Embed Size (px)
Citation preview

Introduction:
Haemophilia A is a bleeding disorder that mostly affects men. Haemophilia A is also known as
classic haemophilia. Bleeding disorder is caused by deficiency in clotting factor VIII. Most of the
cases involved in deficiency of clotting cascade enzyme factor VIII are inherited (congenital) and
in some cases, it is acquired, due to autoantibodies directed against factor VIII, and this usually
more frequent in older patient (Franchini, 2005). Bleeding patterns are quite different between
congenital and acquired haemophilia A (Ma & Carrizosa, 2006). The inheritance of haemophilia
A is sex-linked, and it affects 1 in 5,000 to 1 in 10,000 male live births worldwide. In USA alone,
17,000 people were affected with haemophilia A in 2003. It occurs in all races and ethnic groups
without any exception.
Female rarely suffer from the disease. However female can also develop this disease when
mating male who are affected with haemophilia A with carrier female according to mendelian
inheritance. But for this situation, it is approximately 1 in 50 million female births. Inactivation
of X chromosome during embryonic development of female can also cause them to express this
disease if they are the carrier of the disease.
Figure 1: This is the pattern of inheritance in a sex-linked. Basically female is just a carrier for the
condition and male will have high chance to develop the condition.
History:

Haemophilia was first recognised in second century through a collection of Jewish Rabbinical
writings which mentioned that male babies did not have to be circumcised if two brothers had
already died from the procedure. In twelfth century, Moses Maimonides, Jewish physician,
applied the same circumcision ruling to a son of the mother who had married twice, if one of the
half-brother died during circumcision, so his another half-brother should not undergo
circumcision. In the similar century, Arabic surgeon, Albucasis also described a family where
males died because of bleeding after minor injury.
In 1803, Dr. John Conrad Otto introduced the first and modern description of haemophilia A
after he wrote an article entitled “An account of a haemorrhagic disposition existing in certain
families” (Giangrande, 2004). He identified that the condition was hereditary and affected
males. The word haemophilia for a particular kind of disorder was started in 1828, where a
student at University of Zurich, Hopff, labelled the disorder as ‘haemorrhaphilla’, but then the
name changes to haemophilia (Mercadante, 2008). The first treatment of haemophilia was
introduced in 1840, when Samuel Armstrong Lang performed successful blood transfusion to
treat haemophilia patient in London.
Haemophilia is also known as ‘royal disease’ since most of the noble families in Europe carried
the disease and affected by it. It was started by Queen Victoria (Queen of England from 1837
until 1901), where she was a carrier for the disease. Her eighth child, Leopold, was suffered
from the disease, which was confirmed in 1853. Leopald died at the age of 31 because of brain
haemorrhage and his daughter, Alice who was a carrier for the disease passed the disease to her
son, Viscount Trematon who was also died due to brain haemorrhage in 1928.
Figure 2: Pedigree diagram of haemophilia A for Queen Victoria family
In 1952, haemophilia A and haemophilia B was distinguish as two distinct diseases, caused by
deficiency in factor VIII and factor IX respectively. In 1960, clotting factors were identified and

named and in 1964, clotting process was discussed in detail, and interaction of different factors
during clotting was being termed as coagulation cascade.
Classification:
Severity of haemophilia A can be divided into three: severe, moderate and mild. Patients with
haemophilia A, often suffer from conditions like joint and muscle haemorrhage, easy bruising
and prolonged bleeding time from wounds. Untreated bleeding in the joint will lead to severe
swelling and pain, joint stiffness and inflammation (King, 2009). The most common causes of
death from this disease includes bleeding of internal organ especially brain and bleeding after
minor surgery. Below is the table showing the three different severity of haemophilia A (Rull, 2008).
Category
Severity
Factor VIII
activity level
Age of presentation Percentage of
sufferers
Severe disease Less than 1 % Infancy (before 1 year) 43 – 70%
Moderate disease 1 – 5 % 1- 2 years 15 – 26%
Mild disease More than 5% Older than 2 years 15 – 31%
Severe disease of haemophilia A always associated with neonatal bleeding. One to two percent
of the cases of severe disease manifest intracranial haemorrhage. There are also cases with
spontaneous bleeding into joints, especially the knees, ankles and elbows (Nolan, Vidler & Vora,
2003). Intramuscular haemorrhage is also reported. For a moderate disease, it often presents
with bleeding following venepuncture and in mild disease, bleeding tend to occur after major
trauma or surgery.
The main treatment for haemophilia A is replacement therapy. It is by giving or replacing
clotting factor VIII to the patient by infusion or injection. Replacement therapy used to stop
bleeding as needed basis and helps to prevent bleeding.
Pathophysiology

Factor VIII gene (F8 gene) resides near the telemoric end of long arm of the X chromosome at
Xq28, which made up of 186 kilobases and composed of 26 exons (Riley, 2005) & (King, 2009).
Due to its large size, it is more prone to undergo spontaneous mutation. These include
frameshift mutation, missense mutation, nonsense mutation, gene inversion, deletion and
splicing error (King, 2009). Mutation in this gene causes dysfunctional of factor VIII. The most
common haemophilia A mutation result from intrachromosomal inversion of the intron 22
sequence.
Factor VII is a non-covalent heterodimer which made up of heavy chain, light chain and
connecting region. It is synthesised by liver sinusoidal endothelial cells as a large single-chain
polypeptide (Philip, 2005). Connecting region is made up of B domain which a peripheral
satellite structure that is connected by thin stalk to heavy and light chain. There are three A
domains present on the structure. A1 and A2 domains present on heavy chain and A3 domain
present on light chain. Two C domains are present on factor VIII light chain which located next
to A3 domain. Metal ions, Cu and Ca ions are crucial in stabilizing the heterodimer in order to
maintain the integrity of factor VIII. So basically, the arrangement is like this: A1-A2-B-A3-C1-
C2. Detailed structure is shown on figure 2 below.
Figure 2: Structure of VIII (Hoyer, 1994)

Factor VIII plays major role in intrinsic pathway of blood coagulation cascade where it helps to
accelerate the cleavage of factor X to factor Xa by activated factor IXa (Hoyer, 1994). Factor VIII
is a major cofactor for factor IXa, where in the present of calcium ions and phospholipid, they
will form complex and this complex involves in conversion of factor X to factor Xa. Generation of
factor Xa is important, which act as a cofactor for cleavage of prothrombin (factor II) to
thrombin. Thrombin is a cofactor for conversion of fibrinogen to fibrin, which eventually forms
a fibrin clot. Dysfunctional of factor VIII lead to disruption of normal intrinsic coagulation
cascade.
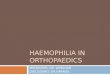
The diagrammatic illustration of coagulation pathway is shown below:
Figure 3: The coagulation pathway, showing the intrinsic pathway, which begins with factor XII
and ultimately terminates with the activation of factor X; the extrinsic pathway, which begins with
factor VII and terminates with the activation of factor X; and the common pathway, which involves
the activation of factor X and ultimately leads to the formation of the fibrin clot (Facci, 1998)
Factor VIII first forms a noncovalent complex with von Willebrand factor (VWF) in the plasma
which protects it from proteolysis and concentrates it at sites of vascular injury (Kaufman et al.,
1989). VWF is serves as binding protein for factor VIII which has capability of binding to
subendothelial matrix protein and adherent platelets. VWF helps to stabilizes Factor VIII
temporarily by competing with low density lipoprotein receptor-related proteins and therefore
inhibit clearance of factor VIII. Beside that VWF also helps in modification of conformational
structure of factor VIII by promoting association of light chain and heavy chain.

Cleavage at light chain of factor VIII by thrombin or factor Xa is required for separation of von
Willebrand factor from factor VIII. This is an important step, which help in the formation of
activated factor VIII (factor VIIIa). Cleavage of heavy chain occurs at Arg 372, which transform
the heavy chain into 54-kd and 44-kd fragments and by the time, factor VIIIa is form (Hoyer,
1994). Separation from von Willebrand factor is essential for factor VIII to undergo
procoagulant activity by binding to the phospholipid surfaces of damaged cells and adherent
activated platelets (Nesheim, et al., 1991). Factor VIIIa also helps to facilitates conformational
change in the active site of factor IXa which permits it to catalyse FX (Ledford-Kraemer, 2006).
Factor VIIIa is an unstable molecule which rapidly loses cofactor function (Hoyer, 1994) and it is
inactivated once it undergoes proteolytic cleavage with activated protein C (Fulcher et al.,
1984). Cleavage of factor VIIIa with protein C occur at two cleavage sites; Arg 336 in A1 subunit
and Arg 562 in A2 subunit (Gale, Cramer, Rozenshteyn & Cruz, 2007).
Acquired haemophilia A can occurs when there is a present of autoantibody against factor VIII.
The antibodies (IgG4k) act as inhibitors which interact with factor VIII, causing inactivation of
factor VIII (Allain, Gaillandre & Lee, 1981). It is much more clinically severe than congenital
haemophilia A. 5 percent to 10 percent of patient with severe haemophilia A due to present of
autoantibody. It is rare with annual incidence of 1 to 2 cases per million people annually, but
equally seen in males and females. Autoantibody directed against factor VIII can cause a
bleeding tendency and basically there are two peaks of age for the onset of acquired
haemophilia (Mannucci & Peyvandi, 2009). In young adult, mostly it occurs in women who
develop this problem during post-partum period. Acquired haemophilia A is more prevalent in
elderly people. It also occurs in patient with B-cell malignancies and connective tissue disorders
such as systemic lupus erythematsus. Acquired Haemophilia A also occurs due to the absence of
factor VIII antigens as a result of gene deletion (Israels & Israels, 1996).

Diagnostic Procedure:
Diagnosis of haemophilia A started when there is unusual bleeding happen in a male patient
(Hoyer, 1994). Diagnosis requires an insight clinical and laboratory evaluation. Further
diagnosis of haemophilia A can then suspected using simple screening test such as prothrombin
time (PT) and activated partial thromboplastin time (APTT). But comfirmation cannot be made
using this test, specific assays are required in identification of the degree of factor VIII
deficiency. Various assays are used in detection of factor VIII deficiency such as 1-stage FVIII
assay, 2-stage FVIII assay, chromogenic factor VIII assay, clot formation and lysis assay (CloFAL)
and Bethesda assay.
In RIPAS Haematology Lab, APTT and PT are use as diagnostic test for suspection of
haemophilia A. They use automated machine to measure the level of APTT and PT of a plasma. If
the PT is normal and APTT is prolonged, it is high possibility that the patient suffer from
defeciency in factor VIII. RIPAS Haematology Lab basically have a reference range specifically
for Brunei’s population, where normal APTT is 34.3 second and within reference range of 26.9
second and 42.6 second. For further comfirmatory diagnostic test of the disease, they usually
send the sample of the plasma to Singapore and they do not normally done it locally in Brunei.

Below is the statistics of coagulation factor deficiency in Brunei Darussalam from June 2009 until
December 2009.
Factor deficiency No. of patient requesting a
test
No. of patient with positive
test
Factor VIII 22 17
Factor IX 15 4
Factor XI 7 3
We can see that, out of 22 patients requested for the test of factor VIII deficiency, 17 patients
were tested positive throughout the 6 months in 2009. This data is collected from haematology
lab RIPAS. This also shows that factor VIII deficiency is quite common in Brunei Darussalam
compare to the other clotting disorder.

Next, I am going to discuss in details of two diagnosis test for an accurate detection of
haemophilia A. The first diagnostic test I going to discuss will be activated partial
thromboplastin time (APTT) test for the initial detection of the disease, then secondly I going to
discuss on further confirmatory diagnosis test of haemophilia A which is using chromogenic
factor VIII assay
(1)Activated Partial Thromboplastin Time (APTT) Test
Activated partial thromboplastin time (APTT) is a global coagulation test sensitive to
deficiencies or abnormalities of clotting factors in intrinsic and common pathway of coagulation
system. The aPTT was first described in 1953 by researchers at the University of North Carolina
at Chapel Hill (Langdell, Wagner & Brinkhous, 1953). The test is known as ‘partial’ because the
reagent in this test does not use tissue factor. Screening with APTT must always be
supplemented with a careful clinical history of the patient’s response to commonly occurring
challenges of haemostasis such as dental extraction, circumcision, tonsillectomy, and accidental
cuts (Koepke, 1991). This test also uses in detection of deficiency in factor IX, XI and XII.
The APTT is a two-staged assay. In first stage, the plasma sample is mixed with phospholipid
(cephalin), an activator (silica or ellagic acid) and calcium. The mixture is incubated for several
minutes. In second stage, calcium chloride is added following activation of contact factor. In the
second stage, Calcium chloride is added to allow activation of IX from Xia to complete
coagulation cascade (Ledford-Kraemer, 2003). Buffer is also added to minimise pH changes in
plasma reaction mixture. The time is measured from the moment plasma sample is mixed with
reagents until clot is forms. A deficiency of the intrinsic pathway will result in prolonged APTT.
It is necessary then to study the history of the individual whether the member of the family have
a bleeding history.
Prolonged APTT can also occur due to the presence of inhibitor towards the factor in intrinsic
pathway. Suspecting patient with acquired Haemophilia A can be done by mixing the patient’s
plasma with normal plasma, and then perform activated partial thromboplastin time (APTT)
test on the mixture. The mixture of normal plasma and the patient’s plasma should be incubated
for up to 2 hours at 37OC. The presence of autoantibody that inhibits factor VIII in the patient’s
plasma will result in prolonged APTT, basically at least 30 seconds longer than the control. This
is because the inhibitor neutralizes factor VIII clotting activity of the normal plasma.

Below is the pathway measured by APTT (Kitchen & McCraw, 2000).
(2) Chromogenic Factor VIII assay
This is a very sensitive assay that has an ability to detect low concentration of factor VIII in
plasma. This technology was first developed in 1970 By M.J. Seghatchian and M.Miller-
Anderson. The principle of this chromogenic factor VIII assay is almost similar with the two-
staged factor VIII assay but it is more accurate compare to when using two-stage factor VIII
assay.
This assay requires reagents cocktail for generation of FXa. Two reagents are use here. The first
reagent contains factor IXa, thrombin, a source of calcium ions and phospholipid. While the
second reagent only contains factor X. This assay also uses chromogenic substrates. This
substrate cleaved by factor Xa and will produce colour change after cleavage. Chromogenic
substrates are artificial peptides which designed to mimic natural substrate for a particular
enzyme. Attached to the peptide is a chromophore, pNA (para-nitroaniline) which responsible
for a colour change when it is release from the peptide after cleavage by an enzyme. It will

produce colour changes that can be measure accurately using optical absorption which directly
proportional to the amount of factor Xa and factor VIIIa. Below is the principle of chromogenic
factor VIII assay
To begin this assay, initially patient’s plasma is incubated together with the two reagents at
37oC. Reagent 1 is mix first with the plasma for about 30 seconds. Then immediately reagent 2 is
added to the mixture. If factor VIII present in the plasma, thrombin in the reagent cocktail will
activates factor VIII to factor VIIIa, in the presence of Ca2+ and phospholipid (Rodgers et.al,
2007). Factor VIIIa acts as cofactor for conversion of factor X to factor Xa. Chromogenic
substrate then added to the mixture. Colour changes are then examined using
spectrophotometer.
There are two methods currently use to measure colour appearance (Ledford-kreamer, 2006):
1) Kinetic method
- In this method, the change in absorbance is read at 405 nm for 30 to 120 seconds.
2) Endpoint method
- Reaction is stopped with an acid and absorbance is measured at 405 nm against a buffer
blank

A reference curve is drawn by plotting the absorbance at 405 nm against concentration on the
graph. Below is an example of data collected from an experiment using chromogenic factor VIII
assay.
Factor VIII
Concentration
(IU/dl)
Absorbance at 405
nm
0 0.04
50 0.19
100 0.32
140 0.44
So using Microsoft excel, I use this data to produce a line graph which is shown below.
With this graph, we can determine the unknown concentration of plasma sample according to
their known absorbance at 405 nm. For example, the absorbance of plasma sample is 0.38 at
505 nm. So according to this graph, the factor VIII concentration is 120 IU/dl.

Conclusion:
Haemophilia A is a blood coagulation disorder that can be congenital and acquired which mostly
occur in male. Patient with haemophilia A suffer from deficiency in factor VIII. Factor VIII is
important in the blood coagulation cascade for cleavage of factor X to factor Xa by activated
factor IXa. Factor VIII bound to von willebrand factor before it gets activated.
There is various techniques use for diagnosis of haemophilia A. Initial screening of haemophilia
A can be done using activated partial thromboplastin time (APTT) and further diagnosis can be
done using one-staged factor VIII assay, two-staged factor VIII assay, chromogenic factor VIII
assay, clot formation and lysis assay (CloFAL) and Bethesda assay.

References:
Allain,J.P., Gaillandre, A. & Lee, H. (1981), Immunochemical characteristisation of antibodies to
factor VIII in hemophillic and non-hemophillic plasmas, j.Lab. Clin. Med. 79, 791-800
Facci, A. (1998), ed. Harrison's Principles of Internal Medicine, 14th edition. New York: McGraw
Hill,
Franchini, M., Gandini, G. & Di Paolantonio, T., (2005) Acquired hemophilia A: a concise review.
Am J Hematol. Sep;80(1):55-63. [abstract]
Fulcher, C.A., Gardiner, J.E., Griffin, J.H., Zimmerman, T.S., Proteolytic inactivation of human
factor VIII procoagulant protein by activated human protein C and its analogy with factor V.
Blood, 1984;63:486-489
Gale,A.J., Cramer, T.J., Rozenshteyn, D. & Cruz, J.R. (2007), Detailed Mechanisms of the
Inactivation of Factor VIIIa by Activated Protein C in the Presence of Its Cofactors, Protein S and
Factor V, The American Society for Biochemistry and Molecular Biology, Inc.
Giangrande, P.L.F.(2004), History of haemophilia, Copyright World Federation of Hemophilia
2006
Hoyer, L. W. (1994). Haemophilia A. The New England Journal of Medicine , 330:1617 (22), 11.
Israel, L.G. & Israels, E.D. (1996), Mechanisms in Haematology, University of Manitoba, Canada
Kaufman, R.J., Wasley, L.C., Davies, M.V., Wise, R.J., Israel, D.I., Dorner, A.J. (1989), Effect of von
willebrand factor coexpression on the synthesis and secretion of factor VIII in Chinese hamster
ovary cells, Mol. Cell Biol, 1989;9:1233-1242
King, M.W. (2009) Haemophilia A, iupui.edu
Kitchen, S. & McCraw, A. (2000), Diagnosis of haemophilia and other bleeding disorder: A
laboratory manual, World Federation of haemophilia,
Koepke, J.A. (1991), Textbook: Practical Laboratory Haemotology, Churchill Livingstone.
Langdell, R.D., Wagner, R.H. & Brinkhous, K.M. (1953). "Effect of antihemophilic factor on one-
stage clotting tests; a presumptive test for hemophilia and a simple one-stage antihemophilic
factor assy procedure". J. Lab. Clin. Med. 41 (4): 637–47.
Ledford-Kreamer, M. (2003), Causes for a Prolonged PT and/or APTT, CLOT-ED, Inc., Copyright
2003. All rights reserved

Ledford-Kreamer, M. (2006), Factor VIII Activity Assay, Coagulation lysis or thrombosis (CLOT-
ED), an educational resource.
Ma, A.D. & Carrizosa,D. (2006), Acquired factor VIII inhibitrors: pathophysiology and treatment,
American Society of Hematology, ©Hematology 2006
Mannucci, P.M. & Peyvandi, F. (2009), Autoimmune haemophilia at rescue, hematologica | 2009;
94(4)
Mercadante, A. (2008), History of haemophilia A, Life style Associated Content, The people’s
media company.
Nesheim, M., Pittman, D.D., Giles, A.R., et al. (1991), The effect of plasma von Willebrand factor
on the binding of human factor VIII to thrombin-activated human platelets, J.Biol Chem 1991;
266:17815-17820
Rodgers, S.E., Duncan, E.M., Barbulescu, D.M., Quinn, D.M. & Lloyd, J.V. (2007) In vitro kinetics of
factor VIII activity in patients with mild haemophilia A and a discrepancy between one-stage
and two-stage factor VIII assay results. Br J Haematol, 136, 138-145
Rull, G.(2008), Haemophilia A (Factor VIII Deficiency) ©EMIS 2008
Hoyer, L. W. (1994). Haemophilia A. The New England Journal of Medicine , 330:1617 (22), 11.
Nolan, B. Vidler, V., Vora, A., et al.(2003). Unsuspected haemophilia in children with single swollen joint. BMJ , 326(7381):151-2.