-
8/12/2019 Pelvic Ring Disruptions
1/8
Pelvic Ring Disruptions
Pelvic ring disruptions are a major cause of mortality and
morbidity inmultiply injured patients. Whereas fatalities result
from uncontrolledretroperitoneal hemorrhage and other associated
injuries, disabilitiessuch as low back pain, leg-length
discrepancies, dyspareunia,
diculties withchildbearing, and impotence are caused by the
anatomic disruption ofthe pelvic ring. Pelvic fractures can be
particularly lethal when theyoccur incombination with signicant
injuries to other major organ systems.!!"#ecause of the high force
necessary to disrupt the pelvic ring in youngpatients, itis not
surprising that up to $%& of these patients have
additionalmusculoskeletal injuries. 'ortality rates in the patient
with high-energypelvic ringinjuries are appro(imately !)& to
*)&. +hese deaths are generally a
result of the injuries commonly associated with this injury
pattern.'ortalityincreases nearly ! times when the patient presents
with hypotension.When combined with either a head or an abdominal
injury that reuiressurgicalintervention, the mortality increases to
)%&. When both proceduresare necessary, mortality increases to
%&.Classifcation
/rthopedic surgeons and traumatologists broadly classify pelvic
ringdisruptions into two major groups0 stable and unstable. 1
stable pelvisis denedas one that can withstand normal physiologic
forces without displacing.+his stability depends on the integrity
of bony and ligamentousstructures 2 3ig.*!4 5. Instability is
generally divided into rotational and verticalcomponents 2 3ig.
*!4!% 5. +hese displacements can be appreciated onthe
initialanteroposterior screening radiograph. 6table injuries
includenondisplaced fractures of the pelvic ring and anterior
displacements ofless than *.) cm.7otational instability is
characteri8ed by widening of the symphysispubis or displacement of
pubic rami fractures of greater than *.) cm.6uperiortranslation of
a hemipelvis through fractures of the sacrum or ilium anddisruption
of the sacroiliac joint by more than ! cm constitute
verticalinstability. 6erial sectioning studies reveal that division
of thesymphyseal ligaments alone leads to diastasis of *.) cm or
less,maintaining stability.!*"
-
8/12/2019 Pelvic Ring Disruptions
2/8
3urther sectioning of the anterior sacroiliac ligaments and
sacrospinousand sacrotuberous ligaments 2pelvic 9oor5 permits
rotational instability.:erticalinstability results only after the
posterior sacroiliac ligaments are alsosectioned. ;isplaced
fractures 2superior and inferior pubic rami
fractures, sacral oriliac wing fracture5 can also result in
similar instability patterns.#ecause the pelvis is a true ring
structure, a signicant anteriordisplacement must beaccompanied by a
corresponding posterior disruption. ;isruptions inthe pelvic ring
are usually a combination of fractures and ligamentousinjuries.n
%& of cases, this is sucient to assess stability and guide
initialtreatment.1nterior injuries are easily identied on this
projection. 'ost unstableposterior injuries can also be
appreciated. 1vulsion fractures at the =)transverseprocess and the
ischial spines indicate ligamentous disruption and areusually
identiable. =arge posterior gapping or displacement of the
hemipelvissuperiorly by more than ! cm indicates complete
posterior disruptionand instability.!*";etailed classication
systems have been developed based on thedirection of force,
stability of the pelvis, location of fracture, or whetherit is an
openor closed injury. +he ?omprehensive Pelvic ;isruption
classication ofthe 1rbeitsgemeinschaft fur /steosynthesefragen 21/5
combines the
-
8/12/2019 Pelvic Ring Disruptions
3/8
mechanism of injury with the degree of pelvic instability. +ype
1 injuriespreserve the integrity of the posterior ligamentous and
bonystructures. +heseinjuries maintain a stable pelvic ring and
usually reuire no furthertreatment unless neurologic injury is
associated with a sacral fracture.
+ype #injuries represent incomplete disruption of the posterior
pelvis. +heseinjuries result in rotational instability of the
pelvis. 1 varying degree ofsacroiliacjoint or sacral disruption is
characteristic. +hese injuries occur withboth anterior and lateral
compression mechanisms. >n type ? pelvicinjuries, thehemipelvis
is vertically, rotationally, and posteriorly unstable.=ateral
compression as well as vertical shear-type fractures areassociated
with intra-abdominal and head injuries. +he most commoncause of
death in a
lateral compression injury to the pelvis is associated closed
headtrauma."+he anteroposterior compression-type injuries have
thegreatest risk forretroperitoneal hemorrhage. >ntrapelvic
visceral injuries are also morecommon in the anteroposterior
patterns. 'ortality in anteroposteriorcompression-type injuries
relates to a combination of retroperitonealbleeding and visceral
injuries."547
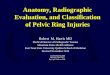
Figure 21-9 Pelvic stability. A,+he intact ligamentous bony
structures of the pelvismaintain its integrity with regard to
stability. +he posterior hinge, consisting of
theposteriorsacroiliac ligaments and the iliolumbar ligaments, is
imperative to maintain vertical
stability. +he sacrospinous prevents rotation, and the
sacrotuberous prevents verticalmigration. 1slong as these, the
anterior sacroiliac, and the symphysis are intact, the pelvis
willremain stable. >f, however, the anterior symphysis is
separated or the sacrum iscrushed posteriorly,as seen in B and C,
the posterior hinge remains intact and the pelvis is usually
stablevertically. +he sacrospinous ligaments are intact, and
rotatory abnormalities are thusprevented.(A to C, From Kellam JF,
Mayo K: Pelvic ring disruptions. In Browner B, Jupiter !B,"evine
#M, !ra$ton P% &eds': )eletal !rauma, *rd ed. P+iladelp+ia, B
aunders,-*./e!orr"age in Pelvic Fracture
+he usual cause of hemorrhage in pelvic fractures is from the
posterior
pelvic venous ple(us and bleeding cancellous bone surfaces.
7arely, inless than!%& of cases, it may be caused by bleeding
from a named artery 2 3ig.*!4!! 5.!" !@" !)" #leeding from a larger
artery is even less freuent. +wolargeseries!A" demonstrated rates
of bleeding from femoral or iliac vessels in!& and %& of
patients. >n light of these studies, initial treatmentshould
focus on
-
8/12/2019 Pelvic Ring Disruptions
4/8
the control of venous bleeding. 7eduction and stabili8ation of
thedisplaced pelvic ring help achieve this. 7eduction leads to a
decreasein pelvic volumeand tamponade of the bleeding vessels
through compression of theviscera and pelvic hematoma.
6tabili8ation maintains the reduction
and avoidsmovement of the hemipelvis, reducing pain and limiting
the disruptionof organi8ing clots. 6ince reduction and
stabili8ation alone usuallycontrolvenous bleeding, patients who do
not respond to these maneuvers aremore likely to have arterial
bleeding.#ta$ili%ation
7eduction and stabili8ation of the pelvis can be achieved by a
varietyof mechanical means 2 3ig. *!4!* 5. When eld personnel
detectunstable pelvicring disruptions on physical e(amination, they
can begin treatment bybinding the pelvis with a rolled sheet or
applying pneumatic antishockgarments2P16Bs5. =ike the air splints
applied to the e(tremities, the garmentfunctions by compressing the
pelvis. >f applied in the eld, P16Bsshould not bede9ated until
the patient is actively being resuscitated in the traumaroom. +he
P16B has as its advantages ease of use, application in theeld,
andreusability. Cowever, it blocks access to the patient and
restrictse(cursion of the diaphragm, and there have been reports of
glutealand thighcompartment syndromes developing after its e(tended
use inhypotensive patients.+he standard method for controlling
pelvic hemorrhage has been theapplication of an anterior e(ternal
(ation frame. Proper application ofan anteriorpelvic54&
Figure 21-1' A, ;ivision of the symphysis pubis will allow the
pelvis to open toappro(imately *.) cm with no damage to any
posterior ligamentous structures. B,;ivision of theanterior
sacroiliac and sacrospinous ligaments, either by direct division of
their bers2rig+t5 or by avulsion of the tip of the ischial spine
2le$t5, allows the pelvis to rotatee(ternally
until the posterior superior iliac spines abut the sacrum. Dote,
however, that theposterior ligamentous structures 2e.g., the
posterior sacroiliac and iliolumbarligaments5 remain intact.
+herefore, no displacement in the vertical plane is possible. C,
;ivision of theposterior tension band ligaments, that is, the
posterior sacroiliac, as well as theiliolumbar, depicted hereon the
left side, plus an avulsion of the transverse process of =) causes
completeinstability of the hemipelvis. Dote that posterior
displacement is now possible. (A toC, From Kellam
-
8/12/2019 Pelvic Ring Disruptions
5/8
JF, Mayo K: Pelvic ring disruptions. In Browner B, Jupiter !B,
"evine #M, !ra$ton P%&eds': )eletal !rauma, *rd ed.
P+iladelp+ia, B aunders, -*./Figure 21-11 >nternal aspect of the
pelvis shows the great vessels in thelumbosacral ple(us as well as
the pelvic 9oor and the pelvic contents, bladder, andrectum. (From
Kellam JF,Mayo K. Pelvic ring disruptions. In Browner B, Jupiter
!B, "evine #M, !ra$ton P%
&eds': )eletal !rauma, *rd ed. P+iladelp+ia, B aunders,
-*./549Figure 21-12 1lgorithm of pelvic fracture management. ?+,
computed tomographyE.3., open reduction and internal
(ationE6l,sacroiliac. (From Kellam JF, Mayo K: Pelvic ring
disruptions. In Browner B, Jupiter !B,"evine #M, !ra$ton P%
&eds': )eletal !rauma, *rd ed. P+iladelp+ia, B aunders,-*./
e(ternal (ator should provide stability to the pelvis and
hematoma,while allowing access to the abdomen for surgical
procedures. 'ultiplestudieshave shown that outcomes can improve
with their routine use.!@" !)" !G"1lthough this device can be
applied in the emergency department, it is
freuentlydeferred until the patient is brought to the operating
suite. >n thesecircumstances, the pelvis can remain displaced
for many hours withvenous bleedingcontinuing uncontrolled. >f an
e(ternal (ator cannot be appliede(peditiously, another method of
provisional stabili8ation must beemployed. 7ecently,devices called
pelvic ?-clamps have been developed that can berapidly applied to
reduce and provisionally stabili8e the pelvis in
theemergencydepartment. +he design allows for compression of the
pelvis throughpercutaneously inserted pins applied to the outer
surface of the ilium.+hey provideadeuate stabili8ation and easy
access to the abdomen or e(tremitieswithout removal of the device 2
3ig. *!4! 5. +he ?-clamps can remainin placethroughout the
resuscitation phase and then be replaced by denitivestabili8ation
methods when the patient is able to undergo theseprocedures.
?aremust be taken in the55'
Figure 21-1( Pelvic ring disruption with massive hemorrhage. A,
1nteroposterior
21P5 radiograph of the pelvis shows disruption of the symphysis
pubis and thesacroiliac joint. B,1P view of the pelvis following
reduction by application of the pelvic stabili8er. C andD, Patient
with the pelvic stabili8er in the standard position and elevated to
allowaccess to theperineum or the hips to be 9e(ed into the
lithotomy position.
application of these clamps because serious complications can
resultfrom misplacement of the pins. 1ccordingly, these devices are
utili8edonly in
-
8/12/2019 Pelvic Ring Disruptions
6/8
rotationally and vertically unstable pelvic ring disruptions and
not instable injury patterns.+he role of angiography in the
diagnosis and management of pelvichemorrhage is controversial.
=arge series have demonstrated theincidence of
arterial hemorrhage amenable to emboli8ation to be
appro(imately!%&.!" !@" 3urthermore, it is even less common for
the bleeding to bethe result of aninjury to a large or named
artery. >n these cases, arteriography withemboli8ation can be
lifesaving. Cowever, catheteri8ation andemboli8ation ofvessels in
the pelvis are technically dicult and time consuming. +heuse of
these techniues should be reserved for those cases when allother
methodsof control of hemorrhage have been e(hausted.!")anage!ent
Algorit"!s
1lgorithms for management of the hypotensive patient with a
pelvicfracture all should begin with a search for the cause of the
shock 2 3ig.*!4!@ 5. 1llpossible causes of bleeding are e(plored.
1uscultation of the chest andreview of the chest radiograph
determine the presence of hemothora(and theneed for thoracostomy.
/nce the hemothora( is either ruled out as acause of shock or is
controlled by chest tubes, a diagnostic peritoneallavage
orultrasound of the abdomen is performed.
-
8/12/2019 Pelvic Ring Disruptions
7/8
=ong-term, denitive care of pelvic ring disruption is dependent
on theseverity and the pattern of injury. 6table fractures or
injury patternsusuallyreuire no more than restricted weight
bearing. 3or the reasonsdescribed previously, unstable injuries
often need to be denitively
(ed. 3reuently,the e(ternal (ator can provide denitive
stabili8ation, if appliedeIectively and reduction has been
maintained. >n cases when the(ator may beobstructing access to
the abdomen or an interim ?-clamp has beenapplied, /7>3 or
closed reduction and percutaneous (ation may beindicated.
Whenrotational or vertical instability is present, both the
anterior and theposterior pelvis must be stabili8ed. 1nteriorly,
the symphysis is oftensecured with aplate and screws. Posteriorly,
more options e(ist. +he sacroiliac joint or
sacral fractures can be secured with plates, bars, or
percutaneouslyinsertedcannulated screws 2 3ig. *!4!) 5.
Pelvic 3ractures>njuries to the pelvic ring should be
diIerentiated between the low-energy,stable fractures and the
high-energy, life-threatening injuries. +he former arecommonly seen
in older adult osteoporotic patients who may have sustainedisolated
fractures of the pubic rami or nondisplaced fractures of the
acetabulior sacrum from a fall. +hese fractures usually do not have
disruption of thepelvic ring or weight-bearing segments and are
considered stable.
Cigh-energy injuries are the result of automobile collisions,
pedestriansand cyclists being struck by motor vehicles, or falls
from signicant heights.!!@A PAR* ++ #PC+F+C C.#+DRA*+.#+hese
injuries are caused by direct crush, either from the anterior or
lateraldirection or vertical shear, or combinations of rotational
stress on the iliacwings. >nitial evaluation of pelvic injuries
includes an 1P radiograph. 3urtherimaging includes inlet and outlet
views. 1ssociated acetabular fracturesand lumbar spine injuries
reuire @)-degree obliue 2Judet5 views and 1Pand lateral radiographs
of the lumbosacral spine. 'ost pelvic injuries willalso need a ?+
scan with -mm cuts to evaluate a posterior injury to thepelvis. 1
?+ scan is best used for evaluation of the sacrum and
sacroiliacjoints.?ontinued, une(plained blood loss despite fracture
stabili8ation and aggressiveresuscitation is an indication for
angiography.
-
8/12/2019 Pelvic Ring Disruptions
8/8
the presence of intraarticular bony fragments. Dondisplaced or
minimallydisplaced fractures are determined after complete
evaluation of theradiographs and acetabular ?+ scans. 7adiographs
should be taken withtraction removed and preferably with stress
applied. 1ny degree of incongruenceinvolving the weight-bearing
surface of the acetabulum is unacceptableand is an indication for
surgical treatment. Dondisplaced fracturesmay be treated with a
period of traction followed by progressive weightbearing.Cip
;islocation;islocation of the hip often is caused by a force
applied to the femur andcan be associated with fractures of the
acetabulum or femoral head. +he mostcommon mechanism of injury is
motor vehicles accidents. 3orce applied toan abducted hip can
result in anterior dislocation, although striking the kneeon a car
dashboard with the hip 9e(ed and adducted, results in posterior
dislocations.Posterior dislocations often are associated with a
fracture of theposterior wall of the acetabulum. ;irect trauma to
the greater trochanter froma lateral direction can result in medial
wall fractures or central acetabularfracturesHdislocations.+horough
evaluation of hip dislocations often reuires Judet
radiographicviews and additional ?+ scans. 6imilar to patients with
pelvic fractures, thesepatients may have other major injuries and
careful evaluation of the chest,abdomen, spine, and neurologic
status is necessary. Prompt reduction of hipdislocations is
essential in minimi8ing the incidence of osteonecrosis of the
femoral head.