Embed Size (px)
Citation preview

SABRINA FERREIRA
PLA/PGA COPOLYMER AS A BONE
SUBSTITUTE IN MAXILLARY SINUS
AUGMENTATION. HISTOLOGICAL, HISTOMETRIC
AND IMMUNOHISTOCHEMISTRY STUDY IN
RABBITS
Araçatuba - SP
2014
1
SABRINA FERREIRA
PLA/PGA COPOLYMER AS A BONE
SUBSTITUTE IN MAXILLARY SINUS
AUGMENTATION. HISTOLOGICAL, HISTOMETRIC
AND IMMUNOHISTOCHEMISTRY STUDY IN
RABBITS
Dissertação apresentada à Faculdade de Odontologia do Campus de Araçatuba - FOA, Universidade Estadual Paulista “Júlio de Mesquita Filho” – UNESP, como pré-requisito para obtenção do título de “Mestre em Odontologia” - área de concentração em Cirurgia e Traumatologia Buco-Maxilo-Facial.
Orientador: Prof. Adj. Idelmo Rangel Garcia Júnior.
Araçatuba - SP
2014
2
Dedicatória, Agradecimentos
e Epígrafe

3
Dedicatória
Àqueles que são donos do meu coração e fonte de vida.
À mamãe (Carmen das Graças Ferreira), que com amor incondicional é minha
fortaleza, meu porto seguro, minha vida. Meu exemplo de amor, fé imensurável, compaixão,
humanidade, de força, garra,... de mulher. Com carinho, sempre nos dizia que o estudo seria
a herança que nos deixaria e que tudo na vida se conquista com muito esforço e dedicação.
Obrigada por todo apoio sempre. Te amo.
Ao meu irmão (Danilo Douglas Ferreira) que apesar de toda correria e da distância,
sempre torceu e rezou muito por mim. Te amo meu irmão e você sabe que sempre estarei ao
seu lado junto com a mamãe. Que Deus te abençoe sempre.
Dedico a estes meus amores esta conquista que é fruto de muito amor à minha
profissão, mas também é fruto de muito sacrifício como meses longe de casa com coração
apertado por não poder cuidar dos meus quando precisaram, ou sem poder estar presente
num abraço em seus aniversários. São vocês as flores que alegram e fortalecem minha
caminhada.

4
Agradecimentos Especiais
Primeiramente, agradeço a Deus por todas as graças e por sua imensa misericórdia.
Obrigado Senhor por cuidar de mim e de minha família, por ser luz no nosso caminho, por
mostrar a cada dia que entregue em suas mãos podemos seguir com passos firmes e sem
medo. Obrigada senhor pelos dias alegrias e pelos dias de tristeza quando o senhor me
confortou em seus braços e, principalmente, obrigada pela vida. E seja feita sempre, Senhor, a
vossa vontade!
Ao meu orientador, Prof. Adj. Idelmo Rangel Garcia Júnior. Muito obrigada por tudo.
Obrigada por acreditar em mim, por me confiar grandes trabalhos seus onde tive a
oportunidade de crescer muito na pesquisa, e por permitir que mesmo em meio ao medo e
as dúvidas eu pudesse passar a dar meus próprios passos. Obrigada pela disponibilidade em
todos os momentos que precisei, por me escutar quando eu precisei falar, pelo apoio
fundamental que tanto me trouxe segurança e pela paciência. Aprendi muito com o senhor,
mas sua humildade, sua humanidade e sua inigualável serenidade de quem dá um passo de
cada vez vou guardar como maiores aprendizados. Receba toda minha admiração e gratidão,
mestre. Que Deus continue abençoando o senhor e sua família.
A querida Profa. Ass. Dra. Roberta Okamoto que tão docemente sempre me recebeu
com carinho, obrigada pela disponibilidade e pela imensa participação neste estudo em sua
co-autoria e em tantos outros. É um honra poder aprender com a senhora.
Aos queridos professores da Disciplina de Cirurgia e Traumatologia Buco-maxilo-facial,
Profa. Ass. Dra. Alessandra Marcondes Aranega, Profa. Ass. Dra. Ana Paula Farnezi Bassi, Profa.
Ass. Dra . Daniela Ponzoni, Prof. Ass. Dr. Francisley Avila Souza e Prof. Adj. Osvaldo Magro
Filho, pela amizade, confiança, pelo bom convívio, pelo respeito e por todo aprendizado.
Recebam meu carinho e admiração.

5
Ao querido Prof. Titular Wilson Roberto Poi, pelo exemplo de professor e mestre que
tanto admiro e respeito. Já lhe disse uma vez, mas quero deixar aqui registrado, já o admirava
antes de ser sua aluna. Na graduação tive a honra de ter um mestre que o senhor também
ajudou a formar (Prof. Titular Ronaldo Célio Mariano) e que também levou pra sua carreira
seu exemplo de docência. Este mesmo mestre que contava histórias de um professor da
UNESP de Araçatuba com quem ele muito aprendeu, Prof Poi. E, agora, na pós-graduação,
eu tive o prazer de conhecê-lo e a honra de ser sua aluna. Obrigada pelos ensinamentos e
pelos abraços tão confortantes que aliviavam a dor da distância dos que amo.
A minha doce Dirce Maria (Maria Dirce Colli Boatto), o que eu faria se Deus não tivesse
colocado esse anjo no meu caminho? Não tenho palavras pra dizer o quão importante você
foi pra mim. Aprendi muito com você, tanto quanto como com meus mestres. Obrigada por
todo carinho e paciência em me ensinar tudo o que você levou uma vida pra aprender. Mas
obrigada mesmo pelo carinho de mãe que confia, que acredita e que protege e defende. Te
amo muito. Que Deus continue abençoado você, Sérgio e suas “crianças”.
Ao Léo (Leonardo Perez Faverani), mais um dos anjos que Deus mandou pra me
ajudar nesta caminhada. Foi mais que amigo, foi família. Obrigada, querido, por tanto
carinho, atenção, lealdade, companheirismo. Muitos são os momentos de dor, mas poucos
são os que aceitam compartilhar a dor do próximo. É muito fácil querer viver a alegria do
outro, difícil é viver a dor e comer o sal junto. Você viveu todas as minhas alegrias, minhas
dores, angústias, medos, dúvidas, ansiedades, não só como espectador, mas como
participante ativo. Saiba que rezo sempre por você e sua família. E, além disso, também foi
Mestre pra mim. Mestre é aquele que não teme transmitir seu conhecimento e que tem
prazer em fazê-lo, aprendi muito com você, obrigada por tudo.
Ao querido André (André Luis da Silva Fabris), que com tanto carinho me acolheu.
Obrigada por essa amizade incontestável, como o Léo, obrigada por viver minhas alegrias,
mas, principalmente, obrigada por viver minhas dores. Sempre que precisei você estava lá.
Passamos por momentos difíceis e delicados que toda amizade proporciona pela liberdade
6
que temos um com o outro, mas sabemos que o guardaremos para sempre são os
verdadeiros gestos de carinho, atenção, dedicação, companheirismo sem esperar nada em
troca. Saiba que estará sempre em meu coração e em minhas orações. Agradeço também
sua querida mãe, Maria Ivone Fabris, por todo carinho com que sempre me recebeu em sua
casa, pela amizade e por torcer por mim, igualmente agradeço ao Gustavo da Silva Fabris, seu
irmão. Deus abençoe sua família e a conserve sempre unida.
À Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), pela
concessão da Bolsa de Mestrado durante todo o curso. Meus sinceros agradecimentos por
promover o apoio financeiro necessário que viabilizou a realização deste sonho.

7
Agradecimentos
À Faculdade de Odontologia de Araçatuba – UNESP, na pessoa da diretora Ana Maria
Pires Soubhia pela oportunidade de realização do curso de Mestrado e por todo carinho com
que fui recebida por esta instituição.
À Coordenação do Programa de Pós-Graduação em Odontologia, da Faculdade de
Odontologia de Araçatuba, da Universidade Estadual Paulista “Julio de Mesquita Filho” na
figura da Profa. Adja. Maria Jose Hitomi Nagata.
Aos queridos funcionários do Departamento de Cirúrgia e Clinica Integrada (Cleide L.
S. Toquetão, Gilmar M. de Oliveira, Odair Vicente, Renato G. de Oliveira, DonaTina, Paulo R
Gratão e Joilson B. Lellis). Muito obrigado pelo carinho e respeito.
As queridas funcionárias Michele, Fran, Paula, Camila, Patrícia, Hélide que com muito
carinho e respeito nos apoiaram durante todo o curso. Obrigada por toda atenção e
empenho.
Ao querido funcionário Sr. Wilson e seu amigo canino Apolo pelo carinho e pelas
conversas. Que Deus os abençoe.
Aos funcionários do Biotério, em especial aos funcionários Sr. Camilo e Sr. João Batista,
que ofereceram suporte para a obtenção dos animais utilizados neste trabalho.
Aos colegas da pós-graduação em Odontologia (Juliana Zorzi Coléte, Patrícia Bermejo,
Bianca Bravim Bomfim, Carlos Alberto Timóteo, Gabriel Ramalho Ferreira, Lamis Meorim
Nogueira, Marial Del Pilal Rodrigues e Juceléia Maciel, Rodrigo Pereira e Giovanna
Francisconi). Pela nossa excelente convivência, pelo companheirismo e aprendizado.
Aos queridos pacientes pela confiança e pela entrega ao permitir nosso aprendizado
por meio de sua dor. Muito obrigada.

8
Epígrafe
“Preparar o futuro significa fundamentar o presente.”
“O Pequeno Príncipe”, Antoine de Saint-Exupéry
9
Abstract
The proposition of this study was evaluate the osteoconductive capability of the solid form of
PLA/PGA copolymer in an experimental model of maxillary sinus grafting. Twenty male white
New Zealand rabbits, each weighing about 3.0kg, were used and were divided into two
groups, according to the sinus filling material, as follows: autogenous bone chips and
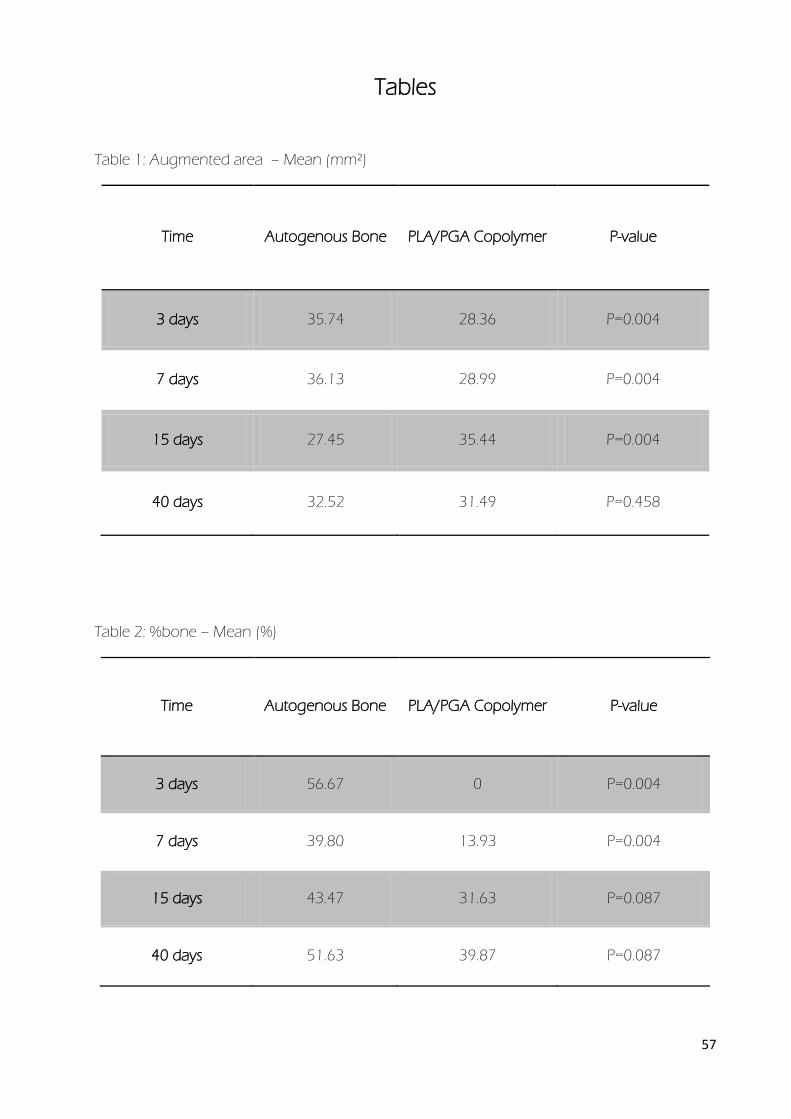
PLA/PGA copolymers. Augmented area differ between the groups after 3, 7 and 15 days
(P=0.004). However, the values became similar on day 40 (P=0.458). After 3 and 7 days the
percentage of bone was statistically significant between autogenous bone and PLA/PGA
copolymer (P=0.004 and P=0.004). After 15 and 40 days the values were comparable in the
two periods (P=0.087 and P=0.087). Immunohistochemistry confirms the results on the
histomorphometric data. In conclusion, PLA/PGA copolymer seems to be suitable as
resorbable material able to induce bone growth in bone defects. This observation suggests
that the material have osteoconductive properties also suitable for application in maxillofacial
surgery.
Key-words: polylactic acid, polyglycolyc acid, autogenous bone, sinus lift, rabbit

10
Resumo
A proposta deste estudo foi avaliar a capacidade osteocondutora da forma sólida do
copolímero de PLA/PGA em um modelo experimental de enxerto em seio maxilar . Vinte
coelhos machos, branco, da raça Nova Zelândia, cada um pesando cerca de 3,0 kg, foram
utilizados e foram divididos em dois grupos de acordo com o material de preenchimento do
seio, como segue: ósseo autógeno particulado e copolímero PLA/PGA . A área aumentada
diferiu entre os grupos após 3, 7 e 15 dias (p = 0,004) . No entanto, os valores tornaram-se
semelhante aos 40 dias (p = 0,458). Depois de 3 e 7 dias, a porcentagem óssea foi
estatisticamente significativa entre osso autógeno e PLA / PGA copolímero (P = 0,004 e P =
0,004). Após 15 e 40 dias os valores foram semelhantes nos dois períodos (P = 0,087 e P =
0,087 ). Imunohistoquímica confirma os resultados sobre os dados histomorfométricos. Em
conclusão, o copolímero de PLA/PGA parece ser adequado como material reabsorvível capaz
de induzir o crescimento do osso em defeitos ósseos. Esta observação sugere que o material
tem propriedades osteocondutoras também apropriado para aplicação em cirurgia maxilo-
facial.
Palavras- chave: ácido polilático, ácido poliglicólico, osso autógeno, elevação do seio, coelho.
11
Listas e Sumário

12
Lista de Figuras
Figure 1: PLA/PGA copolymer 50/50 saturated with calcium phosphate ..................................... 38
Figure 2:. Autogenous bone collection; (a) tibial metaphysic; (b) and (d) autogenous tissue
samples; (c) bone scraper ..................................................................................................................... 38
Figure 3: Surgical procedure steps for sinus lift. (a) Exposure of the nasal dorsum, (b), (c), (d)
and (e) Preparation of the surgical window, (f) PLA/PGA copolymer graft, (g) bone
graft, (h) graft completed. .................................................................................................................... 39
Figure 4: (a) Nose complex and (b) frontal plane ....................................................................................... 40
Figure 5: Captured magnification: Specimen at 15 days after surgery, X1.0, H.E .......................... 41
Figure 6: Histomorphometric analysis : Mensured area, X2.8, H.E. ...................................................... 42
Figure 7: Selected region for histomorphometric analysis: A: imaginary extensions of the pre-
existing cortical bone at the margins of the window; B: center region and C:
membrane region ..................................................................................................................................... 43
Figure 8: Autogenous bone group, 3days ........................................................................................................ 44
Figure 9: Autogenous bone group, 7days ........................................................................................................ 45
Figure 10: Autogenous bone group, 15days .................................................................................................. 46
Figure 11: Autogenous bone group, 40days .................................................................................................. 47
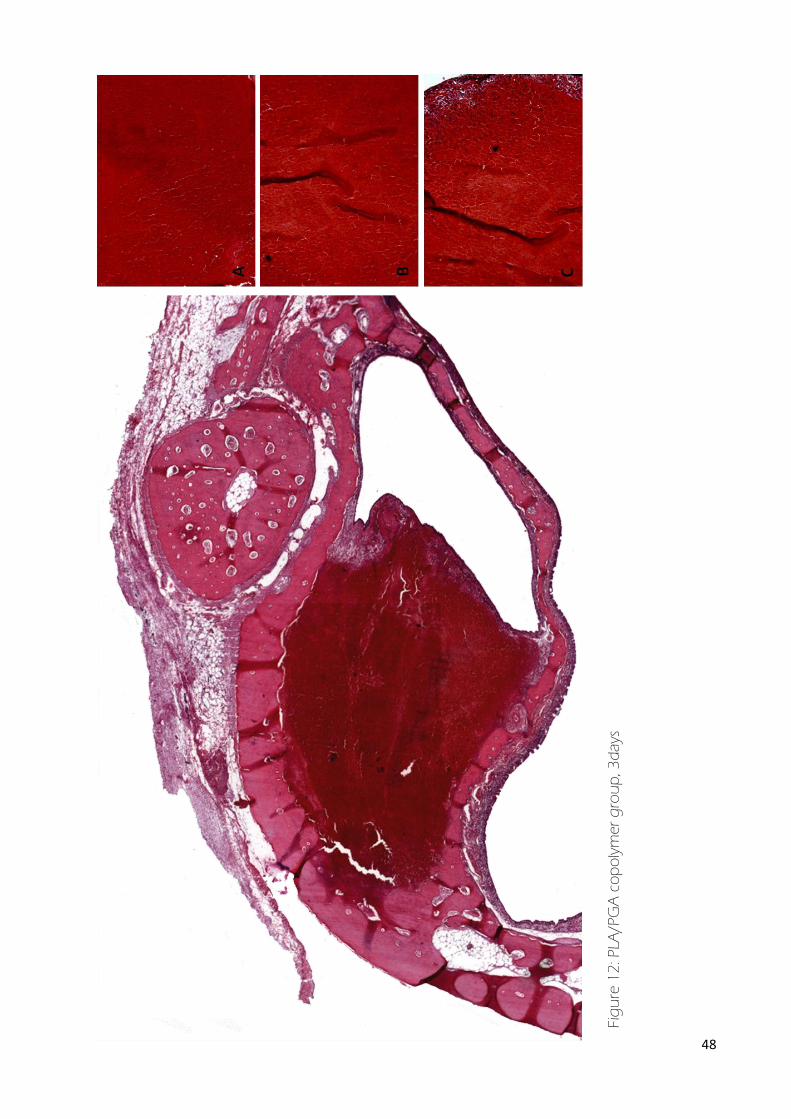
Figure 12: PLA/PGA copolymer group, 3days ................................................................................................ 48
Figure 13: Autogenous bone group, 3days ..................................................................................................... 49
Figure 14: PLA/PGA copolymer group, 15days ............................................................................................. 50
13
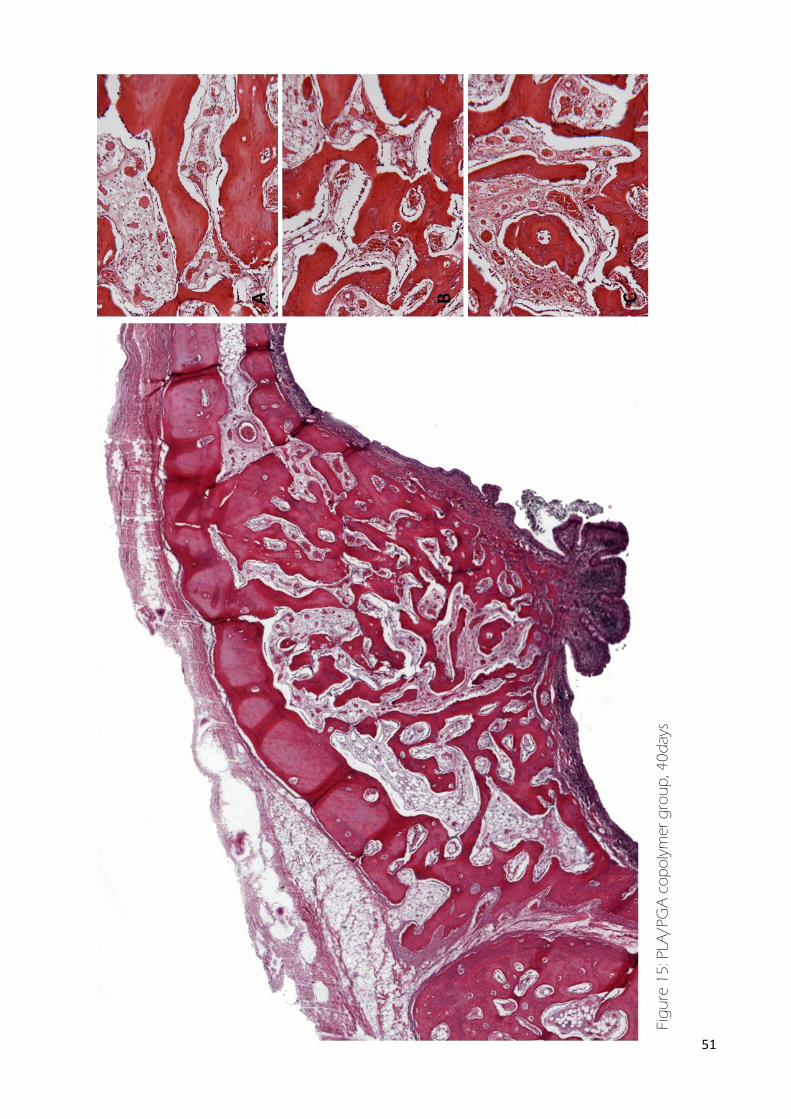
Figure 15: PLA/PGA copolymer group, 40days ............................................................................................. 51
Figure 16: Graphic of augmented area, autogenous bone and PLA/ PGA copolymer groups
................................................................................................................................................................................ 52
Figure 17: Graphic of %bone ................................................................................................................................... 52
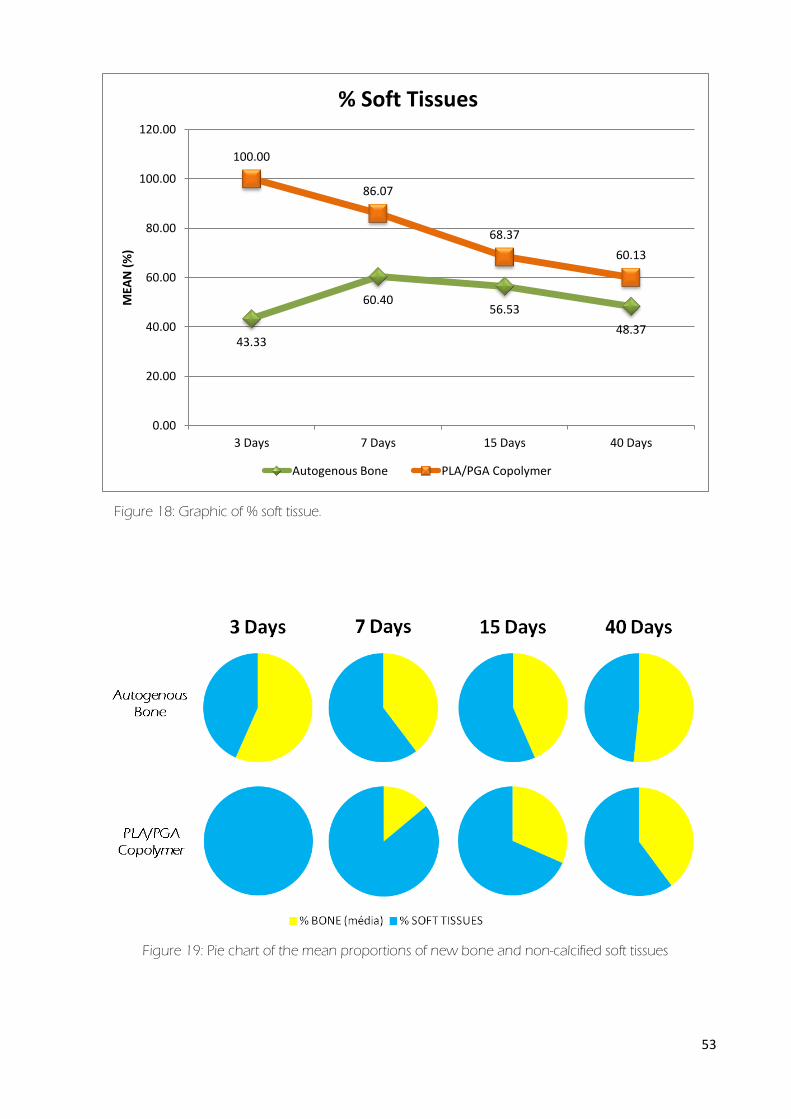
Figure 18: Graphic of % soft tissue ......................................................................................................................... 53
Figure 19: Pie chart of the mean proportions of new bone and non-calcified soft tissues ..... 53
Figure 20: Autogenous bone group; OC immunoreactivity in (a) 3, (b) 7, (c) 15 and (d) 40
days. ................................................................................................................................................................ 54
Figure 21: PLA/PGA copolymer group; OC immunoreactivity in (a) 3, (b) 7, (c) 15 and (d) 40
days ................................................................................................................................................................... 54
Figure 22: Autogenous bone group; TRAP immunoreactivity in (a) 3, (b) 7, (c) 15 and (d) 40
days ................................................................................................................................................................. 55
Figure 23: Figure: PLA/PGA copolymer group; TRAP immunoreactivity in (a) 3, (b) 7, (c) 15
and (d) 40 days........................................................................................................................................... 55
Figure 24: OC and TRAP values at 3, 7, 15 and 40 days in autogenous bone group .............. 56
Figure 25: OC and TRAP values at 3, 7, 15 and 40 days in PLA/PGA copolymer group ......... 56

14
Lista de Tabelas
Table 1: Augmented area – Mean (mm²)............................................................................................................. 57
Table 2: %bone – Mean (%) .......................................................................................................................................... 57
Table 3: % soft tissue – Mean (%) .............................................................................................................................. 58
Lista de Abreviaturas
PLA ........................................................................................................................................... Polylactic acid
PGA ..................................................................................................................................... Polyglycolyc acid
PLA/PGA .................................................................................................................. Poly-Lactide-co-Glycolide
PVP-I ......................................................................................................... Polyvinyl Pyrrolidone Iodine
TRAP ............................................................................................. Tartrate-resistant acid phosphatase
OC .............................................................................................................................................. Osteocalcin
15
Sumário
Introduction .......................................................................................................................................................... 17
Proposition ............................................................................................................................................................ 18
Material and methods ...................................................................................................................................... 19
Copolymer PLA/PGA Production ...................................................................................................... 19
Surgical Procedures .................................................................................................................................. 19
Obtaining Autogenous Bone Graft ........................................................................................ . 20
Sinus Lift ................................................................................................................................................... 20
Histologic Procedures .............................................................................................................................. 21
Histological and Histomorphometric Analysis ............................................................................ 21
Immunohistochemical Analysis .......................................................................................................... 22
Statistical assessment ................................................................................................................................ 22
Results .................................................................................................................................................................. 23
Histologic Findings .................................................................................................................................... 23
Experimental group with autogenous bone graft ........................................................... 23
Experimental group with PLA/PGA copolymer ................................................................. 24
Histomorphometric Analysis ................................................................................................................ 24
Augmented area ............................................................................................................................... 24
% bone, % soft tissues ....................................................................................................................... 25
Immunohistochemical Analysis .......................................................................................................... 25
Discussion .............................................................................................................................................................. 26
References ............................................................................................................................................................. 31
Tabelas e Figuras ...................................................................................................................................................... 37
Anexos .......................................................................................................................................................................... 59

16
“PLA/PGA copolymer as a bone substitute in maxillary sinus
augmentation. Histological, histometric and
immunohistochemistry study in rabbits”

17
Introduction
Loss of teeth promotes severe, irreversible resorption of alveolar bone1, 2
. In the
posterior region of the maxilla, the height extending from the floor of the maxillary sinus to the
alveolar crest decreases. Various procedures for maxillary sinus augmentation have been
developed to increase bone volume and height to promote stability of endosseous implants1,
3, 4.
These procedures require the use of graft materials to maintain the augmented space
and to promote osteogenesis. Early studies advocated the use of autogenous bone to ensure
graft survival and bone formation in the augmented space1, 4
. Blomqvist et al5 reported a
success rate of 82% with implants placed into grafted bone in the maxillary sinus from the iliac
crest; Lundgren et al6 reported a success rate of 80% with such implants. Some authors have
even reported successful short-term sinusal bone augmentation and implant outcomes with
only a blood clot and no grafting material7-11
Moy et al12
and Nishibori et al13
found that the
quantity and quality of bone produced by autogenous bone grafts were superior to those of
bone produced by allografts.
Numerous reports on autogenous grafts at various anatomical sites have been
presented14-17
. Although autogenous bone is still often regarded to be the gold standard in
bone augmentation procedures, morbidity at the donor site as well as reports of significant
levels of resorption, whether intra-oral, extra-oral, block or particulated bone is used,
necessitate the consideration of alternative biomaterials18-21
.
The families of polylactic acid (PLA), polyglycolyc acid (PGA) and their co-polymers
(Poly-Lactide-co-Glycolide, PLA/PGA), both biodegradable, are at the cutting edge of bone
reconstruction procedures. These materials are manufactured in a variety of forms to produce
appliances for use in bone surgery such as tissue barriers22
, fixation devices23, 24
, porous solid
graft25-29
, solid or semi-solid carriers for delivery of growth factor (GF), bone morphogenetic
18
proteins (BMPs) and other bioactive molecules30, 31
. These materials may also serve as
scaffolding to promote specific cell adhesion, differentiation and bone formation26, 29, 31
.
The resorption of PLA and PGA acids occurs through hydrolysis and hydrolytic
mechanisms. Implanted polymers are expected to play their supportive role in the healing
process and then to degrade to matrix products, which are eliminated through the normal
excretory routes and are replaced by the neighboring tissues32, 33
. This polymer is gradually
substituted by new bone over time, but its degradation depends on the formulation,
amorphous/crystalline structure, isomeric characteristics, molecular weight and amount of
material used27, 34
. The exact composition and architecture of the polymeric scaffold becomes
fundamental to promote successful bone regeneration.
Although extensively used in several orthopedic appliances35
, PLA/PGA have been
scarcely applied in oro-maxillo-facial applications. PLA-derived devices were implemented to
prevent alveolar osteitis or dry socket with discordant results by Hooley and Golden36
. PLA
and decalcified freeze-dried bone allografts were clinically studied in the treatment of
periodontal intra-osseous defects by Meadows et al.37
. Results showed a limited amount of
tissue regeneration and the persistence of PLA particles surrounded by soft tissue. A new
PLA/PGA (Fisiograft®
, Ghimas, Italy), manufactured as sponge blocks, gel and powders, was
studied in maxillary sinus floor augmentations29, 38
, as space maker, in alveolar ridge
preservation26
, ridge augmentation with split-crest technique, in the treatment of deep
periodontal intra-osseous defect28
, and in critical bone defects in experimental animals25
with
contrasting results.
Proposition
We therefore histologically, histomorphometrically and immunohistochemically
evaluated the osteoconductive capability of the solid form of PLA/PGA copolymer in an
experimental model of maxillary sinus grafting.

19
Material and methods
Copolymer PLA/PGA Production
PLA/PGA copolymer consisted of a mixture of lactic and glycolic acid 50/50 saturated
with calcium phosphate, extent that make them gain a solid consistency (Figs. 1a and 1b). The
solution pH was controlled by adding the buffer solution. The method used was the
polymeric or Pechini39
method, is a technique that can be applied to the development of
advanced materials precursors. The process is based on the ability of certain organic acids
such as citric, lactic and glycolic have to form chelates. These chelates may be esterified with a
polyalcohol when heated and polymerized at higher temperatures forming a resin.
Surgical Procedures
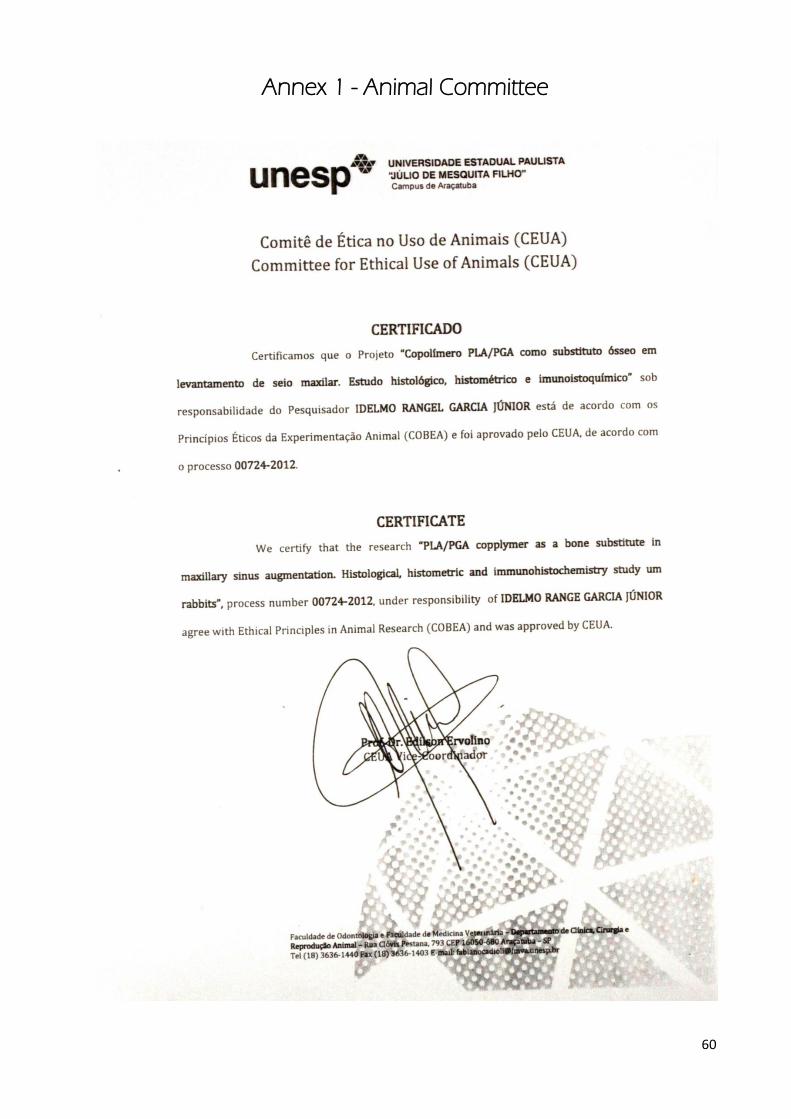
All experimental protocols involving animals were used conformed to procedures
described in the Guiding Principles for the Use of Laboratory Animals and the study approved
by the Animal Committee of Dentistry School of University Estadual Paulista Júlio de Mesquita
Filho, UNESP (00724-2012) (Annex 1).
Twenty male white New Zealand rabbits, each weighing about 3.0kg, were used and
were divided into two groups, according to the sinus filling material, as follows: Group 1:
Control, autogenous bone chips and Group 2: PLA/PGA copolymers particles.
All animals underwent surgeries for bilateral sinus lift procedures. The rabbits were
anesthetized with 1% chloridrate of ketamine (Francotar, Virbac Ltda, São Paulo, Brazil), along
with with a sedative, 2% chloridrate of xylazine (Virbaxyl 2%, Virbac Ltda, São Paulo, Brazil), in
the recommended dose, respectively, 60 mg/kg and 5.0mg/kg intramuscularly, and 0.5ml of
1% lidocaine with epinephrine (1:100000) was injected subcutaneously at the midline of the
nasal dorsum and into the tibial metaphysic.
20
Obtaining Autogenous Bone Graft
Linear incision with approximately 40mm was made in the direction of the long axis in
the tibial metaphysic after previous manual trichotomy and antisepsis preoperative in the right
tibia with friction of gauze soaked in 10% Polyvinyl Pyrrolidone Iodine degermante, with 1%
active iodine (PVP-I 10% Riodeine ®, Rioquímica, São José do Rio Preto) associated with the
topic PVP (10% PVP-I aqueous, with 1% active iodine, Riodeine®, Rioquímica, São José do Rio
Preto). Then, the soft tissue overlying the region was elevated in total thickness, exposing the
bone tissue (Fig. 2a). With the aid of scraper autogenous bone tissue samples were collected
for subsequent filling of the maxillary sinus (Fig. 2b, 2c and 2d). Completed sample collection,
the surgical flap was repositioned and sutured in layers.
Sinus Lift
Surgical interventions were performed under strict sterile conditions. The surgical area
was shaved and disinfected with iodine. The sinus lift surgical procedure was performed
according to Asai, Shimizu e Ooya (2002). A midline incision extending for about 50mm was
made, and the skin and periosteum were elevated sufficiently to expose the nasal bone and
nasoincisal suture line (Fig. 3a). A trephine bur with a 5.0mm internal diameter was used to
delineate the diameter of the bone window for the maxillary sinus access (Fig. 3b and 3c). A
circular window was opened in the nasal bone with the use of a round diamond bur nº 1014
under copious irrigation with saline solution (Fig. 3d). The window was located approximately
20mm anterior to the nasofrontal suture line, 10mm lateral to the midline (Fig. 3e). Care was
taken during this procedure to avoid damaging the sinus mucosa. The sinus membrane was
carefully elevated to allow the insertion and condensation of the graft materials. No
membrane was used to cover the bone window. In the experimental groups, the
compartment was filled with PLA/PGA copolymer (Fig. 3f) and autogenous bone graft (Fig.
3g and h). A suture was placed between the periosteum and skin.

21
Histologic Procedures
After 3, 7, 15 and 40 days of the surgery, five animals were sacrificed with an overdose
of anesthetics. After decapitation and dissection, the entire nose complex, including the nose
and sinus cavities (Fig. 4a), was fixed in buffered 10% formaldehyde (Merck, Darmstadt,
Germany) for 48 h and washed in tap water for 24 h, and immersed in buffered 4% EDTA for
demineralization. Specimens from the normal and experimental groups were slowly
decalcified and were cut in a frontal plane (Fig. 4b). The specimens were then dehydrated,
embedded in paraffin, and sliced into sections about 6µm thick. The sections were stained
with hematoxylin and eosin (Merck & Co., Inc., NJ, USA) for the light microscopic examination.
Some sections were reserved for immunohistochemistry reactions.
Histological and Histomorphometric Analysis
Each image of the calcified specimens at the rostrocaudal midpoint of the antral wall
was digitally captured at magnification X1.0, X2.8 and X160 and sent to the Image J Program
– Version 1.47 (National Institutes of Health (NIH), Bethesda, Maryland, USA). The composition
of the total augmented sinus was identified (in mm²). The proportions (in %) of each
composite (new bone - NB and soft tissue - ST) were obtained. To evaluate the distribution of
regenerated bone in the grafted sinus area as a secondary outcome variable, the above-
mentioned parameters were measured in specific standardized areas. The areas were
randomly selected and photomicrographs were taken in original magnification X160. The
window region was selected within the grafted area interfacing the imaginary extensions of
the pre-existing cortical bone at the margins of the window, the center region was at the
middle of the whole augmented sinus and membrane region. The membrane region was
chosen from just above the Schneiderian membrane (Fig. 5, 6 and 7):
22
Augmented area: defined as the raw surface of the secluded space underneath the
sinus membrane;
% bone, % soft tissues: percentage of the measured augmented area, defined as the
raw surface of the secluded space underneath the sinus membrane.
Immunohistochemical Analysis
Immunohistochemical analysis were performed at 3, 7, 15, and 40 days (n = 5). The
following primary antibodies used for immunohistochemical processing were from Santa Cruz
(Biotechnology, CA): anti-osteocalcin (OC) and tartrate-resistant acid phosphatase (TRAP). As a
secondary antibody, a biotinylated donkey anti–goat antibody (Jackson Immunoresearch
Laboratories, West Grove, PA) was used. The signal of the immunohistochemistry reaction
with an avidin biotin system (Kit ABC-Vectastain Elite ABC–peroxidase standard, reagent A and
B only–PK6100; Vector Laboratories, Burlingame, CA), and diaminobenzidine (Sigma, St. Louis,
MO) was used as chromogen.
Immunohistochemical reactions were controlled to evaluate the specificity of the labels.
Hematoxylin and eosin staining was performed and used as a reference of the
cytoarchitecture of the tissue. Immunohistochemical analysis for consist of a qualitative
examination was stratified by a range of values ranging from 0 to 3 (0 = no protein expression,
1 = protein with little expression, 2 = intermediate protein expression, high protein expression
3 =).
Statistical assessment
All morphometric data were assessed using the Mann-Whitney. The level of statistical
significance was set at 5%.

23
Results
Histologic Findings
Experimental group with autogenous bone graft
After 3 days, the augmented dome-like space formed by the elevated sinus mucosa
was found to be filled with acellular autogenous bone particles and blood clot, osteocytes in
the lacunae disappeared in the grafted bone (Fig. 8).
After 7 days, peripheral newly formed bone trabeculae had irregular surfaces with
numerous osteoblasts and osteoclasts were seen in areas near the sinual membrane and
bone tissue of the nasal complex. Therefore early steps of centripetal new bone formation
were observed progressing from the anterior part of the sinus and the bone walls. Cell
colonization was found everywhere in the cavity, and remnants of clot were sometimes
visible. Remnant acellular autogenous bone particles were seen in the central region of the
space with connective tissue and blood vessels. There was no evidence of acute or chronic
inflammation (Fig. 9).
After 15 days, the newly formed woven bone adjacent to the membrane and bone
tissue of the nasal complex showed osteoclastic resorption and the central region were seen
newly formed woven bone and soft tissue. There were many osteocytes in the newly formed
bone. Woven bone with many osteoblasts was observed around the grafted bone, especially
under the elevated antral membrane (Fig. 10).
After 40 days, the augmented space revealed mature cortical and trabecular bone
with intertrabecular vascularized adipose tissue. The bone chips were completely remodeled
and their remnants were not visible (Fig. 11).
24
Experimental group with PLA/PGA copolymer
After 3 days, the augmented dome-like space formed by the elevated sinus mucosa
was found to be filled with blood clot. Copolymer particles were not observed. Mesenchymal
cell proliferation was only visible at the periphery of the created space, while the blood clot
was still non-invaded by mesenchymal cells in the center of the cavity. No inflammatory cell
infiltration was present (Fig. 12).
After 7 the augmented dome-like space was found to be filled connective tissue with
fibroblasts and blood vessels. Remnant blood clots were seen in the central region of the
space. Peripheral newly formed woven bone was seen. Therefore early steps of centripetal
new bone formation were observed progressing from the anterior part of the sinus and the
bone walls (Fig. 13).
After 15 days, peripheral newly formed bone was seen in areas near the sinual
membrane and bone tissue of the nasal complex. Connective tissue was seen in the central
region of the space with fibroblasts and blood vessels (Fig. 14).
After 40 days, the augmented space revealed mature cortical and trabecular bone
with intertrabecular vascularized adipose tissue. The bone trabeculae showed the minimal
osteoclastic resorption. Some areas near the sinual membrane and bone tissue of the nasal
complex revealed mature cortical and trabecular bone with intertrabecular vascularized
adipose tissue (Fig. 15).
Histomorphometric Analysis
Augmented area
Augmented area differ between the groups after 3, 7 and 15 days(P=0.004). However,
the values became similar on day 40 (P=0.458) (Fig. 16). The comparison of values of 3 and 40
days autogenous bone group and PLA/PGA copolymer group and were also statistically
25
significant (P=0.004 e P=0.004) .Values in mm2 of the augmented area are presented in Table
1.
% bone, % soft tissues
After 3 days, in the autogenous bone group, bone inside the created space under the
membrane constituted 56.67% of the measured augmented area, while in the PLA/PGA
copolymer group, the amount of bone constituted 0%. The percentage of bone was
significantly higher with autogenous bone than with PLA/PGA copolymer (P=0.004).
After 7 days, in the autogenous bone group, bone ingrowths constituted 39.80% of
the measured augmented area, while in the PLA/PGA copolymer group, the amount of bone
ingrowth failed to reach 13.93%. The percentage of bone was significantly higher with
autogenous bone than with PLA/PGA copolymer (P=0.004).
After 15 days, the area occupied by newly formed bone reached, respectively, 43.47%
and 31.63% (P=0.087) for the autogenous bone and the PLA/PGA copolymer groups. The
implanted bone chips could be observed in the central area.
After 40 days, in the autogenous bone and PLA/PGA copolymer groups, the newly
formed bone area increased to 51.63% and 39.87%, respectively. The values were
comparable in the two groups (P=0.087). Detailed results are presented in Table 2 and shows
the correlation between volume changes over time and % bone and % soft tissues within
augmented tissues (Figs 17, 18 and 19) (Tables 2 and 3).
Immunohistochemical Analysis
OC immunoreactivity could be seen in all augmented area for the autogenous bone
group in the early periods of this study, 3 days (intermediate protein expression), with
increased at 7 days (high protein expression) and remaining high on 15 and 40 days (high
protein expression) after surgery (Fig. 20). Similarly to autogenous bone group, in the

26
PLA/PGA copolymer group, OC immunoexpressivity was seen intermediate at 3 days, with
increased at 7 days (high protein expression), remaining high on 15 days (high protein
expression). However, declined at 40 days (intermediate protein expression) after surgery (Fig.
21).
In TRAP immunohistochemistry could be seen in autogenous bone group high protein
expression in the early periods, 3 days. However, this declined at 7 days (intermediate protein
expression). At 15 days after surgery increased expression of TRAP (high protein expression)
with decline at 40 days (intermediate protein expression) (Fig. 22). Differently to the
autogenous bone group, in the PLA/PGA copolymer group TRAP immunoexpressivity had
gradual increased: 3 days protein with little expression, 7 days with intermediate protein
expression and 15 days with high protein expression. However, declined at 40 days
(intermediate protein expression) (Figs. 23, 24 and 25).
Discussion
In posterior maxilla restoration using osseointegrated implants, sinus floor elevation is
often also undertaken by an autogenous bone graft. Autogenous bone graft is considered
the ideal graft to satisfy the following criteria: (1) low risk of infection, (2) low antigenicity, (3)
the ability to produce bone by osteoinduction and osteoconduction, and (4) easy
correction40
. However, the preferred autogenous material causes specific problems such as its
limited supply, attendant donor-site morbidity, and the occasional unsuitability for the
proposed reconstruction because of poor tissue quality, or the extremely difficulty in shaping
the graft18, 19
Although bone grafting represents the standard reconstruction procedure, resorbable
polymers have become very useful auxiliary materials to enhance functional and structural
clinical outcome23, 24, 28, 41
. Among these polymers32
, polylactides are deemed to be very
promising resorbable materials. Polylactide copolymers with different mechanical properties

27
and different degradation rates have been used in numerous studies to enhance the healing
of bone defects24, 32, 33
. Some authors have seen in the degradability properties of PLA/PGA
copolymer a chance for tissue neogenesis 24-26
. Our results seems to confirm these
opportunities.
This rabbit study investigated the area stability of sub-sinusal bone regeneration when
autogenous bone chips or PLA/PGA copolymer 50/50 were used as space fillers. Early bone
formation and the continuing behavior of the regenerated bone with these different types of
filling material were also assessed. Rabbits have similar maxillary sinus ventilation to humans
and a well-defined ostium opening to their nasal cavities. The rabbit sinus lift model is
therefore appropriate and well documented for evaluating bone regeneration physiology in
sub-sinusal bone regeneration42, 43
.
Adequate bone healing was observed with the two space fillers used in the present
study and no signs of inflammation could be detected. Similar findings have already been
reported by several authors29, 42, 43
; unfortunately, the early steps of bone regeneration were
poorly studied in these papers.
In this study, in PLA/PGA copolymer cell proliferation was detected after 7 days only
along the bone wall and under the sinusal membrane, while the central part was still
occupied by a dense cluster of red blood cells, in contrast with the autogenous bone group
where the augmented space was completely invaded by mesenchymal cells. A gradient of
maturity of the newly formed tissue from the native bony walls to the center of the cavity
illustrated the centripetal nature of the regenerative process.
At 15 days, in the PLA/PGA copolymer group, non-mineralized fibrous tissue still
occupied the central area. At 40 days, in the PLA/PGA copolymer group, woven bone was
found everywhere in the remaining cavity. Therefore, PLA/PGA copolymer implanted into
sub-sinusal cavities allowed bone formation. Rimondini et al25
reported that the
histomorphometric data demonstrated that the experimental material is able to promote bone
healing even in a large bone defect such as in rabbit femoral condyles. The bone maturation
28
improved from 30 to 90 days. The data concerning the development of the forming bone
showed that during the 30 to 90 days the material allowed a bone remodeling from reticular
toward a trabecular structure.
Fisiograft®
is a synthetic resorbable sponge formed by 50–50 lactide–glycolide
polymer. This copolymer has shown the fastest degradation rate of the d-l lactide/glycolide
biomaterials, with the polymer degrading in about 50–60 days41
. In the previous study37
PLA
granules were still evident at 6-month surgical re-entry.
In the autogenous bone group, the early healing process was characterized by a
particularly high cellular density along the bone chips, even at a distance from the bony walls.
This picture strongly suggests an osteogenic potential provided by autogenous bone chips. At
15 days, the anatomy of the dense woven bone seemed to be influenced by the initial rolled
shape of the bone chips, now remodeled. The remodeling process continued from 15 days to
40 days yielding, in the long term, rarefied mature bone architecture. According to Schlegel et
al.44
, this remodeling process was also observed in sinus lifts performed in humans with
particulated autogenous bone.
New bone formation was already observed at 2 weeks after grafting. It is of interest
that new bone formation was observed in all parts under the elevated antral membrane,
around the grafted bone, and at the superior part of the original sinus floor. The result
indicates that new bone formation may depend not only on
osteoconduction from the recipient site but also on osteoinduction by bone morphogenetic
protein in the grafted bone and osteogenesis by the bone cells that were grafted with the
bone.
Albrektsson45
reported that early revascularization meant early bone remodeling of a
graft in the rabbit tibia; in the present study, blood vessels were already seen in the grafted
bone at 7 days. It is suggested that early revascularization also assisted in the new bone
formation for the maxillary sinus in the present study.

29
Much newly formed bone was noted under the elevated membrane at 40 days after
grafting. Moreover, continuous cortical bone was observed under this membrane. These
results indicate the difference in bone formation between the continuous bone located under
the elevated membrane and continuous bone located elsewhere. In the present study, the
medullary cavity was filled with many fat cells.
In our study, the mean bone fractions in the grafted area were 56.67%, 39.80%,
43.47% and 51.63%, respectively, at 3, 7, 15, and 40 days after grafting. The bone fraction in
the bone biopsy cores was reported in a few studies; Moy et al46
, for example, indicated that
the composition of bone was 59.4% from chin bone graft, and Lundgren et al47
reported the
mean bone fractions in chin bone grafted areas to be 40% and 48%, respectively, at 6 and 12
months after bone grafting.
It is speculated that the period from 2 weeks to 4 weeks in the present study
corresponds to the period from 6 months to 12 months in human beings48
. Previous
investigations have shown that most osteogenic remodeling of the autogenous bone graft in
a rabbit model will occur within the first 6 to 8 weeks postsurgery45, 48-50
. In cortical bone
healing, full graft vascularization was complete by day 30, with the osteogenic phase ending
by day 3545
. Similar results were found by Roberts et al51
, who determined that the resorption
and reversal phase is approximately 1 week in rabbits; while the duration of the bone
formation phase was about 5 weeks.
Immunohistochemistry confirms the results on the histomorphometric data. During the
period of increase of regeneration area, between 3 and 7 days, the OC values also showed an
increase in both experimental groups. Important to note that the lower expression group in
the copolymer shows an early stage of the process when compared to autogenous bone
group. In both groups, the period 7-15 days it is possible to see a tendency to equilibrium in
the processes of bone formation and remodeling, we see a tendency to balance the values of
OC and TRAP. Increased OC shows the mineralization phase in which it is the bone tissue
after 40 days in the autogenous bone group, since the values of TRAP are consistent the

30
period of remodeling of bone trabeculae, characteristic of this period. Unlike the group
copolymer in the same period seems to still keep the balance-training resorption.
The present study showed that the long-term outcome of augmentation of the sinus
was not the maturation of newly formed bone, but conversely atrophy of bone. Indeed, an
increase in adipose tissue in marrow is observed in all conditions that lead to loss of bone,
such as osteoporosis, age-related osteopenia, or immobilisation52
. This apparent reciprocal
relation between reduced bone density and increased fat can be explained by an imbalance
in the production of bone-forming and fat-forming cells53
.
But an excess of adipose tissue in marrow is considered to put at risk the long-term
ability to maintain the mechanical strength of the skeleton54
. Mechanical stress is an essential
factor for the corticalisation of bone55
. Ideal bone grafts should eventually be absorbed and
encourage formation of new bone, which replenishes lost bone permanently.
In conclusion, PLA/PGA copolymer seems to be suitable as resorbable material able to
induce bone growth in bone defects. This observation suggests that the material have
osteoconductive properties also suitable for application in maxillofacial surgery.

31
References
[1] Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and
bone. J Oral Surg 1980 Aug;38(8):613-6.
[2] Keller EE, Van Roekel NB, Desjardins RP, Tolman DE. Prosthetic-surgical reconstruction
of the severely resorbed maxilla with iliac bone grafting and tissue-integrated prostheses. Int J
Oral Maxillofac Implants 1987 Summer;2(3):155-65.
[3] Tatum H, Jr. Maxillary and sinus implant reconstructions. Dent Clin North Am 1986
Apr;30(2):207-29.
[4] Wood RM, Moore DL. Grafting of the maxillary sinus with intraorally harvested
autogenous bone prior to implant placement. Int J Oral Maxillofac Implants 1988 Fall;3(3):209-
14.
[5] Blomqvist JE, Alberius P, Isaksson S. Retrospective analysis of one-stage maxillary sinus
augmentation with endosseous implants. Int J Oral Maxillofac Implants 1996 Jul-
Aug;11(4):512-21.
[6] Lundgren S, Nystrom E, Nilson H, Gunne J, Lindhagen O. Bone grafting to the
maxillary sinuses, nasal floor and anterior maxilla in the atrophic edentulous maxilla. A two-
stage technique. Int J Oral Maxillofac Surg 1997 Dec;26(6):428-34.
[7] Nedir R, Bischof M, Vazquez L, Szmukler-Moncler S, Bernard JP. Osteotome sinus floor
elevation without grafting material: a 1-year prospective pilot study with ITI implants. Clin Oral
Implants Res 2006 Dec;17(6):679-86.
[8] Nedir R, Bischof M, Vazquez L, Nurdin N, Szmukler-Moncler S, Bernard JP. Osteotome
sinus floor elevation technique without grafting material: 3-year results of a prospective pilot
study. Clin Oral Implants Res 2009 Jul;20(7):701-7.
[9] Gabbert O, Koob A, Schmitter M, Rammelsberg P. Implants placed in combination with
an internal sinus lift without graft material: an analysis of short-term failure. J Clin Periodontol
2009 Feb;36(2):177-83.
[10] Lundgren S, Andersson S, Gualini F, Sennerby L. Bone reformation with sinus
membrane elevation: a new surgical technique for maxillary sinus floor augmentation. Clin
Implant Dent Relat Res 2004;6(3):165-73.
32
[11] Palma VC, Magro-Filho O, de Oliveria JA, Lundgren S, Salata LA, Sennerby L. Bone
reformation and implant integration following maxillary sinus membrane elevation: an
experimental study in primates. Clin Implant Dent Relat Res 2006;8(1):11-24.
[12] Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most
successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants
2007;22 Suppl:49-70.
[13] Nishibori M, Betts NJ, Salama H, Listgarten MA. Short-term healing of autogenous and
allogeneic bone grafts after sinus augmentation: a report of 2 cases. J Periodontol 1994
Oct;65(10):958-66.
[14] Lew D, Marino AA, Startzell JM, Keller JC. A comparative study of osseointegration of
titanium implants in corticocancellous block and corticocancellous chip grafts in canine ilium. J
Oral Maxillofac Surg 1994 Sep;52(9):952-8; discussion 9.
[15] Chen NT, Glowacki J, Bucky LP, Hong HZ, Kim WK, Yaremchuk MJ. The roles of
revascularization and resorption on endurance of craniofacial onlay bone grafts in the rabbit.
Plast Reconstr Surg 1994 Apr;93(4):714-22; discussion 23-4.
[16] Nathanson A. The early ingrowth of an autogenous bone inlay into an artificial defect
in the rabbit mandibula. Scand J Plast Reconstr Surg 1977;11(2):97-108.
[17] Alberius P, Gordh M, Lindberg L, Johnell O. Onlay bone graft behaviour after marrow
exposure of the recipient rat skull bone. Scand J Plast Reconstr Surg Hand Surg 1996
Dec;30(4):257-66.
[18] Araujo MG, Sonohara M, Hayacibara R, Cardaropoli G, Lindhe J. Lateral ridge
augmentation by the use of grafts comprised of autologous bone or a biomaterial. An
experiment in the dog. J Clin Periodontol 2002 Dec;29(12):1122-31.
[19] Cordaro L, Torsello F, Accorsi Ribeiro C, Liberatore M, Mirisola di Torresanto V. Inlay-
onlay grafting for three-dimensional reconstruction of the posterior atrophic maxilla with
mandibular bone. Int J Oral Maxillofac Surg 2010 Apr;39(4):350-7.
[20] Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Piombino P, Guidetti F. Volume
changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae
and mandibles. Int J Oral Maxillofac Surg 2009 Oct;38(10):1059-65.

33
[21] Zijderveld SA, Schulten EA, Aartman IH, ten Bruggenkate CM. Long-term changes in
graft height after maxillary sinus floor elevation with different grafting materials: radiographic
evaluation with a minimum follow-up of 4.5 years. Clin Oral Implants Res 2009 Jul;20(7):691-
700.
[22] Hammerle CH, Lang NP. Single stage surgery combining transmucosal implant
placement with guided bone regeneration and bioresorbable materials. Clin Oral Implants Res
2001 Feb;12(1):9-18.
[23] Peltoniemi H, Ashammakhi N, Kontio R, Waris T, Salo A, Lindqvist C, et al. The use of
bioabsorbable osteofixation devices in craniomaxillofacial surgery. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2002 Jul;94(1):5-14.
[24] Leiggener CS, Curtis R, Muller AA, Pfluger D, Gogolewski S, Rahn BA. Influence of
copolymer composition of polylactide implants on cranial bone regeneration. Biomaterials
2006 Jan;27(2):202-7.
[25] Rimondini L, Nicoli-Aldini N, Fini M, Guzzardella G, Tschon M, Giardino R. In vivo
experimental study on bone regeneration in critical bone defects using an injectable
biodegradable PLA/PGA copolymer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005
Feb;99(2):148-54.
[26] Serino G, Biancu S, Iezzi G, Piattelli A. Ridge preservation following tooth extraction
using a polylactide and polyglycolide sponge as space filler: a clinical and histological study in
humans. Clin Oral Implants Res 2003 Oct;14(5):651-8.
[27] Martin C, Winet H, Bao JY. Acidity near eroding polylactide-polyglycolide in vitro and in
vivo in rabbit tibial bone chambers. Biomaterials 1996 Dec;17(24):2373-80.
[28] Minenna L, Herrero F, Sanz M, Trombelli L. Adjunctive effect of a
polylactide/polyglycolide copolymer in the treatment of deep periodontal intra-osseous
defects: a randomized clinical trial. J Clin Periodontol 2005 May;32(5):456-61.
[29] Zaffe D, Leghissa GC, Pradelli J, Botticelli AR. Histological study on sinus lift grafting by
Fisiograft and Bio-Oss. J Mater Sci Mater Med 2005 Sep;16(9):789-93.
[30] El-Amin SF, Lu HH, Khan Y, Burems J, Mitchell J, Tuan RS, et al. Extracellular matrix
production by human osteoblasts cultured on biodegradable polymers applicable for tissue
engineering. Biomaterials 2003 Mar;24(7):1213-21.
34
[31] Saito N, Okada T, Horiuchi H, Ota H, Takahashi J, Murakami N, et al. Local bone
formation by injection of recombinant human bone morphogenetic protein-2 contained in
polymer carriers. Bone 2003 Apr;32(4):381-6.
[32] Cutright DE, Perez B, Beasley JD, 3rd, Larson WJ, Posey WR. Degradation rates of
polymers and copolymers of polylactic and polyglycolic acids. Oral Surg Oral Med Oral Pathol
1974 Jan;37(1):142-52.
[33] Visscher GE, Robison RL, Maulding HV, Fong JW, Pearson JE, Argentieri GJ.
Biodegradation of and tissue reaction to 50:50 poly(DL-lactide-co-glycolide) microcapsules. J
Biomed Mater Res 1985 Mar;19(3):349-65.
[34] Lu HH, El-Amin SF, Scott KD, Laurencin CT. Three-dimensional, bioactive,
biodegradable, polymer-bioactive glass composite scaffolds with improved mechanical
properties support collagen synthesis and mineralization of human osteoblast-like cells in vitro.
J Biomed Mater Res A 2003 Mar 1;64(3):465-74.
[35] Athanasiou KA, Agrawal CM, Barber FA, Burkhart SS. Orthopaedic applications for PLA-
PGA biodegradable polymers. Arthroscopy 1998 Oct;14(7):726-37.
[36] Hooley JR, Golden DP. The effect of polylactic acid granules on the incidence of
alveolar osteitis after mandibular third molar surgery. A prospective randomized study. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 1995 Sep;80(3):279-83.
[37] Meadows CL, Gher ME, Quintero G, Lafferty TA. A comparison of polylactic acid
granules and decalcified freeze-dried bone allograft in human periodontal osseous defects. J
Periodontol 1993 Feb;64(2):103-9.
[38] Scarano A, Degidi M, Iezzi G, Pecora G, Piattelli M, Orsini G, et al. Maxillary sinus
augmentation with different biomaterials: a comparative histologic and histomorphometric
study in man. Implant Dent 2006 Jun;15(2):197-207.
[39] Hussain A, Jadhav AP, Baek YK, Choi HJ, Lee J, Kang YS. One pot synthesis of exchange
coupled Nd2Fe14B/alpha-Fe by pechini type sol-gel method. J Nanosci Nanotechnol 2013
Nov;13(11):7717-22.
[40] Block MS, Kent JN. Sinus augmentation for dental implants: the use of autogenous
bone. J Oral Maxillofac Surg 1997 Nov;55(11):1281-6.

35
[41] Eppley BL, Reilly M. Degradation characteristics of PLLA-PGA bone fixation devices. J
Craniofac Surg 1997 Mar;8(2):116-20.
[42] Asai S, Shimizu Y, Ooya K. Maxillary sinus augmentation model in rabbits: effect of
occluded nasal ostium on new bone formation. Clin Oral Implants Res 2002 Aug;13(4):405-9.
[43] Sun XJ, Zhang ZY, Wang SY, Gittens SA, Jiang XQ, Chou LL. Maxillary sinus floor
elevation using a tissue-engineered bone complex with OsteoBone and bMSCs in rabbits. Clin
Oral Implants Res 2008 Aug;19(8):804-13.
[44] Schlegel KA, Schultze-Mosgau S, Wiltfang J, Neukam FW, Rupprecht S, Thorwarth M.
Changes of mineralization of free autogenous bone grafts used for sinus floor elevation. Clin
Oral Implants Res 2006 Dec;17(6):673-8.
[45] Albrektsson T. Repair of bone grafts. A vital microscopic and histological investigation in
the rabbit. Scand J Plast Reconstr Surg 1980;14(1):1-12.
[46] Moy PK, Lundgren S, Holmes RE. Maxillary sinus augmentation: histomorphometric
analysis of graft materials for maxillary sinus floor augmentation. J Oral Maxillofac Surg 1993
Aug;51(8):857-62.
[47] Lundgren S, Moy P, Johansson C, Nilsson H. Augmentation of the maxillary sinus floor
with particulated mandible: a histologic and histomorphometric study. Int J Oral Maxillofac
Implants 1996 Nov-Dec;11(6):760-6.
[48] Watanabe K, Niimi A, Ueda M. Autogenous bone grafts in the rabbit maxillary sinus.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999 Jul;88(1):26-32.
[49] Albrektsson T, Linder L. Intravital, long-term follow-up of autologous experimental bone
grafts. Arch Orthop Trauma Surg 1981;98(3):189-93.
[50] Bogoch E, Gschwend N, Rahn B, Moran E, Perren S. Healing of cancellous bone
osteotomy in rabbits--Part I: Regulation of bone volume and the regional acceleratory
phenomenon in normal bone. J Orthop Res 1993 Mar;11(2):285-91.
[51] Roberts WE, Smith RK, Zilberman Y, Mozsary PG, Smith RS. Osseous adaptation to
continuous loading of rigid endosseous implants. Am J Orthod 1984 Aug;86(2):95-111.
[52] Verma S, Rajaratnam JH, Denton J, Hoyland JA, Byers RJ. Adipocytic proportion of
bone marrow is inversely related to bone formation in osteoporosis. J Clin Pathol 2002
Sep;55(9):693-8.

36
[53] Atmani H, Chappard D, Basle MF. Proliferation and differentiation of osteoblasts and
adipocytes in rat bone marrow stromal cell cultures: effects of dexamethasone and calcitriol. J
Cell Biochem 2003 May 15;89(2):364-72.
[54] Nuttall ME, Gimble JM. Is there a therapeutic opportunity to either prevent or treat
osteopenic disorders by inhibiting marrow adipogenesis? Bone 2000 Aug;27(2):177-84.
[55] Frost HM. Perspectives: bone's mechanical usage windows. Bone Miner 1992
Dec;19(3):257-71.
37
Tabelas e Figuras

38
Figures
Figure 1: PLA/PGA copolymer 50/50 saturated with calcium phosphate.
Figure 2: Autogenous bone collection; (a) tibial metaphysic; (b) and (d) autogenous tissue
samples; (c) bone scraper.

39
Figure 3: Surgical procedure steps for sinus lift. (a) Exposure of the nasal dorsum, (b), (c), (d)
and (e) Preparation of the surgical window, (f) PLA/PGA copolymer graft, (g) bone graft, (h)
graft completed.

40
Figure 4: (a) Nose complex and (b) frontal plane.

41
Fig
ure
5: C
ap
ture
d m
ag
nifi
catio
n:
Speci
men
at
15
days
aft
er
surg
ery
, X1
.0, H
.E.

42
Figure 6: Histomorphometric analysis : Mensured area, X2.8, H.E.

43
Fig
ure
7: S
ele
cted
reg
ion
fo
r h
isto
mo
rph
om
etr
ic a
naly
sis:
A:
imag
inary
ext
en
sio
ns
of th
e p
re-e
xist
ing
co
rtic
al b
on
e
at
the m
arg
ins
of th
e w
ind
ow
; B: c
en
ter
reg
ion
an
d C
: mem
bra
ne
reg
ion
.

44
Fig
ure
8: A
uto
ge
no
us
bo
ne g
rou
p, 3
days

45
Fig
ure
9: A
uto
ge
no
us
bo
ne g
rou
p, 7
days

46
Fig
ure
10
: Au
tog
en
ou
s b
on
e g
rou
p, 1
5d
ays

47
Fig
ure
11
: Au
tog
en
ou
s b
on
e g
rou
p, 4
0d
ays
48
Fig
ure
12
: PLA
/PG
A c
op
oly
mer
gro
up
, 3d
ays

49
Fig
ure
13
: PLA
/PG
A c
op
oly
mer
gro
up
, 7d
ays

50
Fig
ure
14
: PLA
/PG
A c
op
oly
mer
gro
up
, 15
days
51
Fig
ure
15
: PLA
/PG
A c
op
oly
mer
gro
up
, 40
days

52
35.74 36.13
27.45
32.52
28.36 28.99
35.44
31.49
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
3 Days 7 Days 15 Days 40 Days
MEA
N (
mm
²)
AUGMENTED AREA
Autogenous Bone PLA/PGA Copolymer
56.67
39.80
43.47
51.63
0
13.93
31.63
39.87
0.00
10.00
20.00
30.00
40.00
50.00
60.00
3 Days 7 Days 15 Days 40 Days
MEA
N (
%)
% Bone
Autogenous Bone PLA/PGA Copolymer
Figure 16: Graphic of augmented area, autogenous bone and PLA/ PGA copolymer
groups.
Figure 17: Graphic of %bone.
53
Figure 19: Pie chart of the mean proportions of new bone and non-calcified soft tissues
43.33
60.40 56.53
48.37
100.00
86.07
68.37
60.13
0.00
20.00
40.00
60.00
80.00
100.00
120.00
3 Days 7 Days 15 Days 40 Days
MEA
N (
%)
% Soft Tissues
Autogenous Bone PLA/PGA Copolymer
Figure 18: Graphic of % soft tissue.

54
Figure 20: Autogenous bone group; OC immunoreactivity in (a) 3, (b) 7, (c) 15 and (d) 40 days.
Figure 21: PLA/PGA copolymer group; OC immunoreactivity in (a) 3, (b) 7, (c) 15 and (d) 40 days.

55
Figure 22: Autogenous bone group; TRAP immunoreactivity in (a) 3, (b) 7, (c) 15 and (d) 40 days.
Figure 23: Figure: PLA/PGA copolymer group; TRAP immunoreactivity in (a) 3, (b) 7, (c) 15 and (d)
40 days.

56
.
Figure 24: OC and TRAP values at 3, 7, 15 and 40 days in autogenous bone group
Figure 25: OC and TRAP values at 3, 7, 15 and 40 days in PLA/PGA copolymer group.
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
3 Days 7 Days 15 Days 40 Days
Autogenous Bone
OC TRAP
0
0.5
1
1.5
2
2.5
3
3.5
3 Days 7 Days 15 Days 40 Days
PLA/PGA Copolymer
OC TRAP
57
Tables
Table 1: Augmented area – Mean (mm²)
Time Autogenous Bone PLA/PGA Copolymer P-value
3 days 35.74 28.36 P=0.004
7 days 36.13 28.99 P=0.004
15 days 27.45 35.44 P=0.004
40 days 32.52 31.49 P=0.458
Table 2: %bone – Mean (%)
Time Autogenous Bone PLA/PGA Copolymer P-value
3 days 56.67 0 P=0.004
7 days 39.80 13.93 P=0.004
15 days 43.47 31.63 P=0.087
40 days 51.63 39.87 P=0.087

58
Table 3: % soft tissue – Mean (%)
Time Autogenous Bone PLA/PGA Copolymer P-value
3 days 43.33 100 P=0.004
7 days 60.40 86.07 P=0.004
15 days 56.53 68.37 P=0.087
40 days 48..37 60.13 P=0.087
59
Anexos
60
Annex 1 - Animal Committee

61
Annex 2 – Article
PLA/PGA copolymer as a bone substitute in maxillary sinus
augmentation. Histological, histometric and immunohistochemistry study in
rabbits
Sabrina Ferreira, DDS1; Roberta Okamoto, DDS, PhD
1; Francisley Ávila Souza, DDS, PhD
1;
Idelmo Rangel Garcia Júnior, DDS, PhD1.
1Division of Surgery and Traumatology Bucco-Maxillo-Facial, Department of Surgery and
General Clinic, Araçatuba Dental School, Univ Estadual Paulista Jºlio de Mesquita Filho –
UNESP, Brazil.
Author responsible for correspondence
Sabrina Ferreira
Telephone: +55 18 3636-3270 / 3636-3237
Rua José Bonifácio, 1193 Vila Mendonça
Department of Surgery and General Clinic
CEP: 16015-050 Araçatuba, SP, Brazil
e-mail: [email protected]
Conflicts of Interest and Source of Funding: none

62
Abstract
The proposition of this study was evaluate the osteoconductive capability of the solid form of
PLA/PGA copolymer in an experimental model of maxillary sinus grafting. Twenty male white
New Zealand rabbits, each weighing about 3.0kg, were used and were divided into two
groups, according to the sinus filling material, as follows: autogenous bone chips and
PLA/PGA copolymers. Augmented area differ between the groups after 3, 7 and 15 days
(P=0.004). However, the values became similar on day 40 (P=0.458). After 3 and 7 days the
percentage of bone was statistically significant between autogenous bone and PLA/PGA
copolymer (P=0.004 and P=0.004). After 15 and 40 days the values were comparable in the
two periods (P=0.087 and P=0.087). Immunohistochemistry confirms the results on the
histomorphometric data. In conclusion, PLA/PGA copolymer seems to be suitable as
resorbable material able to induce bone growth in bone defects. This observation suggests
that the material have osteoconductive properties also suitable for application in maxillofacial
surgery.
Key-words: polylactic acid, polyglycolyc acid, autogenous bone, sinus lift, rabbit
Introduction
Loss of teeth promotes severe, irreversible resorption of alveolar bone1, 2
. In the
posterior region of the maxilla, the height extending from the floor of the maxillary sinus to the
alveolar crest decreases. Various procedures for maxillary sinus augmentation have been
developed to increase bone volume and height to promote stability of endosseous implants1,
3, 4.
63
These procedures require the use of graft materials to maintain the augmented space
and to promote osteogenesis. Early studies advocated the use of autogenous bone to ensure
graft survival and bone formation in the augmented space1, 4
. Blomqvist et al5 reported a
success rate of 82% with implants placed into grafted bone in the maxillary sinus from the iliac
crest; Lundgren et al6 reported a success rate of 80% with such implants. Some authors have
even reported successful short-term sinusal bone augmentation and implant outcomes with
only a blood clot and no grafting material7-11
Moy et al12
and Nishibori et al13
found that the
quantity and quality of bone produced by autogenous bone grafts were superior to those of
bone produced by allografts.
Numerous reports on autogenous grafts at various anatomical sites have been
presented14-17
. Although autogenous bone is still often regarded to be the gold standard in
bone augmentation procedures, morbidity at the donor site as well as reports of significant
levels of resorption, whether intra-oral, extra-oral, block or particulated bone is used,
necessitate the consideration of alternative biomaterials18-21
.
The families of polylactic acid (PLA), polyglycolyc acid (PGA) and their co-polymers
(Poly-Lactide-co-Glycolide, PLA/PGA), both biodegradable, are at the cutting edge of bone
reconstruction procedures. These materials are manufactured in a variety of forms to produce
appliances for use in bone surgery such as tissue barriers22
, fixation devices23, 24
, porous solid
graft25-29
, solid or semi-solid carriers for delivery of growth factor (GF), bone morphogenetic
proteins (BMPs) and other bioactive molecules30, 31
. These materials may also serve as
scaffolding to promote specific cell adhesion, differentiation and bone formation26, 29, 31
.
The resorption of PLA and PGA acids occurs through hydrolysis and hydrolytic
mechanisms. Implanted polymers are expected to play their supportive role in the healing
process and then to degrade to matrix products, which are eliminated through the normal
excretory routes and are replaced by the neighboring tissues32, 33
. This polymer is gradually
substituted by new bone over time, but its degradation depends on the formulation,
amorphous/crystalline structure, isomeric characteristics, molecular weight and amount of

64
material used27, 34
. The exact composition and architecture of the polymeric scaffold becomes
fundamental to promote successful bone regeneration.
Although extensively used in several orthopedic appliances35
, PLA/PGA have been
scarcely applied in oro-maxillo-facial applications. PLA-derived devices were implemented to
prevent alveolar osteitis or dry socket with discordant results by Hooley and Golden36
. PLA
and decalcified freeze-dried bone allografts were clinically studied in the treatment of
periodontal intra-osseous defects by Meadows et al.37
. Results showed a limited amount of
tissue regeneration and the persistence of PLA particles surrounded by soft tissue. A new
PLA/PGA (Fisiograft®
, Ghimas, Italy), manufactured as sponge blocks, gel and powders, was
studied in maxillary sinus floor augmentations29, 38
, as space maker, in alveolar ridge
preservation26
, ridge augmentation with split-crest technique, in the treatment of deep
periodontal intra-osseous defect28
, and in critical bone defects in experimental animals25
with
contrasting results.
Proposition
We therefore histologically, histomorphometrically and immunohistochemically
evaluated the osteoconductive capability of the solid form of PLA/PGA copolymer in an
experimental model of maxillary sinus grafting.
Material and methods
Copolymer PLA/PGA Production
PLA/PGA copolymer consisted of a mixture of lactic and glycolic acid 50/50 saturated
with calcium phosphate, extent that make them gain a solid consistency. The solution pH was
controlled by adding the buffer solution. The method used was the polymeric or Pechini39
method, is a technique that can be applied to the development of advanced materials
65
precursors. The process is based on the ability of certain organic acids such as citric, lactic and
glycolic have to form chelates. These chelates may be esterified with a polyalcohol when
heated and polymerized at higher temperatures forming a resin.
Surgical Procedures
All experimental protocols involving animals were used conformed to procedures
described in the Guiding Principles for the Use of Laboratory Animals and the study approved
by the Animal Committee of Dentistry School of University Estadual Paulista Júlio de Mesquita
Filho, UNESP (00724-2012).
Twenty male white New Zealand rabbits, each weighing about 3.0kg, were used and
were divided into two groups, according to the sinus filling material, as follows: Group 1:
Control, particulate autogenous bone chips and Group 2: PLA/PGA copolymers particles.
All animals underwent surgeries for bilateral sinus lift procedures. The rabbits were
anesthetized with 1% chloridrate of ketamine (Francotar, Virbac Ltda, São Paulo, Brazil), along
with with a sedative, 2% chloridrate of xylazine (Virbaxyl 2%, Virbac Ltda, São Paulo, Brazil), in
the recommended dose, respectively, 60 mg/kg and 5.0mg/kg intramuscularly, and 0.5ml of
1% lidocaine with epinephrine (1:100000) was injected subcutaneously at the midline of the
nasal dorsum and into the tibial metaphysic.
Obtaining Autogenous Bone Graft
Linear incision with approximately 40mm was made in the direction of the long axis in
the tibial metaphysic after previous manual trichotomy and antisepsis preoperative in the right
tibia with friction of gauze soaked in 10% Polyvinyl Pyrrolidone Iodine degermante, with 1%
active iodine (PVP-I 10% Riodeine ®, Rioquímica, São José do Rio Preto) associated with the
topic PVP (10% PVP-I aqueous, with 1% active iodine, Riodeine®, Rioquímica, São José do Rio
66
Preto). Then, the soft tissue overlying the region was elevated in total thickness, exposing the
bone tissue. With the aid of scraper autogenous bone tissue samples were collected for
subsequent filling of the maxillary sinus. Completed sample collection, the surgical flap was
repositioned and sutured in layers.
Sinus Lift
Surgical interventions were performed under strict sterile conditions. The surgical area
was shaved and disinfected with iodine. The sinus lift surgical procedure was performed
according to Asai, Shimizu e Ooya (2002). A midline incision extending for about 50mm was
made, and the skin and periosteum were elevated sufficiently to expose the nasal bone and
nasoincisal suture line. A trephine bur with a 5.0mm internal diameter was used to delineate
the diameter of the bone window for the maxillary sinus access. A circular window was
opened in the nasal bone with the use of a round diamond bur nº 1014 under copious
irrigation with saline solution. The window was located approximately 20mm anterior to the
nasofrontal suture line, 10mm lateral to the midline. Care was taken during this procedure to
avoid damaging the sinus mucosa. The sinus membrane was carefully elevated to allow the
insertion and condensation of the graft materials. No membrane was used to cover the bone
window. In the experimental groups, the compartment was filled with PLA/PGA copolymer
and autogenous bone graft. A suture was placed between the periosteum and skin.
Histologic Procedures
After 3, 7, 15 and 40 days of the surgery, five animals were sacrificed with an overdose
of anesthetics. After decapitation and dissection, the entire nose complex, including the nose
and sinus cavities, was fixed in buffered 10% formaldehyde (Merck, Darmstadt, Germany) for
48 h and washed in tap water for 24 h, and immersed in buffered 4% EDTA for
demineralization. Specimens from the normal and experimental groups were slowly
67
decalcified and were cut in a frontal plane. The specimens were then dehydrated, embedded
in paraffin, and sliced into sections about 6µm thick. The sections were stained with
hematoxylin and eosin (Merck & Co., Inc., NJ, USA) for the light microscopic examination.
Some sections were reserved for immunohistochemistry reactions.
Histological and Histomorphometric Analysis
Each image of the calcified specimens at the rostrocaudal midpoint of the antral wall
was digitally captured at magnification X1.0, X2.8 and X160 and sent to the Image J Program
– Version 1.47 (National Institutes of Health (NIH), Bethesda, Maryland, USA). The composition
of the total augmented sinus was identified (in mm²). The proportions (in %) of each
composite (new bone - NB and soft tissue - ST) were obtained. To evaluate the distribution of
regenerated bone in the grafted sinus area as a secondary outcome variable, the above-
mentioned parameters were measured in specific standardized areas. The areas were
randomly selected and photomicrographs were taken in original magnification X160. The
window region was selected within the grafted area interfacing the imaginary extensions of
the pre-existing cortical bone at the margins of the window, the center region was at the
middle of the whole augmented sinus and membrane region. The membrane region was
chosen from just above the Schneiderian membrane:
Augmented area: defined as the raw surface of the secluded space underneath the
sinus membrane;
% bone, % soft tissues: percentage of the measured augmented area, defined as the
raw surface of the secluded space underneath the sinus membrane.
68
Immunohistochemical Analysis
Immunohistochemical analysis were performed at 3, 7, 15, and 40 days (n = 5). The
following primary antibodies used for immunohistochemical processing were from Santa Cruz
(Biotechnology, CA): anti-osteocalcin (OC) and tartrate-resistant acid phosphatase (TRAP). As a
secondary antibody, a biotinylated donkey anti–goat antibody (Jackson Immunoresearch
Laboratories, West Grove, PA) was used. The signal of the immunohistochemistry reaction
with an avidin biotin system (Kit ABC-Vectastain Elite ABC–peroxidase standard, reagent A and
B only–PK6100; Vector Laboratories, Burlingame, CA), and diaminobenzidine (Sigma, St. Louis,
MO) was used as chromogen.
Immunohistochemical reactions were controlled to evaluate the specificity of the labels.
Hematoxylin and eosin staining was performed and used as a reference of the
cytoarchitecture of the tissue. Immunohistochemical analysis for consist of a qualitative
examination was stratified by a range of values ranging from 0 to 3 (0 = no protein expression,
1 = protein with little expression, 2 = intermediate protein expression, high protein expression
3 =) (Figs 2 and 3).
Statistical assessment
All morphometric data were assessed using the Mann-Whitney. The level of statistical
significance was set at 5%.
Results
Histologic Findings
Experimental group with autogenous bone graft

69
After 3 days, the augmented dome-like space formed by the elevated sinus mucosa
was found to be filled with acellular autogenous bone particles and blood clot, osteocytes in
the lacunae disappeared in the grafted bone.
After 7 days, peripheral newly formed bone trabeculae had irregular surfaces with
numerous osteoblasts and osteoclasts were seen in areas near the sinual membrane and
bone tissue of the nasal complex. Therefore early steps of centripetal new bone formation
were observed progressing from the anterior part of the sinus and the bone walls. Cell
colonization was found everywhere in the cavity, and remnants of clot were sometimes
visible. Remnant acellular autogenous bone particles were seen in the central region of the
space with connective tissue and blood vessels. There was no evidence of acute or chronic
inflammation.
After 15 days, the newly formed woven bone adjacent to the membrane and bone
tissue of the nasal complex showed osteoclastic resorption and the central region were seen
newly formed woven bone and soft tissue. There were many osteocytes in the newly formed
bone. Woven bone with many osteoblasts was observed around the grafted bone, especially
under the elevated antral membrane.
After 40 days, the augmented space revealed mature cortical and trabecular bone
with intertrabecular vascularized adipose tissue. The bone chips were completely remodeled
and their remnants were not visible (Fig. 1).
Experimental group with PLA/PGA copolymer
After 3 days, the augmented dome-like space formed by the elevated sinus mucosa
was found to be filled with blood clot. Copolymer particles were not observed. Mesenchymal
cell proliferation was only visible at the periphery of the created space, while the blood clot
was still non-invaded by mesenchymal cells in the center of the cavity. No inflammatory cell
infiltration was present.

70
After 7 the augmented dome-like space was found to be filled connective tissue with
fibroblasts and blood vessels. Remnant blood clots were seen in the central region of the
space. Peripheral newly formed woven bone was seen. Therefore early steps of centripetal
new bone formation were observed progressing from the anterior part of the sinus and the
bone walls.
After 15 days, peripheral newly formed bone was seen in areas near the sinual
membrane and bone tissue of the nasal complex. Connective tissue was seen in the central
region of the space with fibroblasts and blood vessels.
After 40 days, the augmented space revealed mature cortical and trabecular bone
with intertrabecular vascularized adipose tissue. The bone trabeculae showed the minimal
osteoclastic resorption. Some areas near the sinual membrane and bone tissue of the nasal
complex revealed mature cortical and trabecular bone with intertrabecular vascularized
adipose tissue (Fig.1).
Histomorphometric Analysis
Augmented area
Augmented area differ between the groups after 3, 7 and 15 days(P=0.004). However,
the values became similar on day 40 (P=0.458). The comparison of values of 3 and 40 days
autogenous bone group and PLA/PGA copolymer group and were also statistically significant
(P=0.004 e P=0.004) .Values in mm2 of the augmented area are presented in Table 1.
% bone, % soft tissues
After 3 days, in the autogenous bone group, bone inside the created space under the
membrane constituted 56.67% of the measured augmented area, while in the PLA/PGA
71
copolymer group, the amount of bone constituted 0%. The percentage of bone was
significantly higher with autogenous bone than with PLA/PGA copolymer (P=0.004).
After 7 days, in the autogenous bone group, bone ingrowths constituted 39.80% of
the measured augmented area, while in the PLA/PGA copolymer group, the amount of bone
ingrowth failed to reach 13.93%. The percentage of bone was significantly higher with
autogenous bone than with PLA/PGA copolymer (P=0.004).
After 15 days, the area occupied by newly formed bone reached, respectively, 43.47%
and 31.63% (P=0.087) for the autogenous bone and the PLA/PGA copolymer groups. The
implanted bone chips could be observed in the central area.
After 40 days, in the autogenous bone and PLA/PGA copolymer groups, the newly
formed bone area increased to 51.63% and 39.87%, respectively. The values were
comparable in the three groups (P=0.087). Detailed results are presented in Table 2 and
shows the correlation between volume changes over time and % bone and % soft tissues
within augmented tissues (Tables 2 and 3).
Immunohistochemical Analysis
OC immunoreactivity could be seen in all augmented area for the autogenous bone
group in the early periods of this study, 3 days (intermediate protein expression), with
increased at 7 days (high protein expression) and remaining high on 15 and 40 days (high
protein expression) after surgery. Similarly to autogenous bone group, in the PLA/PGA
copolymer group, OC immunoexpressivity was seen intermediate at 3 days, with increased at
7 days (high protein expression), remaining high on 15 days (high protein expression).
However, declined at 40 days (intermediate protein expression) after surgery.
In TRAP immunohistochemistry could be seen in autogenous bone group high protein
expression in the early periods, 3 days. However, this declined at 7 days (intermediate protein
expression). At 15 days after surgery increased expression of TRAP (high protein expression)

72
with decline at 40 days (intermediate protein expression). Differently to the autogenous bone
group, in the PLA/PGA copolymer group TRAP immunoexpressivity had gradual increased: 3
days protein with little expression, 7 days with intermediate protein expression and 15 days
with high protein expression. However, declined at 40 days (intermediate protein expression)
(Fig. 2).
Discussion
This rabbit study investigated the area stability of sub-sinusal bone regeneration when
autogenous bone chips or PLA/PGA copolymer 50/50 were used as space fillers. Early bone
formation and the continuing behavior of the regenerated bone with these different types of
filling material were also assessed. Rabbits have similar maxillary sinus ventilation to humans
and a well-defined ostium opening to their nasal cavities. The rabbit sinus lift model is
therefore appropriate and well documented for evaluating bone regeneration physiology in
sub-sinusal bone regeneration40, 41
.
Adequate bone healing was observed with the two space fillers used in the present
study and no signs of inflammation could be detected. Similar findings have already been
reported by several authors29, 40, 41
; unfortunately, the early steps of bone regeneration were
poorly studied in these papers.
In this study, in PLA/PGA copolymer cell proliferation was detected after 7 days only
along the bone wall and under the sinusal membrane, while the central part was still
occupied by a dense cluster of red blood cells, in contrast with the autogenous bone group
where the augmented space was completely invaded by mesenchymal cells. A gradient of
maturity of the newly formed tissue from the native bony walls to the center of the cavity
illustrated the centripetal nature of the regenerative process.
At 15 days, in the PLA/PGA copolymer group, non-mineralized fibrous tissue still
occupied the central area. At 40 days, in the PLA/PGA copolymer group, woven bone was
73
found everywhere in the remaining cavity. Therefore, PLA/PGA copolymer implanted into
sub-sinusal cavities allowed bone formation. Rimondini et al25
reported that the
histomorphometric data demonstrated that the experimental material is able to promote bone
healing even in a large bone defect such as in rabbit femoral condyles. The bone maturation
improved from 30 to 90 days. The data concerning the development of the forming bone
showed that during the 30 to 90 days the material allowed a bone remodeling from reticular
toward a trabecular structure.
Fisiograft®
is a synthetic resorbable sponge formed by 50–50 lactide–glycolide
polymer. This copolymer has shown the fastest degradation rate of the d-l lactide/glycolide
biomaterials, with the polymer degrading in about 50–60 days42
. In the previous study37
PLA
granules were still evident at 6-month surgical re-entry.
In the autogenous bone group, the early healing process was characterized by a
particularly high cellular density along the bone chips, even at a distance from the bony walls.
This picture strongly suggests an osteogenic potential provided by autogenous bone chips. At
15 days, the anatomy of the dense woven bone seemed to be influenced by the initial rolled
shape of the bone chips, now remodeled. The remodeling process continued from 15 days to
40 days yielding, in the long term, rarefied mature bone architecture. According to Schlegel et
al.43
, this remodeling process was also observed in sinus lifts performed in humans with
particulated autogenous bone.
New bone formation was already observed at 2 weeks after grafting. It is of interest
that new bone formation was observed in all parts under the elevated antral membrane,
around the grafted bone, and at the superior part of the original sinus floor. The result
indicates that new bone formation may depend not only on osteoconduction from the
recipient site but also on osteoinduction by bone morphogenetic protein in the grafted bone
and osteogenesis by the bone cells that were grafted with the bone.
Albrektsson44
reported that early revascularization meant early bone remodeling of a
graft in the rabbit tibia; in the present study, blood vessels were already seen in the grafted

74
bone at 7 days. It is suggested that early revascularization also assisted in the new bone
formation for the maxillary sinus in the present study.
Much newly formed bone was noted under the elevated membrane at 40 days after
grafting. Moreover, continuous cortical bone was observed under this membrane. These
results indicate the difference in bone formation between the continuous bone located under
the elevated membrane and continuous bone located elsewhere. In the present study, the
medullary cavity was filled with many fat cells.
In our study, the mean bone fractions in the grafted area were 56.67%, 39.80%,
43.47% and 51.63%, respectively, at 3, 7, 15, and 40 days after grafting. The bone fraction in
the bone biopsy cores was reported in a few studies; Moy et al45
, for example, indicated that
the composition of bone was 59.4% from chin bone graft, and Lundgren et al46
reported the
mean bone fractions in chin bone grafted areas to be 40% and 48%, respectively, at 6 and 12
months after bone grafting.
Immunohistochemistry confirms the results on the histomorphometric data. During the
period of increase of regeneration area, between 3 and 7 days, the OC values also showed an
increase in both experimental groups. Important to note that the lower expression group in
the copolymer shows an early stage of the process when compared to autogenous bone
group. In both groups, the period 7-15 days it is possible to see a tendency to equilibrium in
the processes of bone formation and remodeling, we see a tendency to balance the values of
OC and TRAP. Increased OC shows the mineralization phase in which it is the bone tissue
after 40 days in the autogenous bone group, since the values of TRAP are consistent the
period of remodeling of bone trabeculae, characteristic of this period. Unlike the group
copolymer in the same period seems to still keep the balance-training resorption.
The present study showed that the long-term outcome of augmentation of the sinus
was not the maturation of newly formed bone, but conversely atrophy of bone. Indeed, an
increase in adipose tissue in marrow is observed in all conditions that lead to loss of bone,
such as osteoporosis, age-related osteopenia, or immobilisation47
. This apparent reciprocal
75
relation between reduced bone density and increased fat can be explained by an imbalance
in the production of bone-forming and fat-forming cells48
.
But an excess of adipose tissue in marrow is considered to put at risk the long-term
ability to maintain the mechanical strength of the skeleton49
. Mechanical stress is an essential
factor for the corticalisation of bone50
. Ideal bone grafts should eventually be absorbed and
encourage formation of new bone, which replenishes lost bone permanently.
In conclusion, PLA/PGA copolymer seems to be suitable as resorbable material able to
induce bone growth in bone defects. This observation suggests that the material have
osteoconductive properties also suitable for application in maxillofacial surgery.
Reference
[1] Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and
bone. J Oral Surg 1980 Aug;38(8):613-6.
[2] Keller EE, Van Roekel NB, Desjardins RP, Tolman DE. Prosthetic-surgical reconstruction
of the severely resorbed maxilla with iliac bone grafting and tissue-integrated prostheses. Int J
Oral Maxillofac Implants 1987 Summer;2(3):155-65.
[3] Tatum H, Jr. Maxillary and sinus implant reconstructions. Dent Clin North Am 1986
Apr;30(2):207-29.
[4] Wood RM, Moore DL. Grafting of the maxillary sinus with intraorally harvested
autogenous bone prior to implant placement. Int J Oral Maxillofac Implants 1988 Fall;3(3):209-
14.
[5] Blomqvist JE, Alberius P, Isaksson S. Retrospective analysis of one-stage maxillary sinus
augmentation with endosseous implants. Int J Oral Maxillofac Implants 1996 Jul-
Aug;11(4):512-21.

76
[6] Lundgren S, Nystrom E, Nilson H, Gunne J, Lindhagen O. Bone grafting to the
maxillary sinuses, nasal floor and anterior maxilla in the atrophic edentulous maxilla. A two-
stage technique. Int J Oral Maxillofac Surg 1997 Dec;26(6):428-34.
[7] Nedir R, Bischof M, Vazquez L, Szmukler-Moncler S, Bernard JP. Osteotome sinus floor
elevation without grafting material: a 1-year prospective pilot study with ITI implants. Clin Oral
Implants Res 2006 Dec;17(6):679-86.
[8] Nedir R, Bischof M, Vazquez L, Nurdin N, Szmukler-Moncler S, Bernard JP. Osteotome
sinus floor elevation technique without grafting material: 3-year results of a prospective pilot
study. Clin Oral Implants Res 2009 Jul;20(7):701-7.
[9] Gabbert O, Koob A, Schmitter M, Rammelsberg P. Implants placed in combination with
an internal sinus lift without graft material: an analysis of short-term failure. J Clin Periodontol
2009 Feb;36(2):177-83.
[10] Lundgren S, Andersson S, Gualini F, Sennerby L. Bone reformation with sinus
membrane elevation: a new surgical technique for maxillary sinus floor augmentation. Clin
Implant Dent Relat Res 2004;6(3):165-73.
[11] Palma VC, Magro-Filho O, de Oliveria JA, Lundgren S, Salata LA, Sennerby L. Bone
reformation and implant integration following maxillary sinus membrane elevation: an
experimental study in primates. Clin Implant Dent Relat Res 2006;8(1):11-24.
[12] Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most
successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants
2007;22 Suppl:49-70.
[13] Nishibori M, Betts NJ, Salama H, Listgarten MA. Short-term healing of autogenous and
allogeneic bone grafts after sinus augmentation: a report of 2 cases. J Periodontol 1994
Oct;65(10):958-66.
[14] Lew D, Marino AA, Startzell JM, Keller JC. A comparative study of osseointegration of
titanium implants in corticocancellous block and corticocancellous chip grafts in canine ilium. J
Oral Maxillofac Surg 1994 Sep;52(9):952-8; discussion 9.

77
[15] Chen NT, Glowacki J, Bucky LP, Hong HZ, Kim WK, Yaremchuk MJ. The roles of
revascularization and resorption on endurance of craniofacial onlay bone grafts in the rabbit.
Plast Reconstr Surg 1994 Apr;93(4):714-22; discussion 23-4.
[16] Nathanson A. The early ingrowth of an autogenous bone inlay into an artificial defect
in the rabbit mandibula. Scand J Plast Reconstr Surg 1977;11(2):97-108.
[17] Alberius P, Gordh M, Lindberg L, Johnell O. Onlay bone graft behaviour after marrow
exposure of the recipient rat skull bone. Scand J Plast Reconstr Surg Hand Surg 1996
Dec;30(4):257-66.
[18] Araujo MG, Sonohara M, Hayacibara R, Cardaropoli G, Lindhe J. Lateral ridge
augmentation by the use of grafts comprised of autologous bone or a biomaterial. An
experiment in the dog. J Clin Periodontol 2002 Dec;29(12):1122-31.
[19] Cordaro L, Torsello F, Accorsi Ribeiro C, Liberatore M, Mirisola di Torresanto V. Inlay-
onlay grafting for three-dimensional reconstruction of the posterior atrophic maxilla with
mandibular bone. Int J Oral Maxillofac Surg 2010 Apr;39(4):350-7.
[20] Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Piombino P, Guidetti F. Volume
changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae
and mandibles. Int J Oral Maxillofac Surg 2009 Oct;38(10):1059-65.
[21] Zijderveld SA, Schulten EA, Aartman IH, ten Bruggenkate CM. Long-term changes in
graft height after maxillary sinus floor elevation with different grafting materials: radiographic
evaluation with a minimum follow-up of 4.5 years. Clin Oral Implants Res 2009 Jul;20(7):691-
700.
[22] Hammerle CH, Lang NP. Single stage surgery combining transmucosal implant
placement with guided bone regeneration and bioresorbable materials. Clin Oral Implants Res
2001 Feb;12(1):9-18.
[23] Peltoniemi H, Ashammakhi N, Kontio R, Waris T, Salo A, Lindqvist C, et al. The use of
bioabsorbable osteofixation devices in craniomaxillofacial surgery. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2002 Jul;94(1):5-14.
78
[24] Leiggener CS, Curtis R, Muller AA, Pfluger D, Gogolewski S, Rahn BA. Influence of
copolymer composition of polylactide implants on cranial bone regeneration. Biomaterials
2006 Jan;27(2):202-7.
[25] Rimondini L, Nicoli-Aldini N, Fini M, Guzzardella G, Tschon M, Giardino R. In vivo
experimental study on bone regeneration in critical bone defects using an injectable
biodegradable PLA/PGA copolymer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005
Feb;99(2):148-54.
[26] Serino G, Biancu S, Iezzi G, Piattelli A. Ridge preservation following tooth extraction
using a polylactide and polyglycolide sponge as space filler: a clinical and histological study in
humans. Clin Oral Implants Res 2003 Oct;14(5):651-8.
[27] Martin C, Winet H, Bao JY. Acidity near eroding polylactide-polyglycolide in vitro and in
vivo in rabbit tibial bone chambers. Biomaterials 1996 Dec;17(24):2373-80.
[28] Minenna L, Herrero F, Sanz M, Trombelli L. Adjunctive effect of a
polylactide/polyglycolide copolymer in the treatment of deep periodontal intra-osseous
defects: a randomized clinical trial. J Clin Periodontol 2005 May;32(5):456-61.
[29] Zaffe D, Leghissa GC, Pradelli J, Botticelli AR. Histological study on sinus lift grafting by
Fisiograft and Bio-Oss. J Mater Sci Mater Med 2005 Sep;16(9):789-93.
[30] El-Amin SF, Lu HH, Khan Y, Burems J, Mitchell J, Tuan RS, et al. Extracellular matrix
production by human osteoblasts cultured on biodegradable polymers applicable for tissue
engineering. Biomaterials 2003 Mar;24(7):1213-21.
[31] Saito N, Okada T, Horiuchi H, Ota H, Takahashi J, Murakami N, et al. Local bone
formation by injection of recombinant human bone morphogenetic protein-2 contained in
polymer carriers. Bone 2003 Apr;32(4):381-6.
[32] Cutright DE, Perez B, Beasley JD, 3rd, Larson WJ, Posey WR. Degradation rates of
polymers and copolymers of polylactic and polyglycolic acids. Oral Surg Oral Med Oral Pathol
1974 Jan;37(1):142-52.

79
[33] Visscher GE, Robison RL, Maulding HV, Fong JW, Pearson JE, Argentieri GJ.
Biodegradation of and tissue reaction to 50:50 poly(DL-lactide-co-glycolide) microcapsules. J
Biomed Mater Res 1985 Mar;19(3):349-65.
[34] Lu HH, El-Amin SF, Scott KD, Laurencin CT. Three-dimensional, bioactive,
biodegradable, polymer-bioactive glass composite scaffolds with improved mechanical
properties support collagen synthesis and mineralization of human osteoblast-like cells in vitro.
J Biomed Mater Res A 2003 Mar 1;64(3):465-74.
[35] Athanasiou KA, Agrawal CM, Barber FA, Burkhart SS. Orthopaedic applications for PLA-
PGA biodegradable polymers. Arthroscopy 1998 Oct;14(7):726-37.
[36] Hooley JR, Golden DP. The effect of polylactic acid granules on the incidence of
alveolar osteitis after mandibular third molar surgery. A prospective randomized study. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 1995 Sep;80(3):279-83.
[37] Meadows CL, Gher ME, Quintero G, Lafferty TA. A comparison of polylactic acid
granules and decalcified freeze-dried bone allograft in human periodontal osseous defects. J
Periodontol 1993 Feb;64(2):103-9.
[38] Scarano A, Degidi M, Iezzi G, Pecora G, Piattelli M, Orsini G, et al. Maxillary sinus
augmentation with different biomaterials: a comparative histologic and histomorphometric
study in man. Implant Dent 2006 Jun;15(2):197-207.
[39] Hussain A, Jadhav AP, Baek YK, Choi HJ, Lee J, Kang YS. One pot synthesis of exchange
coupled Nd2Fe14B/alpha-Fe by pechini type sol-gel method. J Nanosci Nanotechnol 2013
Nov;13(11):7717-22.
[40] Asai S, Shimizu Y, Ooya K. Maxillary sinus augmentation model in rabbits: effect of
occluded nasal ostium on new bone formation. Clin Oral Implants Res 2002 Aug;13(4):405-9.
[41] Sun XJ, Zhang ZY, Wang SY, Gittens SA, Jiang XQ, Chou LL. Maxillary sinus floor
elevation using a tissue-engineered bone complex with OsteoBone and bMSCs in rabbits. Clin
Oral Implants Res 2008 Aug;19(8):804-13.

80
[42] Eppley BL, Reilly M. Degradation characteristics of PLLA-PGA bone fixation devices. J
Craniofac Surg 1997 Mar;8(2):116-20.
[43] Schlegel KA, Schultze-Mosgau S, Wiltfang J, Neukam FW, Rupprecht S, Thorwarth M.
Changes of mineralization of free autogenous bone grafts used for sinus floor elevation. Clin
Oral Implants Res 2006 Dec;17(6):673-8.
[44] Albrektsson T. Repair of bone grafts. A vital microscopic and histological investigation in
the rabbit. Scand J Plast Reconstr Surg 1980;14(1):1-12.
[45] Moy PK, Lundgren S, Holmes RE. Maxillary sinus augmentation: histomorphometric
analysis of graft materials for maxillary sinus floor augmentation. J Oral Maxillofac Surg 1993
Aug;51(8):857-62.
[46] Lundgren S, Moy P, Johansson C, Nilsson H. Augmentation of the maxillary sinus floor
with particulated mandible: a histologic and histomorphometric study. Int J Oral Maxillofac
Implants 1996 Nov-Dec;11(6):760-6.
[47] Verma S, Rajaratnam JH, Denton J, Hoyland JA, Byers RJ. Adipocytic proportion of
bone marrow is inversely related to bone formation in osteoporosis. J Clin Pathol 2002
Sep;55(9):693-8.
[48] Atmani H, Chappard D, Basle MF. Proliferation and differentiation of osteoblasts and
adipocytes in rat bone marrow stromal cell cultures: effects of dexamethasone and calcitriol. J
Cell Biochem 2003 May 15;89(2):364-72.
[49] Nuttall ME, Gimble JM. Is there a therapeutic opportunity to either prevent or treat
osteopenic disorders by inhibiting marrow adipogenesis? Bone 2000 Aug;27(2):177-84.
[50] Frost HM. Perspectives: bone's mechanical usage windows. Bone Miner 1992
Dec;19(3):257-71.

81
Figure e Table
Fig
ure
1: P
LA/P
GA
co
po
lym
er
at
(a)
3, (
b)
7, (
c) 1
5 a
nd
(d
) 4
0 d
ays
. Au
tog
en
ou
s b
on
e g
rou
p a
t (e
) 3
, (f)
7, (
g)
15
an
d (
h)
40
days
.

82
Figure 2: Autogenous bone group; OC immunoreactivity in (a) 3, (b) 7, (c) 15
and (d) 40 days. PLA/PGA copolymer group; OC immunoreactivity in (e) 3, (f) 7,
(g) 15 and (h) 40 days.

83
Figure 3: Autogenous bone group; TRAP immunoreactivity in (a) 3, (b) 7, (c) 15
and (d) 40 days. PLA/PGA copolymer group; TRAP immunoreactivity in (e) 3, (f)
7, (g) 15 and (h) 40 days.

84
Table 1: Augmented area – Mean (mm²)
Time Autogenous Bone PLA/PGA Copolymer P-value
3 days 35.74 28.36 P=0.004
7 days 36.13 28.99 P=0.004
15 days 27.45 35.44 P=0.004
40 days 32.52 31.49 P=0.458
Table 2: %bone – Mean (%)
Time Autogenous Bone PLA/PGA Copolymer P-value
3 days 56.67 0 P=0.004
7 days 39.80 13.93 P=0.004
15 days 43.47 31.63 P=0.087
40 days 51.63 39.87 P=0.087

85
Table 3: % soft tissue – Mean (%)
Time Autogenous Bone PLA/PGA Copolymer P-value
3 days 43.33 100 P=0.004
7 days 60.40 86.07 P=0.004
15 days 56.53 68.37 P=0.087
40 days 48..37 60.13 P=0.087

86
Anexo 3 – Normas IJOMS
International Journal of Oral & Maxillofacial Surgery
Guide for Authors
Would authors please note that the reference style for the journal has now changed. Please
pay special attention to the guidelines under the heading "References" below
Authors wishing to submit their work to the journal are urged to read this detailed guide for
authors and comply with all the requirements, particularly those relating to manuscript length
and format. This will speed up the reviewing process and reduce the time taken to publish a
paper following acceptance.
Online Submission: Submission and peer-review of all papers is now conducted entirely
online, increasing efficiency for editors, authors, and reviewers, and enhancing publication
speed. Authors requiring further information on online submission are strongly encouraged to
view the system, including a tutorial, at http://ees.elsevier.com/ijoms A comprehensive
Author Support service is available to answer additional enquiries at
[email protected]. Once a paper has been submitted, all subsequent
correspondence between the Editorial Office ([email protected]) and the corresponding
author will be by e-mail.
Editorial Policy: A paper is accepted for publication on the understanding that it has not been
submitted simultaneously to another journal, has been read and approved by all authors, and
that the work has not been published before. The Editors reserve the right to make editorial
and literary corrections. Any opinions expressed or policies advocated do not necessarily
reflect the opinions and policies of the Editors.
Declarations: Upon submission you will be required to complete and upload this form (pdf
version or word version) to declare funding, conflict of interest and to indicate whether ethical
approval was sought. This information must also be inserted into your manuscript under the
87
acknowledgements section with the headings below. If you have no declaration to make
please insert the following statements into your manuscript:
Funding: None; Competing interests: None declared; Ethical approval: Not required; Patient
permission: Not required
PLEASE NOTE that all funding must be declared at first submission, as the addition of funding
at acceptance stage may invalidate the acceptance of your manuscript.
Authorship: All authors should have made substantial contributions to all of the following: (1)
the conception and design of the study, or acquisition of data, or analysis and interpretation of
data (2) drafting the article or revising it critically for important intellectual content (3) final
approval of the version to be submitted.
Normally one or two, and no more than three, authors should appear on a short
communication, technical note or interesting case/lesson learnt. Full length articles may
contain as many authors as appropriate. Minor contributors and non-contributory clinicians
who have allowed their patients to be used in the paper should be acknowledged at the end
of the text and before the references.
The corresponding author is responsible for ensuring that all authors are aware of their
obligations.
Before a paper is accepted all the authors of the paper must sign the Confirmation of
Authorship form. This form confirms that all the named authors agree to publication if the
paper is accepted and that each has had significant input into the paper. Please download
the form and send it to the Editorial Office. (pdf version or word version) It is advisable that to
prevent delay this form is submitted early in the editorial process.
Acknowledgements: All contributors who do not meet the criteria for authorship as defined
above should be listed in an acknowledgements section. Examples of those who might be
acknowledged include a person who provided purely technical help, writing assistance, or a
department chair who provided only general support. Authors should disclose whether they
had any writing assistance and identify the entity that paid for this assistance.
88
Conflict of interest: At the end of the main text, all authors must disclose any financial and
personal relationships with other people or organisations that could inappropriately influence
(bias) their work. Examples of potential conflicts of interest include employment, consultancies,
stock ownership, honoraria, paid expert testimony, patent applications/registrations, and
grants or other funding. If an author has no conflict of interest to declare, this should be
stated.
Role of the funding source: All sources of funding should be declared as an
acknowledgement at the end of the text. Authors should declare the role of study sponsors, if
any, in the study design, in the collection, analysis and interpretation of data; in the writing of
the manuscript; and in the decision to submit the manuscript for publication. If the study
sponsors had no such involvement, the authors should so state.
Open access: This journal offers you the option of making your article freely available to all via
the ScienceDirect platform. To prevent any conflict of interest, you can only make this choice
after receiving notification that your article has been accepted for publication. The fee of
$3,000 excludes taxes and other potential author fees such as color charges. In some cases,
institutions and funding bodies have entered into agreement with Elsevier to meet these fees
on behalf of their authors. Details of these agreements are available at
http://www.elsevier.com/fundingbodies. Authors of accepted articles, who wish to take
advantage of this option, should complete and submit the order form (available at
http://www.elsevier.com/locate/openaccessform.pdf). Whatever access option you choose,
you retain many rights as an author, including the right to post a revised personal version of
your article on your own website. More information can be found here:
http://www.elsevier.com/authorsrights.
Ethics: Work on human beings that is submitted to the International Journal of Oral and
Maxillofacial Surgery should comply with the principles laid down in the Declaration of
Helsinki (Recommendations guiding physicians in biomedical research involving human
subjects. Adopted by the 18th World Medical Assembly, Helsinki, Finland, June 1964,

89
amended by the 29th World Medical Assembly, Tokyo, Japan, October 1975, the 35th World
Medical Assembly, Venice, Italy, October 1983, and the 41st World Medical Assembly, Hong
Kong, September 1989). The manuscript should contain a statement that the work has been
approved by the appropriate ethical committees related to the institution(s) in which it was
performed and that subjects gave informed consent to the work. Studies involving
experiments with animals must state that their care was in accordance with institution
guidelines. Patients' and volunteers' names, initials, and hospital numbers should not be used.
Patient confidentiality: Patients have a right to privacy. Therefore identifying information,
including patients' images, names, initials, or hospital numbers, should not be included in
videos, recordings, written descriptions, photographs, and pedigrees unless the information is
essential for scientific purposes and you have obtained written informed consent for
publication in print and electronic form from the patient (or parent, guardian or next of kin
where applicable). If such consent is made subject to any conditions, The Editor and Publisher
must be made aware of all such conditions. Written consents must be provided to the
Editorial Office on request. Even where consent has been given, identifying details should be
omitted if they are not essential. If identifying characteristics are altered to protect anonymity,
such as in genetic pedigrees, authors should provide assurance that alterations do not distort
scientific meaning and editors should so note. If consent for publication has not been
obtained, personal details of patients included in any part of the paper and in any
supplementary materials (including all illustrations and videos) must be removed before
submission.
Language Editing Services: Papers will only be accepted when they are written in an
acceptable standard of English. Authors, particularly those whose first language is not English,
who require information about language editing and copyediting services pre- and post-
submission should visit
http://www.elsevier.com/wps/find/authorshome.authors/languagepolishing or contact
[email protected] for more information. Please note, Elsevier neither endorses nor

90
takes responsibility for any products, goods or services offered by outside vendors through our
services or in any advertising. For more information please refer to our Terms and Conditions
http://www.elsevier.com/wps/find/termsconditions.cws_home/termsconditions.
Article Types:The following contributions will be accepted for publication. Please take careful
note of the maximum length where applicable. Overlength articles will be returned to the
authors without peer review: • editorials (commissioned by the editor) • clinical papers: no
more than 5000 words and 30 references • research papers: no more than 6000 words and
40 references • review papers - no limit on length or number of references • technical notes
(surgical techniques, new instruments, technical innovations) - no more than 2000 words, 10
references and 4 figures • case reports - no more than 2000 words, 10 references and 2
figures • book reviews • letters to the editor - please see detailed guidelines provided at the
end of the main guide for authors • IAOMS announcements • general announcements.
Please note: Case reports will be considered for publication only if they add new information
to the existing body of knowledge or present new points of view on known diseases.
All authors must have contributed to the paper, not necessarily the patient treatment.
Technical notes and case reports are limited to a maximum of 4 authors, in exceptional
circumstances, 5.
Criteria for Publication: Papers that will be considered for publication should be: • focused •
based on a sound hypothesis and an adequate investigation method analysing a statistically
relevant series, leading to relevant results that back the conclusion • well written in simple,
scientific English grammar and style • presented with a clear message and containing new
information that is relevant for the readership of the journal • Note the comment above
relating to case reports.
Following peer-review, authors are required to resubmit their revised paper within 3 months;
in exceptional circumstances, this timeline may be extended at the editor's discretion.
Presentation of Manuscripts: General points
91
Papers should be submitted in journal style. Failure to do so will result in the paper being
immediately returned to the author and may lead to significant delays in publication. Spelling
may follow British or American usage, but not a mixture of the two. Papers should be double-
spaced with a margin of at least 3 cm all round.
Format: Papers should be set out as follows, with each section beginning on a separate page:
• title page • abstract • text • acknowledgements • references • tables • captions to
illustrations.
Please note that the qualifications of the authors will not be included in the published paper
and should not be listed anywhere on the manuscript.
Title page: The title page should give the following information: • title of the article • full
name of each author • name and address of the department or institution to which the work
should be attributed • name, address, telephone and fax numbers, and e-mail address of the
author responsible for correspondence and to whom requests for offprints should be sent •
sources of support in the form of grants • key words.
If the title is longer than 40 characters (including spaces), a short title should be supplied for
use in the running heads.
Abstract
200 words maximum. Do not use subheadings or abbreviations; write as a continuous
paragraph. Must contain all relevant information, including results and conclusion.
Text: Please ensure that the text of your paper conforms to the following structure:
Introduction, Materials and Methods, Results, Discussion. There is no separate Conclusion
section. There should be no mention of the institution where the work was carried out,
especially in the Materials and Methods section.
Introduction: • Present first the nature and scope of the problem investigated • Review briefly
the pertinent literature • State the rationale for the study • Explain the purpose in writing the
paper • State the method of investigation and the reasons for the choice of a particular
method •; Should be written in the present tense

92
Materials and Methods: • Give the full details, limit references • Should be written in the past
tense • Include exact technical specifications, quantities and generic names • Limit the
number of subheadings, and use the same in the results section • Mention statistical method
• Do not include results in this section
Results: • Do not describe methods • Present results in the past tense • Present
representations rather than endlessly repetitive data • Use tables where appropriate, and do
not repeat information in the text
Discussion: • Discuss - do not recapitulate results • Point out exceptions and lack of
correlations. Do not try to cover up or 'fudge' data • Show how results agree/contrast with
previous work • Discuss the implications of your findings • State your conclusions very clearly
Headings: Headings enhance readability but should be appropriate to the nature of the
paper. They should be kept to a minimum and may be removed by the Editors. Normally only
two categories of headings should be used: major ones should be typed in capital letters;
minor ones should be typed in lower case (with an initial capital letter) at the left hand margin.
Quantitative analysis: If any statistical methods are used, the text should state the test or other
analytical method applied, basic descriptive statistics, critical value obtained, degrees of
freedom, and significance level, e.g. (ANOVA, F=2.34; df=3,46; P<0.001). If a computer data
analysis was involved, the software package should be mentioned. Descriptive statistics may
be presented in the form of a table, or included in the text.
Abbreviations, symbols, and nomenclature: Only standardized terms, which have been
generally accepted, should be used. Unfamiliar abbreviations must be defined when first used.
For further details concerning abbreviations, see Baron DN, ed. Units, symbols, and
abbreviations. A guide for biological and medical editors and authors, London, Royal Society
of Medicine, 1988 (available from The Royal Society of Medicine Services, 1 Wimpole Street,
London W1M 8AE, UK).
The minus sign should be -. If a special designation for teeth is used, a note should explain the
symbols. Scientific names of organisms should be binomials, the generic name only with a

93
capital, and should be italicised in the typescript. Microorganisms should be named according
to the latest edition of the Manual of Clinical Microbiology, American Society of Microbiology.
Drugs: use only generic (non-proprietary) names in the text. Suppliers of drugs used may be
named in the Acknowledgments section. Do not use 'he', 'his' etc where the sex of the person
is unknown; say 'the patient' etc. Avoid inelegant alternatives such as 'he/she'. Patients should
not be automatically designated as 'she', and doctors as 'he'.
References
The journal's reference style has changed. References should be numbered consecutively
throughout the article, beginning with 1 for the first-cited reference. References should be
listed at the end of the paper in the order in which they appear in the text (not listed
alphabetically by author and numbered as previously).
The accuracy of references is the responsibility of the author. References in the text should be
numbered with superscript numerals inside punctuation: for example "Kenneth and Cohen14
showed..."; "each technique has advantages and disadvantages5-13
." Citations in the text to
papers with more than two authors should give the name of the first author followed by "et
al."; for example: "Wang et al37
identified..."
All references cited in the text must be included in the list of references at the end of the
paper. Each reference listed must include the names of all authors. Please see section "Article
Types" for guidance on the maximum number of reference for each type of article.
Titles of journals should be abbreviated according to Index Medicus (see
www.nlm.nih.gov.uk) . When citing papers from monographs and books, give the author,
title of chapter, editor of book, title of book, publisher, place and year of publication, first and
last page numbers. Internet pages and online resources may be included within the text and
should state as a minimum the author(s), title and full URL. The date of access should be
supplied and all URLs should be checked again at proof stage.
94
Examples:
Journal article: Halsband ER, Hirshberg YA, Berg LI. Ketamine hydrochloride in outpatient oral
surgery. J Oral Surg 1971: 29: 472-476.
When citing a paper which has a Digital Object Identifier (DOI), use the following style:
Toschka H, Feifel H. Aesthetic and functional results of harvesting radial forearm flap. Int J Oral
Maxillofac Surg 2001: 30: 45-51. doi: 10.1054/ijom.2000.0005
Book/monograph: Costich ER, White RP. Fundamentals of oral surgery. Philadelphia: WB
Saunders, 1971: 201-220.
Book chapter: Hodge HC, Smith FA. Biological properties of inorganic fluorides. In: Simons JH,
ed.: Fluorine chemistry. New York: Academic Press, 1965: 135.
Internet resource: International Committee of Medical Journal Editors. Uniform requirements
for manuscripts submitted to biomedical journals. http://www.icmje.org [Accessibility
verified March 21, 2008]
Tables
Tables should be used only to clarify important points. Double documentation in the form of
tables and figures is not acceptable. Tables should be numbered consecutively with Arabic
numerals. They should be double spaced on separate pages and contain only horizontal
rules. Do not submit tables as photographs. A short descriptive title should appear above each
table, with any footnotes suitably identified below. Care must be taken to ensure that all units
are included. Ensure that each table is cited in the text.
Figures
All illustrations (e.g. graphs, drawings or photographs) are considered to be figures, and
should be numbered in sequence with Arabic numerals. Each figure should have a caption,
typed double-spaced on a separate page and numbered correspondingly. The minimum
resolution for electronically generated figures is 300 dpi.
Line illustrations: All line illustrations should present a crisp black image on an even white
background (127 x 178 mm (5 x 7 in), or no larger than 203 x 254 mm (8 x 10 in). The size of

95
the lettering should be appropriate, taking into account the necessary size reduction.
Photographs and radiographs: Photomicrographs should show magnification and details of
any staining techniques used. The area(s) of interest must be clearly indicated with arrows or
other symbols.
Colour images are encouraged, but the decision whether an illustration is accepted for
reproduction in colour in the printed journal lies with the editor-in-chief. Figures supplied in
colour will appear in colour in the online version of the journal.
Size of photographs: The final size of photographs will be: (a) single column width (53 mm),
(b) double column width (110 mm), (c) full page width (170 mm). Photographs should ideally
be submitted at the final reproduction size based on the above figures.
Funding body agreements and policies: lsevier has established agreements and developed
policies to allow authors who publish in Elsevier journals to comply with potential manuscript
archiving requirements as specified as conditions of their grant awards. To learn more about
existing agreements and policies please visit http://www.elsevier.com/fundingbodies
Proofs: One set of page proofs in PDF format will be sent by e-mail to the corresponding
author, which they are requested to correct and return within 48 hours. Elsevier now sends
PDF proofs which can be annotated; for this you will need to download Adobe Reader
version 7 available free from http://www.adobe.com/products/acrobat/readstep2.html.
Instructions on how to annotate PDF files will accompany the proofs. The exact system
requirements are given at the Adobe site:
http://www.adobe.com/products/acrobat/acrrsystemreqs.html#70win. If you do not wish to
use the PDF annotations function, you may list the corrections (including replies to the Query
Form) and return to Elsevier in an e-mail. Please list your corrections quoting line number. If,
for any reason, this is not possible, then mark the corrections and any other comments
(including replies to the Query Form) on a printout of your proof and return by fax, or scan
the pages and e-mail, or by post.

96
Please use this proof only for checking the typesetting, editing, completeness and correctness
of the text, tables and figures. Significant changes to the article as accepted for publication will
only be considered at this stage with permission from the Editor. We will do everything
possible to get your article published quickly and accurately. Therefore, it is important to
ensure that all of your corrections are sent back to us in one communication: please check
carefully before replying, as inclusion of any subsequent corrections cannot be guaranteed.
Proofreading is solely your responsibility. Note that Elsevier may proceed with the publication
of your article if no response is received.
Offprints: The corresponding authorwill be provided , at no cost, with a PDF file of the article
via e-mail. The PDF file is a watermarked version of the published article and includes a cover
sheet with the journal cover image and a disclaimer outlining the terms and conditions of use.
Additional paper offprints can be ordered by the authors. An order form with prices will be
sent to the corresponding author.
Accepted Articles: For the facility to track accepted articles and set email alerts to inform you of
when an article's status has changed, visit: http://authors.elsevier.com/TrackPaper.html
There are also detailed artwork guidelines, copyright information, frequently asked questions
and more. Contact details for questions arising after acceptance of an article, especially those
related to proofs, are provided after registration of an article for publication.
Instructions for Letters to the Editor: The IJOMS welcomes Letters to the Editor. To facilitate
submission of the highest quality of Letters to the Editor, the following guidelines should be
followed:
1. Letters are meant to be focus pieces and, therefore, are limited to no more than 600 words,
6 references and a maximum of 2 figures. One reference should include a reference to the
IJOMS article being addressed.
2. It is recommended that you limit your letter to one or two important and critical points to
which you wish to provide a clear and precise discussion regarding the previously published
article.

97
3. One should support all assertion by peer review literature which should be a primary
research or large clinical studies rather than a case report.
4. Please include any financial disclosures at the end of the letter. This would include the
potential conflicts of interest not just related to the specific content of your letter but also the
content of the IJOMS article and other related areas.
5. Please recognize that letters that are essentially in agreement with the author's findings and
offer no additional insights provide little new information for publication. Likewise, letters that
highlight the writer's own research or are otherwise self-promotional will receive a low
publication priority.
6. There may be a need for additional editing. Should editing be required the letter will be
sent back to the author for final approval of the edited version.
7. It is important to use civil and professional discourse. It is not advisable that one adopt a
tone that may be misconstrued to be in anyway insulting.
8. Finally, it is not advisable to provide a letter that is anecdotal. While personal experiences
can have great value in patient care, it is generally not strong evidence to be placed in a letter
to the editor.

98
Catalogação na Publicação (CIP) Serviço Técnico de Biblioteca e Documentação – FOA / UNESP
Ferreira, Sabrina. F273e Copolímero PLA/PGA como substituto ósseo em levantamento de seio maxilar. Estudo histológico, histométrico e imunoistoquímico em coelhos / Sabrina Ferreira. - Araçatuba : [s.n.], 2014 31 f. : il. ; tab. + 1 CD-ROM Dissertação (Mestrado) – Universidade Estadual Paulista, Faculdade de Odontologia de Araçatuba Orientador: Prof. Idelmo Rangel Garcia Júnior 1. Ácido Polilático 2. Ácido Poliglicólico 3. Seio Maxilar 4. Imunoistoquímica Black D7 CDD 617.64