Embed Size (px)
Citation preview

www.apa.org/international/pi
Psychology International ◦ JUNE 2015
Psychology and Mental Health Services in the United Arab Emirates By Fa ma Al‐Darmaki, PhD, and Saad Ibrahim Yaaqeib
CONTENTS
COVER: Psychology and Mental Health Services in the United Arab Emirates
COLLABORATE! Moving Towards a New Relationship with Latin American Psychology ………….....….…...5
Senior Director’s Column………………………….14
UN MATTERS.………..…….….11
Global Mental Health: Tracking and Trekking Across Sectors …16
Selected Review from PsycCRITIQUES ......................20
Recently Published .................................23
ANNOUNCEMENTS ................24
Volume 26, Number 2, June 2015
For an online version, visit: www.apa.org/international/pi
NEWS AND UPDATES FROM THE AMERICAN PSYCHOLOGICAL ASSOCIATION OFFICE OF INTERNATIONAL AFFAIRS | JUNE. 2015
APA Office of International Affairs
PSYCHOLOGY INTERNATIONAL
The United Arab Emirates (UAE) is ranked 21st in world popula on growth, with an increase of 2.71% annually (Central Intelligence Agency World Factbook, 2014). Despite the popula on boom, there are concerns that mental health services and the general field of psychology have not matched the country’s expansion, with a resul ng increase in the level of unmet need (Saberi, 2010; 7Days, 2013; The Na onal, 2014; Al‐Sayed, 2010). The expected growth in demand for psychological treatment in the Gulf Coopera on Council (GCC) countries is 241% (Mourshid, Hediger & Lambert, 2006). This ar cle discusses various aspects of psychological prac ce and Mental health services in the UAE. The Federal Government’s Ministry of Health (MOH) is the official body that manages healthcare legisla on in the country. However, two other semi‐governmental bodies, the Health Authority Abu Dhabi (HAAD) and Dubai Health Authority (DHA) have regulate their respec ve emirates. Currently an independent mental health policy does not exist, but a mental health plan is included in the general health policy (WHO, 2011). The mental health plan was revised in 2010 with emphasis on broader availability of mental health services in the government facili es across the country. There is a shi towards integra ng mental health services into primary care, and alloca ng more resources to smaller community mental health facili es. Data on governmental mental health facili es indicate that there are 3 outpa ent facili es and only one mental hospital (WHO, 2011). There are 25 beds reserved for psychiatric pa ents in the general hospitals, and 80 beds available in the specialized mental hospitals. The rate of mental health professionals per 100,000 is as follows: 0.3 psychiatrists, 0.51 psychologists, 0.25 social workers, 0.04 occupa onal therapists, and 0.04 other health workers. The data on the number of counselors is unavailable. These numbers indicate an extreme shortage of mental health professionals and facili es in the UAE. Recent reports indicate that there are approximately 33,000 mental pa ents in the country, and new admissions to public facili es are put on wai ng lists that can go up to two months (Abed, 2014).

2 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
The field of psychology in UAE began in the 1970s with the establishment of an undergraduate program in psychology in the United Arab Emirates University. The prac ce of providing psychological services such as counseling and psychotherapy remains loosely regulated by the authori es. Several prac oners and academics have voiced out their concerns and expressed a dire need for a mental health act (Alshihabi, 2011; Badawi, 2012; Rizvi & Bell, 2014). The lack of enforced rules of prac ce enabled ‘bogus’ psychologists and mental health workers that exploit legal loopholes to operate in the UAE’s market (Bell, 2014). A panel of professionals from Dubai Health Authority (DHA), Ministry of Health (MOH), Emirates Psychological Associa on and other ins tutes are currently working on regula on guidelines for prac ce of psychology (UAE Psychologist, 2012). Despite the on‐going efforts to establish a regulatory body for the professions of psychology in the UAE, there are s ll a number of challenges hindering progress in this issue. For instance, licensing procedures are going to be different from one emirate to another depending on the local authority’s exis ng guidelines and willingness to get involved (Al‐Maseeh, 2013). The licensing source (federal vs local) will affect the scope of prac ce of professionals. Finally, current legisla ve efforts are directed toward psychiatry and clinical psychology, with no considera on of other psychological professions such as counseling or school psychology. Presently, licensure is obtained from governmental health en es such as the Abu Dhabi Health Authority (HAAD), DHA, and MOH. For counselors, Dubai Community Development Authority provides licensing. The licensure can be obtained with a master level educa on or even with undergraduate degree and few years of experience. The Emirates Psychological Associa on (EPA) was established in 2003 in Dubai by the Ministry of Social Affairs (Kruse, 2011). It is the only officially recognized professional associa on for psychologists in the UAE. EPA’s mission is to raise awareness of mental health issues in the Emirates and to advocate for the public’s access to mental health services. Another mission of EPA is to serve as a liaison between governmental departments and private sectors to be er serve the community. Training psychologists in UAE is very challenging. Most of the Emira s who provide psychological services in schools and in the community mental health agencies have minimal training in applied psychology. The only well‐established public undergraduate program available is in the United Arab Emirates University (UAEU) which is restricted to local students and a very limited number of interna onal students. This is due to the fact that UAEU is a federal ins tu on funded by the government. Similarly, Zayed University (ZU), another federal ins tu on, recently began offering a program in psychology as a major. Expatriate students seeking training in psychology have to enroll in private universi es like Middlesex University Dubai and Herio‐Wa University Dubai that also offer undergraduate programs in psychology. Other universi es like New York University Abu Dhabi, American University in Sharjah offer minors in psychology or hybrid majors involving psychology (Crookes, 2012). At the graduate level, only one clinical psychology masters (MSc) program exists, which was recently introduced in UAEU (Haque, 2011). It is open to both UAE na onals and non‐na onals. However, the clinical program has several challenges like finding adequate internships for students and sufficient resources (culturally relevant textbooks, bilingual faculty) and well‐trained supervisors. The majority of psychologists currently in the UAE have undergone a Western model of training. Despite the global concerns of the limited applicability of Western psychological principles over developing world popula ons, the psychology of the ‘First’ and ‘Second’ worlds is s ll being exported to ‘Third’ worlds with li le a en on to the validity or appropriateness of what is being exported to ethnically diverse popula ons (Moghaddam & Taylor, 1986; Marsella, 2011). Local scholars have expressed their concerns about the compa bility of Western therapeu c models with the UAE’s culture and values (Al‐Darmaki & Sayed, 2009). To address this challenge, an indigenous movement in psychology has been ini ated interna onally (Bhawk, 2011, Hwang, 2005). Prac oners and researchers par cipa ng in the movement adopt psychological treatment models that were developed in a bo om‐up fashion, rather than being adapted or tweaked from foreign models. Scholars in several developing countries around the world like Mexico, Philippines, Taiwan, India, and others have endorsed the indigenous psychology approach (Diaz‐Guerrero, 1977; Enriquez, 1977; Sinha, 1998; Yang, 1997). It is difficult to bridge the UAE’s psychology field into the indigenous movement. Current
(Con nued on page 3)

www.apa.org/international/pi 3
Psychology International ◦ JUNE 2015
professionals are overwhelmed with mee ng the psychosocial needs in the country and barely have any me for research. Therefore, there is an on‐going reliance on Western frameworks in providing mental healthcare and educa on. Mental health is a considerably neglected area of research in the UAE. However, the lack of a en on to mental health research is a regional phenomenon affec ng all of the Gulf Coopera on Council (GCC) countries. Between 1989 and 2008, only 192 studies on mental health were published in the GCC countries. Among these countries, the UAE is the most prolific (Osman & Afifi, 2010). The available studies indicate a high prevalence of psychosoma c disorders, depressive disorders, and anxiety disorders (Ghubash, Hamdi & Bebbington, 1992; Abou‐Saleh, Ghubash & Daradkeh, 2001; Daradkeh, Eapen & Ghubash, 2005) among primary health care a enders. Among the local geriatric popula on, the dominant mental disorders were depression, anxiety and hypochondriasis (Ghubash et al., 2004). One of the main challenges to providing psychological care in the UAE is the social s gma associated with the u liza on of psychological services (Al‐Darmaki, Hassane, Ahammed & Abdulla, 2012; Al‐Darmaki & Sayed, 2009; Eapen & Ghubash, 2004; Almazroui, 2014). Researchers who are interested in conduc ng research within the field of psychology are mainly academicians whose mo va on o en mes for conduc ng research is to get promoted. Most of those researchers are non‐Emira s who may not be culturally aware of issues that should be inves gated. Thus, their research ac vi es may not relate directly to need of the country. In addi on, this research is usually published in English and in interna onal journals and therefore of limited use for prac oners in the UAE. Even though some milestones have been made in the development of the psychology field in the UAE, it is s ll in its ini al phase. The lack of coordina on between higher educa on ins tu ons and health public sectors will keep a shortage of mental health professionals, forcing the government to import exper se to meet the rising demand for psychotherapy in the UAE. It is essen al to establish robust training programs in applied psychology (e.g., clinical, counseling psychology). It has to be made into a na onal priority in order for the major educa onal ins tutes (e.g. UAEU, ZU) to collaborate in mee ng the shortage of local professionals. The authori es have to place and enforce guidelines regula ng the prac ce of psychology, to protect the integrity of the profession and prevent harming clients. Providing ins tu onal support (financial and non‐financial) for local researchers will facilitate the development of indigenous therapeu c models. References Abed, A. (2014, November 12). 33 thousand mental pa ents suffering from shortage of psychotherapists. Emarat AlYoum. Retrieved on February 3, 2015, from h p://www.emaratalyoum.com/local‐sec on/other/2014‐11‐12‐1.727351 [In Arabic] Abou‐Saleh, M. T., Ghubash, R., & Daradkeh, T. K. (2001). Al Ain community psychiatric survey. I. Prevalence and socio‐demographic correlates. Social psychiatry and psychiatric epidemiology, 36(1), 20‐28. Almazroui, A. (2014, January 25). While the s gma persists, so too will mental health issues. The Na onal. Retrieved on February 3, 2015, from h p://www.thena onal.ae/thena onalconversa on/comment/while‐the‐s gma‐persists‐so‐too‐will‐mental‐health‐issues AlShihabi, R. (2011). Licensing needs for psychologists in Abu Dhabi. The UAE Psychologist. 1(2), 4. Al‐Darmaki, F., & Sayed, M. A. (2009). Counseling challenges within the cultural context of the United Arab Emirates. Interna onal handbook of cross‐cultural counseling: Cultural assump ons and prac ces worldwide, 465‐474. Al‐Darmaki, F. R., Hassane, S., Ahammed, S., & Abdullah, A. S. (2012). Developing counselor educa on iden ty in UAE: Evalua on of an undergraduate program. Journal for Interna onal Counselor Educa on, 4(1), 1. Al‐Maseeh, H. (2013). Licensing psychology – no closer to a unified system? The UAE Psychologist. 2 (2), 5. Al‐Sayed, T. (2010, December 21). The UAE suffers from extreme deficiency in mental health facili es. Elaf. Retrieved on February 3, 2015, from h p://www.elaph.com/Web/news/2010/12/619159.html [In Arabic] Badawi, I. (2012). The role of psychologists in promo ng mental health in the UAE. The UAE Psychologist. 1(2), 12‐13. Bhawuk, D. P. (2011). Toward a new paradigm of psychology. In Spirituality and Indian Psychology (pp. 185‐202). Springer New York Central Intelligence Agency. (2014). The world factbook: UAE. Retrieved on February 3, 2015, from h ps://www.cia.gov/library/publica ons/the‐world‐factbook/geos/print/country/countrypdf_ae.pdf Crookes, A. (2012). Psychology educa on in the UAE. The UAE Psychologist. 1(2), 22‐23. Daradkeh, T. K., Eapen, V., & Ghubash, R. (2005). Mental morbidity in primary care in Al Ain (UAE): Applica on of the Arabic transla on of the PRIME‐MD (PHQ) Version. German Journal of Psychiatry, 8(3), 32‐35. 7Days. (2013, April 2013). Experts call for more mental health experts in the UAE. 7days. Retrieved from h p://7daysindubai.com/news‐14031/ Díaz‐Guerrero, R. (1977). A Mexican psychology. American Psychologist, 32(11), 934. Eapen, V., & Ghubash, R. (2004). Mental health problems in children and help seeking pa erns in the UAE. Psychological Reports, 94, 663‐667. Enriquez, V. G. (1977). Filipino psychology in the Third World. Philippine Journal of Psychology, 10(1), 3‐18
4 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
International Council of Psychologists (ICP) 74th Annual Convention in Toronto, Canada
August 1-3, 2015 Web: http://www.icpweb.org/#!events/c226e
Theme: Psychological Contributions to Solving Global Problems
in the 21st Century.
Registration Deadline: July 10, 2015
Ghubash, R., Hamdi, E., & Bebbington, P. (1992). The Dubai community psychiatric survey: I. Prevalence and socio‐demographic correlates. Social psychiatry and psychiatric epidemiology, 27(2), 53‐61. Ghubash, R., El‐Rufaie, O., Zoubeidi, T., Al‐Shboul, Q. M., & Sabri, S. M. (2004). Profile of mental disorders among the elderly United Arab Emirates popula on: sociodemographic correlates. Interna onal journal of geriatric psychiatry, 19(4), 344‐351. Haque, A. (2011). Masters of science in clinical psychology (MSc). The UAE Psychologist. 1(2), 15. Hwang, K. K. (2005). The indigenous movement. The Psychologist, 18(1), 80‐83. Kruse, M. (2011). Emirates psychological associa on: A brief introduc on. The UAE Psychologist. 1(2), 6. Marsella, A. (2011). Twelve cri cal issues for mental health professionals working with ethno‐culturally diverse popula ons. Psychology interna onal. Retrieved 18 February from h p://www.apa.org/interna onal/pi/2011/10/cri cal‐issues.aspx Moghaddam, F. M., & Taylor, D. M. (1986). What cons tutes an ‘appropriate psychology’ for the developing world? Interna onal Journal of Psychology, 21(1‐4), 253‐267. Mourshed M., Hediger V., Lambert T. (2006) Gulf Coopera on Council Health Care: Challenges and Opportuni es. Chapter 2.1. Retrieved from h p://www.weforum.org/pdf/Global_Compe veness_Reports/Reports/chapters/2_1.pdf Osman, O. T., & Afifi, M. (2010). Troubled minds in the Gulf: mental health research in the United Arab Emirates (1989‐2008). Asia‐Pacific Journal of Public Health, 22(3 suppl), 48S‐53S. Rizvi, J. & Bell, J., (2014, October 23). Mental health act needed in UAE. The Na onal. Retrieved on February 3, 2015, from h p://www.gncdubai.com/mental‐health‐act‐needed‐uae‐na onal/ Saberi, M. (2010, December 18). Gulf news: Mental illness is on the rise in UAE. Gulf News Sinha, D. (1998). Changing perspec ves in social psychology in India: A journey towards indigeniza on. Asian Journal of Social Psychology, 1(1), 17‐31. The Na onal. (2014, November 12). UAE lacking in mental health services. The Na onal. UAE Psychologist. (2012). Governing the prac ce of psychology. The UAE Psychologist. 1(2), 8‐9. World Health Organiza on (2011). Mental Health Atlas Country Profiles. Retrieved on February, 3, 2015 from h p://www.who.int/mental_health/evidence/atlas/profiles/are_mh_profile.pdf Yang, K. S. (1997). Indigenizing Westernized Chinese psychology. In M. H. Bond, Working at the interface of cultures: Eighteen lives in social
science (pp. 63‐76). London, New York: Routledge.Ψ
APA-MOU Travel Grant to Columbia or Mexico Web: http://www.apa.org/about/awards/mou-travel-grant.aspx
APA’s MOU travel grant program is designed to promote collaboration and
exchange among U.S.-based APA members and APAGS members with
members of those national psychology associations with which APA has a
formal agreement (Memorandum of Understanding).
Deadline: June 30, 2015
www.apa.org/international/pi 5
Psychology International ◦ JUNE 2015
Moving Towards a New Relationship with Latin American Psychology
By Héctor Torres, PsyD and Andrés Consoli, PhD
Much of the scientific literature produced in the U.S. has been narrowly focused on its own geographical location (Arnett, 2008). Increasing a global perspective within that scientific literature can benefit it in many ways, including providing readers with a more adequate representation of humanity given that the majority of the world population’s living conditions are significantly different from those in the U.S. (Arnett, 2008). There are many other reasons why a more global perspective would benefit U.S. publications, particularly the inclusion of knowledge about developments and perspectives from our neighbors in Latin America and the Caribbean. For instance, there are multiple issues that have no borders and impact all countries in the Americas such as poverty, immigration, violence, drugs and human trafficking, transnational families, and gun control. Addressing these topics jointly can contribute to a psychology that is better equipped to reddress such complex issues. By learning about Latin American psychology and its perspective on these and other issues, we can tap into a great potential for mutual learning and collaborating. This article features a brief overview of Latin American psychology including some of its general characteristics and a few of the existing sources of dissemination of academic information. In addition, we share examples of recent efforts by the National Psychological Association (NLPA) and their members to engage with Latin American Psychology. Finally, the article concludes with a call for efforts to better inform U.S. psychology about Latin American psychology. Overview of Latin American Psychology Latin American psychology’s history is relatively short, yet there is clear evidence of its promising future (Benito, 2012). Given that a detailed account of the history of Latin American psychology is out of the scope of this article, for an in depth account of the history we recommend reading the work of a several authors whom have published on this subject matter (ei. Alarcon, 2004; Ardilla, 2004; Benito, 2012; Consoli & Morgan Consoli, 2012; Consoli, Morgan Consoli, & Klappenbach, 2013; Klappenbach & Pavesi, 1994; Montero & Blanco, 1992; Salas, 2014; Sosa & Valderrama‐Iturbe, 2001). Two important milestones in the development of a Latin American psychology are the formation of professional training starting approximately in 1947 and the establishment of professional organizations for Latin America as a region (Ardila, 2004). Founded in 1951 in Mexico City, the Interamerican Society of Psychology (Sociedad Interamericana de Psicología, SIP) was the first regional psychology organization. SIP, one of the most important psychology organizations in Latin America, continues to promote the development of Latin American psychology by connecting the Caribbean, North, Central, and South America through congresses, publications, awards, and workgroups. Latin American psychology has been prolific in the production and dissemination of its own academic work. Along with the Interamerican Journal of Psychology other important publications include Advances in Latin
(Con nued on page 6)
COLLABORATEE

6 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
American Psychology, Revista Latinoamericana de Psicología, Panamerican Journal of Psychology, Psychology for Latin America, and Latin American Journal of Psychological Science (Benito, 2012). Characteristics of Latin American Psychology Latin American psychology has its roots in European and North American psychology, however it has evolved as an independent scientific perspective where social relevance, contextual realities, and indigenous knowledge figure prominently. Alarcón (2004) and Ardila (2004) described general characteristics and trends of Latin American psychology as they reviewed its development. Based on these two reviews we can describe Latin America psychology’s particularities through the following six characteristics: 1. A reliance on North American and European psychology in the early years that resulted in limited original work and an emphasis on the translation and adaptation of psychometric tools; 2. An initial focus on empirical, objective, and quantitative knowledge that has evolved over time and now encompasses a broad range of interests and methodology; 3. A clear interest in humans as the main subjects of study over animal studies; 4. A preference for pragmatism and works that seek solution to concrete problems; 5. A focus on socially relevant psychology that addressed contextual realities of Latin America; and 6. An emphasis on a psychology that leads to social action. Although in its beginnings Latin American Psychology relied on European and North American psychology’s hegemony, since the 1960’s original Latin American theories and paradigms have surfaced, original work has increased, and there has been a gradual convergence towards a supranational Latin American psychology community, which continues today (Salas, 2014). Moreover, Latin American psychology has been influenced by the socio‐political realities of the region, including state oppression, and the advances contributed by prominent figures such as Paulo Freire in the context of his pedagogy of the oppressed and the conscientization processes (Burton, & Kagan, 2005). Liberation Psychology is a great example of Latin American psychology that is centered on the specific social realities of Latin America and involves a call for action, asking psychologists to engage in changing conditions of social injustice among the underprivileged masses (Martín‐Baró, Aron, & Corne, 1994). Other examples of novel Latin American paradigms include Díaz‐Guerrero’s ethnopsychology and the historic bio‐psychosocial model of human behavior (1972) as well as Ardila’s experimental synthesis of behavior (2006). Similarly, the work of Maritza Montero (2004) and Irma Serrano García (Serrano‐García, López, & Rivera‐Medina, l987) on social community psychology in Latin America and the Caribbean are excellent examples of the commitment among many professionals in the region to redress the challenging social circumstances experienced by the masses. In terms of the areas of scholarly interest, the most prevalent areas in Latin American research included psychometrics and evaluation, social and transcultural psychology, experimental understanding of human behavior, political psychology, cognitive psychology, social community psychology, and psychodynamic approaches, including psychoanalysis (Alarcón, 2004; Ardila, 2004). A recent EBSCO database search conducted by the authors of this article explored if these themes continue to be the most popular and consistent during the present time. The search looked for the key terms: Latin American psychology, and other similar terms such as “Global” and “Hispanic.” We sought for articles generated by Latin American authors whose sample was based in Latin America. We found that overall the before mentioned interests continue to be present, while other new areas of interest have surfaced including health and organizational psychology. Recent Efforts by NLPA The U.S. based National Latina/o Psychological Association (NLPA) strives to advance psychological education and training, scientific practice and organizational change to enhance the overall well‐being of Latina/o populations. In an effort to support a global perspective in his role as 2014 NLPA president the second author
www.apa.org/international/pi 7
Psychology International ◦ JUNE 2015
of this article established the initiative titled “Understanding Latina/o identities across borders through international engagement,”that was implemented by the first author. By bringing awareness to topics beyond U.S. borders the initiative intended to contribute to social transformation affirming human rights and dignity. The three main ventures of this initiative included: First, 2014’s NLPA biennial conference theme was “DREAMers, Immigration, & Social Justice: Advancing a Global Latina/o Psychology Agenda.” Attended by more than 400 members this conference provided opportunities for the exchange of scholarship, advocacy, and learning around this topic. Second, we worked on the initiation of collaborative efforts with other organizations such as the SIP. Lastly, we created an International Special Interest Group that will continue developing efforts in this area. In addition, NLPA’s members have independently engaged in teaching, research, consulting, and service‐related activities in multiple Latin American countries. A short list of recent collaborative efforts include: 1. Jiménez, Vazquez‐Rivera, Platt, and Esteban conducted a study exploring knowledge and attitudes towards gay and lesbians among Spanish speaking psychologists and students in Mexico City; 2. Barrera, Kelman, and Muñoz conducted an RCT on the prevention of postpartum depression among a sample that included more than 10 Latin American countries; 3. Toro‐Alfonso and Urzúa conducted a mixed method study exploring quality of life, mood, social support among gays and lesbians over 60 years old in Puerto Rico and Chile; 4. Fuentes, Paredes, Cobar Catalán de Coma, and Grazioso conducted a training in Guatemala on the ACT Raising Safe Kids program, an early violence prevention program housed in the Violence Prevention Office of the American Psychological Association; 5. Hass collaborated with James Butcher to provide an MMPI‐2 training in Costa Rica; 6. Camacho Valladares and Armas presented at the 2014 LBHI conference on the cultural and psychological resilience of young Mexican women in Ciudad Juarez, Mexico; 7. Puente conducted a Fulbright in Argentina and lecture in 13 different countries; and 7. Domenech Rodríguez, received an NIH’s Fogarty International Center training grant, collaborated on an RCT to test the efficacy of Parent Management Training, and conducted a research on parenting in Puerto Rican families.
Conclusion To understand the value of the current movement in which we are immersed, we must critically look at the past and employ that knowledge to further develop and strengthen the future (Salas, 2014). As Latin American psychology continues to evolve, we wonder what its relation will be to North American Psychology and vice versa. Provided that this relation can be mutually beneficial, efforts in bridging the gap in communication and increasing the awareness of Latin American psychology in the U.S. could lead to important dialogues and perhaps novel collaborative solutions. Specifically, U.S. trained psychologist as well as psychologists‐in‐training could benefit from an appreciation of the novel solutions developed by Latin American psychologists in the context of Liberation Psychology and Social Community Psychology. Moreover, to redress the crisis of limited internships in the U.S. and to facilitate the development of bilingual, culturally competent practitioners and academics a closer relationship with Latin America seems in order.
References
Alarcón, R. (2004). Medio siglo de psicología latinoamericana: Una visión de conjunto. Revista Interamericana de psicología, 38(2), 307‐316.
Ardila, R. (2004). La psicología latinoamericana: El primer medio. Revista Interamericana de Psicología, 38, 317‐322.
Ardila, R. (2006). The experimental synthesis of behaviour. International Journal of Psychology, 41, 462‐467.
Arnett, J. J. (2008). The neglected 95%: Why American psychology needs to become less American. American Psychologist, 63(7), 602‐614. http://dx.doi.org/10.1037/0003‐066X.63.7.602
Benito, E. (2012). Psychological Science in Latin America: Roots, Trends and Challenges. Observer Vol.25, No.4.
Burton, M., & Kagan, C. (2005). Liberation social psychology: Learning from Latin America. Journal of Community and Applied Social Psychology, 15, 63‐78.
(Con nued on page 8)
8 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
Consoli, A. J., & Morgan Consoli, M. L. (2012). Psychology in Latin America: Legacies and contributions ‐ Part 1. International Psychology Bulletin, 16 (3), 71‐74.
Consoli, A. J., Morgan Consoli, M. L., & Klappenbach, H. (2013). Psychology in Latin America: Legacies and contributions ‐ Part 2. International Psychology Bulletin, 17 (2), 36‐41.
Díaz‐Guerrero, R. (1972). Hacia una teoría histórico‐bio‐psico‐socio‐cultural del comportamiento humano. Ciudad de México, México: Trillas.
Klappenbach, H. & Pavesi, P. (1994). Una historia de la psicología en Latinoamérica. Revista Latinoamericana de Psicología, 26, 445‐482.
Martín‐Baró, I., Aron, A., & Corne, S. (Eds.). (1994). Writings for a liberation psychology. Harvard University Press.
Montero, M. (2004). Relaciones entre psicología social comunitaria, psicología crítica y psicología de la liberación: Una respuesta latinoamericana [Relations between community‐social psychology, critical‐social psychology, and social psychology of liberation: A Latin American answer]. Psykhe, 13 (2), 17‐28.
Montero, M., & Blanco, A. (1992). La psicología social en el ámbito iberoamericano. En Libro de ponencias (pp.162‐169). Madrid, España:Congreso Iberoamericano de Psicología
Salas, G. (Ed.) (2014). Historias de psicología en América del Sur: Diálogo y perspectivas.Chile: Nueva Mirada Ediciones.
Serrano‐García, I., López, M. M., & Rivera‐Medina, E. (l987). Towards a social‐community psychology. Journal of Community Psychology. 15, 431‐446.
Sosa, J. J. S., & Valderrama‐Iturbe, P. (2001). Psychology in Latin America: Historical reflections and perspectives. International Journal of Psychology, 36(6), 384‐394.
Vilanova, A., & Di Doménico, C. (1999). La psicología en el cono sur. Datos para una historia. Mar del Plata, Argentina: Universidad Nacional de Mar del Plata.
About the authors: Héctor Torres, PsyD, in an Associate Professor in the Counseling Department at The Chicago School of Professional Psychology. Andrés Consoli, PhD, is an Associate Professor in the Department of Counseling, Clinical, & School Psychology, Gevirtz Graduate School of Education, at the University of California Santa Barbara). Correspondence regarding this article should be address to Héctor Torres at [email protected].Ψ
FOLLOW OUR OFFICE ON TWITTER!!!
@APA_Intl
www.apa.org/international/pi 9
Psychology International ◦ JUNE 2015
The recent earthquakes in Nepal underscore the fragility of human systems in the face of nature – and the importance of prepara on and recovery efforts for natural or other disasters. When disasters strike in the United States, APA has a well‐developed response system of psychologists who have been trained in disaster prepara on, and disaster
response and recovery. The APA Disaster Response Network (DRN) was developed at the na onal level but it is organized and coordinated at the state level. Each DRN member receives Red Cross Disaster Mental Health training and works through the Red Cross. How does this work for interna onal disasters? The DRN does extend to Canada where it works primarily through provincial ministries of health, or with provincial Red Cross chapters. However, this model has not been extended beyond the United States and Canada. What is the role of U.S. psychologists in response to interna onal disasters? When the APA’s Commi ee on Interna onal Rela ons in Psychology (CIRP) considered this ques on almost a decade ago, following the Indian Ocean tsunami, there was lively discussion about whether and how U.S. psychologists, who might not know the language, culture or local context of those affected by disasters, could nonetheless provide effec ve contribu ons. CIRP’s response, formulated in the “APA Statement on
the Role of Psychologists in Interna onal Emergencies” (h p://www.apa.org/interna onal/resources/info/emergency‐statement.aspx) was that with few excep ons, psychologists should primarily work in consul ng or training roles under the auspices of established humanitarian organiza ons with local experience and exper se. The statement cau oned U.S. psychologists against travelling to a disaster‐affected country unless they were invited, experienced, worked from a public health or community perspec ve, and were prepared to provide program support, not direct interven ons. The statement also cau oned psychologists to know about and follow interna onally‐developed guidelines and standards for disaster relief. This statement, and the reasoning behind it, have formed the basis of APA’s procedures for responding to interna onal emergencies. These procedures, adopted in 2010, call on APA to first provide online support and available resources to local psychology organiza ons or other relevant bodies, and then, for major interna onal disasters, to consider developing a plan for contribu ng to long‐term psychosocial recovery efforts. Partners would include the local, na onal psychology associa on if one exists (there is some organized psychology in most countries in the world), as well as interna onal or na onal NGOs or agencies (such as the Red Cross / Red Crescent Socie es). The goal would be to develop training and materials to build a sustained psychosocial recovery process. The goal of any such support would be to contribute to the sustainable development of resources in the affected area, in par cular suppor ng the launch and establishment of psychology organiza ons. Effec vely engaging with interna onal colleagues? CIRP is also approaching how to provide guidance to U.S. psychologists from an educa onal perspec ve. The commi ee has
(Con nued on page 10)
SENIOR DIRECTOR’S COLUMN
How can U.S. Psychology navigate responding to
interna onal disasters? By Merry Bullock, PhD
10 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
developed two brochures in a series “Going Interna onal: A Prac cal Guide for Psychologists” on academic exchange and developing interna onal collabora ve research. They have also developed a dra resolu on on the need for APA and U.S. psychologists to recognize and explore the variety of world‐views affec ng how psychological phenomena are defined, studied and explained around the world, and to understand that the lens of U.S. psychology is not the only lens for psychological science and prac ce. Last, they are currently developing guidelines for “Interna onal Competencies” – knowledge, skills and a tudes that any U. S. psychologist who wants to work interna onally should adopt. Underlying the brochures, resolu on and guidelines is a deep commitment to respec ng and valuing the many approaches to psychology found in the U.S. and around the world.
These resources provide useful background for considering how U.S. psychologists can response to interna onal disasters from a longer term perspec ve. And it is this longer term perspec ve that is important to support. Those who work at the frontline in disaster relief consistently note all too frequently that immediate disaster relief, including psychological first aid, is not followed by sustained a en on to medium or long term psychosocial recovery. Taking a broader, systemic approach, psychologists can contribute to sustainable recovery through research on disaster response, recovery and prepara on, and through lending their exper se to training and educa onal efforts, and through suppor ng the development of local psychological organiza ons. Ψ
Call for Submissions: 3rd Caribbean Regional Conference of Psychology
Port au Prince, Haïti November 7-11, 2016
Web: www.crcp2016.org
Theme: Promoting Caribbean Health with Multiculturalism and
Multilingualism: Challenges and Opportunities.
Early Submission Deadline: September 15, 2015
Free Publication Access: Routledge Journals offers FREE ACCESS to a collection of
over 55 articles on the topic of Diversity & Cultural Psychiatry. You can now view and download each of these
articles for FREE for a limited time. Web: http://explore.tandfonline.com/page/beh/diversity-cultural-
psychiatry-free-article-collection.
Expires: July 31, 2015
www.apa.org/international/pi 11
Psychology International ◦ JUNE 2015
Delegates at the United Na ons (UN) commemorated World Au sm Awareness Day on April 2, which is also commemorated globally on this date. World Au sm Awareness Day was established by the UN General Assembly (A/RES/62/139) on December 18, 2007. Members of the UN General Assembly expressed deep concern regarding the prevalence rates of Au sm throughout the world and the need to address the long term outcomes for children, families, and communi es. The resolu on declared that star ng April 2, 2008, and on this date each year, representa ves of the UN and non‐governmental organiza ons (NGOs) would raise awareness about Au sm throughout the world as well as address the fundamental human rights of persons with Au sm (UN General Assembly, 2007).
In cra ing Resolu on 62/139, members of the UN General Assembly acknowledged the Conven on on the Rights of the Child (UN Human Rights, 1989) and the Conven on on the Rights of Persons with Disabili es (UN Enable, 2006), which guarantee rights and freedoms to (1) live in dignity, (2) live a full life in the community as other children do, and (3) be self‐reliant economically in adulthood. In upholding these rights, the resolu on calls on representa ves of Member States, associated organiza ons (e.g., WHO), and NGOs to encourage early diagnosis, research, and treatment interven ons in order to enhance the growth and development of the individual.
This year’s theme was “Employment: The Au sm Advantage.” This theme captures the poten al for persons with Au sm to
make significant contribu ons in the work place, given their unique individual strengths, which might not be “neurotypical.” These valuable skills might consist of an enhanced capacity to a end to details or perform quick and accurate complex calcula ons. Such a focus on poten al contribu ons to the work place is intended to counter the challenges of widespread discrimina on in the work place as well as limited voca onal training and job opportuni es for those diagnosed with Au sm. A UN report es mates that 80% of adults with Au sm are unemployed (World Au sm Awareness Day, 2015).
From Au sm to Au sm Spectrum Disorder The clinical term for Au sm is Au sm Spectrum Disorder (ASD). People with ASD are described by the DSM‐5 Neurodevelopmental Work Group (APA, 2013) as having a tendency “to have communica on deficits, such as responding inappropriately in conversa ons, misreading nonverbal interac ons, or having difficulty building friendships appropriate to their age. In addi on, people with ASD may be overly dependent on rou nes, highly sensi ve to changes in their environment, or intensely focused on inappropriate items. Again, the symptoms of people with ASD will fall on a con nuum, with some individuals showing mild symptoms and others having much more severe symptoms…. Under the DSM‐5 criteria, individuals with ASD must show symptoms from early childhood, even if those symptoms are not recognized un l later. This criteria change encourages earlier diagnosis of ASD but also allows people whose symptoms may not be fully recognized un l social demands exceed their capacity to receive the diagnosis” (p. 1).
Global Challenges Researchers (e.g., Malcolm‐Smith, Hoogenhout, Ing, Thomas, & de Vries, 2013; Wallace, Fein, Rosanoff, Dawson, Hossain, Brennan, Como, & Shih, 2012) report global awareness about ASD has increased drama cally during the past decade, especially
(Con nued on page 12)
UN MATTERS
Global Awareness of Au sm Spectrum Disorder: Impact and Interven ons
By Juneau Gary and Neal S. Rubin, APA Representa ves at the UN Department of Public Informa on, Column Co‐Editors

12 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
in low and middle income countries (LMIC). Prac oners in LMICs have only recently begun to recognize and treat ASD, considered a common developmental disorder in high income countries (HICs) (e.g., North America and Western Europe). Although global prevalence es mates for ASD are difficult to ascertain because of limited interna onal epidemiological studies, ASD is most likely under‐diagnosed in parts of the world, with individuals going undetected and without treatment, according to Wallace et al. The common sta s c used by researchers to es mate the prevalence of ASD globally is approximately one percent of the popula on worldwide (Malcolm‐Smith et al.; Wallace et al.; Schendel et al., 2013).
The challenge of early detec on and early interven on of ASD is exacerbated by limited exper se, including limited diagnos c and treatment resources in LMICs. For instance, in So. Africa, interven on services and specialized schools are insufficient and overwhelmed; mul ‐lingual standardized assessment tools are limited; and exper se across health care, mental health, social service, and educa onal systems is limited (Malcolm‐Smith et al., 2013). In some LMICs, parents may experience a social s gma for having a child with ASD (or other disability or mental illness). Parents may also encounter barriers to employment or may experience increased levels of parental stress (Wallace et al.). In China, for instance, researchers have reported the parental stress in fathers whose children have been diagnosed with ASD, as using coping mechanisms such as limi ng their father‐child interac ons, reducing their child care responsibili es, and having a tendency to abuse substances (Wang, Michaels, & Day, 2011; McCabe, 2008). Finally, in other LMICs, structural and prac cal barriers (e.g., limited government commitment and local resources, over‐centralized health systems, failure to integrate mental health services into primary health care, limited professional training, and limited local exper se) thwart early and effec ve diagnosis and treatment (Wallace et al.). For these reasons, and others, ASD is o en diagnosed late or undiagnosed in parts of the world.
When ASD is diagnosed, psychoac ve medica ons are commonly prescribed for a en on deficits, aggression, and/or anxiety in countries without access to non‐pharmacological interven ons (Malcolm‐Smith et al., 2013). Medica on is usually administered from childhood through adulthood and the cost of specialized medica ons, over the span of one’s life me, can be financially debilita ng, especially for parents in LMICs (Malcolm‐Smith et al.).
The impact of cultural influences on the presenta on, development, interpreta on, and diagnosis of ASD is seldom inves gated (Chung et al., 2012; Matson, Mahan, Hess, Fodstad, & Neal, 2010). Research is sugges ve that prevalence rates for children diagnosed with ASD, who experience challenging behaviors, vary among cultures and countries as evidenced by Chung et al.’s study repor ng a prevalence rate of challenging behavior of 35.8% in Norway, 64.3% in Ireland and 30% in So. Korea. Chung and colleagues conclude that it is possible for people from different cultures to view challenging behaviors differently and this would affect ASD’s incidence, prevalence, diagnosis, and impact from country to country.
Global Interven ons and Ini a ves On a global level, early detec on and early interven on are basic requirements to treat ASD effec vely. Interven ons usually target social skills, behavior, language/speech skills, and sensory integra on (Malcolm‐Smith et al., 2013). Although ASD research dates back 30+ years in LMICs (e.g., India and the African con nent), within the last decade or so, there has been an increase in LMIC‐related ASD research (Wallace et al., 2012). What follows is our best guess about the progress of diagnosis and treatment of ASD in LMICs, based on our review of the literature.
Research Researchers at the University of Cape Town are inves ga ng if the Early Start Denver Model (an ABA and Pivotal Response
Training‐based interven on) (Rogers & Dawson, 2010), is an effec ve and culturally appropriate interven on for So. African families (Malcolm‐Smith et al., 2013). This model involves parental delivery of services, thus reducing costs.
The interdisciplinary Centre for Au sm Research in Africa has been established at the University of Cape Town to promote interdisciplinary research and collabora on to meet the mul cultural needs of families across So. Africa and other African countries (Malcolm‐Smith et al., 2013). Its priority is the availability of reliable and valid assessment tools, along with local exper se, to administer and interpret them (Malcolm‐Smith et al., 2013).
(Con nued on page 13)

www.apa.org/international/pi 13
Psychology International ◦ JUNE 2015
The Interna onal Collabora on for Au sm Registry Epidemiology (iCARE) (Schendel et al., 2013) was created as a mul ‐na onal consor um, among Australia, Denmark, Finland, Israel, Norway, Sweden, and the United States, to promote global popula on‐based epidemiology research on ASD and its risk factors. It is a unique resource with its mul ‐site data collec on and sharing to advance the understanding of ASD. In spite of its scope and ambi ons, all member sites are HICs with rela vely small non‐Caucasian minority popula ons.
Training Ini al and follow‐up training are important for health care workers, psychologists, and teachers to increase their exper se for
diagnosis and treatment of ASD (Wallace et al., 2012). Professional training has begun in So. Africa for the administra on and interpreta on of the Au sm Diagnos c Observa on Schedule (ADOS) the interna onal gold standard diagnos c tool (and translated for Zulu‐speaking families), and the Au sm Diagnos c Interview‐Revised (ADI‐R) (Malcolm‐Smith et al., 2013).
Interven on training is important for parents/caregivers to receive. Their role is crucial in the consistent and effec ve implementa on of in‐home interven ons or in assis ng prac oners with interven ons (Wallace et al., 2012).
Prac ce The gap between what is urgently needed to diagnose and treat ASD (and mental illness) and what is available to reduce the
burden remains wide. The World Health Organiza on (WHO)’s mental health Gap Ac on Programme (mhGAP) recognizes the need for ac on to reduce this gap. Its mhGAP Evidence Resource Centre is the umbrella structure for numerous and free mul lingual resources (WHO, n.d.). Resources include how to design services for mental, neurological, and substance use disorders in children in LMICs (WHO, 2008) as well as the mhGAP Interven on Guide (WHO, 2010), a technical resource for health care providers.
Awareness, Outreach, and Advocacy In 2008, “Au sm Speaks,” an au sm advocacy organiza on, launched the Global Au sm Public Health (GAPH) Ini a ve the
same year that the UN established World Au sm Awareness Day. The purpose of the GAPH is to develop systema c and sustainable solu ons to enhance global awareness, public health policies, training, service delivery, and research for ASD (Wallace et al., 2012). It has partnered with over 20 countries on six con nents to form collabora ons among local government officials, advocacy leaders, NGO representa ves, mental health and health care professionals, and families. Together, they iden fy community priori es, develop strategic plans, reduce social s gma and misinforma on, establish awareness programs, plan public health infrastructure, conduct local research to design and implement regional or local au sm screening tools and interven on programs, adapt and translate standardized assessment tools based on cultural norms, values, and language, and offer culturally relevant educa onal services. Con nuous technical support is available to facilitate sustainability, an important investment following the ini al flurry of training. Sustainability can be maintained from afar by online training and e‐supervision.
Wallace et al. report examples of GAPH’s success in Albania (through the leadership of the Albanian Children Founda on) and Bangladesh (through the Center for Neurodevelopment and Au sm in Children). Further, in Bangladesh, an interna onal au sm conference (co‐sponsored by the Center for Neurodevelopment and Au sm in Children, Au sm Speaks, Government of Bangladesh, and WHO) a racted interna onal a endees from South Asia (i.e., India, Sri Lanka, Bhutan, Nepal, and Maldives), Southeast Asia (i.e., Thailand, Indonesia, and Myanmar), and the Middle East (i.e., Jordan and the United Arab Emirates). Considering the similar needs shared by many of these countries, the a endees unanimously adapted the Dhaka (Bangladesh) Declara on on Au sm Spectrum Disorders and Developmental Disabili es (Wallace et al.) for implementa on in their respec ve countries.
Cultural and Linguis c Competence Wallace et al. (2012) assert that many clinical features of ASD are universal and Chung et al. (2012) report that the presence
and severity of challenging behaviors in individuals with ASD are similar across countries. When planning effec ve interven ons globally, researchers suggest that many evidence‐based interven ons developed in HICs can be modified for implementa on in LMICs only when local cultural, linguis c, and socio‐poli cal considera ons are acknowledged and incorporated. Specifically, assessment tools and interven on services to be effec ve in diverse environments, must be adapted to align with the local cultural and linguis c needs, socio‐poli cal environment, resources, and barriers experienced by families and professionals in each LMIC (Wallace et al., 2012). For instance, in countries in which mul ‐genera ons typically reside together, prac oners are advised to use cultural and familial sensi vity and include extended family members in “parental” interven on training sessions to assist with implemen ng the interven ons and providing
support.
(Con nued on page 14)
14 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
Conclusion As professional, familial, government, and public awareness of ASD increases globally, the accuracy of prevalence and incidence data will most likely improve and the awareness of the need for increased and culturally relevant interven ons will be heightened. Yet, even with enhanced awareness, many psychologists and health care prac oners in LMICs encounter limited or unavailable resources to diagnose and treat ASD. Leaders of many ini a ves highlighted here, wish to share their resources and knowledge. They are commi ed to the accurate diagnosis and effec ve treatment of ASD in LMICs. We hope that some of their resources, ini a ves, tools, and interven on models will assist psychologists worldwide to collaborate across disciplines and across con nents to increase research about ASD and its risk factors as well as design culturally relevant interven on ini a ves, especially in LMICs. In doing so, the collec ve community of psychologists, health care workers, educators, government leaders, and representa ves of NGOs might meet UN Secretary General Ban Ki‐moon’s “Call to Ac on.” He stated, “People with au sm have enormous poten al. Most have remarkable visual, ar s c, or academic skills. Thanks to the use of assis ve technologies, non‐verbal persons with au sm can communicate and share their un‐tapped capabili es. Recognizing the talents of persons on the au sm spectrum, rather than focusing on their weaknesses, is essen al to crea ng a society that is truly inclusive” (UN News Centre, 2015, p. 1).
References
American Psychiatric Associa on. (2013). Au sm Spectrum Disorder. Retrieved from h p://www.dsm5.org/Documents/Au sm%20Spectrum%20Disorder%20Fact%20Sheet.pdf
Chung, K.M., Woohyun, J., Ben‐Itzchah, E., Zachor, D., Furniss, F., Heyes, K., Matson, J.,
Kozlowski, A., & Barker, A. (2012). Cross cultural differences in challenging behaviors of children with au sm spectrum disorders: An interna onal examina on between Israel, South Korea, the United Kingdom, and the United States of America. Research in Au sm Spectrum Disorders, 6(2), 881‐889. doi: 10.1016/j.rasd.2011.03.016
Malcolm‐Smith, S., Hoogenhout, M., Ing, N., Thomas, K., & de Vries, P. (2013). Au sm spectrum disorder: Global challenges and local opportuni es. Journal of Child and Adolescent Mental Health, 25(1), 1‐5. doi: 10.2989/17280583.2013.767804
Matson, J.L., Mahan, S., Hess, J.A., Fodstad, J.C., & Neal, D. (2010). Progression of challenging behaviors in children and adolescents with au sm spectrum disorders as measured by the Au sm Spectrum Disorders‐Problem Behaviors for Children (ASD‐PBC). Research in Au sm Spectrum Disorders, 4 400–404. doi:10.1016/j.rasd.2009.10.010
McCabe, H. (2008). Au sm and family in the People's Republic of China: Learning from parents’ perspec ves. Research and Prac ce for Persons with Severe Disabili es, 33, 37–47.
Rogers, S. J., & Dawson, G. (2010). Early Start Denver Model for young children with au sm: Promo ng language, learning, and engagement. New York, NY: Guilford Press.
Schendel, D. et al. (2013). The Interna onal Collabora on for Au sm Registry Epidemiology (ICARE): Mul na onal registry‐based inves ga ons of au sm factors and trends. Journal of Au sm Development Disorders, 43, 2650‐2663. doi: 10.1007/s10803‐013‐1815‐x
UN Enable. (2006). Conven on on the Rights of Persons with Disabili es. Retrieved from h p://www.un.org/disabili es/conven on/conven onfull.shtml
UN General Assembly. (2007). Resolu on adopted by the General Assembly on 18 December
2007: 62/139, World Au sm Awareness Day. Retrieved from h p://www.un.org/en/ga/search/view_doc.asp?symbol=A/RES/62/139
UN Human Rights. (1989). Conven on on the Rights of the Child. Retrieved from h p://www.ohchr.org/EN/ProfessionalInterest/Pages/CRC.aspx
UN News Centre. (2015). Remarks on World Au sm Awareness Day. Retrieved from h p://www.un.org/apps/news/infocus/sgspeeches/statments_full.asp?statID=2558#.VVDI9ZPd6_Y
UN News Centre. (2015). Marking World Day, UN calls on businesses to commit to employing people with au sm. Retrieved from h p://www.un.org/apps/news/story.asp?NewsID=50485#.VUYyuJPd6_Z
(Con nued on page 15)

www.apa.org/international/pi 15
Psychology International ◦ JUNE 2015
UN World Au sm Awareness Day. (2015). Employment: The Au sm advantage. Retrieved from h p://www.un.org/en/events/au smday/index.shtml
Wallace, S, Fein, D., Rosanoff, M., Dawson, G., Hossain, S., Brennan, L., Como, A., & Shih, A. (2012). A global public health strategy for au sm spectrum disorders. Au sm Research, 5(3), 211‐217. doi: 10.1002/aur.1236
Wang, P., Michaels, C., & Day, M. (2011). Stresses and coping strategies of Chinese families with children with au sm and other developmental disabili es. Journal of Au sm and Developmental Disorders, 41, 783–795. Doi: 10.1007/s10803‐010‐1099‐3
World Health Organiza on (2008). mhGAP mental health gap ac on programme: Scaling up care for mental, neurological, and substance use disorders. Retrieved from h p://www.who.int/mental_health/evidence/mhGAP/en/
World Health Organiza on (n.d.). mhGAP evidence resource centre. Retrieved from h p://www.who.int/mental_health/mhgap/evidence/en/
World Health Organiza on (2010). mhGAP interven on guide for mental, neurological and substance use disorders in non‐specialized health se ngs. Retrieved from h p://www.who.int/mental_health/publica ons/mhGAP_interven on_guide/en/
About the Co‐authors: Juneau Gary, PsyD (APA main representa ve to DPI is a Professor in the Department of Counselor Educa on at Kean University in New Jersey. Neal S. Rubin, PhD, ABPP (APA representa ve to DPI) is a Professor at the Illinois School of Professional Psychology of Argosy University in Chicago. Both are APA NGO Representa ves to the United Na ons Department of Public Informa on and are co‐editors of this column. Ψ
The APA Office of Interna onal Affairs has
prepared a survey to learn from you how we
can be er serve your needs and meet your
expecta ons as an APA interna onal affiliate
member. Please take a few minutes and
complete the survey: h ps://
www.surveymonkey.com/r/BVGJHJY.
Thank you!
WE WANT TO HEAR FROM YOU!!!
APA international affiliates are eligible:
Join APA’s International Division (Div. 52) and receive a special $15 discount on the
first year’s dues. Membership includes access to the APA Journal International
Perspectives, International Psychology Bulletin, email lists and networking
opportunities. For more information, please visit the APA International Affiliates
corner: http://www.apa.org/international/outreach/initiatives/affiliate-membership/
international-affiliate-corner.aspx.
16 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
Global Mental Health:
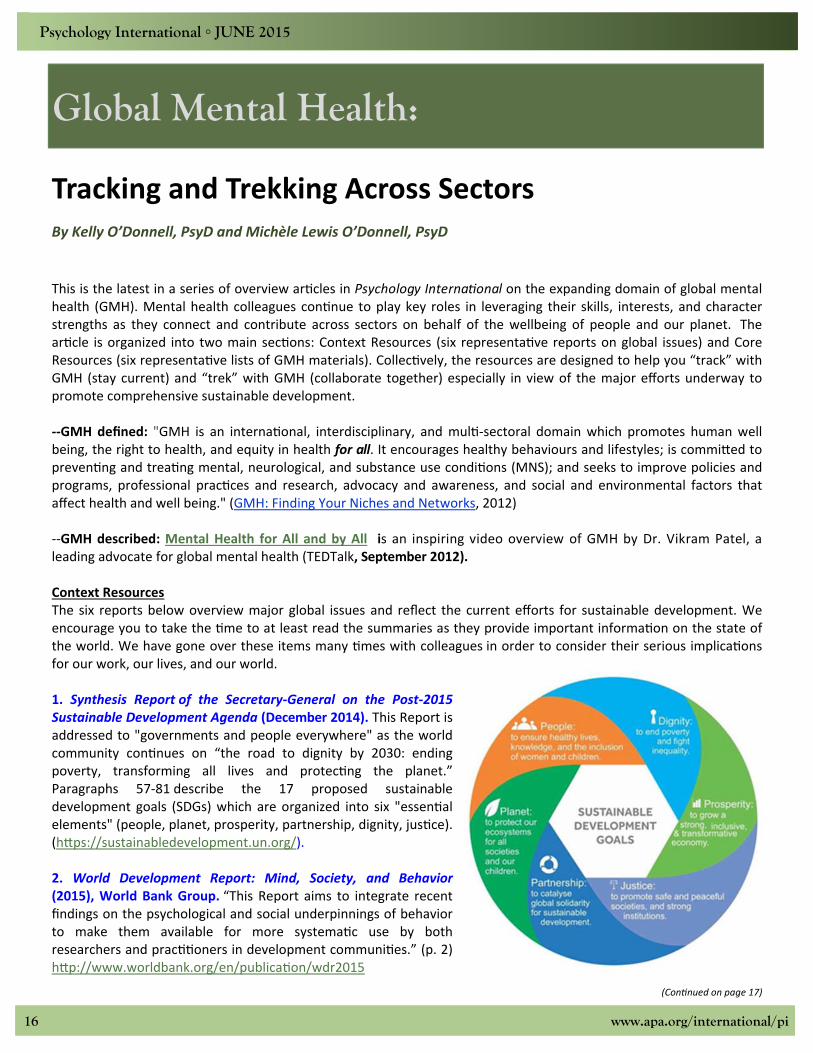
This is the latest in a series of overview ar cles in Psychology Interna onal on the expanding domain of global mental health (GMH). Mental health colleagues con nue to play key roles in leveraging their skills, interests, and character strengths as they connect and contribute across sectors on behalf of the wellbeing of people and our planet. The ar cle is organized into two main sec ons: Context Resources (six representa ve reports on global issues) and Core Resources (six representa ve lists of GMH materials). Collec vely, the resources are designed to help you “track” with GMH (stay current) and “trek” with GMH (collaborate together) especially in view of the major efforts underway to promote comprehensive sustainable development. ‐‐GMH defined: "GMH is an interna onal, interdisciplinary, and mul ‐sectoral domain which promotes human well being, the right to health, and equity in health for all. It encourages healthy behaviours and lifestyles; is commi ed to preven ng and trea ng mental, neurological, and substance use condi ons (MNS); and seeks to improve policies and programs, professional prac ces and research, advocacy and awareness, and social and environmental factors that affect health and well being." (GMH: Finding Your Niches and Networks, 2012) ‐‐GMH described: Mental Health for All and by All is an inspiring video overview of GMH by Dr. Vikram Patel, a leading advocate for global mental health (TEDTalk, September 2012). Context Resources The six reports below overview major global issues and reflect the current efforts for sustainable development. We encourage you to take the me to at least read the summaries as they provide important informa on on the state of the world. We have gone over these items many mes with colleagues in order to consider their serious implica ons for our work, our lives, and our world. 1. Synthesis Report of the Secretary‐General on the Post‐2015 Sustainable Development Agenda (December 2014). This Report is addressed to "governments and people everywhere" as the world community con nues on “the road to dignity by 2030: ending poverty, transforming all lives and protec ng the planet.” Paragraphs 57‐81 describe the 17 proposed sustainable development goals (SDGs) which are organized into six "essen al elements" (people, planet, prosperity, partnership, dignity, jus ce). (h ps://sustainabledevelopment.un.org/).
2. World Development Report: Mind, Society, and Behavior (2015), World Bank Group. “This Report aims to integrate recent findings on the psychological and social underpinnings of behavior to make them available for more systema c use by both researchers and prac oners in development communi es.” (p. 2) h p://www.worldbank.org/en/publica on/wdr2015
(Con nued on page 17)
Tracking and Trekking Across Sectors By Kelly O’Donnell, PsyD and Michèle Lewis O’Donnell, PsyD

www.apa.org/international/pi 17
Psychology International ◦ JUNE 2015
3. Human Development Report: Sustaining Human Development‐‐Reducing Vulnerabili es and Building Resilience (2014); United Na ons Development Program. “Globaliza on has on balance produced major human development gains, especially in many countries of the South. But there is also a widespread sense of precariousness in the world today—in livelihoods, in personal security, in the environment and in global poli cs.” (p. 1) h p://hdr.undp.org/en/2014‐report 4. World Disasters Report: Focus on Culture and Risk (2014), Interna onal Federa on of the Red Cross and Red Crescent Socie es. "This [year’s]…Report takes on a challenging theme that looks at different aspects of how culture affects disaster risk reduc on (DRR) and how disasters and risk influence culture….The one thing that is certain is that we will have less sustained impact if we do not adequately take account of people’s culture, beliefs, and a tudes in rela on to risk." (p. 8). h p://www.ifrc.org/en/publica ons‐and‐reports/world‐disasters‐report/world‐disasters‐report‐2014/
5. White Paper on Peacebuilding (2014), Geneva Peacebuilding Pla orm. "The White Paper on Peacebuilding reflects a 12‐month collabora ve mul ‐stakeholder ini a ve with peacebuilding professionals from all regions coordinated by the Geneva Peacebuilding Pla orm. The…is to present a range of voices and perspec ves about the challenges, opportuni es and future of peacebuilding prac ce.” (p. 3) h p://www.gppla orm.ch/white‐papers/whitepapers 6. Global Health 2035: A World Converging within a Genera on, The Lancet Commission on Inves ng in Health (The Lancet, December 2013). “Prompted by the 20th anniversary of the 1993 World Development Report, a Lancet Commission revisited the case for investment in health and developed a new investment framework to achieve drama c health gains by 2035. Our report has four key messages, each accompanied by opportuni es for ac on by na onal governments of low‐income and middle‐income countries and by the interna onal community.” (online, Execu ve Summary). h p://www.thelancet.com/journals/lancet/ar cle/PIIS0140‐6736(13)62105‐4/fulltext Core Resources This sec on lists examples of recent materials that are shaping the contours of the GMH domain. They are organized into six GMH categories. Note that many of the materials that could not be listed here due to space limita ons are included in the longer version of the ar cle and on our GMH‐Map website. GMH Newsle ers and Updates Movement for Global Mental Health (monthly) Centre for Global Mental Health London School of Hygiene and Tropical Medicine, and King’s Health Partners
(monthly) mhGAP, World Health Organiza on (twice a year) Bulle n, World Federa on for Mental Health (quarterly) Psychology Interna onal, Office of Interna onal Affairs, American Psychological Associa on (4‐6 mes/year). Also as
of April 2015 there is a biweekly news bulle n with informa on about opportuni es for interna onal involvement in mental health.
Centre for Interna onal Mental Health University of Melbourne (monthly) Mental Health Innova on Network (monthly) GlobalTracks, NIMH USA (quarterly, "A Newsle er for GMH Connec ons") Interna onal Union of Psychological Science Bulle n (monthly) GMH Edited Books (see the longer ar cle for special journal issues on GMH) Global Mental Health: Trauma and Recovery (2011, edited by Richard Mollica) Community Mental Health: Pu ng Policy into Prac ce Globally (2011, edited by Graham Thornicro et al.) 21st Century Global Mental Health (2012, edited by Eliot Sorel)
(Con nued on page 18)
18 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
Global Mental Health: Principles and Prac ce (2013, edited by Vikram Patel et al.). Public Mental Health: Global Perspec ves (2013, edited by Lee Kni on, Neil Quinn) Improving Mental Health Care: The Global Challenge (2013, edited by Graham Thornicro et al.) Proceedings of the 30th Interna onal Congress of Psychology (convened 2012, published 2014): ‐‐Psychology Serving Humanity (volume one): Majority World Psychology ‐‐Psychology Serving Humanity(volume two): Western Psychology Global Mental Health Trials (2014, edited by Graham Thornicro , VIkram Patel).
Global Mental Health: Anthropological Perspec ves (2015, edited by Brandon Kohrt, Emily Mendenhall) Re‐Visioning Psychiatry: Cultural Phenomenology, Cri cal Neuroscience, and Global Mental Health (2015, edited by
Laurence Kirmayer, Robert Lemelson, Constance Cummings)
World Health Organiza on, Mental Health Publica ons Click here to access and download their mental health publica ons including technical guidance documents: h p://www.who.int/mental_health/publica ons/en/. Two of the latest publica ons are Preven ng Suicide: A Global Impera ve (2014) and The mhGAP Humanitarian Interven on Guide (2015).
Also note WHO MINDbank, a major online pla orm for MH resources‐‐na onal/interna onal, human rights, development, etc. Training Programs and Courses Chicago School of Professional Psychology, Interna onal Psychology, online doctorate with concentra ons in
Organiza ons/Systems or Trauma Services. MSc Global Mental Health, London‐based course taught jointly between the London School of Hygiene and
Tropical Medicine and King's College London Ins tute of Psychiatry. Click here for the Course prospectus. MSc Global Mental Health: University of Glasgow, College of Medical, Veterinary, and Life Sciences. Programme
brochure. Interna onal Masters in Mental Health Policies and Services, Universidade Nova de Lisboa, Faculdade de Ciências
Médicas. Program brochure. Master of Arts in Counseling Psychology and Global Mental Health: William James College (formerly
Massachuse s School of Professional Psychology). Program brochure. GMH: Trauma and Recovery Cer ficate Program, Harvard Program in Refugee Trauma (on‐site learning in Italy, and
web‐based learning). Cer ficates of comple on are awarded by HPRT and the Harvard Medical School Department of Con nuing Educa on.
Leadership in Mental Health Course, Sangath Centre and London School of Hygiene and Tropical Medicine(Goa, India).
Interna onal Diploma in Mental Health Law and Human Rights, Indian Law Society and WHO. (distance learning program to accommodate working professionals across the globe)
Note that there are individual courses, including GMH overviews, taught as part of graduate studies programs at: Duke University, George Washington University, Columbia University, Fordham University, and Johns Hopkins Bloomberg School of Public Health. Also note there are ongoing special GMH seminars and addi onal courses as part of specific GMH programs at Columbia University, Yale University, University of Washington, University of Toronto, etc.
5. GMH Conferences and Events There are many gatherings that include GMH topics that could be added to the list below, including for example at the interna onal presenta ons at the annual Conven on of the American Psychological Associa on and at other psychology‐related gatherings around the world (see the list at: h p://www.apa.org/interna onal/resources/events.aspx). Note that many of these gatherings have online access to video and powerpoint presenta ons.
(Con nued on page 19)

www.apa.org/international/pi 19
Psychology International ◦ JUNE 2015
June 2014: Solving the Grand Challenges in GMH, NIMH USA and /Grand Challenges Canada, Rockville, MD, (for
power points and notes contact the NIMH Office for Research on Dispari es and Global Mental Health) September 2014: mhGAP Forum and Launch of World Suicide Report. WHO, Geneva (click here for the Forum
Report and click here for the two animated videos on depression: I Had A Black Dog and Living with a Black Dog October 2014: World Mental Health Day—Living with Schizophrenia February 2015: World Innova on Summit for Health (WISH), Qatar‐‐Mental Health and Wellbeing in Children (panel
discussion, video). Note too that the WISH December 2013 event included a strong emphasis on Mental Health with a focus on innova ons (panel discussion, video)
April 2015: Culture and GMH Conference, Society for the Study of Psychiatry and Culture. Providence, Rhode Island, USA
April 2015: Mental Health for All: Connec ng People and Sharing Experience. World Federa on for Mental Health. Lille, France
30 April 2015. UN Psychology Day: Reducing Health Inequali es Within and Among Countries: Psychology's Contribu ons to the United Na on's Post‐2015 Global Agenda. (now in its eighth year)
June 2015: Crossing Boundaries: Mee ng the Needs of Refugee Communi es Around the Globe, William James College (formerly Massachuse s School of Professional Psychology) Newton, Massachuse s USA. Organized by the GMH Program.
6. GMH Cri ques GMH is not without its cri cs. Here are some examples. Toward a New Architecture for Global Mental Health by Laurence Kirmayer and Duncan Pedersen, Transcultural
Psychiatry, December 2014. Interview in the May 2014 MGMH Newsle er, with China Mills and her book Decolonizing Global Mental Health: The
Psychiatriza on of the Majority World (2013). GMH and its Discontents, a summary of conference/workshop at McGill University in July 2012 on GMH: Bridging the
Perspec ves of Cultural Psychology and Public Health. Final Thoughts It is challenging to “track and trek” with the expanding GMH domain. But in many ways this is a welcome development! GMH and civil society organiza ons are increasingly involved in global affairs and in collabora ng with United Na ons agencies—and vice versa. Although not without its flaws and failures (like any human ins tu on), the United Na ons in our view con nues to be crucial for promo ng and protec ng human security/peace, human rights/dignity, and social progress/be er standards of life (as highlighted in the Charter of the United Na ons’ Preamble, 1945). We encourage mental health professionals to “track and trek” with GMH and to connect and contribute across sectors, including the mul ‐faceted efforts of United Na ons, on behalf of our precarious yet precious world. Ψ About the Co‐authors: Drs. Kelly and Michèle O’Donnell are consul ng psychologists based in Geneva with Member Care Associates, Inc. They are Interna onal Affiliates of the American Psychological Associa on and ac vely involved with the NGO Forum for Health UN personnel/agencies and interna onal NGOs. This ar cle is part of GMH‐Map (h ps://sites.google.com/site/gmhmap/), a collabora ve project to compile and share GMH resources via ar cles, training, and a website. Email: [email protected].

20 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
International Book Review: Selected Review from PsycCRITIQUES The book review reprinted here is courtesy of PsycCRITIQUES editor Danny Wedding. PsycCRITIQUES is an online journal that provides reviews of books, monographs, films, and other productions in psychology stretching back to 1956. Readers can also access selected reviews and discuss books important to the science and profession of psychology by visiting the PsycCRITIQUES blog at psyccritiquesblog.apa.org. For more information see www.apa.org/psyccritiques. If you are interested in reviewing, please contact editor Danny Wedding at [email protected].
A Movement for Global Mental Health Equity, Parity, and
Access A review of
Global Mental Health: Principles and Practice
By Vikram Patel, Harry Minas, Alex Cohen, and Martin J. Prince (Eds)
New York, NY: Oxford University Press, 2014. 498 pp. , $59.95
Reviewed by Merry Bullock
PsycCRITIQUES CONTEMPORARY PSYCHOLOGY: APA REVIEW OF BOOKS American Psychological Association
Although the phrase “Global Mental Health (GMH)” was coined just a few years ago (Satcher, 2001), the concerns that it addresses—worldwide incidence of mental disorders, their substan al contribu on to the global burden of disease, strong rela ons between poverty, violence, social disadvantages and mental disorders, and dispropor onal inequi es between higher and lower income countries—have become increasingly salient. The emergence of a GMH discipline can be traced to a series of landmark reports beginning with the 1995 World Health Report (World Health Organiza on, 1995), followed by two Lancet series, Global Mental Health 2007 and Global Mental Health 2011 (Elsevier, 2007, 2011), that focused on mental health as priority global health issues, and culmina ng in the World Health Organiza on’s Mental Health Ac on Plan 2013‐20 (World Health Organiza on, 2013). It may well be that the first quarter of this century comes to be known as the era when mental health assumed a posi on as a central development issue, addressed worldwide. The volume Global Mental Health: Principles and Prac ce is a textbook that provides a broad and deep overview of this emerging field. Edited by GMH gurus Vikram Patel, Harry Minas, Alex Cohen and Mar n Prince, the book covers the history, concepts, ra onale, and scope of applica on using a GMH lens. Close to 500 pages long, with 20 chapters and 55 contributors, the book offers a compendium of informa on, organized around “two.. interconnected needs—scien fic founda ons and prac ce” (p. xi). The book is divided into two parts. Part 1, Principles of Global Mental Health, exemplifies GMH’s cross‐disciplinary founda ons, with chapters on the history of mental health concepts and treatment, classifica on and
(Con nued on page 21)

www.apa.org/international/pi 21
Psychology International ◦ JUNE 2015
diagnosis, epidemiology, development resources, mental health promo on, and interven ons. Embedded in each of the chapters is deep a en on to the global nature of the discussion, no ng cultural, cross cultural and social dimensions of mental disorders and their sequelae. I was par cularly taken with the first chapters on a history of global mental health, and on culture and global mental health. The history chapter, wri en by three of the editors, managed in 20 pages to move from ancient mes, through the middle ages, to a useful lis ng of the major players in the current field of mental health including global agencies, advocacy NGOs and research ins tu ons. While reading this chapter, I learned some interes ng history. For example, part of the new focus on mental health arose from a change in measurement and repor ng. Prior to the 1990s, world health sta s cs were reported in terms of mortality only, which gave focus primarily to those infec ous diseases that could kill. Beginning with the World Health Report of 1993, health sta s cs were also reported in terms of a new measure— “disability adjusted life years” (or DALYs) —which accounted for morbidity (loss of healthy life from disability). For the first me, the global burden of non‐communicable diseases, including mental disorders, could be assessed. As the authors note “much to the surprise of many people . . .about 8% of the global burden of disease . . . [was] due to mental health problems” (p. 12; the present es mate is closer to 13%). This simple change in the lens of analysis prompted a host of projects, ini a ves and policy movements, and also raised worldwide awareness that the resources to address mental health issues—from research to service delivery—were severely lacking in most countries of the world. The focus of the present GMH movement, then, along with the focus of this book, is on understanding how to change this—to understand the demography of mental disorders globally, to understand the universe of culturally relevant interven ons, to understand how to build the resources to tackle these challenges, and to understand how to develop the poli cal will to invest in those resources. The GMH movement is not without its cri cs. There are those who worry that the present public health approach to global mental health will impose largely western models from high income countries on people in other cultures, o en with different beliefs about causes and cures for their health challenges, or that the GMH movement will overshadow a en on to socioeconomic dispari es (cf. Suarez, Logie, & Arocha, 2014; Summerfield, 2008, 2013). Although these cri cisms are not specifically addressed, the authors of the chapters in this volume do address issues in building culturally relevant, sustainable mental health systems that meet local needs. Some of the chapters address this directly. For example, the chapter on “Culture and Global Mental Health” stands out as a strong exposi on of the complex and nuanced ways that culture is important. The authors give cogent examples of how culture ma ers in framing, defining and iden fying distress, in healing, and in developing mental health systems. They add: “the current investment in biologically based diagnoses and investments in psychiatry reflects cultural values more than scien fic evidence. . . ..[there is a] need for an ecosocial approach that characterizes mental health problems in terms of interac ons with the local social environment, including family, community, and other networks” (pp. 44–45). They also address reconciling local cultural prac ces and interna onal norms. As they conclude “Global mental health policy faces an inherent paradox: the effort to share resources and scale up prac ces requires an assump on that more or less standardized interven ons will work across contexts. Yet the claim of responding to local needs requires engagement with pa ents and grass‐roots providers and support systems. Global mental health policy . . . must support bo om up strategies, like those of community based par cipatory ac on research to iden fy indigenous systems of helping and healing . . .” (p. 57). Other chapters on culturally sensi ve research prac ces and on social determinants of mental health are similarly nuanced. I also appreciated the chapters on resource development (“Global Mental Health Resources” and “Strategies for Strengthening Human Resources for Mental Health”), each of which reviewed the landscape of global organiza ons involved in se ng the agenda for the assessment and evalua on of needs, and developed systema c models of resource needs and development possibili es. The case studies cited on resource development in Indonesia and Vietnam were especially valuable.
(Con nued on page 22)

22 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
The chapters in the second part of the book, on vulnerable popula ons (children, women, vic ms of disasters) and on challenges like s gma and discrimina on, provide broad overviews of the literature—serving more to outline what the challenges are than where solu ons might take us. The last chapter, “Genera ng Poli cal Commitment” with a case study of the development of the mental health system in Belize, offered a concise descrip on of how poli cal change can be developed and sustained, and further developed another common theme in the book—that mental health issues are best addressed globally within a human rights framework. This is not a book to be read at one si ng—the chapters are dense and the issues are mul faceted. Yet, issues are clearly laid out, presen ng background on what currently exists (too li le) and what needs to be done. Those chapters that provide case examples are the most successful. I learned a lot from every chapter—the broad mix of disciplines in the authors’ backgrounds assure that anyone from psychology, psychiatry, social work, public health, or related disciplines, would find new material. However, the editors clearly aim to provide a broad overview rather than exposi on of specific tools or skills for global mental health prac ce. I par cularly appreciated the approach, visible in nearly every chapter, which emphasized both history and context. Anyone skimming across chapters in this book would be struck by a small number of common themes: there is inadequate mental health care in most of the world—rich and poor, but especially poor; there is li le research on how to understand mental health problems in the poorer countries of the world (e.g., one chapter claimed that only 1% of mental health efficacy research involved low and middle income countries). No ma er what sta s cs one uses, we know too li le about the demographics, prevalence and severity of mental health issues worldwide (except that they are endemic), about what works to ameliorate them; or about how to address s gma and other barriers to access. As the authors of the chapter on child and adolescent mental health noted, the research gaps have been iden fied—on cost‐effec veness of mental health interven ons; on resilience and protec ve factors; on the development of locally relevant instruments; and on ways to support collabora ons with researchers in low and middle income countries—but the solu ons are elusive. There is redundancy across chapters—not because the authors are repe ve or the editors careless, but because the reali es of global mental health hammer away at the same fundamental issues: there is too li le research on prevalence, common treatments, effec ve treatments, or outcomes; there are two few resources to allow scaling up those interven ons that seem promising; there is too much s gma; there is too li le investment in developing robust research or treatment systems; there are two few human resources spread too thinly to address the enormous burden of mental health issues. Despite this depressingly long list of lacks, there is also genuine op mism that things are changing—recogni on of the enormity of the burden of mental disease, increased a en on to addressing the need for human and material resources, a en on to preven on and to promo on of resilience and increased advocacy at global and local levels. The penul mate chapter in the volume, “Research Priori es, Capacity and Networks,” outlines the goal se ng exercises that have been developed for building capacity for global mental health. The last chapter, “Genera ng Poli cal Commitment for Mental Health System Development,” forms a fi ng capstone to the volume. It discusses broadly the issues in mo va ng policy makers, and provides an example from one country, Belize, of steps taken to increase poli cal will to invest in mental health. The field of GMH is s ll developing. Its paradigms have moved beyond tradi onal psychopathology, diagnosis and treatment to include the social, economic and contextual condi ons and consequences of mental health. This volume contributes to that development by offering a detailed overview of what GMH is, who prac ces it, and what challenges they meet. As such it is important reading for understanding the mul disciplinary, mul sectoral content and frameworks of mental health challenges worldwide. References Elsevier. (2007, September 3). Global mental health 2007 [Clinical series]. Lancet, 370. Retrieved from h p://www.thelancet.com/series/global‐mental‐health Elsevier. (2011, October 18). Global mental health 2011 [Global health series]. Lancet, 378. Retrieved from www.thelancet.com/series/global‐mental‐health‐2011
(Con nued on page 23)

www.apa.org/international/pi 23
Psychology International ◦ JUNE 2015
RECENTLY PUBLISHED
Studying Ethnic Iden ty: Methodological and Conceptual Approaches Across Disciplines (h p://www.apa.org/pubs/books/4318132.aspx?tab=2) Edited by by Carlos E. Santos, PhD, and Adriana J. Umaña‐Taylor, PhD “In this book, editors Carlos Santos and Adriana Umaña‐Taylor bring together a diverse group of social and applied scien sts from a wide range of fields including educa onal anthropology, developmental, community and social psychology, and sociology. Together, they inves gate the process by which ethnic iden ty is formed and maintained throughout the lifespan.” From APA books.
Satcher, D. (2001). From the Surgeon General. Global mental health: Its me has come. Journal of the American Medical Associa on, 285, 1697.h p://dx.doi.org/10.1001/jama.285.13.1697 Suarez, E. B., Logie, C., & Arocha, J. F. (2014). An open debate about the object and purpose of global health knowledge in the context of an interdisciplinary research partnership on HIV/STI preven on priori es in Peru. Globaliza on and Health, 10,40.h p://dx.doi.org/10.1186/1744‐8603‐10‐40 Summerfield, D. (2008). How scien fically valid is the knowledge base of global mental health? Bri sh Medical Journal, 336, 992–994. h p://dx.doi.org/10.1136/ bmj.39513.441030.AD Summerfield, D. (2013). “Global mental health” is an oxymoron and medical imperialism.Bri sh Medical Journal, 346, f3509. h p://dx.doi.org/10.1136/bmj.f3509 World Health Organiza on. (1995). World health report 1995: Bridging the gaps. Geneva: WHO. World Health Organiza on. (2013). Mental health ac on plan 2013–20. Geneva: WHO.
14th European Congress of Psychology (ECP 2015) July 7-10, 2015
Milan, Italy Web: http://www.ecp2015.it/it/
Theme: Linking technology and psychology:
feeding the mind, energy for life
InterAmerican Congress of Psychology (SIP) July 12-16, 2015
Lima, Peru Web: http://sip2015.org/
Registration still open until July 16, 2015
24 www.apa.org/international/pi
Psychology International ◦ JUNE 2015
ANNOUNCEMENTS APA GRANTS, AWARDS AND FELLOWSHIPS APA GRANTS FOR US PSYCHOLOGISTS AND APAGS MEMBERS TO ATTEND INTERNATIONAL CONFERENCES This award will cover or par ally cover conference registra on fees at interna onal conferences held outside the United States and Canada for U.S.‐based psychologists. Deadline: July 1, 2015 Sponsor: Office of International Affairs http://www.apa.org/about/awards/international‐conference‐grant.aspx
SMALL GRANTS FOR THE PROGRAM DEVELOPMENT OF NATIONAL PSYCHOLOGY ASSOCIATIONS Provides funds to national psychology associations for program development from the Committee on International Relations in Psychology (CIRP) of the Office of International Affairs American Psychological Association.Deadlines: Deadline: September 1, 2015 Sponsor: APA Office of International Affairs http://www.apa.org/about/awards/cirp‐small‐grants.aspx
APA‐IUPSYS GLOBAL MENTAL HEALTH FELLOWSHIP The APA‐IUPsyS Global Mental Health Fellowship provides a unique opportunity for a psychologist to spend one year in Geneva, Switzerland, at the World Health Organiza on (WHO), in the Department of Mental Health and Substance Abuse. The fellow will focus on one or more issues related to the WHO Mental Health Ac on Plan. Although the program provides the opportunity to work at WHO on mental health issues. Deadline: September 30, 2015 Sponsor: APA; IUPsyS h p://www.apa.org/about/awards/global‐health‐fellowship.aspx DIVISION INTERNATIONAL ACTIVITIES GRANT (DIAG) PROGRAM This award will provide support for division‐ini ated programs aimed at fostering interna onaliza on and interna onal members outreach. Deadline: March 1, 2016 Sponsor: APA Commi ee on Interna onal Rela ons in Psychology (CIRP) h p://www.apa.org/about/awards/interna onal‐diag.aspx INTERNATIONAL SCIENTIFIC MEETING SUPPORT AWARD The APA Commi ee on Interna onal Rela ons in Psychology (CIRP) invites applica ons for funds for scien fic mee ngs that foster the exchange of knowledge among psychologists across the world. Deadline: March 1, 2016 Sponsor: APA Office of Interna onal Affairs FLORENCE L. DENMARK AN MARY E. REUDER AWARD The award’s purpose is to recognize and encourage other outstanding psychologists who have made similar interna onal contribu ons to further the understanding of women and/or gender. Deadline: May 1, 2016 Sponsor: Division 52
(Con nued on page 25)

www.apa.org/international/pi 25
Psychology International ◦ JUNE 2015
AMERICAN PSYCHOLOGICAL FOUNDATION GRANTS
Frances M. Culberston Travel Grant An award of $1,500 to support women from developing countries who are in the early stages of their careers by providing travel funds to a end conferences in psychology. Deadline: February 15, 2016 Sponsor: American Psychological Founda on h p://www.apa.org/apf/funding/culbertson.aspx?tab=1 Wilhelm Wundt‐William James Award for Excep onal Contribu ons to Trans‐Atlan c Psychology This award for excep onal contribu ons to trans‐Atlan c psychology recognizes a significant record of trans‐Atlan c research collabora on. Deadline: October 31, 2016 Sponsor: American Psychological Founda on h p://www.apa.org/apf/funding/wundt.aspx?tab=1
Psychology International is a publication of the APA Office of International Affairs.
Merry Bullock, PhD, Senior Director
Sally Leverty, International Affairs Assistant
Sharon Asonganyi, MPH, Communications and Program Manager
Please visit www.apa.org/international or email the office at [email protected]
123rd Annual
American Psychological Association
Convention
For more information visit
Web: http://www.apa.org/convention/programming/international/index.aspx





























