Embed Size (px)
Citation preview
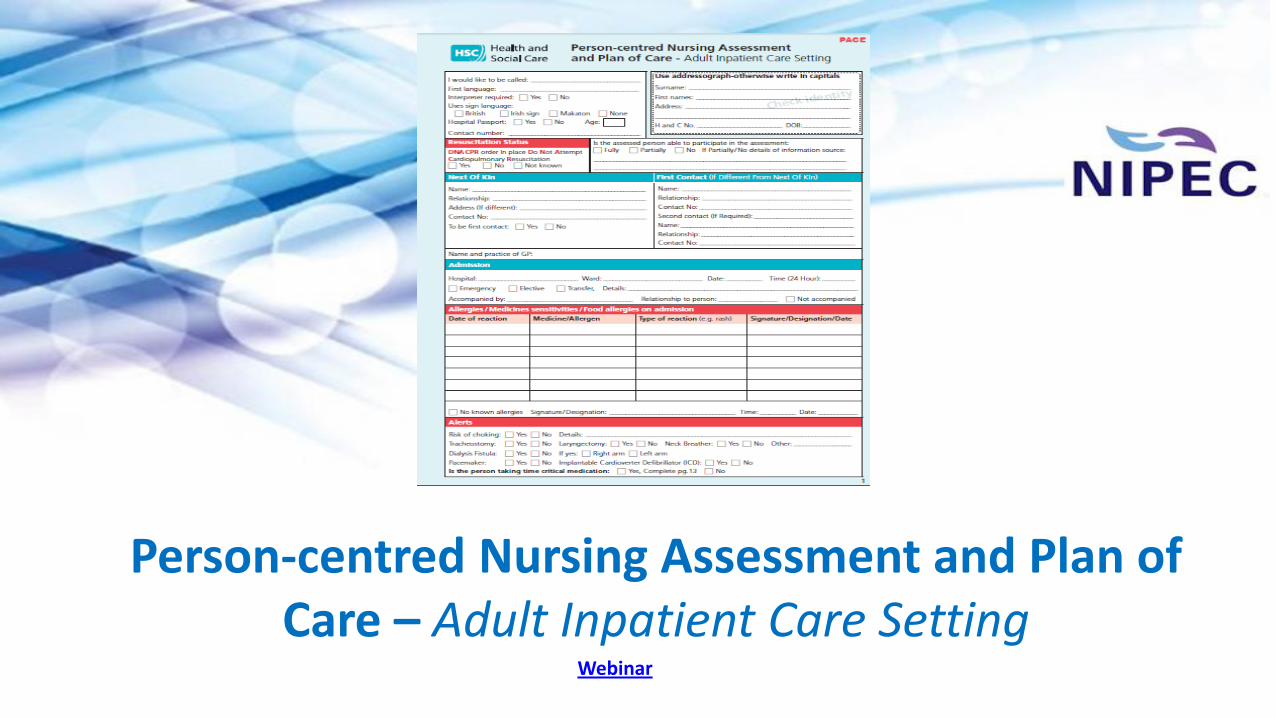
Person-centred Nursing Assessment and Plan of
Care – Adult Inpatient Care Setting Webinar
Why implement the document?
• To provide one document for Registered Nurses to complete when people are admitted into Adult
Inpatient Care Settings
• To reduce variation across the clinical settings in the region
• To prepare for digital adoption (Encompass)
• To ensure the document relates to current evidence within nursing and risk assessment
• To support the introduction of PACE in order to improve the standard of communication between nurses,
and because …..
“Good record keeping is an integral part of nursing and midwifery practice and is an essential component of safe, effective and person centred care provision” (NIPEC, 2017, p. 5).
Nurses and Midwives
MUST
‘Prioritise people’
and ensure
“their needs are recognised, assessed and responded to” (NMC, 2018, p. 6).
Person-centred Nursing Assessment and Plan of Care – Adult Inpatient Care Setting
was
designed, tested, reviewed and refined by ‘Adult
Nurses’ in NI
facilitated by NIPEC

One standard, regional document to be
used for ALL adults in the Adult Inpatient
Care Settings

You will either use ….
PACE (if implemented in your clinical setting)
or
Traditional care planning (if PACE is
not implemented in your clinical setting)
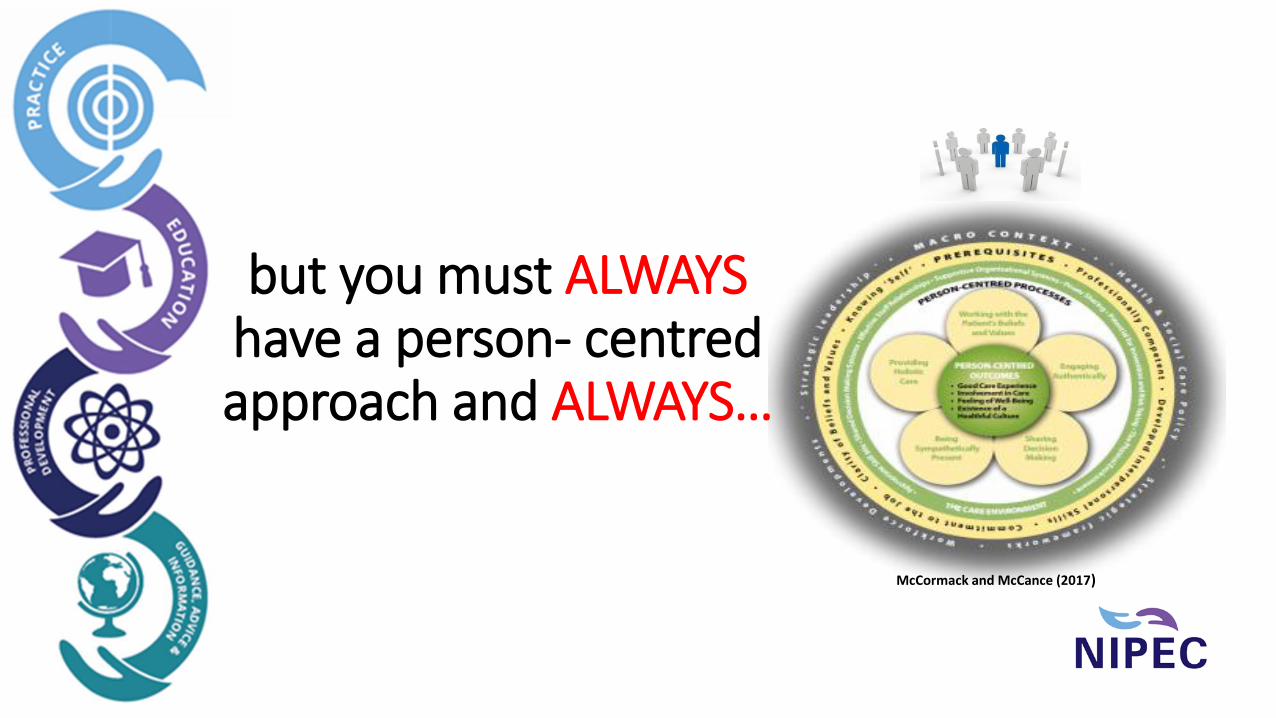
but you must ALWAYS have a person- centred approach and ALWAYS…
McCormack and McCance (2017)
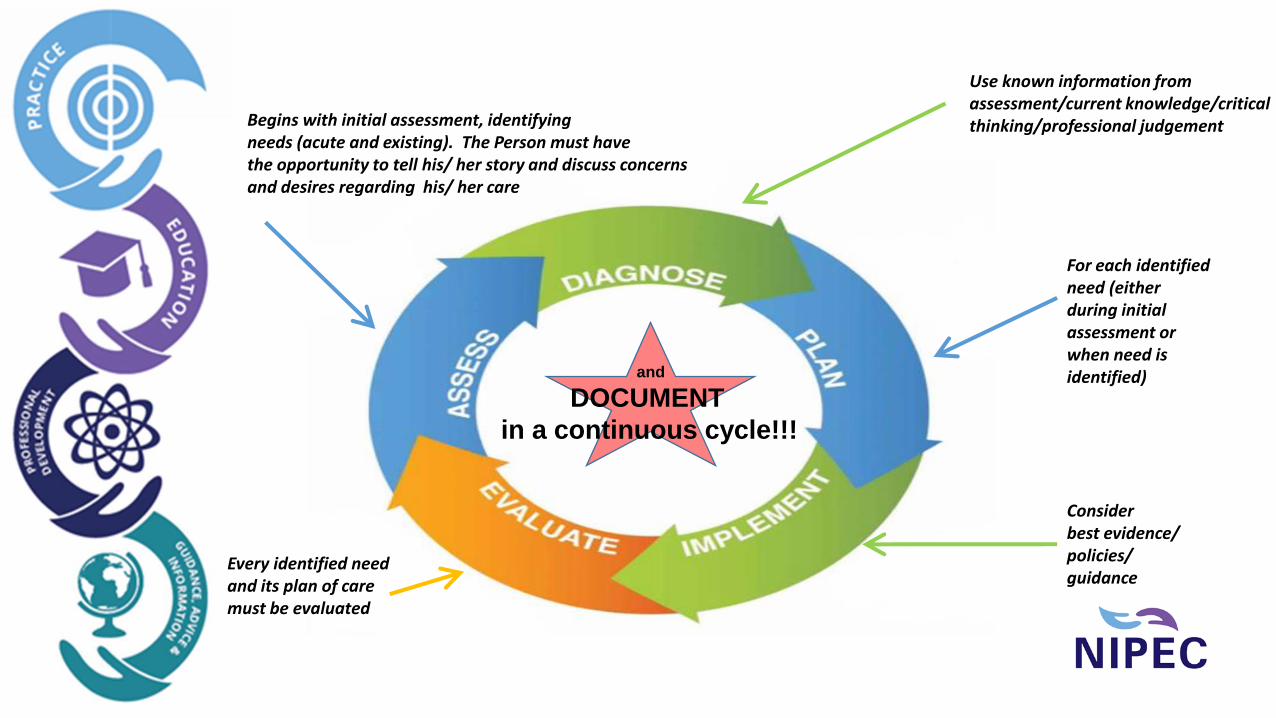
and
DOCUMENT
in a continuous cycle!!!
Begins with initial assessment, identifying needs (acute and existing). The Person must have the opportunity to tell his/ her story and discuss concerns and desires regarding his/ her care
For each identified need (either during initial assessment or when need is identified)
Every identified need and its plan of care must be evaluated
Use known information from assessment/current knowledge/critical thinking/professional judgement
Consider best evidence/ policies/ guidance
for everything we do!!! at everything we do!!!
Nurses should be aware of …..
Imaging from ‘Enabling professionalism in nursing and midwifery’ (NMC, 2018)
The Adult Inpatient Care Setting Document
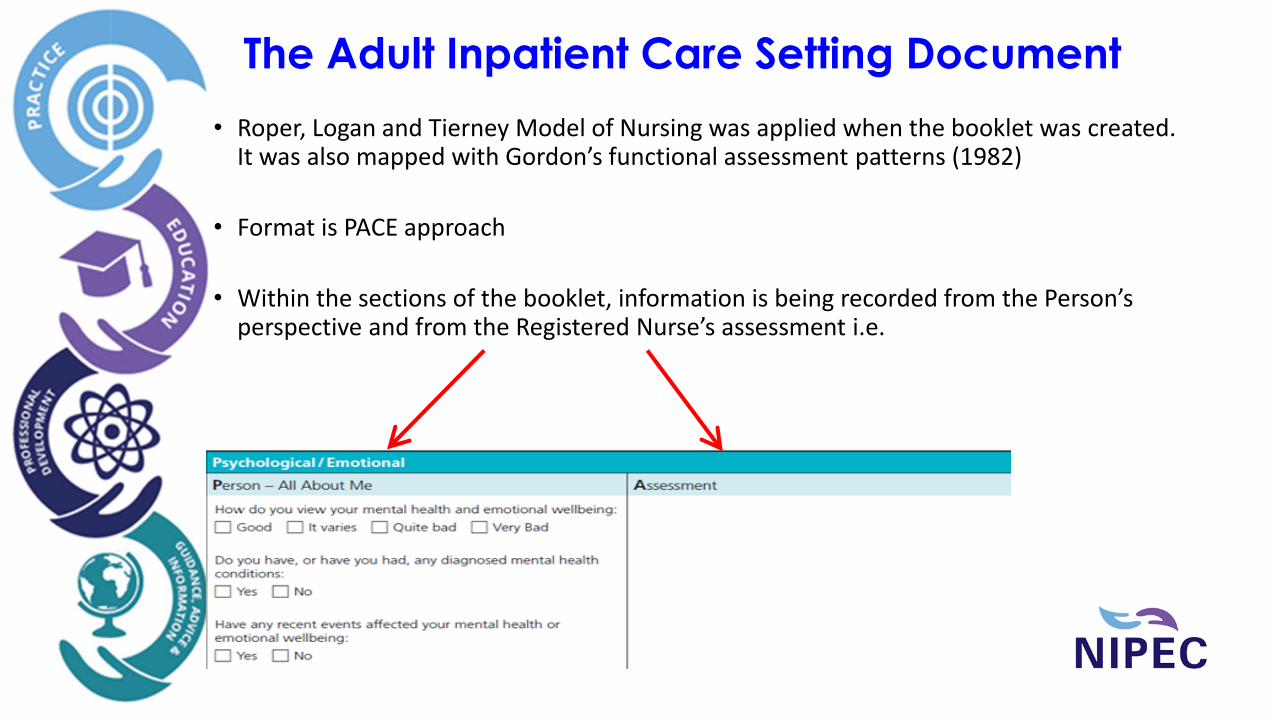
• Roper, Logan and Tierney Model of Nursing was applied when the booklet was created. It was also mapped with Gordon’s functional assessment patterns (1982)
• Format is PACE approach
• Within the sections of the booklet, information is being recorded from the Person’s perspective and from the Registered Nurse’s assessment i.e.

The Adult Inpatient Care Setting Document
• ‘Life critical information’ sections are in red filled banners and are located on mainly on Page 1 e.g.
• Risk assessment sections are in green filled banners e.g.
• Identification of needs sections, whether acute or existing, are in blue filled banners e.g.
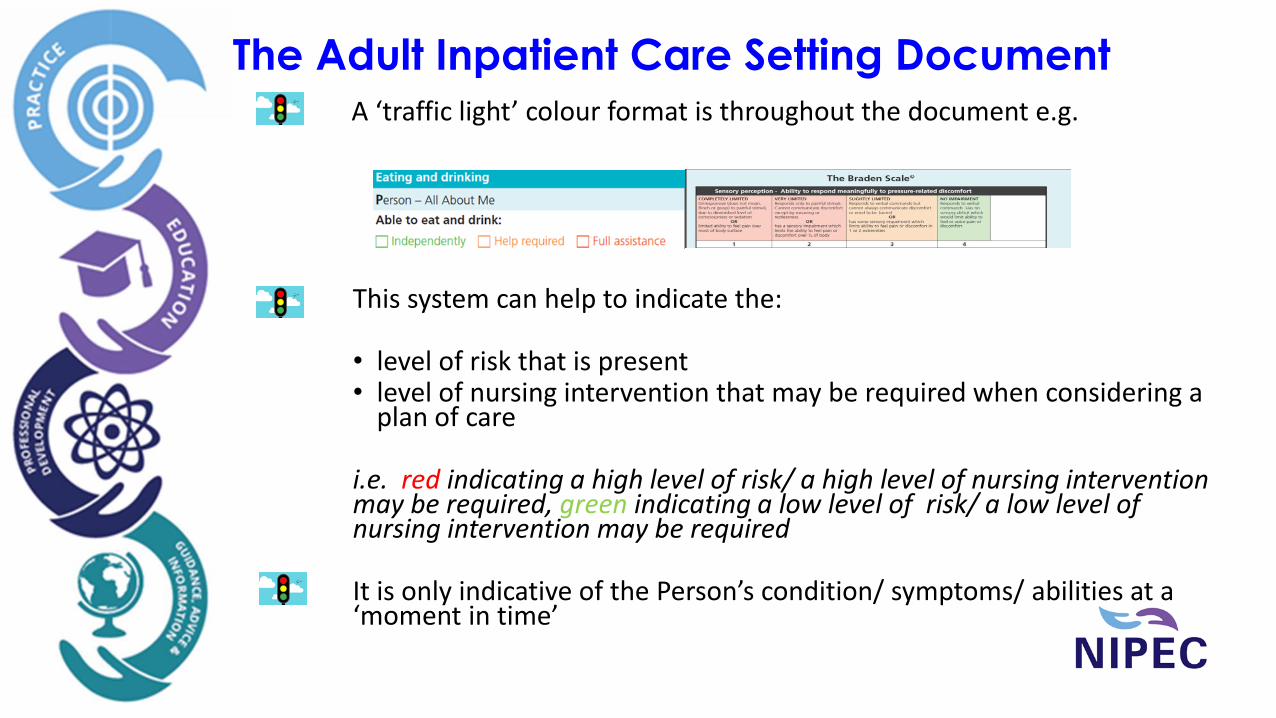
The Adult Inpatient Care Setting Document A ‘traffic light’ colour format is throughout the document e.g.
This system can help to indicate the:
• level of risk that is present • level of nursing intervention that may be required when considering a
plan of care i.e. red indicating a high level of risk/ a high level of nursing intervention may be required, green indicating a low level of risk/ a low level of nursing intervention may be required It is only indicative of the Person’s condition/ symptoms/ abilities at a ‘moment in time’
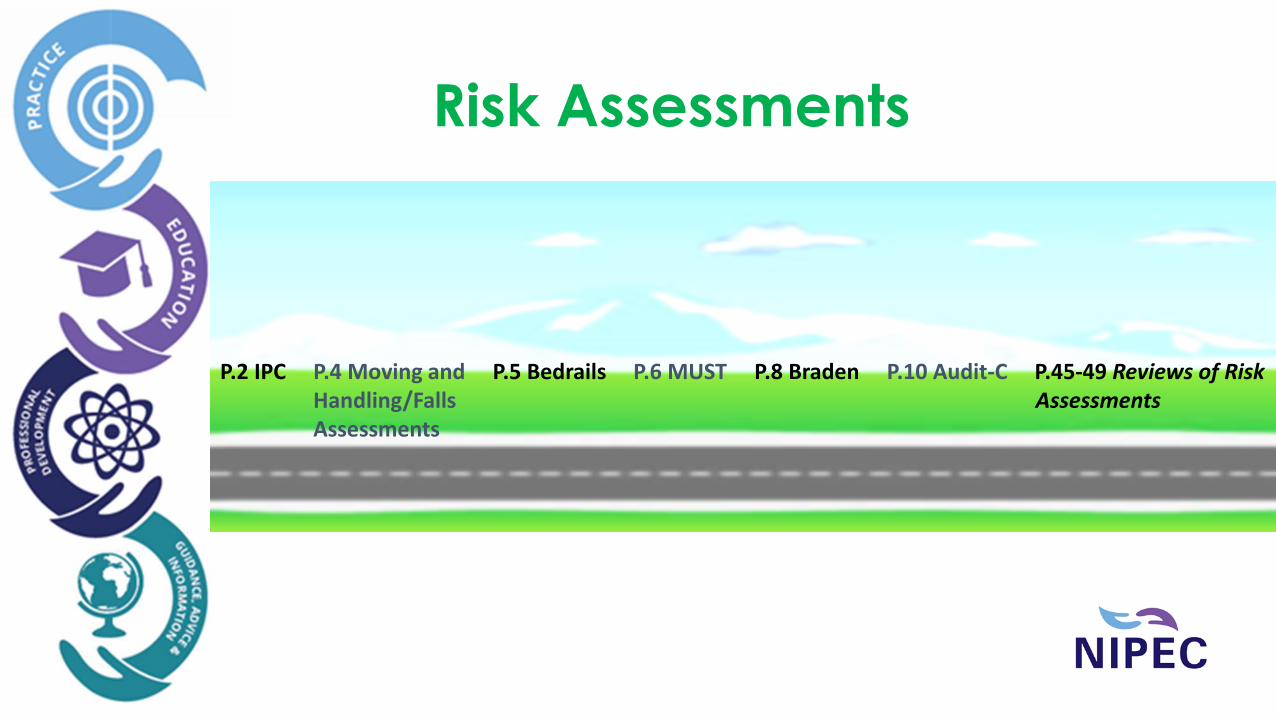
Risk Assessments
P.2 IPC P.4 Moving and P.5 Bedrails P.6 MUST P.8 Braden P.10 Audit-C P.45-49 Reviews of Risk Handling/Falls Assessments Assessments
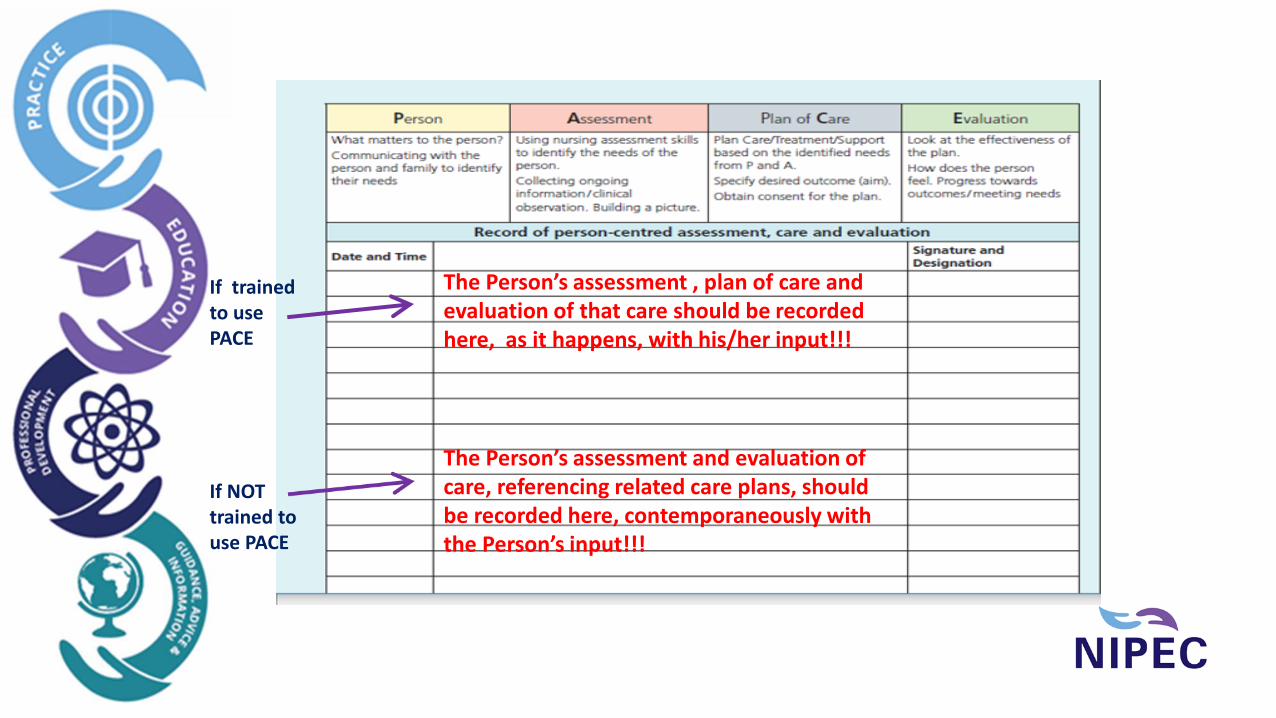
The Person’s assessment , plan of care and evaluation of that care should be recorded here, as it happens, with his/her input!!!
The Person’s assessment and evaluation of care, referencing related care plans, should be recorded here, contemporaneously with the Person’s input!!!
If trained to use PACE If NOT trained to use PACE
Person-centred Nursing Assessment and Plan of Care – Adult Inpatient Care Setting
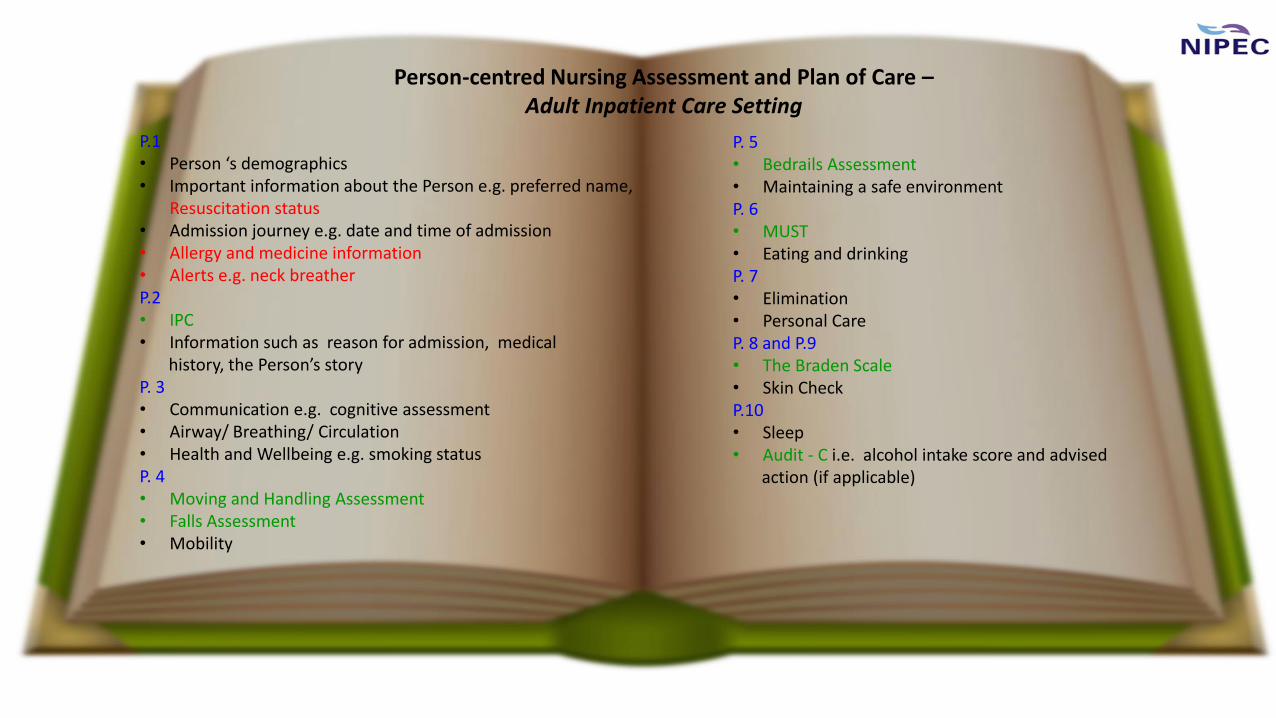
P.1 • Person ‘s demographics • Important information about the Person e.g. preferred name,
Resuscitation status • Admission journey e.g. date and time of admission • Allergy and medicine information • Alerts e.g. neck breather P.2 • IPC • Information such as reason for admission, medical history, the Person’s story P. 3 • Communication e.g. cognitive assessment • Airway/ Breathing/ Circulation • Health and Wellbeing e.g. smoking status P. 4 • Moving and Handling Assessment • Falls Assessment • Mobility
P. 5 • Bedrails Assessment • Maintaining a safe environment P. 6 • MUST • Eating and drinking P. 7 • Elimination • Personal Care P. 8 and P.9 • The Braden Scale • Skin Check P.10 • Sleep • Audit - C i.e. alcohol intake score and advised action (if applicable)

Person-centred Nursing Assessment and Plan of Care – Adult Inpatient Care Setting
P.11 and P.12 • Psychological/ Emotional • Body image • Religious/ Spiritual/ Cultural • Palliative Care (if applicable) • Social e.g. ‘are you a main carer’ question • Social and Home Support • Work and recreation P.13 • Pain • Person’s medications including Time Critical Medications P.14 • Summary of identified needs P.15 • Person’s valuables • Record of incomplete sections from initial assessment
P.16 – p.42 Record of person- centred assessment, care and evaluation P.43 • Hospital/ward transfer • Alerts/ food allergies since admission P.44 • Referrals P.45- 49 • Reviews of risk assessments P.50 & 51 • Discharge information including medication, wound management, transport P.52 • Signature register

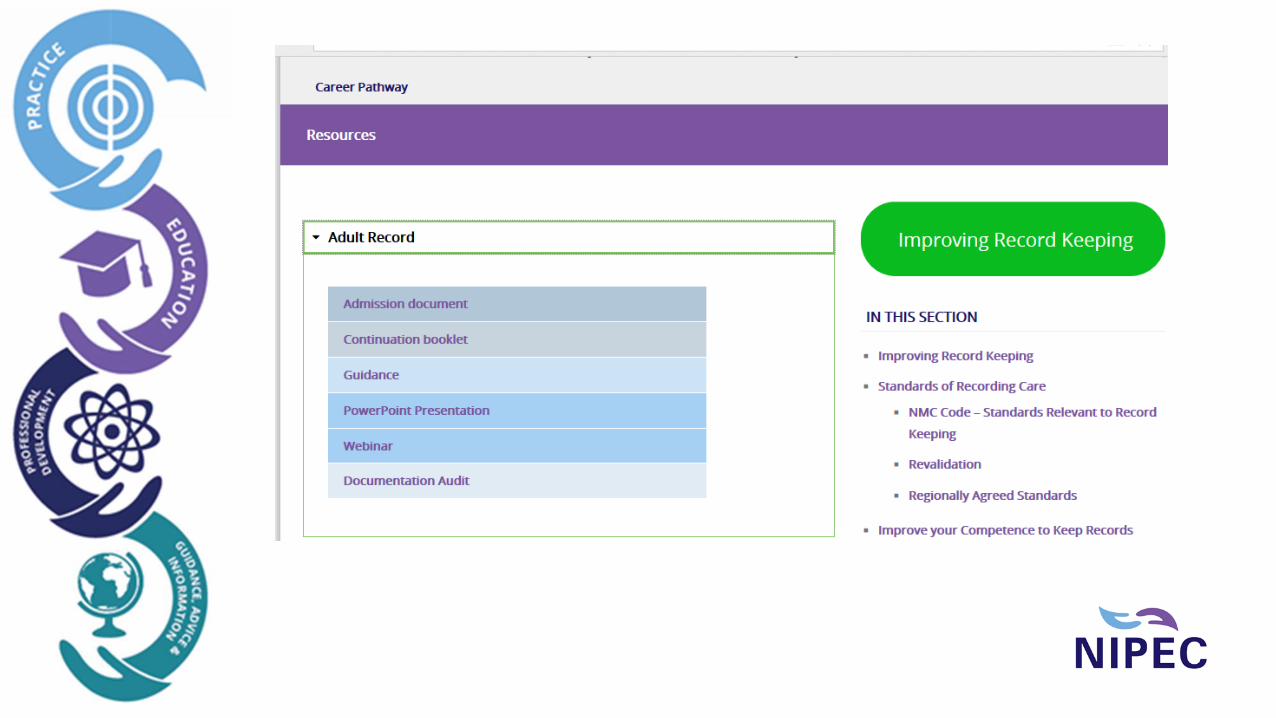
Resources for the Adult Inpatient Care Setting Document
http://www.nipec.hscni.net/resource-section/improve-record-keeping/resources/

The ‘Adult Inpatient Care Setting’ document encourages Registered Nurses to:
Prioritise people by involving “the person for whom the care is being provided for” (NIPEC, 2017, p. 6)
Prioritise people by documenting their person-centred assessment, plan of care and evaluation in a structured, factual and holistic manner, while ensuring the person shares “in decisions about their treatment and care” through “informed consent” (NMC, 2018, p. 7)
Finally…
The ‘Adult Inpatient Care Setting’ document encourages Registered Nurses to:
Practise effectively’ by “keeping clear and accurate records” (NMC, 2018, p. 9) to show that safe, effective, compassionate and person- centred care is being given to people and their families/ carers
Practise effectively by “ keeping clear and accurate records” (NMC, 2018, p. 9) to show evidence of decision making processes and professional ability. This should include documentation showing evidence based ways of working in clinical practice
Practise effectively by being “accountable for your decisions to delegate tasks and duties to other people” (NMC, 2018, P. 12)