Embed Size (px)
Citation preview

REVIEW ARTICLE
Plasmonic photothermal therapy (PPTT)using gold nanoparticles
Xiaohua Huang & Prashant K. Jain & Ivan H. El-Sayed &
Mostafa A. El-Sayed
Received: 26 April 2007 /Accepted: 10 May 2007 /Published online: 3 August 2007# Springer-Verlag London Limited 2007
Abstract The use of lasers, over the past few decades, hasemerged to be highly promising for cancer therapymodalities, most commonly the photothermal therapymethod, which employs light absorbing dyes for achievingthe photothermal damage of tumors, and the photodynamictherapy, which employs chemical photosensitizers thatgenerate singlet oxygen that is capable of tumor destruc-tion. However, recent advances in the field of nanosciencehave seen the emergence of noble metal nanostructureswith unique photophysical properties, well suited forapplications in cancer phototherapy. Noble metal nano-particles, on account of the phenomenon of surfaceplasmon resonance, possess strongly enhanced visible andnear-infrared light absorption, several orders of magnitudemore intense compared to conventional laser phototherapyagents. The use of plasmonic nanoparticles as highlyenhanced photoabsorbing agents has thus introduced amuch more selective and efficient cancer therapy strategy,
viz. plasmonic photothermal therapy (PPTT). The synthetictunability of the optothermal properties and the bio-targeting abilities of the plasmonic gold nanostructuresmake the PPTT method furthermore promising. In thisreview, we discuss the development of the PPTT methodwith special emphasis on the recent in vitro and in vivosuccess using gold nanospheres coupled with visible lasersand gold nanorods and silica–gold nanoshells coupled withnear-infrared lasers.
Keywords Surface plasmon resonance (SPR) .
Plasmonic photothermal therapy (PPTT) . Cancer .
Gold nanospheres . Gold nanorods . Gold nanoshells .
Immunotargeting
Introduction
The use of heat has become one of the major methodsfor tumor therapy since its ancient usage in 1700 BC
when a glowing tip of a firedrill was used for breast cancertherapy [1]. Later heating sources ranging from radio-frequency [2–5] to microwaves [6–9] as well as ultrasoundwaves [10–12] were introduced to induce moderate heatingin a specific target region, which is termed as hyperthermia.Hyperthermia is commonly defined as heating tissue to atemperature in the range 41–47°C for tens of minutes [13].Tumors are selectively destroyed in this temperature rangebecause of their reduced heat tolerance compared to normaltissue, which is due to their poor blood supply. Hyper-thermia causes irreversible cell damage by loosening cellmembranes and denaturing proteins. But the applications ofthe heating sources conventionally employed for hyperther-
Lasers Med Sci (2008) 23:217–228DOI 10.1007/s10103-007-0470-x
X. Huang : P. K. Jain :M. A. El-Sayed (*)Laser Dynamics Laboratory,School of Chemistry and Biochemistry,Georgia Institute of Technology,Atlanta, GA 30332-0400, USAe-mail: [email protected]
I. H. El-SayedDepartment of Otolaryngology—Head and Neck Surgery,Comprehensive Cancer Center,University of California at San Francisco,San Francisco, CA 94143, USA
M. A. El-SayedUniversity of California,Berkeley, CA 94720, USA

mia are limited because of their damage to surroundinghealthy tissues.
A revolution in cancer therapy has taken place by theemerging use of laser light to achieve controlled andconfined thermal damage in the tumor tissue. Laser, theacronym for light amplification by the stimulated emissionof radiation [14], is an optical source that emits photons in acoherent and narrow beam. It was proposed in 1959 [14]and first demonstrated in 1960 [15]. Laser usage in surgerywas first reported by ophthalmologists in 1963 [16] andthen reported for tumor eradication in 1965 [17] followedby wide interest in late 1960s [18–20]. The laser light,usually neodymium–yttrium aluminum garnet (Nd–YAG,1.06 um) and CO2 laser (10.6 um) [21–25] can either betransmitted from optical fiber tip to exposed tumors in theair or delivered into a confined space by inserting the bareend of the fiber into the center of the target tumor, which isoften called interstitial laser hyperthermia [26–30]. Laserlight has the characteristics of monochromaticity, coher-ence, and collimation [31–33]. These properties provide anarrow beam of high intensity, which transmits deep downinto the target tissue with minimal power loss and greatprecision. The biggest disadvantage of laser therapy is itsnonselectivity. Both normal and tumor cells in the path ofthe laser light are damaged. The requirement of the highpower density is another problem. High power laser outputup to tens to hundreds of watts has to be used to efficientlyinduce the tumor oblation [23].
Another type of tumor therapy method is the photody-namic therapy (PDT), also known as photochemotherapy[34–41], which involves cell destruction caused by meansof toxic singlet oxygen and/or other free radicals that areproduced from a sequence of photochemical and photobi-ological processes. These processes are initiated by thereaction of a photosensitizer with tissue oxygen uponexposure to a specific wavelength of light in the visible ornear-infrared (NIR) region. The earliest sensitizer used wasacridine, which was reported in 1900 to kill paramecia [42]and followed by eosin for skin cancer treatment in 1903[43]. Although many chemicals have been later reported forphotochemical therapy, porphyrin-based sensitizers [44–49]lead the role in clinical applications because of theirpreferential retention in cancer tissues and due to the highquantum yields of singlet oxygen produced. The Photofrin®[50], which is a purified hematoporphyrin derivative, hasbeen approved for clinic trials by the US Food and DrugAdministration. Porphyrin-based therapy can only be usedfor tumors on or just under the skin or on the lining ofinternal organs or cavities because it absorbs light shorterthan 640 nm in wavelength. For deep-seated tumors,second generation sensitizers, which have absorbance inthe NIR region, such as core-modified porphyrins [51],chlorins [52] phthalocyanine [53], and naphthalocyanine
[54], have been introduced. A major drawback of PDT isthat the photosensitizing drug stays in the body for a longtime, rendering the patient to be highly sensitive to light.
An alternative to PDT is the photothermal therapy(PTT) in which photothermal agents are employed toachieve the selective heating of the local environment[55–61]. When the PTT agents absorbs light, electronsmake transitions from the ground state to the excited state.The electronic excitation energy subsequently relaxesthrough nonradiative decay channels. This results in theincrease in the kinetic energy leading to the overheating ofthe local environment around the light absorbing species.The heat produced can be employed for local cell or tissuedestruction [62–65]. The photoabsorbing agents can benatural chromophores in the tissue [66–71] or externallyadded dye molecules such as indocyanine green [72, 73],naphthalocyanines [74], and porphyrins coordinated withtransition metals [75]. Natural chromophores, however,suffer from very low absorption. The choice of theexogenous photothermal agents is made on the basis oftheir strong absorption cross sections and highly efficientlight-to-heat conversion. This greatly reduces the amount oflaser energy required to achieve the local damage of thediseased cells, rendering the therapy method less invasive.But the problem with dye molecules is their photobleachingunder laser irradiation.
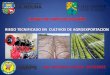
In recent years, the tremendous development of nano-technology has provided a variety of nanostructures withunique optical properties that are useful in biology andbiomedicinal applications [76–83]. From the point of theview of cancer therapeutics, noble metal nanoparticlesbecome very useful as agents for PTT on account of theirenhanced absorption cross sections, which are four to fiveorders of magnitude larger than those offered by conven-tional photoabsorbing dyes. This strong absorption ensureseffective laser therapy at relatively lower energies renderingthe therapy method minimally invasive. Additionally, metalnanostructures have higher photostability, and they do notsuffer from photobleaching. Currently, gold nanospheres[84–91], gold nanorods [92–95], gold nanoshells [96–99],gold nanocages [100, 101], and carbon nanotubes [102] arethe chief nanostructures that have been demonstrated inphotothermal therapeutics due to their strongly enhancedabsorption in the visible and NIR regions on account oftheir surface plasmon resonance (SPR) oscillations. Ofthese structures, the first three nanostructures (see Fig. 1)are especially promising because of their ease of prepara-tion, ready multi-functionalization, and tunable opticalproperties. In the present review, we discuss the photo-thermal properties of these plasmonic nanostructures andtheir application in selective PTT. We propose the nameplasmonic photothermal therapy (PPTT) for this treatmentto distinguish it from PTT and PDT.
218 Lasers Med Sci (2008) 23:217–228

Photothermal properties of plasmonic goldnanoparticles
In 1857, Faraday [103] made colloidal gold for the firsttime by reducing gold chloride with phosphors andrecognized that the reddish color was due to the small sizeof the colloidal gold particles. In 1951, Turkevich et al.[104] simplified the method by using sodium citrate asreducing agents. Since then, the interaction between lightand gold nanoparticles has been widely studied [105–112].Gold nanoparticles absorb light strongly in the visibleregion due to the coherent oscillations of the metalconduction band electrons in strong resonance with visiblefrequencies of light. This phenomenon is known as the SPR[105–113]. The SPR frequency is dependent on the type ofthe metal, the size and shape of the metal nanoparticles, aswell as the dielectric constant of the surrounding medium,thus imparting a unique optical tunability to the nanostruc-tures. When the size increases, the surface plasmon ab-sorption maximum slightly redshifts (Fig. 2a). When thenanoparticles form assemblies or aggregates, the surfaceplasmon absorption maximum redshifts to the NIR region.Interestingly, when the shape of the gold nanoparticles ischanged from sphere to rod, the SPR spectrum splits intotwo bands: a stronger long-wavelength band in the NIRregion due to the longitudinal oscillation of electrons and aweaker short-wavelength band in the visible region around
520 nm due to the transverse electronic oscillation [109,111, 112, 114–118]. Unlike spherical nanoparticles, theabsorption spectrum of the gold nanorods is very sensitiveto the aspect ratio (length/width). With an increase in thenanorod aspect ratio, the SPR absorption wavelengthmaximum of the longitudinal band significantly redshifts(Fig. 2b). Similarly, when the solid gold nanospheres arechanged to gold shell structures, the absorption maximumalso greatly redshifts. In 1998, Halas and coworkers at RiceUniversity [119] developed the gold nanoshell structure,which is composed of a silica core (100–200 nm in diameter)surrounded by a thin layer of gold shells (5–20 nm). Thenanoshells absorb and scatter strongly in the NIR region[120]. The optical resonance of the nanoshells can be tunedby adjusting the ratio of the thickness of the gold shell tothe diameter of the silica core (Fig. 2c). It has been shownthat the smaller this ratio, the more redshifted is the SPRwavelength [97].
The photothermal properties of gold nanoparticles havebeen systematically studied using femtosecond transientabsorption spectroscopy by Link and El-Sayed [111], whohave shown that the photoexcitation of metal nanostruc-tures results in the formation of a heated electron gas thatsubsequently cools rapidly within ∼1 ps by exchangingenergy with the nanoparticle lattice. This is followed byphonon–phonon interactions where the nanoparticle latticecools rapidly by exchanging energy with the surrounding
Fig. 1 Plasmonic gold nanostructures commonly used for PPTT. aNanospheres (transmission electron microscopy [TEM] image repro-duced with permission from [110]; b nanorods (TEM image
reproduced with permission from [115]); c Nanoshells (TEM imagereproduced with permission from [97])
Lasers Med Sci (2008) 23:217–228 219

medium on the timescale of ∼100 ps. This fast energyconversion and dissipation can be readily used for theheating of the local environment by using light radiationwith a frequency strongly overlapping with the nanoparticleSPR absorption band. The intense SPR-enhanced absorp-tion of gold nanoparticles makes the photothermal conver-sion process highly efficient. The absorption cross sectionof gold nanoparticles [121] is typically four to five ordersof magnitude stronger than the strongest absorbing Rhoda-
mine 6G dye molecules [122]. Hot electron temperatures ofseveral thousand kelvins are easily reached in the nano-particles even with laser excitation powers as low as 100 nJand the lattice temperature on the order of a few tens ofdegrees can be achieved [111]. This highly efficient pro-duction of heat energy from the absorbed light energy bygold nanoparticles make them greatly promising in thePPTT of cancers and other diseases. Further, in the case ofgold nanorods and gold nanoshells, this strong absorption canbe tuned to the NIR region (Fig. 2b,c), a region where lightpenetration is optimal due to minimal absorption from tissuechromophores and water [123]. This makes NIR-resonantgold nanostructures very useful for clinical therapy applica-tions involving tumors located deep within bodily tissue.
In addition to the local heating of the surroundingenvironment, which leads to irreversible cell destructionthrough protein denaturation and coagulation as well as cellmembrane destruction, bubble formation around goldnanoparticles is also involved in the case of short pulselaser irradiation, which imposes mechanical stress leadingto cell damage. Irradiation with short laser pulses has beenshown to lead to the rapid heating of the particles and va-porization of a thin layer of fluid surrounding each particle,producing a microscopic version of underwater explosionand cavitation bubble formation [84–86, 88, 124, 125].Zharov et al. [88] also found that nanoclusters formed by theassembly of gold nanoparticles on human breast cancer cellssignificantly enhance the bubble formation causing moreefficient cancer cell killing.
Very recently Khlebtsov et al. theoretically simulated thephotothermal conversion efficiency of the different nano-structures including gold nanospheres, gold nanorods, goldnanoshells, linear chains, 2D arrays, and 3D clusters [91]by calculating their SPR absorption spectra. It was foundthat gold spheres with diameters of about 30–40 nm aremost preferable, as their normalized absorption is maximalin the visible spectrum region. The nanorods with lengthbetween 15 and 70 nm were predicted to be most efficient.Of course, it would also be required that the longitudinalabsorption maximum be matched to the wavelength of theNIR laser to get optimal photothermal efficiency. Goldnanoshells with external diameters of about 50–100 nm andgold shell thicknesses of about 4–8 nm are estimated to bethe most effective due to the strong absorption and lowscattering near 800 nm.
Bioconjugation and targeting
Most laser-based therapeutic methods rely on the use ofendoscopes and fiber optic catheters to deliver lightspecifically to the tumor region and intravenously admin-
Fig. 2 Size, shape, and composition dependence of the surface plasmonabsorption spectrum of plasmonic gold nanostructures. a Nanospheres ofdifferent sizes (reproduced with permission from [110]); b nanorods ofdifferent aspect ratios (reproduced with permission from [118]); c nano-shells of different shell thicknesses (reproduced with permission from[97])
220 Lasers Med Sci (2008) 23:217–228

istered photosensitizers/absorbers to achieve selectivity.However, the use of immunotargeting strategies to deliverthe photodynamic or photothermal agents selectively to thediseased cells and tissue offers an efficient route toachieving selectivity and reducing nonspecific injury tohealthy cells. Metal, especially gold, nanoparticles alloweasy biofunctionalization, thus making them promising forintegration with immunotargeting strategies.
The selectivity of gold nanostructures for photothermalcancer therapy has been demonstrated by their functional-ization with specific tumor-targeting molecules. Twotargeting strategies are commonly used. One involvesnanoparticles passivated by poly (ethylene) glycol (PEG),and the other employs nanoparticles conjugated to anti-bodies specific to biomarkers on the diseased cells. PEG isused to increase the biocompatibility and biostability ofnanoparticles and impart them an increased blood retentiontime. Citrate-capped gold nanospheres, cetyl trimethylam-monium bromide (CTAB)-capped gold nanorods, as well asgold nanoshells have poor stability when they are dispersedin buffer solution due to the aggregating effect of salt ions.By capping the nanoparticles with PEG, the biocompatibil-ity is greatly improved, and nanoparticle aggregation isprevented. PEGylated nanospheres and nanorods can bereadily made by the conjugation of thiol-functionalizedPEG with the gold nanoparticles [126, 127]. In case of invivo applications, PEGylated nanoparticles are preferen-tially accumulated into tumor tissues due to the enhancedpermeability and retention effect, known as the “goldenstandard” for drug design [128–135]. Compared to normaltissue, the blood vessels in tumor tissue are more leaky, andthus, macromolecular or polymeric molecules preferentiallyextravasate into tumor tissue. Due to the decreasedlymphatics, the tumor tissue retains large molecules for alonger time, whereas normal tissue quickly clears out theexternal particles. This tumor targeting method is calledpassive targeting as against the antibody-targeting method[128–135].
The antibody based targeting is more active, specific andefficient. The antibodies are selected to target a specifictumor marker. For instance, anti-epidermal growth factorreceptor (EGFR) antibodies can be employed to targetoverexpressed EGFR on oral cancer cells [89, 90, 92] andcervical cancer cells [136, 137], anti-Her2 for overex-pressed Her2 on breast cancer cells [99] and seprase onbreast cancer cells [88]. The binding of antibodies to goldnanospheres was first reported in the 1950s when anti-bodies were used for the staining of cellular components byelectron microscopy [138]. The antibodies are generallybound to negatively charged citrate-capped gold nano-spheres by nonspecific interactions by adjusting the pH ofthe colloidal solution to be just above the isoelectric point(pI, zero net charge of the protein) of the antibody such that
the antibody has an small net negative charge. The anti-bodies are thus nonspecifically adsorbed onto gold nano-particles while still keeping the nanoparticles negativelycharged, providing stability in colloidal solution. In recentyears, Sokolov et al. [136, 137] used this method to bindanti-EGFR to gold nanospheres, which were then used asoptical labels to detect the overexpressed EGFR on ovariancancer cells by light scattering imaging using a singlewavelength laser. El-Sayed et al. [139] used the samemethod to bind anti-EGFR to gold nanospheres and realizedboth diagnostics using dark field microscopy and therapy oforal cancer cells using a 514 nm argon ion laser [89].
Gold nanorods are capped with CTAB molecules, whichare positively charged [140]. As antibodies are slightlynegatively charged at pH=7.4, antibodies can be adsorbedonto gold nanorods by electrostatic interactions. However,this causes particle aggregation in solution due to theneutralization of the surface charge. For the binding ofantibodies to gold nanorods solution, the surface charge isreversed by adsorption of a PSS− layer [141, 142]. Then,the antibodies are adsorbed onto the PSS− layer probablyby hydrophobic interactions while still stabilizing thenanorods by the negative charge on the antibodies [141,142]. Figure 3a shows the scheme of the antibody bindingto gold nanorods through a PSS bridging layer.
Another method is the use of chemical binding betweena functional group on the antibodies and the metal surfaceof the nanoparticles [143]. The covalent binding of the thiolgroup to gold is used very commonly for nanoparticlesurface bioconjugation. In the work by Liao et al. [126] theantibodies were bound to nanorods with a long chainsuccinimidyl 6-[3′-[2-pyridyldithio]-propionamido] (LC-SPDP) cross-linker hexanoate (see Fig. 3b). LC-SPDP con-sists of a pyridildithio group that binds to the gold nanorodsurface, and an N-hydroxysuccinimide (NHS) ester, whichbinds to the primary amines in the antibodies.
For nanoshell bioconjugation [99], antibody moleculesare first bound to a PEG linker orthopyridyl-disulfide(OPSS)–PEG–NHS through an amidohydroxysuccinimidegroup (NHS). The antibody-PEG linker complex is thenattached to the nanoshell surface through the sulfur-contain-ing OPSS group located at the distal end of the PEG linker.
In addition to antibodies, folic acid can also be used foractive tumor targeting because cancer cells require exces-sive folic acid, which is a ligand for folate receptors [95,102, 144, 145]. Wei and coworkers [95] have conjugatedfolate ligands with oligoethyleneglycol spacers to goldnanorods by in situ dithiocarbamate formation. The folate-conjugated gold nanorods were found to specifically boundto the surface of KB cancer cells. Thus, there exist a varietyof surface chemistry techniques that can be utilized fordesigning biofunctionalized nanoparticles targeted to thedisease biomarker of choice.
Lasers Med Sci (2008) 23:217–228 221

PPTT by visible lasers
In 1999, Lin et al. [125] first reported the selective PTTbased on the use of light-absorbing microparticles thatabsorb light in the visible region. In 2003, they demon-strated selective PPTT using gold nanoparticle immuno-conjugates [84]. Lymphocytes incubated with goldnanoparticles conjugated to antibodies and then exposedto short laser pulses (565 nm wavelength, 20 ns duration)showed cell death with 100 laser pulses at an energy of0.5 J/cm2. The cell death is attributed mainly to thecavitation bubble formation around the nanoparticles. Byadjusting the particle number, size, and laser energy, theresearchers were able to selectively induce cell death ortransiently modify cellular functions without causing celldestruction. In the same year, Zharov et al. [85] studied thethreshold and the dynamics of thermal events around theparticles incorporated into K562 cancer cells using nano-second Nd–YAG laser at 532 nm and a photothermalcontrast technique. They found that, at an energy level of2–3 J/cm2, only one or three laser pulses are sufficient todamage a cell containing 10–15 particles of 20 nm size,whereas at a lower fluence rate of 0.5 J/cm2, at least 50pulses and approximately 100 particles are required toproduce the same harmful effects on the cells.
Recently, El-Sayed and coworkers [89, 90] demonstratedselective PPTT by using gold nanoparticles with a visiblecontinuous wave (CW) laser. In these studies, 40 nm goldnanoparticle were conjugated to anti-EGFR antibodies andthen incubated with both human oral cancer cells andnonmalignant skin cells for 30 min. By using dark fieldlight scattering imaging and surface plasmon absorption
spectroscopy, it was found that gold nanoparticles werepreferentially and specifically bound to the cancer cells,while only a heterogeneous nonspecific distribution of thenanoparticles was seen over the healthy cells [139]. Thenanoparticle-labeled cells were then exposed to a CW argonion laser at 514 nm [89]. It was found that the malignantcells required less than half the laser energy to be killed ascompared to the benign cells (see Fig. 4, [89]). Nophotothermal destruction was observed for any of the celltypes without nanoparticle labeling, even at four times theenergy required to kill the malignant cells labeled with anti-EGFR/gold nanoparticle conjugates. This selective photo-damage of the cancer cells is clearly attributed to the highergold nanoparticle loading on cancer cells due to theoverexpressed EGFR on the cancer cell surface. Highergold nanoparticle labeling results in a consequently higheroptical density. Thus, a lower laser energy is required toraise the temperature above the threshold for destruction, asestimated to be in the range of 70–80°C [90]. This methodcan be extended to other types of cancers as well becausemost types of cancer cells have an overexpression of EGFRreceptors. However, the use of visible light absorbingnanospheres is restricted to skin or near-surface typecancers due to the inability of visible light to penetratethrough skin and tissue.
PPTT by NIR lasers
For in vivo therapy for tumors under skin and deeply seatedwithin tissue, NIR light is required because of its deeppenetration due to minimal absorption of the hemoglobin
Fig. 3 Antibody conjugation ofgold nanorods. a Gold nanorodsare coated with PSS polyelec-trolytes and antibodies areadsorbed onto PSS by nonspe-cific interactions; b antibodiesare covalently bound to the rodsurface by LC-SPDP crosslinker(reproduced with permissionfrom [126])
222 Lasers Med Sci (2008) 23:217–228

and water molecules in tissues in this spectral region.Carbon nanotubes have optical absorbance in the NIRwindow [146] and, thus, have potential for NIR PTT. Daiand coworkers [102] achieved selective cancer celldestruction by the functionalization of single-walled carbonnanotubes with a folate moiety that selectively targets thefolate receptors on tumor cells, while the receptor-freenormal cells are unaffected.
Gold nanorods and nanoshells have been demonstratedfor selective PPTT using CW NIR lasers mainly by the El-Sayed [92] and Halas groups [96, 99], respectively. Byusing dark-field light scattering imaging, El-Sayed andcoworkers found that gold nanorods conjugated to anti-EGFR antibodies were well organized on the surface ofcancer cells with relatively higher binding affinity, whilethey were randomly distributed nonspecifically on andaround the normal cells, similar to the case of the goldnanospheres [92, 139]. A CW Ti:Sapphire laser with awavelength at 800 nm, overlapping with the SPR absorp-tion wavelength maximum of gold nanorods at 800 nm,was used for the photoirradiation of the cells labeled withthe nanorods. It was found that the cancer cells requiredhalf the laser energy (10 W/cm2) to be photothermally
damaged as compared to the normal cells (20 W/cm2), asattributed to the selective targeting of the overexpressedEGFR on the cancer cell surface by the anti-EGFR-conjugated gold nanorods (Fig. 5).
Later, Takahashi et al. [93] in Japan achieved cell deathusing phosphatidylcholine-passivated gold nanorods and apulsed Nd–YAG laser at 1,064 nm. Recently, Wei andcoworkers at Purdue University [95] demonstrated that goldnanorods conjugated to folate ligands can be used forhyperthermic therapy of KB oral cancer cells with a CWTi:Sapphire laser. Severe blebbing of cell membraneswas observed at laser irradiation with power density aslow as 30 J/cm2.
The work by Halas and coworkers has shown that goldnanoshells can be used for PPTT in the NIR region by bothpassive cancer targeting using PEG-conjugated nanoshells[96–98] and active targeting using antibody-conjugatednanoshells [99]. In the antibody case [99], gold nanoshellsconjugated through PEG linkers to anti-Her2 antibodieswere employed for targeting breast cancer cells. A diodelaser at 820 nm was used for photothermal heating (7 min)of the labeled cells (Fig. 6). Only the cancer cells incubatedwith the antibody conjugated gold nanoshells were dam-
Fig. 4 Selective PPTT for can-cer cells by using anti-EGFRconjugated gold nanospheres(reproduced with permissionfrom [89]). After incubationwith anti-EGFR conjugated goldnanoparticles, HaCat normalcells are destroyed at a laserpower threshold of 57 W/cm2,while HSC and HOC cancercells are destroyed at muchlower thresholds of 25 and19 W/cm2, respectively. Thedifference reflects the muchlarger density of anti-EGFRconjugated gold nanospheres onthe surface of the cancer cellscompared to that on the normalcells due to the selective target-ing of EGFR overexpressed oncancer cells
Lasers Med Sci (2008) 23:217–228 223

aged under the laser irradiation. In the PEG case [96], theresearchers demonstrated successful PTT both in vitro and
in vivo. For in vivo therapy, the researchers achievedsuccessful targeting using the PEGylated gold nanoshells
Fig. 6 Selective PPTT for can-cer cells by using anti-Her2antibody conjugated gold nano-shells (reproduced with permis-sion from [99]). Only the cellsincubated with anti-Her2 anti-body conjugated gold nano-shells are damaged under NIRirradiation
Fig. 5 Selective PPTT for can-cer cells in the NIR region byusing anti-EGFR conjugatedgold nanorods (reproduced withpermission from [92]). Afterincubation with anti-EGFR con-jugated gold nanorods, HaCatnormal cells are destroyed at alaser power threshold of 20 W/cm2, while HSC and HOC can-cerous cells are destroyed at amuch lower threshold of 10 W/cm2. The difference reflects themuch larger density of goldnanorods on the surface of thecancer cells compared to that onthe normal cells
224 Lasers Med Sci (2008) 23:217–228

injected directly into the tumor region [96] or deliveredintravenously [98]. It was shown that NIR light of 820 nmat 4 W/cm2 caused irreversible tumor tissue damage. Mostnotably, these studies show that laser dosages required toinduce tissue damage using the plasmonic gold nano-structures are 10- to 25-fold lower than those used instudies employing photoabsorbing dyes such as indocya-nine green dye.
Summary
Plasmonic gold nanostructures thus show great promise forthe selective PTT for cancer as well as other diseases. Wepropose the name PPTT for this treatment. It is realized thata number of variables need to be further addressed, e.g.,stability, biocompatibility, and chemical reactions of nano-particle bioconjugates in physiological environments, bloodretention time, tumor extravasation, the fate of the nano-particles following therapy, etc. We anticipate that thesuccess and promise of the initial use of plasmonicnanoparticles for selective PPTT could be efficientlyextended to clinical stage once the optimal parameters ofthese variables are identified, as is being done throughcurrent research studies.
Acknowledgment We thank the financial support of NCI Center ofCancer Nanotechnology Excellence (CCNE) Award (U54CA119338).
References
1. Breasted JH (1930) The Edwin Smith surgical papyrus, vol 1.University of Chicago
2. Gazelle GS, Goldberg SN, Solbiati L, Livraghi T (2000) Tumorablation with radio-frequency energy. Radiology (Easton, Pa.)217:633–646
3. GoldBerg SN (2001) Radiofrequency tumor ablation: principlesand techniques. Eur J Ultrasound 13(2):129–147
4. Goldberg SN, Dupuy DE (2001) Image-guided radiofrequencytumor ablation: challenges and opportunities—part I. J VascInterv Radiol 12:1021–1032
5. Mirza AN, Fornage BD, Sneige N, Kuerer HM, Newman LA,Ames FC, Singletary SE (2001) Radiofrequency ablation of solidtumors. Cancer J 7:95–102
6. Seegenschmiedt MH, Brady LW, Sauer R (1990) Interstitialthermoradiotherapy: review on technical and clinical aspects.Am J Clin Oncol 13(4):352–363
7. Urano M, Douple E (1992) Physics of microwave hyperthermiain hyperthermia and oncology, vol 3. Springer, Utrecht, TheNetherlands, pp 11–98
8. Sato M, Watanabe Y, Ueda S, Iseki S, Abe Y, Sato N, Kimura S,Okubo K, Onji M (1996) Microwave coagulation therapy forhepatocellular carcinoma. Gastroenterology 110(5):1507–1514
9. Seki T, Wakabayashi M, Nakagawa N, Imamura M, Tamai T,Nishimura A, Yamashiki N, Okamura A, Inoue K (1999)Percutaneous microwave coagulation therapy for patients withsmall hepatocellular carcinoma, Comparison with percutaneousethanol injection therapy. Cancer (Philadelphia) 85:1694–1702
10. Kremkau FW (1979) Cancer therapy with ultrasound: a historicalreview. J Clin Ultrasound 7(4):287–300
11. Huber P, Debus J, Jenne J, Jochle K, van Kaick G, Lorenz WJ,Wannenmacher M (1996) Therapeutic ultrasound in tumortherapy. Principles, applications and new development. Radiol-oge 36(1):64–71
12. Wu F, Chen WZ, Bai J, Zou JZ, Wang ZL, Zhu H, Wang ZB(2001) Pathological changes in human malignant carcinomatreated with high-intensity focused ultrasound. Ultrasound MedBiol 27(8):1099–1106
13. Svaasand LO, Gomer CJ, Morinelli E (1990) On the physicalrationale of laser induced hyperthermia. Lasers Med Sci 5:121–128
14. Gould RG (1959) The LASER, light amplification by stimulatedemission of radiation. The Ann Arbor Conference on OpticalPumping
15. Maiman TH (1960) Stimulated optical radiation in ruby. Nature187:493–494
16. Kapany NS, Peppers NA, Zweng HC, Flocks M (1963) Retinalphotocoagulation by Lasers. Nature 199:146–149
17. Minton JP, Carlton DM, Dearman JR, McKnight WB, KetchamAS (1965) An evaluation of the physical response of malignanttumor implants to pulsed laser radiation. Surg Gynaecol Obstet121:538–544
18. Goldman L (1967) Biomedical aspects of the laser. Springer,New York
19. Goldman L, Rockwell RJ Jr (1968) Laser Systems and theirapplications in medicine and biology. Adv Biomed Eng MedPhys 1:317–382
20. Mullens F, Jennings B, McClusky L (1968) Incision of tissue bycarbon dioxide laser. Am Surg 34:717–729
21. McKenziei AL (1984) Lasers in surgery and medicine. PhysMed Biol 29(6):619–641
22. Boulnois JL (1986) Photophysical processes in recent medicallaser developments. Lasers Med Sci 1(1):47–66
23. Sultan RA (1990) Tumour ablation by laser in general surgery.Lasers Med Sci 5:185–193
24. Gibson KF, Kernohan WG (1993) Lasers in medicine. J MedEng Technol 17(2):51–57
25. Brunetaud JM, Mordon S, Maunoury V, Beacco C (1995) Non-PDT uses of lasers in oncology. Lasers Med Sci 10:3–8
26. Bown SG (1983) Phototherapy of tumours. World J Surg 7:700–709
27. Steger AC, Lees WR, Walmsley K, Bown SG (1989) Interstitiallaser hyperthermia: a new approach to local destruction oftumours. BMJ 299(6695):362–365
28. Masters A, Bown SG (1990) Interstitial laser hyperthermia intumour therapy. Ann Chir Gynaecol 79(4):244–251
29. Masters A, Bown SG (1990) Interstitial laser hyperthermia in thetreatment of tumours. Lasers Med Sci 5:129–136
30. Masters A, Bown SG (1992) Interstitial laser hyperthermia. Br JCancer 8(4):242–249
31. Siegman AE (1986) Lasers, University Science Books. ISBN 0-935702-11-3
32. Silfvast WT (1996) Laser fundamentals, Cambridge UniversityPress. ISBN 0-521-55617-1
33. Svelto O (1998) Principles of lasers, 4th edn. (trans. DavidHanna). Springer. ISBN 0-306-45748
34. Wilson BC (1986) The physics of photodynamic therapy. PhysMed Biol 31:327–360
Lasers Med Sci (2008) 23:217–228 225

35. Danniell MD, Hill JS (1991) A history of PDT. Aust N Z J Surg61:340–348
36. Henderson BW, Dougherty TJ (1992) How does photodynamictherapy work? Photochem Photobiol 55(1):145–157
37. Ochsner MJ (1997) Photophysical and photobiological processesin the photodynamic therapy of tumours. Photochem Photobiol B39(1):1–18
38. Dougherty TJ, Gomer CJ, Henderson BW, Jori G, Kessel D,Korbelik M, Moan J, Peng Q (1998) Photodynamics therapy. JNatl Cancer Inst 90(12):889–905
39. Dolmans DE, Fukumura D, Jain RK (2003) Photodynamictherapy for cancer. Nat Rev Cancer 3(5):380–387
40. Gold MH (2006) Introduction to photodynamic therapy: earlyexperience. Dermatol Clin 25(1):1–4
41. Kim IK, Miller JW (2006) Photodynamic therapy. IntraocularDrug Delivery 129–141
42. Raab O (1900) The effect of fluorescent substances on infusoria.Z Biol 39:524–526
43. Jesionek A, Tappeiner VH (1903) Therapeutische Versuche mitfluoreszierenden Stoffen. Muench Med Wochneshr 47:2042–2044
44. Hausman W (1911) Die sensibilisierende wirkung deshemato-porphyrins. Biochem Z 30:276–286
45. Figge FHJ, Weiland GS, Manganiello LOJ (1948) Affinity ofneoplastic embryonic and traumatized tissue for metalloporphyr-ins. Proc Soc Exp Biol Med 68:640–641
46. Lipson RL, Baldes EJ (1960) The photodynamic properties of aparticular hematoporphyrin derivative. Arch Dermatol 82:508–516
47. Lipson RL, Baldes EJ (1961) Hematoporphyrin derivative: anew aid for endoscopic detection of malignant disease. J ThoracCardiovasc Surg 42:623–629
48. Moan J (1986) Porphyrin photosensitization and phototherapy.Photochem Photobiol 43:681–690
49. Vicente MGH (2001) Porphyrin-based sensitizers in the detec-tion and treatment of cancer: recent progress. Curr Med ChemAnti-Cancer Agents 1(2):175–194
50. Dougherty TJ (1996) A brief history of clinical photodynamictherapy development at Roswell Park cancer institute. J ClinLaser Med 14:219–221
51. Stilts CE, Nelen MI, Hilmey DG, Davies SR, Gollnick SO, OseroffAR, Gibson SL, Hilf R, Detty MR (2000) Water-soluble, core-modified porphyrins as novel, longer-wavelength-absorbing sensi-tizers for photodynamic therapy. Med Chem 43(12):2403–2410
52. Spikes JD (1990) New trends in photobiology (invited review).Chlorins as photosensitizers in biology and medicine. J Photo-chem Photobiol B Biol:259–274
53. Rosenthal I (1990) Phthalocyanines as photodynamic sensitizers.Photochem Photobiol 51:351–356
54. Bonnett R (1995) porphyrin and phthalocyanine photosensitizersfor photodynamic therapy. Chem Soc Rev 24:19–33
55. Anderson RR, Parrish JA (1983) Selective photothermolysis:precise microsurgery by selective absorption of pulsed radiation.Science 220(4596):524–527
56. Parrish JA, Anderson RR, Harrist T, Paul B, Murphy GF (1983)Selective thermal effects with pulsed irradiation from lasers:from organ to organelle. J Invest Dermatol 80:75s–80s
57. Welch AJ (1984) The thermal response of laser-irradiated tissue.IEEE J Quantum Electron 12:1471–1475
58. Jori G, Spikes JD (1990) Photothermal sensitizers: possible usein tumor therapy. J Photochem Photobiol B Biol 6:93–101
59. Soncin M, Busetti A, Fusi F, Jori G, Rodgers MAJ (1999)Irradiation of amelanotic melanoma cells with 532 nm high peakpower pulsed laser radiation in the presence of the photothermal
sensitiser Cu [II]-haematoporphyrin: a new approach to cellphotoinactivation. Photochem Photobiol 69:708–712
60. Camerin M, Rello S, Villanueva A, Ping X, Kenney ME,Rodgers MAJ, Jori G (2005) Photothermal sensitisation as anovel therapeutic approach for tumours: studies at the cellularand animal level. Eur J Cancer 41:1203–1212
61. Camerin M, Rodgers MAJ, Kenney ME, Jori G (2005) Photo-thermal sensitisation: evidence for the lack of oxygen effect onthe photosensitizing activity. Photochem Photobiol Sci 4:251–253
62. Welch AJ (1984) The thermal response of laser irradiated tissue.IEEE J Quantum Electron 20:1471–1481
63. Jacques SL, Prahl SA (1987) Modeling optical and thermaldistributions in tissue during laser irradiation. Lasers Surg Med6:494–503
64. Sturersson C, Andersson-Engels S (1995) A mathematical modelfor predicting the temperature distribution in laser-inducedhyperthermia. Experimental evaluation and applications. PhysMed Biol 40:2037–2052
65. He X, Bischof JC (2003) Quantification of temperature andinjury response in thermal therapy and cryosurgery. Crit RevBiomed Eng 31:355–422
66. Anderson RR, Parrish JA (1981) Microvasculature can beselectively damaged using dye lasers: a basic theory andexperimental evidence in human skin. Lasers Surg Med 1:263–276
67. Greenwald J, Rosen S, Anderson, RR, Harrist T, MacFarland F,Noe J, Parrish JA (1981) Comparative histological studies of thetunable dye (at 577 nm) laser and argon laser: the specificvascular effects of the dye laser. J Invest Dermatol 77:305–310
68. Anderson RR, Parrish JA (1983) Selective photothermolysis:precise micro-surgery by selective absorption of pulsed radiation.Science 200:524–527
69. Morelli JG, Tan OT, Garden J, Margolis R, Seki Y, Bol J, CarneyJM, Anderson ŔR, Furumoto H, Parrish JA (1986) Tunable dyelaser (577 nm) treatment of port wine stains. Lasers Surg Med6:94–99
70. Polla LL, Margolis RJ, Dover JS, Whitaker D, Murphy GF,Jacques SL, Anderson RR (1987) Melanosomes are a primarytarget of Q-switched ruby laser irradiation in guinea pig skin. JInvest Dermatol 89:281–286
71. Ara G, Anderson R, Mandel K, Oseroff AR (1988) Absorptionof ns photoradiation of melanosomes generates acoustic wavesand induces pigmented melanoma cell toxicity. PhotochemPhotobiol 47:37S–40S
72. Chen WR, Adams RL, Heaton E, Dickey DT, Bartels KE,Nordquist RE (1995) Chromophore-enhanced laser tumor tissuephotothermal interaction using an 808 nm diode laser. CancerLett 88:15–19
73. Chen WR, Adams RL, Bartels KE, Nordquist RE (1995)Chromophore-enhanced in vivo tumor cell destruction using anSOS-nm diode laser. Cancer Lett 94:125–131
74. Jori G, Schindl L, Schindl A, Polo L (1996) Novel approachestowards a detailed control of the mechanism and efficiency ofphotosensitized processes in vivo. J Photochem Photobiol AChem 102:101–107
75. Jori G, Spikes JD (1990) Photothermal sensitizers: possible usein tumour therapy. J Photochem Photobiol B Biol 6:93–101
76. El-Sayed MA (2001) Some interesting properties of metalsconfined in time and nanometer space of different shapes. AccChem Res 34:257–264
77. Niemeyer CM (2001) Nanoparticles, proteins, and nucleic acids:Biotechnology meets materials science. Angew Chem Int EdEngl 40:4128–4158
226 Lasers Med Sci (2008) 23:217–228

78. Daniel MC, Astruc D (2004) Gold nanoparticles: Assembly,supramolecular chemistry, quantum-size-related properties, andapplications toward biology, catalysis, and nanotechnology.Chem Rev 104:293–346
79. West JL, Halas NJ (2003) Engineered nanomaterials forbiophotonics applications: improving sensing, imaging, andtherapeutics. Annu Rev Biomed Eng 5:285–292
80. Xia Y, Halas NJ (2005) Shape-controlled synthesis and surfaceplasmonic properties of metallic nanostructures. MRS Bull30:338–348
81. Warren CWC, Maxwell DJ, Gao X, Bailey RE, Han M, Nie S(2002) Luminescent quantum dots for multiplexed biologicaldetection and imaging. Curr Opin Biotechnol 13:40–46
82. Parak WJ, Gerion D, Pellegrino T, Zanchet D, Micheel C,Williams SC, Boudreau R, Le Gros MA, Larabell CA, AlivisatosAP (2003) Biological applications of colloidal nanocrystals.Nanotechnology 14:R15–R27
83. Katz E, Willner I (2004) Integrated nanoparticle-biomoleculehybrid systems: Synthesis, properties, and applications. AngewChem Int Ed 43:6042–6108
84. Pitsillides CM, Joe EK, Wei X, Anderson RR, Lin CP (2003)Selective cell targeting with light-absorbing microparticles andnanoparticles. Biophys J 84:4023–4032
85. Zharov VP, Galitovsky V, Viegas M (2003) Photothermaldetection of local thermal effects during selective nanophoto-thermolysis. Appl Phys Lett 83(24):4897–4899
86. Zharov VP, Galitovskaya E, Viegas M (2004) Photothermalguidance for selective photothermolysis with nanoparticles. ProcSPIE 5319:291–300
87. Hainfeld JF, Slatkin DN, Smilowitz HM (2004) The use of goldnanoparticles to enhance radiotherapy in mice. Phys Med Biol49:N309–N315
88. Zharov VP, Galitovskaya EN, Johnson C, Kelly T (2005)Synergistic enhancement of selective nanophotothermolysis withgold nanoclusters: potential for cancer therapy. Lasers Surg Med37:219–226
89. El-Sayed IH, Huang X, El-Sayed MA (2006) Selective laserphoto-thermal therapy of epithelial carcinoma using anti-EGFRantibody conjugated gold nanoparticles. Cancer Lett 239(1):129–135
90. Huang X, Jain PK, El-Sayed IH, El-Sayed MA (2006)Determination of the minimum temperature required for selec-tive photothermal destruction of cancer cells using immunotar-geted gold nanoparticles. Photochem Photobiol 82(2):412–417
91. Khlebtsov B, Zharov V, Melnikov A, Tuchin V, Khlebtsov N(2006) Optical amplification of photothermal therapy with goldnanoparticles and nanoclusters. Nanotechnology 17:5167–5179
92. Huang X, El-Sayed IH, El-Sayed MA (2006) Cancer cellimaging and photothermal therapy in the near-infrared regionby using gold nanorods. J Am Chem Soc 128(6):2115–2120
93. Takahashi H, Niidome T, Nariai A, Niidome Y, Yamada S (2006)Gold nanorod-sensitized cell death: Microscopic observation ofsingle living cells irradiated by pulsed near-infrared laser light inthe presence of gold nanorods. Chem Lett 35(5):500–501
94. Takahashi H, Niidome T, Nariai A, Niidome Y, Yamada S (2006)Photothermal reshaping of gold nanorods prevents further celldeath. Nanotechnology 17:4431–4435
95. Huff TB, Tong L, Zhao Y, Hansen MN, Cheng JX, Wei A (2007)Hyperthermic effects of gold nanorods on tumor cells. Nano-medicine 2(1):125–132
96. Hirsch LR, Stafford RJ, Bankson JA, Sershen SR, Price RE,Hazle JD, Halas NJ, West JL (2003) Nanoshell-mediated nearinfrared thermal therapy of tumors under MR Guidance. ProcNatl Acad Sci 100:13549–13554
97. Loo CH, Lin A, Hirsch LR, Lee MH, Barton J, Halas NJ, West J,Drezek RA (2004) Nanoshell-enabled photonics-based imagingand therapy of cancer. Tech Cancer Res Treat 3:33–40
98. O’Neal DP, Hirsch LR, Halas NJ, Payne JD, West JL (2004)Photothermal tumor ablation in mice using near infraredabsorbing nanoshells. Cancer Lett 209:171–176
99. Loo C, Lowery A, Halas NJ, West JL, Drezek R (2005)Immunotargeted nanoshells for integrated cancer imaging andtherapy. Nano Lett 5:709–711
100. Chen J, Wiley B, Li ZY, Campbell D, Saeki F, Cang H, Au L,Lee J, Li X, Xie Y (2005) Gold nanocages: engineering theirstructure for biomedical applications. Adv Mater 17:2255–2261
101. Hu M, Petrova H, Chen J, McLellan JM, Siekkinen AR,Marquez M, Li X, Xia Y, Hartland GV (2006) Ultrafast laserstudies of the photothermal properties of gold nanocages. J PhysChem B 110(4):1520–1524
102. Shi Kam NW, O’Connell M, Wisdom JA, Dai H (2005) Carbonnanotubes as multifunctional biological transporters and near-infrared agents for selective cancer cell destruction. Proc NatlAcad Sci 102(33):11600–11605
103. Faraday M (1857) Experimental relations of gold (and othermetals) to light. Philos Trans 147:145–181
104. Turkevich J, Stevenson PC, Hillier J (1951) A study of thenucleation and growth processes in the synthesis of colloidalgold. Discuss Faraday Soc 11:551951
105. Kerker M (1969) The scattering of light and other electromag-netic radiation. Academic, New York
106. Papavassiliou GC (1979) Optical properties of small inorganicand organic metal particles. Prog Solid State Chem 12:185–271
107. Bohren CF, Huffman DR (1983) Absorption and scattering oflight by small particles. Wiley, New York
108. Kreibig U, Vollmer M (1995) Optical properties of metalclusters. Springer, Berlin Heidelberg New York
109. Link S, El-Sayed MA (1999) Spectral properties and relaxationdynamics of surface plasmon electronic oscillations in gold andsilver nanodots and nanorods. J Phys Chem B 103:8410–8426
110. Link S, El-Sayed MA (1999) Size and temperature dependenceof the plasmon absorption of colloidal gold nanoparticles. J PhysChem B 103:4212–4217
111. Link S, El-Sayed MA (2000) Shape and size dependence ofradiative, non-radiative and photothermal properties of goldnanocrystals. Int Rev Phys Chem 19:409–453
112. S Link, El-Sayed MA (2003) Optical properties and ultrafastdynamics of metallic nanocrystals. Ann Rev Phys Chem 54:331–366
113. Mie G (1908) Contribution to the optics of turbid media,especially colloidal metal suspensions. Ann Phys 25:377–445
114. Gans R (1915) Form of ultramicroscopic particles of silver. AnnPhys 47:270–284
115. Link S, Mohamed MB, El-Sayed MA (1999) Simulation of theoptical absorption spectra of gold nanorods as a function of theiraspect ratio and the effect of the medium dielectric constant. JPhys Chem B 103:3073–3077
116. Link S, El-Sayed MA (2005) Simulation of the opticalabsorption spectra of gold nanorods as a function of their aspectratio and the effect of the medium dielectric constant. J PhysChem B 109:10531–10532 (erratum)
117. Murphy CJ, Sau TK, Gole A, Orendorff CJ, Gao J, Gou L,Hunyadi S, Li T (2005) Anisotropic metal nanoparticles:Synthesis, assembly, and optical applications. J Phys Chem B109:13857–13870
118. Nikoobakht B, El-Sayed MA (2003) Preparation and growthmechanism of gold nanorods (NRs) using seed-mediated growthmethod. Chem Mater 15:1957–1962
Lasers Med Sci (2008) 23:217–228 227

119. Oldenburg SJ, Averitt RD, Westcott SL, Halas NJ (1998)Nanoengineering of optical resonances. Chem Phys Lett288:243–247
120. Prodan EM, Radloff C, Halas NJ, Nordlander P (2003) Ahybridization model for the plasmon response of complexnanostructures. Science 302:419–422
121. Jain PK, Lee KS, El-Sayed IH, El-Sayed MA (2006) Calculatedabsorption and scattering properties of gold nanoparticles ofdifferent size, shape, and composition: applications in biologicalimaging and biomedicine. J Phys Chem B 110:7238–7248
122. Du H, Fuh RA, Li J, Corkan A, Lindsey JS (1998) Photo-chemCAD††: a computer-aided design and research tool inphotochemistry. Photochem Photobiol 68:141–142
123. Weissleder R (2001) A clearer vision for in vivo imaging. NatBiotechnol 19:316–317
124. Lin CP, Kelly MW (1998) Cavitation and acoustic emissionaround laser-heated microparticles. Appl Phys Lett 72:2800–2802
125. Lin CP, Kelly MW, Sibayan SAB, Latina MA, Anderson RR(1999) Selective cell killing by microparticle absorption ofpulsed laser radiation. IEEE J Quantum Electron 5:963–968
126. Liao H, Hafner JH (2005) Gold nanorod bioconjugates. ChemMater 17:4636–4641
127. Niidome T, Yamagata M, Okamoto Y, Akiyama Y, Takahashi H,Kawano T, Katayama Y, Niidome Y (2006) PEG-modified goldnanorods with a stealth character for in vivo applications. JControl Release 114:343–347
128. Maeda H (2001) The enhanced permeability and Retention(EPR) effect in tumor Vasculature: the key role of Tumor-selective macromolecular drug targeting. Adv Enzyme Regul41:189–207
129. Maedaa H, Fanga J, Inutsukaa T, Kitamoto Y (2003) Vascularpermeability enhancement in solid tumor: various factors,mechanisms involved and its implications. Int Immunopharma-col 3:319–328
130. Fang J, Sawa T, Maeda H (2003) Factors and mechanism of“EPR”effect and the enhanced antitumor effects of macromolec-ular drugs including SMANCS. Adv Exp Med Biol 519:29–49
131. Paciotti GF, Myer L, Weinreich D, Goia D, Pavel N, McLaughlinRE, Tamarkin L (2004) Colloidal gold: a novel nanoparticlevector for tumor directed drug delivery. Drug Deliv 11:169–183
132. Greish K, Sawa T, Fang J, Akaike T, Maeda H (2004)SMAdoxorubicin, a new polymeric micellar drug for effectivetargeting to solid tumors. J Control Release 97:219–230
133. McNeil SE (2005) Nanotechnology for the biologist. J LeukocBiol 78:585–594
134. Kommareddy S, Amiji M (2007) Biodistribution and pharmaco-kinetic analysis of long-circulating thiolated gelatin nanoparticlesfollowing systemic administration in breast cancer-bearing mice.J Pharm Sci 96(2):397–407
135. Pissuwan D, Valenzuela SM, Cortie MB (2006) Therapeuticpossibilities of plasmonically heated gold nanoparticles. TrendsBiotech 24(2):62–67
136. Sokolov K, Follen M, Aaron J, Pavlova I, Malpica A, Lotan R,Richards-Kortum R (2003) Real-time vital optical imaging ofprecancer using anti–epidermal growth factor receptor antibodiesconjugated to gold nanoparticles. Cancer Res 63:1999–2004
137. Sokolov K, Aaron J, Hsu B, Nida D, Gillanwater A, Follen M,Macaulay C, Adler-Storthz K, Korgel B, Discour M, PasqualiniR, Arap W, Lam W, Richartz-Kortum R (2003) Optical systemsfor in vivo molecular imaging of cancer. Technol Cancer ResTreat 2(6):491–504
138. Hayat MA (1989) Colloidal gold: principles, methods andapplications, vol 1 edn. Academic, San Diego
139. El-Sayed IH, Huang X, El-Sayed MA (2005) Surface plasmonresonance scattering and absorption of anti-EGFR antibodyconjugated gold nanoparticles in cancer diagnostics: applicationsin oral cancer. Nano Lett 5:829–834
140. Nikoobakht B, El-Sayed MA (2001) Evidence for bilayerassembly of cationic surfactants on the surface of gold nanorods.Langmuir 17:6368–6374
141. Ai H, Fang M, Jones SA, Lvov YM (2002) Electrostatic layer-by-layer nanoassembly on biological microtemplates: platelets.Biomacromolecules 3:560–564
142. Caruso F, Niikura K, Furlong DN, Okahata Y (1997) Assemblyof alternating polyelectrolyte and protein multilayer films forimmunosensing. Langmuir 13:3427–3433
143. Liao H, Hafner JH (2005) Gold nanorod bioconjugates. ChemMater 17:4636–4641
144. Leamon CP, Low PS (2001) Folate-mediated targeting: fromdiagnostics to drug and gene delivery. Drug Discov Today 6:44–51
145. Nayak S, Lee H, Chmielewski J, Lyon LA (2004) Folate-mediated cell targeting and cytotoxicity using thermoresponsivemicrogels. J Am Chem Soc 126:10258–10259
146. O’Connell MJ, Bachilo SM, Huffman CB, Moore VC, StranoMS, Haroz EH, Rialon, KL, Boul PJ, Noon WH, Kittrell C, MaJ, Hauge RH, Weisman RB, Smalley RE (2002) Band gapfluorescence from individual single-walled carbon nanotubes.Science 297:593–596
228 Lasers Med Sci (2008) 23:217–228