Embed Size (px)
Citation preview

Introduction to Pediatric Nephrology
19/11/08

Kidney ontogenesis
The embryological development of the kidney is a long and continuous process which begins in the 3rd week and is completed by about 34-35 weeks of fetal life.
Kidney organogenesis is characterised by 3 distinct and linked stages: pronephros, mesonephros and metanephros.

Kidney ontogenesis In humans, the first two are transient structures with little excretory capacity but they are important for the appropriate development of the metanephros, which is the direct precursor of the adult kidney.

METANEPHROS
The final stage of the kidney is the differentation of the metanephros and arise from the ureteric bud and the metanephric blastema (mesenchyme).
The renal pelvis, major and minor calyces and terminal collecting duct are formed by the 10-13th wks of ges.
After morphogenesis each kidney contains approx a million nephrons.

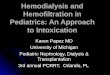
Renal development
3 t.ż.
4-8 t.ż.
5 t.ż.
nefrotomy
przewód Wolffa
Przednercze
Śródnercze
Nerka ostateczna
stek
aorta
pączek moczowodowy
blastema nerki ostatecznej
Pronephros
Mesonephros
Metanephros

Antenatal Period
The most common cause is physiologic dilation.
Metanephric urine production begins at 8 weeks, even before ureteral canalization is complete.
Transient obstruction with hydronephrosis occurs.

Embryology



MOLECULAR ASPECT
The development of the metanephric kidney depends on inductive interaction between the ureteric bud (UB) and the metanephric mesenchyme (MM).
A large number of genes have been found to be crucial during kidney development.

Nephrons
In the fetus at 36 weeks’ gestation there is an adult complement of nephrons- approx. one million
All further growth of the kidney is via hyperplasia mainly in the tubules.

Fetal kidney
Nephrogenesis is completed between the 28 and 36th gestational week in the human, the renal tissue and particularly the tubular cells continue to develop postnatally.
Several of the major transporters in the tubular epithelial cells undergo postnatal maturation

Fetal kidney
Outer cortical glomeruli are relatively underperfused compared with inner cortical glomeruli.
Following birth, renal perfusion to superficial cortical nephrons rises compared with deeper glomeruli

Fetal kidney
Angiotensin-converting enzyme inhibitors and angiotensin-receptor antagonists impair nephrogenesis and so are contraindicated in pregnancy

Production of urine
Production of urine starts at the age of 10-12 weeks of gestation:
1. very dilute urine 2. small amount of urine Fetal urine is a major constituent of amniotic fluid and urinary flow rate increases from 12ml/hr at 32 weeks’gestation to 28ml/hr at 40 weeks’gestation.
Similar increases are described during the maturation of premature newborns.

Glomerular Filtration Rate (GFR)
Glomerular filtration begins between the 9th and 12th week of gestation in humans.
The GFR is relatively low at birth especially in the premature infant.
The values of GFR nearly double between 3 and 7 days and thereafter GFR continues to increase, by 1 to 2 yrs of age the GFR is the same as in an older child- 80% of mature kidney.

GFR
Age GFR (ml/min/1,73m2) Serum creatinine (mg/dl)Premature<30wks30-34wks
5-8ml5-10 ml
<1,6<1,2
Full term<24 hrs3 days to 3 wks1-2 months3-4 months6months to 1 yr
15-25 ml30-50 ml60-70 ml70-80 ml80-100 ml
0,6-1,00,5-0,60,4-0,50,3-0,40,4-0,5
Adults 12020 0,6-1,1 (f)0,6- 1,4 (m)

Kidney of newborn
The kidney of the newborn infant has a limited capacity to regulate the excretion of fluid and electolytes.
The high sodium excretion during the first 2 to 3 weeks often results in a negative sodium balance and predisposes to hyponatremia.

Creatinine Clearance
Newborn: 40-65 ml/min/1.73 m2 <40 yrs: 97-137 ml/min/1.73 m2

Creatinine Clearance

Creatinine Clearance

Cefotaxime
Dose: 50mg/kg/dose 30-36 weeks: 0-14 days: BD, >14 days TDS 37-44 weeks: 0-7 days: BD, >7 days TDS >45 weeks: QID Renal failure: severe renal failure (<10
ml/min/1.73 m2): loading dose normal after that 25mg/kg same frequency

Ceftriaxone:
Dose: 100 mg/kg loading , 80 mg/kg OD Renal failure: severe renal failure (<10
ml/min/1.73 m2): 50mg/kg OD

Ceftazidime
Dose: 30-50 mg/kg/dose 30-36 weeks: 0-14 days: BD, >14 days TDS 37-44 weeks: 0-7 days: BD, >7 days TDS >45 weeks: TDS Renal failure:
Moderate renal failure: (10-50 ml/min/1.73 m2) same dose OD
severe renal failure (<10 ml/min/1.73 m2): ½ dose OD

AMIKACIN
<36 weeks: 12 mg/kg/OD >36 weeks: 15 mg/kg/od In renal failure serum concentration should
be estimated

Ampicillin
Dose: 25-50 mg/kg/dose, upto 100 mg also 30-36 weeks: 0-14 days: BD, >14 days TDS 37-44 weeks: 0-7 days: BD, >7 days TDS >45 weeks: QID Renal failure:
Moderate renal failure: (10-50 ml/min/1.73 m2) same dose 8-12 hrly
severe renal failure (<10 ml/min/1.73 m2): same dose OD

MEROPENEM
20-40 mg/kg/dose 40mg/kg/dose 8hourly in meningitis or
pseudomonas infection Renal failure:
Moderate renal failure: (10-50 ml/min/1.73 m2) ½ dose 12 hrly
severe renal failure (<10 ml/min/1.73 m2): ½ dose OD

PIP-TAZO
50-100 mg/kg/dose 30-36 weeks: 0-14 days: BD, >14 days TDS 37-44 weeks: 0-7 days: BD, >7 days TDS >45 weeks: TDS Renal failure:
40-80 ml/min/1.73 m2: 6hourly 20-40 ml/min/1.73 m2: 8 hourly <20 ml/min/1.73 m2: 12 hourly

VANCOMYCIN
10-15 mg/kg/dose 30-36 weeks: 0-14 days: BD, >14 days TDS 37-44 weeks: 0-14 days: BD, >14 days TDS >45 weeks: QID Renal failure:
Avoid if possible, In Anuric give 15 mg/kg every many days


Renal failure in the newborn
Renal failure in the newborn: severe asphyxia, the majority suffered from nonoliguric renal failure

CAKUT
Congenital Anomalies of Kidney and Urogenital Tract

CAKUT
Chronic renal failure (children):
Obstructive nephropathy- 47%
Reflux nephropathy- 18,5%
Hypo/dysplasia 8,7%

RENAL ABNORMALITIES
Renal agenesis:
bilateral fetal death- Potter syndrome 1:4000 pregnancies
unilateral other organ- 1:2900 pregnancies
abnormalites


Agenesis Aplasia Hypoplasia
Renal abnormalities

RENAL ABNORMALITIES
Hydronephrosis

RENAL ABNORMALITIES
Obstractive uropathy:
a/ ureteropelvic junction obstruction- dilated renal pelvis with/ without caliectasis and no dilation of the ureter
b/ ureterovesical junction obstruction (megaureter)- pelviectasis and caliectasis with significant ureter dilation

RENAL ABNORMALITIES
c/ posterior urethral valve d/ ureterocele- cystic dilatation of the
distal ureter that protrudes into the urinary bladder, may extend past the bladder into urethra
e/ ectopic ureters f/ constriction (stenosis)of urethra

Type I – Type II Type III
Posterior urethral valve

Duplication of urinary tract
Ureter Ureter Ureter
duplex fissus

RENAL ABNORMALITIES
Vesico- ureteral reflux

Frequency of VUR
• Isolated 1% (0.4-4%)
• UTI in the past 29-50%
• Siblings with VUR 32-45%
• Mothers with VUR in the past 60%
Vesico-ureteral reflux

Pediatrics 1999, 103,4
Frequency of VUR according to the child’s age

RENAL ABNORMALITIES
Polycystic kidney:
autosomal dominant p.k.disease
autosomal recessive p.k. disease

Kidney ontogenesis

PRONEPHROS
Pronephros is a transitory non-functional kidney, the first tubules appear the middle of the 3rd week and arise from intermediate mesodermal cells.
The pronephric tubules persist for only a short time and undergo degeneration by the 5th week.
At the time the pronephros is degenerating the mesonephric tubules and duct are developing.

Pronephros


Vesico- ureteral reflux
Normal kidney, ureter, and bladder

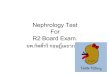
Vesico- ureteral reflux
Grade I Vesicoureteral Reflux:urine (shown in blue) refluxes part-way up the ureter

Vesico- ureteral reflux
Grade II Vesicoureteral Reflux:urine refluxes all the way up the ureter

Vesico- ureteral reflux
Grade III Vesicoureteral Reflux:urine refluxes all the way up the ureter with dilatation of the ureter and calyces (part of the kidney where urine collects)

Vesico- ureteral reflux
Grade IV Vesicoureteral Reflux:urine refluxes all the way up the ureter with marked dilatation of the ureter and
calyces

Vesico- ureteral reflux
Grade V Vesicoureteral Reflux:massive reflux of urine up the ureter with marked tortuosity and dilatation of the ureter and calyces

1 - odc. śródścienny moczowodu
2 - odc. podśluzówkowy
A - RefluxB – Possible refluxC – No reflux
Primary VUR reflux

Io IIo IIIo IVo Vo
International Classification of VUR

Ureterocoele
a thin-walled cystic swelling of the lowermost part of the ureter in its path through the bladder muscle. Ureterocoeles may be either intravesical (in which the orifice of the ureter and the cyst itself protrude into the bladder lumen) or ectopic (in which the ureterocoele is in the submucosa of the bladder and some part extends into the bladder neck or urethra). A ureterocoele is believed to be the result of a defect in the muscular coat of the ureter, and often a defect in the bladder wall itself. Congenital stenosis of the ureteric orifice in the bladder wall is thought to give rise to ureterocoele, and it is commonly associated with ectopic ureters. It is relatively common in both children and young adults, and is bilateral in approximately 10% of cases. It is more likely to occur in females, and is often accompanied by other congenital urinary tract anomalies. Ureterocoeles which occur on single ureters may also be intravesical (formerly referred to as simple ureterocoele) or ectopic.

Theory
speculative theory by Mackenzie (1996): essential hypertension develops in those born with a reduced numbers of nephrons: congenital oligonephropathy.
Low-birth-weight infants are at particular risk for this problem.

TUBULAR FUNCTION: BASIC PRINCIPLES
Absorption: the movement of solute or water from tubular lumen to blood, is the predominant process in the renal handling of Na+, Cl-, H2O, HCO3
-, glucose, amino acid, protein, PO4
+, Ca+, Mg+, urea, uric acid and others.
Secretion: the movement of solute from blood or cell interior to tubular lumen, is important in the renal handling of H+, K+, NH4
+, and a number of organic acids and bases.

Proximal Tubule
absorb the bulk of filtered small solutes . These solutes are present in p.t. fluid at the same concentration as in plasma.
Approx. 60% of the filtered Na+, Cl-, K+, Ca+, and water and more than 90% of the filtered HCO3
- are absorbed along the p.t. Reabsorbs virtually all the filtered glucose and AA by Na-dependent cotransport.
Phosphate transport is regulated by PTH. Secretion (terminal portion of p.t.): organic, anions and cations.

Loop of Henle
dilution of the urine reabsorption of Mg+

Distal Nephron
distal tubule, connecting tubule, collecting tubule
final adjustments in urine composition, tonicity and volume
aldosterone and vasopressin, regulate acid and potassium excretion

Types of Membrane Transport Mechanisms Used in the Kidney
Facilitated or carrier mediated:Glucose, ureaGLUT1 carrier, urea carrier
Active transport (pumps)Na+, K+, Ca+, H+
Na,K-ATPase, H-ATPase, Ca-ATPase Cotransport Cl-, glucose, AA, formate, phosphate Na-K-Cl cotransporter
CountertransportBicarbonate, H+ Cl/ HCO3
exchanger, Na/H antiporter Osmosis H2O Water channels (aquaporins)

Mechanism of Na+ Absorption
tubular Na+ absorption- primary active transport- driven by other enzyme Na,K-ATPase- translocates Na out of the cells/ K+ into cells
the generation of net Na+ movement from tubular lumen to blood is the asymmetrical distribution of this enzyme (exclusively present in the basolateral membrane- the blood side of all nephron segments)

Na+ balance
Immaturity of the tubules in premature infants leads to acidosis and salt wasting, which may impair growth.
Premature newborn infants have shifting volume and salt balance in the first week of life and diuresis experienced by these infants between 24 and 48hrs of life results from expansion of the extracellular space with mobilization of lung fluid.
Term newborn accomplish positive Na+ balance despite a diet low in sodium (breast milk)
Glucosteroids regulate renal Na+ excretion for only limited periods during maturation.

Blood pressure and hypertension in the newborn
no correlation between blood pressure and birthweight below 2000g was found
mechanically ventilated infants and those with low Apgar scores have lower blood pressure than healthy controls.

MESONEPHROS
Mesonephros appears in the 4th week of gestation as a more complex structure immediately after the involution of the pronephric tubules.
Mesonephros contains the vesicles -the precursor of mesonephric nephron and the mesonephric duct. The proximal end of the mesonephric duct forms a 2-layered cup, Bowman’s capsule.

MESONEPHROS
The glomerulus is completed after capillaries vascularise this primitive Bowman’s capsule.
The mesonephric nephrons are capable of producing urine by the 9th weeks of gestation and continue to do so until their involution.
At the mesonephric stage, most cells in this organ have involuted by the 11th-12th week as the metanephros begins functioning.

MOLECULAR ASPECT
A large number of genes have been found to be crucial during kidney development.
These genes encode for transcription factors (WT1, Pax2), growth factors (GDNF) and there receptors, adhesion molecules.
Gene Pax2 encodes for a transcription factor expressed in the kidney as well as in the optic cup, vesicle and other parts of CNS.
This gene is one of the first expressed during kidney ontogenesis in the UB and in the induced MM.

MOLECULAR ASPECT
A spontaneous Pax2 mutant mouse model revealed that the major cause of renal hypoplasia is reduced branching of the UB resulting in kidneys with fewer nephrons
( the number of UB cells undergoing programmed cell death during nephrogenesis)
Pax2: transcription factor: Renal-coloboma syn: 10q13
HNF1: transcription factor: renal hypoplasia, diabetes: 17q21