Embed Size (px)
Citation preview

SLEEP APNEA AND VENTILATORY DISORDERS IN ANESTHESIA (F CHUNG, SECTION EDITOR)
Perioperative Complications in Patients with ObstructiveSleep Apnea
Roop Kaw
Published online: 13 December 2013
� Springer Science + Business Media New York 2013
Abstract Recent literature is full of studies that have
brought forth several perioperative concerns in patients
with known or suspected obstructive sleep apnea. These
issues were first reported as independent observations or
case series, until data emerged from single centers and were
more recently confirmed from analysis of large databases of
hospitalized patients undergoing elective surgery. Among
these, the concerns raised most often are those of difficult
intubation and postoperative respiratory complications
requiring reintubation and mechanical ventilation; positive
airway pressure therapy, unplanned critical care service
admission or prolonged intensive care unit or hospital stay.
Others have reported cardiac events and unexpected/unex-
plained postoperative mortality. While all possible postop-
erative complications are not yet fully established or
understood, the prevention and management of these
complications may sometimes not be as challenging.
Keywords Perioperative � Anesthesia � Obstructive sleep
apnea � Continuous positive airway pressure � Sleep
disordered breathing � Polysomnography
Introduction
The prevalence of obstructive sleep apnea (OSA) among
patients undergoing elective surgery varies according to the
screening or diagnostic method of the study reporting it.
Recently, in the largest single academic registry of surgical
patients undergoing anesthesia, Ramachandran et al. [1]
reported a prevalence of 7 % patients with OSA. Similarly,
Memtsoudis et al. [2] reported a prevalence of sleep apnea
(billed diagnosis) in 1998 versus 2007 to be 0.4 and 2.7 %
for general surgical procedures and 0.4 and 5.5 % for
orthopedic procedures, respectively. Recent studies have
identified some of the specific risks among patients with
OSA in the surgical setting. Since patients with OSA are
prone to hypoxia especially during the night any added
insults during anesthesia induction or recovery, with
sedation or analgesia required in the perioperative setting,
can tend to exacerbate any hypoxia-related complication in
the postoperative period. This review examines the evi-
dence for these complications in detail and also discusses
some recommended strategies and interventions to mini-
mize possible adverse outcomes.
Difficult Intubation (DI)
Both anesthesia and sleep induce reductions in pharyngeal
dilator muscle activation and lung volume, thereby predis-
posing to upper airway obstruction. [3] Upper airway mus-
cular tone can be delayed (100–200 ms) or abolished during
inspiration in patients with OSA [4, 5]. In addition, upper
airway neuromotor responses are impaired in patients with
OSA relative to controls, and variability in collapsibility of
the upper airway between individuals cannot be explained by
structural loads alone [6]. Although DI has not been specif-
ically studied among patients with OSA, its major predictor,
as reported by Kheterpal et al. [7] among a cohort of 50,000
anesthetized patients, is body mass index (BMI)[30 kg/m2;
OSA and neck circumference[40 cm can also predict OSA
in the general population. The same can be said of clinical
predictors of DI such as the Mallampati score and short
R. Kaw (&)
Departments of Hospital Medicine and Anesthesiology
Outcomes Research, Cleveland Clinic, 9500 Euclid Avenue,
Cleveland, OH 44195, USA
e-mail: [email protected]
123
Curr Anesthesiol Rep (2014) 4:37–41
DOI 10.1007/s40140-013-0044-3

thyromental span [8]. Indeed, a close relationship has been
suggested between DI and the presence of OSA [9].
Strategies to Mitigate DI and/or Mask Ventilation
Isono et al. [10] reported passive closing pressures (PCLOSE)
among anesthetised OSA patients to be up to 9 cm H2O higher
than among non-OSA patients and recommended reduction
by about 10 cm of H2O. Proper positioning of the patient in the
sitting position can decrease the PCLOSE by 6 cmH2O and is
advantageous for mask ventilation. Similarly, the sniffing or
the ramp position will decrease the PCLOSE by 4 cmH2O,
also allowing both tracheal intubation and ventilation. Awake
intubation (with regional anesthesia and or sedation) and rapid
induction are preferred over slow induction when DI is sus-
pected [11]. Negative inspiratory pressure from spontaneous
breathing can induce negative constricting forces in the air-
way, which can progressively increase to -50 cm H2O and
cannot be possibly ameliorated by continuous positive airway
pressure (CPAP) during pharyngeal obstruction [12]. Pha-
ryngeal airway closure can be prevented by application of
10 cm of positive end expiratory pressure (PEEP) during
positive pressure ventilation in even the most severe cases of
OSA.
Postoperative Respiratory Failure
The other main concern among patients with OSA is post-
operative respiratory failure. In 1997, Ostermeier et al. [13]
reported three cases of sudden postoperative respiratory
arrest associated with epidural opioids in patients with sleep
apnea. All three patients died. Recently, looking at a large
inpatient database, Memtsoudis et al. [2] reported a five-
fold increase in intubation and mechanical ventilation after
orthopedic surgery (n *50,000) and two-fold increase after
general surgery (n *50,000) among patients with OSA
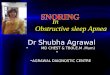
compared to controls. Our group confirmed a higher prev-
alence of postoperative respiratory failure in a meta-ana-
lysis of 3,942 patients with OSA (OR, 2.43; p = 0.003)
compared to controls [14] (Fig. 1). More recently, Mokhlesi
et al. [15], also using the NIS database, looked at postop-
erative outcomes among different surgical categories and
again found a higher need for emergent intubation and
postoperative mechanical ventilation unchanged across all
surgical categories. Interestingly enough, after adjusting for
the age, sex and Charleston comorbidity index, patients
without sleep-disordered breathing (SDB) requiring emer-
gent intubation had significantly worse outcomes compared
to those with SDB requiring emergent intubation. The need
for emergent intubation and mechanical ventilation was
higher on the day of surgery or the first postoperative day
compared to patients without SDB. Among possible
explanations for both of these findings provided by the
authors was that events requiring intubation and mechanical
ventilation in patients with SDB could be mostly related to a
rapidly reversible upper airway complication in the setting
of opioid and sedative use in the immediate postoperative
period or perhaps a lower threshold was used for intubating
patients with OSA or transferring them to the intensive care
unit (ICU). Both of these studies using the NIS data [2, 15]
were dominated by the orthopedic surgical cohort
(n *1,000,000) and showed a steadily increasing preva-
lence of OSA from the start of the study period to the end.
Early reports among patients with obesity hypoventilation
syndrome (OHS) undergoing elective surgery show that the
incidence of postoperative respiratory failure may be even
higher and that OHS is more likely to be unrecognized
before elective non-cardiac surgery when compared to OSA
[16]. Another subset of patients with OSA on chronic opiate
Study or Subgroup
Ahmad 2008Finkel 2009Gali 2009Gupta 2001Kaw 2006Kaw 2009Luizaga 2010Sabers 2003Vasu 2010
Total (95% CI)
Total eventsHeterogeneity: Chi² = 7.06, df = 6 (P = 0.31); I² = 15%Test for overall effect: Z = 2.93 (P = 0.003)
Events
01065
16014
33
Total
31661221101
37270
69234
56
1680
Events
1002
164010
24
Total
92117
472101185202
22234
79
3421
Weight
15.3%1.6%
12.8%31.5%29.4%
6.8%2.6%
100.0%
M-H, Fixed, 95% CI
0.09 [0.00, 2.41]9.62 [0.39, 236.37]
Not estimable3.13 [0.62, 15.87]
1.65 [0.56, 4.83]3.12 [1.03, 9.47]
Not estimable1.00 [0.06, 16.08]
13.63 [0.72, 258.43]
2.43 [1.34, 4.39]
OSA Non-OSA Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours OSA Favours Non-OSA
Fig. 1 Postoperative respiratory failure as reported among patients with OSA undergoing elective surgery. From ‘‘In the December 2012 BJA …,’’
Br. J. Anaesth. (2012), 109 (6): vi, with permission from Oxford University Press
38 Curr Anesthesiol Rep (2014) 4:37–41
123

therapy has been shown to fail CPAP therapy more often
than those who are not chronically on opioids for pain
control [17••]. This has been attributed to the presence of
central sleep apnea during CPAP, a condition known as
complex sleep apnea, as well as poorly understood breath-
ing patterns.
Depending upon the definition used among the different
studies reported in the literature as well as their respective
sample size, postoperative respiratory failure has not been
consistently reported among patients with OSA. Moreover,
some of the single-center studies were originally initiated
as quality improvement (QI) projects and hence by design
report fewer postoperative respiratory complications than
others [18–21]. Among other reasons for variations in
reporting of postoperative complications between different
studies are whether OSA was diagnosed clinically by
screening or by a gold standard test and, especially among
the case control studies, whether the comparison was
against a group of ‘true controls’ (OSA excluded by formal
polysomnography).
Unanticipated ICU Transfer
Although ICU transfer has been used as an outcome measure
among patients with OSA who undergo surgery, it is not
always easy to track as patients are often sent to ICU over-
night for observation. After excluding studies [22] that made
specific mention of such practices, our meta-analysis showed
that the presence of OSA was significantly associated with
higher odds of ICU transfer [105/2,062 (5.09 %) versus
58/3,681 (1.57 %), respectively; OR 2.29, 95 % CI
1.62–3.24, p B 0.00001, (I2 = 57–68 %, p B 0.02] after
surgery. It is even harder to get this information from the two
recent studies reporting on a large number of surgical
patients as NIS data [12, 14] do not report use of advanced
services such as critical care, step down and telemetry ser-
vices when reporting or estimating charges. A recent study
using the STOP-BANG score as a predictor of postoperative
critical care admission reported OR of 2.2 (95 % CI 1.1–4.6;
p = 0.037), 3.2 (95 % CI 1.2–8.1; p = 0.017) and 5.1 (95 %
CI: 1.8–14.9; p = 0.002) for STOP-BANG scores of 4, 5
and C6, respectively [23].
Postoperative Mortality
Gami et al. [24], looking at autopsy reports, reviewed 112
reports of sudden death and found that almost half of the
patients with polysomnographically confirmed OSA died
during sleep hours (12 midnight to 6.00 am) compared to
21 % of those without OSA (RR: 2.57). More recently, the
same group of authors showed that OSA independently
predicted sudden cardiac death (SCD), and among these
patients, the lowest nocturnal oxygen desaturation and AHI
were independent predictors of SCD [4, 25]. A few studies
that have looked at postoperative mortality [14, 25] did not
find any association between OSA and mortality after
elective surgery. In fact, Mokhlesi et al. found lower
mortality among patients with OSA undergoing cardiac
(OR 0.54; 95 % CI 0.40–0.73; p \ 0.001), orthopedic (OR
0.65; 95 % CI 0.45–0.95; p = 0.03) and abdominal surgery
(0.38; 95 % CI 0.22–0.65; p = 0.001) compared to those
without OSA. The study used administrative data that limit
the validity of the OSA diagnosis as well as use of
advanced and critical care services; hence, the investigators
cannot provide any plausible explanation for this result and
advise cautious interpretation. Recently, Lockhart et al.
[26] did not find any difference in 30-day and 1-year
postoperative mortality among patients with OSA under-
going elective surgery compared to controls. However,
patients who screened as high risk for OSA by the Flemon,
STOP or STOP-BANG criteria revealed higher mortality at
1 year compared to the group that screened as low risk for
OSA, but no causal inferences can be made. This observed
lack of association between postoperative mortality and
OSA does not necessarily mean that death cannot be an
expected sentinel event in a postoperative patient with
OSA especially if exposed to additional insults such as a
failed airway, an unmonitored respiratory depression opi-
oid and/or sedative administration especially with PCA
infusions and others. Clearly the incidence of such events
in the perioperative setting when reported from the large
administrative databases is low enough to pass any statis-
tical rigor of association.
Perioperative Risk Reduction Strategies in Obstructive
Sleep Apnea (OSA)
Some patients present with DI and airway management
issues. Patients with known OSA using CPAP at home
should be advised to bring their machine to the hospital at
the preoperative visit. Patients who are noncompliant
should be encouraged to use it more consistently. In
patients with previously undiagnosed OSA and high clin-
ical suspicion of OSA based on preoperative assessment, if
significant use of opioids and sedation is anticipated based
on the type of the surgical procedure, consideration should
be given to inpatient surgery as opposed to ambulatory
surgery. Wherever possible regional anesthesia and blocks
are preferred and for general anesthesia, short-acting agents
such as desflurane and propofol are recommended. A
recent study on sleep apnea patients undergoing total joint
arthroplasty found that patients undergoing surgery under
neuraxial anesthesia had significantly lower rates of major
Curr Anesthesiol Rep (2014) 4:37–41 39
123

complications compared to cases in which combined
neuraxial and general or general anesthesia was used
[27••]. When using general anesthesia, the possibility of DI
should be kept in mind, and preparation for induction and
intubation should follow the ASA difficult airway guide-
lines [28]. Full reversal of neuromuscular blockade (when
applicable) with use a nerve stimulator should be verified
prior to extubation [29]. These patients must be fully
awake, normothermic, hemodynamically stable, and
spontaneously breathing with an adequate respiratory rate
and tidal volume prior to breathing.
Multimodal analgesia involving the use of NSAIDS,
acetaminophen, tramadol, ketamine, pregabalin and COX-
2 inhibitors should be considered to minimize the use of
opioids in the postoperative setting [30]. OSA patients
receiving opioids are more likely than patients receiving
nonopiod analgesia to have perioperative oxygen desatu-
ration [31]. Patients undergoing ambulatory surgeries
should be observed for an extended period of time prior to
their discharge home [32]. Continuous pulse oximetry
monitoring is recommended in the postoperative setting in
patients at risk for respiratory complications of OSA.
Cautious use of supplemental oxygen is advised after
extubation until the patient is able to maintain his/her
baseline oxygen saturation on room air. If frequent or
severe airway obstruction or hypoxemia is noted in the
postoperative monitoring period, consideration should be
made to initiate CPAP of NIPPV.
The role of CPAP used perioperatively among patients
with OSA has not been well studied. Indirect evidence can be
obtained from patients undergoing bariatric surgery who
happen to have a higher prevalence of OSA and have often
had the chance to have a treatment plan initiated before sur-
gery. Although some series have reported higher postopera-
tive complication rates among bariatric surgical patients with
OSA, in others most patients were preoperatively diagnosed
and treated with PAP therapy; the presence or severity of
OSA did not lead to a higher postoperative complication rate.
[33]. Among patients with OSA cardioverted for atrial
fibrillation, those treated with CPAP were less likely to
develop recurrent atrial fibrillation within 12 months of car-
dioversion compared to patients without treatment with CPAP
[34]. A recent study randomized patients with a high Sleep
Apnea Clinical Score (SACS) undergoing elective orthopedic
surgery to standard care with auto-PAP and to standard care
alone. No differences in length of stay (p = 0.65) or sec-
ondary outcomes (including unplanned ICU transfer,
arrhythmia, MI or delirium) were observed between the two
groups [35••]. Some of the main limitations of this study,
were incomplete resolution of OSA as suggested by a median
residual AHI of 13.5 events/h, inability to distinguish central
sleep apnea from OSA and limited adherence in a hospital
setting. Conclusive evidence mandating empiric use of CPAP
perioperatively among patients not currently using it is still
lacking. More studies are needed.
Conclusions
Clinicians taking care of patients with OSA are often
intrigued and concerned about safe perioperative care.
Studies to date have shown that OSA is vastly underesti-
mated in the general population and often undiagnosed in
surgical patients; hence, it can lead to higher postoperative
morbidity. Early clinical recognition of OSA can definitely
help in designing a safer careplan.
Compliance with Ethics Guidelines
Conflict of Interest Roop Kaw declares that he has no conflict of
interest.
Human and Animal Rights and Informed Consent This article
does not contain any studies with human or animal subjects per-
formed by any of the authors.
References
Papers of particular interest, published recently, have been
highlighted as:•• Of major importance.
1. Ramachandran SK, Kheterpal S, Consens F, Shanks A, Doherty
TM, Morris M, Tremper KK. Derivation and validation of a
simple perioperative sleep apnea prediction score. Anesth Analg.
2010;110(4):1007–15.
2. Memtsoudis S, Liu SS, Ma Y, et al. Perioperative pulmonary
outcomes in patients with sleep apnea after non-cardiac surgery.
Anesth Analg. 2011;112:113–21.
3. Hillman DR, Platt PR, Eastwood PR. Anesthesia, sleep, and
upper airway collapsibility. Anesthesiol Clin. 2010;28:443–55.
4. Remmers JE, deGroot WJ, Sauerland EK, et al. Pathogenesis of
upper airway occlusion during sleep. J Appl Physiol.
1978;44:931–8.
5. Strohl KP, Hensley MJ, Hallett M, et al. Activation of upper
airway muscles before onset of inspiration in normal humans.
J Appl Physiol. 1980;49:638–42.
6. McGinley BM, Schwartz AR, Schneider H, Kirkness JP, Smith
PL, Patil SP. Upper airway neuromuscular compensation during
sleep is defective in obstructive sleep apnea. J Appl Physiol.
2008;105:197–205.
7. Kheterpal S, Martin L, Shanks AM, et al. Prediction and out-
comes of impossible mask ventilation: a review of 50,000 anes-
thetics. Anesthesiology. 2009;110:891–7.
8. Shiga T, Wajima Z, Inoue T, Sakamoto A. Predicting difficult intu-
bation in apparently normal patients: a meta-analysis of bedside
screening test performance. Anesthesiology. 2005;103:429–37.
9. Hiremath AS, Hillman DR, James AL, et al. Relationship
between difficult tracheal intubation and obstructive sleep
apnoea. Br J Anaesth. 1998;80:606–11.
10. Isono S. Optimal combination of head, mandible and body
positions for pharyngeal airway maintenance during perioperative
40 Curr Anesthesiol Rep (2014) 4:37–41
123

period: lesson from pharyngeal closing pressures. Semin Anesth.
2007;26:83–93.
11. Benumof JL. Management of the difficult airway. With special
emphasis on awake intubation. Anesthesiology. 1991;75:1087–110.
12. Sato Y, Ikeda A, Ishikawa T, Isono S. How can we improve mask
ventilation in patients with obstructive sleep apnea during anes-
thesia induction. J Anesth. 2013;27(1):152–6.
13. Ostermeier AM, Roizen MF, Hautkappe M, Klock PA, Klafta
JM. Three sudden postoperative respiratory arrests associated
with epidural opioids in patients with sleep apnea. Anesth Analg.
1997;85:452–6.
14. Kaw R, Chung F, Pasupuleti V, Mehta J, Gay PC, Hernandez AV.
Meta-analysis of the association between obstructive sleep apnoea
and postoperative outcome. Br J Anaesth. 2012;109:897–906.
15. Mokhlesi B, Hovda MD, Vekhter B, Arora VM, Chung F,
Meltzer DO. Sleep-disordered breathing and postoperative out-
comes after elective surgery: analysis of the Nationwide Inpatient
Sample. Chest. 2013;144(3):903–14.
16. Kaw R, Pasupuleti V, Walker E, et al. Obesity hypoventilation
syndrome: an emerging and unrecognized risk factor among
surgical patients. Am J Respir Crit Care Med. 2011;183:A3147.
17. •• Guillenminault C, Cao M, Yue HJ, Chawla P. Obstructive
sleep apnea and chronic opioid use. Lung. 2010;188:459–468.
This important study describes two new abnormal breathing
patterns among non-obese patients with OSA who were on
chronic opioid therapy which have not been reported so far.
These patterns as well as central sleep apneas were completely
eliminated with bi-level PAP therapy with a back-up rate.
18. Hwang D, Shakir N, Limann B, Sison C, Kalra S, Shulman L, Souza
Ade C, Greenberg H. Association of sleep-disordered breathing with
postoperative complications. Chest. 2008;133(5):1128–34.
19. Gali B, Whalen FX, Gay PC, et al. Management plan to reduce
risks in perioperative care of patients with presumed obstructive
sleep apnea syndrome. J Clin Sleep Med. 2007;3:582–8.
20. Finkel KJ, Searleman AC, Tymkew H. Prevalence of undiag-
nosed obstructive sleep apnea among adult surgical patients in an
academic medical center. Sleep Med. 2009;10:753–8.
21. Gali B, Whalen FX, Schroeder DR, Gay PC, Plevak DJ. Identi-
fication of patients at risk for postoperative respiratory compli-
cations using a preoperative obstructive sleep apnea screening
tool and post-obstructive anesthesia care assessment. Anesthesi-
ology. 2009;110:869–77.
22. Liao P, Yegneswaran B, Vairavanathan S, Zilberman P, Chung F.
Postoperative complications in patients with obstructive sleep
apnea: a retrospective cohort matched study. Can J Anaesth.
2009;56(11):819–28.
23. Chia P, Seet E, Macachor JD, Iyer US, Wu D. The association of
preoperative STOP-BANG scores with postoperative critical care
admission. Anesthesia. 2013;68(9):950–2. doi:10.1111/anae.12369.
24. Gami AS, Howard DE, Olson EJ, Somers VK. Day night pattern
of sudden death in obstructive sleep apnea. N Engl J Med.
2005;352(12):1206–14.
25. Gami AS, Olson EJ, Shen WK, Wright RS, Ballman KV, Hodge
DO, Herges RM, Howard DE, Somers VK. Obstructive sleep
apnea and the risk of sudden cardiac death: a longitudinal study
of 10,701 adults. J Am Coll Cardiol. 2013;62(7):610–8.
26. Lockhart EM, Willingham MD, Abdallah AB, Helsten DL, Be-
dair BA, Thomas J, Duntley S, Avidan MS. Obstructive sleep
apnea screening and postoperative mortality in a large surgical
cohort. Sleep Med. 2013;14(5):407–15.
27. •• Memtsoudis SG, Stundner O, Rasul R, et al. Sleep apnea and
total joint arthroplasty under various types of anesthesia: a pop-
ulation-based study of perioperative outcomes. Reg Anesth Pain
Med. 2013;38:274–281. This important study using a large
pharmaceutical database is amongst the first ones to compare
outcomes among patients with OSA undergoing joint replacement
surgery using different types of anesthesia. Lower rates of
mechanical ventilation; critical care service admission, blood
transfusion and lower length of stay were reported among
patients who underwent surgery under neuraxial anesthesia.
28. Rosenblatt WH, Whipple J. The difficult airway algorithm of the
American Society of Anesthesiologists. Anesth Analg.
2003;96:1233.
29. Murphy GS, Szokol JW, Marymont JH, Greenberg SB, Avram
MJ, Vender JS. Residual neuromuscular blockade and critical
respiratory events in the postanesthesia care unit. Anesth Analg.
2008;107:130–7.
30. Chung SA, Yuan H, Chung F. A systematic review of obstructive
sleep apnea and it’s implications for anesthesiologists. Anesth
Analg. 2008;107:1543–63.
31. Bolden N, Smith CE, Auckley D, Makarski J, Avula R. Periop-
erative complications during use of an obstructive sleep apnea
protocol following surgery and anesthesia. Anesth Analg.
2007;105:1869–70.
32. Gross JB, Bachenberg KL, Benumof JL, American Society of
Anesthesiologists Task Force on Perioperative Management,
et al. Practice guidelines for the perioperative management of
patients with obstructive sleep apnea: a report by the American
Society of Anesthesiologists Task Force on Perioperative Man-
agement of patients with obstructive sleep apnea. Anesthesiology.
2006;104:1081–93.
33. Weingarten TN, Flores AS, McKenzie JA, et al. Obstructive sleep
apnoea and perioperative complications in bariatric patients. Br J
Anaesth. 2011;106:131–9.
34. Kanagala R, Murali NS, Friedman PA, et al. Obstructive sleep
apnea and the recurrence of atrial fibrillation. Circulation.
2003;107:2589–94.
35. •• O’gorman SM, Gay PC, Morgenthaler TI. Does auto-titrating
positive airway pressure therapy improve postoperative outcome
in patients at risk for obstructive sleep apnea syndrome? A ran-
domized controlled clinical trial. Chest. 2013;144:72–78. This
important trial randomized patients suspected to be at high risk
for OSA to standard care versus standard care?empirical auto-
titrating positive airway pressure therapy (APAP) after elective
joint replacement surgery and found no difference in length of
stay, ICU transfer, cardiac events/arrhythmia, delirium between
the two groups.
Curr Anesthesiol Rep (2014) 4:37–41 41
123