Embed Size (px)
Citation preview

PERIODONTITIS AND DEMENTIA – A SYSTEMATIC REVIEW
Sam Asher
Master thesis
Public Health
School of Medicine
Faculty of Health Sciences
University of Eastern Finland
December 2018

2
UNIVERSITY OF EASTERN FINLAND, Faculty of Health Sciences,
Institute of Public Health and Clinical Nutrition, Public Health.
ASHER S.: Periodontitis and Dementia - a systemic review.
Master's thesis, 96 Pages.
Instructors: Professor Tomi-Pekka Tuomainen, Adjunct Professor Alina Solomon and Ruth
Stephen.
December 2018.
Keywords: Dementia, Alzheimer’s disease, cognitive impairment, memory impairment, cognitive
deterioration, periodontitis, tooth loss.
ABSTRACT
Several studies indicate a possible association between periodontitis and dementia. Additionally, the
available scientific literature also suggests that periodontitis may be related to cognitive impairment.
This review aimed to systematically assess and evaluate the scientific literature on the impact of
periodontitis on the risk of dementia and cognitive impairment.
The online scientific databases (PubMed and Scopus) were searched for original English language,
longitudinal studies that assessed the role of periodontitis in determining the risk of dementia and
cognitive impairment. In total 10 studies complied with the inclusion criteria, with 5 concerning
dementia as the outcome and 5 cognitive impairment. The studies included in this review were also
assessed for the quality of evidence in four major and one minor domain.
Four studies reported association between periodontitis and dementia. Evidence supporting the possible
role of periodontitis in elevating the risk of dementia was of low to moderate quality. In the case of
cognitive impairment, although there seemed to be higher likelihood of cognitive impairment with poor
periodontal status, results were less straightforward. All five studies with cognitive impairment as the
outcome were of low quality.
This review suggests that periodontitis is likely to increase the risk of dementia. However, the amount
and quality of evidence currently available is insufficient and of moderate to low quality to draw any
firm conclusions. Further studies with better study designs, longer study duration and more
comprehensive assessment of periodontitis and cognitive status are needed to elucidate the association
of periodontal health with cognition and dementia.

3
ABBREVIATIONS
Aβ: Amyloid beta
ABL: Alveolar bone loss/loss of alveolar bone
AD: Alzheimer’s disease
APOE: Apolipoprotein E
APP: Amyloid precursor protein
ARIC: The atherosclerosis risk in communities study
BBB: Blood brain barrier
BOP: Bleeding on probing
CAL: Clinical attachment loss/loss of clinical attachment
CPI: Community periodontal index
CPITN: Community periodontal index for treatment needs
CRP: Serum C-reactive protein
CSF: Cerebrospinal fluid
CVDs: Cardiovascular diseases
DLB: Dementia with Lewy bodies
DMFT: Decayed, missing, and filled teeth index
DSM: Diagnostic and statistical manual of mental disorders
DSS: Digit symbol substitution
DWR: Delayed word recall
FINGER: Finnish geriatric intervention study to prevent cognitive impairment and disability
GBI: Gingival bleeding index
GCF: Gingival crevicular fluid
GDS: Geriatric depression scale
HEPESE: Hispanic established populations for epidemiologic studies of the elderly
ICD: International statistical classification of diseases and related health problems
IL-6: Interleukin-6
LHID: Longitudinal health insurance database
LPS: Lipopolysaccharide
MAPT: Multi-domain Alzheimer preventive trial
MCI: Mild cognitive impairment or Cognitive impairment

4
MMI: Mild memory impairment
MMSE: Mini mental state examination
MRI: Magnetic resonance imaging
NHI: National health insurance - Taiwan
NHIRD: National health insurance research database of Taiwan
NSAIDs: Non-steroidal anti-inflammatory drugs
PAQUIDENT: Paquid dental study - France
PCI: Plaque control index
PDI: Periodontal disease index
PPDs: Periodontal pocket depths
PreDIVA: Prevention of dementia by intensive vascular care
PSP: Progressive supra-nuclear palsy
ROS: Reactive oxygen species
TBI: Traumatic brain injury
TNF- α: Tumor necrosis factor alpha
VaD: Vascular dementia
VCI: Vascular cognitive impairment
WF: Word fluency test.
WHO: World health organization
WMS-R: Wechsler memory scale – revised

5
TABLE OF CONTENTS
1. INTRODUCTION ................................................................................................................................ 8
2. LITERATURE REVIEW ..................................................................................................................... 9
2.1 PERIODONTITIS ............................................................................................................................... 9
2.1.1 Definition ...................................................................................................................................... 9
2.1.2 Prevalence ................................................................................................................................... 10
2.1.3 Types of Periodontitis ................................................................................................................. 10
2.1.4 Pathophysiology of Periodontitis ................................................................................................ 11
2.1.5 Diagnosis of Periodontitis ........................................................................................................... 16
2.1.6 Treatment of Periodontitis .......................................................................................................... 17
2.1.7 Risk factors for Periodontitis ...................................................................................................... 18
2.2 DEMENTIA AND COGNITIVE IMPAIRMENT ........................................................................... 22
2.2.1 Dementia ..................................................................................................................................... 22
2.2.2 Cognitive impairment ................................................................................................................. 27
2.2.3 Diagnostic criteria for Dementia and Cognitive impairment ...................................................... 28
2.2.4 Risk factors for Dementia and Cognitive impairment ................................................................ 31
2.2.5 Possible prevention strategies for Dementia and Cognitive impairment .................................... 39
3 AIMS AND METHODS ...................................................................................................................... 41
3.1 AIMS ................................................................................................................................................. 41
3.1.1 General Objective ....................................................................................................................... 41
3.1.2 Specific Objectives ..................................................................................................................... 42
3.1.3 Novelty compared to previous reviews ....................................................................................... 42
3.2 METHODOLOY .............................................................................................................................. 42
3.2.1 Inclusion criteria ......................................................................................................................... 43
3.2.2 Exclusion criteria ........................................................................................................................ 43
3.3.3 Quality assessment ...................................................................................................................... 44
4 RESULTS ............................................................................................................................................ 47
4.1 STUDIES WITH DEMENTIA AS THE OUTCOME ..................................................................... 49
4.1.1 Designs and settings .................................................................................................................... 49
4.1.2 Study population and duration .................................................................................................... 49
4.1.3 Periodontitis assessment ............................................................................................................. 50

6
4.1.4 Dementia assessment .................................................................................................................. 50
4.1.5 Periodontitis-Dementia association............................................................................................. 50
4.1.6 Quality assessment of studies assessing Dementia ..................................................................... 56
4.2 STUDIES WITH COGNITIVE IMPAIRMENT AS THE OUTCOME ......................................... 59
4.2.1 Design and settings ..................................................................................................................... 59
4.2.2 Study population and study duration .......................................................................................... 59
4.2.3 Periodontitis assessment ............................................................................................................. 60
4.2.4 Cognitive impairment assessment ............................................................................................... 60
4.2.5 Periodontitis-Cognitive impairment association ......................................................................... 61
4.2.6 Quality assessment of studies assessing Cognitive impairment ................................................. 68
5 DISCUSSION ..................................................................................................................................... 71
5.1 STUDIES ON PERIODONTITIS AND DEMENTIA ..................................................................... 71
5.1.1 Overall findings........................................................................................................................... 71
5.1.2 Measures of Periodontitis............................................................................................................ 71
5.1.3 Association between Periodontitis and Dementia based on periodontal pocket depths ............. 72
5.1.4 Association between Periodontitis and Dementia based on tooth loss ....................................... 72
5.1.5 Comparison between results based on different measures of Periodontal health ....................... 72
5.1.6 Severity of Periodontitis.............................................................................................................. 73
5.2 STUDIES ON PERIODONTITIS AND COGNITIVE IMPAIRMENT .......................................... 74
5.2.1 Overall findings........................................................................................................................... 74
5.2.2 Measures of Periodontitis............................................................................................................ 74
5.2.3 Association between Periodontitis and Cognitive impairment based on periodontal pocket
depths .............................................................................................................................................. 75
5.2.4 Association between Periodontitis and Cognitive impairment based on tooth loss ................... 75
5.2.5 Variability in Cognitive assessment ............................................................................................ 76
5.3 MECHANISMS ................................................................................................................................ 76
5.4 STRENGTHS AND LIMITATIONS .............................................................................................. 79
5.5 CONCLUSION AND FUTURE DIRECTIONS .............................................................................. 80
6. REFERENCES.................................................................................................................................... 82

7
LIST OF FIGURES AND TABLES
Figure 1: Search Results (Prisma flow diagram) ................................................................................... 48
Table 1: Community periodontal index (WHO 2005) ............................................................................ 17
Table 3: Risk and protective factors for Dementia and Cognitive impairment ...................................... 38
Table 4: MEDLINE search strategy PubMed July 2017 (run on date 18.07.2017) ................................ 43
Table 5: Studies assessing the association between Periodontitis and Dementia ................................... 52
Table 6: Quality assessment of the studies assessing Dementia ............................................................. 57
Table 7: Studies assessing the association between Periodontitis and Cognitive impairment ............... 63
Table 8: Quality assessment of studies assessing cognitive impairment ................................................ 69

8
1 INTRODUCTION
Periodontitis is the inflammation of tooth supporting tissues. In severe cases, deterioration of
periodontal tissues culminates into tooth loss (Silva et al. 2017). Chronic periodontitis is the most
common form of periodontitis affecting about one third of world population (Branco et al. 2015). It
arises as an inflammatory response mounted against sub-gingival plaque bacteria. Although it is
primarily an infectious pathology, dysregulated or hyperactive immune response plays a crucial role in
its development and progression (Suresh et al. 2017). The impact of periodontitis spreads beyond oral
health and is proposed to affect systemic health. It is regarded as an important determinant for systemic
conditions like diabetes, cardiovascular diseases and adverse pregnancy outcomes (Pitiphat et al. 2008,
Macedo Paizan & Vilela-Martin 2014, Lönn J et al. 2018).
Dementia is a syndrome characterized by progressive deterioration of cognitive function and functional
incapacitation. It is mainly prevalent in elderly individuals, with 5-7% of 60 years or older individuals
affected by it worldwide (LoGiudice & Watson 2014). Age and genetic predisposition are the major
risk factors for dementia (Kalantarian et al 2013). Furthermore, number of lifestyle and environmental
factors are proposed to be important determinants of dementia (Ylilauri et al. 2017). Dementia is
caused by a number of pathologies, with Alzheimer’s disease (AD) being the most common cause,
followed by vascular cognitive impairment (VCI) and dementia with Lewy bodies (DLB) (Tzeng et al.
2016).
Dementia pathology (mainly AD) may occur years before the first symptoms appear. Studies have
highlighted the role of periodontitis in the progression of dementia and cognitive deterioration (Dintica
et al. 2018, Gusman et al. 2018). However, more research is needed to establish its role as a risk factor
for dementia. A few studies have indicated that periodontitis increases the risk of dementia and
cognitive decline (Oh et al. 2018). Multiple mechanisms have been proposed, such as the inflammatory
model (Gallart-Palau et al. 2017). Tooth loss, a direct consequence of periodontitis, also independently
increases the risk of dementia and cognitive impairment (Nilsson et al. 2013).
With a significant rise in elderly population, prevalence of dementia alone is projected to surpass 100
million by 2050 (Koch & Jensen 2016). It is hence important to identify risk factors which can
contribute towards understanding the multifactorial etiology of the disease. In view of these notions,

9
the role of periodontitis as a modifiable risk factor for dementia and cognitive impairment needs to be
investigated.
2 LITERATURE REVIEW
2.1 PERIODONTITIS
2.1.1 Definition
Periodontitis is the inflammation of tooth supporting tissues that results in deterioration of periodontal
ligament and resorption of alveolar bone. It is characterized by gingival inflammation, formation of
periodontal pockets, clinical attachment loss and resorption of alveolar bone. Periodontal pockets form
as the widening of gingival sulcus due to gingival inflammation. Whereas clinical attachment loss
(CAL) is the term describing the apical migration of junctional epithelium, that forms the base of the
healthy gingival sulcus. As the inflammation spreads to the alveolar bone it causes its resorption that
may eventually culminate into tooth loss (Newnan et al. 2012).
Chronic periodontitis is the most common form of periodontitis that arises in response to sub gingival
plaque bacteria (Armitage 1999). Several plaque bacteria, predominantly gram-negative species such as
Porphyromonas gingivalis are associated with periodontitis (Hajishengallis 2012). Although
periodontitis is triggered by plaque bacteria, host immune response prompted against bacterial stimulus
plays a predominant role in determining the extent and severity of periodontal tissue breakdown
(Kinane & Marshall 2001).
Several factors such as poor oral hygiene, diabetes, medication and smoking significantly increases the
risk of periodontitis. Periodontitis is a slowly progressing chronic pathology, however, in the presence
of multiple predisposing factors, periodontal tissue breakdown undergoes frequent acute exacerbations
(Genco & Borgnakke 2013).
The clinical consequences of periodontitis spreads beyond its effects on oral cavity. In addition to
causing difficulty in mastication and speech, periodontitis adversely affects psychosocial wellbeing and
overall quality of life. Furthermore, it is suggested to be a risk factor for multiple systemic diseases

10
such as diabetes, cardiovascular diseases and adverse pregnancy outcomes (Gross et al. 2017). Chronic
periodontitis serves as a constant trigger for the expression of inflammatory mediators and is proposed
to increase the risk of many systemic diseases such as cardiovascular diseases (CVDs) and diabetes.
Furthermore, increasing evidence also suggest that periodontitis facilitate in the development of
neurodegenerative disorders such as dementia (Kamer et al. 2012, Kamer et al. 2015, Nilsson et al.
2017).
2.1.2 Prevalence
Periodontitis is the 6th most common chronic disease affecting about one third of world’s population. It
is mostly prevalent in adults (35 years or older) but is also observed in younger individuals (Silva et al.
2017). The prevalence of periodontitis has been reported to lie between 20-50% worldwide, however
most estimates are believed to underestimate the absolute numbers, with prevalence among the middle-
aged individuals (35-44 years old) alone estimated to be between 15-20% globally (WHO 2012). About
10-15% of world’s population is affected by severe periodontitis that often culminates into tooth loss if
left untreated (Ballini et al. 2015).
The prevalence of periodontitis increases with age. Severe periodontitis, in particular, is relatively more
prevalent among elderly individuals. Age-related factors such as increased prevalence of systemic
diseases, decreased effectiveness and frequency of oral health practices and propensity to have general
systemic inflammatory state is suggested to contribute to increased susceptibility of periodontitis
among the elderly. The prevalence of periodontitis has been on a rise, attributed to increase in
population and increased proportion of elderly. Furthermore, people are retaining more teeth well into
their old age that could explain for high prevalence of periodontitis (Kassebaum et al. 2017).
2.1.3 Types of Periodontitis
2.1.3.1 General classification of Periodontitis
Periodontitis is mainly classified into aggressive and chronic types, with each type further stratified
into localized and generalized subtypes. In addition to aggressive and chronic periodontitis other less
common types of periodontal diseases include periodontitis as a manifestation of systemic diseases,

11
necrotizing periodontal diseases, periodontitis associated with endodontic lesions and periodontal
disease as part of developmental or acquired deformity diseases (Armitage 1999).
Chronic periodontitis initiates as the inflammation of gingiva triggered by plaque bacteria, giving rise
to gingivitis. If left untreated or uncontained by the immune response mounted to deal with the
bacterial challenge, gingival inflammation spreads to periodontal ligament and alveolar bone resulting
in progression of gingivitis into periodontitis (Armitage 1999).
2.1.3.2 Classification of Chronic Periodontitis
Chronic periodontitis is divided into localized and generalized types which demonstrates the extent of
dentition affected by periodontal disease. This classification of chronic periodontitis is based on the
percentage of sites or teeth that exhibits clinical attachment loss and resorption of alveolar bone.
Diagnosis of localized periodontitis is assigned when less than 30% of teeth or sites displays clinical
attachment loss and alveolar bone resorption. Whereas general periodontitis indicates the involvement
of more than 30% of teeth or sites (Wiebe & Putnins 2000).
2.1.3.3 Mild, Moderate and Severe Periodontitis
Furthermore, periodontitis is also categorized as “mild periodontitis”, “moderate periodontitis”
and “severe or advanced periodontitis”, depicting severity of periodontitis. The severity of periodontitis
is ascertained by measuring amount of clinical attachment loss. Mild periodontitis presents with 1-2
mm of clinical attachment loss, while moderate periodontitis infers 3-4 mm of attachment loss. Clinical
attachment loss of 5 mm or beyond is referred to as severe periodontitis (Wiebe & Putnins 2000).
2.1.4 Pathophysiology of Periodontitis
2.1.4.1 Characteristics of Periodontitis
The classical features of periodontitis comprise of gingival inflammation, periodontal pocket
formation, clinical attachment loss and resorption of alveolar bone. Relatively less frequently
encountered features include gingival recession and tooth mobility, observed in severe periodontitis.
Gingival inflammation incurs a number of changes in the healthy gingiva including gingival swelling,
loss of gingival stippling and changes in color and contour of gingiva (Loesche & Grossman 2001).

12
On the spread of gingival inflammation, gingival sulcus increases in depth, eventually leading to
striping away of gingiva from the tooth surface. This marks the formation of periodontal pockets and
transition of gingivitis into periodontitis. Degree of periodontal pocket depth may be indicative of
severity of periodontal disease. However, such should be implied with caution as it underestimates the
disease in case of gingival recession where periodontal pockets remain shallow and overestimates in
cases where gingiva is extensively swollen (Loesche & Grossman 2001).
Clinical attachment loss assesses position of junctional epithelium against the tooth and is a measure of
extent of apical migration of junctional epithelium. It is a superior indicator of periodontal tissue
destruction in comparison to periodontal pocket depth and accounts for gingival changes such as
gingival recession or gingival overgrowth (Armitage & Cullinan 2010). Alveolar bone resorption is
another classical feature of periodontitis, which in severe cases is clinically manifested as loosening of
teeth. It may be clinically assessed during periodontal probing, however in majority of instances
radiographic assessment is undertaken for adequately determining the extent and pattern of bone loss
(Cochran 2008).
2.1.4.2 Etiology of Periodontitis
Dental Plaque
Periodontitis is an infectious disease caused by pathogenic bacteria in mature dental plaque. The
microbial biofilm called ‘dental plaque’ is the tenacious admixture of oral bacteria in a complex
extracellular matrix that forms on tooth surface. Hundreds of bacteria have been isolated from dental
plaque, majority of which are commensal in nature, having no pathological significance (Paster et al.
2001). However, multiple bacterial species predominantly the gram-negative types such as
Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola and Prevotella intermedia are
implicated as periodontal pathogens responsible for triggering the host immune response leading to the
development and establishment of periodontitis (Socransky et al. 1998). The extracellular component
of plaque is mainly derived from saliva and comprises of various organic and inorganic salivary
components (Peterson et al. 2014).
13
Dental plaque is classified as supra-gingival and sub-gingival plaque according to its position relative
to gingival margin. Supra-gingival plaque is part of dental plaque lying above the gingival margin
whereas part of dental plaque sheltered within gingival sulcus is referred to as sub-gingival plaque. It is
the sub-gingival plaque that holds key importance in pathogenesis of periodontitis. The overall
composition and pattern of sub-gingival plaque vary little from supra-gingival plaque. However, it is
more resolute, achieves maturation at a relatively faster pace and harbors more potent and greater
proportion of periodontal pathogens such as spirochetes. The formation and maturation of plaque is
driven by inter-microbial interaction, facilitated by presence of local and systemic factors. Furthermore,
host immune system is also suggested to play a significant part in establishing and sustaining the
dysbiosis that triggers the pathological process leading to periodontitis (Loesche & Grossman 2001).
Formation of plaque starts with the development of a layer of organic matrix called acquired pellicle
upon which successively various bacterial species colonize. The aerobic non-pathogenic bacteria are
the first to populate followed by virulent gram-negative anaerobic types (Darveau et al. 1997). The host
inflammatory response triggered by sub-gingival plaque clinically manifests as gingival inflammation.
The gingival inflammation leads to increase in size of gingival sulcus that allows further accumulation
of sub-gingival plaque. This subsequently produces an immune response of even larger magnitude
leading to progression of gingivitis towards periodontitis (Cekici at al. 2014).
Host immune response
The immune response in periodontitis is complex and involves both the innate and acquired segments
of immune system. However, there is no clear delineation between the effects of innate and acquired
immune system with both working in cooperation and overlapping the effects of each other. Although
periodontitis is triggered by plaque bacteria and can essentially be categorized as an infectious disease,
it is the host immune response that plays the chief role in the pathological process leading to
destruction of periodontal tissues (Wilensky et al. 2015).
This is supported by the finding that poor oral hygiene which is indicative of extensive accumulation of
plaque dominated by gram negative bacteria, does not always coincides with the development of
periodontitis (Meyle & Chapple 2015). On the other hand, susceptible individuals can develop severe
periodontitis even in the presence of plaque scarcely populated by periodontal pathogens, although the

14
classical periodontal pathogens are demonstrated in such individuals as well. Another important finding
advocating the more significant part of host immune system in periodontitis is the fact that although
several periodontal pathogens have been linked with periodontitis in general or with specific types of
periodontitis. No single pathogen has yet been found to be the sufficient cause of periodontitis
(Hajishengallis 2015).
It is proposed that in susceptible individuals, the host immune system is dysregulated that leads to a
hyperactive immune response against plaque bacteria. This hyperactive immune response leads to
extensive periodontal tissue breakdown, even if the microbial challenge is minimal (Khan et al. 2015).
The hallmark features of periodontitis, namely, periodontal pocket formation, clinical attachment loss
and resorption of alveolar bone are brought about by cytokines released by immune cells to counteract
microbial challenge (Shah et al. 2017). Furthermore, established risk factors for periodontitis such as
systemic comorbidities increase the risk of periodontitis by contributing to dysregulation of host
immune response (Zhu & Nikolajczyk 2014).
The inflammatory response in periodontitis is initially mounted as a physiological response to contain
the bacterial stimulus, which converts into a pathological chronic inflammation if the inflammation
fails to clear the constant stream of bacterial stimulation. After the recognition of bacteria or bacterial
products by innate immune system, chemokines and cytokines are expressed to recruit phagocytes.
Furthermore, the complement system is also triggered to contain the bacterial challenge (Cekici et al.
2014).
As the innate immune system is overwhelmed by the bacterial challenge it causes the activation of
acquired segment of immune system, bringing in other types of immune cells to counteract the
periodontal infection. The acquired immune system works side by side along with the already
functional innate immune system. In majority of the cases, there establishes an equilibrium between
constant bacterial stimulus and continuous counteractive immune response leading to establishment of
mild or moderate chronic periodontitis. However, in susceptible subjects the immune response is
dysregulated that leads to extensive destruction of periodontal tissues, which clinically manifests as
severe periodontitis (Cekici et al. 2014).

15
2.1.4.3 Development and Progression of Periodontitis
Periodontitis develops in a stepwise manner, progressing in severity as the host inflammatory response
becomes more potent. Initially only the gingiva is involved, clinically apparent as gingivitis. But as the
inflammation spreads it involves periodontal ligament and alveolar bone in pathological process,
resulting in eventual loss of clinical attachment and resorption of alveolar bone thus producing
periodontitis (Robinson 1995).
The initial lesion of periodontitis develops within 2 to 4 days of plaque accumulation, which is
clinically indistinguishable from healthy gingiva. The only discernible changes are at the histological
level, brought about by resident leukocytes and endothelial cells. There is migration of neutrophils to
the site of inflammation in response to cytokines released by junctional epithelium, accompanied with
increased flow of gingival crevicular fluid (GCF). On progression of initial lesion to early lesion,
gingival inflammation becomes clinically evident and is accompanied by further increase in GCF flow.
Histologically, there is increased proportion of neutrophils at the affected site, along with migration of
other types of leukocytes such as macrophages (Cekici et al. 2014).
If the microbial challenge is not cleared and further exacerbation of inflammatory response occurs,
early lesion progresses into established lesion, which presents clinically as chronic gingivitis of
moderate to severe intensity. At this stage gingival inflammation is well pronounced, with proliferation
of epithelium into underlying connective tissue. The cell infiltrate is now predominantly populated by
lymphocytes and plasma cells, with junctional epithelium beginning to detach from tooth surface at this
point (Cekici et al. 2014).
Any further damage to periodontium marks the formation of advanced lesion and transition of
gingivitis into periodontitis. The inflammatory response reaches its peak and leads to apical migration
of junctional epithelium clinically manifested as clinical attachment loss. Furthermore, the
inflammatory process involves tooth supporting alveolar bone leading to its resorption. The GFC is
predominantly concentrated by neutrophils, while underlying connective tissues are populated by
plasma cells (Cekici et al. 2014).

16
2.1.5 Diagnosis of Periodontitis
Diagnosis of periodontitis is based on clinical findings which includes periodontal pocket formation
(with or without gingival recession), bleeding on probing (BOP), clinical attachment loss and alveolar
bone loss. These clinical findings are calibrated to determine the extent of periodontal damage and are
usually supplemented with radiographic assessment which is valuable in determining the extent and
severity of periodontitis, as well as in delineating the pattern and extent of alveolar bone loss (Highfield
2009). These measures form the basis of diagnostic criteria highlighted in standard diagnostic manuals
such as International Statistical Classification of Diseases and Related Health Problems (ICD) (WHO
2016).
Clinical features are enough to ascertain the presence of periodontitis, but to conclusively highlight a
certain case, as of chronic periodontitis, clinical findings are assessed in context of age, presence of
sub-gingival plaque, local risk factors and pace of disease progression, along with medical and dental
history (Highfield 2009).
A number of indices of periodontal health such as Community Periodontal Index for Treatment Needs
(CPITN), Periodontal Disease Index (PDI) and Community Periodontal Index (CPI) among others are
used for screening and diagnosing periodontitis both at the clinical and epidemiological level (Beltrán-
Aguilar et al. 2012). Although different periodontal indices assess periodontal health based on above
mentioned measures of periodontitis. Not all measures are employed by each index and there exists
variation in the number and combination of measures used (Buenco et al. 2015). Most of these indices
do not only provide estimation of periodontal health but also provide an approximate estimate of
treatment that is needed to be administered (Dhingra & Vandana 2011).
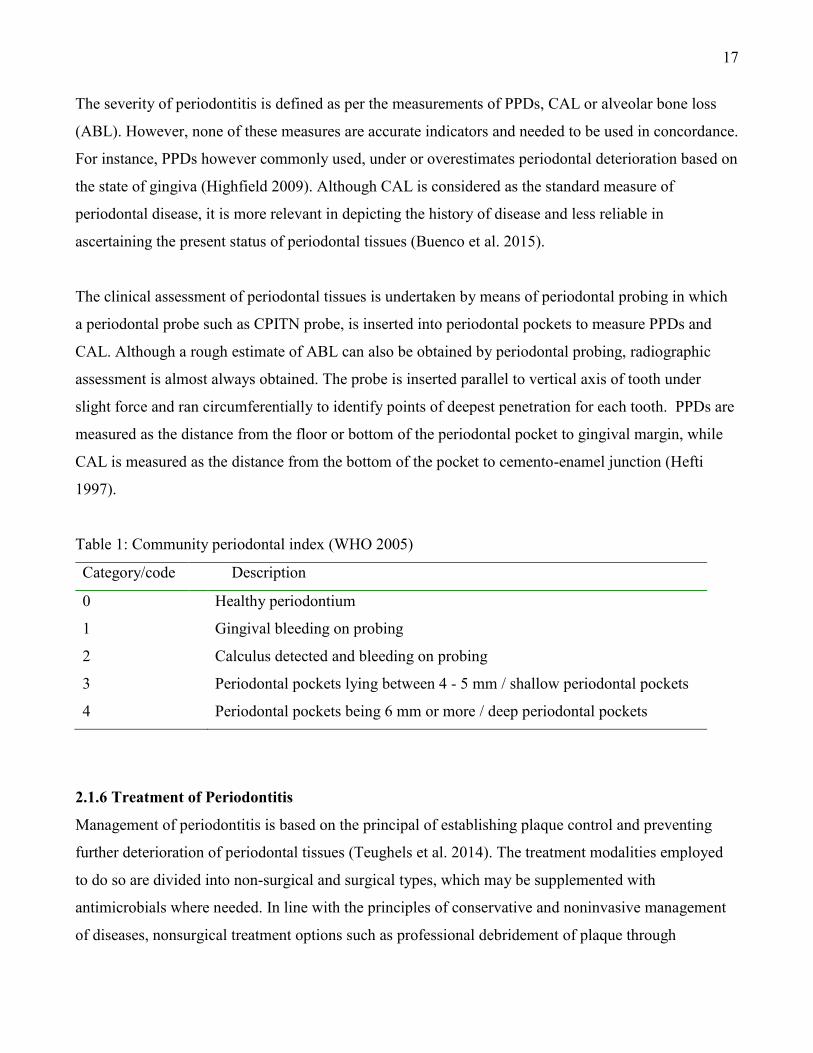
One of the most commonly used periodontal index is community periodontal index (CPI) which is a
modified version of community periodontal index of treatment needs. CPI assesses the periodontal
status through periodontal probing, clinical attachment loss, gingival bleeding and presence of calculus
(Table 1). Instead of screening the entire dentition CPI assesses only a limited number of teeth that are
found to be representative of entire dentition, thereby delivering a comprehensive assessment of
periodontal health in an efficient manner (Dhingra & Vandana 2011).
17
The severity of periodontitis is defined as per the measurements of PPDs, CAL or alveolar bone loss
(ABL). However, none of these measures are accurate indicators and needed to be used in concordance.
For instance, PPDs however commonly used, under or overestimates periodontal deterioration based on
the state of gingiva (Highfield 2009). Although CAL is considered as the standard measure of
periodontal disease, it is more relevant in depicting the history of disease and less reliable in
ascertaining the present status of periodontal tissues (Buenco et al. 2015).
The clinical assessment of periodontal tissues is undertaken by means of periodontal probing in which
a periodontal probe such as CPITN probe, is inserted into periodontal pockets to measure PPDs and
CAL. Although a rough estimate of ABL can also be obtained by periodontal probing, radiographic
assessment is almost always obtained. The probe is inserted parallel to vertical axis of tooth under
slight force and ran circumferentially to identify points of deepest penetration for each tooth. PPDs are
measured as the distance from the floor or bottom of the periodontal pocket to gingival margin, while
CAL is measured as the distance from the bottom of the pocket to cemento-enamel junction (Hefti
1997).
Table 1: Community periodontal index (WHO 2005)
Category/code Description
0
1
2
3
4
Healthy periodontium
Gingival bleeding on probing
Calculus detected and bleeding on probing
Periodontal pockets lying between 4 - 5 mm / shallow periodontal pockets
Periodontal pockets being 6 mm or more / deep periodontal pockets
2.1.6 Treatment of Periodontitis
Management of periodontitis is based on the principal of establishing plaque control and preventing
further deterioration of periodontal tissues (Teughels et al. 2014). The treatment modalities employed
to do so are divided into non-surgical and surgical types, which may be supplemented with
antimicrobials where needed. In line with the principles of conservative and noninvasive management
of diseases, nonsurgical treatment options such as professional debridement of plaque through

18
techniques such as scaling are first undertaken (Newman et al. 2012). Surgical treatment such as
gingivectomy is reserved for severe cases or undertaken in cases where extent of periodontal damage is
extensive or non-surgical measures have failed (Drisko 2014).
Any active manipulation of periodontium, whether surgical or non-surgical are delivered to remove
plaque and increase the effectiveness of oral hygiene practices undertaken thereafter (Gao et al. 2014).
Regardless of the treatment modality opted for, instituting oral hygiene measures and controlling for
risk factors forms an integral part of treatment plan (Genco & Borgnakke 2013).
2.1.7 Risk factors for Periodontitis
Multiple local, systemic and lifestyle factors increase the risk of periodontitis. Several mechanisms
have been proposed by which various factors individually or synergistically impart elevated risk of
periodontitis. The main pathway by which most of the established risk factors predisposes to
periodontitis is dysregulation of immune response (Jain & Mulay 2014, Hong M et al. 2016).
Furthermore, multiple factors also assist in the development of periodontitis by facilitating maturation n
of plaque and establishment of dysbiosis (Loesche & Grossman 2001, Albandar 2002).
Majority of the risk factors for periodontitis are modifiable in nature that render periodontitis to
preventive regimens. Furthermore, non-modifiable factors such as age and gender are also suggested to
increase the risk of periodontitis through indirect pathways that can also be explored as targets for
preventive strategies (Genco & Borgnakke 2013, Persson 2017).
2.1.7.1 Non-modifiable factor
Age
The prevalence and severity of periodontitis increases with age. The prevalence of severe periodontitis
is 15% higher among the elderly individuals as compared to general population (Khocht et al. 2010).
This is evident by the association between CAL and increasing age, with increase in CAL being
consistent with advancing age. Apart of this increase in CAL is down to gingival recession which itself
is an indicative of progressing periodontal deterioration (Billings et al. 2018).

19
The exact mechanism by which advancing age predisposes to periodontitis is not known. However,
ageing is not considered to be a direct contributor to the development of periodontitis. This is supported
by lack of association between age-related changes in periodontium, such as higher fibrotic content or
decrease vascularity of periodontium, and risk of periodontitis. Ageing is proposed to elevate the risk
of periodontitis through age-related factors such as presence of systemic diseases, malnutrition,
decreased dexterity and decreased frequency of regular dental visits (Persson 2017).
Gender
Men are 50% more likely to have periodontitis as compared to women. Moreover, risk of severe
periodontitis among men is three times to that for women. The exact mechanism by which men are
more prone to periodontitis is still poorly understood. It is proposed that higher prevalence of lifestyle
and behavioral risk factors such as poor oral hygiene and smoking among men is mainly responsible
for the difference in risk of periodontitis between genders (Genco & Borgnakke 2013).
2.1.7.2 Modifiable factors
Systemic factors
Systemic risk factors such as diabetes, obesity and use of medication for systemic diseases increase the
risk of periodontitis. The exact mechanism by which individual systemic diseases contribute to the
development of periodontitis is still poorly understood. However, it is suggested that systemic risk
factors facilitate in the development of periodontitis by impairing metabolic control and causing
dysregulation of immune response (Casanova et al 2014). The alterations caused by systemic factors in
the immune system varies from mounting a deficient immune response against bacterial stimulus to the
development of hyperactive inflammatory response (Silva et al. 2015).
Diabetes
Most widely accepted systemic risk factor for periodontitis is diabetes. The prevalence of periodontitis
among individuals with diabetes is three times to that of general population. Moreover, individuals with
diabetes are also more likely to develop severe periodontitis and undergo rampant destruction of
periodontium (Preshaw et al. 2012). The impact of diabetes on periodontium is so pronounced that it is
regarded as one of the complications of diabetes. Diabetes is proposed to establish a general

20
inflammatory state that contributes in the dysregulation of immune response mounted against plaque
bacteria (Chapple et al. 2013).
Obesity and metabolic syndrome
Several studies indicate increased risk of periodontitis as a function of obesity and metabolic syndrome.
Increasing evidence indicates that obesity do not only increase susceptibility to developing
periodontitis, but obese individuals also demonstrate greater loss of clinical attachment as compared to
controls. The mechanism by which obesity facilitates in the development of periodontitis is still under
study. However, it is suggested that obesity predisposes to periodontitis partly by modulating the
immune response and facilitating in the establishment of dysbiosis (Genco & Borgnakke 2013).
Metabolic syndrome is also proposed to be an independent risk factor for periodontitis. Indeed,
individual metabolic changes such as hypertension, dyslipidemia and insulin resistance are all found to
increase the risk of periodontitis. These metabolic disturbances are suggested to facilitate in the
development of periodontitis by impairment of immune response and contributing to systemic
inflammation (Reynolds 2014).
Osteoporosis, low dietary calcium and vitamin D deficiency
Osteoporosis is another systemic factor that has been shown to increase the risk of periodontitis. Many
studies have demonstrated that systemic osteoporosis also effects the jaw bones and thereby contributes
to tooth loss. Furthermore, it is suggested that osteoporosis facilitates tooth loss indirectly by increasing
the likelihood of developing periodontitis. However, the exact nature and magnitude of the effect of
osteoporosis on periodontitis remains unclear (Martínez-Maestre et al. 2010).
In addition to osteoporosis, low dietary intake of calcium and vitamin D deficiency have also been
found to increase the risk of periodontitis and tooth loss. Calcium deficiency is also found to impact the
severity of periodontitis. The exact mechanism by which either of these deficient states contribute to
periodontitis are still poorly understood. However, impairment of bone metabolism is cited as one of
the possible pathways by which calcium and vitamin D deficiency adversely impacts periodontal health
(Nishida et al. 2000).

21
Medication
Different classes of medicines such as antihypertensive drugs, narcotic analgesics and antihistamines
are associated with increased risk of periodontitis. Multiple mechanisms have been proposed by which
different medicine impart increased risk of periodontitis. Among the most commonly observed oral
effect of systemic medicines is decreased salivary flow (Al-Jehani 2014). Saliva is the primary
defensive mechanism by which host resist and maintain the bacterial stimulus from dental plaque to a
minimum. Decrease in the composition or volume of saliva significantly impairs plaque control and
increases the risk of periodontitis (Mariotti & Hefti 2015). Another important class of drugs that
increase the risk of periodontitis is calcium channel blockers. Calcium channel blockers are associated
with gingival overgrowth which hinders plaque control by sheltering plaque in resultant pseudo
periodontal pockets. This allows for the maturation of plaque that subsequently increase the risk of
periodontitis (Scully 2003).
Life style factors
Poor oral hygiene
Lack of adequate oral hygiene measures facilitates deposition and maturation of plaque that triggers
chronic inflammatory pathology of periodontitis (Albandar 2002). Local retentive factors such as mal-
aligned teeth and ill-fitting restorations further contribute to increased risk of periodontitis by
facilitating plaque retention and making oral hygiene measures ineffective (Loesche &Grossman 2001).
Smoking
Smoking is regarded as the single most important preventable risk factor for periodontitis. The
prevalence of periodontitis among smokers is almost twice to that of non-smokers. Smoking do not
only contribute to the development and progression of periodontitis but is also a strong determinant of
severity of periodontitis (Nociti et al. 2015). The exact mechanism by which smoking increases the risk
of periodontitis is still not clearly understood. However, smoking is suggested to cause changes in
immune system such as decreased production of immunoglobulins and increased expression of reactive
oxygen species (ROS), that increases periodontal tissue destruction (Johannsen et al. 2014).

22
Alcohol intake
Many studies indicate negative effect of alcohol intake on periodontal health. However, effect of
alcohol intake varies between genders and amount of alcohol consumed. Alcohol intake have been
found to cause more detrimental effects on periodontal health in men as compared to women. Moderate
alcohol intake has been found to cause little to no adverse effect on periodontal health, however,
excessive consumption of alcohol significantly increases risk of periodontitis (Kongstad et al. 2008).
Alcohol intake is proposed to impact periodontal health by alteration of plaque composition towards a
more pathogenic type and increased expression of pro-inflammatory cytokines (Suwama et al 2018).
Psychological Stress and Depression
In addition to its negative effects on general health, stress is a significant determinant of periodontal
health. It has been found to incur a number of physiological changes that may directly or indirectly
contribute to increased risk of periodontitis. One such change is decreased salivary flow that aids in
dysbiosis and subsequent development of periodontitis (Reners & Brecx 2007). Furthermore, stress has
also been found to reduce the effectiveness of periodontal treatment (Bakri et al. 2013).
Another important factor that increases the susceptibility of developing periodontitis is depression. The
exact mechanism by which depression contributes to the development of periodontitis is yet poorly
understood. However, evidence suggests that depression significantly impairs immune response and
adversely effects wound healing that can directly contribute to the development of periodontitis.
Furthermore, depression is also likely to negatively affect lifestyle habits thereby indirectly
predisposing to periodontitis (Reynolds 2014).
2.2 DEMENTIA AND COGNITIVE IMPAIRMENT
2.2.1 Dementia
2.2.1.1 Definition and prevalence
Dementia is a syndrome characterized by progressive deterioration of cognitive function. Extent of
cognitive deterioration observed in dementia is well beyond age-related cognitive decline and is
essentially accompanied by functional incapacitation or functional dependence which leaves

23
individuals dependent on caregivers for carrying out day to day activities. It is highly prevalent among
the elderly, with 5-7% of 60 years old or older individuals affected by it worldwide. Old age is the most
significant predisposing factor for dementia, with prevalence of dementia reported between 20-50%
among 85 years or older individuals (Slavin et al. 2013, WHO 2017).
The effects of dementia extend beyond the affected individual, with significant social and
psychological burden experienced by caregivers and family members. Several factors such as chronic
systemic diseases including CVDs, are implicated as risk factors of dementia. Many extensively
studied risk factors are non-modifiable in nature, however increasingly greater number of studies are
now being carried out with focus on modifiable risk factors (LoGiudice & Watson 2014).
Cognition is the mental ability or function to acquire, process, utilize and implement information or
knowledge. Cognition is not a single process but is a constellation of multiple domains such as
memory, thinking, orientation, language and judgement among others. All or several of these are
usually involved at the same time in the processing of each piece of information (Woodford & George
2007).
Dementia affects multiple cognitive domains, although the pattern, number of cognitive domains
affected, and the extent of deterioration depends on underlying pathology (LoGiudice & Watson 2014).
For instance, memory is most commonly and extensively affected cognitive domain in Alzheimer’s
disease (Aggarwal et al 2015), while executive function is most commonly compromised in vascular
dementia (Ying et al. 2016). In addition to functional dependence, cognitive deterioration is often
accompanied with or preceded by behavioral and psychiatric symptoms such as agitation, anxiety,
depression, delusions, hallucinations, sleep and appetite disturbances (Cerejeira et al. 2012).
Around 50 million people are affected by dementia worldwide, with around 8-10 million new cases
encountered on yearly basis. These numbers are projected to increase significantly in the next few
decades owing to the increase in the number of elderly individuals worldwide. According to one
estimate, prevalence of dementia is projected to surpass 150 million by 2050 (WHO 2017). Owing to
the personal, societal and socioeconomic cost, dementia stands out among the foremost healthcare
challenges of present time. Additionally, lack of availability of effective treatment, strongly advocates

24
studies into determining the modifiable risk factors and subsequent development of preventive
strategies (Koch & Jensen 2016).
2.2.1.2 Types of Dementia
A number of pathologies are implicated in the development of dementia. Most of these underlying
pathologies either belong to the neurodegenerative or cerebrovascular class of diseases. However, other
conditions such as HIV infection, thyroid diseases and normal pressure hydrocephalus are implicated as
the etiological factor leading to the development of dementia (WHO 2012).
The underlying disease that contributes to the development of dementia forms the basis of classification
of dementia into its subtypes. In many cases a single underlying disease is clearly delineated. However,
in others more than one disease occurs simultaneously. Even in cases where a single underlying cause
is identifiable, there may lie significant variability in its presentation. Furthermore, signs and symptoms
between different types often overlap (LoGiudice & Watson 2014).
Alzheimer’s disease is the most prevalent type of dementia, with 60-70% of individuals having AD.
AD is followed by vascular dementia (VaD) and dementia with Lewy bodies with each contributing
between 10-20% of dementia cases (Tripathi et al. 2014). Other less common types of dementia include
frontotemporal dementia, dementia due to Parkinson's disease, Creutzfeldt-Jakob disease and
Huntington’s disease (Reith & Mühl-Benninghaus 2015) (Table 2).
Alzheimer’s disease
Alzheimer's disease is clinically characterized by deterioration of multiple cognitive domains, of which
memory is most extensively compromised. Pathological findings include intracellular accumulation of
tau protein in the form of neurofibrillary tangles and extracellular deposits of amyloid protein (Shanthi
et al. 2015). The exact mechanism that leads to its development is still not clearly understood.
However, neuroinflammation and oxidative stress are suggested to be important pathological processes
in regard to the development of AD (Gurav 2014).
Vascular dementia

25
Vascular dementia is characterized by the presence of cerebrovascular lesions. It is further stratified
into subtypes such as multi-infarct dementia, single infarct dementia and subcortical dementia among
others (Benisty 2013, Lam et al. 2014). VaD often develops in individuals with a history of ischemic
stroke, which is proposed to cause progressive cognitive deterioration if experienced repeatedly.
Executive dysfunction and psychomotor slowing are usually the most pronounced cognitive changes in
VaD (Iadecola 2013).
Dementia with Lewy bodies
Dementia with Lewy bodies (DLB) is characterized by the presence of abnormal protein inclusions of
α-synuclein within neurons. Other neuropathological changes seen in DLB includes deterioration of
tegmental dopamine cell population and basal forebrain cholinergic population. Along with general
deficit in cognitive domains, DLB presents with hallucinations, impairment of executive function and
visuospatial dysfunction (Gomperts 2016).
Mixed dementia
Mixed dementia is a term reserved for cases of dementia where more than one underlying pathology is
suspected to be present. In cases of mixed dementia, a dominant type of pathology can be identified.
However, there can also be extensive overlapping of clinical characteristics, making the exact
determination of contributory pathological processes difficult. Most commonly observed combinations
in mixed dementia are of AD and VaD or AD with DLB (Bhogal et al. 2013).
26
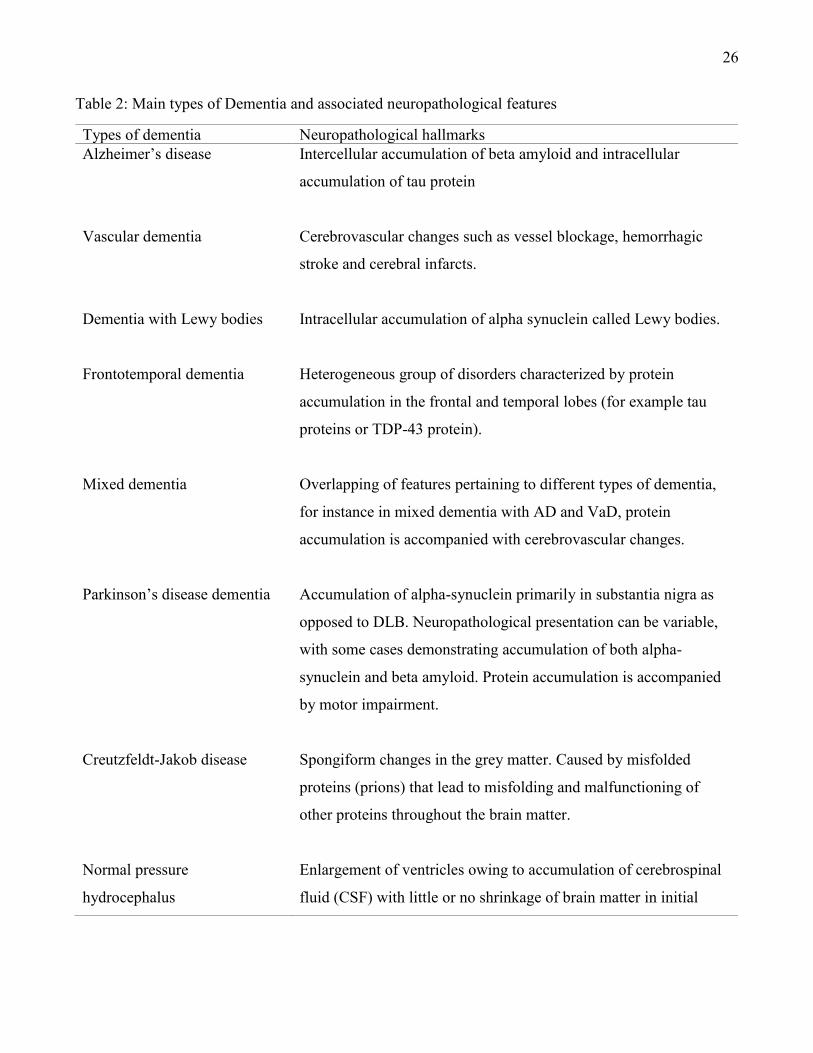
Table 2: Main types of Dementia and associated neuropathological features
Types of dementia Neuropathological hallmarks
Alzheimer’s disease
Vascular dementia
Dementia with Lewy bodies
Frontotemporal dementia
Mixed dementia
Parkinson’s disease dementia
Creutzfeldt-Jakob disease
Normal pressure
hydrocephalus
Intercellular accumulation of beta amyloid and intracellular
accumulation of tau protein
Cerebrovascular changes such as vessel blockage, hemorrhagic
stroke and cerebral infarcts.
Intracellular accumulation of alpha synuclein called Lewy bodies.
Heterogeneous group of disorders characterized by protein
accumulation in the frontal and temporal lobes (for example tau
proteins or TDP-43 protein).
Overlapping of features pertaining to different types of dementia,
for instance in mixed dementia with AD and VaD, protein
accumulation is accompanied with cerebrovascular changes.
Accumulation of alpha-synuclein primarily in substantia nigra as
opposed to DLB. Neuropathological presentation can be variable,
with some cases demonstrating accumulation of both alpha-
synuclein and beta amyloid. Protein accumulation is accompanied
by motor impairment.
Spongiform changes in the grey matter. Caused by misfolded
proteins (prions) that lead to misfolding and malfunctioning of
other proteins throughout the brain matter.
Enlargement of ventricles owing to accumulation of cerebrospinal
fluid (CSF) with little or no shrinkage of brain matter in initial

27
stages, enabling it to be distinguished from other types of
dementia.
2.2.2 Cognitive impairment
2.2.2.1 Definition and prevalence
Mild Cognitive Impairment (MCI) is defined as a pathological deterioration of cognitive function that
does not meet the criteria for dementia or is not severe enough to be categorized as dementia. As per
the definition, MCI has long been labelled as the prodromal phase of dementia or the intermediate state
between healthy cognition and dementia. One of the significant differences between MCI and dementia
is that functional capacity or functional independence is essentially preserved in MCI. There is a
significantly greater risk of developing dementia among the individuals with MCI. The broad definition
of MCI highlights the incomplete understanding of this pathology, which make its diagnosis and
management difficult and prone to subjectivity (Langa & Levine 2014).
It is estimated that the prevalence of MCI is four times to that of dementia with prevalence values
ranging between 3-42%. In general, rough estimates put the overall prevalence of MCI between 16-
20% among the 65 years or older individuals which increases dramatically in subsequent decades
(Roberts & Knopman 2013). Multiple factors such as systemic diseases and sedentary life style
increase the risk of developing MCI (Eshkoor et al. 2015). The underlying etiology of MCI and the
exact mechanisms that leads to its development are still poorly understood. Neurodegenerative diseases
are proposed to be a primary cause of MCI (Aggarwal 2007). The diagnosis of MCI is based on clinical
finding of cognitive impairment in one or more cognitive domains based on cognitive tests such as
Mini mental scale examination (MMSE) or other standardized tests (Knopman et al. 2009).
Individuals with MCI carry a significantly higher risk of developing dementia, with 1 out of every 5
individuals with MCI developing dementia. Conversion rate of specific types of MCI differ
significantly and there appears a pattern of higher conversion risk of certain types of MCI into specific
forms of dementia, such as conversion of amnestic MCI into AD (Knopman & Petersen 2014). The
exact mechanism and the risk factors that leads to the conversion of MCI into dementia is yet not

28
delineated. Despite significantly higher risk of developing dementia, some cases of MCI revert to
normal cognitive state, while others may stabilize with limited or no discernible progression (Roberts et
al. 2012). The factors that causes a specific group of individuals with MCI to develop dementia, while
others are preserved are still under investigation (Trzepacz et al. 2014).
MCI not only increases the risk of dementia, but it also significantly impairs general quality of life
(Knopman & Petersen 2014). This in addition to increased proportion of ageing population, personal
and socioeconomic cost of its management makes it a major healthcare challenge (Eshkoor et al 2014).
2.2.2.2 Types of Mild cognitive impairment (MCI)
MCI is broadly classified into two types, amnestic and non-amnestic. This categorization is based on
the cognitive domains most prominently affected by the neurodegenerative process. Amnestic MCI is
the cognitive impairment in which memory is greatly impaired, while other cognitive domains are
either subtly involved or are persevered. Non-amnestic MCI refers to cognitive impairment involving
deterioration of non-amnestic cognitive domains such as executive functioning, language and so forth.
The two basic types are further classified into single and multiple domain subtypes. In single domain
subtypes only one cognitive domain is affected, while cases of multiple domain subtypes involve more
than one cognitive domain (Petersen 2011).
The prevalence of amnestic MCI is almost twice to that of non-amnestic types. Amnestic MCI carries a
higher risk of conversion into AD as compared to any other type of dementia. Similarly, individuals
with non-amnestic types of MCI are at greater risk of developing types of dementia other than AD.
There is also increasing evidence suggesting that multi-domain MCI subtypes are more likely to
progress into dementia as compared to single domain MCI subtypes (Petersen RC et al. 2010). Another
important difference between the amnestic and non-amnestic MCI, is higher prevalence of behavioral
changes in non-amnestic MCI (Mortimer et al. 2013).
2.2.3 Diagnostic criteria for Dementia and Mild Cognitive Impairment
The diagnosis of dementia and MCI is complex and based primarily on the clinical findings of
cognitive impairment and its effects on functional independence. These two attributes form the core of
the diagnostic criteria defined in standard diagnostic manuals such as Diagnostic and Statistical Manual

29
of Mental Disorders (DSM) and International Statistical Classification of Diseases and Related Health
Problems (ICD) among others (American Psychiatric Association 2013). The general criteria for
dementia and cognitive impairment in either DSM or ICD are similar. However, subtle differences
pertaining to behavioral changes and involved cognitive domains that delineate between subtypes do
impact the prevalence values and breakdown of different types (Wancata et al. 2007).
Findings from medical examination are supplemented with neuropsychological assessment, which
provides a measure of the type and extent of the impairment. The neuropsychological assessment uses a
battery of cognitive tests such as Mini-Mental State Examination (MMSE) or other more complex tests.
Neuroimaging is also used which is helpful in identifying and quantifying pathological changes in the
brain (Echavarri et al. 2012). More recent diagnostic criteria for research also take into account
cerebrospinal fluid (CSF) biomarkers such as tau and β-amyloid proteins.
The diagnostic criteria for neurodegenerative disorders have evolved over time and are likely to
undergo further refinement as the mechanisms leading to their development become clearer. There
have been significant differences in the diagnostic criteria of dementia and MCI in DSM-5 as compared
to previous versions. The term “dementia” was removed from DSM-5, and the heading of Delirium,
Dementia, and Amnestic and Other Cognitive Disorders was replaced with Neurocognitive Disorders.
The category of Major Neurocognitive Disorder was introduced, corresponding to the previous
Dementia category as given in older versions of DSM (American Psychiatric Association 2013).
Furthermore, a new category of Mild Neurocognitive Disorder was introduced that corresponds with
the definition and presentation of MCI. No specific criteria for MCI had been listed in previous DSM
versions.
The diagnostic criteria for Major Neurocognitive Disorder are based on 2 major clinical findings.
Firstly, the subject should demonstrate cognitive deterioration of pathological nature in any cognitive
domain, and secondly, cognitive deterioration needs to be severe enough to impair individual’s ability
to carry out day to day tasks (Sachdev et al. 2014). The updated criteria in DSM-5 for dementia are
different from earlier versions where deterioration of memory held key importance and required
demonstration of deterioration of multiple cognitive domains for a formal diagnosis of dementia to be
made. Although classical features of cognitive impairment and functional incapacitation are

30
demonstrated by all forms of dementia to varying degree, specific types of dementia are delineated on
the basis of neuropathological findings inherent to each type (Hugo & Ganguli 2014).
The introduction in DSM-5 of more specific criteria for Mild Neurocognitive Disorder acknowledges
the fact that more and more old individuals with cognitive decline seek medical care early, before they
develop dementia. One important purpose of emphasizing MCI as a separate diagnosis has been to
facilitate early diagnosis and treatment of the underlying disease, before it progresses to the more
severe stage of dementia. In addition, it also acknowledges the fact that MCI may not always be
progressive in nature. The diagnostic principle is similar to Major Neurocognitive Disorder or dementia
except that in MCI, cognitive impairment is not severe enough to affect individual’s ability to carry out
day to day task (Sachdev et al. 2015).
In addition to subjective assessment of cognition, neuropsychological assessment using standardized
tests is recommended in DSM-5. The battery of cognitive tests not only aids in screening the
individuals with cognitive deficits but also enables to calibrate degree of cognitive deficit that in turn
facilitates in differentiating between MCI and dementia. Although DSM-5 does not specify exactly
which battery of cognitive tests should be used, it provides some guidelines regarding the degree of
cognitive deterioration likely to be experienced in major and mild neurocognitive disorders.
Neuropsychological assessment falling between 1 to 2 standard deviation of normative mean is
suggested to indicate mild neurocognitive disorder, while for major neurocognitive disorder the value
lies 2 or more standard deviation below normative mean (Sachdev et al. 2015).
In general, for evaluation of cognitive function and assessing orientation, immediate memory,
language, calculation, short-term recall and attention, MMSE is the most widely used test. Score ranges
from 0 to 30, with a score of 24 or below suggesting dementia, although a threshold for MCI has not
been universally established (Tombaugh & McIntyre 1992, Lancu and Olmer 2006). Additionally,
other than MMSE, a range of more detailed and sensitive neuropsychological test batteries are
available. Majority of these tests assess multiple cognitive domains; however, a number of cognitive
tests also evaluate specific cognitive domains that help in distinguishing between different types of
cognitive impairment. For instance, Wechsler memory scale –Revised (WMS-R) is used for assessment

31
of memory, whereas Boston naming test is employed for assessing language and executive function can
be specifically assessed through digit symbol substitution test (Stokin et al. 2015).
2.2.4 Risk factors for Dementia and Mild cognitive impairment
Dementia and MCI are regarded as multifactorial conditions. Many demographic, systemic and life
style factors are implicated for contributing to the overall risk of dementia and MCI. Many of these
factors often occur and interact across the entire life span and are through various pathways proposed to
result in cognitive deterioration. While some of these risk factors such as age and family history are
non-modifiable, many modifiable risk factors such as diabetes, CVDs and various lifestyle factors have
been identified (Table 3). Owing to the debilitating nature of these pathologies and lack of availability
of effective treatment, modifiable factors are a subject of several epidemiological studies looking into
the preventive strategies for dementia and MCI (Sindi et al. 2015).
2.2.4.1 Non-modifiable risk factors
Demographic factors
Demographic factors such as age and gender significantly increase the risk of dementia and cognitive
impairment.
Age
Age is regarded as the strongest risk factor for either condition with majority of the cases occurring in
6th decade of life or thereafter (Kalantarian et al 2013). The incidence of dementia increases
dramatically with age, doubling in less than 6 years. Indeed 70% of all dementia cases occur in 75
years or older individuals (Fratiglioni et al. 2000). The incidence of dementia is found to increase from
just 3.1 cases per 1000 among the 60-64 years old age group to 175.0 cases per 1000 among the 95
years or older age group (WHO 2012). The same pattern seems to be followed by MCI. Although the
incidence values for MCI varies from 5.1 to 168 per 1000 persons, as in the case of dementia, incidence
of MCI tends to increase with advancing age (Roberts & Knopman 2013).
Gender

32
Gender is also found to independently influence the risk of dementia and MCI. Women are found to be
at a greater risk of dementia, with factors such as higher life expectancy and hormonal changes after
menopause being suggested as possible explanations (Rocca et al. 2014). Contrary to dementia several
studies have reported greater risk of MCI in men, with men being twice more likely to have MCI than
women. Higher prevalence of systemic diseases and relatively less healthy life style such as increased
alcohol consumption and smoking among men as compared to women have been suggested as potential
causes of increased risk of MCI among men (Roberts et al 2012). However, more studies are needed to
conclusively determine the role of gender differences in the risk of cognitive impairment.
Genetic factors
Genetic factors such as familial aggregation and different individual genes are found to increase the
risk of dementia and MCI. Studies have reported 25 to 50% increase in risk of dementia among
individuals with family history of dementia (Milne et al. 2008), while the risk of cognitive impairment
also substantially increases in individuals with family history (Locke et al. 2009). Furthermore, the
degree of cognitive deterioration may be more pronounced in cases with familial aggregation
(Scarabino et al. 2016).
Several different genes are implicated in increasing the risk of developing dementia. This is particularly
true for AD, in which presence of ε4 allele of Apolipoprotein E (ApoE ε4) is regarded as an established
risk factor, with at least 15-20% of all cases of dementia attributed to it. Moreover, ApoE ε4 is found to
decrease the age of dementia onset and also adversely affect its responsiveness to interventions (Teruel
et al. 2011).
2.2.4.2 Modifiable risk factors
Cardiovascular and metabolic risk factors
Systemic factors such as cardiovascular and metabolic diseases, significantly add to the risk of
dementia and MCI. Although multiple mechanisms have been postulated to explain for the effect of
systemic diseases on cognition, the exact mechanisms by which systemic diseases contribute to the
development of cognitive deterioration are not fully clarified. Regardless of the systemic risk factor

33
involved, increasing evidence suggests that significant reduction in the risk of cognitive deterioration
may be possible through the management of systemic diseases (Baumgart et al. 2015).
Cardiovascular diseases
A wide range of cardiovascular pathologies such as atrial fibrillation, thrombotic events, heart failure
and hypertension increase the risk of dementia and cognitive impairment (Da la Torre 2012, Wand et
al. 2015). A number of possible mechanisms such as cerebral hypo-perfusion and cerebral infarction
among others are cited as leading to subsequent cognitive deterioration (Etgen et al. 2011).
Additionally, the time frame during which cardiovascular risk factors develop, appears to be important
for the risk of late-life cognitive deterioration. Risk factors such as hypertension in midlife seem to be
consistently associated with increased risk of dementia and cognitive impairment later on. Studies on
hypertension at older ages have reported conflicting results. However, further studies are required to
conclusively determine the magnitude and time span of effects of CVDs on cognition (Corrada et al.
2017).
Diabetes
Diabetes is another important condition that independently elevates the risk of dementia and MCI. This
is particularly true for vascular dementia with studies reporting up to 60% increased risk of vascular
dementia in people with diabetes. Furthermore, diabetes is also found to increase the risk of
progression of MCI to dementia (Chatterjee et al. 2016). It is suggested that cerebrovascular
disturbances produced by diabetes explain the increased risk of cognitive decline and dementia.
Additionally, impairment of metabolic control is also suggested to contribute towards the adverse
effects of diabetes on cognition (Hardigan et al. 2016).
Diabetes also demonstrates an association with AD. Individuals with diabetes carry significantly
greater risk of developing AD, with studies indicating a link between diabetes and accumulation of
amyloid (Chung et al. 2018). Multiple mechanisms such as impairment of insulin signaling, oxidative
stress and mitochondrial dysfunction are attributed to the impact of diabetes on elevating the risk of
AD. However, further studies are required to clearly elucidate the exact mechanisms (Yang & Song
2013).

34
Obesity and metabolic syndrome
Obesity and metabolic syndrome have been reported as significant risk factors for dementia and
cognitive impairment (Miller & Spencer 2014, Rizzi et al. 2014, Tynkkyen et al. 2016, Ylilauri et al.
2017). The effect of obesity on the risk of dementia appears to be age-dependent. Obesity in midlife
significantly elevates the risk of cognitive deterioration, but like hypertension its contribution to the
development of cognitive deterioration is less clear at older ages (Singh-Manoux et al. 2018).
A decline in body mass index has been reported to occur over time in people who develop dementia
later on. This may explain why some studies have reported contradictory findings, indicating that
higher body mass index at older ages may be protective against dementia (Qizilbash et al. 2015).
Further studies are still needed to determine the exact nature and magnitude of the effect that obesity
has on cognitive deterioration.
Metabolic syndrome is also suggested to elevate the risk of cognitive deterioration. Indeed, different
constituent pathological disturbances seen in metabolic syndrome, such as dyslipidemia, are found to
be risk factors for cognitive deterioration (Liu et al. 2015, Salameh et al. 2016).
The biological mechanisms behind the impact of obesity and metabolic syndrome on dementia risk are
still poorly understood. They are suggested to increase the risk of cognitive deterioration through their
effects on general health. Obesity and subsequent increased adiposity increase the risk of developing
other systemic pathologies, that are in turn are established risk factors for cognitive deterioration
(Gustafson 2006). Furthermore, obesity is also found to be associated with brain atrophy (Ho e al.
2010).
Lifestyle, psychological and other risk factors
Early life adversities
Factors indicative of early life adversities such as low education and poor socioeconomic status and
related factors significantly increase the risk of dementia and cognitive impairment. Both poor
socioeconomic status and low education can affect lifestyle, access to health care services and
awareness regarding diseases and corresponding adoption of preventive measures, thereby contributing
to an individual’s risk of multiple pathologies including dementia (McDowell et al. 2007).

35
The exact pathological mechanisms by which early life adversities contribute to the development of
cognitive deterioration are not fully known. However, they are believed to affect brain development
and compromise attainment of cognitive reserve that in turn decreases the resistance against
neuropathological changes leading to the development of cognitive deterioration (Russ et al. 2014).
Moreover, they are also proposed to increase the risk of dementia and cognitive impairment by
increasing the likelihood of developing systemic diseases that in turn independently increase the risk of
cognitive deterioration (Xu et al. 2014).
Smoking
Smoking is one of the most commonly implicated life style factors in cognitive deterioration. Current
smokers carry significantly higher risk of dementia and MCI as compared to non-smokers and former
smokers. The mechanisms by which smoking imparts adverse effects on cognition are not fully clear,
although the impact of smoking on cardiovascular health may at least partly explain the effects.
However, the effects are suggested to be of reversible nature, evident by reduction of dementia risk
upon smoking cessation. The reduction in dementia risk on smoking cessation is significant, with
formers smokers carrying almost same risk of dementia as non-smokers (Zhong et al. 2015).
Alcohol intake
Alcohol intake is another important lifestyle factor with significant bearing on cognition.
Current evidence indicates that alcohol exerts a range of effects on cognition which depends on the
quantity of alcohol consumed. Both heavy alcohol intake and complete abstinence from alcohol have
been reported to increase the risk of cognitive decline, while mild to moderate alcohol intake suggested
to impart a certain degree of protection against cognitive impairment (Kim et al 2016, Sabia et al.
2018).
Depression of central nervous system, neurotoxicity and impairment of cerebrovascular function are
implicated as possible pathways by which heavy alcohol intake leads to detrimental effects on
cognition (Wilhelm et al. 2015). However, the mechanism by which abstinence from alcohol increases
the risk of cognitive deterioration and the pathway by which mild to moderate alcohol consumption
provides a protective effect are still not known (Wood et al. 2016, Sabia et al. 2018).

36
Depression
Several studies have indicated that the risk of cognitive deterioration is significantly higher in
individuals with depression. Furthermore, there is also evidence that indicates increase in severity of
depression increases the severity of cognitive deterioration (Gutzmann & Qazi 2015).
The exact part that depression plays in cognitive deterioration is not clear, although, studies have
observed some similarities in brain changes in people with depression and those with dementia,
indicating a likely link between the pathological entities (Bennett & Thomas 2014). However,
depression may also be a consequence of the neurodegenerative disease process, and one of the first
symptoms to accompany the development of cognitive impairment (Zulkifly et al. 2016).
Head injury
History of head injury is another factor linked with increased risk of dementia. The risk is found to be
particularly significant in cases where head injury was accompanied with loss of consciousness.
Repeated minor head injuries such as concussion have been found to produce structural changes in the
brain. These structural changes compounded over time are believed to elevate the risk of developing
dementia (Hugo & Ganguli 2014).

37

38
Table 2: Risk and protective factors for Dementia and Cognitive impairment
Risk factors Protective factors
Non-modifiable:
Demographic factors:
Age
Gender
Genetic factors:
Different genes particularly ApoE ε4
Family history
Non-modifiable:
Genetic factors:
Different genes such as ApoE ε2
Modifiable:
Systemic factors:
Cardiovascular diseases
Stroke
Diabetes
Hypertension
Obesity
Lifestyle factors:
Sedentary lifestyle
Smoking
Heavy alcohol intake
Unhealthy dietary habits such as diets rich in
saturated fats
Others:
Depression
Psychological stress
Traumatic head injury
Modifiable:
Socioeconomic factors:
High education
High income
Lifestyle factors:
Physical activity
Participation in cognitively stimulating activities
Participation in social activities
Mild to moderate alcohol intake
Healthy diet such as Mediterranean diet or diet
rich in omega 3 and antioxidants
Pharmacological agents:
Antihypertensives
Statins
NSAIDs

39
2.2.5 Possible prevention strategies for Dementia and Mild cognitive impairment
Many modifiable factors have been proposed to significantly reduce the risk of dementia and cognitive
impairment (Savica and Petersen 2011). Among these factors, physical activity and higher education
are found to be most impactful (Schlosser Covell et al. 2015, Mirza et al. 2016). Moreover, healthy
dietary practices such as diets rich in omega 3 and antioxidants, bilingualism and participation in social
and cognitively stimulating activities also render some protective effect against cognitive deterioration
(Hu et al 2013, Ramakrishnan et al. 2017, Zhou et al. 2018).
The exact mechanism by which these factors provide protection against cognitive deterioration are still
poorly understood. Healthy lifestyle practices such as physical activity and Mediterranean diet are
believed to prevent metabolic disturbances and systemic inflammation that are in turn regarded as
independent risk factors for dementia and cognitive impairment (Petersson and Philippou 2016).
Whereas, social and cognitively stimulating factors such as higher education, bilingualism, continuous
learning and social activities are suggested to render protective effect against cognitive deterioration by
means of 'cognitive reserve' (Paillard-Borg et al. 2009). Cognitive reserve is a term referring to the
individual’s ability to tolerate or cope with the pathological changes by means of the way in which
cognitive tasks are processed and performed (Russ et al. 2013).
In addition to lifestyle factors, evidence suggests that a number of pharmacological agents such as
antihypertensive dugs, statins and anti-inflammatory agents like non-steroidal anti-inflammatory drugs
(NSAIDs) may provide protective effect against dementia and cognitive impairment (Pan et al. 2018,
Tan et al. 2018, Xue ta al. 2018). The underlying principle in the proposed effect of these agents is to
reduce the risk of systemic diseases that in turn are risk factors for cognitive deterioration. However,
the evidence regarding rigorous use of any of these agents in preventive regimens is not enough.
Indeed, some studies have also produced contradictory results, especially in case of NSAIDs, where
use of suggested pharmacological agents in old age may predispose to a greater risk of cognitive
deterioration. Furthermore, the dosage, duration of use and time span during which they may render
protective effect are still under investigation (DeLoach & Beall 2018).

40
Several clinical trials involving different lifestyle changes or pharmacological agents have been
conducted. Although some positive effects have been observed, the magnitude of the effect has not
been of much practical significance (Sindi et al. 2015). There are 3 main reasons cited for this limited
success. Firstly, most of the trials were focused on determining the effect of targeting a single risk
factor, which does not consider the multifactorial nature of dementia. Secondly, dementia is a chronic
pathology that results from the interplay of several risk factors over a life span. Thereby, preventive
measures are also needed to be applied with a life course perspective, rather than administering them in
old age when the underlying pathology may already have been in development for years (Mangialasche
et al. 2012).
Thirdly, several risk factors such as hypertension and obesity seem to have age- or time-dependent
effects, suggesting that there may be an optimal time window when preventive interventions need to be
administered to achieve maximum benefit (Richard et al. 2009, Corrada et al. 2017, Singh-Manoux et
al. 2018). Moreover, methodological limitations such as small sample size and short duration of the
study are reasoned for the inconclusive effects (Mangialasche et al. 2012).
2.2.5.1 Multi-domain trials in Dementia prevention
Several recent clinical trials have attempted to prevent dementia and MCI by applying multidomain
preventive interventions that aim to target multiple risk factors simultaneously. Examples of such major
trials include Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability
(FINGER), Multidomain Alzheimer Preventive Trial (MAPT) and the Prevention of Dementia by
Intensive Vascular Care (PreDIVA). These trials are based on controlling for systemic and vascular
factors in conjunction with introduction of lifestyle changes. Lifestyle changes comprise physical
activity, healthy nutrition, social and cognitively stimulating activities that have been suggested to
increase resilience against cognitive deterioration (Andrieu et al. 2011).
FINGER is a multidomain, multicenter interventional study conducted on 1260 individuals. It is the
first large 2-year trial that has shown significant positive effects on cognition for a multidomain
lifestyle intervention. The intervention comprised of vascular risk factors management, nutritional
guidance, physical activity and engagement in social and cognitively stimulating activities (Ngandu et
al. 2015). MAPT is a French multidomain, multicenter interventional study conducted on 1680

41
individuals. It also tested the efficacy of multidomain intervention including omega 3 supplementation
in reducing the risk of dementia (Tabue-Teguo et al. 2018).
PreDIVA was another interventional study conducted on 3534 individuals that adopted multidomain
strategy against dementia prevention. It analyzed the difference in risk of dementia between individuals
receiving standard care for cardiovascular factors and individuals that received intensive vascular care.
Intensive care regimen adopted in PreDIVA managed cardiovascular factors through multidomain
strategy including medication, nutritional and lifestyle alterations (Moll van Charante et al. 2017). The
MAPT and PreDIVA trials have several differences from FINGER, for example different target
population and intensity of the multidomain intervention. These 2 trials did not show a significant
impact on the main cognitive outcome (specific cognitive tests in MAPT, and dementia in PreDIVA).
3 AIMS AND METHODS
3.1 AIMS
3.1.1 General Objective
The general objective was to conduct a systematic review of original research articles that assessed the
association between periodontitis and dementia. This review also aimed to study the role of
periodontitis in the development of cognitive impairment. Due to the limited number of studies that
were published at the time when the search strategy for this review was undertaken, all the studies
evaluating periodontitis against cognitive decline, mild cognitive impairment, memory impairment and
cognitive dysfunction were included in this review.
All the studies, pertaining to various endpoints of cognition were addressed under the main outcome of
cognitive impairment, to assess the effect of periodontitis on cognitive impairment or on cognition in
general. The assessment of the effect of periodontitis on cognition was carried out to assess
contribution of periodontitis in the development of mild cognitive impairment which in turn increases
risk of dementia (Petersen et al. 2001). This might render more insight into the impact of periodontitis
on the overall continuum extending from healthy cognition right up to dementia.

42
3.1.2 Specific Objectives
This systematic review has following specific objectives:
1. To study whether periodontitis is a risk factor for dementia.
2. To study whether periodontitis is a risk factor for cognitive impairment.
3. To assess quality of evidence of studies evaluating the association between periodontitis and
dementia
4. To assess quality of evidence of studies evaluating the association between periodontitis and
cognitive impairment?
3.1.3 Novelty compared to previous reviews
Although in the past few years, few reviews addressing the association of periodontitis and dementia
have been conducted (Shen et al. 2016), most of them evaluated the role of periodontitis on the
progression of dementia. Furthermore, as to our knowledge none of the reviews solely focused on
longitudinal studies and included only a handful of studies with different study designs. This review
focuses on longitudinal studies and includes more recent studies compared to previous reviews.
Additionally, this review also focuses on studies assessing association between periodontal health and
cognitive impairment. Furthermore, quality assessment of the included studies was also carried out to
evaluate the overall quality of evidence that is currently available in regard to the role of periodontitis
on cognition.
3.2 METHODOLOGY
This systematic review was limited to observational longitudinal studies. Studies that directly assessed
association between periodontitis and dementia were searched on PubMed and Scopus. The search was
restricted to English language publications and was conducted by using keywords
“PERIODONTITIS”, “GINGIVITIS”, “TOOTH LOSS”, “DEMENTIA”, “PROSPECTIVE”,
“RETROSPECTIVE”, “COHORT”, “FOLLOW UP” and “LONGITUDINAL”.
The same search strategy was further expanded with search terms like “MEMORY IMPAIRMENT”,
“COGNITIVE IMPAIRMENT” and “COGNITIVE DETERIORATION” to retrieve studies that were
primarily studying the role of periodontitis in the development of cognitive impairment. Detail of the
search strategy is given in Table 4. Qualitative assessment of included studies was also conducted as

43
part of the review. The included studies were evaluated on four major domains and one minor domain
to determine overall quality of each study and risk of bias in each study. A cumulative grading was
assigned to each study based on grades attained in individual domains.
3.2.1 Inclusion criteria
Following is the inclusion criteria that was defined for this review:
• Longitudinal observational studies.
• Studies that recruited individuals without dementia at baseline. Studies with a mix of
cognitively healthy individuals and individuals with cognitive impairment at baseline were also
included if they conducted a separate analysis for incident dementia and incident cognitive
impairment.
• Studies having periodontitis as the exposure (either assessed directly or evaluated through
specifically justified proxy measures such as tooth loss).
• Dementia as the outcome of interest (for part of the review assessing periodontitis as a risk
factor for dementia) and cognitive impairment as the outcome (for part of the review assessing
periodontitis as a risk factor for impairment).
• Studies having a well-defined criterion for diagnosis of exposure and outcome.
3.2.2 Exclusion criteria
Cross sectional studies and studies that recruited individuals with dementia at baseline were excluded.
Table 3: MEDLINE search strategy PubMed July 2017 (run on date 18.07.2017)
((periodontitis) OR gingivitis) OR tooth loss
(((cognitive impairment) OR dementia) OR memory) OR cognitive deterioration
(#1 AND #2)
((((periodontitis) OR gingivitis) OR tooth loss)) AND ((((cognitive impairment) OR dementia) OR
memory impairment) OR cognitive deterioration)
((((cohort) OR prospective) OR longitudinal) OR follow up) OR retrospective
(#3 AND #4)
44
3.3.3 Quality assessment
Due to lack of availability of standardized validated tools for quality assessment of longitudinal studies,
method employed by Shamliyan et al (2011) was modified to meet the specific requirements of this
review. The quality assessment was undertaken in four major domains and one minor. Grades in
individual domains were combined to produce overall grading for each study.
Following are the domains in which each study was assessed:
1. Population representativeness: based on subdomains of age, subject selection and sample size.
2. Assessment of Exposure (Periodontitis): based on diagnostic method(s) and criteria used for
evaluation of periodontitis.
3. Length of follow up period/study duration.
4. Assessment of Outcome (Dementia and Cognitive impairment): based on diagnostic method(s)
and criteria used for the evaluation of outcome.
5. The minor domain is drop out or attrition of study participants.
3.3.3.1 Systematic evaluation of studies
Population representativeness
The representativeness of study population was based on 3 subdomains, age, random or non-random
selection and sample size. The subdomain of age was dichotomized into 2 groups, less than 65 years
old and 65 years or older. We categorized it as such, due to better probability of assessing longer-term
risk pertaining to chronic diseases such as dementia in younger individuals (less than 65 years old).
Secondly, older individuals are also likely to present with multiple comorbidities that may confound
association in question and offer significantly less time for follow up.
Furthermore, older individuals are also likely to have asymptomatic or preclinical disease (outcome) in
question as prevalence of both dementia and cognitive impairment increases significantly after 65 years
of age, making risk assessment in that age group less reliable and non-representative for majority of
general population (Kalantarian et al 2013).

45
The cut-off point of 65 years, although commonly mentioned in the literature, is somewhat arbitrary
and should be interpreted as such. Considering that chronic diseases such as dementia take decades to
develop, individuals may remain clinically asymptomatic for a long time. This may also apply to
individuals younger than 65 years.
The subdomain of random or non-random selection was stratified as such, due to inherent limitations of
non-randomized subject selection such as reduced validity and limitations encountered in
generalization of findings. Lastly, adequate cut-off for sample size was established at 1000, as cohort
studies require larger sample size as compared to case-control studies to convey same degree of
reliability that a case-control study would render with a smaller sample. Secondly, cohort studies
evaluate rate of outcome rather than prevalence of outcome, which is much smaller than prevalence and
thereby larger sample size is required in cohort studies to yield reliable findings (Tanaka et al. 2015).
Each study was graded as either “GOOD”, “MODERATE” or “LOW” depending on the following
criteria:
• Age ≤65 years AND random selection AND sample size>1000 = Good (G)
• At least two out of: Age ≤65 years, random selection, sample size >1000 = Moderate (M)
• At least two out of: Age >65 years, non-random selection, sample size<1000 = Low (L)
Exposure assessment (Periodontitis)
The grading of this domain was based on method(s) or criteria used for the assessment of periodontitis.
Each study was graded as “GOOD”, “MODERATE” or “LOW” for this domain.
a. GOOD: Studies with clinically-diagnosed periodontitis using standardized method of
periodontal examination such as measurement of periodontal pocket depths (PPDs) and/or
Clinical attachment loss (CAL) and/or alveolar bone loss (ABL) or as per the criteria
highlighted in ICD.
b. MODERATE: Studies with clinically-diagnosed periodontitis using other non-specific objective
measures of periodontal health like Gingival bleeding index (GBI), Plaque control index (PCI)
and number of missing teeth recorded by dentist or other dental medicine professional.
c. LOW: Studies that assessed periodontal status based on self- reported data such as tooth count
or presence of gingival bleeding.

46
Assessment of the Outcome (Dementia and Cognitive impairment)
Studies with dementia as the outcome were grouped separately from those studies that assessed
periodontitis and cognitive impairment. The domain of outcome assessment was graded as either
“GOOD” or “LOW”.
a. GOOD: Studies that used standard diagnostic criteria as underlined in DSM or ICD to infer
diagnosis of dementia. In case of cognitive impairment validated diagnostic criteria signified
use of standardized cognitive tests, such as MMSE, to determine the presence and degree of
cognitive impairment.
b. LOW: Studies that did not diagnose outcome(s) of interest by employing standard diagnostic
criteria or used poorly defined diagnostic criteria.
Length of follow-up period / Study duration
Although there is no standard study duration for optimal assessment of dementia risk factors, in general
studies with longer study duration in the range of decades provide more reliable scientific evidence as
compared to studies of shorter duration (Vincent et al. 2012). The following assessment was used for
study duration:
a. GOOD: Studies that had a follow up period of 20 or more years.
b. MODERATE: Studies with a follow-up period of 10-19 years.
c. LOW: Studies with less than 10 years of follow-up period.
Loss of follow-up/ Drop out
Attrition is another important aspect that defines the quality of a longitudinal study. Higher degree of
participant drop-out yields lower degree of reliability to the findings. Subsequently, a study may fail to
add intended knowledge to the body of evidence and answer the question of interest (Hill et al. 2016).
Significant loss to follow up could indicate differences between participants, and thus lead to
overestimation of the effect of exposure onto the outcome (Howe et al. 2013).
Considering the outcomes under study and mean age of participants, each study was graded as
“GOOD”, “MODERATE” or “LOW” as per the following criteria:
a. GOOD: Studies with dropout of 20% or less.

47
b. MODERATE: Studies with drop-out of 20-40%.
c. LOW: Studies with more than 40% drop-out.
Overall quality of evidence
Cumulative grading for overall quality of a study was derived by summation of grades in individual
domains for respective studies. Each study was graded as either “GOOD”, “MODERATE” or “LOW”
for overall quality. The overall grading for each study was derived as follows:
a. GOOD: “GOOD” in all major domains and “GOOD” or “MODERATE” in minor domain.
b. MODERATE: “GOOD” or “MODERATE” in all major domains but does not meet the criteria
for good quality of evidence.
c. LOW: “LOW” in at least one major domain.
4 RESULTS
The specific search strategy produced 46 articles. After reviewing through the abstracts of each article
31 studies were identified. After going through the full text, 10 articles fulfilled the inclusion criteria
(Figure 1). Five of these studies had dementia as the outcome (Stein et al. 2007, Arrive et al. 2012,
Tzeng et al. 2016, Lee YL et al 2017, Lee YT et al. 2017), while five studies assessed association
between periodontitis and cognitive impairment (Kaye et al. 2010, Reyes-Ortiz et al. 2013, Okamoto et
al. 2015, Naorungroj et al. 2015, Okamoto et al. 2017). The reference list of each study was hand-
searched in order to capture any potential study that may have been missed by the adopted search
strategy.

48
Figure 1: Search Results (Prisma flow diagram)
Records identified through database
searching
(n = 46)
Sc
reen
ing
In
clu
ded
Elig
ibili
ty
Iden
tifi
cati
on
Additional records identified through
other sources
(n = 0)
Records after duplicates removed
(n = 46)
Records screened
(n = 46)
Records excluded
(n = 15)
Full-text articles assessed for
eligibility
(n =31)
Full-text articles excluded,
with reasons
(n = 21)
Studies included in
qualitative synthesis
(n = 10)

49
4.1 STUDIES WITH DEMENTIA AS THE OUTCOME
The studies assessing the association between periodontitis and dementia are given in Table 5.
4.1.1 Designs and settings
All five studies were population based, longitudinal studies (Stein et al. 2007, Arrive et al. 2012, Tzeng
et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). Two studies were prospective cohorts (Arrive et
al. 2012, Lee YT et al. 2017) and three were retrospective studies (Stein et al. 2007, Tzeng et al. 2016,
Lee YL et al. 2017). Three studies were from Taiwan (Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et
al. 2017), one from France (Arrive et al. 2012) and one from US (Stein et al. 2007). Four studies had
both male and female participants (Arrive et al. 2012, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et
al. 2017), whereas one study had female participants only (Stein et al. 2007).
All three studies from Taiwan based their investigation on data from National health insurance research
database (NHIRD) of Taiwan (Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). The study
from France recruited participants from Paquid dental study (Arrive et al. 2012), and study from US
was based on participants from NUN study (Stein et al. 2007).
4.1.2 Study population and duration
Three studies were conducted on participants who were 65 years or older (Stein et al. 2007, Arrive et
al. 2012, Lee YT et al. 2017), while two studies adopted more diverse age criterion (Tzeng et al. 2016,
Lee YL et al. 2017), with one cohort comprising of 45 years or older participants (Lee YL et al. 2017),
while one had participants aged 20 years or more (Tzeng et al 2016).
Two studies had a sample size of less than 500 participants (Stein et al. 2007, Arrive et al. 2012), while
sample size of two studies lied between 5000 and 10,000 participants (Tzeng et al. 2016, Lee YT et al.
2017). One study had a sample size of more than 180,000 participants (Lee YL et al. 2017).
Three studies had a follow-up period of 10 years (Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al.
2017), whereas one study had a follow-up period of 12 years (Stein et al. 2007) and one 15 years
(Arrive et al 2012).

50
4.1.3 Periodontitis assessment
All five studies defined periodontitis as deterioration of tooth supporting tissues (Stein et al. 2007,
Arrive et al. 2012, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). In general, multiple
measures such as tooth loss and PPDs were used to assess periodontal health. Three studies assessed
periodontitis according to ICD criteria based on PPDs and other objective measures (Tzeng et al. 2016,
Lee YL et al. 2017, Lee YT et al. 2017), while two studies used multiple oral health measures (Stein et
al. 2007, Arrive et al. 2012). One study also used a questionnaire to supplement findings of objective
measures (Arrive et al. 2012).
4.1.4 Dementia assessment
Two studies used DSM criteria for the assessment of dementia (Arrive et al. 2012, Tzeng et al. 2016).
One of these two studies diagnosed dementia according to DSM-IV R criteria (Tzeng et al 2016), while
one used DSM- III R (Arrive et al 2012). Two studies diagnosed dementia using ICD-9 codes (Lee YL
et al. 2017, Lee YT et al 2017), while one study-based assessment of dementia on the diagnostic
criteria adopted in NUN study. NUN study based their diagnosis of dementia on cognitive test results
(MMSE, DWR, etc.) and clinical finding of memory impairment. Furthermore, diagnostic criteria of
NUN study included impairment in at least one non-memory cognitive domain and inability to perform
day to day activities (Stein et al. 2007).
In all five studies participants were thoroughly examined by specialists to reach a conclusive diagnosis
(Stein et al. 2007, Arrive et al. 2012, Tzeng et al. 2016, Lee TL et al. 2017, Lee YT et al. 2017).
Clinical findings were supplemented with neuropathological evidence where available (Stein et al.
2007).
4.1.5 Periodontitis-Dementia association
Four studies reported higher risk of dementia for individuals with poor periodontal health (Stein et al
2007, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). One study found inverse association
between tooth loss and dementia onset, however this association only applied to subjects with lower
education (Arrive et al. 2012).

51
Three studies that used ICD criteria for periodontal assessment found that individuals with periodontitis
were significantly more likely to develop dementia as compared to those without periodontitis (Tzeng
et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). One of these studies concluded that severity of
periodontitis may be important in determining the risk of dementia pertaining to periodontitis (Lee YL
et al. 2017). Although the study conducted by Stein et al (2007) showed a positive association between
fewer teeth and dementia, it found no association between alveolar bone loss and dementia.

52
Table 4: Studies assessing the association between Periodontitis and Dementia
Study Design and
setting
Study population Follow-
up
(years)
Periodontitis
assessment
Dementia
assessment
Results
Lee YL
et al. 2017
Lee YT et al.
2017
Retrospective
population
based,
Longitudinal
health insurance
database (LHID
2000), National
health insurance
(NHI) Taiwan.
Prospective
population
based,
182,747 participants
(97,802 participants with
dental prophylaxis,
19,674 participants with no
treatment,
59,898 with tooth
extraction,
5,373 participants with
intensive periodontal
treatment),
45 years or older
6056 participants
(3028 cases, 3028 controls),
10
10
ICD-9-CM
523.0–523.5
ICD-9-CM
codes 523.3–5
ICD-9-CM
codes (290.X,
331.0).
ICD-9-CM
codes 290.0–
290.4, 294.1,
Participants with severe
periodontitis and those without
treatment were at greater risk of
developing dementia
Reference group: participants
with dental prophylaxis.
HR: 1.14 (CI: 1.04 – 1.24) for
participants with no treatment
HR: 1.10 (CI: 1.04 – 1.16) for
participants with tooth
extraction.
HR: 1.18 (CI: 0.97 – 1.43) for
participants with intensive
periodontal treatment.
Periodontitis increased the risk
of dementia.
HR: 1.16 (CI: 1.01–1.32)

53
Tzeng et al. 2016
Arrive et al. 2012
Longitudinal
health insurance
database (LHID
2000), National
health insurance
(NHI), Taiwan
Retrospective
population
based,
Longitudinal
health insurance
database (LHID
2000), National
health insurance
(NHI), Taiwan
Prospective
population
based, Paquid
Dental study
65 years or older (median
age 74,42 years)
2,207 participants with
periodontitis and 6,621
controls,
20 years or older
405 participants (348
participants with PPDs
measurements)
66-80 years (mean age 70)
10
15
(median
10
years)
ICD-9-CM
codes: 523.4
and 523.1
Number of
teeth, and
temporo-
mandibular
joint function,
and 331.0–
331.2.
DSM-IV R
DSM-III R
Participants with periodontitis
were more likely to develop
dementia as compared to
controls.
HR: 2.54 (CI: 1.297 - 3.352), p
= 0.002
No significant associations in
participants with higher
education. However, for
participants with lower
education tooth loss seemed to

54
Stein et al. 2007
(PAQUIDENT).
France
Retrospective
analysis
of prospective
101 participants,
75 - 98 years old (mean age
84 years)
12
DMFT
(decayed,
missing, and
filled teeth
index) and
questionnaire
regarding
dental health.
For 348
dentate
participants
bleeding on
probing, PPDs
using
Community
Periodontal
Index criteria
were noted.
MMSE,
Delayed Word
Recall, Boston
have a protective effect against
dementia.
HR: 1.07 (CI: 0.57–2.02) for
participants with 11 or more
missing teeth and higher
education
HR: 0.30 (CI: 0.11–0.79) for
participants 11 or more missing
teeth and lower education
HR:) 0.42 (CI: 0.15–1.15) for
PPDs for individuals with
higher education,
HR: 0.97 (CI: 0.29–3.19) for
PPDs for participants with
lower education.
Tooth loss was associated with
increased risk of dementia.

55
study, subset of
NUN study,
convenience
sample - United
States
Naming Test,
verbal fluency
test,
Constructional
praxis test.
The diagnosis
of dementia
was based on
the criteria
used in
NUN study.
HR: 2.20 (CI: 1.1 - 4.5) for
tooth loss
HR: 2.40 (CI: 0.86-6.6) for
alveolar bone loss
OR: odds ratio, HR: hazard ratio, ICD: International Statistical Classification of Diseases and Related Health Problems, DSM: Diagnostic
and Statistical Manual of Mental Disorder

56
4.1.6 Quality assessment of studies assessing Dementia
The quality assessment of the studies assessing association between periodontitis and dementia is given
in Table 6. According to the derived criteria of quality assessment, two studies received “moderate”
grading (Arrive et al. 2012, Lee YT et al. 2017), while three studies were assigned “low” grading (Stein
et al. 2007, Tzeng et al. 2016, Lee YL et al. 2017). Two studies had moderate grading in population
representativeness (Arrive et al. 2012, Lee YT et al. 2017) while three received low grading (Stein et
al. 2007, Tzeng et al. 2016, Lee YL et al. 2017). Population representativeness turned out to be the
main difference between the five studies, as all other domains produced same grading for all five
studies.
All five studies had moderate grading in study duration, with follow up period lying between 10 and 19
years (Stein et al. 2007, Arrive et al. 2012, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017).
All five studies received good grading in domains of exposure and outcome assessment (Stein et al.
2007, Arrive et al. 2012, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). All five studies
used standard assessment measures like PPDs to assess periodontal health, thereby they were assigned
good grading for exposure assessment (Stein et al. 2007, Arrive et al. 2012, Tzeng et al. 2016, Lee YL
et al. 2017, Lee YT et al. 2017).
Four studies assessed cognitive health and made subsequent diagnosis of dementia using the clinical
criteria in ICD or DSM, yielding good grading to each of them for outcome assessment (Arrive et al.
2012, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017). Even though one study used
cognitive tests rather than ICD or DSM criteria for outcome assessment, it also yielded good grading
for outcome assessment, as their derived criteria were similar with standardized criteria highlighted in
diagnostic manuals. Furthermore, their clinical assessment of dementia was confirmed with neuro-
pathological findings (Stein et al. 2007). None of the five studies had subject attrition or dropout of
more than 20%, thereby all five studies were graded good for minor domain (Stein et al. 2007, Arrive
et al. 2012, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017).

57
Table 5: Quality assessment of the studies assessing Dementia
Study Population
representativeness
Study
duration
Exposure
assessment
Outcome
assessment
Dropout Overall
quality of
evidence
Lee YL
et al.
2017
Lee YT
et al.
2017
Tzeng et
al. 2016
Arrive et
al. 2012
Arrive et
al. 2012
L
M
M
L
L
M
M
M
M
M
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
L
M
M
L
L
Major domains of quality assessment
1) Population Representativeness
• Age ≤65 years AND random selection AND sample size>1000 = Good (G)
• At least two out of: Age ≤65 years, random selection, sample size >1000 = Moderate (M)
• At least two out of: Age >65 years, non-random selection, sample size<1000 = Low (L)
2) Exposure Assessment
• Objective standard measurement using one or more of the following: CAL and/or PPDs,
CPITN, radiographs or using the criteria highlighted in ICD= Good (G)
• Objective measurement using non-specific oral health indexes (GBI, PCI and number of
missing teeth) = Moderate (M)
• Self-report = Low (L)
3) Length of follow up
• ≥20 years = Good (G)
• 10-19 years = Moderate (M)
• <9 years = Low (L)
58
4) Outcome Assessment
Valid if standard validated diagnostic criteria are used. If validated criteria are used it is taken
equivalent to Good (G) and if non-validated criteria are used it is taken as low (L).
Minor Domain of quality assessment
5) Drop-out
• <20% = Good (G)
• 20% to 40% = Moderate (M)
• >40% = Low (L)
Overall quality of evidence
• Good (G) = “Good” in all major domains, AND “good” or “moderate” in the minor domain
• Moderate (M) = “Good” or “moderate” in all major domains OR does not meet the
abovementioned requirements for good quality of evidence
• Low (L) = “Low” in at least one major domain.

59
4.2 STUDIES WITH COGNITIVE IMPAIRMENT AS THE OUTCOME
The studies assessing the association between periodontitis and cognitive impairment are given in
Table 7.
4.2.1 Design and settings
All five studies were population-based, prospective studies (Kaye et al. 2010, Reyes-Ortiz et al. 2013,
Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017). Three studies were from US (Kaye
et al. 2010, Reyes-Ortiz et al. 2013, Naorungroj et al. 2015) and two were from Japan (Okamoto et al.
2015, Okamoto et al. 2017). Four studies had both male and female participants (Reyes-Ortiz et al.
2013, Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017), while one study had male
participants only (Kaye et al. 2010).
The two studies from Japan used data from Fujiwara-kyo cohort (Okamoto et al. 2015, Okamoto et al.
2017), while one study from US was conducted on participants of Veterans Affairs Dental Longitudinal
Study (Kaye et al. 2010), One study had participants from a subset of ARIC study (The Atherosclerosis
Risk in Communities Study) (Naorungroj et al 2015), whereas one study was based on Mexican
American participants from the Hispanic Established Populations for Epidemiologic Studies of the
Elderly (Reyes-Ortiz et al 2013).
4.2.2 Study population and study duration
Four studies had a relatively narrow age range for participants, mainly focusing on elderly population
(Reyes-Ortiz et al. 2013, Naorungroj et al 2015, Okamoto et al. 2015, Okamoto et al. 2017). Three
studies recruited participants who were 65 years or older (Reyes-Ortiz et al. 2013, Okamoto et al. 2015,
Okamoto et al. 2017) whereas participants in one study were between 52 to 75 years at baseline
(Naorungroj et al 2015). Study from Kaye et al. (2010) adopted a wider inclusion criterion and
recruited both middle aged and young adults, with the lowest age bound of 28 years at baseline.

60
Three studies had a sample size of less than 1000 participants (Kaye et al. 2010, Naorungroj et al. 2015,
Okamoto et al. 2017), while sample size of two studies ranged between 2000 and 3500 (Reyes-Ortiz et
al. 2013, Okamoto et al. 2015). Out of the five studies, three studies had a follow-up of 5 years (Reyes-
Ortiz et al. 2013, Okamoto et al. 2015, Okamoto et al. 2017), whereas one study had a follow up of 8
years (Naorungroj et al. 2015) and one of 32 years (Kaye et al 2010).
4.2.3 Periodontitis assessment
All five studies defined periodontitis as deterioration of tooth supporting tissues (Kaye et al. 2010,
Reyes-Ortiz et al. 2013, Naorungroj et al 2015, Okamoto et al. 2015, Okamoto et al. 2017). All five
studies used tooth count for periodontal assessment (Kaye et al. 2010, Reyes-Ortiz et al. 2013,
Naorungroj et al 2015, Okamoto et al. 2015, Okamoto et al. 2017), four of which supplemented tooth
count with other measures (Kaye et al. 2010, Naorungroj et al 2015, Okamoto et al. 2015, Okamoto et
al. 2017), while study by Reyes et al (2013) had no other measure to assess periodontal health.
Four studies assessed periodontal health objectively (Kaye et al. 2010, Naorungroj et al 2015, Okamoto
et al. 2015, Okamoto et al. 2017), while one study used subjective data (Reyes-Ortiz et al. 2013). In
addition to tooth count, four studies used PPDs (Kaye et al. 2010, Naorungroj et al 2015, Okamoto et
al. 2015, Okamoto et al. 2017), while one study also had measurements on alveolar bone loss (Kaye et
al. 2010). Kaye et al (2010) also used a questionnaire to supplement findings of PPDs, ABL and tooth
count. Whereas Naorungroj et al (2015) conducted an interview as part of exposure assessment in
addition to objective measures of PPDs and tooth count.
4.2.4 Cognitive impairment assessment
In three studies cognitive decline was the outcome. Cognitive decline was defined as change in
cognition over time and was measured as the difference between baseline and final cognitive test scores
(Kaye et al. 2010, Reyes-Ortiz et al. 2013, Naorungroj et al. 2015). Two studies defined outcome as
mild memory impairment (MMI). In these studies, MMI referred to decline or impairment of memory
while other cognitive domains remain intact. Furthermore, it was treated as a milder form of cognitive
deterioration as compared to MCI (Okamoto et al. 2015, Okamoto et al. 2017). One of these studies
analyzed MMI as the only outcome measure (Okamoto et al. 2017), while the other study also included
cases of MCI in secondary analysis (Okamoto et al. 2015).

61
All five studies assessed cognitive status objectively by means of standardized cognitive tests (Kaye et
al. 2010, Reyes-Ortiz et al. 2013, Naorungroj et al 2015, Okamoto et al. 2015, Okamoto et al. 2017).
Four studies used more than one cognitive test (Kaye et al. 2010, Naorungroj et al 2015, Okamoto et al.
2015, Okamoto et al. 2017), while one study employed only one cognitive test for outcome assessment
(Reyes-Ortiz et al. 2013). MMSE was the most commonly used cognitive test, employed by four of the
five studies (Kaye et al. 2010, Reyes-Ortiz et al. 2013, Okamoto et al. 2015, Okamoto et al. 2017),
whereas three studies used recall test (Okamoto et al. 2015, Naorungroj et al. 2015, Okamoto et al.
2017).
4.2.5 Periodontitis-Cognitive impairment association
Overall results were conflicting on the association of periodontitis and cognitive impairment. The
overall quality of evidence was low. Four studies did indicate positive association between low tooth
count and cognitive impairment (Kaye et al. 2010, Reyes-Ortiz et al. 2013, Okamoto et al. 2015,
Okamoto et al. 2017). One of these studies reported positive association only in the subjects with
positive status for ApoE ε4 (Kaye et al. 2010), while one reported positive association between rate of
tooth loss and cognitive decline (Okamoto et al. 2017).
Two studies reported positive association between low tooth count and cognitive decline (Kaye et al.
2010, Reyes-Ortiz et al. 2013). One study reported positive association between low tooth count and
MMI (Okamoto et al. 2017), while one study reported positive association between low tooth count and
MMI and MCI (Okamoto et al. 2015). The study conducted by Naorungroj et al (2015) reported higher
risk of cognitive decline in individuals with complete tooth loss.
Four studies analyzed association between PPDs and cognitive impairment (Kaye et al. 2010,
Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017). Three of these studies showed no
association between PPDs and cognitive impairment either with cognitive decline (Naorungroj et al.
2015) or with MMI (Okamoto et al. 2017) or MMI and MCI (Okamoto et al. 2015). However, study
conducted by Kaye et al (2010) observed positive association between PPDs and cognitive decline.

62
Furthermore, it also reported higher risk of cognitive decline as a function of alveolar bone loss (Kaye
et al. 2010)

63
Table 6: Studies assessing the association between Periodontitis and Cognitive impairment
Study Design and
setting
Study
population
Follow-up
(years)
Periodontitis
assessment
Cognitive
impairment
assessment
Results
Okamoto
et al. 2017
Prospective
population based,
Fujiwara-kyo
study, Japan
537
participants
(179 cases,
358
controls),
65 years or
above.
5
Tooth count and
PPDs using
Community
Periodontal Index
criteria.
Mild memory
impairment
(MMI) -
(MMI was
defined as no
impairment of
ADL, normal
general cognitive
function: MMSE
score ≥24,
presence of
objective memory
impairment
Recall test, score
≤ 1, and absence
of depression)
MMSE and
Recall test.
No association between PPDs and MMI.
Reference group: PPDs: CPI codes (0-3)
and absence of ApoE ε4.
OR: 0.96 (CI: 0.37–2.45) for code 4 and
presence of ApoE ε4
OR: 0.73 (CI: 0.43–1.25) for code 4 and
absence of ApoE ε4
OR: 1.01 (CI: 0.56–1.83) for code (0-3)
and absence of ApoE ε4
No significant association between tooth
loss and MMI, although presence of ApoE
ε4 modulated the effect of tooth loss on
MMI
Reference group: 9 or more teeth
remaining and absence of ApoE ε4.
OR: 0.99 (CI: 0.58–1.68) for 9 or less teeth
remaining and presence of ApoE ε4.

64
Okamoto
et al. 2015
Prospective
population based,
Fujiwara-kyo
study, Japan
2158
participants.
(2335 total,
177
edentulous),
65 years or
older.
5
Tooth count and
PPDs using
Community
Periodontal Index
criteria.
Mild memory
impairment
(MMI)
MMI: normal
cognitive
function, no
functional
incapacitation but
deterioration of
memory as
assessed by the 3-
word delayed
recall test in
MMSE - “MMI
status,” MMSE
score of 24 or
more, plus Recall
OR: 2.82 (CI: 1.15–6.9) for 8 or less teeth
remaining and presence of ApoE ε4
OR: 1.03 (CI: 0.59–1.81) for 8 or less teeth
remaining and absence of ApoE ε4.
Significant association between having
17–24 remaining teeth and MMI, and total
tooth loss (edentulism) and MMI. No
association between PPDs and MMI.
OR: 1.04 (0.74–1.47) for PPDs
Reference group: 25 or more teeth
remaining.
OR: 1.58 (1.12–2.25) for 17-24 teeth
present
OR: 1.17 (0.73–1.88) for 9-16 teeth
present
OR: 1.08 (0.64–1.80) for 1-8 teeth present

65
Naorungroj
et al. 2015
Prospective
population based,
Subset of ARIC
study, United
States
785
participants,
558 with
PPDs
assessment.
52–75 years
8
Self-reported tooth
count, PPDs,
bleeding on
probing, interview,
collection of
gingival crevicular
fluid and dental
plaque
Periodontal disease
was classified
according to
Biofilm gingival
interface index
score of or 1, and
GDS (Geriatric
Depression Scale
) score of 5 or
lower.
MMSE and
Recall test. DSM
R3rd edition.
Cognitive decline.
Delayed Word
Recall (DWR),
Digit Symbol
Substitution
(DSS) and Word
Fluency (WF)
test.
Tooth loss and periodontal disease did not
predict greater cognitive decline.
The exposure-outcome association was
presented as a change in cognitive test
scores against oral health measures
Beta estimate for PPDs (severe
periodontitis) with corresponding standard
error and p values:
DWR: −0.16 (SE: 0.21), p = 0.6040
DSS: −0.28 (SE: 1.56), p = 0.5165
WF: −0.50 (SE: 1.79), p = 0.6225

66
Reyes-
Ortiz et al.
2013
Prospective
population based,
Mexican
Americans
participants,
Hispanic
Established
Populations for
Epidemiologic
Studies of the
Elderly (Hispanic
EPESE), United
States.
3032
participants
(1967
participants
in the final
wave)
65 years or
older
5
classification that
comprises of PPDs
and bleeding on
probing to
conclude presence
and extent of
periodontitis.
Self-reported tooth
count
Cognitive decline.
MMSE.
Beta estimate for PPDs (severe
periodontitis) with corresponding standard
error and p values as a function of time:
DWR: 0.45 (SE: 0.27), p = 0.5655
DSS:0.55 (SE: 1.14), p = 0.7636
WF: −0.96 (SE: 1.17), p = 0.2173
Fewer teeth was associated with greater
cognitive decline over time as assessed
through drop in MMSE score.
Estimate change in MMSE over five year
follow up period, negative sign indicates
decline.
Estimate= -0.12, (SE ± 0.05, p <0.01) for
overall drop in MMSE score.

67
Kaye et al.
2010
Prospective
population based,
Veterans Affairs
Dental
Longitudinal
Study.
(convenience
sample, men only
study), United
States
597
participants,
28–70 years
32 PPDs, radiographic
alveolar bone
height, tooth count,
new caries and
restorations.
Additionally, a
questionnaire
regarding oral
hygiene practices
was also
administered.
Cognitive decline
– fall of cognitive
scores below the
cut-off value (25
points or less than
90% of age and
education specific
scores on MMSE
or less than 10
points on SCT).
MMSE and
Spatial Copying
Task (SCT).
Rate of tooth loss and periodontal disease
progression indicated increased risk of
cognitive impairment.
Oral health measures against MMSE,
SCT:
HR: 1.03 (C:1.00 – 1.07), 1.03 (CI: 1.01,
1.06) - per additional tooth with alveolar
bone loss progression/decade (tooth loss)
HR: 1.04 (1.01, 1.09), 1.04 (1.01, 1.06) -
per additional tooth with pocket depth
progression/decade (PPDs)
HR: 1.09 (1.01, 1.18), 1.12 (1.05, 1.18) -
per additional tooth lost/decade (Alveolar
bone loss)
HR: 1.02 (0.97, 1.08), 1.05 (1.01, 1.08) -
per additional tooth with new caries and/or
restorations/decade.
OR: odds ratio, HR: hazards ratio

68
4.2.6 Quality assessment of studies assessing Cognitive impairment
The quality assessment of the studies assessing association between periodontitis and cognitive
impairment is given in Table 8. All five studies received “low” grading (Kaye et al. 2010, Reyes Ortiz
et al. 2013, Okamoto et al. 2015, Naorungroj et al. 2015, Okamoto et al. 2017). Unlike studies with
dementia, studies concerning cognitive impairment were quite dissimilar in individual domains. Two
studies received moderate grading for population representativeness (Reyes-Ortiz et al. 2013, Okamoto
et al. 2015), while three were assigned low grading (Kaye et al. 2010, Naorungroj et al. 2015, Okamoto
et al. 2017). Four studies were given low grade for study duration as each of these four studies followed
participants for less than 10 years (Reyes-Ortiz et al. 2013, Okamoto et al. 2015, Naorungroj et al.
2015, Okamoto et al. 2017) while one study received good grade for study duration, as it followed the
participants for up to 32 years (Kaye et al. 2010).
Four studies were assigned good grading for exposure assessment as they used standard measures such
as PPDs for assessment of periodontitis (Kaye et al. 2010, Okamoto et al. 2015, Naorungroj et al. 2015,
Okamoto et al. 2017), While study conducted by Reyes-Ortiz et al (2013) assessed periodontal status
subjectively and received low grade for exposure assessment. All five studies received good grading
for assessment of cognitive status. The cognitive health and subsequent diagnosis of cognitive
impairment either as cognitive impairment (MMI or MCI) or cognitive decline was made using
cognitive tests (Kaye et al. 2010, Reyes-Ortiz et al. 2013, Okamoto et al. 2015, Naorungroj et al. 2015,
Okamoto et al. 2017).
Three studies had subject attrition or dropout of less than 20% that yielded good grading for minor
domain (Kaye et al. 2010, Naorungroj et al. 2015, Okamoto et al. 2017). Whereas two studies had 20%
- 40% of subject attrition and were thus assigned moderate grading (Reyes-Ortiz et al. 2012, Okamoto
et al. 2015).

69
Table 7: Quality assessment of studies assessing cognitive impairment
Study Population
representativeness
Study
duration
Exposure
assessment
Outcome
assessment
Drop
out
Overall
quality of
evidence
Okamoto et al.
2017
Naorungroj et
al. 2015
Okamoto et al.
2015
Reyes-Ortiz et
al. 2013
Kaye et al.
2010
L
L
M
M
L
L
L
L
L
G
G
G
G
L
G
G
G
G
G
G
G
G
M
M
G
L
L
L
L
L
Major domains of quality assessment
1) Population Representativeness
• Age ≤65 years AND random selection AND sample size>1000 = Good (G)
• At least two out of: Age ≤65 years, random selection, sample size >1000 = Moderate (M)
• At least two out of: Age >65 years, non-random selection, sample size<1000 = Low (L)
2) Exposure Assessment
• Objective standard measurement using one or more of the following: CAL and/or PPDs,
CPITN, radiographs = Good (G)
• Objective measurement using non-specific oral health indexes (GBI, PCI and number of
missing teeth) = Moderate (M)
• Self-report = Low (L)
3) Length of follow up
• ≥20 years = Good (G)
• 10-19 years = Moderate (M)
• <10years = Low (L)
4) Outcome Assessment
Valid if standard validated diagnostic criteria are used.
Minor Domain of quality assessment
5) Drop-out:
• <20% = Good (G)
• 20% to 40% = Moderate (M)

70
• >40% = Low (L)
Overall quality of evidence
• Good (G) = “Good” in all major domains, AND “good” or “moderate” in the minor domain
• Moderate (M) = “Good” or “moderate” in all major domains OR does not meet the
abovementioned requirements for good quality of evidence
• Low (L) = “Low” in at least one major domain.

71
5 DISCUSSION
In general, periodontitis appeared to contribute to the overall risk of dementia, whereas concerning
cognitive impairment the results were less conclusive. However, lack of uniformity in the definition
and assessment criteria of periodontitis and variability in study populations hindered cumulative
assessment of studies and a more exact estimation of the effect size of periodontitis on the risk of
dementia and cognitive impairment.
Furthermore, the lack of consensus in the definition and assessment of cognitive impairment made
it difficult to assess in more detail the interplay between periodontal health and cognitive
impairment. Multiple co-factors such as age (Stein et al. 2007, Kaye et al. 2010, Reyes-Ortiz et al.
2013, Naorungroj et al. 2015, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017), systemic
diseases (Okamoto et al. 2015, Tzeng et al. 2016, Lee YL et al. 2017, Lee YT et al. 2017, Okamoto
et al. 2017) and low socioeconomic status (Arrive et al. 2012, Tzeng et al. 2016, Lee YL et al.
2017) were observed to be significant modulators of the effect of periodontitis on dementia and
cognitive impairment.
5.1 STUDIES ON PERIODONTITIS AND DEMENTIA
5.1.1 Overall findings
Currently available evidence suggests a positive association between periodontitis and dementia,
with overall low to moderate quality of evidence. Four studies analyzed periodontitis in relation to
incident dementia (Stein et al. 2007, Arrive et al. 2012, Tzeng et al. 2016, Lee YT et al. 2017),
while one study assessed the possible effect of periodontitis severity on dementia risk (Lee YL et al.
2007). Though periodontitis appears to add to the overall risk of dementia, findings need to be
interpreted with caution, give the limitations of the included studies and subsequently limited
quality of evidence.
5.1.2 Measures of Periodontitis
Different measures, either individually or in combination, were used to assess periodontitis,
including periodontal pocket depth, tooth loss and alveolar bone loss. PPDs indicated a positive
association between periodontitis and dementia, whereas tooth loss provided conflicting results.
While ABL had no significant effect on risk of dementia, only one study assessed periodontal health
through alveolar bone loss (Stein et al. 2007).
72
5.1.3 Association between Periodontitis and Dementia based on periodontal pocket depths
Three studies, assessing difference in incident dementia between individuals with periodontitis and
those without, used periodontal pocket depths (PPDs) to assess periodontal status (Arrive et al.
2012, Tzeng et al. 2016, Lee YT et al. 2017). Two of these studies were of moderate quality and
both showed significant association between periodontitis and dementia (Tzeng et al. 2015, Lee YT
et al. 2017), while the remaining study rendered low quality of evidence and observed no significant
effect of PPDs on dementia (Arrive et al. 2012). Both studies that reported significantly greater risk
of dementia proposed inflammation as a possible mechanism behind the impact of poor periodontal
health on risk of dementia (Tzeng et al. 2015, Lee YT et al. 2017).
5.1.4 Association between Periodontitis and Dementia based on tooth loss
Two studies assessed periodontal status through tooth loss, with both studies providing low quality
of evidence (Stein et al. 2007, Arrive et al. 2012). One of them showed significant association
between tooth loss and dementia (Stein et al. 2007), while the other one observed no significant
effect of tooth loss on risk of dementia (Arrive et al. 2012).
Indeed, the study conducted by Arrive et al (2012) observed a protective effect of tooth loss against
dementia in individuals with lower education as compared to those with higher education. A
possible explanation for this peculiar finding was provided, i.e. the tendency among the individuals
with lower education to lose teeth earlier in life. Losing teeth earlier in life may subsequently
decrease the inflammatory burden associated with periodontitis in the long run, thereby, somewhat
decreasing the risk of dementia (Arrive et al. 2012). However, this finding should be interpreted
with caution, given that low education is a strong risk factor for dementia (Beydoun et al. 2014).
Although tooth loss is a relevant proxy measure of periodontitis, tooth loss can have other causes
such as dental caries or traumatic incidents. Therefore, conclusions regarding associations between
periodontitis and incident dementia based on tooth loss alone should be carefully drawn.
5.1.5 Comparison between results based on different measures of Periodontal health
Although only one study of low quality of evidence indicated a positive association between tooth
loss and dementia, 2 studies of moderate quality positively linking PPDs with dementia. The effect
size of tooth loss on dementia risk was of higher magnitude (Stein et al. 2007), than that observed
with PPDs (Tzeng et al. 2015, Lee YT et al. 2017).

73
Since tooth loss resulting from periodontitis is an indicator of periodontitis severity, this finding
may suggest that more severe periodontitis is associated with higher risk of dementia. A possible
mechanism could be the likelihood of increased inflammatory load due to increase in severity of
periodontitis. While edentulism (complete tooth loss), by the same principle, may significantly
lower the inflammatory burden contributed by periodontal tissue, other related factors such as
decreased masticatory stimulation and nutritional deficits may contribute to higher dementia risk. It
is also possible that the inflammatory burden produced by severe periodontitis prior to complete
tooth loss may have already triggered pathological changes leading to cognitive decline and
dementia.
However, severity of periodontitis is an important topic that should be further investigated in future
studies on risk factors for dementia and cognitive impairment. Several methodological
improvements will be needed to investigate the exact effects of tooth loss and edentulism as
indicators for severity of periodontitis. For example, comprehensive recording of the cause of tooth
loss should be undertaken, in addition to addressing the limitations of small sample size and
inadequate study design. Both cause and time-period of tooth loss should be considered and
accounted for, as the timeline of tooth loss would assist in estimating the past, present and
cumulative life-long burden of periodontal disease and their significance in determining the risk of
dementia and cognitive impairment. Another factor that should be considered is progression in
PPDs or CAL, which are more objective indicators of severity of periodontitis.
5.1.6 Severity of Periodontitis
The possible role of periodontitis in dementia as a function of its severity, and the impact of
periodontal treatment, are suggested by the study conducted by Lee YL et al (2017). They based
their evaluation on the periodontal treatment delivered to participants at the baseline, which was
representative of the severity of periodontal disease. This study observed that administration of no
periodontal treatment or dental extraction (tooth loss) at baseline was related to higher risk of
dementia as compared to dental prophylaxis or comprehensive periodontal treatment.
Individuals who required dental extraction at baseline were diagnosed with severe periodontitis.
Although the periodontal status at the end of the study was not known, such individuals may have
been more likely to develop severe periodontitis later on as well, which may explain their increased
risk of dementia. On the other hand, individuals who received no dental treatment carried a slightly
higher risk of dementia. The reasons why no or only limited dental treatment was administered are
74
not fully clear. If these individuals were diagnosed with mild periodontitis, their periodontal status
may have worsened over time due to lack of treatment, thereby leading to a greater chronic
inflammatory load. Whereas inflammatory burden may have been at least partly reduced in
individuals with dental extraction, provided that their periodontal health remained stable thereafter.
Although conclusions regarding exact mechanisms cannot be drawn from this study, it seems that
both presence of periodontitis and its severity have a role in determining overall risk of dementia.
The importance of early and adequate treatment of periodontitis is also emphasized. Differences in
the risk of dementia pertaining to past, present and cumulative life-long burden of periodontitis, as
well as quality of treatment, should be further investigated.
5.2 STUDIES ON PERIODONTITIS AND COGNITIVE IMPAIRMENT
5.2.1 Overall findings
While a few of the findings suggested that poorer periodontal health may be related to cognitive
impairment, non-significant results were reported as well (Kaye et al. 2010, Reyes-Ortiz et al. 2013,
Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017). Three of the five studies
assessed periodontal status against cognitive decline (Kaye et al. 2010, Reyes-Ortiz et al. 2013,
Naorungroj et al. 2015), while two studies evaluated periodontal status against risk of cognitive or
memory impairment (Okamoto et al. 2015, Okamoto et al. 2017). Neither risk of cognitive decline
nor memory impairment were significantly related to poor periodontal health (Kaye et al. 2010,
Reyes-Ortiz et al. 2013, Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017).
5.2.2 Measures of Periodontitis
Similar to the studies with dementia as the outcome, different measures including periodontal
pocket depth, tooth loss and alveolar bone loss were used to assess periodontitis either individually
or in combination. Assessment of periodontal status through PPDs against cognitive status showed
no association between periodontitis and dementia (Kaye et al. 2010, Naorungroj et al. 2015,
Okamoto et al. 2015, Okamoto et al. 2017), whereas tooth loss provided conflicting results (Kaye et
al. 2010, Reyes-Ortiz et al. 2013, Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al.
2017). The study conducted by Kaye et al (2010) observed a positive association between rate of
alveolar bone loss and cognitive impairment. However, since this is the only study that assessed
periodontal health through alveolar bone loss, findings need to be verified in further research.

75
5.2.3 Association between Periodontitis and Cognitive impairment based on periodontal
pocket depths
Four of the five studies evaluated association between periodontitis and cognitive impairment based
on periodontal pocket depths (Kaye et al. 2010, Naorungroj et al. 2015, Okamoto et al. 2015,
Okamoto et al. 2017). Three of these studies found no correlation between PPDs and cognitive
impairment (Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017), while one study
indicated increased risk of cognitive impairment as a function of increased rate of periodontal
pocket formation. Increased rate of periodontal pocket formation may infer presence of severe
periodontitis and/or progression in severity at a faster pace, which may lead to a greater
inflammatory burden and subsequently greater risk of dementia (Kaye et al. 2010).
5.2.4 Association between Periodontitis and Cognitive impairment based on tooth loss
All five studies assessed periodontitis through tooth loss (Kaye et al. 2010, Reyes-Ortiz et al. 2013,
Naorungroj et al. 2015, Okamoto et al. 2015, Okamoto et al. 2017), with three studies indicating
positive association between tooth loss and cognitive impairment (Kaye et al. 2010, Reyes-Ortiz et
al. 2013, Okamoto et al. 2015), while two studies observed no association (Naorungroj et al. 2015,
Okamoto et al. 2017).
Among the three studies with positive correlation between periodontitis and cognitive impairment,
one observed increased risk of cognitive impairment with higher rate of tooth loss. This may confer
significance to severity of periodontitis in affecting the risk of cognitive impairment (Kaye et al.
2010). Another study reported significantly greater risk of cognitive impairment in individuals
having 17-24 teeth in comparison to individuals with 25 or more teeth. But the effect was not
significant with extensive tooth loss (16 or less teeth present), except for complete tooth loss
(edentulism). A possible reason for this disparity in the association between extent of tooth loss and
cognitive impairment may have been the mechanisms connecting periodontal health and cognitive
impairment. And possible proportion of contribution made by each pathological mechanism relative
to time and severity of periodontitis (Okamoto et al. 2015).
One study observed significant effect of tooth loss on cognitive impairment in individuals with
ApoE ε4. The combined effect of tooth loss and ApoE ε4 was greater than the effect of either factor
alone. ApoE ε4 is an established risk factor for AD and is proposed to increase amyloid induced
inflammatory response and adversely affect the integrity of the blood-brain barrier (BBB). BBB
provides a route for systemic inflammation to directly impact the brain that may increase the

76
likelihood of developing dementia. Tooth loss, as a consequence of severe periodontitis, has been
suggested to contribute to the overall inflammatory burden (significantly added to by ApoE ε4) and
subsequent risk of cognitive deterioration.
5.2.5 Variability in Cognitive assessment
When considering cognitive impairment, multiple factors may affect the assessment of its presence,
progression and severity. Firstly, there was a lack of uniformity in definition of cognitive
impairment in the included studies, which used either mild memory impairment, mild cognitive
impairment or cognitive decline as outcomes. This lack of uniformity made comparisons of findings
between different studies difficult.
Secondly, there are no universally accepted criteria for defining cognitive impairment, with
differences between the procedures and tests employed in both research and clinical practice. This
leads to significant variability in results of studies using cognitive impairment as the outcome.
Thirdly, results from cognitive tests may be prone to misclassification (Wood et al. 2006).
Cognitive tests are sensitive to factors such as age and educational level, which increase the
difficulty of accurately assessing cognitive status and degree of cognitive impairment (Dellasega &
Morris 1993).
Given that cognition is composed of multiple domains, it cannot be properly assessed by means of a
single cognitive test (Synder et al. 2011). To better evaluate cognitive status, test batteries
comprising multiple cognitive tests need to be applied. Also, cognitive test batteries need to include
domain specific tests as well, to comprehensively assess specific cognitive domains in addition to
global cognitive status (Lancu & Olmer 2006).
5.3 MECHANISMS
Dementia is a multifactorial pathology and it is likely that multiple different causal pathways
concomitantly and/or synergistically contribute to its development. Periodontitis and dementia share
several common risk factors such as various systemic diseases, old age and smoking. This indicates
a complex interplay between multiple factors and mechanisms in determining the impact of
periodontitis on cognition. Moreover, this also underlines the possibility of common pathways
being part of the pathogenesis of periodontitis, cognitive impairment and dementia, and an interplay
between theses pathologies (Cerajewska et al. 2015).

77
Several mechanisms have been proposed to explain the contribution of periodontitis to the
development of dementia and cognitive impairment. Periodontitis may increase the risk of
neurodegeneration by contributing to the development and/or maintenance of systemic
inflammation. Systemic inflammation is an independent determinant of risk of cognitive
deterioration and has been suggested to facilitate the development of neuroinflammation.
Neuroinflammation is considered to be one of the central events in the pathogenesis and progression
of cognitive deterioration (Gallart-Palau et al. 2017).
Periodontal pathogens are a source of constant low-grade bacteremia and subsequent trigger for the
expression of proinflammatory cytokines. This low-grade focal inflammation constantly trickles
into systemic circulation adding to the systemic inflammatory load produced by other chronic
diseases such as CVDs and diabetes (Hajishengallis 2015). Periodontitis is independently associated
with increasing systemic concentration of pro-inflammatory cytokines, evident by increased
expression of systemic inflammatory markers such as C reactive protein (CRP) and tumor necrosis
factor alpha (TNF-α) (Nilsson et al. 2017).
Systemic cytokines are known to cross the blood brain barrier (BBB) and elicit inflammatory
response from glial cells. These systemic cytokines are suggested to either stimulate the glial cells
to produce neuroinflammation by the release of local inflammatory mediators or add to the already
existing inflammation elicited by other risk factors (Hasturk & Kantarci 2014). Inflammatory
cytokines were also proposed to trigger production of β-amyloid protein and promote
phosphorylation of tau protein, linking inflammation to protein accumulation and subsequent
neurodegeneration (Cai et al. 2014).
Moreover, cytokines were suggested to facilitate neurodegenerative processes by multiple other
mechanisms, such as, by causing direct neuronal damage and by increasing the permeability of
BBB. The weakening of BBB has been suggested to provide direct access to periodontal pathogens
and their products to the brain. Periodontal pathogens were proposed to be directly detrimental to
brain, by starting a cascade of pathological changes leading to neuroinflammation and potentially
neurodegeneration (Cai et al. 2014).
Other significant pathological changes brought about by the inflammatory process that may
contribute to the development of cognitive impairment include decrease in the concentration of
acetylcholine and increased expression of reactive oxygen species (ROS). Inflammatory cytokines

78
were found to significantly decrease the concentration of acetylcholine, both by inhibiting its
production and by facilitating its breakdown. Increased expression of ROS was associated with
deterioration of neuronal function, while reduction in the concentration of acetylcholine was
suggested to produce atrophic changes in the brain (Cunningham 2013).
Tooth loss, a direct consequence of severe periodontitis, also independently increases the risk of
dementia and cognitive impairment (Nilsson et al. 2014). Tooth loss may result in chronic
nutritional deficits such as deficiency of Vitamin B, Vitamin E and antioxidants that adversely
affect cognition, and, in the long run increase the risk of dementia. Furthermore, tooth loss was
suggested to be directly detrimental to cognitive health by facilitating the development of atrophic
changes in the brain. These atrophic changes are believed to result because of reduction in sensory
input from masticatory apparatus (Kobayashi et al. 2018).
This is consistent with animal studies showing development of learning and memory deficits as a
function of decreased masticatory stimulus due to tooth loss. Reduced brain stimulation has also
been found to decrease the number of pyramidal cells in the brain leading to reduced acetylcholine
levels in hippocampus and subsequently to memory deficit (Minn et al. 2013). Tooth loss was also
associated with decreased cerebral blood flow and was found to affect oxygen concentration in the
blood. Such changes in the cerebral circulation are also suggestive of adverse effects of tooth loss
on brain (Tonsekar et al. 2017).
Another pathway through which periodontitis may contribute to cognitive deterioration is through
the direct involvement of periodontal pathogens. Periodontal pathogens and their products may
directly transmigrate through the blood brain barrier and invoke neuroinflammation. Periodontal
pathogens are also believed to reach the brain through nerve plexus in the head region such as
through the trigeminal nerve (Shoemark & Allen 2015). However, an infectious etiology of
cognitive impairment and dementia seems to be a rather distant possibility particularly through
periodontal pathogens, considering their relatively limited virulence, and the scarce amount of
evidence supporting this hypothesis (Shaik et al. 2014).
However, the continuous presence of periodontal pathogens throughout life and subsequent constant
presence of low-grade inflammation in periodontal tissues lends a certain degree of support to the
possible role of periodontal pathogens in the overall risk of dementia. Periodontal pathogens have
also been suggested to directly stimulate the innate immune system and glial cells to mount an

79
inflammatory response. Glial cells have an important role in the induction and maintenance of
neuroinflammation. The glial cells in the elderly have been found to be hypersensitive and liable to
produce an exaggerated inflammatory response, which is a common pathological trait for both
periodontitis and dementia (Harding et al. 2017).
Studies have also observed increased expression of neurofibrillary tangles in mice, owing to
lipopolysaccharide (LPS) induced chronic inflammation. LPS is a component of bacterial cell wall
and its ability to effect protein metabolism in the brain supports a possible contribution of bacterial
infection in the overall risk of neurodegeneration (Gurav 2014). Other possible pathways through
which periodontal pathogens were proposed to increase the risk of dementia include increased
expression of reactive oxygen species. Moreover, initial studies also suggest that periodontal
pathogens might modulate the risk of dementia and cognitive impairment through their effects on
adaptive immune system and host gene expression (Olsen et al. 2016, Carter et al. 2017). However,
further studies are needed to clearly understand the role of periodontal pathogens in
neurodegeneration and the exact mechanism by which periodontal health impact cognition.
5.4 STRENGTHS AND LIMITATIONS
To the best of our knowledge, this is the first review to assess the association between periodontitis
and dementia based specifically on longitudinal studies. Secondly, this review also evaluates quality
of evidence based on the risk of bias in each study. Another strength of this review is the
assessment of association between periodontitis and cognitive impairment. The inclusion of
cognitive impairment enables a clearer assessment of the possible impact of poor periodontal health
on the continuum of cognition.
However, the limited number of available studies, variability in the definition and assessment of
exposure and outcome and inconclusiveness of available evidence strongly supports the need for
further studies to understand the links between periodontitis, cognition and dementia.
There is a possibility that some studies may not have been captured by the adopted search strategy,
due to two main reasons. Firstly, the search strategy was limited to PubMed and Scopus, and
secondly, search strategy was applicable to English language publications only. Furthermore, due to
lack of validated assessment tools for quality assessment of longitudinal studies, assessment criteria
were tailored for this review. This is inherently prone to limitations, such as limited consideration of
measures relating to internal validity of studies.

80
Moreover, meta-analysis of the included studies was not conducted which may have been more
informative in highlighting the effect of poor periodontal status on the continuum of cognition. The
conductance of meta-analysis was deterred in part due to the variability in the assessment methods
used to evaluate periodontal health as well as cognitive impairment. Furthermore, studies with
cognitive impairment also lacked uniformity in terms of definition of the outcome of interest
making statistical comparison difficult. Additionally, because of limited number of studies and
heterogeneity in study populations meta-analysis was not undertaken.
5.5 CONCLUSION AND FUTURE DIRECTIONS
Due to limitations pertaining to each included study and the overall quality of evidence, the role of
periodontitis in the development of dementia and cognitive impairment needs to be further
explored. Nevertheless, it seems likely that periodontitis contributes to the overall risk of dementia
and may even elevate the risk of cognitive impairment. Therefore, further well-designed
longitudinal studies of adequate size and duration should be conducted to explore in more detail the
magnitude of the effects and the underlying mechanisms. Comprehensive assessment of
periodontitis, such as through use of multiple assessment measures including CAL, should be
included in future studies.
Future studies should also consider various aspects of periodontitis such as its severity and past,
present, and the cumulative burden of poor periodontal health, as possible factors affecting
cognitive health. If possible, recording of both extent and cause of tooth loss should be carried out
to better determine the extent of periodontal disease, and separately evaluate the effects of tooth loss
as a consequence of periodontal disease and as an independent determinant of cognitive health. Any
teeth replacement such as dentures and implants need to be noted, and their effects evaluated.
Concerning cognitive impairment as outcome, comprehensive assessment of cognition should be
carried out through test batteries instead of single tests. Cognitive outcomes will need to be well
defined according to standardized criteria to allow for comparisons to be made. Specific cognitive
domains should be assessed in addition to global cognition, in order to determine potential effects of
periodontitis on various cognitive domains. Such analyses may also facilitate in distinguishing the
effects of periodontitis on various types of dementia.

81
It is likely that multiple pathological pathways are involved in conferring increased risk of dementia
and cognitive impairment due to periodontitis. Among the most probable of these pathways is
progression of localized periodontal inflammation into systemic inflammation. Systemic
inflammation, together with other comorbidities, may elicit or add to neuroinflammation that
eventually may lead to dementia. For example, increased concentration of inflammatory markers
such as C reactive protein and interleukin-6 (IL-6) have been associated with both periodontitis and
dementia.
However, well-designed longitudinal studies evaluating changes in inflammation markers in
relation to periodontitis and cognition have not been conducted. Therefore, thorough evaluation of
inflammation markers at multiple time points during the course of the study, should be undertaken
in future studies to clarify the mechanisms by which periodontitis contributes to neurodegeneration.
Furthermore, nutritional deficits as a function of tooth loss should be considered in relation to
cognitive deterioration, as well as the impact of teeth replacement.
Additionally, the impact of periodontitis on risk of progression of cognitive impairment to dementia
should be analyzed. This may facilitate in outlining the timeline, interplay of various confounders
and magnitude of impact that periodontitis has on the overall risk and development of dementia.
Both dementia and cognitive impairment are projected to increase significantly in the next few
decades. Periodontitis is now widely accepted to be more than a passive determinant of general
health, and this review adds to previous literature indicating a possible contribution of periodontitis
to the overall risk of dementia and cognitive impairment. Since periodontitis is a preventable
disease, preventive strategies for cognitive deterioration incorporating prevention and management
of periodontitis could be effectively designed to reduce the risk of cognitive impairment and
dementia.
Since periodontitis shares multiple risk factors with dementia, its prevention may have broader
effects on the risk of dementia by reducing other common risk factors. More studies investigating
various dimensions of the periodontitis-cognition association, such as severity of periodontitis,
direct role of periodontal pathogens and possible interplay between different pathological pathways
must be carried out to conclusively determine the nature and extent of association between
periodontitis and cognitive deterioration.

82
6 REFERENCES
1. Aggarwal NT, Shah RC, Bennett DA. Alzheimer's disease: Unique markers for diagnosis &
new treatment modalities. Indian J Med Res. 2015 Oct; 142(4):369-82.
2. Aggarwal NT. Mild cognitive impairment. Panminerva Med. 2007; 49(4):183-189.
3. Albandar JM. Global risk factors and risk indicators for periodontal diseases. Periodontol
2000. 2002; 29:177-206.
4. AlJehani YA. Risk Factors of Periodontal Disease: Review of the Literature Int J Dent. 2014;
2014: 182513.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
6. Andrieu S, Aboderin I, Baeyens JP, Beard J, Benetos A, Berrut G, Brainin M, Cha HB, Chen
LK, Du P, Forette B, Forette F, Franco A, Fratiglioni L, Gillette-Guyonnet S, Gold G, Gomez
F, Guimaraes R, Gustafson D, Khachaturian A, Luchsinger J, Mangialasche F, Mathiex-
Fortunet H, Michel JP, Richard E, Schneider LS, Solomon A, Vellas B. IAGG workshop:
health promotion program on prevention of late onset dementia. J Nutr Health Aging. 2011
Aug; 15(7):562-75.
7. Armitage GC, Cullinan MP. Comparison of the clinical features of chronic and aggressive
periodontitis. Periodontol 2000. 2010 Jun; 53:12-27.
8. Armitage GC. Development of a classification system for periodontal diseases and
conditions. Ann Periodontol. 1999 Dec; 4(1):1-6
9. Arrivé E, Letenneur L, Matharan F, Laporte C, Helmer C, Barberger-Gateau P, Miquel JL,
Dartigues JF. Oral health condition of French elderly and risk of dementia: a longitudinal
cohort study. Community Dent Oral Epidemiol. 2012 Jun; 40(3):230-8.
10. Bakri I, Douglas CW, Rawlinson A. The effects of stress on periodontal treatment: a
longitudinal investigation using clinical and biological markers. J Clin Periodontol. 2013 Oct;
40(10):955-61.
11. Ballini A, Cantore S, Farronato D, Cirulli N, Inchingolo F, Papa F, Malcangi G, Inchingolo
AD, Dipalma G, Sardaro N, Lippolis R, Santacroce L, Coscia MF, Pettini F, De Vito
D, Scacco S. Periodontal disease and bone pathogenesis: The crosstalk between cytokines and
porphyromonas gingivalis. J Biol Regul Homeost Agents. 2015; 29(2):273-281.
12. Baumgart M, Snyder HM, Carrillo MC, Fazio S, Kim H, Johns H. Summary of the evidence
on modifiable risk factors for cognitive decline and dementia: A population-based perspective.
Alzheimers Dement. 2015 Jun;11(6):718-26.

83
13. Benisty S. Current concepts in vascular dementia. Geriatr Psychol Neuropsychiatr Vieil. 2013;
11(2):171-180.
14. Bennett S, Thomas AJ Depression and dementia: cause, consequence or coincidence?
Maturitas. 2014 Oct;79(2):184-90.
15. Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic
studies of modifiable factors associated with cognition and dementia: systematic review and
meta-analysis. BMC Public Health. 2014 Jun 24; 14:643.
16. Bhogal P, Mahoney C, Graeme-Baker S, Roy A, Shah S, Fraioli F, Cowley P, Jäger HR. The
common dementias: a pictorial review. Eur Radiol. 2013 Dec;23(12):3405-17
17. Billings M, Holtfreter B, Papapanou PN, Mitnik GL, Kocher T, Dye BA. Age-dependent
distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and
SHIP-TREND 2008 to 2012. J Clin Periodontol. 2018 Jun;45
18. Branco P, Weidlich P, Oppermann RV, Rosing CK. Early supra- and subgingival plaque
formation in experimental gingivitis in smokers and never-smokers. Oral Health Prev Dent.
2015; 13(1):13-20.
19. Cai Z, Hussain MD, Yan LJ. Microglia, neuroinflammation, and beta-amyloid protein in
Alzheimer's disease. Int J Neurosci. 2014 May; 124(5):307-21.
20. Casanova L, Hughes FJ, Preshaw PM. Diabetes and periodontal disease: a two-way
relationship. Br Dent J. 2014 Oct; 217(8):433-7.
21. Cekici A, Kantarci A, Hasturk H, Van Dyke T. Inflammatory and immune pathways in the
pathogenesis of periodontal disease. Periodontol 2000. 2014 Feb; 64(1): 57–80.
22. Cerajewska TL, Davies M, West NX. Periodontitis: a potential risk factor for Alzheimer's
disease. Br Dent J. 2015 Jan; 218(1):29-34.
23. Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and Psychological Symptoms of
Dementia. Front Neurol. 2012; 3: 73.
24. Chapple IL, Genco R; working group 2 of the joint EFP/AAP workshop. Diabetes and
periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and
Systemic Diseases. J Periodontol. 2013 Apr; 84(4 Suppl): S106-12.
25. Chatterjee S, Peters S, Woodward M, Arango SM, Batty GD, Beckett N, Beiser A,Borenstein
A, Crane PK, Haan M, Hassing LB, Hayden KM, Kiyohara Y, Larson EB, Li CY, Ninomiya
T, Ohara T, Peters R, Russ TC, Seshadri S, Strand BH, Walker R, Xu W,Huxley RR. Type 2
Diabetes as a risk factor for dementia in women compared with men: A Pooled Analysis of 2.3
Million People Comprising More Than 100,000 Cases of Dementia. Diabetes Care. 2016 Feb;
39(2): 300–307.
84
26. Chung JY, Kim HS, Song J. Iron metabolism in diabetes-induced Alzheimer's disease: a focus
on insulin resistance in the brain. Biometals. 2018 Jul 24.
27. Cochran DL. Inflammation and bone loss in periodontal disease. J Periodontol. 2008 Aug;
79(8 Suppl):1569-76.
28. Corrada MM, Hayden KM, Paganini-Hill A, Bullain SS, DeMoss J, Aguirre C, Brookmeyer R,
Kawas CH. Age of onset of hypertension and risk of dementia in the oldest-old: The 90+
Study. Alzheimers Dement. 2017 Feb;13(2):103-110.
29. Cunningham C. Microglia and neurodegeneration: the role of systemic inflammation. Glia.
2013 Jan; 61(1):71-90.
30. Darveau RP, Tanner A, Page RC. The microbial challenge in periodontitis. Periodontol
2000. 1997 Jun; 14:12-32.
31. Dellasega C, Morris D. The MMSE to assess the cognitive state of elders. Mini-Mental State
Examination. J Neurosci Nurs. 1993 Jun; 25(3):147-52.
32. DeLoach T, Beall J. Diuretics: A possible keystone in upholding cognitive health. Ment Health
Clin. 2018 Mar 26;8(1):33-40.
33. Dhingra K, Vandana KL. Indices for measuring periodontitis: a literature review. Int Dent J.
2011 Apr;61(2):76-84.
34. Dintica CS, Rizzuto D, Marseglia A, Kalpouzos G, Welmer AK, Wårdh I, Bäckman L, Xu W.
Tooth loss is associated with accelerated cognitive decline and volumetric brain differences: a
population-based study. Neurobiol Aging. 2018 Mar 9; 67:23-30.
35. Drisko CL. Periodontal debridement: Still the treatment of choice. J Evid Based Dent Pract.
2014; 14 Suppl: 33-41. e1.
36. Echávarri C, Burgmans S, Caballero MC, García-Bragado F, Verhey FR, Uylings HB. Co-
occurrence of different pathologies in dementia: implications for dementia diagnosis. J
Alzheimers Dis. 2012;30(4):909-17.
37. Eshkoor SA, Hamid TA Mun CY, Ng CK. Mild cognitive impairment and its management in
older people. Clin Interv Aging. 2015 Apr 10; 10:687-93.
38. Etgen T, Sander D0, Bickel H, Förstl H. Mild Cognitive Impairment and Dementia. The
Importance of Modifiable Risk Factors. Dtsch Arztebl Int. 2011 Nov; 108(44): 743–750.
39. Fratiglioni L, Launer LJ, Andersen K, Breteler MM, Copeland JR, Dartigues JF, Lobo A,
Martinez-Lage J, Soininen H, Hofman A. Incidence of dementia and major subtypes in
Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly
Research Group. Neurology. 2000;54(11 Suppl 5): S10-5.

85
40. Gallart-Palau X, Serra A, Lee BST, Guo X, Sze SK. Brain ureido degenerative protein
modifications are associated with neuroinflammation and proteinopathy in Alzheimer’s
disease with cerebrovascular disease. J Neuroinflammation. 2017; 14(1):175.
41. Gao X, Lo EC, Kot SC, Chan KC. Motivational interviewing in improving oral health: A
systematic review of randomized controlled trials. J Periodontol. 2014; 85(3):426-437.
42. Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontol 2000. 2013 Jun;
62(1):59-94.
43. Gillette-Guyonnet S, Andrieu S, Dantoine T, Dartigues JF, Touchon J, Vellas B; MAPT Study
Group. Commentary on "A roadmap for the prevention of dementia II. Leon Thal Symposium
2008." The Multidomain Alzheimer Preventive Trial (MAPT): a new approach to the
prevention of Alzheimer's disease. Alzheimers Dement. 2009 Mar;5(2):114-21.
44. Gomperts SN. Lewy body dementias: Dementia with Lewy bodies and Parkinson disease
dementia. Continuum (Minneap Minn). 2016; 22(2 Dementia):435-463.
45. Gross AJ, Paskett KT, Cheever VJ, Lipsky MS. Periodontitis: A global disease and the
primary care provider's role. Postgrad Med J. 2017; 93(1103):560-565.
46. Gurav AN. Alzheimer's disease and periodontitis--an elusive link. Rev Assoc Med Bras
(1992). 2014 Mar-Apr;60(2):173-80.
47. Gusman DJR, Mello-Neto JM, Alves BES, Matheus HR, Ervolino E, Theodoro LH, de
Almeida JM. Periodontal disease severity in subjects with dementia: A systematic review and
meta-analysis. Arch Gerontol Geriatr. 2018 May - Jun; 76:147-159.
48. Gustafson D. Adiposity indices and dementia. Lancet Neurol. 2006 Aug;5(8):713-20.
49. Gutzmann H, Qazi A. Depression associated with dementia. Z Gerontol Geriatr. 2015
Jun;48(4):305-11.
50. Hajishengallis G, Richard P. Darveau RP, Curtis MA. The Keystone Pathogen Hypothesis.
Nat Rev Microbiol. 2012 Oct; 10(10): 717–725.
51. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation.
Nat Rev Immunol. 2015 Jan; 15(1):30-44
52. Hardigan T, Ward R, Ergul A. Cerebrovascular Complications of Diabetes: Focus on
Cognitive Dysfunction. Clin Sci (Lond). 2016 Oct 1; 130(20): 1807–1822.
53. Hasturk H, Kantarci A. Activation and resolution of periodontal inflammation and its systemic
impact. Periodontol 2000. 2015 Oct; 69(1):255-73.
54. Hefti AF. Periodontal probing. Crit Rev Oral Biol Med. 1997; 8(3):336-56.
55. Highfield J. Diagnosis and classification of periodontal disease. Aust Dent J. 2009 Sep; 54
Suppl 1: S11-26.

86
56. Ho AJ, Raji CA, Becker JT, Lopez OL, Kuller LH, Hua X, Lee S, Hibar D, Dinov ID, Stein
JL, Jack CR Jr, Weiner MW, Toga AW, Thompson PM; Cardiovascular Health Study; ADNI.
Obesity is linked with lower brain volume in 700 AD and MCI patients. Neurobiol Aging.
2010 Aug;31(8):1326-39
57. Hong M, Kim HY, Seok H, Yeo CD, Kim YS, Song JY, Lee YB, Lee DH, Lee JI, Lee, TK
Ahn HS, Ko YH, Jeong SC, Chae HS, Sohn TS. Prevalence and risk factors of periodontitis
among adults with or without diabetes mellitus. Korean J Intern Med. 2016 Sep; 31(5): 910–
919.
58. Hu N, Yu JT, Tan L, Wang YL, Sun L, Tan L. Nutrition and the risk of Alzheimer's disease.
Biomed Res Int. 2013; 2013:524820.
59. Hugo J, Ganguli M. Dementia and Cognitive Impairment: Epidemiology, Diagnosis, and
Treatment. Clin Geriatr Med. 2014 Aug; 30(3): 421–442.
60. Iadecola C. The pathobiology of vascular dementia. Neuron. 2013; 80(4):844-866.
61. Jain H, Mulay S. Relationship between periodontitis and systemic diseases: leptin, a new
biomarker? Indian J Dent Res. 2014 Sep-Oct; 25(5):657-61.
62. Johannsen A, Susin C, Gustafsson A. Smoking and inflammation: evidence for a synergistic
role in chronic disease. Periodontol 2000. 2014 Feb; 64(1):111-26.
63. Kalantarian S, Stern TA, Mansour M, Ruskin JN. Cognitive Impairment Associated with
Atrial Fibrillation: A Meta-analysis. Ann Intern Med. 2013 Mar 5; 158(5 0 1): 338–346.
64. Kamer AR, Morse DE, Holm-Pedersen P, Mortensen EL, Avlund K. Periodontal inflammation
in relation to cognitive function in an older adult Danish population. J Alzheimers Dis.
2012;28(3):613-24.
65. Kamer AR, Pirraglia E, Tsui W, Rusinek H, Vallabhajosula S, Mosconi L, Yi L, McHugh P,
Craig RG, Svetcov S, Linker R6, Shi C6, Glodzik L2, Williams S2, Corby P7, Saxena D, de
Leon MJ. Periodontal disease associates with higher brain amyloid load in normal elderly.
Neurobiol Aging. 2015 Feb;36(2):627-33.
66. Kassebaum NJ, Smith AGC, Bernabe E, Fleming TD, Reynolds AE, Vos T, Murray
CJL, Marcenes W. Global, regional, and national prevalence, incidence, and disability-
adjusted life years for oral conditions for 195 countries, 1990-2015: A systematic analysis for
the global burden of diseases, injuries, and risk factors. J Dent Res. 2017; 96(4):380-387.
67. Kaye EK, Valencia A, Baba N, Spiro A 3rd, Dietrich T, Garcia RI. Tooth loss and periodontal
disease predict poor cognitive function in older men. J Am Geriatr Soc. 2010 Ap; 58(4):713-8.
68. Keyfacts. Dementia. World Health Ortagnization. 2017. http://www.who.int/news-room/fact-
sheets/detail/dementia (Accessed 25.2.2018).

87
69. Khan S, Cabanilla LL. Periodontal probing depth measurement: a review. Compend Contin
Educ Dent. 2009 Jan-Feb; 30(1):12-4, 16, 18-21; quiz 22, 36.
70. Khan S, Roslan Saub R, Vaithilingam RD, Safii SH, Vethakkan SR, Baharuddin NA.
Prevalence of chronic periodontitis in an obese population: a preliminary study. BMC Oral
Health. 2015; 15: 114.
71. Khocht A, Janal M, Turner B. Periodontal health in Down syndrome: Contributions of mental
disability, personal, and professional dental care. Spec Care Dentist. 2010; 30(3):118-123.
72. Kim S, Kim Y, Park SM. Association between alcohol drinking behaviour and cognitive
function: results from a nationwide longitudinal study of South Korea. BMJ Open. 2016 Apr
26; 6(4): e010494.
73. Kinane DF, Marshall GJ. Periodontal manifestations of systemic disease. Aust Dent J. 2001
Mar; 46(1):2-12.
74. Knopman DS, Petersen RC. Mild Cognitive Impairment and Mild Dementia: A Clinical
Perspective. Mayo Clin Proc. 2014 Oct; 89(10): 1452–1459.
75. Knopman DS, Roberts RO, Geda YE, Boeve BF, Pankratz VS, Cha RH, Tangalos EG, Ivnik
RJ, Petersen RC. Association of prior stroke with cognitive function and cognitive
impairment: a population-based study. Arch Neurol. 2009 May; 66(5):614-9.
76. Koch M, Jensen MK. HDL-cholesterol and apolipoproteins in relation to dementia. Curr Opin
Lipidol. 2016 Feb; 27(1): 76–87.
77. Kongstad J, Hvidtfeldt UA, Grønbaek M, Jontell M, Stoltze K, Holmstrup P. Amount and type
of alcohol and periodontitis in the Copenhagen City Heart Study. J Clin Periodontol. 2008
Dec; 35(12):1032-9.
78. Lam SM, Wang Y, Duan X, Wenk MR, Kalaria RN, Chen CP, Lai MK, Shui G. Brain
lipidomes of subcortical ischemic vascular dementia and mixed dementia. Neurobiol Aging.
2014 Oct;35(10):2369-81.
79. Lancu I, Olmer A. The mini-mental state examination--an up-to-date review. Harefuah. 2006
Sep; 145(9):687-90, 701.
80. Langa KM, Levine DA. The diagnosis and management of mild cognitive impairment: a
clinical review. JAMA. 2014 Dec 17; 312(23):2551-61.
81. Lee YL, Hu HY, Huang LY, Chou P, Chu D. Periodontal Disease Associated with Higher
Risk of Dementia: Population-Based Cohort Study in Taiwan. J Am Geriatr Soc. 2017 Sep;
65(9):1975-1980.

88
82. Lee YT, Lee HC, Hu CJ, Huang LK, Chao SP, Lin CP, Su EC, Lee YC, Chen CC.
Periodontitis as a Modifiable Risk Factor for Dementia: A Nationwide Population-Based
Cohort Study. J Am Geriatr Soc. 2017 Feb; 65(2):301-305.
83. Liu M, He Y, Jiang B, Wu L, Wang J, Yang S, Wang Y. Association between metabolic
syndrome and mild cognitive impairment and its age difference in a Chinese community
elderly population. Clin Endocrinol (Oxf). 2015 Jun;82(6):844-53
84. Locke D, Ivnik R, Cha R, Knopman D, Tangalos E, Boeve B, Petersen R, Smith G. Age,
family history, and memory and future risk for cognitive impairment. J Clin Exp
Neuropsychol. 2009 Jan; 31(1): 111–116.
85. Loesche WJ, Grossman NS. Periodontal disease as a specific, albeit chronic, infection:
diagnosis and treatment. Clin Microbiol Rev. 2001 Oct; 14(4):727-52
86. LoGiudice D, Watson R. Dementia in older people: an update. Intern Med J. 2014
Nov;44(11):1066-73.
87. Lönn J, Ljunggren S, Klarström-Engström K, Demirel I, Bengtsson T, Karlsson H. Lipoprotein
modifications by gingipains of Porphyromonas gingivalis. J Periodontal Res. 2018 Jan 17.
88. Lourida I, Soni M, Thompson-Coon J, Purandare N, Lang IA, Ukoumunne OC, Llewellyn DJ.
89. Macedo Paizan ML, Vilela-Martin JF. Is there an association between periodontitis and
hypertension? Curr Cardiol Rev. 2014 Nov;10(4):355-61.
90. Mangialasche F, Kivipelto M, Solomon A, Fratiglioni L. Dementia prevention: current
epidemiological evidence and future perspective. Alzheimers Res Ther. 2012; 4(1): 6.
91. Mariotti A, Hefti AF. Defining periodontal health. BMC Oral Health. 2015; 15(Suppl 1): S6.
92. Martínez-Maestre MÁ, González-Cejudo C, Machuca G, Torrejón R, Castelo-Branco C.
Periodontitis and osteoporosis: a systematic review. Climacteric. 2010 Dec;13(6):523-9
93. McDowell I, Xi G, Lindsay J, Tierney M. Mapping the connections between education and
dementia. J Clin Exp Neuropsychol. 2007 Feb;29(2):127-41.
94. Meyle J, Chapple I. Molecular aspects of the pathogenesis of periodontitis. Periodontol
2000. 2015 Oct; 69(1):7-17.
95. Miller AA, Spencer SJ. Obesity and neuroinflammation: a pathway to cognitive impairment.
Brain Behav Immun. 2014 Nov; 42:10-21
96. Milne BJ, Moffitt TE, Crump R, Poulton R, Rutter M, Sears MR, Taylor A, Caspi A. How
should we construct psychiatric family history scores? A comparison of alternative approaches
from the Dunedin Family Health History Study. Psychol Med. 2008 Dec; 38(12): 1793–1802.

89
97. Mirza SS, Portegies ML, Wolters FJ, Hofman A, Koudstaal PJ, Tiemeier H, Ikram MA.
Higher Education Is Associated with a Lower Risk of Dementia after a Stroke or TIA. The
Rotterdam Study. Neuroepidemiology. 2016;46(2):120-7.
98. Moll van Charante EP, Richard E, Eurelings LS, van Dalen JW, Ligthart SA, van Bussel EF,
Hoevenaar-Blom MP, Vermeulen M, van Gool WA. Is dementia preventable through intensive
vascular care? The preDIVA trial. Ned Tijdschr Geneeskd. 2017;161: D1184
99. Mortimer AM, Likeman M, Lewis TT. Neuroimaging in dementia: a practical guide. Pract
Neurol. 2013 Apr; 13(2):92-103
100. Naorungroj S, Schoenbach VJ, Wruck L, Mosley TH, Gottesman RF, Alonso A, Heiss G,
Beck J, Slade GD. Tooth loss, periodontal disease, and cognitive decline in the
Atherosclerosis Risk in Communities (ARIC) study. Community Dent Oral Epidemiol. 2015
Feb;43(1):47-57. doi: 10.1111/cdoe.12128. Epub 2014 Nov 3
101. Nazir MA. Prevalence of periodontal disease, its association with systemic diseases and
prevention. Int J Health Sci (Qassim). 2017 Apr-Jun; 11(2): 72–80.
102. Newman MG, Takei HH, Klokkevold PR, Carranza FA. Carranza’s Clinical Periodontology.
Elsevier Saunders 2012.
103. Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Antikainen R, Bäckman L,
Hänninen T, Jula A, Laatikainen T, Lindström J, Mangialasche F, Paajanen T, Pajala S,
Peltonen M, Rauramaa R, Stigsdotter-Neely A, Strandberg T, Tuomilehto J, Soininen H,
Kivipelto M. A 2-year multidomain intervention of diet, exercise, cognitive training, and
vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people
(FINGER): a randomised controlled trial. Lancet. 2015 Jun 6;385(9984):2255-63.
104. Nilsson H, Berglund JS, Renvert S. Periodontitis, tooth loss and cognitive functions among
older adults. Clin Oral Investig. 2017 Dec 21. Mortimer AM, Likeman M, Lewis TT.
Neuroimaging in dementia: a practical guide. Pract Neurol. 2013 Apr; 13(2):92-103.
105. Nilsson H, Berglund JS, Renvert S. Periodontitis, tooth loss and cognitive functions among
older adults. Clin Oral Investig. 2017 Dec 21.
106. Nishida M, Grossi SG, Dunford RG, Ho AW, Trevisan M, Genco RJ.Calcium and the risk
for periodontal disease. J Periodontol. 2000 Jul;71(7):1057-66.
107. Nociti FH,Jr, Casati MZ, Duarte PM. Current perspective of the impact of smoking on the
progression and treatment of periodontitis. Periodontol 2000. 2015; 67(1):187-210.
108. Oh B, Han DH, Han KT, Liu X, Ukken J, Chang C, Dounis K, Yoo JW. Association between
residual teeth number in later life and incidence of dementia: A systematic review and meta-
analysis. BMC Geriatr. 2018 Feb 17; 18(1):48.

90
109. Okamoto N, Morikawa M, Amano N, Yanagi M, Takasawa S, Kurumatani N. Effects of
Tooth Loss and the Apolipoprotein E ɛ4 Allele on Mild Memory Impairment in the Fujiwara-
kyo Study of Japan: A Nested Case-Control Study. J Alzheimers Dis. 2017; 55(2):575-583.
110. Okamoto N, Morikawa M, Tomioka K, Yanagi M, Amano N, Kurumatani N. Association
between tooth loss and the development of mild memory impairment in the elderly: the
Fujiwara-kyo Study. J Alzheimers Dis. 2015; 44(3):777-86.
111. Paillard-Borg S, Fratiglioni L, Winblad B, Wang HX. Leisure activities in late life in relation
to dementia risk: principal component analysis. Dement Geriatr Cogn Disord.
2009;28(2):136-44.
112. Pan ML, Hsu CC, Chen YM, Yu HK, Hu GC. Statin Use and the Risk of Dementia in
Patients with Stroke: A Nationwide Population-Based Cohort Study. J Stroke Cerebrovasc
Dis. 2018 Aug 4.
113. Paster BJ, Boches SK, Galvin JL, Ericson RE, Lau CN, Levanos VA, Sahasrabudhe A,
Dewhirst FE. Bacterial Diversity in Human Subgingival Plaque. J Bacteriol. 2001 Jun;
183(12): 3770–3783.
114. Periodontal country profiles. Oral Health. World Health Organization 2005.
http://www.who.int/oral_health/databases/niigata/en/ (Accessed 20.03.2018)
115. Persson GR. Dental geriatrics and periodontitis. Periodontol 2000. 2017; 74(1):102-115.
116. Petersen RC. Clinical practice. Mild cognitive impairment. N Engl J Med. 2011 Jun
9;364(23):2227-34
117. Peterson SN, Meissner T, Su AI, Snesrud E, Ong AC, Schork NJ, Bretz WA. Functional
expression of dental plaque microbiota. Front Cell Infect Microbiol. 2014; 4: 108.
118. Petersson SD, Philippou E. Mediterranean Diet, Cognitive Function, and Dementia: A
Systematic Review of the Evidence. Adv Nutr. 2016 Sep 15; 7(5):889-904.
119. Pilgram TK, Hildebolt CF, Yokoyama-Crothers N, Dotson M, Cohen SC, Hauser JF,
Kardaris E. Relationships between longitudinal changes in radiographic alveolar bone height
and probing depth measurements: data from postmenopausal women. J Periodontol. 1999
Aug; 70(8):829-33.
120. Pitiphat W, Joshipura KJ, Gillman MW, Williams PL, Douglass CW, Rich-Edwards JW.
Maternal periodontitis and adverse pregnancy outcomes. Community Dent Oral Epidemiol.
2008 Feb;36(1):3-11. doi: 10.1111/j.1600-0528.2006.00363. x.
121. Preshaw PM, Alba AL, Herrera D, Jepsen S, Konstantinidis A, Makrilakis K, Taylor R.
Periodontitis and diabetes: a two-way relationship. Diabetologia. 2012 Jan; 55(1): 21–31.

91
122. Qizilbash N, Gregson J, Johnson ME, Pearce N, Douglas I, Wing K, Evans SJW, Pocock
SJ.BMI and risk of dementia in two million people over two decades: a retrospective cohort
study. Lancet Diabetes Endocrinol. 2015 Jun;3(6):431-436.
123. Ramakrishnan S, Mekala S, Mamidipudi A, Yareeda S, Mridula R, Bak TH, Alladi S, Kaul
S. Comparative Effects of Education and Bilingualism on the Onset of Mild Cognitive
Impairment. Dement Geriatr Cogn Disord. 2017;44(3-4):222-231.
124. Regier DA, Kuhl EA, Kupfer DJ. The DSM-5: Classification and criteria changes. World
Psychiatry. 2013 Jun;12(2):92-8.
125. Reith W, Muhl-Benninghaus R. Differential diagnostics of dementia type diseases. Radiologe.
2015 May;55(5):378-85
126. Reners M, Brecx M. Stress and periodontal disease. Int J Dent Hyg. 2007 Nov; 5(4):199-204.
127. Reyes-Ortiz CA, Luque JS, Eriksson CK, Self-reported tooth loss and cognitive function:
Data from the Hispanic Established Populations for Epidemiologic Studies of the Elderly
(Hispanic EPESE). Colomb Med (Cali). 2013 Sep 30; 44(3):139-45. eCollection 2013 Jul.
128. Reynolds MA. Modifiable risk factors in periodontitis: at the intersection of aging and
disease. Periodontol 2000. 2014 Feb;64(1):7-19.
129. Richard E, Van den Heuvel E, Moll van Charante EP, Achthoven L, Vermeulen M, Bindels
PJ, Van Gool WA. Prevention of dementia by intensive vascular care (PreDIVA): a cluster-
randomized trial in progress. Alzheimer Dis Assoc Disord. 2009 Jul-Sep;23(3):198-204.
130. Rizzi L, Rosset I, Roriz-Cruz M. Global epidemiology of dementia: Alzheimer's and vascular
types. Biomed Res Int. 2014; 2014:908915. Epub 2014 Jun 25.
131. Roberts R, Knopman DS. Classification and epidemiology of MCI. Clin Geriatr Med. 2013
Nov;29(4):753-72.
132. Roberts RO, Geda YE, Knopman DS, Cha RH, Pankratz VS, Boeve BF, Tangalos EG, Ivnik
RJ, Rocca WA, Petersen RC. The incidence of MCI differs by subtype and is higher in men:
The Mayo Clinic Study of Aging. Neurology. 2012 Jan 31; 78(5):342-51
133. Robinson PJ. Gingivitis: a prelude to periodontitis? J Clin Dent. 1995; 6 Spec No: 41-5.
134. Rocca WA, Mielke MM, Vemuri , Miller VM. Sex and gender differences in the causes of
dementia: a narrative review. Maturitas. 2014 Oct; 79(2): 196–201.
135. Rubenstein J. ICD-10: are you ready? Curr Urol Rep. 2014 Nov;15(11):449.
136. Russ TC, Kivimäki M, Starr JM, Stamatakis E, Batty GD. Height in relation to dementia
death: individual participant meta-analysis of 18 UK prospective cohort studies. Br J
Psychiatry. 2014 Nov; 205(5): 348–354
92
137. Russ TC, Stamatakis E, Hamer M, Starr JM, Kivimäki M, Batty GD. Socioeconomic status
as a risk factor for dementia death: individual participant meta-analysis of 86 508 men and
women from the UK. Br J Psychiatry. 2013 Jul; 203(1):10-7.
138. Sabia S, Fayosse A, Dumurgier J, Dugravot A, Akbaraly T, Britton A, Kivimäki M, Singh-
Manoux A. Alcohol consumption and risk of dementia: 23-year follow-up of Whitehall II
cohort study. BMJ. 2018 Aug 1;362: k2927.
139. Sachdev PS Mohan A Lauren Taylor L, Jeste DV. DSM-5 and mental disorders in older
individuals: an overview. Harv Rev Psychiatry. 2015 Sep-Oct; 23(5): 320–328.
140. Sachdev PS, Blacker D, Blazer DG, Ganguli M, Jeste DV, Paulsen JS, Petersen RC.
Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol. 2014
Nov;10(11):634-42.
141. Salameh TS, Rhea EM, Banks WA, Hanson AJ. Insulin resistance, dyslipidemia, and
apolipoprotein E interactions as mechanisms in cognitive impairment and Alzheimer's
disease. Exp Biol Med (Maywood). 2016 Sep;241(15):1676-83.
142. Savica R, Petersen RC. Prevention of dementia. Psychiatr Clin North Am. 2011
Mar;34(1):127-45.
143. Scarabino D, Gambina G, Broggio E, Pelliccia F, Corbo RM. Influence of family history of
dementia in the development and progression of late-onset Alzheimer's disease. Am J Med
Genet B Neuropsychiatr Genet. 2016 Mar;171B (2):250-6.
144. Schlosser Covell GE, Hoffman-Snyder CR, Wellik KE, Woodruff BK, Geda YE, Caselli RJ,
Demaerschalk BM, Wingerchuk DM. Physical activity level and future risk of mild cognitive
impairment or dementia: a critically appraised topic. Neurologist. 2015 Feb; 19(3):89-91.
145. Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003 Jul; 9(4):165-76.
146. Shah R, Thomas R, Mehta DS. Neutrophil priming: Implications in periodontal disease. J
Indian Soc Periodontol. 2017 May-Jun; 21(3):180-185
147. Shaik MM, Ahmad S, Gan SH, Abuzenadah AM, Ahmad E, Tabrez S, Ahmed F, Kamal MA.
How do periodontal infections affect the onset and progression of Alzheimer's disease? CNS
Neurol Disord Drug Targets. 2014 Apr; 13(3):460-6.
148. Shamliyan TA, Kane RL, Ansari MT, Raman G, Berkman ND, Grant M, Janes G, Maglione
M, Moher D, Nasser M, Robinson KA, Segal JB, Tsouros S. Development quality criteria to
evaluate nontherapeutic studies of incidence, prevalence, or risk factors of chronic diseases:
pilot study of new checklists. J Clin Epidemiol. 2011 Jun; 64(6):637-57.

93
149. Shanthi KB, Krishnan S, Rani P. A systematic review and meta-analysis of plasma amyloid 1-
42 and tau as biomarkers for Alzheimer's disease. SAGE Open Med. 2015 Aug 10;
3:2050312115598250
150. Shoemark DK, Allen SJ.The microbiome and disease: reviewing the links between the oral
microbiome, aging, and Alzheimer's disease. J Alzheimers Dis. 2015; 43(3):725-38.
151. Silva MF, Cademartori MG, Leite FRM, Lopez R, Demarco FF, Nascimento GG. Is
periodontitis associated with halitosis? A systematic review and meta-regression analysis. J
Clin Periodontol. 2017.
152. Silva N, Abusleme L, Bravo D, Dutzan N, Garcia-Sesnich J, Vernal R, Hernández
M, Gamonal J. Host response mechanisms in periodontal diseases. J Appl Oral Sci. 2015
May-Jun; 23(3):329-55.
153. Sindi S, Mangialasche F, Kivipelto M. Advances in the prevention of Alzheimer's Disease
F1000Prime Rep. 2015; 7: 50.
154. Singh-Manoux A, Dugravot A, Shipley M, Brunner EJ, Elbaz A, Sabia S, Kivimaki M.
Obesity trajectories and risk of dementia: 28 years of follow-up in the Whitehall II Study.
Alzheimers Dement. 2018 Feb;14(2):178-186.
155. Slavin MJ, Brodaty H, Sachdev PS. Challenges of diagnosing dementia in the oldest old
population. J Gerontol A Biol Sci Med Sci. 2013 Sep;68(9):1103-11.
156. Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr. Microbial complexes in
subgingival plaque. J Clin Periodontol. 1998 Feb; 25(2):134-44.
157. Stein PS, Desrosiers M, Donegan SJ, Yepes JF, Kryscio RJ. Tooth loss, dementia and
neuropathology in the Nun study. J Am Dent Assoc. 2007 Oct; 138(10):1314-22; quiz 1381-2.
158. Stokin GB, Krell-Roesch J, Petersen RC, Geda YE. Mild Neurocognitive Disorder: An Old
Wine in a New Bottle. Harv Rev Psychiatry. 2015 Sep; 23(5): 368–376.
159. Suresh S, Mahendra J, Kumar ARP, Singh G, Jayaraman S, Paul R.Comparative analysis of
subgingival red complex bacteria in obese and normal weight subjects with and without
chronic periodontitis. J Indian Soc Periodontol. 2017 May-Jun; 21(3):186-191.
160. Suwama K, Yoshihara A, Watanabe R, Stegaroiu R, Shibata S, Miyazaki H. Relationship
between alcohol consumption and periodontal tissue condition in community-dwelling elderly
Japanese. Gerodontology. 2018 Mar 25.
161. Tabue-Teguo M, Barreto de Souza P, Cantet C, Andrieu S, Simo N, Fougère B, Dartigues JF,
Vellas B. Effect of Multidomain Intervention, Omega-3 Polyunsaturated Fatty Acids
Supplementation or their Combinaison on Cognitive Function in Non-Demented Older Adults

94
According to Frail Status: Results from the MAPT Study. J Nutr Health Aging.
2018;22(8):923-927.
162. Tan ECK, Qiu C, Liang Y, Wang R, Bell JS, Fastbom J, Fratiglioni L, Johnell K.
Antihypertensive Medication Regimen Intensity and Incident Dementia in an Older
Population. J Am Med Dir Assoc. 2018 Jul;19(7):577-583.
163. Teruel BM, Rodríguez JJL, McKeigue P, Mesa TC, Fuentes E, Cepero AV, Hernandez
MAG, Copeland JRM, Ferri CP, Prince MJ. Interactions between genetic admixture, ethnic
identity, ApoE genotype and dementia prevalence in an admixed Cuban sample; a cross-
sectional population survey and nested case-control study. BMC Med Genet. 2011; 12: 43.
164. Teughels W, Dhondt R, Dekeyser C, Quirynen M. Treatment of aggressive periodontitis.
Periodontol 2000. 2014; 65(1):107-133.
165. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J
Am Geriatr Soc. 1992 Sep;40(9):922-35.
166. Tonsekar PP, Jiang SS, Yue G. Periodontal disease, tooth loss and dementia: Is there a link?
A systematic review. Gerodontology. 2017 Jun;34(2):151-163.
167. Tripathi M, Tripathi M, Damle N, Kushwaha S, Jaimini A, D’Souza MM, Sharma R, Saw
S, Mondal A. Differential Diagnosis of Neurodegenerative Dementias Using Metabolic
Phenotypes on F-18 FDG PET/CT. Neuroradiol J. 2014 Feb; 27(1): 13–21.
168. Trzepacz PT, Yu P, Sun J, Schuh K, Case M, Witte MM, Hochstetler H, Hake A;
Alzheimer's Disease Neuroimaging Initiative. Comparison of neuroimaging modalities for the
prediction of conversion from mild cognitive impairment to Alzheimer's dementia. Neurobiol
Aging. 2014 Jan;35(1):143-51
169. Tynkkynen J, Hernesniemi JA, Laatikainen T, Havulinna AS, Sundvall J, Leiviskä J, Salo P,
Salomaa V. Apolipoproteins and HDL cholesterol do not associate with the risk of future
dementia and Alzheimer's disease: The National Finnish population study (FINRISK). Age
(Dordr). 2016 Dec; 38(5-6):465-473.
170. Tzeng NS, Chung CH, Yeh CB, Huang RY, Yuh DY, Huang SY, Lu RB, Chang HA, Kao
YC, Chiang WS, Chou YC, Chien WC. Are Chronic Periodontitis and Gingivitis Associated
with Dementia? A Nationwide, Retrospective, Matched-Cohort Study in Taiwan.
Neuroepidemiology. 2016; 47(2):82-93. Epub 2016 Sep 13.
171. Wancata J, Börjesson-Hanson A, Ostling S, Sjögren K, Skoog I. Diagnostic criteria influence
dementia prevalence. Am J Geriatr Psychiatry. 2007 Dec;15(12):1034-45.
172. Wiebe CB, Putnins EE. The periodontal disease classification system of the American
Academy of Periodontology--an update. J Can Dent Assoc. 2000 Dec; 66(11):594-7.

95
173. Wilensky A, Chaushu S, Shapira L The role of natural killer cells in periodontitis.
Periodontol 2000. 2015 Oct; 69(1):128-41
174. Wood RY, Giuliano KK, Bignell CU, Pritham WW. Assessing cognitive ability in research:
use of MMSE with minority populations and elderly adults with low education levels. J
Gerontol Nurs. 2006 Apr; 32(4):45-54.
175. Woodford HJ, George J. Cognitive assessment in the elderly: a review of clinical methods.
QJM. 2007 Aug;100(8):469-84. Epub 2007 Jun 12.
176. World Health Organization, Alzheimer’s Disease International. Dementia: a public health
priority. World health organization. 2012.
http://www.who.int/mental_health/publications/dementia_report_2012/en/ (Accessed
20.06.2018)
177. World Health Organization. International Classification of Diseases and Health Related
Problems. Geneva: World Health Organization 2016.
178. Xu S, Xie B, Song M, Yu L, Wang L, An C, Zhu Q, Han K, Zhao X, Zhang R, Dong L, Chai
N, Gao Y, Zhang Q, Wang X. High prevalence of mild cognitive impairment in the elderly: a
community-based study in four cities of the Hebei province, china. Neuroepidemiology. 2014;
42(2):123-30.
179. Xue YH, Peng YS, Ting HF, Peijer Hsieh J, Huang YK, Wang YH, Chiou JY, Wei JC.
Etoricoxib and Diclofenac Might Reduce the Risk of Dementia in Patients with Osteoarthritis:
A Nation-Wide, Population-Based Retrospective Cohort Study. Dement Geriatr Cogn Disord.
2018 Jun 28;45(5-6):262-271
180. Yang Y, Song W. Molecular links between Alzheimer's disease and diabetes mellitus.
Neuroscience. 2013 Oct 10;250:140-50
181. Ying H, Jianping C, Jianqing Y, Shanquan Z. Cognitive variations among vascular dementia
subtypes caused by small-, large-, or mixed-vessel disease. Arch Med Sci. 2016 Aug 1; 12(4):
747–753.
182. Ylilauri MP, Voutilainen S, Lönnroos E, Mursu J, Virtanen HE, Koskinen TT, Salonen JT,
Tuomainen TP, Virtanen JK. Association of dietary cholesterol and egg intakes with the risk
of incident dementia or Alzheimer disease: the Kuopio Ischemic Heart Disease Risk Factor
Study. Am J Clin Nutr. 2017 Feb; 105(2):476-484.
183. Zhong G, Wang Y, Zhang Y, Guo JJ, Zhao Y. Smoking Is Associated with an Increased Risk
of Dementia: A Meta-Analysis of Prospective Cohort Studies with Investigation of Potential
Effect Modifiers. PLoS One. 2015; 10(3): e0118333.

96
184. Zhou Z, Wang P, Fang Y. Social Engagement and Its Change are associated with Dementia
Risk among Chinese Older Adults: A Longitudinal Study. Sci Rep. 2018 Jan 24; 8(1):1551.
185. Zhu M, Nikolajczyk BS. Immune Cells Link Obesity-associated Type 2 Diabetes and
Periodontitis. J Dent Res. 2014 Apr; 93(4): 346–352.
186. Zulkifly MFM, Ghazali SE, Din NC, Singh DKA, Subramaniam P. A Review of Risk
Factors for Cognitive Impairment in Stroke Survivors. Scientific World Journal. 2016; 2016:
3456943.