Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISMVol. 48, No. 12, December 2003, pp 3359–3370DOI 10.1002/art.11420© 2003, American College of Rheumatology
Physical Functioning Over Three Years in Knee Osteoarthritis
Role of Psychosocial, Local Mechanical, and Neuromuscular Factors
Leena Sharma, September Cahue, Jing Song, Karen Hayes, Yi-Chung Pai, and Dorothy Dunlop
Objective. To identify factors that predict a poorphysical function outcome over 3 years in individualswith knee osteoarthritis (OA), in an effort to aid in thedevelopment of strategies to prevent such functionallimitations and consequential disability.
Methods. Community-recruited individuals withknee OA underwent baseline, 18-month, and 3-yearassessments of candidate risk factors and physicalfunction. Risk factors were age, body mass index (BMI),knee pain intensity (on a visual analog scale [VAS]),local mechanical and neuromuscular factors (varus-valgus laxity, malalignment, proprioceptive inaccuracy,quadriceps strength, hamstring strength), activity level(Physical Activity Scale for the Elderly, amount ofaerobic exercise), and psychosocial factors (Short-Form36 [SF-36] mental health and role-functioning emo-tional subscales, self-efficacy using the Arthritis Self-Efficacy Scale physical function subscale, and socialsupport using the Medical Outcomes Study Social Sup-port Survey). Outcome was assessed using the WesternOntario and McMaster Universities Osteoarthritis In-dex (WOMAC) physical function scale and rate ofchair-stand performance. Participants were grouped byquintile of baseline WOMAC score. The baseline to3-year outcome was considered “good” when functionimproved by 1 or more quintiles or remained within the2 highest function groups, and was considered “poor”when function declined by 1 or more quintiles or re-
mained within the 3 lowest function groups. The sameapproach was taken for chair-stand outcome. Logisticregression was used to evaluate both the baseline leveland the baseline to 18-month change in each factor as apredictor of physical function outcome over 3 years,adjusting for age, BMI, knee pain intensity, diseaseseverity, and additional potential confounders.
Results. Factors that significantly increased thelikelihood of a poor WOMAC outcome were baselinelaxity (crude odds ratio [OR] 1.48/3°, 95% confidenceinterval [95% CI] 1.02–2.14), BMI (OR 1.26/5 units,95% CI 1.01–1.57), knee pain intensity (OR 1.21/20 mmon VAS, 95% CI 1.00–1.47), and baseline to 18-monthincrease in knee pain (OR 1.32/20 mm on VAS, 95% CI1.06–1.65). Factors that significantly protected against apoor WOMAC outcome were better baseline mentalhealth (OR 0.62/5 points, 95% CI 0.44–0.87), self-efficacy (OR 0.79/5 points, 95% CI 0.67–0.93), and socialsupport (OR 0.86/10 points, 95% CI 0.75–0.98), andgreater amount of aerobic exercise (OR 0.75/60 minuteseach week, 95% CI 0.63–0.89). Factors that increasedthe likelihood for a poor function outcome by thechair-stand performance rate were age and propriocep-tive inaccuracy, and factors that reduced the likelihoodfor poor chair-stand outcome were strength (attenuatedafter adjusting for pain intensity or self-efficacy), self-efficacy, and aerobic exercise. Individuals who sustainedhigh function and those who sustained low function overthe 3 years were described.
Conclusion. Factors placing individuals with kneeOA at greater risk of a poor function outcome by at least1 of the 2 function measures included the local factorslaxity and proprioceptive inaccuracy, as well as age,BMI, and knee pain intensity. Factors protectingagainst a poor function outcome included strength, thepsychosocial factors mental health, self-efficacy, andsocial support, and the activity level measured by theamount of aerobic exercise per week. The identification
Supported by National Institute of Arthritis and Musculoskel-etal and Skin Diseases grants P60-AR-48098 and R01-AR-48748, andby National Center for Research Resources grant RR-00048.
Leena Sharma, MD, September Cahue, BS, Jing Song, MS,Karen Hayes, PhD, Yi-Chung Pai, PhD, Dorothy Dunlop, PhD:Northwestern University, Chicago, Illinois.
Address correspondence and reprint requests to LeenaSharma, MD, Feinberg School of Medicine, Northwestern University,300 E. Superior, 3-715, Chicago IL 60611. E-mail: [email protected].
Submitted for publication March 10, 2003; accepted in revisedform September 4, 2003.
3359

of these factors provides possible targets for rehabilita-tive and self-management strategies to prevent dis-ability.
Knee osteoarthritis (OA) is a leading cause ofchronic disability in older persons (1). As defined byJette et al, disability is the impaired performance ofexpected socially defined life tasks, in a typical sociocul-tural and physical environment (2). Physical functionlimitation, or difficulty with physical tasks and activities,is fundamental to the development of disability in OA.Pain is likely to be a central factor in the physicalfunction limitation of knee OA, both due to its directeffects on function and as a route through which otherfactors operate. However, pain is not the only source offunctional limitation in knee OA (3). In the Framinghamstudy, limited function was more likely to occur inconjunction with moderately severe OA and infrequentpain than with milder OA and frequent pain (4). Iden-tification of factors, in addition to pain, that contributeto poor physical function provides an opportunity tobroaden the strategies to prevent disability.
The literature dealing with physical function lim-itation in knee OA includes a wealth of cross-sectionalstudies but few longitudinal studies. These publishedOA studies and/or longitudinal reports not limited tosubjects with arthritis have introduced several factors aspotential determinants of physical function outcome inknee OA, including obesity, comorbidity, depressivesymptoms, low social support, and low levels of physicalactivity. Self-efficacy, defined by Bandura (5) as thebelief in one’s capacities to mobilize the internal re-sources and course of action needed to meet givensituational demands, predicted physical function out-come in a longitudinal study of older adults with kneepain (6,7).
Local impairments of knee function in knee OAmay also have some bearing on difficulty with physicaltasks and activities. Several local factors influence kneefunction, including varus-valgus knee stability, by con-tributing to tibiofemoral congruence and load distribu-tion across the articular surface; hip-knee-ankle align-ment, by proportionately dividing load between themedial and lateral compartments; muscle activity, byadding stability, controlling the stop and start of jointmotion, and compensating for gravity; and joint propri-oception, or the perception of joint position, by provid-ing input to the nervous system to guide periarticularmuscle activity. Although these factors may be impairedin some individuals prior to disease development, theyalso may be made worse by OA (8–10). In the examina-
tion of the relationship between the disease itself andlimitation of function in knee OA, the disease has beenconsidered globally, using radiographic severity as asurrogate, whereas the impact of specific disease-associated impairments on limitation of function hasreceived little attention.
There is no established approach to define andanalyze physical function over time in studies of kneeOA. The examination of change in a function measurebetween baseline and followup is limited by its failure tocapture the possibility of a sustained high level offunction as a good outcome or a sustained low level offunction as a bad outcome. Also, the meaning of smallincrements of change in a function measure, treated as acontinuous variable, is unclear. Ideally, the approachtaken to assess outcome should capture an individual’sexperience over time, and should achieve this in aninterpretable way.
Advancing knowledge of factors contributing to apoor physical function outcome will aid in the develop-ment of strategies to prevent function limitation andconsequential disability. The goal of this prospectivestudy was to identify the factors that predict a poorphysical function outcome assessed over 3 years inindividuals with knee OA.
PATIENTS AND METHODS
Sample. Mechanical Factors in Arthritis of the Knee(MAK) is a prospective, observational, longitudinal study offunction decline and OA disease progression in a cohort ofindividuals with established knee OA that began in 1997, andis described in previous reports (for example, refs. 9–14).Participants were recruited from the community through ad-vertising in periodicals targeting elderly persons, announce-ments at 67 neighborhood organizations, letters to members ofthe registry of the Buehler Center on Aging at NorthwesternUniversity, and local medical center referrals.
Inclusion/exclusion criteria were based on recommen-dations from the multidisciplinary workshop sponsored by theNational Institute of Arthritis and Musculoskeletal and SkinDiseases and National Institute on Aging (15). Inclusioncriteria were presence of definite tibiofemoral osteophytes(Kellgren/Lawrence [K/L] radiographic severity grade �2) in 1or both knees, confirmed on study protocol radiographs, and aLikert category rating of at least “a little” difficulty with 2 ormore of the Western Ontario and McMaster UniversitiesOsteoarthritis Index (WOMAC) physical function scale items.Exclusion criteria were having received a corticosteroid injec-tion within the previous 3 months or a history of avascularnecrosis, rheumatoid or other inflammatory arthritis, periar-ticular fracture, Paget’s disease, villonodular synovitis, jointinfection, ochronosis, neuropathic arthropathy, acromegaly,hemochromatosis, Wilson disease, osteochondromatosis, gout,pseudogout, or osteopetrosis. Approval was obtained from the
3360 SHARMA ET AL

Office for the Protection of Research Subjects InstitutionalReview Board of Northwestern University.
Measurement of candidate risk factors. Candidate riskfactors were measured at baseline and at 18 months offollowup. Varus-valgus laxity was measured using a previouslydescribed device and protocol that provide thigh and ankleimmobilization, a stable knee angle, and fixed varus and valgusload (9,11). Laxity was measured as the angular deviation aftervarus and valgus load (expressed in degrees). All laxity mea-surements were performed by the same examiner and assistant(LS and SC). Our reliability with this device in persons withknee OA and varying body habitus was very good (within-session intraclass correlation coefficient [ICC] 0.85–0.96,between-session ICC 0.84–0.90) (9,11). Total rotation, which isthe sum of varus and valgus rotation for each knee, wasanalyzed as a continuous variable.
Quadriceps strength and hamstring strength were mea-sured isokinetically at 120°/second to assess maximal torqueduring movement (expressed in ft-lbs), using a computer-driven isokinetic dynamometer (Cybex Medical, Hauppauge,NY). A single tester assessed all patients, in accordance with apreviously described protocol (11). To determine measure-ment reliability, actual test repetitions for each type of test,each muscle group, and each leg were analyzed. All ICCsexceeded 0.98.
Alignment was measured from a single anteroposteriorradiograph of the full lower extremity, which was acquiredusing a graduated grid cassette. Alignment of the knee jointwas assessed as the angle formed by the intersection of themechanical axes of the femur (the line from femoral headcenter to femoral intercondylar notch center) and the tibia (theline from ankle talus center to the center of the tibial spinetips), following previously described acquisition and measure-ment protocols (12). One experienced reader (LS) made allmeasurements. Reliability of the alignment assessments forboth varus and valgus knees was high (ICCs 0.98–0.99). Theabsolute value of severity of malalignment was analyzed as acontinuous variable and was expressed as degrees from neutral(0°) in either the varus or valgus direction.
Proprioceptive inaccuracy was measured as the differ-ence between actual knee-motion onset and the participant’sdetection of motion, using a previously described apparatusand protocol that provide computer-controlled, passive, angu-lar knee motion at 0.3° per second and a precise measurementof angular displacement (10,13). Visual, auditory, vibration,cutaneous tension, and pressure cues to limb motion wereeliminated. The participant was seated with the back sup-ported, hips flexed to 70°, and knees flexed to 90°. In each trial,both legs were moved to a starting position of 45° knee flexion.ICCs for the assessments of participants with and without OAby a single experienced tester were 0.94 for the left leg and 0.95for the right leg. Proprioceptive inaccuracy was analyzed as acontinuous variable.
Body mass index (BMI) was measured as the weight (inkg) divided by the height (in m2). Knee pain intensity wasmeasured using separate 100-mm visual analog scales (VAS)for pain in the right and left knees in the last week. Radio-graphs were obtained with individuals in a standing, semiflexedposition, following the Buckland-Wright protocol (includingknee position, beam alignment, markers to account for mag-nification, and fluoroscopic confirmation of knee position).
The specific MAK protocol has been described previously(9,11,12,14).
Disease severity was assessed using the K/L globalradiographic grading system (0 � normal, 1 � possible osteo-phytes, 2 � definite osteophytes and possible joint spacenarrowing, 3 � moderate/multiple osteophytes, definite nar-rowing, some sclerosis, and possible attrition, 4 � largeosteophytes, marked narrowing, severe sclerosis, and definiteattrition). Bilateral knee OA was defined as a K/L grade of �2in both knees. Comorbidity was assessed using a questionnaireadaptation of the Charlson Index (higher score � greatercomorbidity) (16). High test–retest reliability and strong cor-relation with the medical record–based Charlson Index hasbeen demonstrated (16).
Physical activity was assessed using the Physical Activ-ity Scale for the Elderly (PASE), a self-report measure ofglobal activity that assesses recreational, occupational, andhousehold activities (higher score � greater activity) (17).PASE was designed to assess activities commonly engaged inby older persons, and its construct validity and test–retestreliability have been demonstrated in community-dwellingolder adults (17). Aerobic exercise was scored according to theamount of walking (for exercise), swimming, water aerobics,bicycling (including stationary), and exercise on aerobic equip-ment (stairmaster, rowing, or skiing machine) per week.
Psychological status was assessed using the mentalhealth and role-functioning emotional subscales of the 36-itemShort-Form (SF-36) (higher value � better). Criterion validityhas been demonstrated for these individual scales, with signif-icant and consistent associations with a range of validationcriteria (18). Reliability for the individual scales has beendemonstrated (19). Self-efficacy for lower extremity functionwas assessed using the lower extremity questions of theArthritis Self-Efficacy Scale function subscale (self-rating ofdegree of certainty in one’s ability to walk 100 feet on flatground in 20 seconds, walk 10 steps downstairs in 7 seconds,and get out of an armless chair without using hands forsupport) (higher value � better) (20). Construct and concur-rent validity and test–retest reliability for the subscales havebeen demonstrated in patients with arthritis (20). Social sup-port was assessed using the Medical Outcomes Study SocialSupport Survey (higher value � better) (21). This surveyrepresents several dimensions of support: emotional/informational, tangible, affectionate, and positive social inter-action. High convergent and discriminant validity of the items,construct validity, and reliability have been demonstrated inpatients with chronic conditions (21).
Physical function outcome from baseline to 3 years.Physical function was assessed at baseline and at 3 years byusing the Likert version of the WOMAC physical functionscale and the rate of chair-stand performance. The WOMAC isa disease-specific (for knee or hip OA) self-report instrumentwith 17 questions comprising the physical function scale. It isextensively validated and widely recommended and used instudies of individuals with knee OA (22,23). The possible rangeof the physical function scale is 0–68, and a higher scoreindicates worse function. The WOMAC scores were catego-rized using quintiles of the MAK cohort at baseline, rangingfrom individuals with the best WOMAC function scores tothose with the worst function, as follows: first quintile(WOMAC 0–7), second quintile (WOMAC 8–14), third quin-
PREDICTORS OF 3-YEAR PHYSICAL FUNCTION OUTCOME IN KNEE OA 3361

tile (WOMAC 15–22), fourth quintile (WOMAC 23–33), andfifth quintile (WOMAC �33).
As a task closely signifying knee status, chair-standperformance was assessed, i.e., time required for 5 repetitionsof rising from a chair and sitting down, using the protocoldescribed by Guralnik et al (24). Among community-dwellingelderly individuals, those with better performance in thischair-stand test had significantly less mobility-related disabilityand less disability in activities of daily living 4 years later (24).The rate of performance on the chair-stand test was used inour analysis; this value was expressed as the number of standsper minute calculated from the time required to complete 5chair stands. The use of rate allows the inclusion of individualswho cannot complete the test (i.e., those with a rate of 0). Thechair-stand rate was categorized using MAK cohort quintiles atbaseline, ranging from those with the worst chair-stand perfor-mance to those with the best, as follows: first quintile (�15.0),second quintile (�15.0 and �20.4), third quintile (�20.4 and�23.8), fourth quintile (�23.8 and �27.5), and fifth quintile(�27.5).
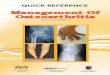
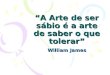
To characterize the baseline to 3-year function experi-ence of each participant, quintile grids were used. The quintilegrid captures practical, meaningful profiles of good and poorfunction over time. The WOMAC outcome grid is shown inFigure 1. The shaded squares represent a good baseline to3-year WOMAC function outcome, i.e., moving into a higherfunction group or remaining within the 2 highest functiongroups. Squares that are not shaded represent a poor baselineto 3-year WOMAC function outcome, i.e., moving into a lowerfunction group or remaining within the 3 lowest functiongroups. The chair-stand outcome grid is shown in Figure 2.Good and poor baseline to 3-year chair-stand outcomes arerepresented by shaded squares (moving into a faster chair-stand group or remaining within the 2 fastest groups) andnonshaded squares (moving into a slower group or remainingwithin the 3 slowest groups), respectively.
Statistical analysis. Analyses were restricted to indi-viduals who participated in both the baseline and 3-yearassessments and who did not undergo total knee replacementduring the study. Univariate screening was used to identify riskfactors related to poor baseline to 3-year function outcome,using logistic regression. Odds ratios (ORs) from continuousvariables are expressed per a specific clinically relevant incre-ment, rather than per measured unit, to aid interpretation. Forknee-specific variables, the maximal value of the 2 knees perparticipant was used for sample description and analyses.Adjusted ORs, controlling for age, BMI, knee pain intensity,disease severity, and other potential confounders, were esti-mated using multiple logistic regression.
The approach taken to consider additional potentialconfounders was based on scientific rationale, rather thanderived by statistical criteria. There were several potentialconfounders in the age–physical function relationship.Strength and proprioceptive acuity are known to decline withage (13,25,26). Alternatively, an age effect might be due to lessaerobic exercise, reduced self-efficacy, or greater comorbidity.Laxity is correlated, albeit modestly, with reduced strength(11) and greater malalignment (12). In theory, other psycho-social factors may confound the relationship between socialsupport and function outcome. An effect of aerobic exercisemay be mediated by strength, proprioceptive accuracy, mental
health, or self-efficacy. Self-efficacy may be a confounder inthe strength–function relationship.
To explore the robustness of the study results, sensi-tivity analyses included a subgroup analysis among the women,summing the values for the right and left knees (in contrast tousing the maximal value), and altering the definition of a goodoutcome defined from the quintile grid. Finally, the outcomeapproach taken afforded us the opportunity to describe indi-viduals with sustained high function and those with sustainedlow function.
RESULTS
Sample characteristics. Among 285 participants,257 (90%) completed the 3-year study. Reasons for notcompleting included incapacitation from another medi-cal condition (8 participants), death (7 participants),moving out of the region (6 participants), and anxietyover coming into downtown Chicago due to the events ofSeptember 11, 2001 (7 participants). Among the 257subjects who completed the study, 21 underwent totalknee replacement during the study period and wereexcluded from the analyses. The 236 participants whocompleted the study without total knee replacementrepresent the sample in this report. The participants had
Figure 1. Defining good and poor outcome as assessed by the physicalfunction scale of the Western Ontario and McMaster UniversitiesOsteoarthritis Index (WOMAC) (scale 0–68; higher score indicatesworse function). The baseline to 3-year outcome was “good” when aparticipant moved into a higher function group or remained within the2 highest function groups, and outcome was “poor” when a subjectmoved into a lower function group or remained within the 3 lowestfunction groups. Quintile groups were defined by the cut-off values ofthe WOMAC score quintiles at baseline.
3362 SHARMA ET AL

a mean � SD age of 68.6 � 10.8 years, and 172 (73%)were women. The sample was predominantly white(80% versus 16% African American, 3% Hispanic, and1% other), and 50% were married, 17% were single,15% were divorced, and 18% were widowed.
The mean BMI at baseline was 30.6 kg/m2 (�SD6.1), the mean knee pain intensity on a VAS was 38.9mm (�SD 26.8), the mean varus-valgus laxity was 5.9°(�SD 2.1), the mean quadriceps strength was 55.9 ft-lbs(�SD 29.2), the mean malalignment was 5.1° (�SD 3.4),and the mean proprioceptive inaccuracy was 2.4° (�SD1.8). The higher K/L disease severity grade (of the 2knees) was 2 in 43% of participants, 3 in 35%, and 4 in22%. The 28 participants who did not complete thestudy were similar at baseline to those who completedthe study without total knee replacement, except that thenonparticipants reported greater pain intensity (49.5mm versus 38.9 mm on a VAS).
Of the 236 participants, 113 had a good baselineto 3-year WOMAC function outcome, and 123 had apoor outcome. Participants with a good and poor base-line to 3-year chair-stand outcome numbered 80 and156, respectively. Univariate screening was used to iden-
tify the risk factors associated with a poor baseline to3-year function outcome. Risk factors screened includedbaseline age, sex, marital status, comorbidity, radio-graphic severity of knee OA, prevalence of bilateralversus unilateral knee OA, BMI, knee pain intensity,mechanical factors (varus-valgus laxity, malalignment),neuromuscular factors (proprioceptive inaccuracy,quadriceps strength, hamstring strength), activity level(overall physical activity, amount of aerobic exercise),and psychosocial factors (mental health, role-functioning emotional subscale, self-efficacy, social sup-port), as well as the baseline to 18-month change in eachfactor.
Relationship between candidate risk factors andWOMAC function outcome over 3 years. Table 1 pre-sents the mean value of each factor at baseline in boththe good and the poor WOMAC outcome groups. TheBMI, knee pain intensity, laxity, scores on mental health,self-efficacy, and social support, and amount of aerobicexercise per week were significantly different betweenthe 2 outcome groups. Categorical factors that did notdiffer between participants with good outcome andthose with poor outcome included sex (69% versus 79%female, respectively), marital status (50% versus 49%married, respectively), disease severity (higher K/L score
Figure 2. Defining good and poor outcome as assessed by the chair-stand performance rate (time required for 5 repetitions of rising froma chair and sitting down, calculated as the number of stands perminute) (higher rate indicates better function). The baseline to 3-yearoutcome was “good” when a participant moved into a higher functiongroup or remained within the 2 highest function groups, and outcomewas “poor” when a subject moved into a lower function group orremained within the 3 lowest function groups. Quintile groups weredefined by the cut-off values of the chair-stand rate quintiles atbaseline.
Table 1. Baseline risk factor levels in subjects with good versus poorWOMAC outcome*
Risk factorSubjects with goodWOMAC outcome
Subjects with poorWOMACoutcome
Age, years 69.4 � 10.4 67.6 � 11.4Comorbidity score 0.9 � 1.7 1.1 � 1.7BMI, kg/m2 29.9 � 6.2 31.6 � 5.9†Knee pain intensity, mm
on VAS35.8 � 28.3 42.7 � 24.5†
Laxity, degrees 5.6 � 2.1 6.2 � 2.2†Alignment, degrees 4.9 � 3.3 5.4 � 3.5Proprioceptive inaccuracy,
degrees2.2 � 1.3 2.6 � 2.3
Quadriceps strength, ft-lbs 57.5 � 28.4 54.0 � 30.2Hamstring strength, ft-lbs 34.9 � 18.1 32.1 � 19.6Mental health score 25.1 � 3.5 23.6 � 4.3‡Role-functioning
emotional score5.3 � 1.1 5.2 � 1.2
Self-efficacy score 22.9 � 7.8 19.7 � 8.7‡Social support score 62.2 � 20.4 56.5 � 17.7†Physical activity score 140.3 � 75.6 126.1 � 61.8Aerobic exercise per week
score6.0 � 3.4 5.1 � 3.0†
* Values are the mean � SD. WOMAC � Western Ontario andMcMaster Universities Osteoarthritis Index; BMI � body mass index;VAS � visual analog scale.† P � 0.05 versus good outcome group.‡ P � 0.01 versus good outcome group.
PREDICTORS OF 3-YEAR PHYSICAL FUNCTION OUTCOME IN KNEE OA 3363

of 2 in 47%, 3 in 35%, and 4 in 18% versus higher K/Lscore of 2 in 39%, 3 in 34%, and 4 in 27%, respectively),and prevalence of bilateral knee OA (89% in bothgroups).
Table 2 presents the unadjusted OR for a poorWOMAC outcome from baseline to 3 years, and the ORafter adjustment for age, BMI, knee pain intensity, anddisease severity. Baseline factors that significantly in-creased the likelihood of a poor WOMAC functionoutcome over 3 years were a higher BMI, greater kneepain intensity, and increased laxity, whereas better men-tal health, self-efficacy, and social support and moreaerobic exercise were protective factors. The only factorin which the baseline to 18-month change predicted theWOMAC outcome over 3 years was knee pain intensity.After adjustment, the OR for the baseline to 18-monthincrease in pain intensity notably increased to 1.48, froman unadjusted OR of 1.32. For the other factors, theORs either were not affected by adjustment or movedslightly toward unity.
Each of the following relationships persisted afterfurther adjustment for additional potential confounders:laxity–WOMAC outcome after adjustment for align-ment or strength (either as continuous or categoricalvariables), social support–WOMAC outcome after ad-justment for mental health or self-efficacy, and aerobicexercise–WOMAC outcome after adjustment forstrength, mental health, or self-efficacy.
Relationship between candidate risk factors andchair-stand performance outcome over 3 years. Table 3presents the mean value of each factor in the good
outcome and poor outcome groups according to chair-stand performance rating. Age, proprioceptive inaccu-racy, quadriceps strength, hamstring strength, scores onthe role-functioning emotional and self-efficacy sub-scales, and amount of aerobic exercise per week differedsignificantly between the good and poor outcomegroups. Categorical factors that did not differ betweenparticipants with good outcome and those with pooroutcome included sex (75% versus 72% female, respec-
Table 2. Factors associated with physical function outcome assessed by WOMAC*
Risk factorUnadjusted OR for poor
outcome/increment (95% CI)Adjusted OR for poor
outcome/increment (95% CI)
BMI, kg/m2 1.26/5 units (1.01–1.57) 1.14/5 units (0.89–1.46)†Knee pain intensity, mm on VAS 1.21/20 mm (1.00–1.47) 1.12/20 mm (0.90–1.40)‡0–18-month increase in knee
pain intensity, mm on VAS1.32/20 mm (1.06–1.65) 1.48/20 mm (1.12–1.95)‡
Laxity, degrees 1.48/3° (1.02–2.14) 1.58/3° (1.04–2.40)§Mental health score 0.62/5 points (0.44–0.87) 0.58/5 points (0.39–0.86)§Self-efficacy score 0.79/5 points (0.67–0.93) 0.80/5 points (0.65–0.98)§Social support score 0.86/10 points (0.75–0.98) 0.85/10 points (0.73–0.98)§Amount of aerobic exercise score 0.75/60 minutes (0.63–0.89) 0.84/60 minutes (0.69–1.02)§
* Odds ratios (ORs) are presented for poor Western Ontario and McMaster Universities OsteoarthritisIndex (WOMAC) outcome per given increment of each factor. Increments were based on clinicallymeaningful or achievable change, or if not known, 20% of the mean baseline value. 95% CI � 95%confidence interval; BMI � body mass index; VAS � visual analog scale.† Adjusted for age, knee pain intensity, and disease severity (higher Kellgren/Lawrence [K/L] grade of the2 knees).‡ Adjusted for age, BMI, and disease severity (higher K/L grade of the 2 knees).§ Adjusted for age, BMI, knee pain intensity, and disease severity (higher K/L grade of the 2 knees).
Table 3. Baseline risk factor levels in subjects with good versus poorchair-stand outcome*
Risk factor
Subjects withgood chair
standoutcome
Subjects withpoor chair
standoutcome
Age, years 65.9 � 11.6 70.1 � 10.2†Comorbidity score 0.9 � 1.5 1.1 � 1.8BMI, kg/m2 30.5 � 6.2 30.7 � 6.1Knee pain intensity, mm on VAS 37.6 � 27.7 39.5 � 26.5Laxity, degrees 5.7 � 2.1 6.2 � 2.2Alignment, degrees 5.1 � 3.4 5.1 � 3.4Proprioceptive inaccuracy degrees 2.1 � 1.2 2.5 � 2.0‡Quadriceps strength, ft-lbs 63.1 � 32.8 52.3 � 26.6‡Hamstring strength, ft-lbs 37.8 � 20.2 31.5 � 17.6‡Mental health score 24.8 � 4.0 24.3 � 3.9Role-functioning emotional score 5.4 � 1.0 5.2 � 1.1‡Self-efficacy score 23.3 � 7.8 20.6 � 8.4‡Social support score 60.9 � 19.5 59.1 � 19.4Physical activity score 141.4 � 70.7 130.2 � 69.7Aerobic exercise per week score 6.3 � 3.2 5.2 � 3.3‡
* Values are the mean � SD. See Table 2 for definitions.† P � 0.01 versus good outcome group.‡ P � 0.05 versus good outcome group.
3364 SHARMA ET AL

tively), marital status (51% versus 49% married, respec-tively), disease severity (higher K/L grade of 2 in 41%, 3in 36%, and 4 in 23% versus higher K/L grade of 2 in45%, 3 in 34%, and 4 in 21%, respectively), and preva-lence of bilateral knee OA (90% in both groups).
Table 4 presents the unadjusted OR for a poorchair-stand outcome, and the OR after adjustment forage, BMI, knee pain intensity, and disease severity. Therisk of a poor chair-stand performance outcome over 3years was increased by greater baseline age and propri-oceptive inaccuracy (the increase in risk approachedsignificance), whereas greater baseline quadricepsstrength and hamstring strength, better self-efficacy, andmore aerobic exercise were protective factors. None ofthe baseline to 18-month change variables were signifi-cant risk factors. For most factors, the OR was notaffected by adjustment or was slightly attenuated. Forthe strength variables, the attenuation was somewhatgreater.
Each of the following relationships persisted afterfurther adjustment for additional potential confounders:age–chair-stand outcome after adjustment for strength,proprioceptive acuity, aerobic exercise, reduced self-efficacy, or greater comorbidity, and aerobic exercise–chair-stand outcome after adjustment for strength, pro-prioceptive acuity, or mental health. The strength–function relationship did not persist after adjustment forself-efficacy (i.e., for quadriceps strength, the OR ad-justed for age, BMI, pain, disease severity, and self-efficacy was 0.95/20 ft-lbs, 95% CI 0.73–1.23)
Sex was not linked to outcome, and when theanalyses were restricted to women, the results weresimilar. The number of men in the cohort was notsufficient to examine them as a separate group. Resultswere minimally altered by adjusting for baseline quintile,
by considering the sum of values for the right and leftknee as the knee-specific independent variables (asopposed to the maximal value), or by changing thedefinition of good outcome to include those who re-mained in the 3 highest function quintiles (as opposed tothe 2 highest function quintiles).
Risk factor levels by subgroups of function out-come. The outcome approach used in this study affordedus the opportunity to provide some characterization ofthe individuals in the outcome categories according totheir baseline attributes. The outcome subgroups weredivided among individuals with knee OA who, over 3years, sustained a high level of function, improved infunction, declined in function, or sustained a low level offunction. The mean values of each factor are presentedfor each subgroup in Tables 5 (for WOMAC) and 6 (forchair-stand).
In terms of the baseline to 3-year WOMACoutcome, individuals with sustained high function hadthe best values for several factors, and had a strikinglylower BMI, less knee pain, and greater self-efficacycompared with those with sustained low function (Table5). Persons who persisted at a low level of function(compared with those who improved) appeared to havegreater laxity, less social support, and minimal change inthe intensity of pain between baseline and 18 months(versus a decrease in pain in those whose functionimproved), and they were performing less aerobic exer-cise on average.
With regard to the baseline to 3-year chair-standoutcome, individuals with sustained high function hadsuperior values for several factors, and had substantiallybetter self-efficacy and quadriceps strength (Table 6).Persons who persisted at a low level of function (com-
Table 4. Factors associated with physical function outcome assessed by chair-stand performance*
Risk factorUnadjusted OR for poor
outcome/increment (95% CI)Adjusted OR for poor
outcome/increment (95% CI)
Age, years 1.20/5 years (1.06–1.36) 1.34/5 years (1.15–1.57)†Proprioceptive inaccuracy, degrees 1.18/1° (0.98–1.42) 1.09/1° (0.88–1.34)‡Quadriceps strength, ft-lbs 0.78/20 ft-lbs (0.65–0.94) 0.88/20 ft-lbs (0.70–1.11)‡Hamstring strength, ft-lbs 0.70/20 ft-lbs (0.52–0.94) 0.86/20 ft-lbs (0.60–1.23)‡Role-functioning emotional score 0.86/1 unit (0.66–1.10) 0.99/1 unit (0.75–1.32)‡Self-efficacy score 0.78/5 points (0.62–0.97) 0.86/5 points (0.68–1.09)‡Amount of aerobic exercise score 0.82/60 minutes (0.71–0.97) 0.86/60 minutes (0.71–1.05)‡
* ORs are presented for poor chair-stand outcome per given increment of each factor. Increments werebased on clinically meaningful or achievable change, or if not known, 20% of the mean baseline value. SeeTable 2 for definitions.† Adjusted for BMI, knee pain intensity, and disease severity (higher K/L grade of the 2 knees).‡ Adjusted for age, BMI, knee pain intensity, and disease severity (higher K/L grade of the 2 knees).
PREDICTORS OF 3-YEAR PHYSICAL FUNCTION OUTCOME IN KNEE OA 3365

pared with those who improved) appeared to be olderand weaker, and were performing less aerobic exercise.
DISCUSSION
The likelihood of a poor function outcome asassessed by the WOMAC over 3 years in persons withknee OA was increased by the presence of greatervarus-valgus laxity, BMI, and knee pain intensity atbaseline and a larger baseline to 18-month increase inpain intensity, and was decreased by better baselinemental health, self-efficacy, and social support and moreaerobic exercise. The likelihood of a poor outcome asassessed by chair-stand performance was increased by anolder age and greater proprioceptive inaccuracy (ap-proaching significance), and was reduced by greaterstrength and self-efficacy and more aerobic exercise.The effect of strength was somewhat reduced by adjust-ing for age, pain, and BMI, and was lost after adjustingfor self-efficacy. The WOMAC and chair-stand perfor-mance rating identified different factors, supporting the
concept that self-report and performance measures eachcapture unique aspects of functioning and should not besubstituted for each other. The change in most riskfactors from baseline to 18 months did not predict theoutcome over 3 years, possibly reflecting the generallysmall amount of change between baseline and 18months.
The level of self-efficacy predicted the outcomesby both the self-report and the performance functionmeasures. Differences in self-efficacy between personswho sustained high function and those who declined infunction or sustained low function appeared larger thanfor any other factor. Our results are consistent withthose reported by Rejeski et al, who found, in theObservational Arthritis Study in Seniors (OASIS), thatin older persons with knee pain, self-efficacy predictedboth the self-reported and stair-climb performance out-comes, after adjusting for pain and strength (7). In thecurrent study, there was similarly no evidence of con-founding by either the intensity of pain or strength. In
Table 5. Baseline levels of risk factors within WOMAC outcome subgroups*
Risk factor
Stayed in high functionquintile group
(n � 48)
Moved tobetter group
(n � 84)
Moved toworse group
(n � 54)
Stayed in low functionquintile group
(n � 50)
BMI, kg/m2 27.7 � 4.7 31.1 � 6.6 31.1 � 5.8 32.1 � 5.9†Knee pain intensity, mm on VAS 18.1 � 17.4 45.9 � 28.4 36.4 � 22.5 49.6 � 25.0†0–18-month increase in pain 1.8 � 18.8 �9.9 � 26.3 2.0 � 23.9 2.8 � 24.1Laxity, degrees 5.7 � 1.8 5.6 � 2.2 5.9 � 2.1 6.5 � 2.3‡Mental health score 26.4 � 2.6 24.3 � 3.8 24.1 � 3.9 23.1 � 4.7†Self-efficacy score 26.7 � 4.6 21.0 � 8.4 22.1 � 8.1 17.1 � 8.6†Social support score 62.9 � 19.0 61.8 � 21.2 59.3 � 17.7 53.5 � 17.4‡Aerobic exercise per week score 6.1 � 3.2 6.0 � 3.6 5.1 � 3.1 5.0 � 3.0
* Values are the mean � SD. See Table 2 for definitions.† P � 0.0001 versus those who stayed in the high function quintile group.‡ P � 0.05 versus those who stayed in the high function quintile group.
Table 6. Baseline levels of risk factors within chair-stand outcome subgroups*
Risk factor
Stayed in high functionquintile group
(n � 33)
Moved tobetter group
(n � 47)
Moved toworse group
(n � 84)
Stayed in low functionquintile group
(n � 72)
Age, years 66.7 � 10.8 65.2 � 12.2 69.6 � 10.1 70.7 � 10.3Proprioceptive inaccuracy, degrees 1.5 � 1.0 2.5 � 1.2 2.4 � 1.9 2.7 � 2.1†Quadriceps strength, ft-lbs 73.0 � 31.1 56.2 � 32.6 60.0 � 25.2 43.3 � 25.4‡Hamstring strength, ft-lbs 43.2 � 19.2 34.1 � 20.2 36.4 � 16.8 25.8 � 17.0‡Self-efficacy score 27.0 � 4.8 20.4 � 8.5 22.9 � 7.1 18.1 � 9.1‡Aerobic exercise per week score 7.0 � 3.0 5.8 � 3.3 5.4 � 3.3 5.0 � 3.3§
* Values are the mean � SD.† P � 0.001 versus those who stayed in high function quintile group.‡ P � 0.0001 versus those who stayed in high function quintile group.§ P � 0.01 versus those who stayed in high function quintile group.
3366 SHARMA ET AL

addition, we found no evidence of confounding bymental health status or aerobic exercise.
This study is the first to show evidence of therelationship between greater baseline varus-valgus laxityand increased odds of a poor baseline to 3-yearWOMAC function outcome. Both persons who sus-tained high function and those who improved had lowerlevels of laxity. Cross-sectional relationships betweenlaxity and function (see ref. 11, which also involves thecohort of the current study), and between symptoms ofinstability and function (27) have been reported in kneeOA. Varus-valgus laxity increased the likelihood of OAafter ligament injury (28,29), was worse in persons withOA (even in their nonarthritic knees) than in elderlycontrols, and was made worse by aspects of the disease(9). The mechanism of the laxity–function relationshipmay, in theory, be related to symptoms of pain orinstability, the effects of laxity on knee function, or both.We found no evidence of mediation by pain, or con-founding by age, strength, or alignment.
The link between aerobic exercise and functionoutcome is consistent with the long-term benefit ofaerobic exercise on disability in activities of daily living,as demonstrated in the Fitness, Arthritis, and SeniorsTrial (30), and is consistent with the cross-sectionalrelationship between low aerobic capacity and poorfunction (6). Those subjects who sustained high functionwere performing the greatest amount of aerobic exer-cise. Adjustment for each of several factors, BMI, kneepain intensity, mental health, proprioceptive inaccuracy,self-efficacy, or strength, did not attenuate the relation-ship between aerobic exercise and function outcome,suggesting that aerobic exercise did not act throughthese factors, at least as measured here. The effect ofaerobic exercise may be mediated by improvement inaerobic capacity or aspects of neuromuscular functionnot captured by strength and the accuracy of knee-motion detection.
Specific, coordinated quadriceps and hamstringactivity is required to achieve the knee and hip move-ments that occur during the chair-stand task. Given themuscle specificity of this task, and the abundant evi-dence of a cross-sectional relationship between strengthand function (6,11,31–35), it is surprising that the pro-tective effect of strength was not greater and that therewas attenuation after adjustment. However, these resultsare consistent with the relatively modest effect ofstrengthening exercise on physical function in the longterm (36), and with the finding, in both of the studiesthat have considered this question, that strength doesnot protect against knee OA disease progression (14,37).
As a muscle parameter, strength may not be the bestsurrogate for the vast contribution from muscle to jointfunction and task performance; other measures of mus-cle activity may be more closely related to the risk ofpoor physical function.
The strength–function outcome relationship waslost after additional adjustment for self-efficacy. Ourresults support a close relationship between strength,knee pain intensity, and self-efficacy in their effect onphysical function in knee OA. Pain may acutely reducethe maximal voluntary contraction and lead to chronicactivity revision or avoidance. A downward spiral ofpain, weakness, and reduced self-efficacy may lead tosubstantial reduction in activity. In support of thisparadigm, subjects with knee OA and pain were weakerthan those without pain (34), and in OASIS, there wasevidence of an interaction between strength and pain(38) as well as strength and self-efficacy (7), in evaluat-ing the effects on physical function.
Proprioceptive inaccuracy, measured as a greaterdelay before detecting slow, passive knee motion, wasassociated with a poor chair-stand performance outcome(approaching significance). Various approaches to as-sess joint-position sense have been developed and ap-plied in clinical studies, which reflect the status ofdifferent pathways that contribute to proprioceptiveawareness under a variety of circumstances. A relation-ship between proprioceptive inaccuracy assessed atstudy baseline and physical function over the ensuingyears has not previously been reported. Proprioceptiveaccuracy declines with age (13), was worse in personswith OA even in their nonarthritic knee than in healthyelderly subjects (10), and was correlated with physicalfunction in cross-sectional studies of knee OA (13,39–41). The results of the current study are noteworthy,especially since this was a passive test; dynamic joint-position sense inaccuracy may play a greater role inphysical tasks and activities and more strongly predictphysical function outcome.
Knee alignment strongly influences the risk oftibiofemoral OA disease progression (12). In the currentstudy, malalignment as a continuous variable was notsignificantly linked to function outcome. However, as wehave previously reported, the malalignment–functionrelationship in knee OA appears to be nonlinear; par-ticipants with 2 knees that had alignment of �5° (eithervarus or valgus) were more likely to experience a poorfunction outcome than were those with both knees moreneutrally aligned (12).
Both baseline knee pain intensity and the base-line to 18-month change in pain predicted function
PREDICTORS OF 3-YEAR PHYSICAL FUNCTION OUTCOME IN KNEE OA 3367

outcome. There is a paucity of information concerningthe longitudinal relationship between pain intensity andphysical function in knee OA. In the OASIS study,baseline knee pain intensity during ambulation andtransfer predicted a decline in performance during stair-climb and car tasks, respectively, but not self-reportedfunction (38). The relationship between knee pain in-tensity and function decline was not significant afteraccounting for self-efficacy and the self-efficacy–strength interaction (7). In the National Health andNutrition Examination Survey I, presence of knee painpredicted difficulty in mobility, transfer, and instrumen-tal activities of daily living 10 years later (42). Otherreports describe a cross-sectional relationship betweenknee pain and function in those with knee OA (6,43) andin studies not limited to persons with OA (35,44).
Age predicted the chair-stand performance out-come, which is consistent with the finding that age wasassociated with an increased risk of losing mobility overthe next 4 years in the Established Populations forEpidemiologic Studies of the Elderly (45). The currentstudy is notable in 2 ways. First, a longitudinal relation-ship between age and function outcome, adjusting forcomorbidity, was demonstrated in a cohort of individualswith established knee OA. Second, the examination ofneuromuscular factors afforded an opportunity to ex-plore mechanisms of the age effect. Although greaterage is associated with reductions in strength and propri-oceptive acuity, the age–function relationship did notappear to be mediated by these factors. It remainspossible that age exerts its effect via other neuromuscu-lar factors, i.e., sensory and/or motor impairments notcaptured by strength or the accuracy of detection ofpassive motion.
We found a relationship between BMI at baselineand the WOMAC function outcome over 3 years. Alongitudinal relationship between BMI and physicalfunction in individuals with knee OA has not beenpreviously reported. In cross-sectional studies not lim-ited to individuals with OA, obesity was associated withself-reported difficulty with activities (by Health Assess-ment Questionnaire, in the lower limb) even afteradjusting for pain (43), and higher body weight wasassociated with slower task performance (35).
A relationship between depressive symptoms andphysical function has been described in longitudinalstudies not limited to individuals with arthritis, as sum-marized by Ormel et al (46), and in cross-sectionalstudies of knee OA (31,34,47,48). The demonstration inthe current study that the status of mental healthpredicts subsequent physical function is important, given
how function assessment might be biased by depressivesymptoms.
The approach of the current study provided anopportunity to describe persons with knee OA in specificoutcome subgroups. The values presented in Tables 5and 6 are unadjusted, but in this format, they illustratethe attributes of individuals who sustain high function orlow function as they might be encountered in clinical orscreening settings. Those who sustained high functionhad the best values for most factors, but their highself-efficacy, low BMI, low pain intensity, and greaterlevel of aerobic exercise were especially noteworthy.
The distinctive characteristics of the functionsubgroups would not have been evident if “change” in afunction measure had been the defined outcome. Thechoice, in some observational studies, to focus on changemay be intended as a way of inferring causation. How-ever, in OA, change may require several years. Thenumber of individuals who showed no change in func-tion over 3 years was substantial: 98 (42%) remained inthe same WOMAC group, and 105 subjects (44%)remained in the same chair-stand group. A focus onchange ignores those with persistently high or lowfunction, and thus effectively lumps these individualstogether in the same group and reduces the ability todetect the effects of factors responsible for an individu-al’s state of function. In a chronic disease that is slow toevolve, factors related to persistent low- or high-functionstates are of particular importance to the developmentof prevention or intervention programs.
This study has limitations. It would have been ofvalue to separately analyze the effect of a risk factor onchange in function status and on persistence in a givengroup. However, the modeling to achieve this requiredproblematic post hoc exclusions of groups of subjects.Our approach gave weight to the need to identify factorslinked to the persistence of low-function states or de-cline, both of which are problematic to the individual.We were able to confirm the findings separately inwomen, but not in men, due to the smaller number ofmen in the cohort. This confirmation in women wasimportant, given that the impact of knee OA on physicalfunction has been shown to be greater in older womenthan in other age and sex subgroups (42). The smallamount of change in most factors between baseline and18 months limited our ability to evaluate the impact ofchange in a given factor with outcome. Also, it is possiblethat a larger sample may have enabled us to detect aneffect of the 18-month data. The absence of a linkbetween comorbidity and function outcome may be
3368 SHARMA ET AL

related to the small number of comorbidities present, onaverage, in this cohort.
These results have implications for future studiesand for strategies to optimize physical function in kneeOA. Treatment of pain is believed to be the crux ofdisability prevention in knee OA, and the results of thecurrent study provide additional, longitudinal supportfor this. However, several modifiable factors were iden-tified that were independently linked to function out-come after adjusting for pain intensity, which supports amultifaceted approach. Results of short-term studieshave suggested the greater benefit of combined ap-proaches (e.g., acupuncture/diet/exercise versus paintherapy alone [49]). Moreover, the effect sizes forstrengthening interventions appear to be enlarged byincorporating pain management, attention to psychoso-cial factors, self-management, or aerobic exercise intothe intervention (50,51).
The current study supports a key place for self-efficacy enhancement in strategies to optimize physicalfunction. Components of perceived self-efficacy includeskill, experience, general self-worth, and motivation(20); each of these is addressed in self-managementeducation, which has been shown to be beneficial inshort-term studies in arthritis patients (52). Our resultssuggest that aerobic exercise may have greater impactthan a general increase in physical activity. Althoughorthoses specifically for varus-valgus laxity may havevalue and should be developed, novel dynamic ap-proaches are also emerging. Fitzgerald et al tailoredagility and perturbation training techniques, which wereused for anterior cruciate ligament deficiency, to addressthe functional instability of individuals with knee OA(27). Such techniques may also enhance periarticularmuscle activity and dynamic proprioceptive acuity. Theeffect of exercise that is restricted to strengthening hasbeen modest in long-term trials (36). Although strengthmaintenance is important, parameters of periarticularmuscle function other than strength may better predict agood physical function outcome and may constitute abetter target for disability-prevention strategies.
In conclusion, factors placing individuals withknee OA at greater risk of a poor function outcome byat least 1 of the 2 function measures included the localfactors laxity and proprioceptive inaccuracy, as well asage, BMI, and knee pain intensity. Factors protectingagainst a poor function outcome included strength, thepsychosocial factors mental health, self-efficacy, andsocial support, and the activity factor amount of aerobicexercise per week. The identification of these factorsdescribes individuals with knee OA who are at greater
risk of a poor physical function outcome and providespossible targets for rehabilitative and self-managementstrategies to prevent disability.
REFERENCES
1. Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang Y,Wilson PW, et al. The effects of specific medical conditions on thefunctional limitations of elders in the Framingham Study. Am JPublic Health 1994;84:351–7.
2. Jette AM, Haley SM, Coster WJ, Kooyoemjian JT, Levenson S,Heeren T. Late life Function and Disability Instrument (FDI). JGerontol Med Sci 2002;57A:M209–16.
3. Guccione AA. Osteoarthritis, comorbidity, and physical disability.In: Hamerman D, editor. Osteoarthritis: public health implicationsfor an aging population. Baltimore: The Johns Hopkins UniversityPress; 1997. p. 84–98.
4. Guccione AA, Felson DT, Anderson JJ. Defining arthritis andmeasuring functional status in elders: methodological issues in thestudy of disease and disability. Am J Public Health 1990;80:945–9.
5. Bandura A. Self-efficacy mechanism in physiological activationand health-promoting behavior. In: Madden J, editor. Neurobiol-ogy of learning, emotion, and affect. New York: Raven Press;1991. p. 229.
6. Rejeski WJ, Craven T, Ettinger WH, McFarlane M, Shumaker S.Self-efficacy and pain in disability with osteoarthritis of the knee.J Gerontol B Psychol Sci Soc Sci 1996;51:P24–9.
7. Rejeski WJ, Miller ME, Foy C, Messier S, Rapp S. Self-efficacyand the progression of functional limitations and self-reporteddisability in older adults with knee pain. J Gerontol B Psychol SciSoc Sci 2001;56:S261–5.
8. Tetsworth K, Paley D. Malalignment and degenerative arthro-pathy. Orthop Clin North Am 1994;25:367–77.
9. Sharma L, Lou C, Felson DT, Dunlop DD, Kirwan-Mellis G,Hayes KW, et al. Laxity in healthy and osteoarthritic knees.Arthritis Rheum 1999;42:861–70.
10. Sharma L, Pai Y-C, Holtkamp K, Rymer WZ. Is knee jointproprioception worse in the arthritic knee versus the unaffectedknee in unilateral knee osteoarthritis? Arthritis Rheum 1997;40:1518–25.
11. Sharma L, Hayes KW, Felson DT, Buchanan TS, Kirwan-Mellis G,Lou C, et al. Does laxity alter the relationship between strengthand physical function in knee osteoarthritis? Arthritis Rheum1999;42:25–32.
12. Sharma L, Song J, Felson DT, Cahue S, Shamiyeh E, Dunlop DD.The role of knee alignment in disease progression and functionaldecline in knee osteoarthritis. JAMA 2001;286:188–95.
13. Pai Y-C, Rymer WZ, Chang RW, Sharma L. Effect of age andosteoarthritis on knee proprioception. Arthritis Rheum 1997;40:2260–5.
14. Sharma L, Dunlop D, Cahue S, Song J, Hayes K. Quadricepsstrength and osteoarthritis progression in malaligned and laxknees. Ann Intern Med 2003;138:613–9.
15. Dieppe P, Altman RD, Buckwalter JA, Felson DT, Hascall V,Lohmander LS, et al. Standardization of methods used to assessthe progression of osteoarthritis of the hip or knee joints. In:Kuettner KE, Goldberg VM, editors. Osteoarthritic disorders.Rosemont (IL): American Academy of Orthopaedic Surgeons;1995. p. 481–96.
16. Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Cancomorbidity be measured by questionnaire rather than medicalrecord review? Med Care 1996;34:73–84.
17. Washburn RA, Smith KW, Jette AM, Janney CA. The PhysicalActivity Scale for the Elderly (PASE): development and evalua-tion. J Clin Epidemiol 1993;46:153–62.
PREDICTORS OF 3-YEAR PHYSICAL FUNCTION OUTCOME IN KNEE OA 3369

18. Ware JE Jr, Snow KK, Kosinski M, Gandek B. SF-36 healthsurvey: manual and interpretation guide. Boston: The HealthInstitute, New England Medical Center; 1993.
19. McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD. The MOS 36item Short-Form Health Survey (SF-36). III. Tests of data quality,scaling assumptions, and reliability across diverse patient groups.Med Care 1994;32:40–66.
20. Lorig K, Chastain RL, Ung E, Shoor S, Holman HR. Developmentand evaluation of a scale to measure perceived self-efficacy inpeople with arthritis. Arthritis Rheum 1989;32:37–44.
21. Sherbourne CD, Stewart AL. The MOS social support survey. SocSci Med 1991;32:705–14.
22. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt L.Validation study of WOMAC: a health status instrument formeasuring clinically important patient relevant outcomes followingtotal hip and knee arthroplasty in osteoarthritis. J Ortho Rheum1988;1:95–108.
23. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW.Validation study of WOMAC: a health status instrument formeasuring clinically important patient relevant outcomes to anti-rheumatic drug therapy in patients with osteoarthritis of the hip orknee. J Rheumatol 1988;15:1833–40.
24. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB.Lower-extremity function in persons over the age of 70 years as apredictor of subsequent disability. N Engl J Med 1995;332:556–61.
25. Stoll T, Huber E, Seifert B, Michel BA, Stucki G. Maximalisometric muscle strength: normative values and gender-specificrelation to age. Clin Rheumatol 2000;19:105–13.
26. Baumgartner RN, Stauber PM, McHugh D, Koehler KM, GarryPJ. Cross-sectional age differences in body composition in persons60� years of age. J Gerontol 1995;50A:M307–16.
27. Fitzgerald GK, Childs JD, Ridge TM, Irrgang JJ. Agility andperturbation training for a physically active individual with kneeosteoarthritis. Phys Ther 2002;82:372–82.
28. Kannus P. Nonoperative treatment of grade II and III sprains ofthe lateral ligament compartment of the knee. Am J Sports Med1989;17:83–8.
29. Kannus P. Long-term results of conservatively treated medialcollateral ligament injuries of the knee joint. Clin Orthop 1988;226:103–12.
30. Penninx BWJ, Messier SP, Rejeski WJ, Williamson JD, DiBari M,Cavazzini C, et al. Physical exercise and the prevention of disabilityin activities of daily living in older persons with osteoarthritis. ArchIntern Med 2001;161:2309–16.
31. Van Baar ME, Dekker J, Lemmens JAM, Oostendorp RAB,Bijlsma JWJ. Pain and disability in patients with osteoarthritis ofhip or knee: the relationship with articular, kinesiological, andpsychological characteristics. J Rheumatol 1998;25:125–33.
32. McAlindon TE, Cooper C, Kirwan JR, Dieppe PA. Determinantsof disability in osteoarthritis of the knee. Ann Rheum Dis 1993;52:258–62.
33. Fisher NM, Pendergast DR, Gresham GE, Calkins E. Musclerehabilitation: its effect on muscular and functional performanceof patients with knee osteoarthritis. Arch Phys Med Rehabil1991;72:367–74.
34. O’Reilly S, Jones A, Muir KR, Doherty M. Quadriceps weaknessin knee osteoarthritis: the effect on pain and disability. AnnRheum Dis 1998;57:588–94.
35. Ling SM, Fried LP, Garrett ES, Fan M-Y, Rantanen T, BathonJM. Knee osteoarthritis compromises early mobility function: theWomen’s Health and Aging Study II. J Rheumatol 2003;30:114–20.
36. Ettinger WH, Burns R, Messier SP, Applegate W, Rejeski WJ,Morgan T, et al. A randomized trial comparing aerobic exerciseand resistance exercise with a health education program in olderadults with knee osteoarthritis: the Fitness Arthritis and SeniorsTrial. JAMA 1997;277:25–31.
37. Brandt KD, Heilman DK, Slemenda C, Katz BP, Mazzuca SA,Braunstein EM, et al. Quadriceps strength in women with radio-graphically progressive osteoarthritis of the knee and those withstable radiographic changes. J Rheumatol 1999;26:2431–7.
38. Miller ME, Rejeski WJ, Messier SP, Loeser RF. Modifiers ofchange in physical functioning in older adults with knee pain: theObservational Arthritis Study in Seniors (OASIS). Arthritis CareRes 2001;45:331–9.
39. Skinner HB, Barrack RL, Cook SD, Haddad RJ Jr. Joint positionsense in total knee arthroplasty. J Orthop Res 1984;1:276–83.
40. Marks R. Proprioceptive sensibility in women with normal andosteoarthritic knee joints. Clin Rheumatol 1993;12:170–5.
41. Marks R. An investigation of the influence of age, clinical status,pain and position sense on stair walking in women with osteoar-throsis. Int J Rehabil Res 1994;17:151–8.
42. Davis MA, Ettinger WH, Neuhaus JM, Mallon KP. Knee osteo-arthritis and physical functioning: evidence from the NHANES IEpidemiologic Followup Study. J Rheumatol 1991;18:591–8.
43. Odding E, Valkenburg HA, Algra D, Vandenouweland FA,Grobbee DE, Hofman A. Associations of radiological osteoarthri-tis of the hip and knee with locomotor disability in the RotterdamStudy. Ann Rheum Dis 1998;57:203–8.
44. Jordan J, Luta G, Renner J, Dragomir A, Hochberg M, Fryer J.Knee pain and knee osteoarthritis severity in self-reported taskspecific disability: the Johnston County Osteoarthritis Project.J Rheumatol 1997;24:1344–9.
45. Guralnik JM, LaCroix AZ, Abbott RD, Berkman LF, SatterfieldS, Evans DA, et al. Maintaining mobility in late life. I. Demo-graphic characteristics and chronic conditions. Am J Epidemiol1993;137:845–57.
46. Ormel J, Rijsdijk FV, Sullivan M, van Sonderen E, Kempen GIJM.Temporal and reciprocal relationship between IADL/ADL disabil-ity and depressive symptoms in late life. J Gerontol B Psychol SciSoc Sci 2002;57:P338–47.
47. Salaffi F, Cavalieri F, Nolli M, Ferracciolli G. Analysis of disabilityin knee osteoarthritis: relationship with age and psychologicalvariables but not with radiographic score. J Rheumatol 1991;18:1581–6.
48. Summers MN, Haley WE, Reveille JD, Alarcon GS. Radiographicassessment and psychologic variables as predictors of pain andfunctional impairment in osteoarthritis of the knee or hip. Arthri-tis Rheum 1988;31:204–9.
49. Huang MH, Chen CH, Chen TW, Weng MC, Wang WT, WangYL. The effects of weight reduction on the rehabilitation ofpatients with knee osteoarthritis and obesity. Arthritis Care Res2000;13:398–405.
50. Van Baar ME, Assendelft WJJ, Dekker J, Oostendorp RA,Bijlsma JW. Effectiveness of exercise therapy in patients withosteoarthritis of the hip or knee: a systematic review of random-ized clinical trials. Arthritis Rheum 1999;43:1361–9.
51. Baker K, McAlindon T. Exercise for knee osteoarthritis. CurrOpin Rheumatol 2000;12:456–63.
52. Bodenheimer T, Lorig K, Holman H, Grumbach K. Patientself-management of chronic disease in primary care. JAMA 2002;288:2469–75.
3370 SHARMA ET AL