Embed Size (px)
Citation preview

158
IMPACT OF CHLORAMPHENICOL USE ON BACTERIALRESISTANCE IN A NEONATAL INTENSIVE CARE UNIT
SIR,-Dr Mulhall and her colleagues (Feb 5, p 284) concluded thatchloramphenicol should be the drug of choice for neonatal
meningitis. While evaluating chloramphenicol in the treatment ofserious bacterial infections in the newborn 1,2 we also monitored theeffect of liberal chloramphenicol use on the antibiotic susceptibilitypatterns of bacterial pathogens isolated from infants in the 37-bedintensive care nursery at the Hospital for Sick Children, Toronto.For 9 months (phase 1) treatment for suspected neonatal sepsis
was with ampicillin and gentamicin. In phase 2 (7 months) it wasampicillin and gentamicin, ampicillin and amikacin, or ampicillinand chloramphenicol, each regimen being started on a group ofneonates every third day. In phase 3 (5 months) babies withsuspected sepsis were assigned, on an alternate day basis, to
ampicillin and gentamicin or to ampicillin and amikacin. Theduration of antibiotic therapy depended on the bacteriological,radiological, and clinical findings, as follows:
Negative bacterial cultures, no X-ray evidence of pneumoma, stable clinicalstatus after 72 h therapy.-Antibiotics discontinued.
Infection by gram-positive organism.-AntiblOtic regimen usually altered tosingle drug therapy with the most active penicillin.
InfectIOn by gram-negative organum resistant to assigned regimen. -Treatmentaltered to include an antibiotic active against the isolate.
InfectIOn bv gram-negative organzsm sensitive to current therapy.-No changein therapy.
Antibiotics were given for 14 days for septicaemia or urinary tract infectionfor 21 days for documented bacterial meningitis, and for 7-10 days to babieswho, though culture negative, had a chest X-ray suggestive of pneumonia orwere clinically unstable.
Throughout the study we monitored resistance to
chloramphenicol, amikacin, and gentamicin of Escherichia coli andKlebsiella spp from clinical specimens, using the agar dilutionmethod. Resistance was defined by a minimal inhibitoryconcentration of >16 (chloramphenicol) 8 (amikacin), and 2g/ml (gentamicin). During phases 2 and 3 chloramphenicolresistance amongst gram-negative isolates in the stools of the
nursery population was also assessed. Stool samples were collectedweekly from all patients. For bacteriological analysis 70 mg sampleswere suspended in sterile normal saline, shaken vigorously, andplated on to MacConkey agar with or without 8 g/mlchloramphenicol. Gram-negative isolates were analysed by a pourplate technique if the patient was on antibiotics at the time of stoolcollection or by serial 2-fold dilutions of the original suspendedsample if he or she was not.43 pathogens (E coli or Klebsiella) were isolated from infected
neonates during this study. Chloramphenicol resistance (0/10 inphase 1) increased to 9/18 (50%) in phase 2 and fell in phase 3 to0/15. Gentamicin resistance (40% in phase 1) and amikacinresistance (20%) were not detected in phases 2 and 3.The frequency of chloramphenicol resistance amongst gram-
negative enteric flora during phases 2 and 3 was not different. 39%of 87 stools which yielded organisms on culture during phase 2contained chloramphenicol resistant gram-negative isolates
compared with 43% of 256 submitted stools during phase 3. Of 251stool specimens collected from babies more than 4 days of age whowere receiving antibiotics, 131 (52%) had no organisms isolatedwhile of 257 stool specimens collected from babies not receivingantibiotics only 51 (20%) had sterile stools.
In neonatal intensive care units the empirical initiation ofantibiotic therapy is a common practice-on one estimate 15-28babies receive antibiotics for every one who is actually infected.3 3The risk is the emergence of resistant organisms, as we found forchloramphenicol. The considerable evidence from neonatalintensive care units of a direct correlation between the widespreaduse of a specific antibiotic and resistance amongst gram-negative
1. Rajchgot P, Prober CG, Soldin S, Golas C, Good F, Harding E, MacLeod S. Initiationof chloramphenicol therapy in the newborn infant. J Pediatr 1982; 101: 1018-21.
2. Rajchgot P. Prober CG. Soldin S, Golas C, Good F, Harding E, MacLeod S. Towardsoptimization of antibiotic therapy in the neonate Clin Pharmacol Ther 1983; 33:551-55.
3 Hammerschlag MR, Klein JO, Herschel M, Chen FCJ, Fernin R. Patterns of use ofantibiotics in two newborn nurseries N Engl J Med 1977; 296: 1268.
organisms includes one assessment4 of chloramphenicol. The florafrom two nurseries were compared, one using kanamycin andpenicillin for the empirical treatment of babies with suspectedsepsis and the other using chloramphenicol. In the nursery whichroutinely used chloramphenicol 43% of E coli strains were resistantto >20 fg/ml of chloramphenicol whereas in the other nursery only1307o were resistant.In our study stool surveillance was not predictive of the sensitivity
of gram-negative pathogens, a lack of relationship noted in anotherintensive care nursery setting.5 The suppressive effect of systemicantibiotics on neonatal gastrointestinal flora that we found has alsobeen recorded by Bennet et al. 6Our study raises serious concern about the liberal use of
chloramphenicol in an intensive care nursery. The widespreadintroduction of any antimicrobial agent into such a setting should beaccompanied by careful surveillance, though surveillance culturesof colonising flora seems to be of doubtful value.
Supported in part by research grant PR 922 from the Ontario Ministry ofHealth.
Divisions of Infectious Diseasesand Clinical Pharmacologyand Department of Bacteriology,
Hospital for Sick Childrenand University of Toronto,
Toronto, Ontario, Canada M5G 1X8
CHARLES G. PROBERPERCY RAJCHGOTROBERT M. BANNATYNEROSE CHEUNGFRANCIS GOODELIZABETH HARDINGSTUART MACLEOD
PLASMA FRACTIONATION METHODS AND T-CELLSUBSETS IN HAEMOPHILIA
SIR,-Abnormalities of T-lymphocyte subset distribution,characterised by low helper/suppressor (T4/T8), ratios are commonin US haemophiliacs treated with commercial factor VIIIconcentrates. However, patients with acquired immunodeficiencysyndrome (AIDS) represent a very small proportion of thoseexposed to factor VIII.7,8 In the UK more than half the factor VIIIused is derived from commercial donors in the United States9 andpublic attention has focused on the possibility that importedconcentrates might carry greater risks than similar products made inthe UK from volunteer donor plasma. The evidence from Scotland(May 28, p 1226) and Australia (July 2, p 50) for low T4/T8 ratios inpatients treated exclusively with locally produced blood productsargues against this possibility. US -patients treated with
cryoprecipate from volunteer donors have been reported to havenormal T4/T8 ratios, but the validity of this finding has beenquestioned 10 and others have found abnormal results. 11 lWe have studied 64 patients with haemophilia A (mean age 32,
range 4-80) treated with both commercial and NHS factor VIIIconcentrates, 22 patients with haemophilia B (mean age 34, range3-61) treated with NHS factor IX concentrate alone, and 31untransfused healthy male controls (mean age 31, range 23-44).Only 1 patient had clinical features of AIDS; a patient withhaemophilia A had unexplained lymphadenopathy. The patientswere subdivided into those who had received more or less than25 000 units of concentrate in 1982, a figure which approximates toaverage annual usage per patient in the UK.9 Amounts used in 1982reflected the intensity of treatment in previous years. Tlymphocytes were typed by flow cytometry on an ’EPICS’V’ cellsorter.
4. Dery P, Marks MI, MacKay E. Susceptibilities of bacteria to different antibioticregimens. Study in two nursery populations. Am J Dis Child 1975; 129: 328-330.
5. White RD, Townsend TR, Stephens MA, Moxon ER. Are surveillance of resistantenteric bacilli and antimicrobial usage among neonates in a newborn intensive careunit useful? Pediatrics 1981; 68: 1-4.
6 Bennet R, Eriksson M, Nord CE, Zetterstrom R. Suppression of aerobic and anaerobicfaecal flora in newborns receiving parenteral gentamicin and ampicillin. ActaPaediatr Scand 1982; 71: 559-64.
7. Desforges JF AIDS and preventative treatment in hemophilia. N Engl J Med 1983,308: 94-95.
8. White GC, Lesesne HR. Hemophilia, hepatitis and the acquired immunodeficiencysyndrome. Ann Intern Med 1983; 98: 403-04.
9. Rizza CR, Spooner RJD. Treatment of haemophilia and related disorders in Britainand Northern Ireland during 1976-80: Report on behalf of the directors of
haemophilia centres in the United Kingdom. Br Med J 1983; 286: 929-33.10. Levine PH. T-cell subsets in hemophilia. N Engl J Med 1983: 308: 1293.11. Counts RB, Hansen JA. T-cell subsets in hemophilia. N Engl J Med 1983; 308: 1292

159
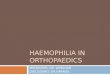
T lymphocyte helper/suppressor ratios in haemophiliacs andcontrols.
Horizontal bars indicate mean values.
21 of the 47 patients with haemophilia A in the high exposuregroup, but only 1 of the 17 in the low exposure group, had T4/T8ratios below the lowest control value (figure). All the patients withhaemophilia B had normal ratios. Differences between the highexposure haemophilia A group and the controls and between thehigh and low exposure haemophilia A groups were significant(Mann Whitney test, p<0 000 and <0 - 005, respectively). Therewere no significant differences between the factor IX treatedpatients and controls.The observed differences between factor VIII and IX treated
patients seem more likely to be causally related to differences infractionation methods than to differences in donor plasma sources,since small numbers of US patients treated with commercial factorIX concentrates have also been found to have normal T4/T8 ratios. 12NHS factor VIII concentrate is prepared by aluminium hydroxideabsorption of cryoprecipitate, whereas factor IX is fractionatedfrom cryosupernatant using DEAE cellulose. Comparativeexamination of fractionation intermediates and procedures may be amore profitable approach to resolution of the problem oftransfusion-induced immunological abnormalities than attention todonor pool sources. Our observations also suggest that low T4/T8ratios may have simple biochemical causes and should not
necessarily be regarded as being predictive of AIDS.
Haemophilia Centreand Department of Immunology,
Royal Free Hospital,London NW3 2QG
CHRISTINE A. LEE
G. JANOSSYJ. ASHLEYP. B. A. KERNOFF
STATISTICS, T-LYMPHOCYTE SUBPOPULATIONS,AND HAEMOPHILIA
SIR,-The paper by Dr Luban and colleagues (March 5, p 503)reporting abnormal distributions ofT-lymphocyte subpopulationsin children and adolescents with haemophilia was interesting and,with other reports,I.3 suggests that acquired immunodeficiency12. Kessler CM, Schulof RS, Goldstein AL,Naylor PH, Luben NLC, Kelleher JF,
Reaman GH Abnormal T-lymphocyte subpopulations associated with transfusionof blood-derived products. Lancet 1983; i: 991-92.
1. Lederman MM, Ratnoff OD, Scillian JJ, Jones PK, Schacter B. Impaired cell-mediatedimmunity in patients with classic hemophilia. N Engl J Med 1983; 308: 79-83.
2. Menitove, JE, Aster RH, Casper JT et al. T-lymphocyte subpopulations in patientswith classic hemophilia treated with cryoprecipitate and lyophilized concentrates. NEngl J Med 1983; 308: 83-86.
3. Goldsmith JC, Moseley PL, Monick M, Brady M, Hunninghake GW. T-lymphocytesubpopulation abnormalities in apparently healthy patients with hemophilia. AnnIntern Med 1983, 98: 294-96.
syndrome is occurring in haemophiliacs in the United States.
However, Luban et al fell prey to statistical errors when theycompared indices of immune function in the 5 most abnormalhaemophiliacs with data from the other 20 haemophiliacs and withdata from 22 controls.
Comparing values below some cut-off point in a frequencydistribution with those above is a not uncommon error: it is like
backing the winner after a horse race is over. Luban et al should nothave used helper/suppressor ratios to define the 5 "abnormal"haemophiliacs (those with ratios below I - 0) and then comparedthese 5 with the remaining 20 "normal" haemophiliacs with respectto that same ratio. The comparison would have been valid if same 5and 20 patients had been identified before the ratio data wereexamined. Mantel4 provides another example, for a drug given topatients with advanced disease: "suppose that a minimum
requirement for an individual to be classified as a responder is thatthe individual survive at least 12 weeks. A comparison of survivalcurves for responders and nonresponders will then show no earlydeaths for responders, but perhaps many for nonresponders. Theproper comparison should have been for survival beyond 12weeks ..."The comparison of the 5 smallest helper/suppressor ratios of the
haemophiliacs with all the values for the 22 controls, was againbased on posthoc examination of the data-thereby leading to anexaggerated level of significance (p<0-01, presumably one-sided,but the test procedure was not given). Was there a significantdifference between ratios for the 5 abnormal haemophiliacs and the5 controls with the smallest ratios? If we assume that no control hada helper/suppressor ratio below I - 0 and that the cut-off ratio of 1 - 0 0was chosen a priori then the two groups (5/25 vs 0/22) can becompared by Fisher’s exact test, which gives a p value of 0 - 035 (one-sided). Yet even here caution is in order. Two samples can becompared by selecting a cut-off point and then forming a 2 x 2 tablefor the numbers of observations above and below it. However, if acut-off point is selected posthoc so as to maximise the chi squarestatistic, allowance has to be made.5,6
Department of Environmental Medicine,New York University Medical Center,New York, NY 10016, USA
BERNARD S. PASTERNACKMICHAEL MARMOR
FEAR OF AIDS AND GONORRHOEA RATES INHOMOSEXUAL MEN
SIR,-Since June, 1980, the Centers for Disease Control hasreceived reports of 1450 patients with acquired immunodeficiencysyndrome (AIDS) of whom 558 (38-57o) have died. In 1982,coverage of AIDS by medical journals and by national and localnews media mushroomed, and by the end of 1982 most homosexualmen in Denver, Colorado, knew that about 75% of all AIDS caseswere homosexual, that AIDS was probably caused by a sexuallytransmitted agent, and that the major risk factor for AIDS appearedto be the number of male sexual partners per year. It was to be
expected that fear of acquiring an untreatable, ultimately fataldisease of unknown aetiology would influence sexual behaviour.Rates of infection with Neisseria gonorrhoeae should be a sensitive
indicator of changing sexual behaviour because this infection iscommon in homosexual men, it is easy to detect, and the incubationperiod is short. The Denver Metro Health Clinic records over26 000 patient visits per year which include 60% of reported cases ofgonorrhoea from Denver. The table compares rates of gonorrhoeaduring the first three months of 1982 and 1983. It demonstrates asharp reduction both in the prevalence of infection (by 32%) and inthe number of cases (by 39%) in homosexual men but not in hetero-sexual men and women.After a long period of increasingly unrestricted sexual activity and
the resultant higher rates of sexually transmitted diseases, including
4 Mantel N. An uncontrolled clinical trial-treatment response or spontaneousimprovement? Controlled Clin Trials 1982; 3: 369-70.
5. Miller R, Siegmund D. Maximally selected chi square statistics Biometrics 1982; 38:1011-16.
6. Halpern J. Maximally selected chi square statistics for small samples. Biometrics 1982;38: 1017-23.