Embed Size (px)
Citation preview

ARTICLE IN PRESS
Ann Anat 189 (2007) 412—417
0940-9602/$ - sdoi:10.1016/j.
�CorrespondE-mail addr
www.elsevier.de/aanat
Plate osteosynthesis of the mandibular condyle
Gunter Lauera,�, Dominik Haima, Peter Proffb, Gerd Richterc,Winnie Pradela, Jochen Fanghaneld, Eckhard Pillinga,Tomasz Gedrangeb, Ronald Maia
aDepartment of Oral and Maxillofacial Surgery, Medical Faculty ‘‘Carl Gustav Carus’’, Technische Universitaet Dresden,Fetscherstrabe 74, D-01307 Dresden, GermanybClinic for Orthodontics and Preventive and Paediatric Dentistry, University of Greifswald Dental School,Rotgerberstrabe 8, D-17487 Greifswald, GermanycDepartment of Prosthetic Dentistry, Medical Faculty ‘‘Carl Gustav Carus’’, Technische Universitaet Dresden,Fetscherstrabe 74, D-01307 Dresden, GermanydDepartment of Oral Anatomy, University of Greifswald Dental School, Rotgerberstrabe 8, D-17487 Greifswald,Germany
Received 21 December 2006; accepted 20 February 2007
KEYWORDSCondylar neckfractures;Mandible;Biomechanical load;Plate design;Plating technique;Osteosynthesis
ee front matter & 2007aanat.2007.02.021
ing author. Tel.: +49 351ess: guenter.lauer@unik
SummaryThe aim of this study is to evaluate and compare the biomechanical stability ofvarious osteosynthesis materials for mandible condylar-process fractures.On 160 porcine mandibles, four different monocortical plating techniques (40 pergroup) were investigated. Condyles were fractured at a defined location from theincisure to the posterior border. After correct anatomical reduction the fractureswere plated, using four different techniques. Osteosynthesis materials used werethe delta plate, the trapezoid plate, the dynamic compression plate and doublemini-plates. Each group was subjected to linear loading in lateral to medial, medialto lateral, anterior to posterior and posterior to anterior directions by a universalmechanical testing machine TIRAtest 2720. Yield load, yield displacement weremeasured for the different plates.Statistically significant differences were noted between the fixation groups in allfour directions. Rigid internal fixation with double mini plates showed the beststability in all directions except posterior to anterior. In this direction, the delta-plate resisted the highest loads. In the three other directions, the delta plate wassecond best with data similar to double miniplates but lower in magnitude.& 2007 Elsevier GmbH. All rights reserved.
Elsevier GmbH. All rights reserved.
458 5205; fax: +49 351 458 5382.linikum-dresden.de (G. Lauer).

ARTICLE IN PRESS
Plate osteosynthesis of the mandibular condyle 413
Introduction
Mandible condylar fractures are frequent ac-counting for 25–45% of all mandibular fractures(Gassner et al., 2003). Treatment of condylarfractures with rigid internal fixation has madesignificant advances over the past years dueto improved understanding of biomechanicalprinciples, advances in fixation technique andinstrumentation (Haug et al., 2002) and due toscientifically based research of treatment outcome(Worsaae and Thorn, 1994; Eckelt et al., 2006). Thetherapeutic goals in condylar fracture managementare to re-establish premorbid anatomy, to providefracture stabilisation and to restore the function-ality with least morbidity. This can be achieved viaan open extraoral approach to the joint area andosteosynthesis. Different osteosynthesis platingsystems are in use. Clinical and biomechanicalstudies provide data that the application of twoplates is most reliable as they neutralise tensionand pressure forces best (Choi et al., 2001; Meyeret al., 2002). However, particularly in higherfractures the use of double miniplates and ingeneral the extraoral surgical access is relatedwith a certain risk to the facial nerve andsubsequent facial nerve palsy.
To minimise this hazard the intraoral approachwith endoscopic assistance has proved to beadvantageous, in addition providing good controlof the fracture reduction and plate osteosynthesis(Jacobovicz et al., 1998; Lachner et al., 1991).However, this approach is related with a limitedspace, which makes application of double platesdifficult. These disadvantages may be overcomeby using plates of modified design such as thecompression plate, the trapezoid plate or therecently developed delta plate (Lauer et al.,2007). However, a direct comparison of thesedifferent miniplates has not been performed yet.Therefore, the aim of this study was to examine thedifferent plates advocated for the condylar frac-ture treatment, with a particular focus on theplates that are especially designed for condylarneck fractures.
Figure 1. Condylar process of a pig’s mandible withreduced fracture and rigid internal fixation via a deltaplate.
Materials and methods
A total of 160 porcine mandibles were used inthis study, because porcine mandibles have a greatdegree of similarity to human bone. For thatreason, they offer more realistic conditions con-cerning the anchorage of screws and the creation ofthe fracture, e.g. the rough borders help with the
anatomical correct reduction, as well as with thetransmission of the load compared to syntheticbone.
To minimize variables in this investigation, allscrews used for plate fixation were 5.0mmin length, 2.0mm in outer diameter, self-tappingand fabricated of titanium (Martin, Tuttlingen,Germany).
Sample preparation: The condylar necks ofporcine mandibles were uniformly fractured fromthe sigmoid notch to a point approximately two-thirds between the inferior border and the head ofthe condyle. Fractures were reduced and fixed withthe 4 different types of plates, 40 mandibles foreach type of plate.
The newly developed delta plate (Fa. Medartis,Basel, Switzerland) was used in Group I (n ¼ 40)(Fig. 1). Further, two 2.0 miniplates (Martin,Tuttlingen, Germany) (Group II) (Fig. 2), thetrapezoid plate (Fa. Medartis, Basel, Switzerland)(Group III) (Fig. 3) and the 2.0 dynamic compressionplate (Medartis, Basel, Switzerland) (Group IV)(Fig. 4) were applied in 40 mandibles per group.
The bases of the mandibles were cast in blocks ofpolymethyl methacrylate and then placed in theuniversal mechanical testing machine TIRA test2720 (Fa TIRA GmbH, Schalkau, Germany).
Linear loading: At the head region, all porcinemandibles were subjected to linear increasingloading in lateral to medial, medial to lateral,anterior to posterior and posterior to anteriordirections using the universal mechanical testingmachine TIRA test 2720. The testing machine
ARTICLE IN PRESS
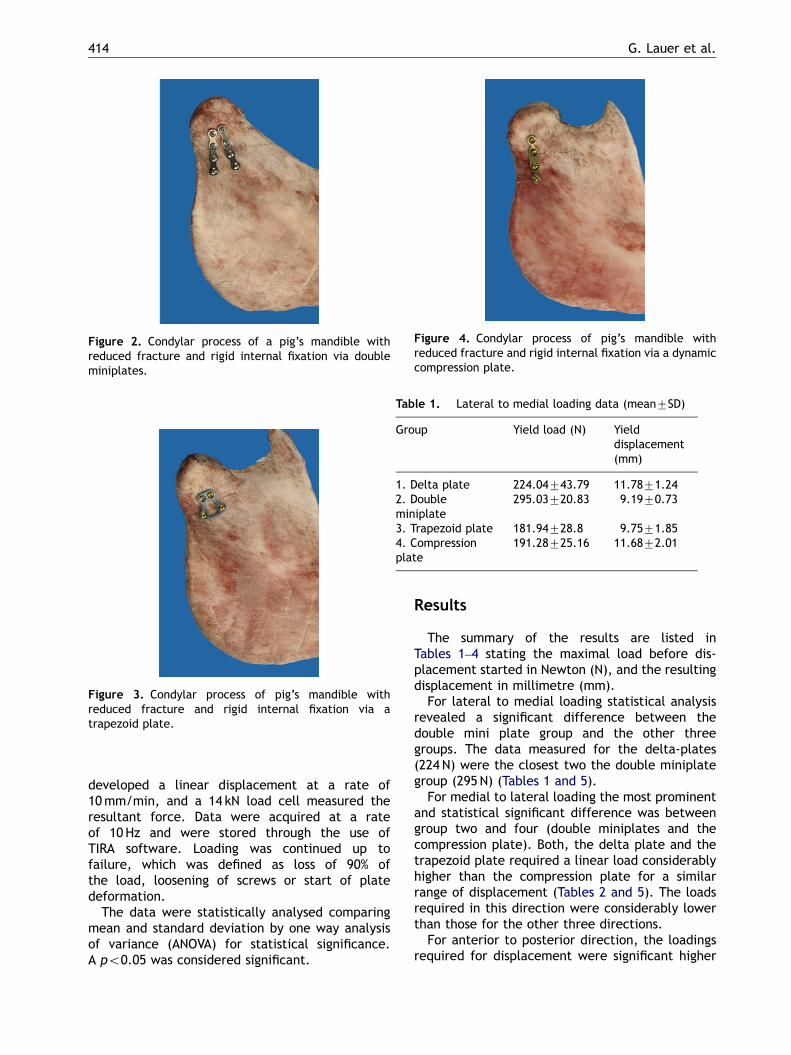
Figure 2. Condylar process of a pig’s mandible withreduced fracture and rigid internal fixation via doubleminiplates.
Figure 3. Condylar process of pig’s mandible withreduced fracture and rigid internal fixation via atrapezoid plate.
Figure 4. Condylar process of pig’s mandible withreduced fracture and rigid internal fixation via a dynamiccompression plate.
Table 1. Lateral to medial loading data (mean7SD)
Group Yield load (N) Yielddisplacement(mm)
1. Delta plate 224.04743.79 11.7871.242. Doubleminiplate
295.03720.83 9.1970.73
3. Trapezoid plate 181.94728.8 9.7571.854. Compressionplate
191.28725.16 11.6872.01
G. Lauer et al.414
developed a linear displacement at a rate of10mm/min, and a 14 kN load cell measured theresultant force. Data were acquired at a rateof 10 Hz and were stored through the use ofTIRA software. Loading was continued up tofailure, which was defined as loss of 90% ofthe load, loosening of screws or start of platedeformation.
The data were statistically analysed comparingmean and standard deviation by one way analysisof variance (ANOVA) for statistical significance.A po0.05 was considered significant.
Results
The summary of the results are listed inTables 1–4 stating the maximal load before dis-placement started in Newton (N), and the resultingdisplacement in millimetre (mm).
For lateral to medial loading statistical analysisrevealed a significant difference between thedouble mini plate group and the other threegroups. The data measured for the delta-plates(224 N) were the closest two the double miniplategroup (295N) (Tables 1 and 5).
For medial to lateral loading the most prominentand statistical significant difference was betweengroup two and four (double miniplates and thecompression plate). Both, the delta plate and thetrapezoid plate required a linear load considerablyhigher than the compression plate for a similarrange of displacement (Tables 2 and 5). The loadsrequired in this direction were considerably lowerthan those for the other three directions.
For anterior to posterior direction, the loadingsrequired for displacement were significant higher

ARTICLE IN PRESS
Table 2. Medial to lateral loading data (mean7SD)
Group Yield load (N) Yield displacement (mm)
1. Delta plate 20.1174.47 13.974.972. Double miniplate 24.2875.32 14.5272.343. Trapezoid plate 19.9773.83 14.4273.324. Compression plate 14.1772.86 14.0972.37
Table 3. Anterior to posterior loading data (mean7SD)
Group Yield load (N) Yield displacement (mm)
1. Delta plate 521.27109.73 8.3170.602. Double miniplate 545.247106.44 5.8170.693. Trapezoid plate 202.22724.04 11.9772.754. Compression plate 275.47737.65 9.0572.02
Table 4. Posterior to anterior loading data (mean7SD)
Group Yield load (N) Yield displacement (mm)
1. Delta plate 716.127121.96 4.1570.502. Double miniplate 569.08764.96 12.3571.453. Trapezoid plate 304.03740.35 8.5671.34. Compression plate 455.28772.48 11.9872.66
Table 5. Summary of the statistical analysis for linear loading
Test Statistically significantdifference
Between groups F, significance
Lateral to medial Yes Group 2 and all other groups(1, 3, 4)
F(3, 36) ¼ 15.245,0.0005
Medial to lateral Yes Group 2 and group 4, not betweenthe other groups
F(3, 36) ¼ 6.413,0.001
Anterior to posterior Yes groups 1,2 and groups 3,4 F(3, 36) ¼ 23.405,0.0001
Posterior to anterior Yes Groups 1 and all other groups F(3, 36) ¼ 26.332,0.0001
Plate osteosynthesis of the mandibular condyle 415
between groups1, 2 (delta-plate 521N, double miniplate 545 N) and groups 3, 4 (trapezoid plate 202 N,compression plate 275 N) (Tables 3 and 5).
For posterior to anterior loading there weresignificant differences between group 1 (deltaplate 716N) and all the other three groups meaningthat the load to achieve a displacement was thehighest when using the delta plate (Tables 4 and 5).
Discussion
The biomechanics of the human skull with itsnumerous connections and dependencies is com-
plex (Fanghanel et al., 2006; Gundlach, 1999;Sellers and Crompton, 2004). Mandibular condylefractures are frequent (Gassner et al., 2003) andprospective and multi-centre studies (Worsaae andThorn, 1994; Eckelt et al., 2006) provide evidence,that open surgical treatment avoids compromisedfunction and malocclusion (De Riu et al., 2001;Ellis et al., 2000). However, the extraoral surgicalapproach has the risk of facial nerve palsy whichcan be avoided using the intraoral approach(Lachner et al., 1991). Although endoscopic-assisted techniques help in fracture visualisation(Jacobovicz et al., 1998), due to anatomy andbiomechanics the mandibular condyle is a demand-ing site for rigid internal fixation.

ARTICLE IN PRESS
G. Lauer et al.416
Several plate types and techniques like adaptionminiplates, mini dynamic compression plates anddouble miniplates have been evaluated in variousclinical follow-up studies (Choi et al., 2001) andspecially designed plates like the trapezoid and thedelta plate were developed (Wilk et al., 1997;Lauer et al., 2007). However, for direct comparisonof the different plating systems a standardisedbiomechanical model of the condylar neck isnecessary mimicking the fact that highest tensionappears on the anterior and lateral border (Throck-morton and Dechow, 1994). Therefore, severalmodels like formalin-fixed human cadaver mand-ibles (Choi et al., 1999) and synthetic mandiblereplicas (Haug et al., 2002) have been suggested. Inthis biomechanical study, the sheep mandiblecadaver model was chosen as its osseous consis-tency is analogous to fresh human bone – importantfor the grip of the screws – although the anatomicalshape differs from the human bone.
In a cadaver model Choi et al. (1999) comparedone miniplate, one minidynamic compression plate,one 2.4mm plate and double miniplates. Using onlyforces from anterior–superior to posterior–inferiorthe double miniplates provided the best resultfollowed by the 2.4 plate and the mini dynamiccompression plate. In a synthetic mandible modelHaug et al. (2002) tested a zygomatic dynamiccompression plate, a mini dynamic compressionplate, a locking adaption plate and a conventionaladaption plate with 6 screws each. Forces in fourdifferent directions and torsion were applied. Minidynamic compression plates provided the bestresults but no double plating was tested. In ourfracture model, the condyles or the plates,respectively, were also subjected to forces in thefour different directions (posterior to anterior,anterior to posterior, medial to lateral, lateralto medial). Double miniplates fixed with eightscrews in total provided the best results in threeof four directions. The delta plate was secondbest. In the posterior anterior direction thedelta plate was the best. It best imitates theconfiguration of the double plates, however, is fixedto the bone by four screws only. The three-dimensionality of the delta plate provides an‘‘internal’’ stability due to its triangular shape aswell as more optimal leverage. For loads fromposterior or anterior onto the proximal fragment,the base of the plate fastening in the distalfragment provides an optimal leverage due to thedistance between these screws. Particularly inthe areas of highest stress at the anterior and thelateral border (Throckmorton and Dechow, 1994)the plate acts like a triangle with its sides takingthe load like a tension band.
Both the delta and the dynamic compressionplate have the gliding hole feature. Compressionstabilizes the fracture when driving home thescrews (Niederdellmann et al., 1975). In this modelwith 100% correct anatomical reduction this fea-ture may help to utilise the interdigitations of thefractured bone as both plates gained better resultsthan the trapezoid plate except for the lateral tilt.
These biomechanical data are in accordance withthose from several clinical follow-up studies, wherestability of different plating techniques have beenassessed (Choi et al., 2001). The least complica-tions occurred when miniplates with a thickness of1mm or more, double miniplates or compressionminiplates were used.
Conclusion
In conclusion, in comparing four different platingtechniques for condylar fracture osteosynthesis thisstudy confirms clinical findings of the benefit of thedouble plating technique as being the gold stan-dard. However, data also provide evidence that thedelta plate is reliable in the condylar area. Thedelta plate was always second best, except forposterior to anterior load, here it was best.
References
Choi, B.H., Kim, K.M., Kim, H.J., Kim, M.K., 1999.Evaluation of condylar neck fracture plating techni-ques. J. Craniomaxillofac. Surg. 27, 109–112.
Choi, B.H., Yi, Ch.K., Yoo, J.H., 2001. Clinical evaluationof 3 types of plate osteosynthesis for fixation ofcondylar neck fractures. J. Oral Maxillofac. Surg. 59,734–737.
De Riu, G., Gamba, U., Anghinoni, M., Sesenna, E., 2001.A comparison of open and closed treatment ofcondylar fractures: a change in philosophy. Int.J. Oral Maxillofac. Surg. 30, 384–389.
Eckelt, U., Schneider, M., Erasmus, F., Gerlach, K.L.,Kuhlisch, E., Loukota, R., Rasse, M., Schubert, J.,Terheyden, H., 2006. Open versus closed treatment offractures of the mandibular condylar process – aprospective randomized multicentre study. J. Cranio-maxillofac. Surg. 34, 306–314.
Ellis III, E., Simon, P., Throckmorton, G.S., 2000. Occlusalresults after open or closed treatment of fractures ofthe mandibular condylar process. J. Oral Maxillofac.Surg. 58, 260–268.
Fanghanel, J., Gedrange, T., Proff, P., 2006. The face-physiognomic expressiveness and human identity. Ann.Anat. 188, 261–266.
Gassner, R., Tuli, T., Hachl, O., Rudisch, A., Ulmer, H.,2003. Cranio-maxillofacial trauma: a 10 year review of

ARTICLE IN PRESS
Plate osteosynthesis of the mandibular condyle 417
9543 cases with 21 067 injuries. J. Craniomaxillofac.Surg. 31, 51–61.
Gundlach, K.K., 1999. Malformations of the temporo-mandibular joint in laboratory animals and in man.Ann. Anat. 181, 73–75.
Haug, R.H., Peterson, G.P., Goltz, M., 2002. A biomecha-nical evaluation of mandibular condyle fracture platingtechniques. J. Oral Maxillofac. Surg. 60, 73–80.
Jacobovicz, J., Lee, C., Trabulsy, T., 1998. Endoscopicrepair of mandibular subcondylar fractures. Plast.Reconstr. Surg. 101, 437–441.
Lachner, J., Clanton, J.T., Waite, P.D., 1991. Openreduction and internal rigid fixation of subcondylarfractures via an intraoral approach. Oral Surg. OralMed. Oral Pathol. 71, 257–261.
Lauer, G., Pradel, W., Schneider, M., Eckelt, U., 2007. Anew three-dimensional plate for transoral endoscopic-assisted osteosynthesis of condylar neck fractures. J.Oral Maxillofac. Surg., in press.
Meyer, C., Kahn, J.L., Boutemi, P., Wilk, A., 2002.Photoelastic analysis of bone deformation in the
region of the mandibular condyle during mastication.J. Cranio Maxillofac. Surg. 30, 160–169.
Niederdellmann, H., Schilli, W., Ewers, R., Akuamoa-Boateng, E., 1975. Photoelastic behaviour ofosteosynthesis plates with different arrangement ofscrews holes for mandibular fractures. J. Oral Surg. 4,27–31.
Sellers, W.I., Crompton, R.H., 2004. Using sensitivityanalysis to validate the predictions of a biomechanicalmodel of bite forces. Ann. Anat. 186, 89–95.
Throckmorton, G.S., Dechow, P.C., 1994. In vitro strainmeasurements in the condylar process of the humanmandible. Arch. Oral Biol. 39, 853–867.
Wilk, A., Biotchane, I., Rosenstiel, M., Charles, X., Meyer,C., 1997. Osteosynthesis of subcondylar fracturesusing a retroangular 3-dimensional stabilization plate.Rev. Stomatol. Chir. Maxillofac. 98, 40–44.
Worsaae, N., Thorn, J.J., 1994. Surgical versus nonsurgi-cal treatment of unilateral dislocated low subcondylarfractures: a clinical study of 52 cases. J. OralMaxillofac. Surg. 52, 353–360.







![Current Advances in Mandibular Condyle Reconstruction · The LIPUS is considered the preferred method of mechanical stimulation, also known as “preferred bioreactor” [25]. 5](https://img.dokumen.tips/doc/110x75/5e96a9d67ba2de640562addd/current-advances-in-mandibular-condyle-reconstruction-the-lipus-is-considered-the.jpg)






![Analysis of Tibial Condyle Fractures Treated by minimally Invasive Plate Osteosynthesis [MIPO]](https://img.dokumen.tips/doc/110x75/587d03a51a28ab1e7e8b6f45/analysis-of-tibial-condyle-fractures-treated-by-minimally-invasive-plate-osteosynthesis.jpg)














