Embed Size (px)
Citation preview
Pharmacotherapy of diabetes mellitus
台大藥理所 蘇銘嘉老師
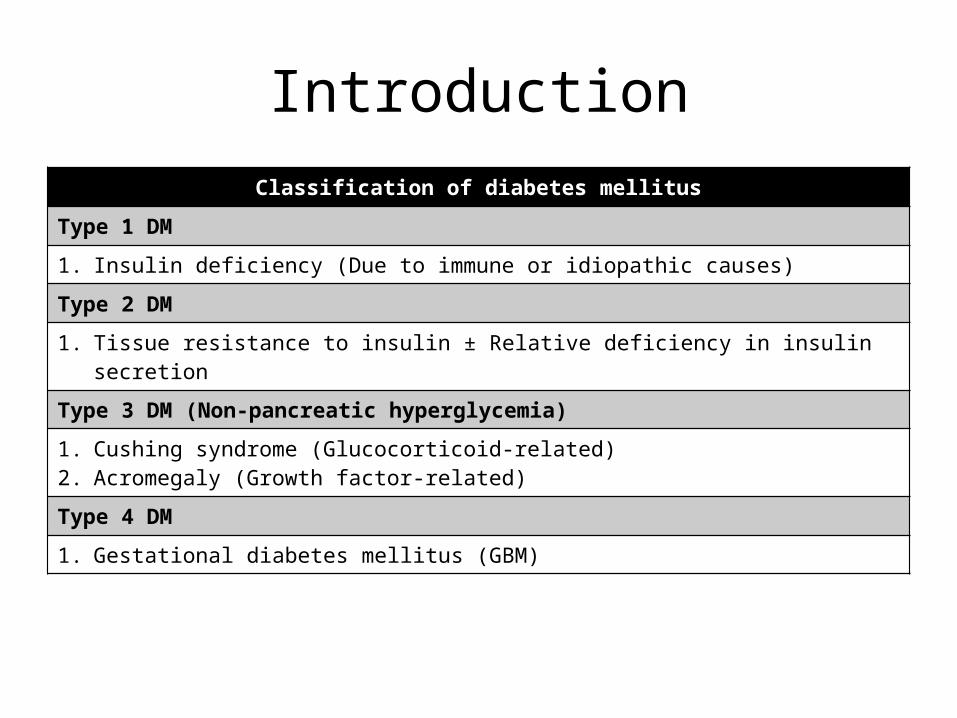
IntroductionClassification of diabetes mellitus
Type 1 DM
1. Insulin deficiency (Due to immune or idiopathic causes)
Type 2 DM
1. Tissue resistance to insulin ± Relative deficiency in insulin secretion
Type 3 DM (Non-pancreatic hyperglycemia)
1. Cushing syndrome (Glucocorticoid-related)2. Acromegaly (Growth factor-related)
Type 4 DM
1. Gestational diabetes mellitus (GBM)
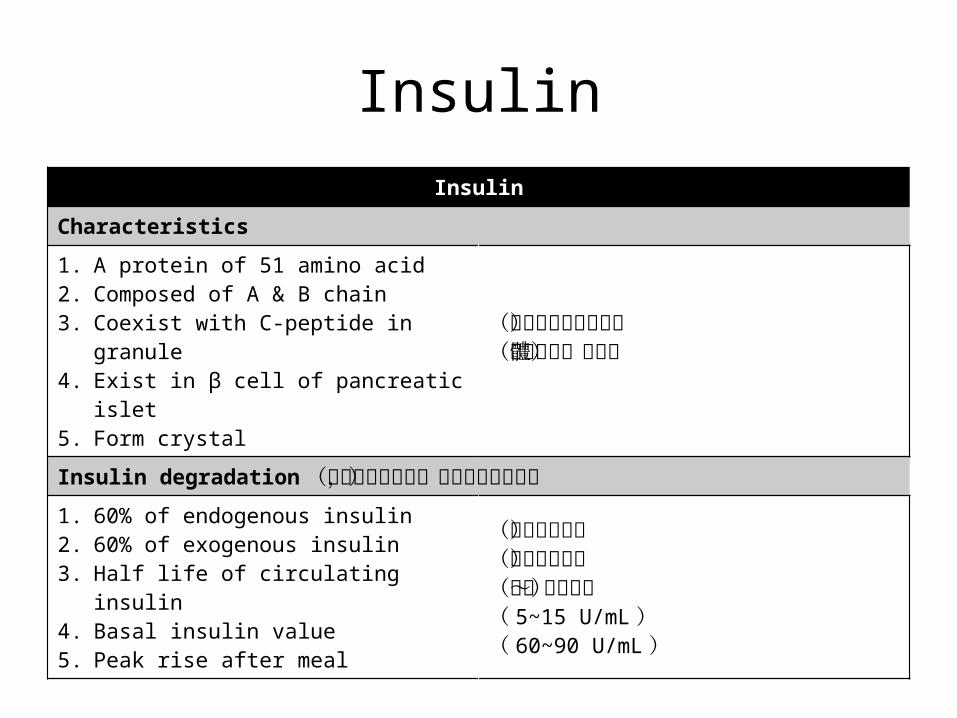
InsulinInsulin
Characteristics
1. A protein of 51 amino acid2. Composed of A & B chain3. Coexist with C-peptide in granule4. Exist in β cell of pancreatic islet5. Form crystal
(通常以雙硫鍵連結)(由高基氏體分泌)
Insulin degradation(須注意來源不同,代謝方式也不同)
1. 60% of endogenous insulin2. 60% of exogenous insulin 3. Half life of circulating insulin4. Basal insulin value5. Peak rise after meal
(由肝臟分解)(由腎臟分解)(三~五分鐘)( 5~15 U/mL )( 60~90 U/mL )
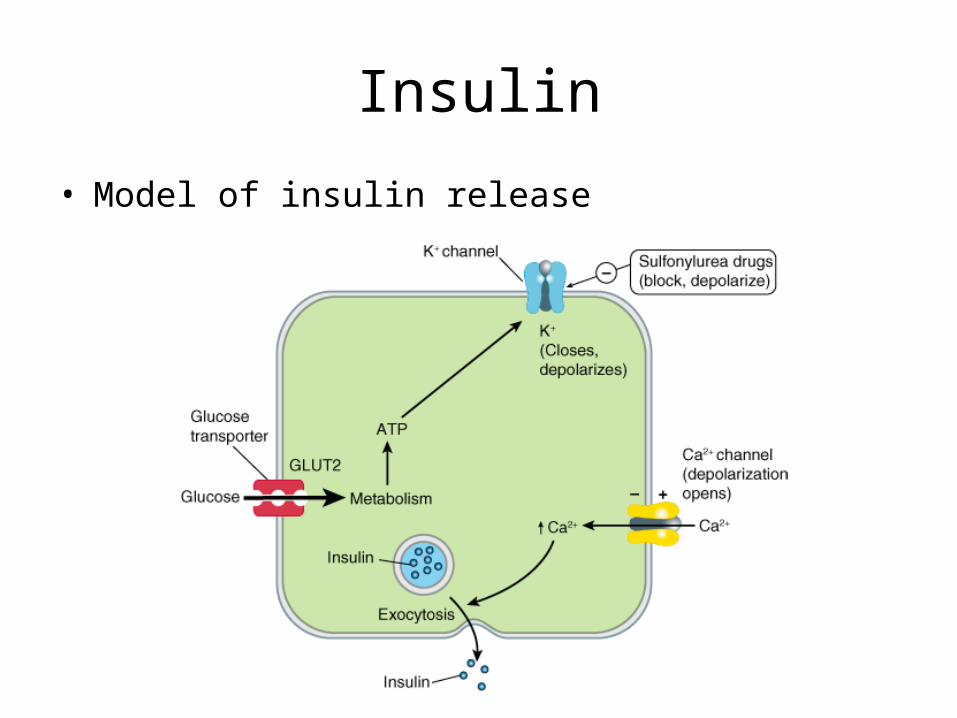
Insulin
• Model of insulin release
InsulinInsulin
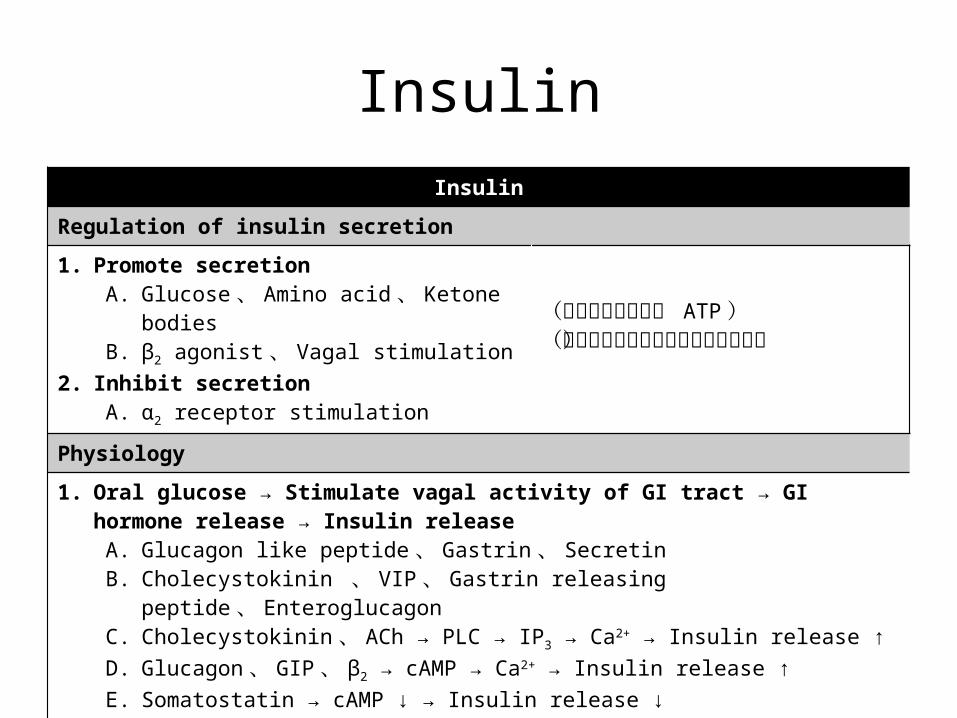
Regulation of insulin secretion
1. Promote secretionA. Glucose 、 Amino acid 、 Ketone bodiesB. β2 agonist 、 Vagal stimulation
2. Inhibit secretionA. α2 receptor stimulation
(因為代謝後會產生 ATP )(因為其能使得肝醣分解和糖質新生)
Physiology
1. Oral glucose → Stimulate vagal activity of GI tract → GI hormone release → Insulin releaseA. Glucagon like peptide 、 Gastrin 、 SecretinB. Cholecystokinin 、 VIP 、 Gastrin releasing peptide 、 EnteroglucagonC. Cholecystokinin 、 ACh → PLC → IP3 → Ca2+ → Insulin release ↑
D. Glucagon 、 GIP 、 β2 → cAMP → Ca2+ → Insulin release ↑E. Somatostatin → cAMP ↓ → Insulin release ↓
2. Important conceptsA. 白天時交感活性上升,促使胰島素分泌及肌肉中葡萄糖的代謝B. 晚上時副交感活性上升,促使胰島素分泌,但此時葡萄糖是儲存的狀態
InsulinInsulin
Physiology
1. Glucagon like peptideA. Promote insulin secretionB. Inhibit glucagon secretionC. Inhibit gastric empty
2. Glucokinase in β islet & liver cellA. Glucose metabolism relatedB. Defect in enzyme leads to decreased effect of glucose-induced insulin secretion
3. In blood streamA. β islet → α islet → δ islet (體抑素的作用必須第二循環)
InsulinInsulin
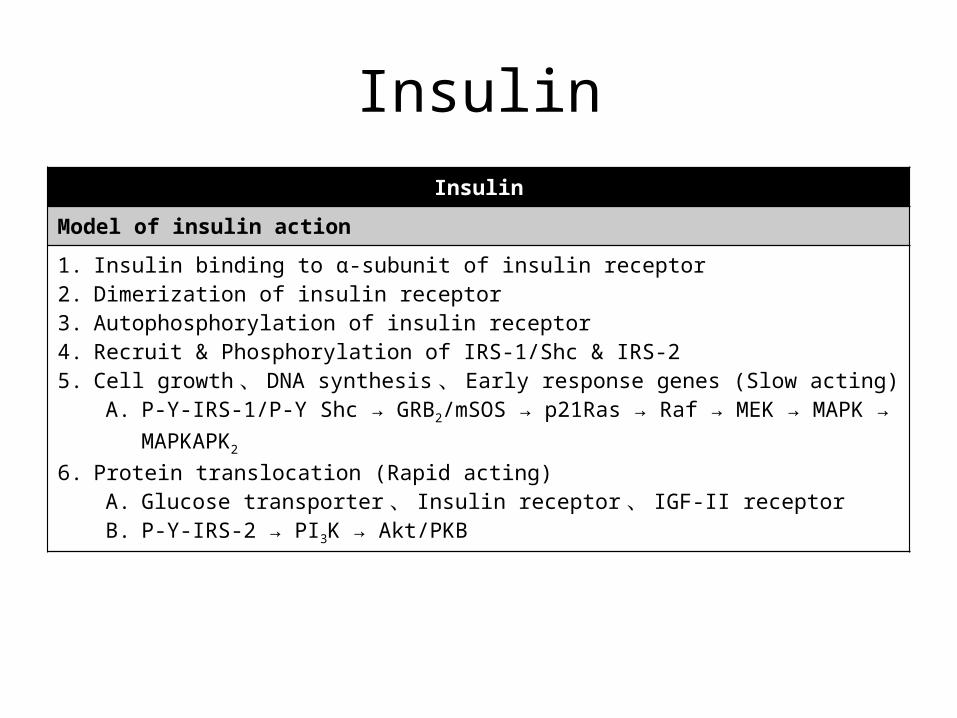
Model of insulin action
1. Insulin binding to α-subunit of insulin receptor2. Dimerization of insulin receptor3. Autophosphorylation of insulin receptor4. Recruit & Phosphorylation of IRS-1/Shc & IRS-25. Cell growth 、 DNA synthesis 、 Early response genes (Slow acting)
A. P-Y-IRS-1/P-Y Shc → GRB2/mSOS → p21Ras → Raf → MEK → MAPK → MAPKAPK2
6. Protein translocation (Rapid acting)A. Glucose transporter 、 Insulin receptor 、 IGF-II receptorB. P-Y-IRS-2 → PI3K → Akt/PKB
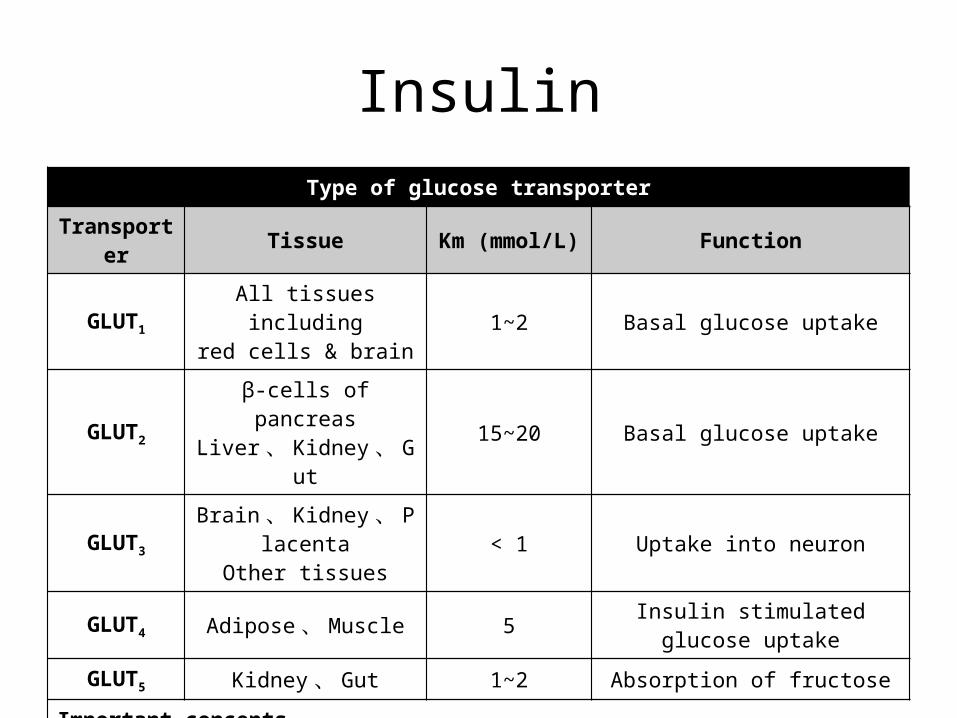
InsulinType of glucose transporter
Transporter Tissue Km (mmol/L) Function
GLUT1All tissues including
red cells & brain 1~2 Basal glucose uptake
GLUT2
β-cells of pancreasLiver 、 Kidney 、 Gut
15~20 Basal glucose uptake
GLUT3
Brain 、 Kidney 、 Placenta
Other tissues< 1 Uptake into neuron
GLUT4 Adipose 、 Muscle 5 Insulin stimulated glucose uptake
GLUT5 Kidney 、 Gut 1~2 Absorption of fructose
Important concepts1. 須注意這些 transporter 都是 carrier 而不是主動運輸2. GLUT3 對葡萄糖親合力最高,因為不僅是對葡萄糖需求高,通常血流到此濃度也低
InsulinInsulin
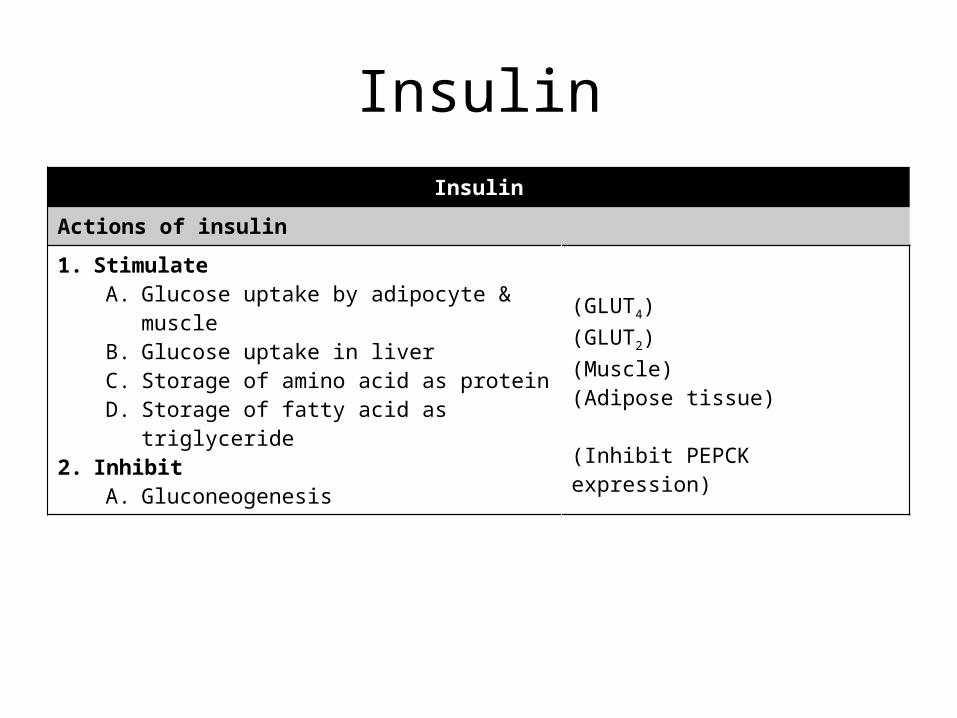
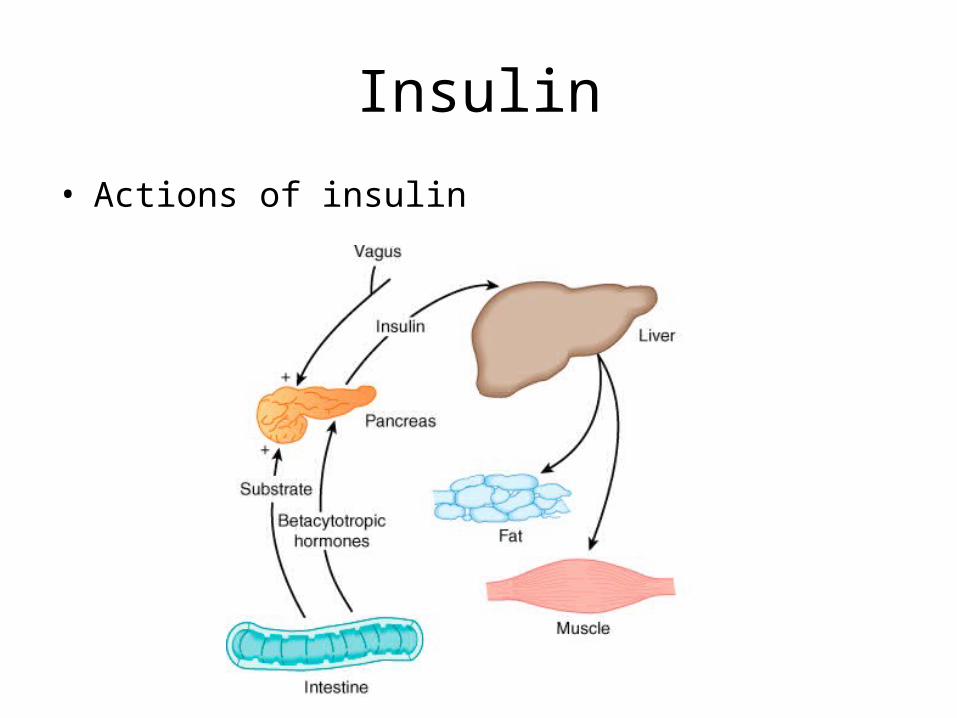
Actions of insulin
1. StimulateA. Glucose uptake by adipocyte & muscleB. Glucose uptake in liverC. Storage of amino acid as proteinD. Storage of fatty acid as triglyceride
2. InhibitA. Gluconeogenesis
(GLUT4)(GLUT2)(Muscle)(Adipose tissue)
(Inhibit PEPCK expression)
Insulin
• Actions of insulin
InsulinInsulin
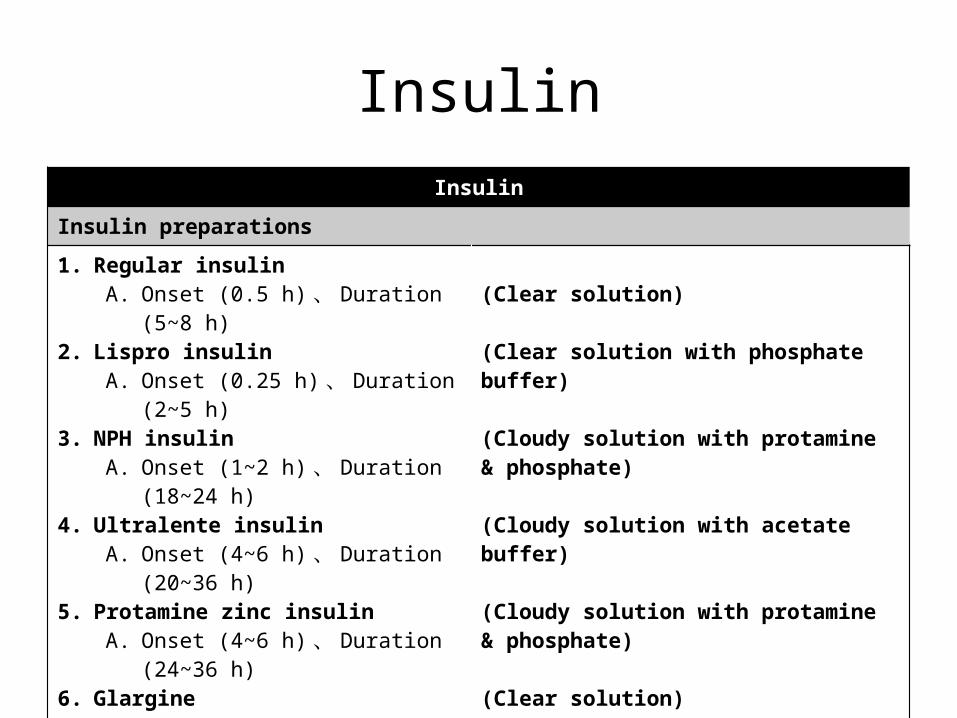
Insulin preparations
1. Regular insulinA. Onset (0.5 h) 、 Duration (5~8 h)
2. Lispro insulinA. Onset (0.25 h) 、 Duration (2~5 h)
3. NPH insulinA. Onset (1~2 h) 、 Duration (18~24 h)
4. Ultralente insulinA. Onset (4~6 h) 、 Duration (20~36 h)
5. Protamine zinc insulinA. Onset (4~6 h) 、 Duration (24~36 h)
6. GlargineA. Onset (2~5 h) 、 Duration (18~24 h)
(Clear solution)
(Clear solution with phosphate buffer)
(Cloudy solution with protamine & phosphate)
(Cloudy solution with acetate buffer)
(Cloudy solution with protamine & phosphate)
(Clear solution)
Insulin
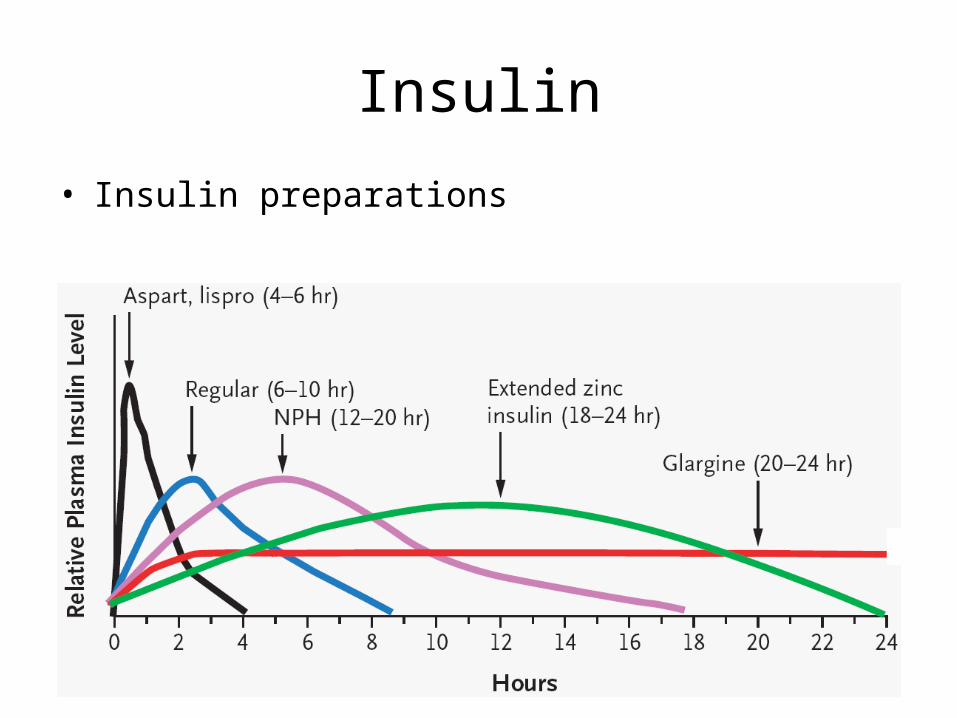
• Insulin preparations
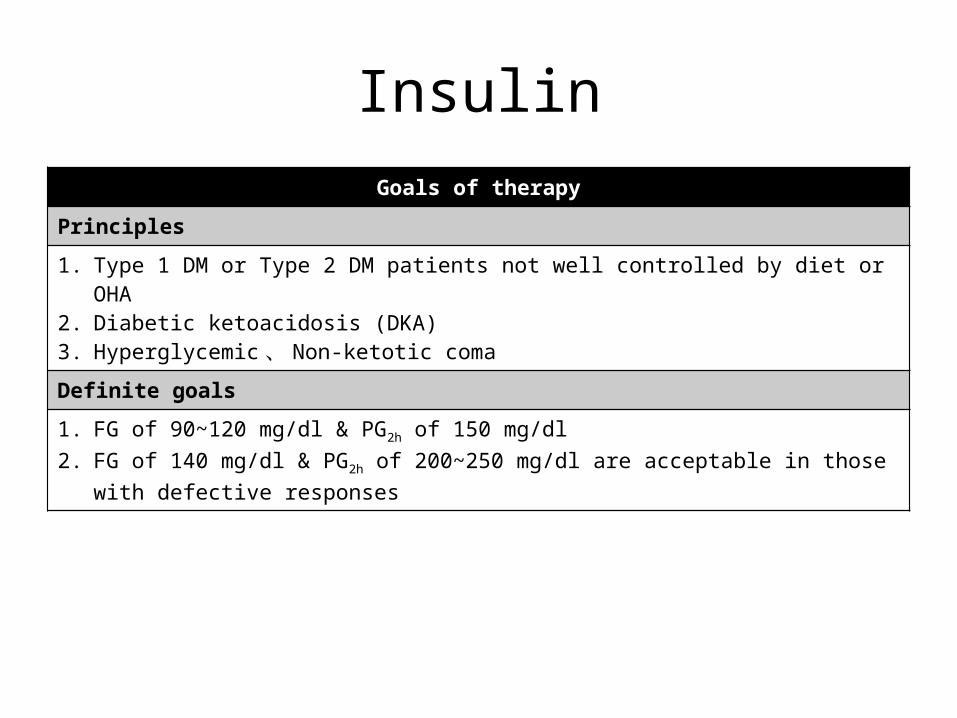
InsulinGoals of therapy
Principles
1. Type 1 DM or Type 2 DM patients not well controlled by diet or OHA2. Diabetic ketoacidosis (DKA)3. Hyperglycemic 、 Non-ketotic coma
Definite goals
1. FG of 90~120 mg/dl & PG2h of 150 mg/dl2. FG of 140 mg/dl & PG2h of 200~250 mg/dl are acceptable in those with defective responses
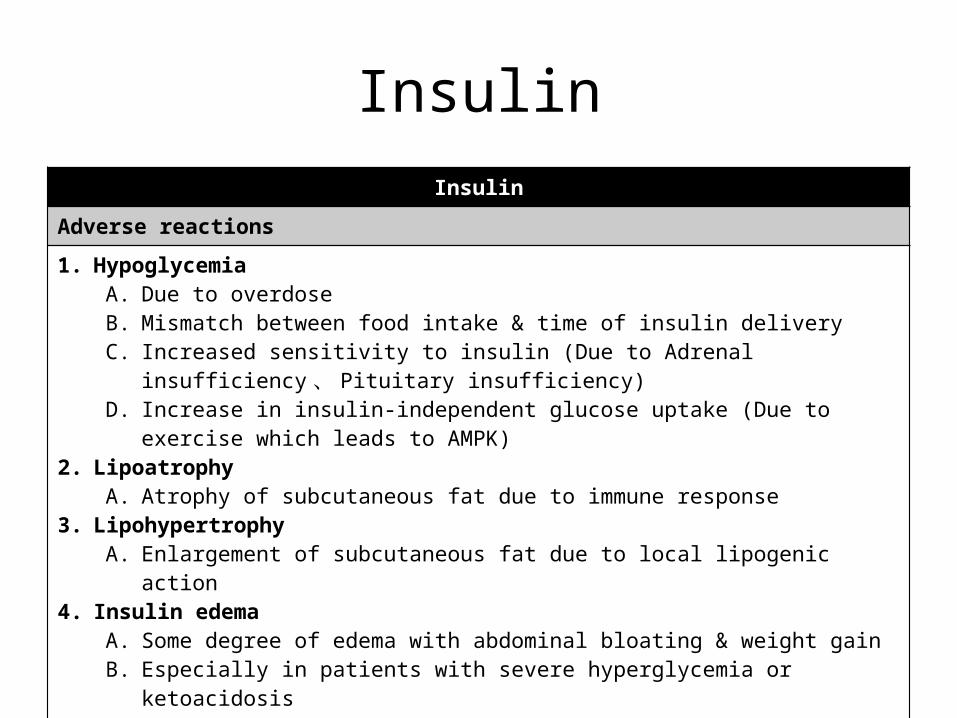
InsulinInsulin
Adverse reactions
1. HypoglycemiaA. Due to overdoseB. Mismatch between food intake & time of insulin deliveryC. Increased sensitivity to insulin (Due to Adrenal insufficiency 、 Pituitary insufficiency)D. Increase in insulin-independent glucose uptake (Due to exercise which leads to AMPK)
2. LipoatrophyA. Atrophy of subcutaneous fat due to immune response
3. LipohypertrophyA. Enlargement of subcutaneous fat due to local lipogenic action
4. Insulin edemaA. Some degree of edema with abdominal bloating & weight gainB. Especially in patients with severe hyperglycemia or ketoacidosisC. Attributed primarily to retention of Na+
D. Disappears spontaneously within several days to a week5. Insulin allergy & resistance
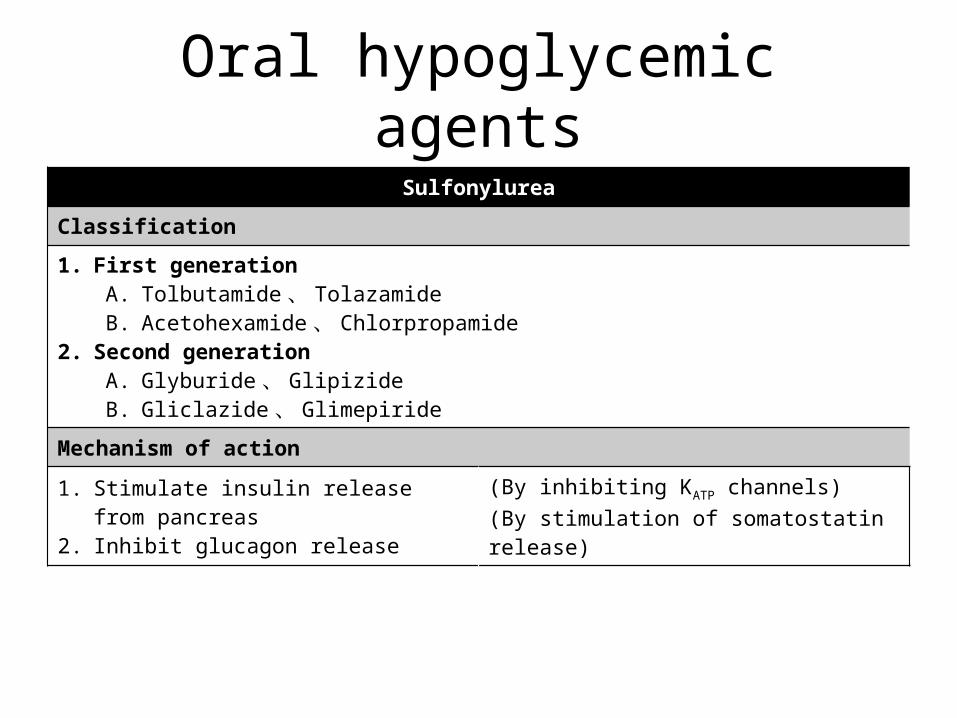
Oral hypoglycemic agentsSulfonylurea
Classification
1. First generationA. Tolbutamide 、 TolazamideB. Acetohexamide 、 Chlorpropamide
2. Second generationA. Glyburide 、 GlipizideB. Gliclazide 、 Glimepiride
Mechanism of action
1. Stimulate insulin release from pancreas2. Inhibit glucagon release
(By inhibiting KATP channels)(By stimulation of somatostatin release)
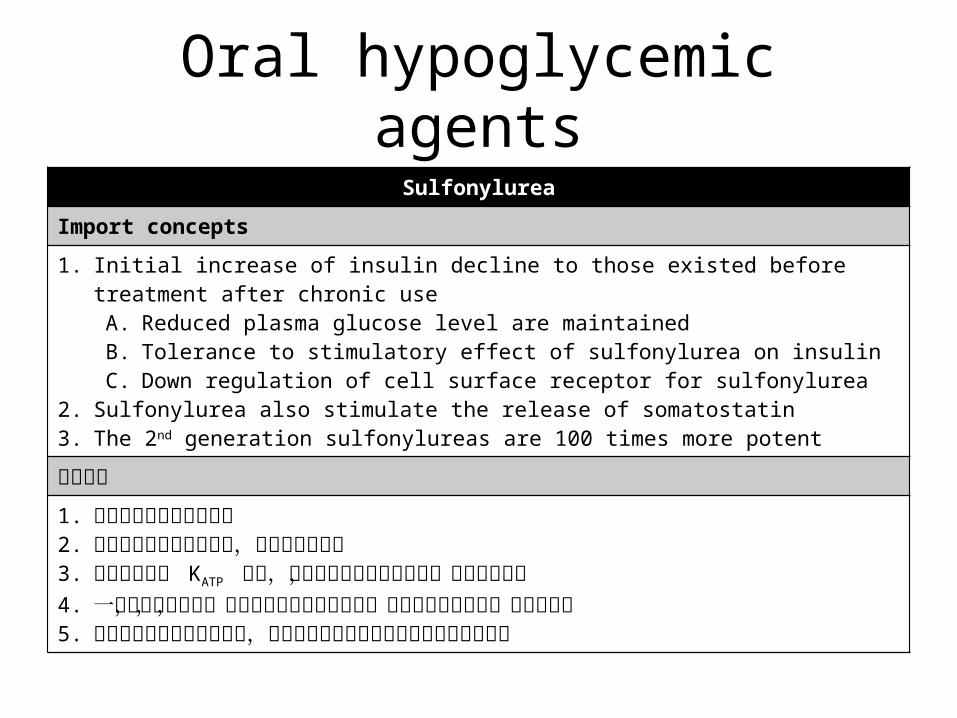
Oral hypoglycemic agentsSulfonylurea
Import concepts
1. Initial increase of insulin decline to those existed before treatment after chronic useA. Reduced plasma glucose level are maintainedB. Tolerance to stimulatory effect of sulfonylurea on insulin C. Down regulation of cell surface receptor for sulfonylurea
2. Sulfonylurea also stimulate the release of somatostatin3. The 2nd generation sulfonylureas are 100 times more potent
重要觀念
1. 主要作用在第二型糖尿病2. 結合位置在通道旁的位置,並非是通道本身3. 胰臟和心臟的 KATP 通道,其和藥物的結合位不相同,因此具選擇性4. 一開始選擇此藥時,血中的胰島素含量會上升,但是長期使用之後,含量會下降5. 但是降血糖的效果可以維持,可能是因為周邊組織對胰島素的敏感度升高
Oral hypoglycemic agentsSulfonylurea
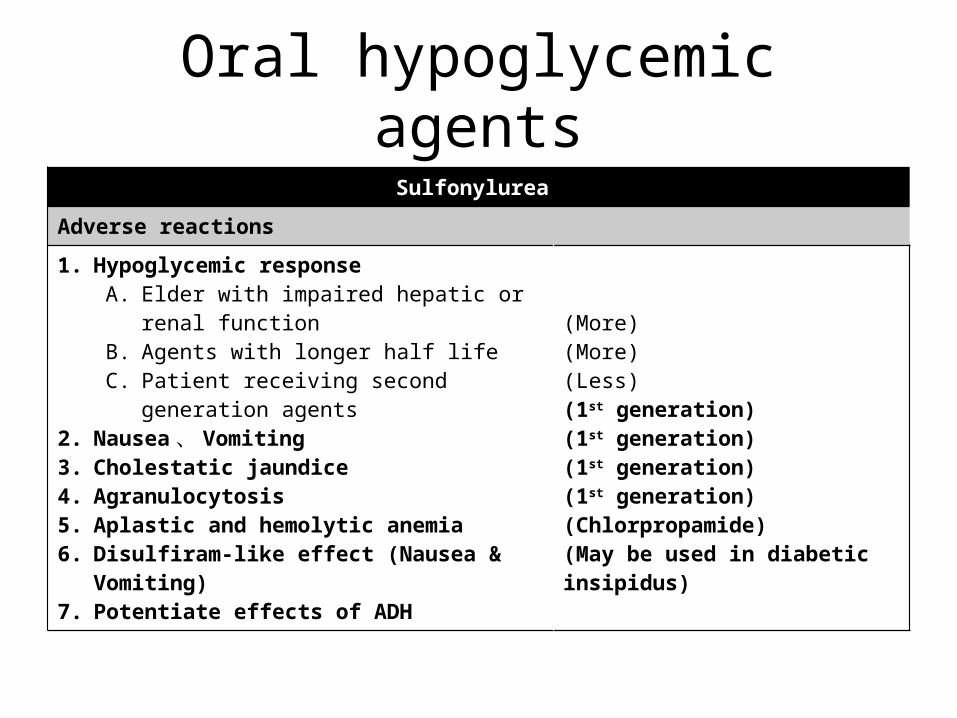
Adverse reactions
1. Hypoglycemic responseA. Elder with impaired hepatic or renal functionB. Agents with longer half lifeC. Patient receiving second generation agents
2. Nausea、 Vomiting3. Cholestatic jaundice4. Agranulocytosis5. Aplastic and hemolytic anemia6. Disulfiram-like effect (Nausea & Vomiting)7. Potentiate effects of ADH
(More)(More)(Less)(1st generation)(1st generation)(1st generation)(1st generation)(Chlorpropamide)(May be used in diabetic insipidus)
Oral hypoglycemic agentsSulfonylurea
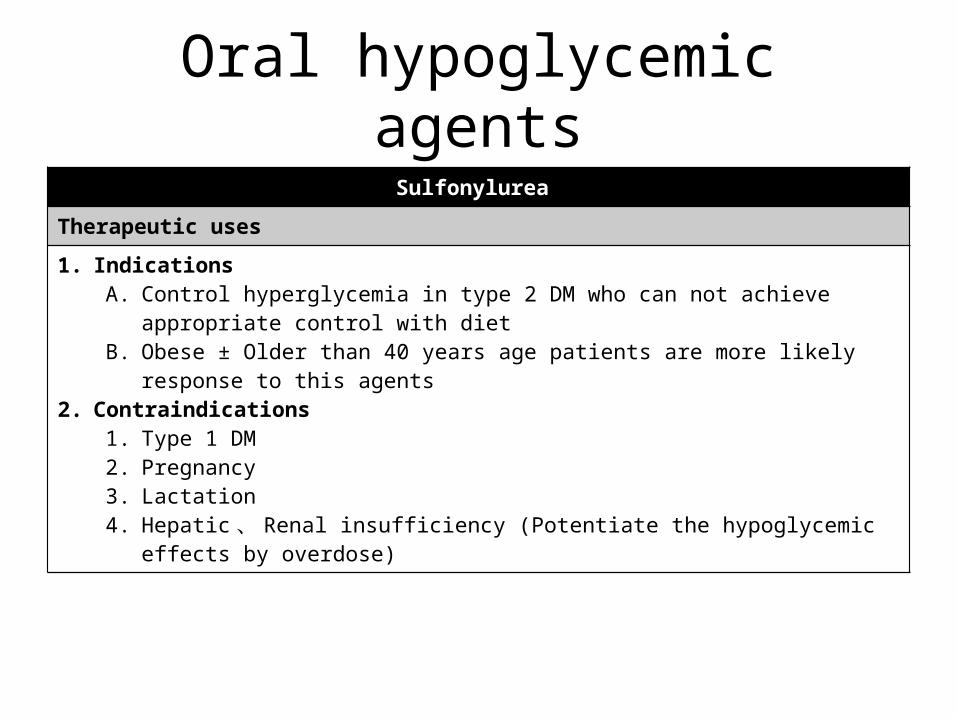
Therapeutic uses
1. IndicationsA. Control hyperglycemia in type 2 DM who can not achieve appropriate control with dietB. Obese ± Older than 40 years age patients are more likely response to this agents
2. Contraindications1. Type 1 DM2. Pregnancy3. Lactation4. Hepatic 、 Renal insufficiency (Potentiate the hypoglycemic effects by overdose)
Oral hypoglycemic agentsMeglitinides
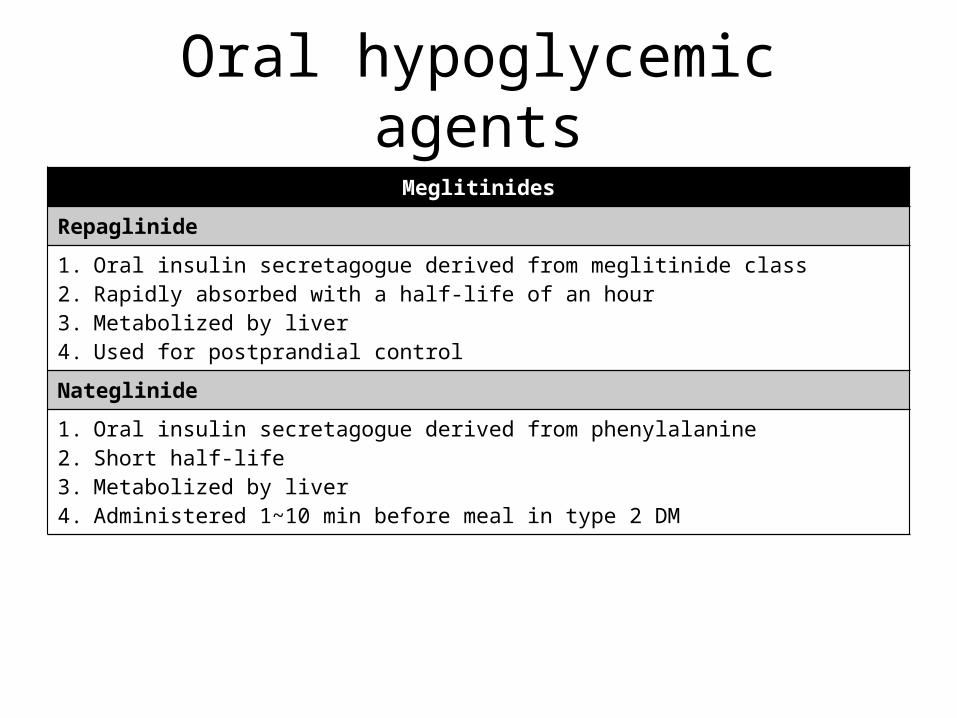
Repaglinide
1. Oral insulin secretagogue derived from meglitinide class2. Rapidly absorbed with a half-life of an hour3. Metabolized by liver4. Used for postprandial control
Nateglinide
1. Oral insulin secretagogue derived from phenylalanine2. Short half-life3. Metabolized by liver4. Administered 1~10 min before meal in type 2 DM
Oral hypoglycemic agentsα-glucosidase inhibitors
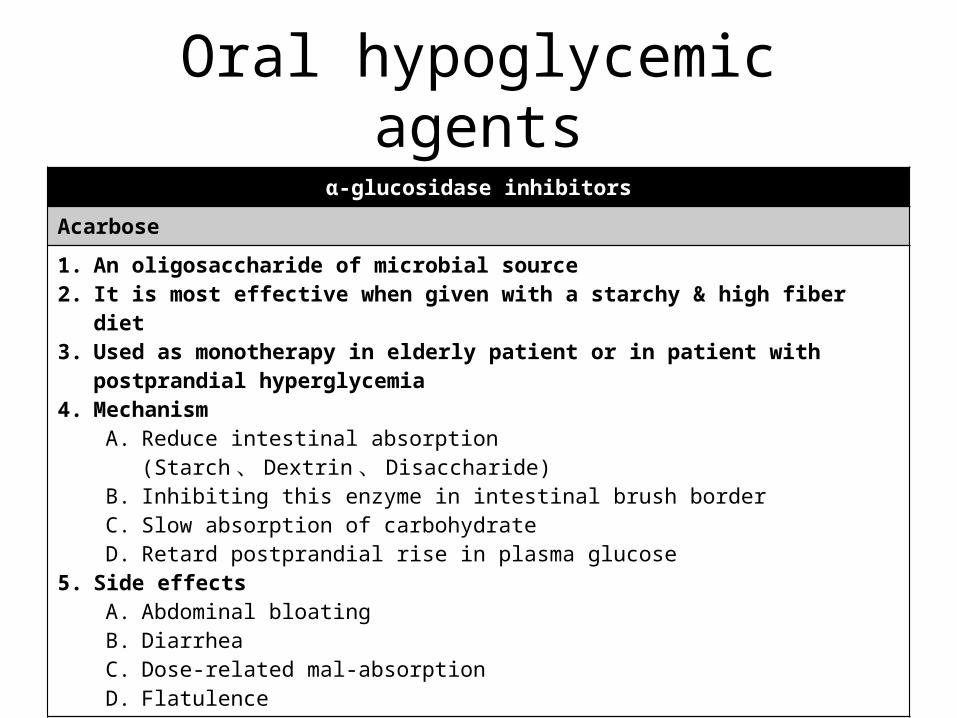
Acarbose
1. An oligosaccharide of microbial source2. It is most effective when given with a starchy & high fiber diet3. Used as monotherapy in elderly patient or in patient with postprandial hyperglycemia4. Mechanism
A. Reduce intestinal absorption (Starch 、 Dextrin 、 Disaccharide)B. Inhibiting this enzyme in intestinal brush borderC. Slow absorption of carbohydrateD. Retard postprandial rise in plasma glucose
5. Side effectsA. Abdominal bloatingB. DiarrheaC. Dose-related mal-absorptionD. Flatulence
Oral hypoglycemic agentsBiguanides
Metformin
1. Given alone or combined with sulfonylurea improve glycemic & lipid control2. Metformin is the only agent to reduce macrovascular & microvascular events in type 2 DM3. Characteristics
A. Half life 2 hoursB. Excreted unchanged in urineC. Patient with renal failure should not receive this agent
4. Side effectsA. Abdominal discomfort 、 AnorexiaB. Diarrhea 、 Metallic tasteC. Reduced intestinal Vit B12 & folate absorption
Oral hypoglycemic agentsBiguanides
Metformin
1. MechanismA. It doesn’t cause insulin release & hypoglycemiaB. Inhibit hepatic & renal gluconeogenesisC. Slowing glucose uptake from GI tractD. Reduce glucagon levelE. Stimulate glycolysis in tissueF. Activation of AMPK
2. Important conceptsA. 因為抑制糖質新生,因此會影響乳酸代謝,進而造成乳酸中毒B. 能促進骨骼肌對葡萄糖攝取,也能抑制須大量消耗 ATP 的合成路徑,因此能降低
肥胖,為其特殊的地方;此外能間接透過活化 AMPK 上游來活化 AMPK ,使脂肪酸進入骨骼肌代謝,使得原本堆積的脂肪降低
Oral hypoglycemic agentsThiazolidinediones
Rosiglitazone & Pioglitazone
1. This agent tends to lower TG and increase HDL & LDL2. Mechanism
A. Activate insulin response gene1) A selective agonist for nuclear PPARγ
B. Lower insulin resistance1) Enhancing synthesis & translocation of glucose transporter in muscle & adipose
C. Lower glucose production by liver3. Side effects
A. Anemia 、 Weight gainB. Edema 、 Volume expressionC. Contraindicated in patient with class 3 & 4 heart failure





























