Embed Size (px)
Citation preview

Pediatric Adjusting
Normal Pediatric Variants… Considerations for Pediatric Adjusting Underdeveloped cervical lordosis Low vertebral height Horizontal facets (until age 10) Undeveloped uncinates (until age 7) Spine is flexible
Cartilage, ligaments are more elastic, discs are expansile
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002. & Lustrin ES, Karakas SP, Ortiz AO et al. Pediatric Cervical Spine: Normal Anatomy, Variants and Trauma. RadioGraphics 2003; 23:539-60.
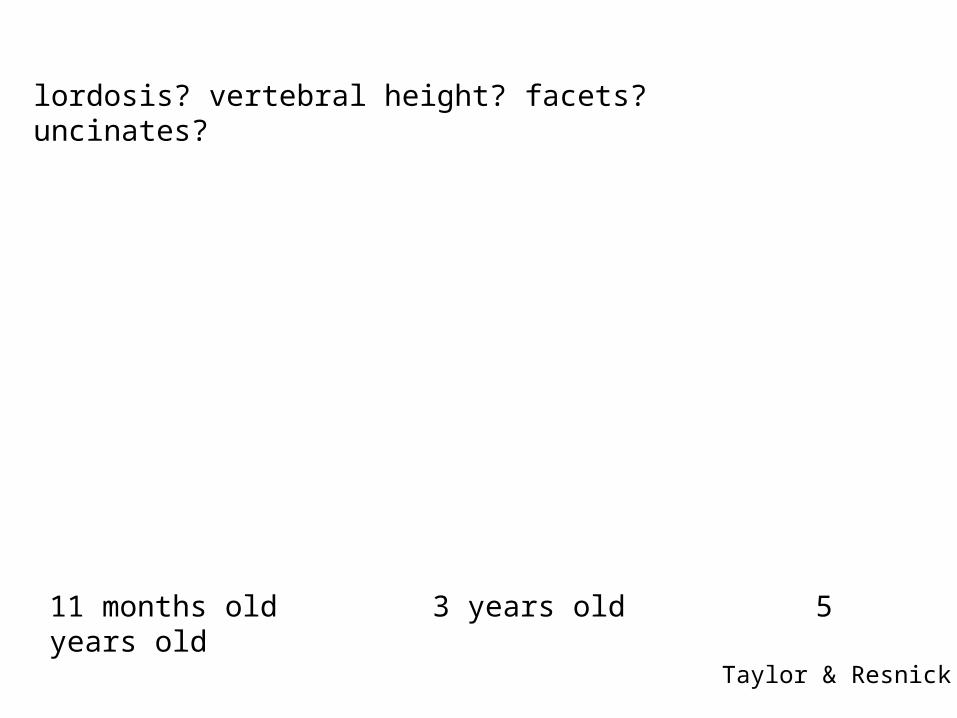
11 months old 3 years old 5 years old
Taylor & Resnick
lordosis? vertebral height? facets? uncinates?
Considerations & Adaptations Minimize excessive range of motion & forces
C-spine: minimum rotation Reduce depth of thrust
*Sometimes, pre-stress can effect a correction...
Pediatric vertebrae are much smaller cervical spine of a newborn is <2 inches in length
High degree of specificity is required Contact points: pad of the finger-tip or thumb tip
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
Clues in the History
A 2 day old whose proud parents report, “He‘s so strong, he can hold his head up already...”
Mother tells you, “He won‘t cuddle like other babies.“ pulls away when held against your shoulder only comfortable in the “football hold”
Problems breastfeeding, diaper habits, sleeping, etc. can all be signs of subluxation!

Occiput
Findings Fixation between Co/C1* Increased tension in suboccipital muscles
unilateral/bilateral
*If significantly fixed, infant may become irritable even with light palpation
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
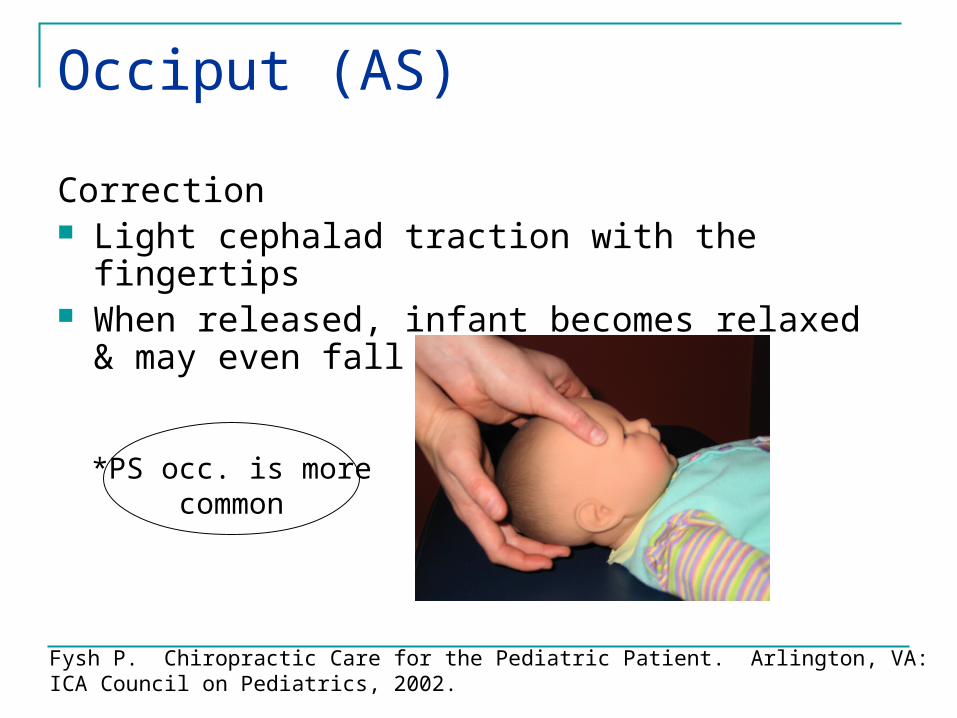
Occiput (AS)
Correction Light cephalad traction with the fingertips When released, infant becomes relaxed & may even
fall asleep
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
*PS occ. is more common

Atlas
Findings Fixation at C1
We’ll add… T&T Instrumentation Etc.
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
Palpate atlas laterality seated/upright…

Atlas
Correction Place lateral tip of the index finger against the
prominent C1 transverse Laterally bend to the side of contact until end-range A quick, light, low-amplitude thrust is delivered to the
tip of the C1 transverse toward the neutral position
*Not uncommon for a young baby to cry 15-20 seconds (stimulates the Moro response)
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.

C2 – C7
Findings Muscle spasm – usually side of spinous process
deviation Fixation – spinous does not move away with lateral
bend
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.

C2 – C7
Correction Tip of index finger on articular pillar Rotate head 25-30 degrees Laterally bend the neck over contact finger If no release is felt, apply a light thrust
Remember the joints of Lushka only begin to develop between 6-9 years of age…
Without coupled motion, this may be a way to limit excessive rotation when adjusting infants and young children.
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
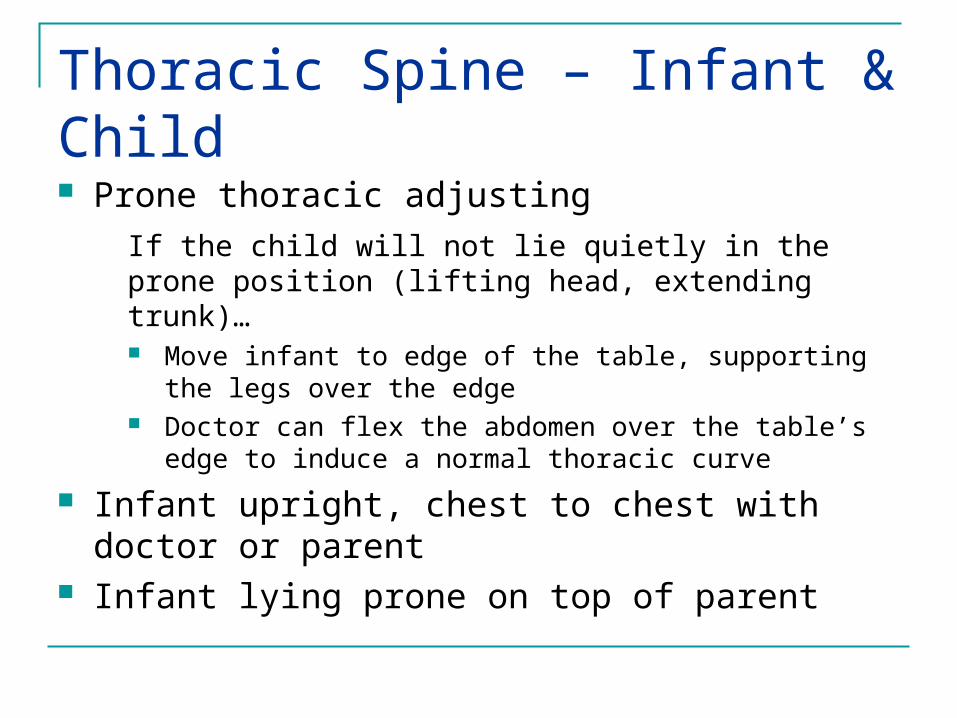
Thoracic Spine – Infant & Child Prone thoracic adjusting
If the child will not lie quietly in the prone position (lifting head, extending trunk)… Move infant to edge of the table, supporting the legs over the
edge Doctor can flex the abdomen over the table’s edge to induce a
normal thoracic curve
Infant upright, chest to chest with doctor or parent Infant lying prone on top of parent

Thoracics
Correction DTH - thumbs on either side of the spinous process
Anterior adjusting Not recommended for children under 3 years of
age Flexible rib cage
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
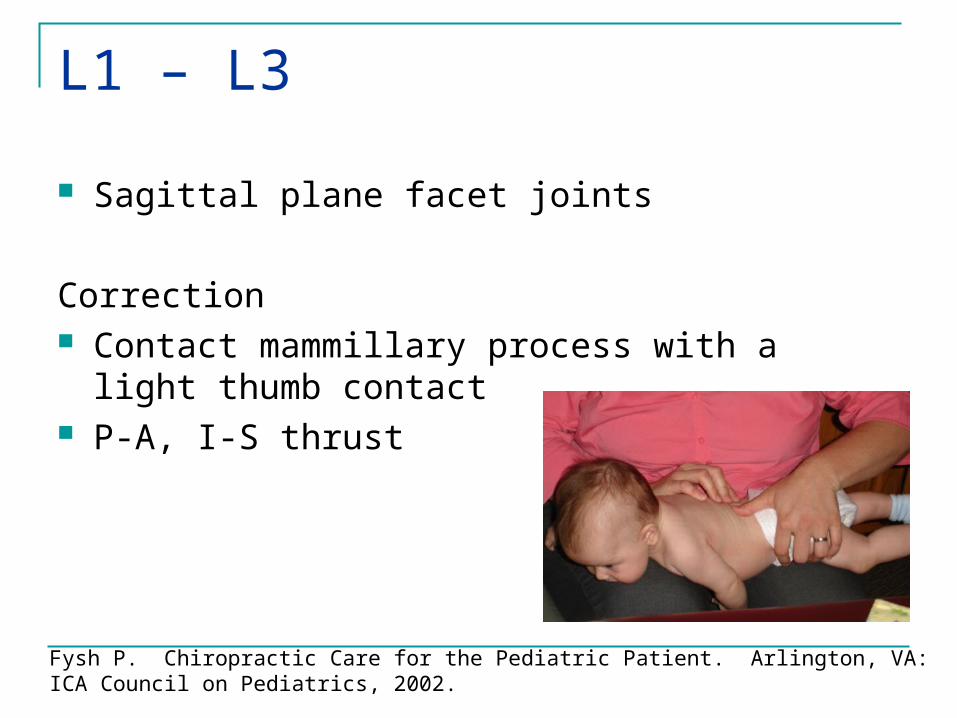
L1 – L3
Sagittal plane facet joints
Correction Contact mammillary process with a light thumb
contact P-A, I-S thrust
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.

L4 – L5
Correction Contact the spinous process (side of spinous
rotation) with a light thumb contact Apply light pressure over the contralateral
mammilary process (stabilization) Thrust toward the spinous process
*Side Posture: reserved for children >1 year
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
Sacro-iliacGluteal Cleft Deviation Pinch gluteal cheeks together, cleft should be midline If it deviates...
may either be to the side of posterior-inferior sacroiliac subluxation (P-R, PI-R, P-L, PI-L) or to the side of anterior-inferior sacral movement at the lumbosacral junction
Other things to note... Hold infant upright, legs dangling
ilium rotation Gluteal fold observation
sacral tiltsFysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.

Sacro-iliac
Correction Prone or side posture
Light adjustive thrust
Direction appropriate to correct PI, AS, In or Ex
Fysh P. Chiropractic Care for the Pediatric Patient. Arlington, VA: ICA Council on Pediatrics, 2002.
Motion palpation Can be a challenge, be creative Similar to adults but more subtle (smaller, squirming, etc.)
Leg checks Must consider variable growth rates in long bones Make sure other findings match
Pay attention to the child… Squirming, fussiness, clutching at your hand, etc.
Tips For SuccessJust because it sticks
out doesn‘t mean it‘s subluxated!

Chiropractic Activator Buddy
eBay

Pediatric Drop Piece

Pediatric Chiropractic Reference Texts Anrig & Plaugher. Pediatric Chiropractic. Baltimore, MD: Lippincott
Williams & Wilkins, 1998. Davies NJ. Chiropractic Pediatrics. London: Churchill Livingstone,
2000. Fysh. Chiropractic Care for the Pediatric Patient. Arlington VA:
ICACCP, 2002.
Current Chiropractic Research…
Asthma Colic Enuresis LBP
Otitis HeadacheSIDS Autism

Chiropractic and Asthma
Gibbs AL. Chiropractic co-management of medically treated asthma. Clin Chiropr: SEP 2005(8:3) 140-144.
Ressel O, Rudy R. Vertebral subluxation correlated with somatic, visceral and immune complaints: an analysis of 650 children under chiropractic care. J Vert Sublux Res: 2004 (OCT:18) Online access only 23p.
Schetchikova NV. Asthma: An Enigma Epidemic (Part 1). J Am Chiropr Assoc: June 2003 (40:6) 22-29.
Schetchikova NV. Asthma: An Enigma Epidemic , Part II-Asthma Treatment. J Am Chiropr Assoc: JUL 2003 (40:7) 30-37.
Blum CL. Role of chiropractic and sacro- occipital technique in asthma treatment. J Chiropr Med: MAR 2002(1:1) 16-22.
Clinical Trial: Asthmatics and Chiropractic. J Am Chiropr Assoc: FEB 2001 (38:2)46-47.
Wellness Alert: Hold Your Breath. J Am Chiropr Assoc: MAR 2001(38:3) 30-38.
Chiropractic and Colic
Miller J, Croci SC. Cry baby, why baby? Beyond colic: Is it time to widen our views? J Clin Chiropr Pediatr: 2005(6:3) 419-423.
Hipperson AJ. Chiropractic management of infantile colic. Clin Chiropr: DEC 2004 (7:4) 180-186.
Hewitt EG. Chiropractic care and the irritable infant. J Clin Chiropr Pediatr: SUM 2004(6:2) 394-397.
Leach RA. Differential compliance instrument in the treatment of infantile colic: a report of two cases. J Manipulative Physiol Ther:JAN 2002(25:1) 58-62.
Nilsson N, Wiberg JMM. Infants with colic may have had a faster delivery: a short preliminary report. J Manipulative Physiol Ther:MAR/APR 2000(23:3) 208-210.
Working with young patients. J Am Chiropr Assoc:FEB 1999 (36:2) 12-15.

Chiropractic and Enuresis
McCormick J. Improvement in nocturnal enuresis with chiropractic care: A case study. J Clin Chiropr Pediatr:2006(7:1) 464-465.
Bachman TR, Lantz CA. Management of pediatric asthma and enuresis with probable traumatic etiology. ICA Rev: JAN/FEB 1995(51:1) 44-46.
Marko RB. Bed-Wetting: Two case studies. Chiropr Pediatr: APR 1994(1:1) 21-22.
Langely C. Epileptic seizures, nocturnal enuresis, ADD. Chiropr Pediatr: APR 1994 (1:1) 22.
Bomerth PR. Functional nocturnal enuresis. J Manipulative Physiol Ther:NOV/DEC 1994(17:9) 596-600.
Aker PD, Kreitz BG. Nocturnal Enuresis: Treatment implications for the chiropractor. J Manipulative Physiol Ther: SEP 1994(17:7) 465-473.

Chiropractic and Otitis
Saunders L. Chiropractic treatment of otitis media with effusion: a case report and literature review of the epidemiological risk factors towards the condition and that influence the outcome of chiropractic treatment. Clin Chiropr: DEC 2004(7:4)168-173.
Nelson-Hassel T. Pediatric Cephalgia. J Clin Chiropr Pediatr: SUM 2004(6:2) 383-386.
Chiropractic Approach to the Ear. J Am Chiropractic Assoc: AUG 2002 (39:8) 12-14+.
Chiropractic for Infants and Children. J Am Chiropractic Assoc: FEB 1999(36:2) 7-8.
Boline PD, Evans RL, Sawyer CE. A feasibility study of chiropractic spinal manipulation versus sham spinal manipulation for chronic otitis media with effusion in children. J Manipulative Physiol Ther: JUN 1999(22:5) 292-298.
Canty A. A Mother’s Perspective. J Clin Chiropr Pediatr: AUG 1998 (3:1) 201.
Chiropractic and SIDS
Dvorak D. Sudden Infant Death Syndrome. Chiropr Pediatr: JAN 1997(2:4) 10-11.
Burns RE, Schneier M. Atlanto-occipital hypermobility in sudden infant death syndrome. Chiropr: JUL 1991(7:2) 33-38.
Bonci AS, Wynne CD. The interface between sudden infant death syndrome and chiropractic. J Chiropr Res: SPR 1989(5:3) 78-80.
Banks BD, Beck RW, Columbus M. Sudden infant death syndrome: A literature review with chiropractic implications. J Manipulative Physiol Ther: OCT 1987(10:5) 246-52.





























