<0.5• LDH pl/sLDH pl/s <0.6<0.6• LDH <200LDH <200

Albumine Gradient:Albumine Gradient: Serum albumine- Pleural fluid albumineSerum albumine- Pleural fluid albumine <1.2 gr/dl<1.2 gr/dl EksudateEksudate >1.2 gr/dl>1.2 gr/dl TransudateTransudate
Pleural Cholesterol >60 mg/dl: EksudatePleural Cholesterol >60 mg/dl: Eksudate Pl/S bilirubine >0.6:Pl/S bilirubine >0.6: ExudateExudate

Transudative Pl. Eff.Transudative Pl. Eff. Increased hydrostatic Increased hydrostatic
pressurepressure• Congestive heart failureCongestive heart failure• Constrictive pericarditisConstrictive pericarditis• Pericardial effusionPericardial effusion• Pulmonary thromboemboliPulmonary thromboemboli
Decreased oncotic Decreased oncotic pressurepressure
• CirrhosisCirrhosis• Nephyrotic syndromeNephyrotic syndrome• MalnutritionMalnutrition
Increased capillary Increased capillary permeabilitypermeability
• Myxedema Myxedema • Pulmonary thromboemboliPulmonary thromboemboli
Transperitoneal transportTransperitoneal transport• Peritoneal dialysisPeritoneal dialysis• AscitesAscites
Exudative Pl. Eff.Exudative Pl. Eff. Infectious diseasesInfectious diseases
• Pnomonia, lung abscessPnomonia, lung abscess• TuberculosisTuberculosis• Fungal infectionsFungal infections• Subphrenic abscessSubphrenic abscess
Neoplastic diseasesNeoplastic diseases• MetastaticMetastatic• MesotheliomaMesothelioma• LymphomaLymphoma
Immunologic reactionsImmunologic reactions• Dressler syndromeDressler syndrome• Sistemic Lupus Er.Sistemic Lupus Er.• Rheumatoid artritisRheumatoid artritis• Churg strauss syndromeChurg strauss syndrome• Wegener granulomatosisWegener granulomatosis

Exudative Pl EffExudative Pl Eff Gastrointestinal Gastrointestinal
diseasedisease• PancreatitisPancreatitis• Causes of peritoneal Causes of peritoneal
exudaexuda Drug inducedDrug induced
• NitrofurantoinNitrofurantoin• DantroleneDantrolene• MethysergideMethysergide• BromocriptineBromocriptine• ProcarbasineProcarbasine• AmiodoroneAmiodorone
PostsurgicalPostsurgical Pulmonary Pulmonary
thromboembolismthromboembolism

Exudative Pl EffExudative Pl Eff SarcoidosisSarcoidosis Uremic pleuritisUremic pleuritis Asbestos exposureAsbestos exposure ChylothoraxChylothorax HemothoraxHemothorax

If the effusion is transudative the main If the effusion is transudative the main cause should be treatedcause should be treated
If the effusion is exudative and not If the effusion is exudative and not emphyema further diagnostic procedures emphyema further diagnostic procedures should be consideredshould be considered Cytologic examinationCytologic examination Closed pleural needle biopsyClosed pleural needle biopsy Thoracoscopy (VATS)Thoracoscopy (VATS) ThoracotomyThoracotomy

Special characteristics:Special characteristics:Milky appearanceMilky appearance
ChylothoraxChylothorax Triglyceride >110 Triglyceride >110
mg/dlmg/dl Pl TG/sTG>1Pl TG/sTG>1 Cholesterol crystal (-)Cholesterol crystal (-) Pl Ch/s Ch<1Pl Ch/s Ch<1 Chylomicrons (+)Chylomicrons (+)
PseudochylothoraxPseudochylothorax Triglyseride <50 mg/dlTriglyseride <50 mg/dl Pl TG/sTG<1Pl TG/sTG<1 Cholesterol>250 mg/dlCholesterol>250 mg/dl Pl Ch/s Ch>1Pl Ch/s Ch>1
EmphyemaEmphyema PH<7.20PH<7.20 Low GlucoseLow Glucose

Microbiologic evaluationMicrobiologic evaluation
RBC >100 000/mmRBC >100 000/mm33 Trauma,Trauma, Pulmonary infarctionPulmonary infarction malignancymalignancy
WBC > 1000/mmWBC > 1000/mm33 : exudate : exudate > 10 000/mm> 10 000/mm33 : emphyema, parapnomonic : emphyema, parapnomonic
effusion (PNL predominates)effusion (PNL predominates)
Mesothelial cells<5%: tuberculosis possibleMesothelial cells<5%: tuberculosis possible
Lymphocytes >50% : tuberculosis, malignancy, Lymphocytes >50% : tuberculosis, malignancy, lymphoma, fungus, myxedemalymphoma, fungus, myxedema

Gram stainingGram staining Ziehl-Neelsen stainingZiehl-Neelsen staining Cultures for specific and nonspecific Cultures for specific and nonspecific
infectionsinfections PCRPCR

Infectious pleuresy, emphyemaInfectious pleuresy, emphyema
Bacterial pneumonia is associated with an Bacterial pneumonia is associated with an effusion in 40% of caseseffusion in 40% of cases
The effusion may be parapneumonic The effusion may be parapneumonic without infection (uncomplicated) or without infection (uncomplicated) or culture positive (complicated, emphyema)culture positive (complicated, emphyema)
Parapneumonic effusions are treated with Parapneumonic effusions are treated with appropiate antibioticsappropiate antibiotics
Tube drainage is indicated if emphyema Tube drainage is indicated if emphyema occursoccurs

Other Pleural DiseasesOther Pleural Diseases HemothoraxHemothorax
Plevral fluid htc>50% of serumPlevral fluid htc>50% of serum Can be traumatic or nontraumatic:Can be traumatic or nontraumatic:
• İatrogenicİatrogenic• Pulmonary infarctionPulmonary infarction• TumorsTumors• Rupture of aneurismRupture of aneurism• Anticoagulan treatmentAnticoagulan treatment• Thoracic endometriosisThoracic endometriosis
Treatment: Treatment: • intrapleural drainageintrapleural drainage• thoracotomythoracotomy

FibrothoraxFibrothorax A thick fibrous tissue formed on visceral A thick fibrous tissue formed on visceral
pleurapleura Cause:Cause:
• EmpyemaEmpyema• TuberculosisTuberculosis• HemothoraxHemothorax
Treatment: DecorticationTreatment: Decortication

PneumothoraxPneumothorax
Presence of free air between the visceral and Presence of free air between the visceral and parietal pleuraparietal pleura
Divided into 3Divided into 3• SpontaneousSpontaneous
Primary idiopathicPrimary idiopathic SecondarySecondary
• TraumaticTraumatic• IatrogenicIatrogenic

Primary Spontaneous Primary Spontaneous PneumothoraxPneumothorax
Mostly occurs in young, male, smokersMostly occurs in young, male, smokers There is no obvious underlying pulmonary There is no obvious underlying pulmonary
disease disease Subpleural blebs and bullae probably play Subpleural blebs and bullae probably play
a role in pathogenesisa role in pathogenesis Symptoms can be an acute unset of Symptoms can be an acute unset of
dyspnea and unilateral chest pain but can dyspnea and unilateral chest pain but can be absent also depending on the size of be absent also depending on the size of the pneumothoraxthe pneumothorax

Physical examination:Physical examination: HypersonorityHypersonority on percusion on percusion Reduced breath sounds, reduced VT, enlarged Reduced breath sounds, reduced VT, enlarged
hemithoraxhemithorax Hypotension and cardiac tamponade may occur Hypotension and cardiac tamponade may occur
depending on the size of the pneumothoraxdepending on the size of the pneumothorax Radiology:Radiology:
Pleural line Pleural line Hyperlucency at the peripheryHyperlucency at the periphery Mediastinal shiftMediastinal shift Expiration film can be used when the lesion is not Expiration film can be used when the lesion is not
apparentapparent



Measurement of the average Measurement of the average diameters of the collapsed diameters of the collapsed lung and the affected lung and the affected hemithorax can be usedhemithorax can be used
100-(8100-(833/11/1133)100=% 62)100=% 62 Simple observation with rest Simple observation with rest
and supplemental oxygen can and supplemental oxygen can be used for asymptomatic be used for asymptomatic patients with a small (<20%) patients with a small (<20%) pxpx
Intercostal drainage is Intercostal drainage is indicated in large pxindicated in large px
A recurrent spontaneous A recurrent spontaneous pneumothorax (30-50% risk) is pneumothorax (30-50% risk) is an indication for surgeryan indication for surgery
Quantification of the size of the pneumothorax is Quantification of the size of the pneumothorax is helpfull in the decision of treatment helpfull in the decision of treatment

Secondary Spontaneous Secondary Spontaneous PneumothoraxPneumothorax
Patients have an underlying pulmonary disease:Patients have an underlying pulmonary disease: COPDCOPD AsthmaAsthma Congenital cysts and bullaeCongenital cysts and bullae Interstitial lung fibrosing diseasesInterstitial lung fibrosing diseases Cystic fibrosisCystic fibrosis Hystiocytosis XHystiocytosis X Whooping coughWhooping cough LymphangiomyomatosisLymphangiomyomatosis Pleural endometriosis, catamenial pneumothoraxPleural endometriosis, catamenial pneumothorax Pleural malignancyPleural malignancy SarcoidosisSarcoidosis Bacterial pneumonia and Pneumocystis PneumoniaBacterial pneumonia and Pneumocystis Pneumonia

Traumatic and Iatrogenic Traumatic and Iatrogenic PneumothoraxPneumothorax
Iatrogenic pneumothorax can be seen Iatrogenic pneumothorax can be seen during:during: ThorasentesisThorasentesis Pleural needle biopsyPleural needle biopsy Transthoracic lung aspiration biopsyTransthoracic lung aspiration biopsy Mechanical ventilationMechanical ventilation Central venous catheterizationCentral venous catheterization TracheostomyTracheostomy Cardiopulmonary resusitationCardiopulmonary resusitation

Pleural NeoplasmsPleural Neoplasms
Benign:Benign: Pleural lipomaPleural lipoma Local pleural fibroma (Fibrous mesothelioma)Local pleural fibroma (Fibrous mesothelioma)
Malign:Malign: Diffuse malign mesotheliomaDiffuse malign mesothelioma

Malign Pleural effusionsMalign Pleural effusions
Diffuse Malign MesotheliomaDiffuse Malign Mesothelioma Bronchial carcinoma (adenocarcinoma) Bronchial carcinoma (adenocarcinoma) LymphomaLymphoma Breast carcinomaBreast carcinoma Other adenocarcinomasOther adenocarcinomas

Malignant MesotheliomaMalignant Mesothelioma
Primary tumour of pleural, pericardial, peritonial Primary tumour of pleural, pericardial, peritonial mesotheliummesothelium
Etiology: 70-90% asbest exposure:Etiology: 70-90% asbest exposure: Occupational: asbest is resistant to heat and friction Occupational: asbest is resistant to heat and friction
so used in building, water pipes, brakes, isolation so used in building, water pipes, brakes, isolation systems, textilesystems, textile
Environmental: Eskişehir, Kütahya, Bilecik, Yozgat, Environmental: Eskişehir, Kütahya, Bilecik, Yozgat, Sivas, DiyarbakırSivas, Diyarbakır
Latent period is 30-40 years in occupational Latent period is 30-40 years in occupational exposureexposure
Smoking dramaticaly increase the risk of cancer Smoking dramaticaly increase the risk of cancer in asbest exposurein asbest exposure

Erionite is another fibrous zeolite found in soil, Erionite is another fibrous zeolite found in soil, high in Nevşehir: Tuzköy, Karain, Sarıhıdır high in Nevşehir: Tuzköy, Karain, Sarıhıdır area in Turkey. It is more carcinogenic than area in Turkey. It is more carcinogenic than asbest. asbest.
49% of total deaths in the villages of Ürgüp are 49% of total deaths in the villages of Ürgüp are due to DMMdue to DMM

The most common clinical presentations are The most common clinical presentations are dyspnea, chest pain, unilateral decreased dyspnea, chest pain, unilateral decreased volume of the affected hemithorax (frozen chest) volume of the affected hemithorax (frozen chest) (inspite of fluid accumilation)(inspite of fluid accumilation)
Nodular thickening of the pleura, irregular Nodular thickening of the pleura, irregular thickening of the interlobar fissure, absence of thickening of the interlobar fissure, absence of mediastinal shift with massive pleural effusion mediastinal shift with massive pleural effusion (frozen chest)(frozen chest)
Diagnosis by histologic examinationDiagnosis by histologic examination Treatment oncologic and surgical if possible, Treatment oncologic and surgical if possible,
prognosis is poorprognosis is poor


-END-