Embed Size (px)
Citation preview

Performance Standards for Maternal and Neonatal Health
NORMAL LABOR AND DELIVERY (NLD)
Facility Name: __________________________ District: _________________________ Province: _________________________
Date of Assessment: ____________________ (day/month/year)
Assessor(s) Name(s):
1. ________________________________________________________________
2. ________________________________________________________________
3. ________________________________________________________________
Contacted People Names:
1. ________________________________________________________________
2. ________________________________________________________________
3. ________________________________________________________________

STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
NLD-01
The provider in charge prepares equipment, supplies and the environment to conduct clean and safe deliveries
01 Ensures that the delivery room is clean. (DETAILS IN FOLLOWING PAGE)
02 Ensures that the supplies and equipment to perform normal deliveries are available. (DETAILS IN FOLLOWING PAGE)
03 Ensures that the supplies and equipment to manage the normal newborn including appropriate room temperature are available. (DETAILS IN FOLLOWING PAGE)
04 Ensures that the supplies and equipment to manage any maternal or newborn complication are available. (DETAILS IN FOLLOWING PAGE)
05 Ensures that the supplies and materials for infection prevention are available.
06 Ensures that the clerking notes, partograph, and all necessary registers are available.
NLD – 02 The provider performs a rapid initial assessment of the pregnant women in labor to identify complications and prioritize admissions.
01
Observe when pregnant women arrive at the facility to check if the provider: Assesses for all emergency and priority signs immediately. (DETAILS IN THE FOLLOWING PAGE).
If emergency or priority signs are present, initiates the designated emergency response procedures and begins appropriate treatment and/or referral (see performance standards for EmOC)
Makes an immediate assessment of whether delivery is imminent (pushing, grunting, bulging thin perineum, or vagina gaping and head visible):
02 If birth is imminent, prepares for birth / If birth is not imminent, continues with care as follows
NLD-03 The provider treats the pregnant woman in labor in a cordial manner.
01 The provider ensures that she/he speaks the language spoken by the woman or seeks someone who can assist in this regard
Makes sure that the woman’s bodily privacy is protected (curtains, doors that close, cloths to cover the woman, etc.)
02 Greets the woman and her husband or companion in a cordial manner
03 Introduces her/himself
04 Explains care before any examination or procedures
05 Discreetly asks woman if she would like someone to remain with her during the examination, labor and delivery
06 Facilitates the presence of the support person of the woman’s choice, as appropriate (if the setting allows) / Ensures that ONLY the people the woman desires are present
07 Responds to questions using easy-to-understand language
08 Responds to her immediate needs (thirst, hunger, cold/hot, need to urinate, etc.)
2
MNH Performance Standards – Normal Labor and Delivery
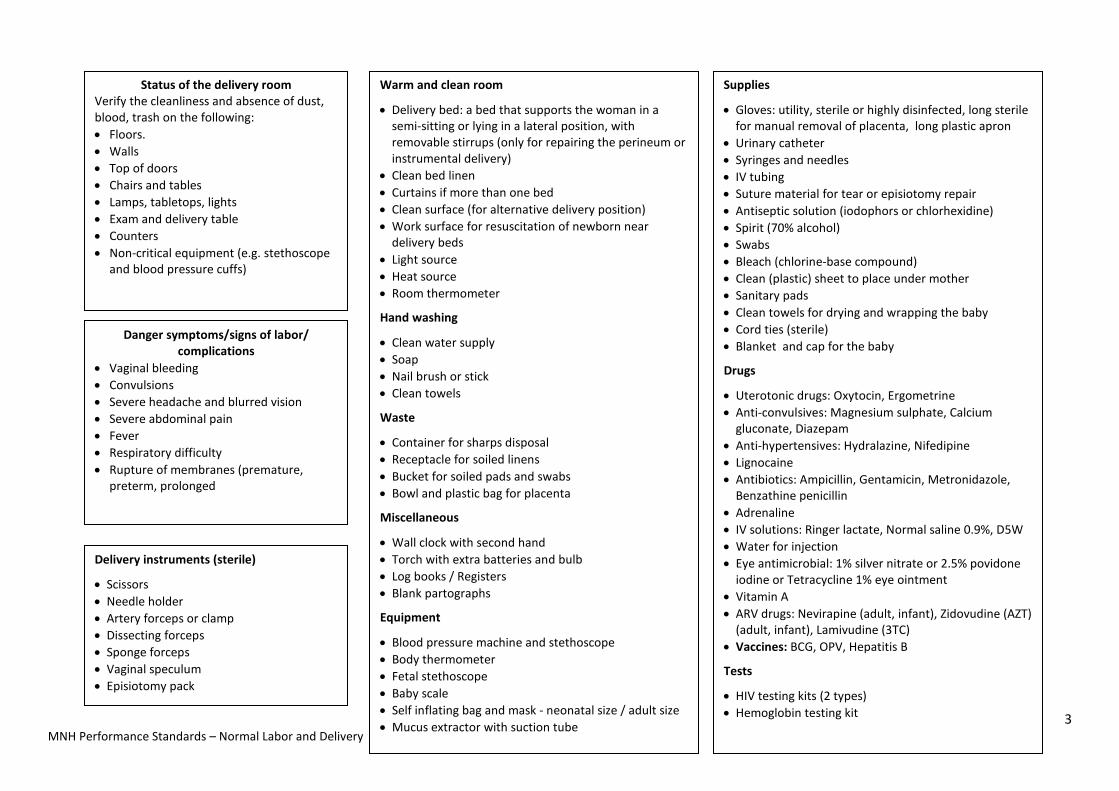
Warm and clean room
• Delivery bed: a bed that supports the woman in a semi-sitting or lying in a lateral position, with removable stirrups (only for repairing the perineum or instrumental delivery)
• Clean bed linen • Curtains if more than one bed • Clean surface (for alternative delivery position) • Work surface for resuscitation of newborn near
delivery beds • Light source • Heat source • Room thermometer
Hand washing
• Clean water supply • Soap • Nail brush or stick • Clean towels
Waste
• Container for sharps disposal • Receptacle for soiled linens • Bucket for soiled pads and swabs • Bowl and plastic bag for placenta
Miscellaneous
• Wall clock with second hand • Torch with extra batteries and bulb • Log books / Registers • Blank partographs
Equipment
• Blood pressure machine and stethoscope • Body thermometer • Fetal stethoscope • Baby scale • Self inflating bag and mask - neonatal size / adult size • Mucus extractor with suction tube
Supplies
• Gloves: utility, sterile or highly disinfected, long sterile for manual removal of placenta, long plastic apron
• Urinary catheter • Syringes and needles • IV tubing • Suture material for tear or episiotomy repair • Antiseptic solution (iodophors or chlorhexidine) • Spirit (70% alcohol) • Swabs • Bleach (chlorine-base compound) • Clean (plastic) sheet to place under mother • Sanitary pads • Clean towels for drying and wrapping the baby • Cord ties (sterile) • Blanket and cap for the baby
Drugs
• Uterotonic drugs: Oxytocin, Ergometrine • Anti-convulsives: Magnesium sulphate, Calcium
gluconate, Diazepam • Anti-hypertensives: Hydralazine, Nifedipine • Lignocaine • Antibiotics: Ampicillin, Gentamicin, Metronidazole,
Benzathine penicillin • Adrenaline • IV solutions: Ringer lactate, Normal saline 0.9%, D5W • Water for injection • Eye antimicrobial: 1% silver nitrate or 2.5% povidone
iodine or Tetracycline 1% eye ointment • Vitamin A • ARV drugs: Nevirapine (adult, infant), Zidovudine (AZT)
(adult, infant), Lamivudine (3TC) • Vaccines: BCG, OPV, Hepatitis B
Tests
• HIV testing kits (2 types) • Hemoglobin testing kit
Status of the delivery room Verify the cleanliness and absence of dust, blood, trash on the following: • Floors. • Walls • Top of doors • Chairs and tables • Lamps, tabletops, lights • Exam and delivery table • Counters • Non-critical equipment (e.g. stethoscope
and blood pressure cuffs)
Danger symptoms/signs of labor/ complications
• Vaginal bleeding • Convulsions • Severe headache and blurred vision • Severe abdominal pain • Fever • Respiratory difficulty • Rupture of membranes (premature,
preterm, prolonged
Delivery instruments (sterile)
• Scissors • Needle holder • Artery forceps or clamp • Dissecting forceps • Sponge forceps • Vaginal speculum • Episiotomy pack
3
MNH Performance Standards – Normal Labor and Delivery

STANDARD N° VERIFICATION CRITERIA OBSERVATION (YES, NO, N.A.) COMMENTS
NLD-04 The provider properly reviews and fills out the clinical history of the woman in labor.
01 Asks the woman about her current labor. DETAILS IN THE FOLLOWING PAGE.
02 Checks the woman’s antenatal record or asks for information about the pregnancy
03 Checks the woman’s record or asks about medical and surgical history 04 Checks the woman’s antenatal record or asks about HIV status
05 if HIV status is known to be positive – looks at antenatal record and asks about ARV drugs, most recent CD4 count, and any documents related to her HIV care
06 Asks the woman how she plans to feed her baby. 07 Reviews the woman’s individualized birth plan with her 08 Avoids asking questions during contractions
09 Records the information in the client’s notes
NLD-05 The provider properly conducts a physical examination between contractions.
01 Ensures privacy during the entire process of the provision of care or at least during examination. DETAILS IN THE FOLLOWING PAGE.
02 Explains to the woman and her husband/companion what the provider is going to do and encourages her to ask questions
03 Asks the woman to urinate and the provider tests the urine for albumin, glucose and ketones.
04 Performs hand hygiene. DETAILS IN THE FOLLOWING PAGE.
05 Observes the woman’s emotional response
06 Observes the woman’s response to contractions
07 Takes vital signs or delegates the task to an assistant: DETAILS IN THE FOLLOWING PAGE.
08 Checks the conjunctiva and palms of hands for pallor (clinical anemia)
09 If suspicious of anemia, sends blood for hemoglobin test or /does a hemoglobinometer test.
4
MNH Performance Standards – Normal Labor and Delivery

Danger symptoms/signs of labor complications
- Vaginal bleeding - Convulsions - Severe headache and blurred vision - Severe abdominal pain - Persistent strong contractions - Respiratory difficulty - Fever - Rupture of membranes (preterm, premature or
prolonged)
Antenatal card information
- Obstetric history - General medical problems - Use of medications or herbs - Background of the woman and her partner with
regard to sexually transmitted infections (STIs), HIV and tuberculosis (TB) and medical/surgical conditions that render delivery high risk.
- Gestational age, last menstrual period (LMP), and estimated date of childbirth (EDC) for current pregnancy
- Complications detected during current pregnancy and their management
- Fetal growth and development - Hemoglobin at last antenatal visit - Syphilis (RPR) status - STI identification during pregnancy and treatment - Tetanus immunization status - HIV status - ARV prophylaxis – MER including HAART (National
Guidelines)
Questions about current labour
- When the painful regular contractions began - How frequently they are occurring - If her “bag of waters” broke: when, what colour, and
what smell it had, any cord prolapse - Whether she feels the baby’s movements - Whether she has taken any drugs or traditional
medicine - If she has any concerns
Privacy measures
- Woman remains covered with a sheet - Area is separated with curtains, sheets, or screens,
as appropriate - The minimum number of individuals are present
during examinations and delivery (the provider attending the delivery and a family member—the individual chosen by the woman)
Hands hygiene
Washes their hands with water and soap for 10-15 seconds, paying attention to areas under the finger nails and between the fingers
Dries hands with an individual clean towel or air dries them
OR Rub both hands with approximately 5 ml of alcohol gel
70%, paying attention below to the areas the under the finger nails and between the fingers, until dry
Vital signs
- Temperature. - Pulse - Blood pressure (BP)
- Checks that the needle is at the zero mark at the start and the end of the measurement
- Checks to see that the screw valve on the ball works properly before using the BP machine
- Pumps up the bladder and watches for any air leaks before checking BP
- Chooses the correct cuff size - Removes all tight clothes from around the arm - Does not check BP during a contraction - Makes sure that the woman is as relaxed and
comfortable as possible - If diastolic BP is 90 mmHg or more, checks urine
for protein - If diastolic BP is 90 mmHg or more and the
woman has proteinuria, checks biceps or patellar reflexes
- If diastolic BP is 110 mmHg or more with proteinuria, manages as severe pre-eclampsia
- Respiratory rate
5
MNH Performance Standards – Normal Labor and Delivery

STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
NLD-06
The provider properly conducts the obstetric examination between contractions if time allows.
01 Observes the shape and size of the abdomen and checks for the presence of scars and other skin lesions
02 Avoids examining the woman during a contraction
03 Measures fundal height
04 Determines presentation, fetal lie and degree of engagement by abdominal palpation
05 Evaluates and grades uterine contractions (frequency and duration over a 10 minute period)
06 Asks if the baby is moving regularly and observes for fetal movement during the examination
07 Auscultates fetal heart rate (FHR) over a 10 minute period (fetal heart rate and changes before, during, and after a contraction)
08 Records the results of the obstetric examination on
09 Explains her findings to the woman and her husband/companion
NLD-07
The provider properly conducts a vaginal examination.
01 Explains to the woman in easy-to-understand language what she is going to do
02 Performs hand hygiene after removing gloves
03 Puts on surgical sterile or high-level disinfected (HLD) gloves on both hands
04 Examines the vulva (ulcers, blood, liquid, secretion)
05 Cleans the vulva with an antiseptic
06 If the membranes are ruptured, then conducts a vaginal cleansing with chlorhexidine prior to vaginal examinations
07 Assesses cervical dilatation, molding, and level of presenting part, Caput, State of the MRS, if ruptured the color of liquor
08 Properly disposes of gloves
09 Performs hand hygiene after removing gloves
10 Explains to the woman the findings and what they mean.
11 Registers findings
6
MNH Performance Standards – Normal Labor and Delivery

STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
NLD-08 Health care provider decides on stage and phase in labor and develops a plan of care
01 Calculates gestational age 02 Order s the appropriate laboratory exams. DETAILS ARE ON THE PAGE BELOW 03 Makes a plan of care based on stage of labor and findings on examination.
04 Records all findings – if cervix is 4 cm or more dilated, records on the partograph; if the cervix is less than 4 cm, records on the woman’s chart
05 Discusses the care decisions with the woman and her husband/companion if possible 06 Provides information to the woman and support person on the plan of care 07 Provides supportive car. (DETAILS IN THE FOLLOWING PAGE).
08 Provides information to companion on danger signs and how to support the woman in labor, including breathing exercises, massage, bathing, etc.
09 Helps the woman take a bath to ensure cleanliness
NLD-09 Health care provider provides counseling and testing for woman in labor with unknown HIV status.
01 Offers HIV testing and counseling 02 Provides counseling for negative or positive test results
03
If results were positive, discusses mother-to-child transmission of HIV, and tells the woman that she will get medicines (ARVs) right away to reduce the risk of transmitting infection to her baby (if early labor and time allows) and that the baby will also receive ARVs after delivery
NLD-10 If the woman’s HIV status is positive, the healthcare provider gives her appropriate antiretroviral prophylaxis
01 Checks if the woman is on HAART or received ARV prophylaxis during the ANC 02 Makes sure woman is in true labor
03
If woman is not on HAART and/or did not receive ARV Prophylaxis and is in labor: • Explains the importance of ARV Prophylaxis to prevent mother-to-child
transmission • Administers ARVs for prophylaxis immediately according to national PMTCT
guidelines or advises the mother to continue with HAART
04 • Informs /reminds the woman that the baby should receive ARV Prophylaxis after birth
7
MNH Performance Standards – Normal Labor and Delivery

Possible additional exams • If pallor, check haemoglobin • If diastolic BP ≥90 mmHg, check urine for protein • If diastolic BP ≥90 mmHg with proteinuria, check reflexes • If signs of dehydration, check urine for ketones • If HIV status is unknown or if HIV-negative and HIV test was
>6 weeks previous, offer voluntary counselling for rapid testing for HIV
• HIV status is positive, consider checking CD4 count if recent CD4 count is not available
Monitoring during latent phase of labor (<4 cm cervical dilatation)
At every observation
• Asks the woman how she is feeling. • Assesses for all emergency and priority signs/symptoms
immediately and, if present, initiates the designated emergency response procedures and begins appropriate treatment and/or referral.
• Makes an immediate assessment of whether delivery is imminent (pushing, grunting, bulging thin perineum, or vagina gaping and head visible): If so, prepared for birth; If not, continued as follows
• Observes the woman’s emotional response • Observes the woman’s response to contractions • Observes the woman’s eyes, mouth and skin to check for
signs of dehydration • Asks the woman if she needs to empty her bladder (Saves
urine for testing, if necessary)
Monitors the following:
• Blood pressure (every 2 hours) • Pulse (hourly) • Temperature (every 4 hours unless elevated) • The number and duration of contractions in a 10-minute
period (hourly) • Fetal heart rate (hourly) • Fetal descent abdominally (before cervical exam) • Cervical dilatation (4-hourly)
8
MNH Performance Standards – Normal Labor and Delivery

Supportive care during labor
Communication
• Explains all procedures, seek permission, and discuss findings with the woman • Keeps her informed about the progress of labor • Praises her, encourages and reassures her that things are going well • Ensures and respects privacy during examinations and discussions • If known HIV positive, finds out what she has told the companion. Respects her
wishes
Cleanliness
• Encourages the woman to bathe or shower or wash herself and genitals at the onset of labor
• Washes the vulva and perineal areas before each examination • Washes hands with soap before and after each examination • Ensures cleanliness of labor and birthing area(s) • Clean sup spills immediately • DOES NOT give enema
Mobility
• Encourages the woman to walk around freely during the first stage of labor • Supports the woman’s choice of position (left lateral, squatting, kneeling, standing
supported by the companion) for each stage of labor and deliver
Urination
• Encourages the woman to empty her bladder frequently • Reminds her every 2 hours
Eating, drinking
• Encourages the woman to eat and drink as she wishes throughout labor. • If the woman has visible severe wasting or tires during labor, makes sure she eats
and drinks
Supportive care during labor
Breathing technique
• Teaches her to notice her normal breathing. • Encourages her to breathe out more slowly, making a sighing noise, and to
relax with each breath. • If she feels dizzy, unwell, is feeling pins-and-needles (tingling) in her face,
hands and feet, encourages her to breathe more slowly. • To prevent pushing at the end of first stage of labor, teaches her to pant, to
breathe with an open mouth, to take in 2 short breaths followed by a long breath out.
• During delivery of the head, asks her not to push but to breathe steadily or to pant.
Pain and discomfort relief
• Suggests change of position • Encourages mobility, as comfortable for her • Encourages companion to:
- massage the woman’s back if she finds this helpful - hold the woman’s hand and sponge her face between contractions
• Encourages her to use the breathing technique • Encourages warm bath or shower, if available • If woman is distressed or anxious, investigates the cause
Asks the woman and birth companion to call for help if:
• The woman is bearing down with contractions. • There is vaginal bleeding. • She is suddenly in much more pain. • She loses consciousness or has fits. • There is any other concern.
9
MNH Performance Standards – Normal Labor and Delivery
STANDARD N° VERIFICATION CRITERIA OBSERVATION (YES, NO, N.A.)
COMMENTS
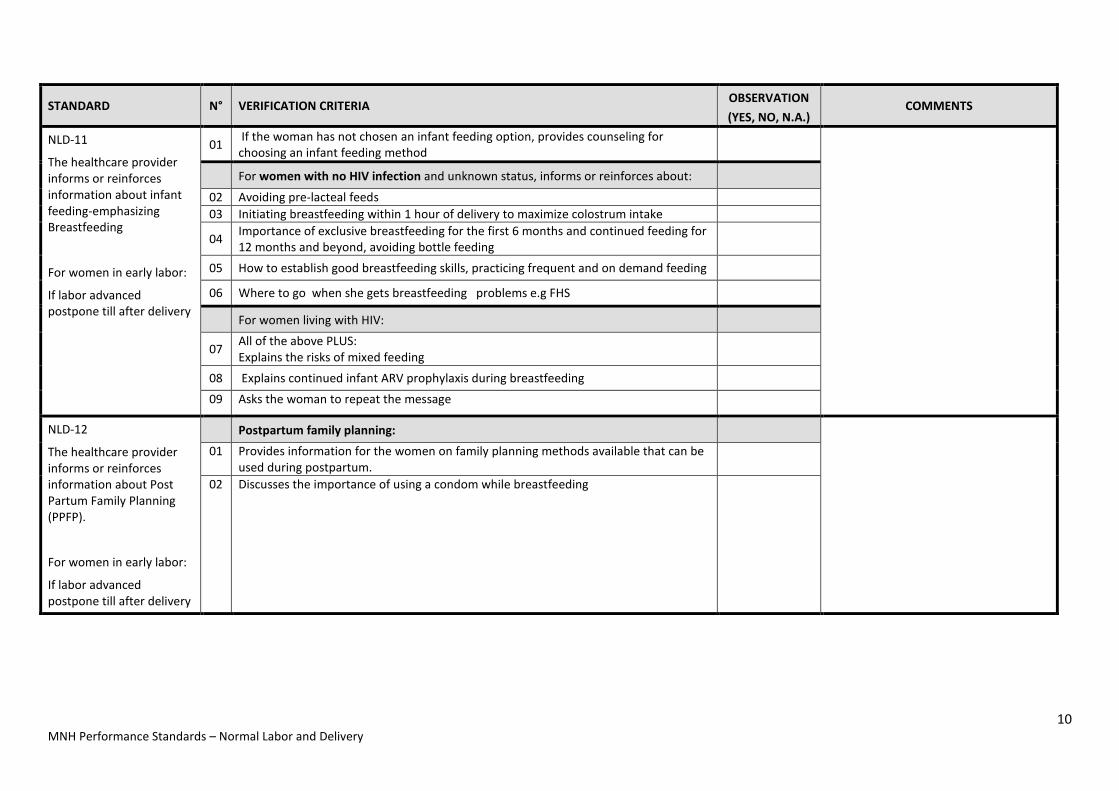
NLD-11
The healthcare provider informs or reinforces information about infant feeding-emphasizing Breastfeeding
For women in early labor:
If labor advanced postpone till after delivery
01 If the woman has not chosen an infant feeding option, provides counseling for choosing an infant feeding method
For women with no HIV infection and unknown status, informs or reinforces about:
02 Avoiding pre-lacteal feeds 03 Initiating breastfeeding within 1 hour of delivery to maximize colostrum intake
04 Importance of exclusive breastfeeding for the first 6 months and continued feeding for 12 months and beyond, avoiding bottle feeding
05 How to establish good breastfeeding skills, practicing frequent and on demand feeding
06 Where to go when she gets breastfeeding problems e.g FHS
For women living with HIV:
07 All of the above PLUS: Explains the risks of mixed feeding
08 Explains continued infant ARV prophylaxis during breastfeeding 09 Asks the woman to repeat the message
NLD-12
The healthcare provider informs or reinforces information about Post Partum Family Planning (PPFP).
For women in early labor:
If labor advanced postpone till after delivery
Postpartum family planning:
01 Provides information for the women on family planning methods available that can be used during postpartum.
02 Discusses the importance of using a condom while breastfeeding
10
MNH Performance Standards – Normal Labor and Delivery
STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
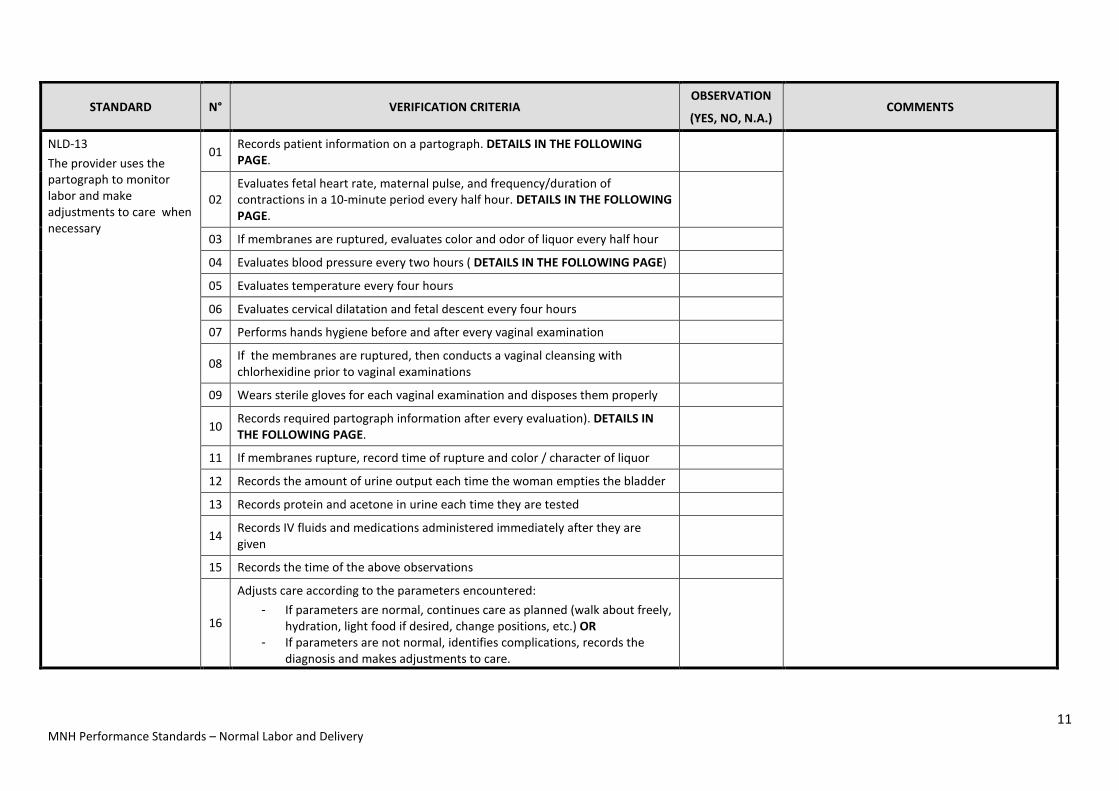
NLD-13 The provider uses the partograph to monitor labor and make adjustments to care when necessary
01 Records patient information on a partograph. DETAILS IN THE FOLLOWING PAGE.
02 Evaluates fetal heart rate, maternal pulse, and frequency/duration of contractions in a 10-minute period every half hour. DETAILS IN THE FOLLOWING PAGE.
03 If membranes are ruptured, evaluates color and odor of liquor every half hour
04 Evaluates blood pressure every two hours ( DETAILS IN THE FOLLOWING PAGE)
05 Evaluates temperature every four hours
06 Evaluates cervical dilatation and fetal descent every four hours
07 Performs hands hygiene before and after every vaginal examination
08 If the membranes are ruptured, then conducts a vaginal cleansing with chlorhexidine prior to vaginal examinations
09 Wears sterile gloves for each vaginal examination and disposes them properly
10 Records required partograph information after every evaluation). DETAILS IN THE FOLLOWING PAGE.
11 If membranes rupture, record time of rupture and color / character of liquor
12 Records the amount of urine output each time the woman empties the bladder
13 Records protein and acetone in urine each time they are tested
14 Records IV fluids and medications administered immediately after they are given
15 Records the time of the above observations
16
Adjusts care according to the parameters encountered: - If parameters are normal, continues care as planned (walk about freely,
hydration, light food if desired, change positions, etc.) OR - If parameters are not normal, identifies complications, records the
diagnosis and makes adjustments to care.
11 MNH Performance Standards – Normal Labor and Delivery

Partograph details:
Patient information: - Name - Gravida, Parity - Hospital number - Date and time of admission - Time of ruptured membranes - Time of onset of labour Information to be recorded every half hour - Fetal heart rate - Uterine contractions- frequency and duration - Maternal pulse a - Amount of IV solution with Oxytocin in
drops/minute if the woman was commenced on Oxytocin
Information to be recorded every two hours - Maternal blood pressure - Descent by abdominal examination Information to be recorded every four hours - Cervical dilatation - Descent - Temperature Documentation at every vaginal examination: - Records the condition of the membranes and
characteristics of the amniotic fluid - Records the degree of molding of the presentation - Graphs cervical dilation - Graphs the descent of the head or buttocks Information to be recorded as it occurs - Urine – amount, presence of protein or ketones - Administration of any medications - Administration of IV fluids
12
MNH Performance Standards – Normal Labor and Delivery

STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
NLD-13
The provider prepares to assist the delivery/ birth.
01 Provider prepares delivery pack and other essential materials according to National Guidelines.
02 Allows the woman to give birth in the position she wants and in the same bed where she has labored (if possible)
03 Ensures privacy of the woman. - Woman remains covered with a sheet - Area is separated with curtains, sheets, or screens, as
appropriate - The minimum number of individuals present during birth
(including the individual chosen by the woman)
04 Explains to the woman how to help herself and manage the bearing down process (when and how)
05 Encourages and speaks kindly to the woman during labor
06 Encourages the woman to ask questions and responds in easy-to-understand language
07 Makes sure the woman’s bladder is empty
08 Makes sure the woman is clean
09 Registers procedures in clinical record
13
MNH Performance Standards – Normal Labor and Delivery
STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
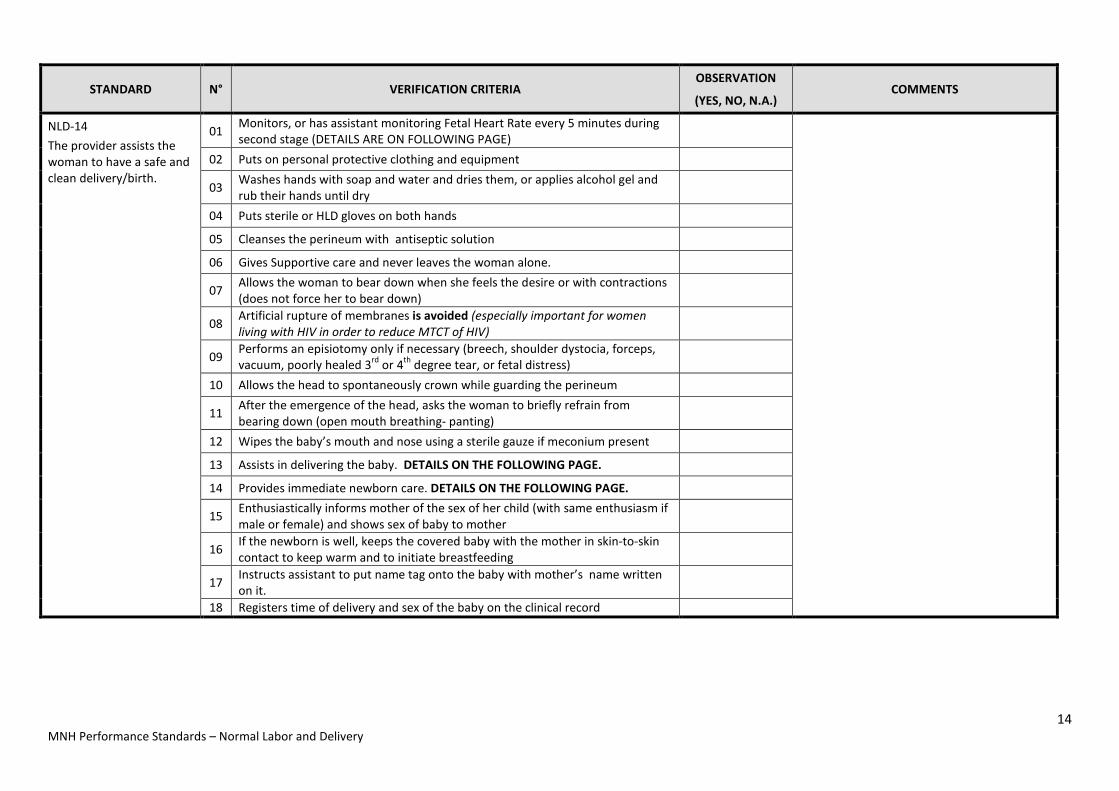
NLD-14 The provider assists the woman to have a safe and clean delivery/birth.
01 Monitors, or has assistant monitoring Fetal Heart Rate every 5 minutes during second stage (DETAILS ARE ON FOLLOWING PAGE)
02 Puts on personal protective clothing and equipment
03 Washes hands with soap and water and dries them, or applies alcohol gel and rub their hands until dry
04 Puts sterile or HLD gloves on both hands
05 Cleanses the perineum with antiseptic solution
06 Gives Supportive care and never leaves the woman alone.
07 Allows the woman to bear down when she feels the desire or with contractions (does not force her to bear down)
08 Artificial rupture of membranes is avoided (especially important for women living with HIV in order to reduce MTCT of HIV)
09 Performs an episiotomy only if necessary (breech, shoulder dystocia, forceps, vacuum, poorly healed 3rd or 4th degree tear, or fetal distress)
10 Allows the head to spontaneously crown while guarding the perineum
11 After the emergence of the head, asks the woman to briefly refrain from bearing down (open mouth breathing- panting)
12 Wipes the baby’s mouth and nose using a sterile gauze if meconium present
13 Assists in delivering the baby. DETAILS ON THE FOLLOWING PAGE.
14 Provides immediate newborn care. DETAILS ON THE FOLLOWING PAGE.
15 Enthusiastically informs mother of the sex of her child (with same enthusiasm if male or female) and shows sex of baby to mother
16 If the newborn is well, keeps the covered baby with the mother in skin-to-skin contact to keep warm and to initiate breastfeeding
17 Instructs assistant to put name tag onto the baby with mother’s name written on it.
18 Registers time of delivery and sex of the baby on the clinical record
14
MNH Performance Standards – Normal Labor and Delivery

• MONITOR Every 5 minutes : o For emergency signs, using rapid
assessment o Frequency, intensity and duration of
contractions o Fetal heart rate o Perineum thinning and bulging o Visible descent of fetal head or during
contraction o Mood and behaviour (distressed,
anxious) • Records findings regularly in Labour
record and Partograph
Delivering the baby; steps during the second stage • Quickly palpates to determine nuchal
cord; if it is loose, slide it over the baby’s head; if it is very tight, clamp it in two places and cut it before unraveling it from around the baby’s neck
• Allows spontaneous external rotation without manipulation if it happens quickly
• Carefully takes the baby’s head in both hands and applies downward traction until the anterior shoulder has emerged (no neck holding)
• Guides the baby’s head and chest upward until the posterior shoulder has emerged
• Holds the baby by the trunk and places it on a dry towel on the mother’s abdomen
• Dries baby gently, assesses the baby's breathing , removes wet towel
• Covers both the mother and infant with a dry, warm cloth or towel to prevent heat loss
• Covers the baby’s head with a cloth or, if available, a cap
Immediate newborn care
• When the baby is born, receives her in a clean, dry cloth. • Places the baby on the mother’s abdomen. • Thoroughly dries the baby and wipes each eye with a clean
part of cloth. • Removes the wet cloth • Places the baby in skin-to-skin contact with the mother to
maintain warmth • Covers the baby—including the head—with a clean, dry cloth
while keeping the face unobstructed • Assesses the baby’s breathing while drying the baby
o If the baby is not crying or breathing at least 30 times per minute within 30 seconds of birth, calls for help and begins resuscitation
o If the baby is breathing normally, continues with immediate care of the newborn
• If the mother is not able to hold the baby, asks her companion or an assistant to care for the baby. Otherwise, the baby should remain with the mother
15
MNH Performance Standards – Normal Labor and Delivery
STANDARD N° VERIFICATION CRITERIA OBSERVATION (YES, NO, N.A.) COMMENTS
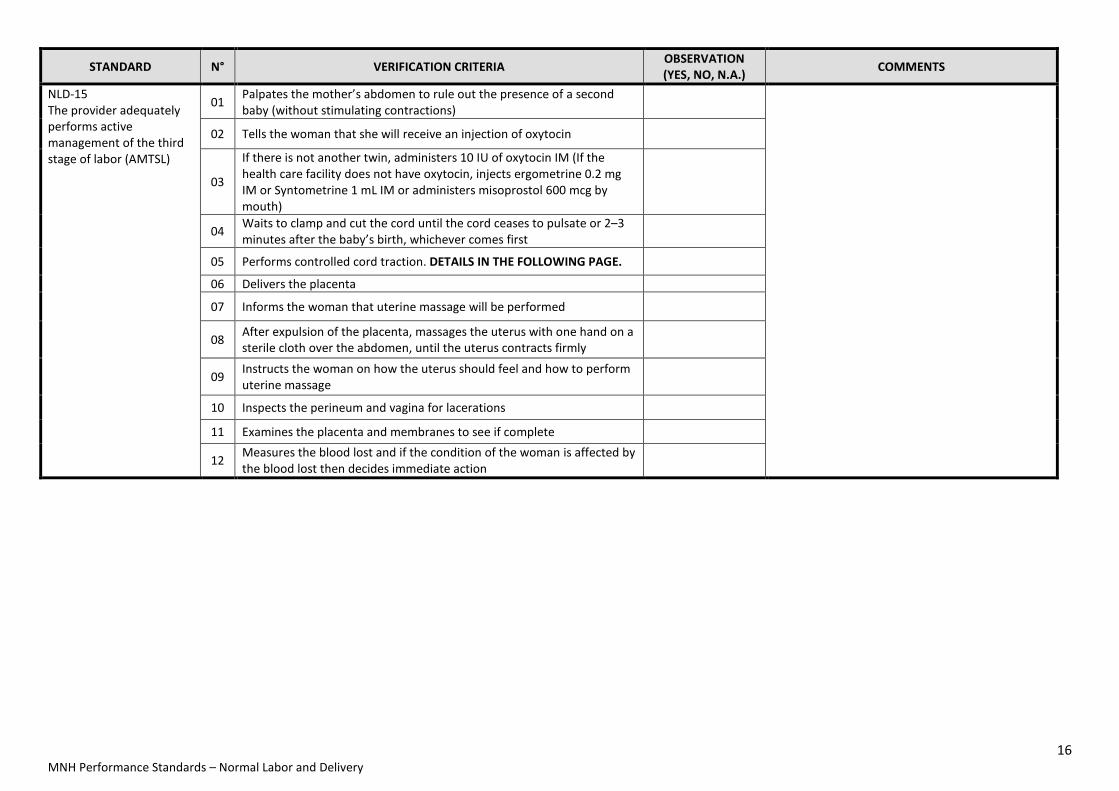
NLD-15 The provider adequately performs active management of the third stage of labor (AMTSL)
01 Palpates the mother’s abdomen to rule out the presence of a second baby (without stimulating contractions)
02 Tells the woman that she will receive an injection of oxytocin
03
If there is not another twin, administers 10 IU of oxytocin IM (If the health care facility does not have oxytocin, injects ergometrine 0.2 mg IM or Syntometrine 1 mL IM or administers misoprostol 600 mcg by mouth)
04 Waits to clamp and cut the cord until the cord ceases to pulsate or 2–3 minutes after the baby’s birth, whichever comes first
05 Performs controlled cord traction. DETAILS IN THE FOLLOWING PAGE.
06 Delivers the placenta
07 Informs the woman that uterine massage will be performed
08 After expulsion of the placenta, massages the uterus with one hand on a sterile cloth over the abdomen, until the uterus contracts firmly
09 Instructs the woman on how the uterus should feel and how to perform uterine massage
10 Inspects the perineum and vagina for lacerations
11 Examines the placenta and membranes to see if complete
12 Measures the blood lost and if the condition of the woman is affected by the blood lost then decides immediate action
16
MNH Performance Standards – Normal Labor and Delivery

Controlled cord traction (CCT)
• Place the clamp close to the woman’s perineum to make CCT easier.
• Keep slight tension on the cord and await a strong uterine contraction (2–3 minutes).
• When there is a uterine contraction, apply countertraction to the uterus with the hand above the pubic bone (apply pressure on the uterus in an upward direction—towards the woman’s head).
• While applying countertraction to the uterus, apply firm, steady traction to the cord, pulling downward on the cord following the direction of the birth canal.
• If the placenta does not descend during 30 to 40 seconds of controlled cord traction and there are no signs of placental separation), stop controlled cord traction.
• Gently hold the cord and wait until the uterus is well contracted again. If necessary, clamp the cord closer to the perineum as it lengthens.
• When there is another contraction, repeat steps 1 through 5
Delivery of the placenta
• As the placenta delivers, hold it in both hands and gently turn it until the membranes are twisted.
• Slowly and gently pull to complete the delivery. Move membranes up and down until they deliver.
• Place the placenta in the receptacle provided (for later examination)
Clamp and cut the cord
• Wait to clamp and cut the cord until the cord ceases to pulsate or 2–3 minutes after the baby’s birth, whichever comes first
NOTE: Refer to national protocols for cord cutting if the woman is infected with HIV
NOTE: Clamp and cut the cord immediately if the baby is not breathing
• Place one clamp 4 cm from the baby’s abdomen.
• Gently milk the cord towards the woman’s perineum and place a second clamp on the cord approximately 1 cm from the first clamp.
• Cut the cord using sterile scissors, covering the scissors with gauze to prevent blood spurts. Do NOT use the same scissors used for episiotomy.
• Tie the cord only after the provider performs AMTSL and completes initial care of the mother and baby
17
MNH Performance Standards – Normal Labor and Delivery

STANDARD N° VERIFICATION CRITERIA OBSERVATION (YES, NO, N.A.) COMMENTS
NLD-16 The provider adequately performs immediate postpartum care.
01 Informs the woman what she is going to do before proceeding, then carefully examines the vagina and perineum
02 Gently cleanses the vulva and perineum with clean, warm water or a nonalcoholic antiseptic solution
03 Sutures tears, if necessary 04 Covers the perineum with a clean sanitary pad 05 Makes sure that the woman is comfortable (clean, hydrated and warmly
covered)
06 Assist woman to empty her bladder 07 Keeps the woman in the delivery room for at least 1 hour after
childbirth; and does not discharge the woman and her newborn until at least 12 hours after childbirth
08 Informs woman of findings 09 Registers information in clinical record
NLD-17 The provider properly monitors the newborn and provides essential initial newborn care, and subsequent care.
01 Keeps the woman and her newborn together and never leaves them alone
02 Ensures that the baby is well covered, is with the mother and has began to suckle within one hour of birth
03 Provides routine essential care of the newborn. DETAILS IN THE FOLLOWING PAGE.
04 Ensures Baby is warm at all times. DETAILS IN THE FOLLOWING PAGE.
05 Monitors the baby closely during at least the first six hours after birth (at the same time as the postpartum woman is monitored) DETAILS IN THE FOLLOWING PAGE.
06 Supervises breastfeeding - baby attachment to breast
07 Assesses baby for any jaundice
08 Monitors and records passage of meconium and urine
09 Informs parents of findings
10 Gives the baby the appropriate immunizations and issues the appropriate under-five card
18
MNH Performance Standards – Normal Labor and Delivery

Essential Newborn Care • Cleanliness: Prevention of newborn infections
o Assures a clean delivery o Assures clean cord care o Assures clean hands (providers, mother, family
members) o Verifies maternal tetanus toxoid status
• Thermal protection o Warms room for delivery o Immediately dries the baby after birth o Avoids separating baby from mother whenever
possible o Facilitates skin-to-skin contact
• Early and exclusive breastfeeding o Facilitates initiation within one hour after birth o Counsels the mother about on demand feeding o Counsels the mother to avoid prelacteal feeds or other
fluids/food • Initiation of breathing, resuscitation
o Promptly recognizes and manages birth asphyxia • Eye care
o Cleans the eyes immediately after birth o Applies silver nitrate drops or antibiotic ointment
within the first hour of birth o Promptly diagnoses and manages ophthalmia
• Provides the following immunizations at birth: o OPV o BCG o Hepatitis B
• Administers Vitamin K • Prevention of maternal-to-child transmission of HIV
o Gives ARV drugs for prophylaxis to infant o Explains administration of ARV drugs to the mother and
family o Advises on early and exclusive breastfeeding o Counsels on use of condoms while breastfeeding
• Performs a comprehensive exam at 6 hours and before discharge
Monitoring the newborn Assess the baby in general when the mother is assessed: • immediately after birth then • every 15 minutes for 2 hours, then • every 30 minutes for 1 hour, then • every hour for the next 3 hours
o Respiration o Color o Temperature - touch the baby’s hands and feet
and check axillary temperature if they are cold o Umbilical cord for bleeding o Presence of other danger signs
Danger signs in the newborn • Rapid respirations (more than 60 respirations per
minute) • Slow respirations (less than 30 respirations per
minute) • Flaring of the nostrils • Grunting • Severe subcostal retractions • Poor sucking/not sucking • Cyanosis, especially of the lips and tongue (Cyanosis of
the hands and feet may also be due to hypothermia for which the baby needs to be warmed)
• Hypothermia: body feeling cold (temperature <36.5 °C)
• Fever: usually later in the postnatal period (temperature >37.5 °C)
• Convulsions • Umbilical cord bleeding usually in the first day or two;
needs retying of the cord; referral not required if that is the only sign
Procedure for warming up the baby • Verifies body temperature by checking
axillary temperature • Makes sure that baby is kept warm by
maintaining skin-to-skin contact • If skin-to-skin contact is not possible, re-
wraps the baby, including the head and places the baby under a heat source or incubator
• Continues to monitor temperature on an hourly basis or until temperature stabilizes
19
MNH Performance Standards – Normal Labor and Delivery

STANDARD N° VERIFICATION CRITERIA OBSERVATION
(YES, NO, N.A.) COMMENTS
NLD-18
The provider properly disposes of the used instruments and medical waste after assisting the birth.
01 Puts on gloves while disposing of used instruments and medical waste
02 Discards the placenta in a leak-proof container with a plastic liner
03 Disposes of medical waste (gauze, etc.) in a plastic container with a plastic liner.
04 Puts the soiled linen in a leak-proof container
05 Opens (un-hinges) all instruments and immerses them in a 0.5% chlorine solution for 10 minutes
06 Disposes of all sharps and syringes per national Infection Prevention guidelines. the sharps container
07 Removes and disposes of gloves and Performs hand hygiene after removing gloves according to Infection Prevention guidelines
NLD-19
The provider properly monitors the woman and provides essential initial and subsequent postpartum care.
01 Keeps the woman in the maternity ward to be closely monitored for at least two hours after the birth
02 Monitors specific indicators in the woman during at least the first six hours postpartum. DETAILS IN THE FOLLOWING PAGE.
03 Provides care and counsel for the woman after delivery and before discharge. DETAILS IN THE FOLLOWING PAGE.
05 Responds immediately if there are complications (see performance standards for EmOC)
06 Informs the woman of all findings
07 Records the information on the woman’s clinical record NLD - 20 The HF provides Family Planning care at the maternity ward during the immediate postpartum period.
01 Provides information for the women after delivery on family planning methods available that can be used during postpartum.
02 Support woman to choose a contraceptive method according her preference and clinical condition.
03 Provides specifics information related to the contraceptive method chosen.
04 Encourages client to ask questions and addresses them with an easy-to-understand language
05 Provides method of choice as appropriate
20
MNH Performance Standards – Normal Labor and Delivery

Care for the Woman after delivery of the placenta
• Ensures the woman has sanitary napkins or clean material to collect vaginal blood.
• Encourages the woman to eat, drink, and rest. • Encourages the woman to empty her bladder and ensure that she
has passed urine. • Asks the woman’s companion to watch her and call for help if
bleeding or pain increases, if the woman feels dizzy or has severe headaches, visual disturbance, or epigastric distress.
• Keeps the mother and baby together • Never leaves the woman and newborn alone. • Performs a comprehensive exam at 6 hours and before discharge • Counsels the woman on:
o Complication readiness plan (danger signs and how to respond)
o Hygiene o Breast care o Rest o Responsibilities when caring for a baby o Exercise o Nutrition o Resumption of sexual activity o Safer sexual practices (HIV positive and negative prevention) o Birth spacing o Postpartum contraception o Information on findings and plan of care o Routine care visits
• Provides preventive measures: o Iron-folate tablets o Vitamin A o Tetanus toxoid vaccination, if due o Mebendazole, if due o Paracetamol
• Provides counseling on LAM or provides the family planning method of the woman’s choice if not breastfeeding
• Documents all findings and care provided.
Monitoring the postpartum woman Assess the woman in general when the baby is assessed: Immediately after birth then every 15 minutes for 2 hours, then every 30 minutes for 1 hour, then every hour for the next 3 hours • Vital signs: o blood pressure o pulse
• Vaginal bleeding • Uterine hardness Every 4 hours • Temperature • Respiration Every hour • Bladder (help the woman empty her bladder
if it is distended) • Breastfeeding • Psychological reaction
Danger signs in the postpartum woman • Systolic BP ≤90; Diastolic BP ≤60 • vaginal bleeding:
o more than 2 or 3 pads soaked in 20-30 minutes after delivery OR
o bleeding increases rather than decreases after delivery.
• Convulsions • fast or difficult breathing • fever • too weak to get out of bed • abdominal pain • feels ill • urine dribbling or pain on micturition • pain in the perineum or draining pus • foul-smelling lochia
Additional care for postpartum women living with HIV • Determines how much the woman has told her partner and family and respects this
confidentiality. • Is sensitive to her special concerns and fears. Gives her additional support • Advises on the importance of good nutrition • Advises her that she is more prone to infections and should seek medical help as soon as
possible if she has signs / symptoms of an infection • Tells her that lochia can cause infection in other people and therefore she should dispose of
blood stained sanitary pads safely (list local options). • Counsels her on family planning • Counsels on ARV drug regimen • Explains the risks of HIV transmission during breastfeeding / mixed feeding • Counsels on importance of always using condoms • Advises her to visit HIV services 2 weeks after delivery for further assessment
MNH Performance Standards – Normal Labor and Delivery
21

TOTAL STANDARDS FOR NLD: 20
A. TOTAL STANDARDS OBSERVED:
B. TOTAL STANDARDS ACHIEVED:
C. PERCENTAGE OF ACHIEVEMENT: (A
B 100×)
MNH Performance Standards – Normal Labor and Delivery
22









![[SẢN] W4.3 - The partograph WHO 1993 - The Partograph Part II WHO 1993](https://img.dokumen.tips/doc/110x75/577cbcc01a28aba7118dc1c6/san-w43-the-partograph-who-1993-the-partograph-part-ii-who-1993-httpbsquochoaiga.jpg)



















