-
Pranav M. Patel, MD, FACC, FSCAIDirector, Cardiac
Catheterization Lab
University of California, IrvineDivision of Cardiology
Peripheral Artery Disease (PAD): Diagnosis and Management
-
Acknowledgments
Consultant : Sanofi-Aventis, Terumo, Daiichi Sankayo
ACC/AHA (www.americanheart.org and www.acc.org) website
http://www.americanheart.org/�
-
What is P.A.D.? Peripheral Arterial Disease (P.A.D.) is a
common
yet serious disease. P.A.D. occurs when extra cholesterol and
fat
circulating in the blood collects in the walls of the arteries
that supply blood to your limbs.
P.A.D. can affect your quality of life, make walking difficult,
or worse, increase your risk of heart attack, stroke, leg
amputation, and even death.
A National Public Awareness Campaign from the P.A.D. Coalition
and the National Heart, Lung, and Blood Institute
-
Why should you learn about P.A.D.?
P.A.D. affects 8 to 12 million people within the U.S.,
especially those over age 50.
Early diagnosis and treatment of P.A.D. can help to… Prevent
disability and restore your mobility Stop the disease from
progressing Lower your risk for heart attack, heart disease,
and stroke
-
Peripheral Arterial Disease
-
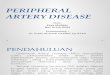
Ness J, Aronow WS. J Am Geriatric Soc. 1999;47:1255-1256.
Overlap of Atherosclerotic Disease
Patients with one manifestation often havecoexistent disease in
other vascular beds
CoronaryArtery
DiseaseCerebrovascular
Disease
Peripheral Arterial Disease6%
16%40%
11% 3%
15%
9%
38% overlap of 2 vascular beds
N= 1802 patientsMean age = 80 yrs (60-102)
-
How do you know if you have P.A.D.?
Most people with P.A.D. do not have the typical signs and
symptoms of the disease.
People who do experience symptoms often fail to report them
because they think they are a natural part of aging.
-
What are the signs and symptoms of P.A.D.?
Claudication—fatigue, heaviness, tiredness, cramping in the leg
muscles (buttocks, thigh, or calf) that occurs during activities
such as walking or climbing stairs
The pain or discomfort goes away once the activity is stopped or
during rest.
-
What causes P.A.D.?
Plaque builds up on artery walls, blocking flow of blood to the
arteries of the limbs, often the legs.
The cause of plaque buildup is unknown in most cases.
However, there are some conditions and habits that raise your
chance of developing P.A.D.
-
Are you at risk for P.A.D.? Are you over age 50? Do you smoke or
used to smoke? Do you have diabetes? Do you have high blood
pressure? Do you have high blood cholesterol? Do you have a
personal history of vascular disease,
heart attack, or stroke? Are you African American?
-
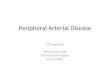
0% 5% 10% 15% 20% 25% 30% 35%
29%
11.7%
19.8%
19.1%
14.5%
4.3%
Prevalence of PAD
PARTNERS5Aged >70 years, or 50–69 years with a history
diabetes or smoking
San Diego2Mean age 66 years
Diehm4Aged 65 years
Rotterdam3Aged >55 years
NHANES1Aged 70 years
NHANES1Aged >40 years
NHANES=National Health and Nutrition Examination Study;
PARTNERS=PAD Awareness, Risk, and Treatment: New Resources for
Survival [program].1. Selvin E, Erlinger TP. Circulation.
2004;110:738-743.2. Criqui MH, et al. Circulation.
1985;71:510-515.3. Diehm C, et al. Atherosclerosis.
2004;172:95-105. 4. Meijer WT, et al. Arterioscler Thromb Vasc
Biol. 1998;18:185-192. 5. Hirsch AT, et al. JAMA.
2001;286:1317-1324.
In a primary care population defined by age and common risk
factors,
the prevalence of PAD was approximately one in
three patients
-
29% of Patients in a Target Population Were Diagnosed With PAD
Using An Office-Based ABI
Patients diagnosed with PADPAD onlyPAD and CVD
PARTNERS: Prevalence of PAD and Other CVD in Primary Care
Practices
29%44%
56%
ABI=ankle-brachial index; CVD=cardiovascular disease.
Hirsch, AT et al. JAMA. 2001;286:1317-24.
-
1. Meijer WT, et al. Arterioscler Thromb Vasc Biol.
1998;18:185-192. 2. Criqui MH, et al. Circulation.
1985;71:510-515.
Rotterdam Study (ABI
-
Gender Differences in the Prevalence of PAD
Adapted from Diehm C. Atherosclerosis. 2004;172:95-105 with
permission from Elsevier.
Prev
alen
ce (%
)
Women
Men
6880 Consecutive Patients (61% Female) in 344 Primary Care
Offices
85Age (years)
18
-
Ethnicity and PAD:The San Diego Population Study
NHW Black Hispanic Asian0123456789
10
Frac
tion
of P
opul
atio
n W
ith P
AD
(%)
NHW = Non-hispanic white. Reprinted with permission from Criqui,
et al. Circulation. 2005:112:2703-07.
-
More signs and symptoms of P.A.D. Cramping or pain in the legs
and/or feet at rest that
often disturbs sleep Sores or wounds on toes, feet, or legs that
heal
slowly, poorly, or not at all Color changes in the skin of the
feet, including
paleness or blueness A lower temperature in one leg compared to
the
other leg Poor nail growth and decreased hair growth on toes
and legs
-
Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192.
Relative Risk
Smoking
Diabetes
Hypertension
Hypercholesterolemia
Hyperhomocysteinemia
C-Reactive Protein
Reduced Increased
Risk Factors for PAD
1 2 3 4 5 60
-
Cardiologists and PADRationale
Coexistence of CAD & PAD Common risk factors &
modification Expertise in clinical evaluation of the patient
Expertise in risk factor adjustment Interest in longitudinal
follow-up and global
approach to patients disease
-
At risk for P.A.D.? Then…
Discuss this concern with your health care provider. Ask your
health care provider if you should be
screened or tested for P.A.D.
-
Think you may be at risk? Ask your health care provider…
Does my medical history put me at higher risk for P.A.D.?
Which screening tests or exams are right for me? If I have
P.A.D., what steps should I take to treat it? What steps can I take
to reduce my risk for heart
attack and stroke?
-
Physical Exam Findings of PAD
Limb examination (and comparison with the opposite limb)
includes: Absent or diminished femoral or pedal pulses (especially
after exercising
the limb) Pulse intensity - 0: absent, 1: diminished, 2: normal
, 3: bounding
Arterial bruits Hair loss Poor nail growth (brittle nails) Dry,
scaly, atrophic skin Dependent rubor Pallor with leg elevation
after 1 minute at 60 degrees (normal color
should return in 10 to 15 seconds; longer than 40 seconds
indicates severe ischemia)
Ischemic tissue ulceration (punched-out, painful, with little
bleeding), gangrene
Lesho EP, et al. Am Fam Physician. 2004;69:525-533.
The Physical Exam Should BePerformed With Patient’s Pants/Shoes
Off
-
More questions for your health care provider…
What is my blood sugar level? If I have diabetes, what should I
do about it?
What is my blood pressure? Do I need to do anything about
it?
What are my cholesterol numbers? Do I need to do anything about
them?
What can I do to quit smoking?
-
The First Tool to Establish the PAD Diagnosis:A Standardized
Physical Examination
Pulse assessment0 = absent1 = weak
2 = present (easily found)
-
http://www.nhlbi.nih.gov/health/dci/Diseases/pad/pad_diagnosis.html
ABI Procedure = Ankle/Brachial Index
-
Exercise ABI Testing
Confirms the PAD diagnosis
Assesses the functional severity of claudication
May “unmask” PAD when resting the ABI is normal
Aids differentiation of intermittent claudication vs.
pseudoclaudication diagnoses
-
Magnetic Resonance Angiography (MRA)
MRA has virtually replaced contrast arteriography for PAD
diagnosis
No ionizing radiation Non-iodine–based intravenous contrast
medium ~10% of patients cannot utilize MRA because of:
− Claustrophobia− Pacemaker/implantable cardioverter-
defibrillator− Obesity
• Gadolinium use in individuals with an eGFR
-
Computed Tomographic Angiography (CTA)
Requires iodinated contrast
Requires ionizing radiation
Produces excellent arterial picture
-
RightFem-Pop
BPG
CTA DSA(Pre-PTA)
LeftSFA
Stenosis
-
The overall goals for treating P.A.D.
Reducing the risk for heart attack and stroke Reducing any
symptoms Improving quality of life and mobility
-
Two main treatment approaches1. Reduce cardiovascular risk
Get help to quit smoking Lower blood pressure Lower LDL (bad)
cholesterol Manage diabetes Take anti-platelet medicines such as
aspirin or
clopidogrel Follow a healthy eating plan
-
Two main treatment approaches
2. Relieve leg pain symptoms Get regular exercise Special PAD
exercise program Medicines are available to improve
walking ability Special procedures or surgery, if needed
-
PAD: Prevention is Key
-
Risk Factors for PADNonmodifiable
Age Sex Family History (Race)
Modifiable
Cigarette smoking Diabetes mellitus Hypertension Dyslipidemia
Inflammatory Markers
(CRP) Hyperviscosity Hypercoagulability Hyperhomocysteminemia
Chronic renal
insufficiency
-
Effect of Smoking Cessation on Survival
0
20
40
60
80
100
0 1 2 3 4 5
Australian censusTobacco abstinenceContinued tobacco use
Years Postoperative
Faulkner KW, et al. Med J Aust. 1983;1:217-219.
133 Patients observed after bypass graft or lumbar
sympathectomyC
umul
ativ
e Su
rviv
al (%
)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb
IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb
IIIIIIIII
-
Intensive Antihypertensive Therapy in PAD: The ABCD Trial
0
10
20
30
40
Moderate treatment n = 227
Odd
s of
MI,
Stro
ke
or V
ascu
lar D
eath
Baseline ABI
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3
Intensive treatment n = 227*enalapril or nisoldipine
Reprinted with permission from Mehler, et al. Circulation.
2003;107;753-756.
-
Effects of Exercise Training on Claudication
Gardner AW, Poehlman ET. JAMA. 1995;274:975-980.
Exercise Training
Control
200
0
20
40
60
80
100
120
140
160
180
Onset of Claudication Pain
Maximal Claudication Pain
Chan
ge in
Tre
adm
ill W
alki
ng
Dis
tanc
e (%
)
Meta-analysis of 21 Studies
*
*
* P < 0.05
-
How can I reduce my risk for P.A.D.?
Don’t smoke/quit smoking. If you have diabetes, high blood
pressure, and/or
high cholesterol, talk to your health care provider about how to
manage your condition.
Eat a healthy diet full of fruits, vegetables, and whole
grains.
Be active for 30 minutes a day.
-
To Learn More about P.A.D. Visit:
P.A.D. Coalitionwww.PADCoalition.org
Vascular Disease Foundation www.vdf.org
Stay in Circulationwww.aboutpad.org
http://www.padcoalition.org/�http://www.vdf.org/�
-
Long-Term Survival in Patients With PAD
Criqui MH et al. N Engl J Med. 1992;326:381-386. Copyright ©
1992 Massachusetts Medical Society. All rights reserved.
Normal subjects
Asymptomatic PAD
Symptomatic PAD
Severe symptomatic PAD
100
75
50
25
0 2 4 6 8 10 12
Surv
ival
(%)
Year
-
PAD is often underestimated, under-evaluated, and requires
proper diagnosis:
ABI is a non-invasive, easily performed measurement that
reliably predicts ischemic risk in PAD patients
Symptoms of intermittent claudication (PAD) serves as an
important marker for systemic atherosclerotic complications
Key Points
-
Key Points
Aggressive management of modifiable risk factors is paramount in
decreasing risk for atherothromboembolic complications
Proactive and vigilant management of patients identified with
PAD will significantly decrease premature mortality & morbidity
increase the quality of life
Atherosclerosis: Systemic Problem
Peripheral Artery Disease (PAD): Diagnosis and
ManagementAcknowledgmentsWhat is P.A.D.?Why should you learn about
P.A.D.?Peripheral Arterial DiseaseOverlap of �Atherosclerotic
DiseaseHow do you know if you have P.A.D.?What are the signs and
symptoms of P.A.D.?What causes P.A.D.?Are you at risk for
P.A.D.?Prevalence of PAD�PARTNERS: Prevalence of PAD �and Other CVD
in Primary Care PracticesSlide Number 14Gender Differences in the
�Prevalence of PADEthnicity and PAD:�The San Diego Population
StudyMore signs and symptoms of P.A.D.Slide Number 18Cardiologists
and PAD�RationaleAt risk for P.A.D.? Then…Think you may be at risk?
Ask your health care provider…Physical Exam Findings of PADSlide
Number 25More questions for your health care provider…The First
Tool to Establish the PAD Diagnosis:�A Standardized Physical
ExaminationABI Procedure = Ankle/Brachial IndexExercise ABI
TestingMagnetic Resonance Angiography (MRA)Computed Tomographic
Angiography (CTA)Slide Number 32The overall goals for treating
P.A.D. Two main treatment approachesTwo main treatment
approachesPAD: Prevention is KeyRisk Factors for PADEffect of
Smoking Cessation on SurvivalIntensive Antihypertensive Therapy in
PAD: The ABCD TrialEffects of Exercise Training �on ClaudicationHow
can I reduce my risk for P.A.D.?To Learn More about P.A.D.
Visit:Long-Term Survival in Patients With PADSlide Number 44Key
Points