Embed Size (px)
Citation preview
Dr.manjunathDr.manjunath
Associate professorAssociate professorSSMCSSMC
Tumkur Tumkur
History History • 1961 - thalidomide disaster• 1968 – WHO pilot research project for
international drug monitoring• 1971 – WHO meeting
1.to advocate establishment of national centers for drug monitoring2.to provide guidelines3.to identify the contribution that national centers might take to the international system

Contd.Contd.• 1984 – international society of
pharmacoepidemiology • 1992 – european society of
pharmacovigilance• 2002 – WHO pharmacovigilance• 2004 – national pharmacovigilance
advisory committee (NHAC) with DGHS as chairman and drug controller general of india as member secretary
• 24 peripheral centers, 6 regional centers and 2 zonal centers

Widening horizonsWidening horizons• Illegal sale of medicines and drugs of
abuse over internet• Increasing self medication practices• Widespread manufacture and sale of
counterfeit and substandard medicines• Increasing use of traditional medicines
outside the confines of traditional culture of use
• Increasing use medicines of different systems with potential for drug interactions
Post marketing surveillancePost marketing surveillance
• Monitoring of drug safety after introducing into the market through various systems
• Need 1.To assess risk benefit ratio2.To confirm safety and efficacy 3.To detect less common
adverse effects
Methods of surveillanceMethods of surveillance
• Anecdotal reporting• Voluntary reporting• Intensive event reporting• Cohort studies (prospective)• Case control studies (retrospective)• Population statistics• Meta-analysis
Organizations involvedOrganizations involved• WHO – collaborating center for international drug
monitoring is Uppsala monitoring centre provides activities and events in PV
• CIOMS – council for international organizations of medical sciences-safety information communication between regulators and industries.
• ICH – international conference on harmonization discusses scientific and technical aspects of product registration.
• WHO-ART – WHO adverse reaction terminology for coding clinical information to drug therapy.

Frequency of ADRFrequency of ADR
• Very common>=1/10• Common >=1/100 and <1/10• Uncommon >=1/1000 and <1/100• Rare >=1/10000 and
<1/1000• Very rare <1/10000

Causality assessmentCausality assessment• Certain : proven on dechallenge and
rechallenge• Probable : dechallenge confirms.cannot
rechallenge• Possible : can be explained by concurrent
disease or other drugs• Unlikely : not documented in literature• Unclassified : additional data is awaited so
not documented• Unclassifiable : additional data has come
but not fit into any categories

Methods of causality Methods of causality assessmentassessment
• WHO assessment scale• Naranjo’s scale • European ABO system• Karch and Lasagna’s scale• Kramer scale• Bayesian network• Yale logarithm• Spanish imputation system
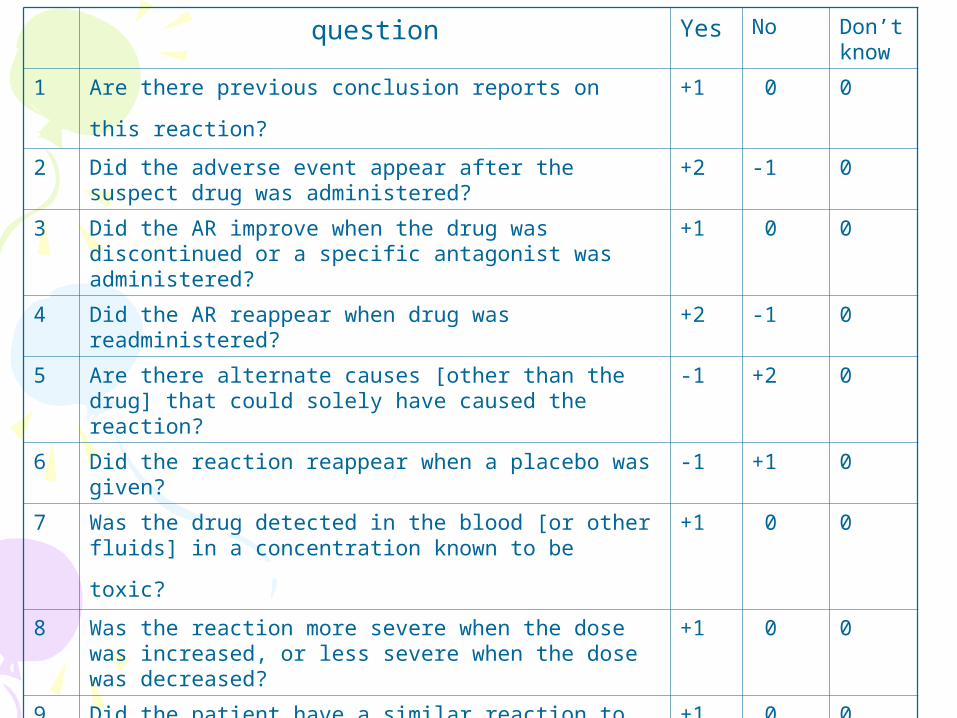
question Yes No Don’t know
1 Are there previous conclusion reports on this
reaction? +1 0 0
2 Did the adverse event appear after the suspect drug was administered?
+2 -1 0
3 Did the AR improve when the drug was discontinued or a specific antagonist was administered?
+1 0 0
4 Did the AR reappear when drug was readministered? +2 -1 0
5 Are there alternate causes [other than the drug] that could solely have caused the reaction?
-1 +2 0
6 Did the reaction reappear when a placebo was given?
-1 +1 0
7 Was the drug detected in the blood [or other fluids]
in a concentration known to be toxic? +1 0 0
8 Was the reaction more severe when the dose was increased, or less severe when the dose was decreased?
+1 0 0
9 Did the patient have a similar reaction to the same
or similar drugs in any previous exposure? +1 0 0
10 Was the adverse event confirmed by objective evidence?
+1 0 0

InterpretationInterpretation
• > 9 = definite• 5-8 = probable• 1-4 = possible• 0 = unlikely

Schedule Y requirementSchedule Y requirement• Unsuspected adverse event is
communicated from1.Sponsor to regulatory authorities
within 14 days2. Investigator to sponsor within 24
hours3. Investigator to ethics committee
within 7 days

Partners in Partners in pharmacovigilancepharmacovigilance
• The WHO quality assurance and safety : medicines team
• The uppasala monitoring centre• National pharmacovigilance centres• The pharmaceutical industry• Hospitals and academia• Health professionals• Patients • Others partners

Benefits of monitoringBenefits of monitoring• Improvement in patient care and safety in
relation to use of medicines and interventions.• Improvement of public health and safety.• Assessment of benefit, harm, effectiveness and
risk of medicines.• Encouragement of safe rational and more cost
effective use of medicines• Increase public awareness through
communication• Education and clinical training in pharacovigilance• Empowerment and involvement of practitioners,
patients and public

How to recognize ADRHow to recognize ADR• Ensure the medicine ordered is the medicine
received and actually taken by the patient.• Verify the onset of suspected ADR was after the
drug was taken, not before and discuss carefully the observation made by the patient.
• Determine the time interval between the beginning of drug treatment and the onset of event.
• Evaluate the suspected ADR after discontinuing the drugs or reducing the dose and monitor the patient’s status. If appropriate restart and monitor the recurrence.
• Analyze the alternative causes that could on their own have caused the reaction.

Contd.Contd.
• Use relevant up to date literature and personal experience on the drugs and ADR to verify previous reports on the reaction-through pharmacovigilance center and drug information center.
• Report any suspected ADR to the reporting center in the hospital or national ADR center.

Ethics in pharmacovigilanceEthics in pharmacovigilance• The Erice declaration provides framework of values and
practice for collection, analysis and subsequent communication of drug safety issues.
• It asserts scientific and clinical issues on the one hand and right of the public to be openly and fully informed on the other.
• It requires the active commitment of all involved regulators, policy makers, health personnel, journalists and (not last) pharmaceutical manufacturers.
• Information about drug safety programmes should be easily available to the public so that the central role of patient in safe and rational use of drugs is understood.
• Available information is not always reliable and scientifically valid. Direct advertising to the consumer resulting self medication, illicit sale of medicines over internet and over prescribing by doctor on demand.

The Erice Declaration(1997)The Erice Declaration(1997)• Challenges all these players
– Public health administration– Health professionals– The pharmaceutical industry– Government– Drug regulators– The media– Consumers to strive towards the highest ethical,
professional and scientific standards in protecting and promoting the safe use of medicines
The declaration urges governments and others involved in determining policies relating to the benefit, harm, effectiveness and risk of medicines to account for what they communicate to the public and patients.

Protecting patient Protecting patient confidentialityconfidentiality

Pharmacovigilance in Pharmacovigilance in clinical practiceclinical practice

Educational strategiesEducational strategies• Integrating pharmacovigilance in UG
education• Basic training of health professionals• Training of health workers• Consumer education and information• Drug bulletins to prescribers and
consumers• Drug information centers to be established

What is ADR monitoring ?What is ADR monitoring ?
• Systemically collecting information about adverse drug experiences with the aim of, through feed back to the parties involved, contribute to continuously improving drug therapy.

Aim : To detectAim : To detect
• Serious unexpected ADRs• Increased or unexpectedly high
frequency of known significant ADRs• To prepare list of ADRs not
previously reported• To disseminate the information
through regular bulletins, reports, and articles in the press
Need for monitoringNeed for monitoring• Short coming of premarketing studies-which
reveal most common and acute untoward effect
• Increase cost of patient care• Medication : 10-57% is self medication• Our country has vast population, poverty
and rich research ground• Accelerated approval and rapid introduction
of new drugs• Paucity of ADR data

Who reportsWho reports ? ?
• Doctors-hospital level,MO from PHC,GP’s
• Dentists • Drug manufacturers• Pharmacists and nurses

Types of ADRTypes of ADRType Type of
effectFeatures examples
A Augmented Common, predictable, low mortality
Bradycardia–β-blockers
B Bizarre Uncommon, unpredictable, high morbidity & high mortality
Anaphylaxis - Penicillin
C Chronic Dose related & time related Dyskinesia - Levodopa
D Delayed Time Related Teratogenesis
E End of use Withdrawal of chronic therapy abruptly
Corticosteroids
F Failure Unexpected failure of therapy Oral contraceptive failure - Rifampin

What to reportWhat to report ? ?• New drugs – all suspected adverse
reaction• Established drugs
- All serious reactions-well recognized- All reactions to vaccines- Unexpected high frequency of a known adverse reaction- All reactions to pregnant & lactating women including new born

Where to reportWhere to report ? ?
• Nearest ADR monitoring centers• Peripheral centers• Regional centers national center
at new Delhi• Directly on internet
www.fda.gov/MedWatch

Reasons not to reportReasons not to report• Uncertain association• Too trivial to report• Too well known to report• Unaware- existence of national center• Unaware- of the need of to report of ADRs• Not enough time• Non availability of ADR forms• Too bureaucratic• Legal issues• Lack of feed back

Thank youThank youDr.manjunathDr.manjunath





























