Embed Size (px)
Citation preview

Pharmacoliinetics of F 105, a human monoclonal antibody, in persons infected with human immunodeficiency virus type 1
F105 is a human monoclonal antibody that binds to the CD4 binding site of human immunodeficiency virus type 1 gp120 and neutralizes clinical and laboratory isolates of the human immunodeficiency virus. This phase I study investigated the disposition of the antibody in humans. F105 was administered over a 60-minute period at two dose levels, 100 and 500 mg/m”. Blood samples were obtained for up to 56 days. The clearance of the antibody was 0.33 ml/min with a corresponding half-life of approximately 13 days. Peak concentrations achieved at the higher dose level were 216.19 t: 9.62 pg/ml. The disposition of the drug was linear for the doses studied. Simulations were performed to design future studies aimed at investigating the efficacy of the antibody. This study concluded that F105 can be administered as a bolus dose every 21 days. (Clin Pharmacol Ther 1996;59:662-7.)
Erika J. Wolfe, PharmD, Lisa A. Cavacini, PhD, Matthew H. Samore, MD, Marshall R Posner, MD, Carolyn Kozial, RN, Cathie Spino, DSc, Carol Braun Trapnell, MD, Nzeera Ketter, MD, Scott Hammer, MD, and John G. Gambertoglio, PharmD Sm. Francisco, Cal& Boston, Muss., and Bethesda and Rockville, Md.
Current treatment of human immunodeficiency virus (HIV) infection relies mainly on the antiret- roviral agents, which inhibit viral replication. Al- though these therapies have been relatively suc- cessful at slowing the progression of the disease, adverse reactions and drug resistance remain problematic. Immune therapies have to date been used as an adjunct for treating viral diseases such as cytomegalovirus infection. Also under investi- gation are high-titer immune globulins to HIV-l obtained by plasmaphoresis of infected persons.
From the Division of Clinical Pharmacy, University of California, San Francisco; Harvard Medical School, School of Public Health, and New England Deaconess Hospital, Boston; the National Institutes of Allergy and Infectious Disease, Bethesda; and the U.S. Food and Drug Administration, Rockville.
Supported in part by grants from the AIDS Clinical Trials Group of the National Institutes of Allergy and Infectious Diseases, Bethesda, Md.; grant Al-27663 for the University of Califor- nia, San Francisco (Dr. Gambertoglio); and grant AI-26926 for the New England Deaconess Hospital/Harvard Medical School (Drs. Posner and Cavacini).
Received for publication Sept. 26, 1995; accepted Jan. 27, 1996. Reprint requests: John G. Gambertoglio, PharmD, Division of
Clinical Pharmacy, C-152, University of California, San Fran- cisco, San Francisco, CA 94143-0622.
1311ll2365
662
The standardization and preparation of this prod- uct, however, is burdensome.’ F105 is a human monoclonal IgGlk antibody developed from a subject with HIV infection. It binds to the CD4 binding region of viral gp120 and neutralizes lab- oratory strains and primary isolates of HIV.2,3 Neutralizing antibodies that are able to bind a number of HIV isolates, such as F105, bind the conformational epitopes and generally develop later in the course of the disease. The humoral response to HIV in early infection is directed to the V3 loop of viral gp120,495 which is variable. These antibodies directed to the V3 loop are not as broadly neutralizing as antibodies that bind conformational epitopes. Thus administration of F105 early in the course of infection may delay disease progression. In fact, studies suggest that the presence of broadly neutralizing antibodies are associated with a good prognosis.6,7 In addi- tion, the absence of native F105 in the serum of patients infected with HIV has been correlated with disease progression.8 The purpose of this study is to describe the disposition of F105 in humans and to develop a dosage schedule for studies designed to investigate the efficacy of the antibody.

CLINICAL PHARhtACOLOGY .& ‘THERAPEUTICS VOLUME 5’). NUMBER 6 Wolf et al. 663
METHODS This phase I, nonrandomized, open-label dose-
escalating study involved eight patients. A single intravenous dose of F10.5 was administered over a 60-minute period at two dose levels. Subjects were entered in the study two at a time and a minimum of 1 week elapsed between entry of each set of subjects to assess drug safety. The study was approved by the institutional review board of the New England Dea- coness Hospital. Informed consent was obtained be- fore subjects enrolled in the study.
Patients. Patients were positive for HIV and their CD4 counts were between 200 and 500 cells/mm” during the screening period. They were required to have adequate hematologic function, with a hemo- globin level ~7.5 gm/dl, an absolute neutrophil count 21000 cells/mm”, and a platelet count r75,000/mm3; adequate liver function, with aspar- tate aminotransferase (AST), alanine aminotrans- ferase (ALT), and alkaline phosphatase 45 times the upper limit of normal; and adequate kidney function, with serum creatinine cl.5 times the up- per limit of normal or an estimated creatinine clear- ance of 270 ml/min (with use of the Cockcroft and Gault equation). Patients received stable antiretro- viral therapy for 3 months before baseline evalua- tion and were not included if they had a diagnosis of acquired immunodeficiency syndrome.
Drug administration. F105, supplied in glass vials containing 5 mg/ml of the drug (Centocor, Inc., Malvern, Pa.), was administered to four subjects each at doses of 100 and 500 mg/m*. It was infused at a concentration of 2.5 mg/ml over a l-hour period with use of a calibrated infusion pump. Patients remained in the clinic for 12 hours after administra- tion of the drug for blood sampling and observation. Adverse events were recorded and graded for sever- ity on a scale of grade I (mild) to grade IV (severe).
Sample processing. Blood was collected in (yellow top) tubes that contained acid-citrate-dextrose solu- tion for measurement of F105 concentration before administration and at 0.5, 1, 1.08, 1.5, 2, 4, 6, 8, 12, and 24 hours from the beginning of the infusion. Additional samples were obtained at 2, 4, 7, 10, 14, 21, 28, 35, 42, 49, and 56 days. The blood was immediately centrifuged and the plasma was re- moved for storage at -20” C until analysis.
FI 05 idiotype-specific enzyme-linked immunosorbent assay. Details of the assay have been published pre- viously.’ Briefly, the assay is a double idiotype enzyme-linked immunosorbent assay that uses a mu- rine monoclonal anti-F105 capture antibody and a
detect antibody. The sensitivity of the assay is 0.015 kg/ml. The concentration of F105 in test sera was determined from a standard curve generated from known concentrations of F105 diluted in sera ob- tained before therapy. The dilution of serum chosen for the standard curve was l:lO, which represented the lowest sera dilution tested in the assay. With the exception of serum from one patient, all sera sam- ples obtained before therapy were negative in this enzyme-linked immunosorbent assay, as were nor- mal control sera samples (more than 15 samples were tested). For the patient with serum that was positive before therapy, F105 was diluted in normal control sera. All samples were performed in tripli- cate, and only the assays with replicates within 5% of each other were considered valid.
Phurmucokinetic analysis. The data were analyzed with use of noncompartmental procedures. The area under the plasma concentration versus time curve (AUC) was calculated with use of the linear trape- zoidal rule for increasing concentrations and the log-trapezoidal rule for decreasing concentrations. Extrapolation of AUC to infinity was determined by dividing the last observed data point by the elimina- tion rate constant (A,), which was obtained by re- gression of the terminal linear portion of the curve. Plasma clearance (CL) was calculated with use of the equation:
CL = Dose/AUC,,,.,,
The volume of distribution at steady-state (Vss) was calculated as:
V,, = [Dose * (AUMC/AUC2)] - (~/2. Dose/AU(Z)
in which AUMC is the area under the first-moment versus time curve from zero to infinity and r is the infusion duration. Mean residence time (MRT) was calculated as Vss/CL. The half-life (t,,*) was calcu- lated by dividing 0.693 by A,.
Curve fitting of individual subject data was per- formed with use of RStrip (Micromath, Salt Lake City, Utah), a computer modeling program. The model was selected with use of the Akaike informa- tion criterion of RStrip and by visual inspection. The mean of each parameter (A, (x, B, p), obtained by curve fitting, was used for simulations with PharmSim (Thomas Jefferson University, Philadel- phia, Pa.).
Statistical analysis. Patient characteristics and pharmacokinetic parameters of the two dosage groups were compared with use of the Mann- Whitney U test. The nonparametric equivalent of

100 mg/m’ 011726~ 011689e 011719j 011724h
Mean 2 SD
50.91 387 0.37 8.7 12.9 0.086 47.56 375 0.38 10.1 14.2 0.094 30.41 347 0.40 10.1 15.8 0.118 36.06 430 0.26 18.6 22.5 0.151
41.24 ? 9.62 385 2 35 0.35 + 0.063 1 1.9 2 4.5 16.3 -c 4.3 0. 112 2 0.029
500 mgim’ 011691i 010448e 011727a 011728k
166.79 276.76 208.63 212.60
1849 0.41 17.3 22.3 0.142 1846 0.31 10.5 13.1 0.099 2375 0.26 13.2 17.5 0.101 2202 0.29 13.9 18.6 0.108
Mean ? SD 216.19 -c 45.39 2068 + 264 0.32 5 0.065 13.7 ? 2.8 17.9 t 3.8 0.113 L 0.020
p Value 0.77* 0.56* 0.56 0.25 0.56 1.00
C max, Maximal concentration; AUC, area under the plasma concentration-time curve; CL, plasma clearance; t,,2, half-life; MRT, mean residence time; Vss, volume of distribution at steady state.
*p Value was calculated after correction for the difference in dose.
664 Wolf et al. CLINICAL PHARMACOLOGY&THERAPEUTICS
JUNE 1996
Table I. Patient characteristics Patient Gender
100 mgim” 011726~ Male 011689e Male 011719j Male 011724h Female
Mean t SD
500 mgim’ 011691i Male 010448e Male 011727a Male 011728k Male
Mean t SD
p Value
Age W Weight (kg) Height (cm) CD4 (cells/mm3)
36 79.5 185 450 40 82.3 185 340 51 77.3 186 230 36 56.8 160 550
41 ? 7 74.0 +- 11.6 179 + 13 393 2 138
26 91.8 185 280 42 58.6 165 400 36 64.5 172 200 39 73.2 173 450
36 k 7 72.0 ? 14.5 174 2 8 333 2 114
0.55 0.77 0.33 0.47
Table II. Pharmacokinetic parameters
Patient Cm, (b&4 AX (N * day/ml) CL (mlimin) t,, @ys) MRT (days) Vs, Wk9
the unpaired t test was chosen because of the small sample size.
RESULTS No significant differences in age, weight, height,
or baseline CD4 cell counts existed between the low- and high-dose groups (Table I). The mean 2 SD peak plasma concentrations (C,,) achieved in the low- and high-dose groups were 41.24 2 9.62 and 216.19 2 45.39 &g/ml, respectively. The concentra- tions on days 21 and 56 in the 100 mg/m’ dose group were 6.11 -C 0.66 and 0.78 + 0.57 &ml. For the 500
mg/m* dose group, the concentrations on days 21 and 56 were 28.02 + 5.82 and 6.07 ? 2.09 ug/ml, respectively. The C,, and AUC values were ap- proximately five times higher in the 500 mg/m2 dose group. The antibody was eliminated slowly, with a t,,, of approximately 13 days, and had a low clear- ante of 0.35 +- 0.063 and 0.32 -+ 0.065 ml/min for the 100 mg/m” and 500 mg/m’ doses, respectively. In addition to a long t,,2 and low clearance, the anti- body had a relatively small steady-state volume of distribution of 0.11 L/kg. There were no significant differences in any of the pharmacokinetic parame-

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 59, NC’MBER 6 Wolfe et al. 665
. I I
0 2b 3b .
sb &I 6b
Time (days)
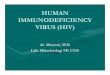
Fig. 1. Mean plasma concentration-time profiles of F105 in four subjects each, after intrave- nous infusion of 100 (circles) and 500 (triangles) mgim’.
ters calculated between the dose levels (Table II). The mean plasma concentration-time profiles for both dosage groups are displayed in Fig. 1.
A two-compartment model best described the data (Fig. 2). AUC estimates by the compartmental analysis were similar to the noncompartmental cal- culations. The mean distribution t,,z was 2.8 days and the mean elimination t,,, was 16.5 days.
DISCUSSION The t,,, of F105 in monkeys is 9 days, and on the
basis of interspecies differences, it was anticipated to be longer in humans.’ By comparison the t,,z of human serum IgG is reported to be 21 days. How- ever, this t,,, may be an underestimate, because it is based on radiolabeled IgG with a sampling duration of only 14 days.‘“,” Human monoclonal antibodies have an advantage of longer t,,z values than murine monoclonal antibodies or chimeric mouse/human monoclonals. For example, the t,,, of F105 seen in this study was 13 days compared with two anti-HIV IgG K murine monoclonal antibodies that displayed t,,, values of 1.3 days12 and a chimeric human/mouse antitumor antibody that displayed a t,,, of 4 days.13 The longer t,,2 values of human monoclonal anti-
0.00 20.00 40.00 Time (hours)
6I 00
Fig. 2. Plasma concentration-time profiles and the fitted curve for subject 011726h (squares) in the 100 mgim’ dosage group and subject 010448e (triangles) in the 500 mg/m’ dosage group.
bodies may allow for less frequent administration of these antibodies. This is a big advantage because therapeutic antibodies are expensive and require parenteral administration. The volume of distribu-

666 Wolf et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
JUNE I996
220 200,
180,
160,
140,
120,
100,
60 _
60 _
40,
20
I 1 I 21 42 63
Time (days)
Fig. 3. Simulation of 500 mgim’ F105 given every 21 days with use of the mean parameters for A, B, IX, and B obtained by curve fitting.
tion of F105 was approximately 8 L, which is nearly assess the tolerability of multiple doses and poten- twice the volume of plasma but less than the volume tial viral load reduction because dosage strategies of extracellular water. This suggests that the protein for this type of antibody remain speculative at this is mainly but not exclusively confined to the vascular time. Treatment with monoclonal antibodies such as space, which is consistent with the distribution of human serum IgG.lO,ll
F105 remains a promising therapeutic approach for patients with HIV infection.
The disposition of F105 appears to be linear for the doses studied; as demonstrated by the C,,, and AUC values, which were approximately five times greater in the 500 mg/m* dosage group compared with the 100 mg/m2 dosage group (Fig. 1).
References 1.
F105 has demonstrated neutralizing capacity to- ward primary and laboratory strains of the HIV virus. The concentration resulting in 50% inhibition (IC,,) for the IIIB and MN strains are 0.14 and 10 p&ml, respectively.* Although it is not known whether peak or trough concentrations are most important for optimal neutralizing capacity, it is presumed that maintaining the concentration above the IC,, of known laboratory strains is desirable. Multiple simulations of proposed dosage schedules were performed to select a dose and interval for future efficacy studies of F105. On the basis of these simulations, a dose of 500 mg/m2 every 21 days would achieve predicted mean steady-state peak and trough concentrations of approximately 220 and 40 t&ml, respectively, which would be achieved after the third dose (Fig. 3). The dosage interval of 21 days predicts minimal accumulation in most pa- tients. Studies of long-term dosage are under way to
2.
3.
4.
5.
6.
Cummins LM, Weinholf KJ, Matthews TJ, et al. Prep- aration and characterization of an intravenous solu- tion of IgG from human immunodeficiency virus- seropositive donors. Blood 1991;5:1111-7. Posner MR, Cavacini LA, Emes CL, Power J, Byrn R. Neutralization of HIV-l by F105, a human monoclo- nal antibody to the CD4 binding site of gp120. J Acquir Immune Defic Syndr 1993;6:7-14. Posner MR, Hideshina T, Cannon T, Mukherjee M, Mayer KH, Byrn RA. An IgG human monoclonal antibody that reacts with HIV-l/gpl20, inhibits virus binding to cells, and neutralizes infection. J Immunol 1991;146:4325-32. Starcich BR, Hahn BH, Shaw GS, et al. Identification and characterization of conserved and variable re- gions in the envelope gene of HTLV-IIIILAV, the retrovirus of AIDS. Cell 1986;45:637-48. Ho DD, Sarngadharan MG, Hirsch MS, et al. Human immunodeficiency virus neutralizing antibodies recog- nize several conserved domains on the envelope gly- coproteins. J Virol 1987;61:2024-8. Robert-Guroff M, Goedert JJ, Naugle CJ, Jennings AM, Battner WA, Gallo RC. Spectrum of HIV-l

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLL’ME 59, NUhlRER 6 Wolf et al. 667
neutralizing antibodies in a cohort of homosexual men: results of a 6-year prospective study. AIDS Res Hum Retroviruses 1988;4:343-50.
7. Lu W, Ahih Wk, Tourani JM, Eme D, Alter HJ, Andrieu JM. Lack of isolate-specific neutralizing ac- tivity is correlated with an increased viral burden in rapidly progressing HIV-l infected patients. AIDS 1993;7(suppl 2):S91-9.
8. Cavacini LA, Emes CL, Power J, et al. Loss of serum antibodies to a conformational epitope of HIV-l/ gp120 identified by a human monoclonal antibody is associated with disease progression. J Acquir Immune Defic Syndr 1993;6:1093-102.
9. Cavacini LA, Power J, Emes CL, Mace K, Treaty G, Posner MR. Plasma pharmacokinetics and biological activity of a human immunodefiency virus type 1 neu- tralizing human monoclonal antibody, F105, in cyno-
molgus monkeys. J Immunother Emphasis Tumor Im- munol 1994;4:251-6.
10. Solomon A, Waldmann TA, Fhaey JL. Metabolism of normal 6.6s y-globulin in normal subjects and in pa- tients with macroglobulinemia and multiple myeloma. J Lab Clin Med 1963;62:1-17.
11. Morel1 A, Terry WD, Waldman TA. Metabolic prop- erties of IgG subclasses in man. J Clin Invest 1970;49: 673-80.
12. Hinkula J, Gratt G, Gillan G, et al. Immunological and virological interaction in patients receiving passive immunotherapy with HIV-l neutralizing antibodies. J Acquir Immune Defic Syndr 1994;7:940-51.
13. LoBuglioli AF, Wheeler RH, Trang J, et al. Mouse/ human chimeric monoclonal antibody in man: kinetics and immune response. Proc Nat1 Acad Sci USA 1989; 86:4220-4.
Availability of Journal Back Issues
As a service to our subscribers, copies of back issues of Clinical Pharmacology 6 Therapeutics for the preceding 5 years are maintained and are available for purchase from the publisher, Mosby-Year Book, Inc., at a cost of $12.50 per issue. The following quantity discounts are available: 25% off quantities of 12 to 23, and 33% off quantities of24 or more. Please write to Mosby-Year Book, Inc., Subscription Services, 11830 Westline Industrial Dr., St. Louis, MO 63146-3318, or call (800)453-4351 or (314)453-4351 for information on availability of particular issues. Ifunavailable from the publisher, photocopies ofcomplete issues are available from UMI, 300 N. Zeeb Rd., Ann Arbor, MI 48106 (313)761-4700.