Embed Size (px)
Citation preview

Pharmacologic Versus Direct-CurrentElectrical Cardioversion of Atrial Flutter
and FibrillationIsabelle C. Van Gelder, MD, PhD, Anton E. Tuinenburg, MD,Bas S. Schoonderwoerd, MD, Robert G. Tieleman, MD, and
Harry J.G.M. Crijns, MD, PhD
Conversion of atrial flutter and atrial fibrillation (AF) canbe achieved by either pharmacologic or direct-current(DC) electrical cardioversion. DC electrical cardioversionis more effective and restores sinus rhythm instanta-neously; however, general anesthesia is necessary,which can cause severe complications. On the otherhand, pharmacologic cardioversion is less effective.First, time to conversion is unpredictable and may berelatively long, especially with oral drug therapy. Also,the rate of conversion is lower and depends on durationof AF. In addition, safety is an important issue. Adversedrug reactions include bradycardia, paradoxical tachy-cardia due to enhanced atrioventricular conduction, ven-tricular proarrhythmia, and acute heart failure. In par-oxysmal AF, drug therapy is usually aimed at an acuteconversion. Class IA and IC drugs are more efficaciousthan the class III drugs sotalol, amiodarone, and ibutil-ide. By contrast, class III drugs are more effective for theconversion of atrial flutter. Acute conversion out-of-hos-pital (“pill in the pocket approach”) should be done onlyif the drug used appeared effective and safe after a few
in-hospital trials. In persistent AF, DC conversion is pre-ferred because drugs are particularly ineffective if thearrhythmia has lasted >24–48 hours. The latter prob-ably relates to electrical and anatomical remodeling ofthe atria during ongoing atrial fibrillation and flutter.Nevertheless, a wait-and-see approach using, for exam-ple, oral amiodarone may be adopted with late DCconversion if the drug fails to convert persistent AF.However, the consequences of remodeling seem to dic-tate an early conversion. In this respect, echocardio-graphy-guided DC cardioversion may become increas-ingly important in AF. It will prevent treatment resistanceand potentially reduces embolic complications. In a hy-brid approach, antiarrhythmic drugs may be used toenhance DC conversion and prevent (sub)acute recur-rences of AF. However, it may increase the defibrillationthreshold, especially if class IC drugs are used. Newtreatment options such as automatic defibrillation (im-plantable atrioverter) are still investigational. Q1999by Excerpta Medica, Inc.
Am J Cardiol 1999;84:147R–151R
A fter establishing the indication for conversion, thequestion arises whether it should be achieved by
pharmacologic or direct current (DC) electrical car-dioversion. In this respect, the advantages and disad-vantages of both strategies should be carefullyweighed (Table I). In general, DC cardioversion ismore effective than pharmacologic cardioversion.However, it necessitates general anesthesia with po-tentially severe complications. Not only are drugs lesseffective, but time to conversion is unpredictable andmay be relatively long, especially with oral therapy.Furthermore, antiarrhythmic drugs may induce brady-cardia, tachycardia due to enhanced atrioventricularconduction, ventricular proarrhythmia, and acute heartfailure.
Both pharmacologic and electrical cardioversion, andmaintenance of sinus rhythm thereafter, become moredifficult the longer the arrhythmia exists.1,2 Recent datarevealed that the latter possibly relates to deleterious
electrical and (ultra)structural remodeling of the atria.3,4
It is generally believed that sinus rhythm has severalpotential benefits compared with atrial fibrillation (AF):relief of symptoms, reduced risk of thromboemboliccomplications, and an improved exercise tolerance. Be-cause electrical and anatomical remodeling in the atriaseem to affect the chance of restoration of sinus rhythm(“atrial fibrillation begets atrial fibrillation”),5 early car-dioversion—either pharmacologic or electrical—shouldbe attempted.
PHARMACOLOGIC CONVERSION OFPAROXYSMAL AF AND ATRIALFLUTTER
Paroxysmal AF has a high tendency to convertspontaneously (Figure 1).6,7 Danias et al7 identified356 patients (45% male, mean age 686 16 years)with AF ,72 hours duration. Spontaneous conversionoccurred in up to 70% of patients, predominantly inpatients with AF for,24 hours. Converting AF oratrial flutter either electrically or with drugs dependson efficacy and safety, acceptance of either strategy bypatient and physician, and the stability of the patient.In an emergency situation, such as in AF with hemo-dynamic instability or fast ventricular rate in the set-ting of Wolff–Parkinson–White (WPW) syndrome,
From the Department of Cardiology, University Hospital Groningen,Groningen, The Netherlands.
Dr. Van Gelder was supported by The Netherlands Heart Foun-dation, grant 94.014.
Address for reprints: Harry J.G.M. Crijns, MD, Department ofCardiology, Thoraxcenter, University Hospital, Groningen, P.O. Box30.001, 9700 RB Groningen, The Netherlands.
147R©1999 by Excerpta Medica, Inc. 0002-9149/99/$20.00All rights reserved. PII S0002-9149(99)00715-8

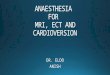
immediate DC cardioversion is appropriate. Con-versely, if the attack in the setting of WPW is rela-tively well tolerated, intravenous flecainide8 (not ap-proved in the United States) or procainamide may beused. In hemodynamically stable patients, antiarrhyth-mic drugs can be administered to accelerate restora-tion of sinus rhythm. Figure 1 shows conversion rateswith placebo and various antiarrhythmic drugs in re-cent-onset AF. It demonstrates that, with time, thecumulative conversion rate increases both on placeboand drugs. Although the different data points do notrepresent direct comparisons, it is clear that drugsfacilitate conversion and that class IC drugs are mosteffective compared with agents from class III.6 Thus,class IC drugs are first-choice therapy for conversionof an acute paroxysm of AF. Conversion rates up to90% are found 1 hour after intravenous flecainide orpropafenone. Success of treatment is strongly relatedto the previous duration of AF. Unfortunately, intra-venous class IC antiarrhythmic drugs are not availablein the United States. However, both flecainide and
propafenone can also be administered orally with suc-cess rates of.70% at 8 hours.6 Oral drug conversionmay be self-administeredonly if the patient is clini-cally stable and if the agent is safe and effectivein-hospital.6 Conditions in which class IC antiarrhyth-mic drugs should not be administered for this indica-tion include heart failure, presence of impaired cardiacfunction, acute ischemia, known sick sinus syndrome,or atrioventricular conduction disturbances. In thesepatients, proarrhythmic effects or conduction distur-bances may occur.9–11 Although class IC drugs maybe considered first-choice therapy for AF, amiodaroneis recommended for hemodynamically compromisedpatients because of its less negative inotropic effect,and even if unsuccessful for conversion, it may con-trol the ventricular rate.12 For acute conversion of AF,intravenous class IA drugs and sotalol are consideredineffective, which only became apparent after thesedrugs had been used as “active” comparators in trialsstudying new class III agents.13 The newer class IIIdrug ibutilide, with maximal early conversion rates of
FIGURE 1. Conversion of paroxysmal atrial fibrillation <3 days. Conversion rates in relationto time after start of the infusion found in studies investigating the efficacy of class IC (fle-cainide and propafenone), class IA and III drugs (procainamide, quinidine, sotalol, ibutilide,dofetilide), and amiodarone are presented. The curve indicating placebo conversion wasconstructed from placebo conversion rates. Class IC drugs appear most efficacious. Note thelate onset of conversion with amiodarone. (Adapted from Eur Heart J.6)
TABLE I Advantages and Disadvantages of Pharmacologic Versus ElectricalCardioversion of Atrial Fibrillation (AF) and Flutter
PharmacologicCardioversion
ElectricalCardioversion
Advantages ● No need for anesthesia ● Immediate effect● “Pill-in-the-pocket” approach
after proving feasibility● May be repeated immediately
● Highly effective, even in long-lasting AF● Safe in hemodynamically unstable
patients● General anesthesia needed● Thromboembolism risk
Disadvantages ● Negative inotropic effect● Proarrhythmia● Time consuming● Only effective if AF is of
short duration● Thromboembolism risk
148R THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 (9A) NOVEMBER 4, 1999

47%, is also less effective than class IC drugs.14
Digitalis, b blockers, and calcium antagonists are in-effective for acute conversion of AF.6,15,16
In contrast, class III antiarrhythmic drugs, includ-ing ibutilide, are more effective than class IC drugs forthe conversion of atrial flutter.14,17 A comparison be-tween intravenous ibutilide and sotalol indicated thatibutilide is more effective for conversion of atrialflutter.18 However, proarrhythmic events (torsade depointes) were more common in ibutilide-treated pa-tients (7.3% vs 3.7%). Clearly, more controlled dataare needed in this area, especially on proarrhythmiceffects.14,17,18
PHARMACOLOGIC CONVERSION OFPERSISTENT ATRIAL FIBRILLATION
Class III and class IA antiarrhythmic drugs seemmore effective than class IC drugs for chemical con-version of persistent AF (duration of AF.24–48hours, no spontaneous conversion).18 Oral amiodaroneand quinidine are successful in restoring sinus rhythmin approximately 20% to 50%, respectively, of pa-tients with persistent AF. Amiodarone may convert upto 20% of refractory AF and atrial flutter patients,19
obviating electrical cardioversion. Preliminary datasuggest that ibutilide and the class III drug dofetilidemay convert persistent AF of longer duration, even inpatients with impaired cardiac function, but safetymay be an issue.14,18,20An advantage of amiodarone isits ability to lower ventricular rates before conversion,whereas not only quinidine but also class IC drugsmay be associated with an uncontrolled ventricularrate. Other problems with chronic oral drugs includetorsade de pointes at conversion (class IA and IIIdrugs, except amiodarone, which has a low proar-rhythmia risk) and paradoxically, rapid ventricularrates due to enhanced atrioventricular conduction(class IC drugs). Thus, prolonged out-of-hospital load-ing seems to be safe only with amiodarone.
DC ELECTRICAL CARDIOVERSION OFAF OR ATRIAL FLUTTER
DC electrical cardioversion is an effective methodfor terminating both paroxysmal and persistent AF. Itssuccess rate is 70–90%. Usually the anterior-lateralpaddle position is applied, but a randomized compar-ison with the alternative anterior-posterior paddle po-sition is lacking. Success of DC shock is related toseveral clinical parameters: First, and of greatest im-portance, previous arrhythmia of long duration signif-icantly reduces its success rate.1,21,22Other parameterslowering its success rate are higher age and larger leftatrial size. Based on data from numerous studies, DCelectrical cardioversion for persistent AF is unlikely tosucceed in patients with AF.3 years or left atrial size.60 mm (long-axis view). Success of cardioversion isa matter of definition and may have consequences forthe selection of patients for the serial cardioversionapproach and for an implantable atrial defibrillator. Infact, there is no accepted definition. For practicalreasons, we consider defibrillation successful if sinusrhythm lasts at least a few hours after the shock, (i.e.,
the minimum time interval our clinical cardioversionprotocol allows until discharge of the patient). Lownand coworkers21 counted immediate restoration of si-nus rhythm, presumably lasting from a few minutes to1 hour. It is not known whether patients with veryearly versus those with later subacute recurrencesrespond differently to a serial cardioversion strategyor the implantable defibrillator. However, it may behypothesized that patients with persistent AF main-taining sinus rhythm for a few days may benefit fromrepeated prompt cardioversions at the time of AFrecurrence. Hypothetically, due to a longer period insinus rhythm and only a short period in AF, electro-physiologic5 and (ultra)structural3,4,23 alterations fa-voring persistence of AF may be reversed progres-sively each time sinus rhythm is restored, therebyenhancing long-term maintenance of sinus rhythm.
LATE CONVERSION OFPAROXYSMAL AND PERSISTENTATRIAL FIBRILLATION
A wait-and-see approach may be adopted usingoral amiodarone with late DC conversion if amioda-rone fails to convert paroxysmal or persistent AF.Although the consequences of remodeling seem todictate early conversion, for some patients the wait-and-see approach may be preferable, as it is moreconvenient and prevents hospital admission. An ex-ample of such a strategy is amiodarone loading for4–6 weeks followed by DC cardioversion if AF doesnot convert chemically.19,24
In the case of late conversion of paroxysmal AF,class IC antiarrhythmic drugs should not be institutedduring AF or atrial flutter, as enhanced atrioventricu-lar conduction, proarrhythmia, and conduction distur-bances are more likely to occur during higher heartrates present during the arrhythmia. Sotalol, althoughnot effective for acute conversion, may be an alterna-tive because it effectively reduces heart rate, therebyenhancing restoration of sinus rhythm, possibly byameliorating left atrial dilatation. Unfortunately, thisstrategy may lead to torsade de pointes at the time ofconversion to sinus rhythm and should therefore beapplied after try-out in-hospital to monitor adverseevents.
HYBRID THERAPYIn a hybrid approach, drugs may be used to en-
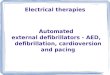
hance DC conversion and prevent acute recurrencesafter conversion. Advantages of this approach are thatat the moment of restoration of sinus rhythm, adequateplasma levels are present, lowering (sub)acute re-lapses, which in turn improves outcome of the serialcardioversion approach (Figure 2). Furthermore,chemical conversion may occur and, hypothetically,certain drugs may prevent or reverse atrial remodel-ing. In contrast, loading may increase the defibrillationthreshold, especially if class IC drugs are used, andwarrants a longer hospitalization due to the risk ofproarrhythmic events during loading. Biancioni et al25
recently described the beneficial effects of oral in-hospital loading with the class IC antiarrhythmic drug
A SYMPOSIUM: CARDIAC ARRHYTHMIAS 149R

propafenone for 48 hours. Compared with those whowere randomized to placebo, a comparable number ofpatients were successfully cardioverted using DCshock (84% vs 83%). However, at discharge after 48hours, significantly more patients randomized topropafenone were in sinus rhythm (74% vs 53%, p,0.05).
Evidence that pretreatment with the calcium antag-onist verapamil during AF may improve outcome ofthe cardioversion strategy is, so far, only observa-tional. In a nonrandomized retrospective study in 61patients with persistent AF, multivariate analysis re-vealed that the use of intracellular calcium-loweringdrugs during AF (to control the ventricular rate) wasthe only significant variable related to maintenance ofsinus rhythm after cardioversion.26 Additional evi-dence was demonstrated in a study investigating theefficacy of amiodarone loading on chemical conver-sion in patients with persistent AF. One of the param-eters significantly influencing amiodarone conversionwas concomitant treatment with calcium-loweringdrugs.24 Preliminary prospective data confirm this ob-servation.27
THROMBOEMBOLIC COMPLICATIONSRELATED TO CARDIOVERSION:STUNNING, HIBERNATION, ORBOTH?
Spontaneous, chemical, but especially electricalcardioversion of AF may lead to stunning of the atriaas detected on an echocardiogram.28–30 The echocar-diographic definition of stunning is standstill of theatrial wall, atrial dilatation, the emergence of sponta-neous echo contrast, and the development of intra-atrial thrombi, especially in the left atrial appendage.
The term stunning in the setting of ischemia refers toa postischemic situation in which myocardium is vi-able but does not function (absence of contraction).31
If blood flow is not restored but remains minimal, thissituation may lead to hibernation, especially in thecase of repetitive stunning. Hibernation is character-ized by specific microscopic findings. Recently,Ausma and Borgers4,32 have shown that the atria har-boring chronic AF show hibernation, which is similarto that found in intermittent ischemia. In part, one hasto deal with a semantic problem. Characterizing thepostconversion situation as stunning does not seemcorrect; if anything, there ishibernation rather thanstunning, especially in patients with long-lasting AF.Using the term stunning to indicate postshock orpostchemical cardioversion spontaneous echo contrastsuggests that the act of electrical shock or the act ofcardioversion itself is responsible for the spontaneousecho contrast and the associated atrial thombogenicityin the atria. Although conversion to sinus rhythm iscrucial for the emergence of spontaneous echo con-trast, it can only emerge when AF is chronic ratherthan acute. This means that the duration of AF33,34andthe development of a pathoanatomical picture of hi-bernation (and possibly associated with endothelialendocardial dysfunction with an increase in von Wil-lebrand factor and soluble thrombomodulin as indica-tors of endothelial dysfunction and indicators ofthrombogenicity)35 form the basis of so called “post-conversion stunning.”
CONCLUSIONSThe decision whether pharmacologic or electrical
cardioversion should be applied depends on severalparameters. The first step is to evaluate hemodynamic
FIGURE 2. Hypothetical curve demonstrating the time course of relapses of atrial fibrillationafter restoration of sinus rhythm. Note that most relapses (40–50%) occur during the first 2weeks after restoration of sinus rhythm.
150R THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 84 (9A) NOVEMBER 4, 1999

stability. Immediate cardioversion using DC shockrather than intravenous drugs may be indicated. Thenext step is to assess the duration of AF, because thelonger the arrhythmia exists the less successful chem-ical conversion is. A third step may be to decidewhether the conversion should be effected acutely or await-and-see procedure should be followed. As aguideline, the following strategy can be applied: Forthe acute conversion of paroxysmal AF, start a classIC antiarrhythmic drug in hemodynamically stablepatients. Intravenous sotalol and other class III anti-arrhythmic drugs are not useful foracuteconversionof paroxysmal AF. In hemodynamically unstable pa-tients with AF of short duration, DC electrical cardio-version is first-choice therapy. Avoid intravenous an-tiarrhythmic drugs if AF has been long-standing (ar-bitrarily: longer than a few days/weeks) because theydo not work very well in long-standing AF. On theother hand, in the persistent form of AF, oral amio-darone may be effective in a wait-and-see strategy,with late DC conversion if amiodarone fails. Parox-ysmal atrial flutter may be terminated by class IIIdrugs but not by class IC drugs. Stunning (or hiber-nation) of the atria occurs in AF of longer duration butis dependent on conversion to sinus rhythm. However,it does not depend on the mode of conversion.
1. Van Gelder IC, Crijns HJGM, Tieleman RG, Bru¨gemann J, De Kam PJ,Gosselink ATM, Verheugt FWA, Lie KI. Value and limitation of electricalcardioversion in patients with chronic atrial fibrillation: importance of arrhythmiarisk factors and oral anticoagulation. Arch Intern Med1996;156:2585–2592.2. Sopher SM, Camm AJ. Atrial fibrillation: maintenance of sinus rhythm versusrate control.Am J Cardiol1996;77(suppl):24A–38A.3. Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA,Weyman AE. Atrial enlargement as a consequence of atrial fibrillation.Circula-tion 1990;82:792–797.4. Ausma J, Wijffels M, Thone JF, Wouters L, Allessie M, Borgers M. Structuralchanges of atrial myocardium due to sustained atrial fibrillation in the goat.Circulation 1997;96:3157–3163.5. Wijffels MCEF, Kirchof CJHJ, Dorland R, Allessie MA. Atrial fibrillationbegets atrial fibrillation: a study in awake chronically instrumented goats.Cir-culation 1995;92:1954–1968.6. Fresco C, Proclemer A, on behalf of the PAFIT-2 Investigators. Managementof recent onset atrial fibrillation.Eur Heart J1996;17(suppl C):41–47.7. Danias PG, Caulfield TA, Weigner MJ, Silverman DI, Manning WJ. Likeli-hood of spontaneous conversion of atrial fibrillation to sinus rhythm.J Am CollCardiol 1998;31:588–594.8. Crijns HJ, Den Heijer P, Van Wijk LM, Lie KI. Successful use of flecainidein atrial fibrillation with rapid ventricular rate in the Wolff-Parkinson-Whitesyndrome.Am Heart J1989;115:1317–1321.9. Levine JH, Morganroth J, Kadish AH. Mechanism and risk factors forproarrhythmia with type IA compared with IC antiarrhythmic drug therapy.Circulation 1989;80:1063–1069.10. Murgatroyd FD, Camm AJ. Atrial arrhythmias.Lancet1993;341:1317–1322.11. Flaker GC, Blackshear JL, McBride R, Kronmal RA, Halperin JL, Hart RG,on behalf of the Stroke Prevention in Atrial Fibrillation Investigators. Antiar-rhythmic drug therapy and cardiac mortality in atrial fibrillation. J Am CollCardiol 1992;20:527–532.12. Hou Z-Y, Chang M-S, Chen C-Y, Tu M-S, Lin S-L, Chiang H-T, WoosleyRL. Acute treatment of recent-onset atrial fibrillation and flutter with a tailoreddosing regimen of intravenous amiodarone: a randomized, digoxin-controlledstudy.Eur Heart J1995;16:521–528.13. Reisinger J, Gatterer E, Heinze G, Wiesinger K, Zeindlhofer E, GattermeierM, Poelzl G, Kratzer H, Ebner A, Hohenwallner W, Lenz K, Slany J, Kuhn P.
Prospective comparison of flecainide versus sotalol for immediate cardioversionof atrial fibrillation. Am J Cardiol1998;81:1450–1454.14. Stambler BS, Wood MA, Ellenbogen KA, Perry KT, Wakefield LK,VanderLugt JT, and the Ibutilide Repeat Dose Study investigators. Efficacy andsafety of repeated intravenous doses of ibutilide for rapid conversion of atrialflutter or fibrillation.Circulation 1996;94:1613–1621.15. Falk RH, Knowlton AA, Bernard SA, Gotlieb NE, Battinelli NJ. Digoxin forconverting recent-onset atrial fibrillation to sinus rhythm.Ann Intern Med1987;106:503–506.16. Noc M, Stajer D, Horvat M. Intravenous amiodarone versus verapamil foracute conversion of paroxysmal atrial fibrillation to sinus rhythm.Am J Cardiol1990;65:679–680.17. Crijns HJGM, Van Gelder IC, Kingma JH, Dunselman PHJM, GosselinkATM, Lie KI. Atrial flutter can be terminated by a class III antiarrhythmic drugbut not by a class IC drug.Eur Heart J1994;15:1403–1408.18. Vos MA, Golitsyn SR, Stangl K, Ruda MY, Van Wijk L, Harry JD, Perry KT,Touboul P, Steinbeck G, Wellens HJJ, for the Ibutilide/ Sotalol Comparator StudyGroup. Superiority of ibutilide (a new class III agent) over DL-sotalol in con-verting atrial flutter and atrial fibrillation.Heart 1998;79:568–575.19. Gosselink ATM, Crijns HJ, Van Gelder IC, Hillige H, Wiesfeld ACP, Lie KI.Low-dose amiodarone for maintenance of sinus rhythm after cardioversion ofatrial fibrillation or flutter.JAMA 1992;267:3289–3293.20. Pedersen OD, The Diamond study group. Dofetilide in the treatment of atrialfibrillation in patients with impaired left ventricular function: atrial fibrillation inthe Diamond study. (Abstr.)Circulation 1998;98:I-632.21. Lown B. Electrical cardioversion of cardiac arrhythmias.Br Heart J 1967;29:469–487.22. Van Gelder IC, Crijns HJ, Van Gilst WH, Verwer R, Lie KI. Prediction ofuneventful cardioversion and maintenance of sinus rhythm from direct-currentelectrical cardioversion of chronic atrial fibrillation and flutter.Am J Cardiol1991;68:41–46.23. Bailey GWH, Braniff BA, Hancock EW, Cohn KE. Relation of left atrialpathology to AF in mitral valvular disease.Ann Intern Med1968;69:13–20.24. Tieleman RG, Gosselink ATM, Crijns HJGM, Van Gelder IC, Van Den BergMP, De Kam PJ, Van Gilst WH, Lie KI. Efficacy, safety and determinants ofconversion of atrial fibrillation and flutter with oral amiodarone.Am J Cardiol1997;79:53–57.25. Bianconi L, Mennuni M, Lukic V, Castro A, Chieffi M, Santini M. Effect oforal propafenone administration before electrical cardioversion of chronic atrialfibrillation: placebo controlled study. J Am Coll Cardiol1996;28:700–706.26. Tieleman RG, Van Gelder IC, Crijns HJGM, De Kam PJ, Van Den Berg MP,Haaksma J, Van Der Woude HJ, Allessie MA. Early recurrences of atrialfibrillation after electrical cardioversion: a result of fibrillation-induced electricalremodeling of the atria?J Am Coll Cardiol1998;31:167–173.27. Natale A, Tomassoni G, Beheiry S, Kim YH, Pisano E, Leonelli F, PotenzaM. Prospective randomized evaluation of combined therapy with amiodarone anda calcium antagonist for treatment of refractory atrial fibrillation. (Abstr.)Cir-culation 1998;98:I-103.28. Grimm RA, Stewart WJ, Maloney JD, Cohen GI, Pearce GL, Salcedo EE,Klein AL. Impact of electrical cardioversion for atrial fibrillation on left atrialappendage function and spontaneous echo contrast: characterization by simulta-neous transesophageal echocardiography. J Am Coll Cardiol 1993;22:1359–1366.29. Fatkin D, Kelly RP, Feneley MP. Relations between left atrial appendageblood flow velocity, spontaneous echocardiographic contrast and thromboem-bolic risk in vivo. J Am Coll Cardiol1994;23:961–969.30. Grimm RA, Leung DY, Black IW, Stewart WJ, Thomas JD, Klein AL. Leftatrial appendage “stunning” after spontaneous conversion of atrial fibrillationdemonstrated by transesophageal Doppler echocardiography.Am Heart J1995;130:174–176.31. Marban E. Myocardial stunning and hibernation: the physiology behind thecolloquialisms.Circulation 1991;83:681–688.32. Ausma J, Wijffels M, Van Eys G, Koide M, Ramaekers F, Allessie M,Borgers M. Dedifferentiation of atrial cardiomyocytes as a result of chronic atrialfibrillation. Am J Pathol1997;151:985–997.33. Manning WJ, Silverman DI, Katz SE, Riley MF, Come PC, Doherty RM,Munson JT, Douglas PS. Impaired left atrial mechanical function after cardio-version: relation to the duration of atrial fibrillation. J Am Coll Cardiol1994;23:1535–1540.34. Verhorst PM, Kamp O, Visser CA, Verheugt FW. Left atrial appendage flowvelocity assessment using transesophageal echocardiography in nonrheumaticatrial fibrillation and systemic embolism.Am J Cardiol1993;71:192–196.35. Oltrona L, Broccolino M, Merlini PA, Spinola A, Pezzano A, Mannucci PM.Activation of the hemostatic mechanism after pharmacologic cardioversion ofacute nonvalvular atrial fibrillation.Circulation 1997;95:2003–2006.
A SYMPOSIUM: CARDIAC ARRHYTHMIAS 151R