Embed Size (px)
Citation preview

PD MASTERCLASS 2018INCREMENTAL DIALYSIS PRESCRIPTION–DOING IT RIGHT
DR ESTHER TAN ZHAO ZHI
11:00-11:30AM
7TH OCTOBER 2018
LE MERIDIEN PUTRAJAYA

OUTLINE
• PD Adequacy
•What is Incremental PD - Definition
•Why Incremental PD – benefits and drawbacks
•Who is a candidate for Incremental PD
• How to prescribe Incremental PD
• Strategies to improve success for Incremental PD

BROAD VIEW OF DIALYSIS ADEQUACY
Anemia management
Good nutrition
BP control
Adequate solute
removal
Fluid and electrolytes hemostasis
BMDmanagement
Dialysisadequacy

BROAD VIEW OF DIALYSIS ADEQUACY
Anemia management
Good nutrition
BP control
Adequate solute
removal
Fluid and electrolytes hemostasis
BMDmanagement
Dialysisadequacy
Kt/v

PD ADEQUACY
• Incremental peritoneal dialysis refers to the practice of starting peritoneal dialysis at a lower dose than is typically prescribed for someone without residual renal function (RRF).
• As the RRF declines, the dose is gradually increased.
Auguste BL, Bargman JM. Incremental peritoneal dialysis: New ideas about an old Approach. Seminars in Dialysis. 2018;1–4
Total solute clearance = Peritoneal/Dialysis Clearance + Residual Renal Function Clearance

Auguste BL, Bargman JM. Incremental peritoneal dialysis: New ideas about an old Approach. Seminars in Dialysis. 2018;1–4
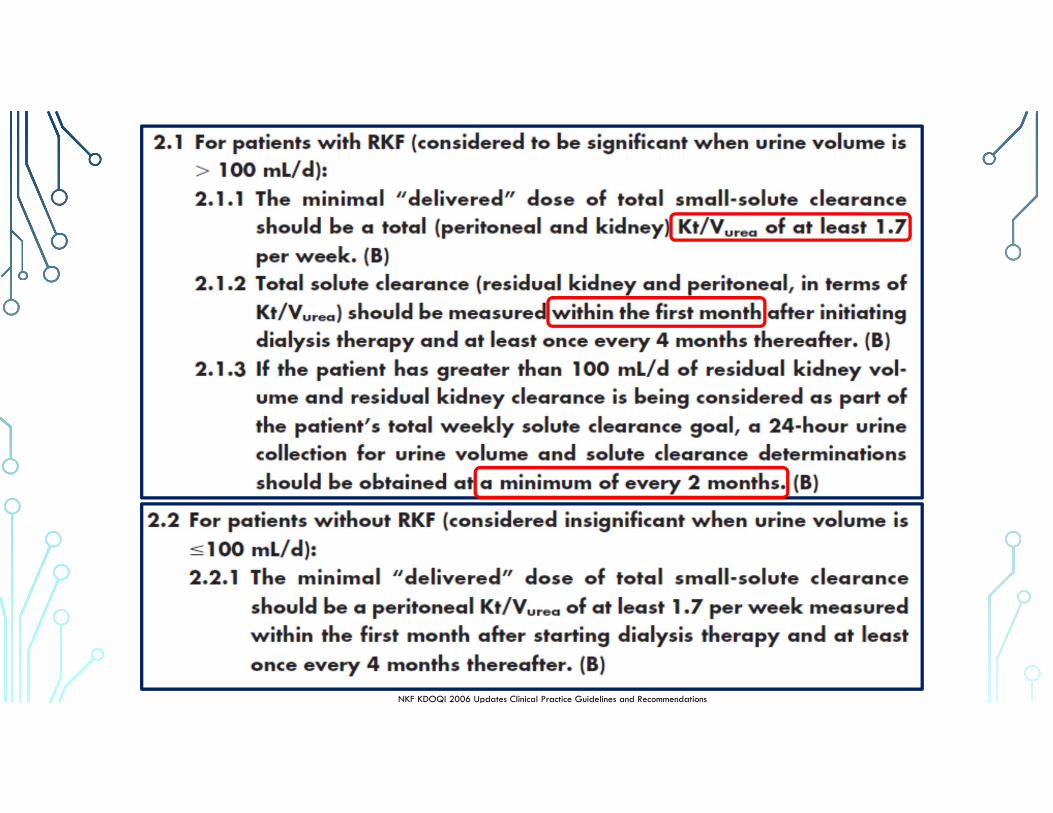
NKF KDOQI 2006 Updates Clinical Practice Guidelines and Recommendations

FULL DOSE PERITONEAL DIALYSIS
• “Full-Dose PD” was defined as :
• CAPD with at least 8 L daily or
• APD with a cycler treatment every night and with at least 1 day dwell each day.
• It is recognized that standard PD prescriptions may differ between countries.
• These “Full-Dose PD” patients can be subdivided into those who achieve the Kt/V target with peritoneal Kt/V alone and those who achieve it through a combination of both peritoneal and residual renal clearance.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016
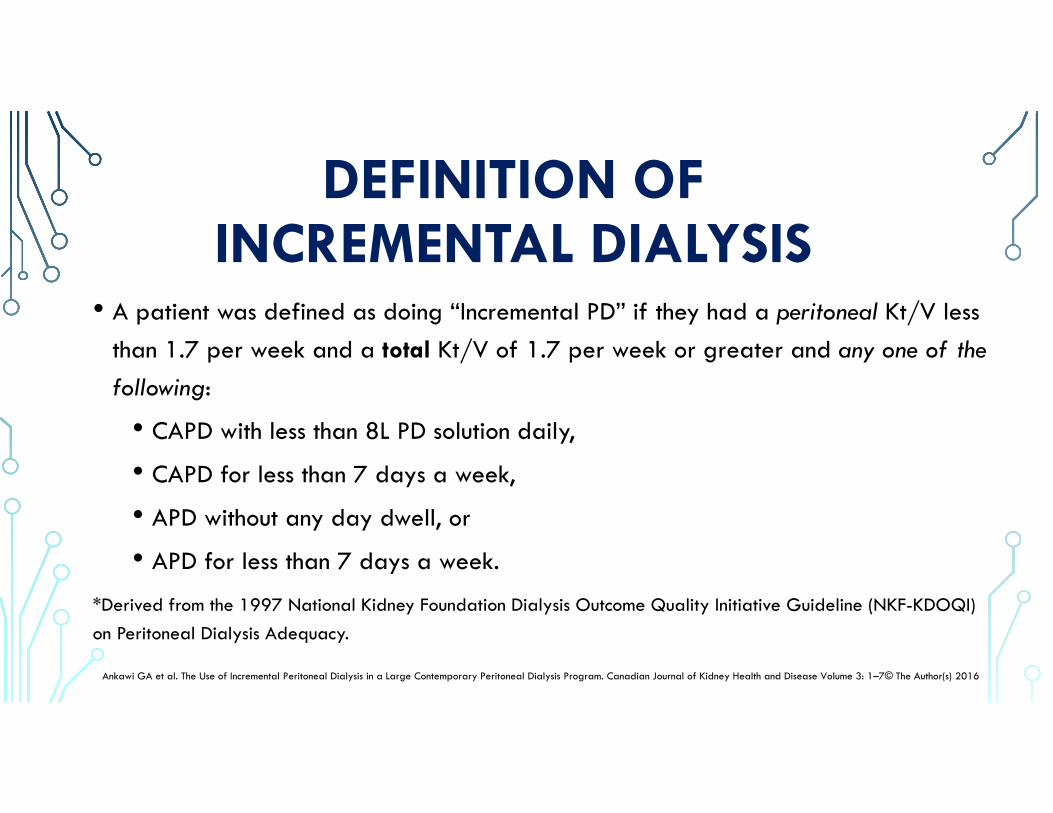
DEFINITION OF INCREMENTAL DIALYSIS
• A patient was defined as doing “Incremental PD” if they had a peritoneal Kt/V less than 1.7 per week and a total Kt/V of 1.7 per week or greater and any one of the following:
• CAPD with less than 8L PD solution daily,
• CAPD for less than 7 days a week,
• APD without any day dwell, or
• APD for less than 7 days a week.
*Derived from the 1997 National Kidney Foundation Dialysis Outcome Quality Initiative Guideline (NKF-KDOQI) on Peritoneal Dialysis Adequacy.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016

• The rationale for incremental PD rests on deductions from a number of well-proven premises. • First, it has been well shown that (within the usual therapeutic range), higher
peritoneal clearances are not associated with improved outcomes.
• Second, renal clearance is associated with superior outcomes in a way that equivalent amounts of peritoneal clearance are not.
• Hence, if 2 patients have the same total clearance but one derives it from a mix of renal and peritoneal clearance while the other has it from peritoneal clearance alone, the former has been associated with better survival.
• A patient receiving incremental PD is therefore unlikely to be disadvantaged.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016

BENEFITS OF INCREMENTAL PD• First, the PD prescription is less onerous with specifically less need for day dwells in
those on APD and less need frequent exchanges for those on CAPD.
• The result is greater simplicity and less workload for the patient or their caregivers.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016
• Incremental PD presents an excellent opportunity to provide patients with an initialsmall dose of dialysis while continually addressing patient fears and misconceptions as they adjust to the therapy.

BENEFITS OF INCREMENTAL PD
• Another advantage is that incremental PD prescriptions are less costly than standard ones, because less solution is required.
• CAPD with 3 dwells costs 25% less than CAPD with 4 dwells daily.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016

BENEFITS OF INCREMENTAL PD• There is less exposure of the peritoneal membrane to glucose and
glucose degradation products when less solution is used and there is less absorption of glucose systemically.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016
2L1.36%
2L1.36%
2L1.36%
2L1.36%
Total Glucose Absorbed 27.2gx4
= 108.8g
2L1.36%
2L1.36%
2L1.36%
Total Glucose Absorbed 27.2gx3
= 81.6g
Viglino G, Neri L, Barbieri S. Incremental peritoneal dialysis: Effects on the choice of dialysis modality, residual renal function and adequacy. Kidney International (2008) 73, S52–S55; doi:10.1038/sj.ki.5002601
• The effects of Incremental Dialysis (Incr_Dial) on RRF and dialytic adequacy were assessed in 11 patients treated with 2 CAPD exchanges per day for a total of 106 months (mean±sd 9.7±6.5), and then treated with three CAPD exchanges per day for an additional 105 months (9.4±8.3). Median actuarial survival on CAPD-2 before requiring additional dose of dialysis was 8.1 months.
• All patients used 25mmol/l bicarbonate/15mmol/l lactate-buffered, glucose-based dialysis solutions (Physioneal; Baxter Healthcare, Rome, Italy, SpA).
• 11 patients (males 7; mean age 66.1 ± 10.3 years; BMI in males: 30.1 ± 3.7; BMI in females:27.4 ± 2.7) had the following etiologies of ESRD : • 7 with diabetes, 2 with nephroangiosclerosis, 1 with glomerulonephritis, and 1 with adult polycystic kidney
disease (APKD).

• for patients with a GFR >5mls/min, PD is initiated with :
• 2 exchanges per day (CAPD) or
• 4 sessions per week (APD).
• The PD dose is ↑ in proportion to the reduction in the GFR as follows:
• GFR ≤5 and >3mls/min = 3 CAPD exchanges or 5 APD sessions
• GFR <3 mls/min = full dialysis dose (Full_Dial).
Incr_Dial Full_Dial
• 4 exchanges per day for CAPD and 6 or 7 sessions per week for APD.
Viglino G, Neri L, Barbieri S. Incremental peritoneal dialysis: Effects on the choice of dialysis modality, residual renal function and adequacy. Kidney International (2008) 73, S52–S55; doi:10.1038/sj.ki.5002601

Viglino G, Neri L, Barbieri S. Incremental peritoneal dialysis: Effects on the choice of dialysis modality, residual renal function and adequacy. Kidney International (2008) 73, S52–S55; doi:10.1038/sj.ki.5002601
(15 pt on CAPD2, 5 on CAPD3)
(1 pt on APD4, 4 on APD5)

• During Incr_Dial, a slowing is noted in the loss of GFR compared to the pre-dialysis period.
• This result seems particularly significant, considering the high percentage of diabetic patients (7/11 pts) examined for whom there is a high risk of a rapid decrease in RRF.
Viglino G, Neri L, Barbieri S. Incremental peritoneal dialysis: Effects on the choice of dialysis modality, residual renal function and adequacy. Kidney International (2008) 73, S52–S55; doi:10.1038/sj.ki.5002601

Viglino G, Neri L, Barbieri S. Incremental peritoneal dialysis: Effects on the choice of dialysis modality, residual renal function and adequacy. Kidney International (2008) 73, S52–S55; doi:10.1038/sj.ki.5002601

• Single-centre cohort study. Enrollment period: January 2002–December 2007; end of follow up:December 2012.
• Incremental dialysis dose (incrPD) was defined as one or two dwell times per day on CAPD.
• Standard dialysis dose (stPD) was defined as 3–5 dwell times per day, 7 days a week, for CAPD and seven nights a week for APD.
• 29 (28 %) were in the incrPD group and 76 (72 %) in the stPD group (total 105 patients)
Sandrini M et al. Incremental peritoneal dialysis: a 10 year single-centre experience. J Nephrol (2016) 29:871–879

Sandrini M et al. Incremental peritoneal dialysis: a 10 year single-centre experience. J Nephrol (2016) 29:871–879
• The results of this study suggest a protective role of incrPD on RRF which was stable in incrPD in the first 6 months whereas it significantly decreased in stPD.
• This stability could be the reason for a median duration of incrPD of 17 months, which could positively affect the patients’ quality of life on PD due to a lesser burden of dialysis procedures.
• Patients on incrPD need a closer clinical follow-up to reduce the risk of under-dialysis.
Median duration of incrPD was 17 months

Sandrini M et al. Incremental peritoneal dialysis: a 10 year single-centre experience. J Nephrol (2016) 29:871–879

Sandrini M et al. Incremental peritoneal dialysis: a 10 year single-centre experience. J Nephrol (2016) 29:871–879

Sandrini M et al. Incremental peritoneal dialysis: a 10 year single-centre experience. J Nephrol (2016) 29:871–879

Wang AY-M, Lai K-N. The importance of residual renal function in dialysis patients. Kidney International (2006) 69, 1726–1732

PRESERVATION OF RESIDUAL RENAL FUNCTION
• The benefits of retaining residual renal function (RRF) appear to be greater than one would expect from simply enhanced small solute clearance.
• RRF is associated with lower levels of β2-microglobulin, improved anaemia control, blood pressure, nutritional status and bone mineral metabolism.
• Volume control is also better due to its significant contribution to fluid and sodium removal.
Krediet RT et al. Augmenting solute clearance in peritoneal dialysis. Kidney International, Vol. 54 (1998), pp. 2218–2225Wong J et al. Incremental haemodialysis. Nephrol Dial Transplant (2015) 30: 1639–1648
The residual renal clearances are NOT equivalent to peritoneal clearances.

DRAWBACKS OF INCREMENTAL PD• First, it requires regular monitoring of residual renal function as its rate of loss is
unpredictable.
• Some centers measure renal function every 3 months in patients on incremental prescriptions.
• An alternative might be to measure it every 6 months and also if there is a change in the patient’s health or an intercurrent illness likely to lead to a fall in (RRF).
• Second, patients who start PD with an incremental prescription may find it challenging to transition to a more intensive full prescription.
Ankawi GA et al. The Use of Incremental Peritoneal Dialysis in a Large Contemporary Peritoneal Dialysis Program. Canadian Journal of Kidney Health and Disease Volume 3: 1–7© The Author(s) 2016

WHO IS A CANDIDATE FOR INCREMENTAL PD?
• By definition requires significant residual renal function (GFR>5 mLs/min) :• Not appropriate for patients with no residual renal function
• Requires clinical judgement:• Patient’s body size and dialysis requirements
• Other measures of metabolic control, other than urea clearances: bicarbonate level, but could be potassium and phosphate levels
• Ability to achieve adequate volume control
• Patients adherent to treatment and willing to convert to full dose PD / intensification of treatment when RRF falls.
Bargman JM, Girsberger M. Visions in a Crystal Ball: The Future of Peritoneal Dialysis. Blood Purif 2018;45:218–223

INCREMENTAL PD IN SPECIAL POPULATIONS• PD in chronic heart failure, such as patients with cardiorenal syndrome requiring
dialysis due to recurrent refractory volume overload.
• In a study by Courivaud et al, left ventricular ejection fraction improved significantly after the initiation of PD. Furthermore, there was an impressive 90% reduction in hospitalization days after the initiation of PD.
Bargman JM, Girsberger M. Visions in a Crystal Ball: The Future of Peritoneal Dialysis. Blood Purif 2018;45:218–223Courivaud D et al. Peritoneal Dialysis reduces the number of hospitalization days in heart failure patients refractory to diuretics. Peritoneal Dialysis International, Vol. 34, pp. 100–108

HOW TO PRESCRIBE INCREMENTAL PD?FACTORS TO CONSIDER
• Patient’s lifestyle• Patient’s body size• Patient’s RRF• Peritoneal Membrane Type• Volume/Ultrafiltration
Requirements• Solute clearance Requirements
• CAPD or APD• Type of solutions• Fill Volume of exchanges• Number of exchanges• Dwell Time
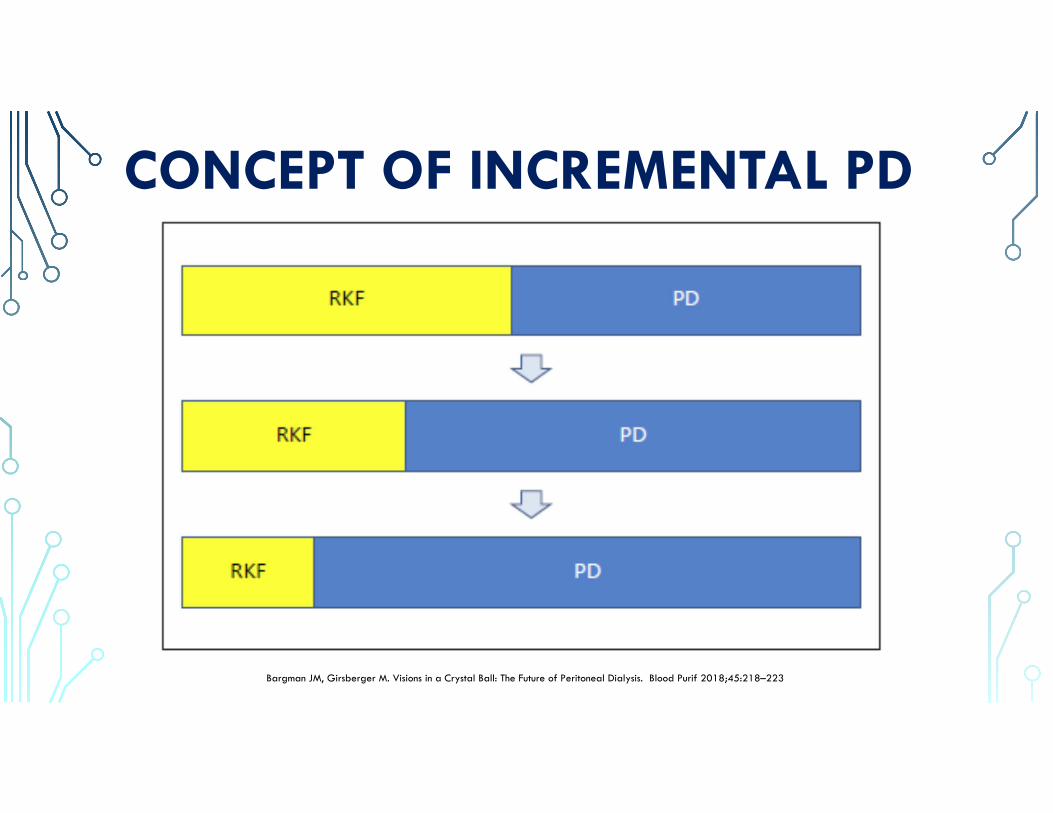
CONCEPT OF INCREMENTAL PD
Bargman JM, Girsberger M. Visions in a Crystal Ball: The Future of Peritoneal Dialysis. Blood Purif 2018;45:218–223
INCREMENTAL PD PRESCRIPTION• The dose of incremental peritoneal dialysis can be individualized according to
patient needs.
• Some patients can start with CAPD with 1 exchange overnight.
• If patients prefer to have no fluid in the abdomen overnight, then 2 daytime exchanges is a reasonable alternative.
• Exchanges for 4 hours each is recommended as opposed to 12 hour exchanges, as fluid reabsorption can occur with longer dwells.
Auguste BL, Bargman JM. Incremental peritoneal dialysis: New ideas about an old Approach. Seminars in Dialysis. 2018;1–4

INCREMENTAL PD WITH CAPDSingle overnight exchange: Glucose or icodextrin
Dry Night
Partially Dry Day
Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055

INCREMENTAL PD PRESCRIPTION
• For those patient on nocturnal intermittent peritoneal dialysis (NIPD), they can be started with 2 or 3 exchanges overnight, typically with 1.5 L fill volumes.
• New peritoneal dialysis patients will also need time to adjust to the fill volumes.
• The fill volume and number of exchanges can be gradually increased as residual renal function (RRF) falls.
Auguste BL, Bargman JM. Incremental peritoneal dialysis: New ideas about an old Approach. Seminars in Dialysis. 2018;1–4

INCREMENTAL PD WITH APD
Dry Day: Classic NIPD
Partially Dry Day
•One concern with incremental peritoneal dialysis (PD) is whether urea clearance targets are achievable with an incremental regimen.
• In this report, a large database of PD patients, across all membrane transport types were used, and urea kinetic modeling determinations of possible incremental regimens performed for an individual membrane type.
Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055

Results for high transport patients with 40 L of total body waterGuest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
• White squares indicate either total weekly urea Kt/V <1.7 or net UF was ≤−100 mL.
• Gray squares indicate total weekly urea Kt/V was ≥1.7 and net UF was 0 to −100mLs.
• Black squares indicate total weekly urea Kt/V was ≥1.7 and net UF was ≥0 mL.

Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for high average transport patients with 40 L of total body water

Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for low average transport patients with 40 L of total body water

Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for low transport patients with 40 L of total body water

• Results were illustrated for patients with a total body water (TBW) of 40L (approximately a body weight of 73 kg).
• Similar results for patients with TBW of 50L (approximately a body weight of 91 kg) except that the GFR requirements are 2-3 mLs/min/1.73 m2 higher than for a patient with TBW of 40 L.
Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055

Results for high transport patients with 40 L of total body waterGuest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for high transport patients with 50 L of total body water

Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for high average transport patients with 40 L of total body waterResults for high average transport patients with 50 L of total body water

Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for low average transport patients with 40 L of total body waterResults for low average transport patients with 50 L of total body water

Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055
Results for low transport patients with 40 L of total body waterResults for low transport patients with 50 L of total body water

• These results demonstrate patients with significant RRF at the start of dialysis may not need the full-dose dialysis regimen compared to longer-term dialysis patients who may be anuric.
• However, therapy should also focus on the ultrafiltration (UF) needs of the patients, as the clearance targets will be met with most patients who have significant RRF.
• It should be emphasized that some patients who meet urea targets may require additional exchanges for adequate UF—a separate consideration from the goal of reaching a certain target Kt/V.
Guest S et al. Kinetic Modeling of Incremental Ambulatory Peritoneal Dialysis Exchanges. Perit Dial Int: inPress http://dx.doi.org/10.3747/pdi.2016.00055


WHY INCREMENTAL PD?• Reduces burden of treatment with a less intensive regimen better quality of life
and giving patient time to adjust to PD
• Cost reduction
• Reduces local and systemic glucose exposure
• May be better tolerated in the frail or elderly patient
• May result in longer preservation of residual renal function (RRF) —the single parameter most associated with longer-term survival in PD

STRATEGIES FOR SUCCESS WITH INCREMENTAL PD
• Patient selection and education. Ensure that they will be adherent to therapy when the time comes to increase dialysis dose.
• Requires regular monitoring of residual renal function:• Every 3 months is sufficient (some literature mention monthly monitoring of
residual urine volume)
• In addition, careful assessment of metabolic control (K, HCO3, Phosphate), and volume/hypertension.
Auguste BL, Bargman JM. Incremental peritoneal dialysis: New ideas about an old Approach. Seminars in Dialysis. 2018;1–4

• Transition of patients from CKD to dialysis is an art.
• Requires timely placement of dialysis access.
• Incremental PD:• Reduces burden of treatment, reduces glucose exposure, resource-sparing,
preserves residual renal function (RRF).
• Limited outcome data
• In order to obtain good compliance, patients should be given adequate information about the future need to increase the dose of dialysis when RRF declines.
TAKE HOME MESSAGES

TAKE HOME MESSAGES• Two things are necessary to start dialysis with incremental PD:• a well-organized pre-dialysis outpatient clinic providing adequate information and
building enough rapport with the patient.
• a close clinical and laboratory follow-up to avoid that a sudden reduction in RRF could precipitate the patient towards a condition of underdialysis.
• Incremental PD can only be successful if all the participating parties (patients, their families, the dialysis staff, payer of services) understand and approve of the strategy.
• In the absence of this understanding, incremental PD is likely to be problematic.

TAKE HOME MESSAGES
• For the nephrologist, this demands a major time commitment for education of patients in the pre-dialysis run-up so that patients and their family understands that additional dialysis will be added over time as necessary.
• Not all patients or situations are conducive to incremental dialysis.
• Incremental dialysis is a component of a truly integrated care approach to end-stage renal disease.