Embed Size (px)
Citation preview
Patient Level Opioid Risk Management
A Supplement to the PainEDU.org Manual
Nathaniel P. Katz, M.D., M.S.
Copyright 2007, Inflexxion®, Inc. All rights reserved. 320 Needham Street, Suite 100 Newton, MA 02464
1
Patient Level Opioid Risk Management
Contents I. Risks of Opioid Therapy II. Terminology III. Regulation of Opioids IV. Risk Minimization in Clinical Practice
a. Comparison with Other Medical Conditions b. Algorithm for Opioid treatment of Chronic Pain c. Initial Patient Assessment
i. Risk Assessment and Triage ii. Risk Factors for Prescription Opioid Abuse
d. Initiating an Opioid Trial e. The Follow-Up Visit
i. Urine Toxicology and Other Sources of Information f. Management Plans
i. Continuation of Opioid Therapy ii. Dose Adjustment
iii. Adding a Long-Acting Opioid iv. Opioid Rotation v. Exit Strategies
g. Consultation and Referral h. Documentation i. Protecting Collaterals and the Community
V. Summary VI. References VII. Appendices
a. Initial Evaluation Guide b. Triage Guide c. SOAPP d. Sample Patient Treatment Agreement e. Medication Flowchart f. Patient Education Brochure g. Pain Assessment and Documentation Tool (PADT) h. Opioid Rotation i. Exit Strategy
2

I. Risks of Opioid Therapy Chronic pain is a major public health problem in the US, and opioids, for better or worse, remain an essential tool in the armamentarium against acute and chronic pain. Owing to substantial efforts to improve awareness and treatment of chronic pain, the availability of opioids has increased dramatically in the past several decades. Although much more remains to be done to ensure appropriate access to opioids, opioid prescribing is currently at the highest level in decades, allowing patients with cancer and non-cancer pain unprecedented access to these analgesics. Opioids, like all medications, are associated with risks, and the prevalence of negative consequences of opioid use has risen concomitantly with their increased use (Table 1). The risks of greatest concern have been abuse and addiction. Prescription opioid abuse is rising faster than any other type of drug abuse, and is now second only to marijuana in terms of prevalence of abuse and addiction, and ahead of cocaine and heroin by many measures. Current projections suggest that approximately 1.5 million Americans meet criteria for abuse or addiction to prescription opioids, which is nearly 1% of the population. While some clinicians have been comforted by a mythology that addiction does not occur in “legitimate” pain patients, the reality is that there is significant overlap between patients with pain and those with addictive disorders; because the prevalence of chronic pain and of addiction are so high, no clinician is free of treating patients with co-morbid pain and addiction. This becomes clear when one considers that the background rate of active substance abuse is approximately 10% in the general US population; that substance abuse increases the risk for certain types of pain; that 20-40% of pain patients on opioids have substance abuse problems; and that pain is the number one reason patients see doctors. The presence of co-morbid addiction significantly complicates the treatment of pain, and the presence of co-morbid pain significantly complicates the treatment of addiction. A unique feature of prescription drug abuse as a complication of medical prescribing is that the problem occurs not only in patients but in their families and the community. Since one of the major sources of abused prescription opioids is the prescriptions of friends and family, it is clear that many of the patients to whom we prescribe are the source of medications that put their family and the community at risk, either from intentional diversion by the patient, or by theft or other unintentional pathways to diversion. The prescriber therefore has unique obligations to prescribe opioids in a manner that minimizes potential harm to non-patient collaterals. Side effects, such as nausea, vomiting, dizziness, sweating, and constipation, are commonly experienced risks of opioid therapy that can to a great extent be prevented or treated. Another risk of opioid therapy, which has not been widely publicized although observed for centuries, is endocrine disturbance, particularly testosterone deficiency. These risks will not be discussed in detail in this chapter as they are presented elsewhere.
3
M
R M
R I Riim“psdc MR
MR
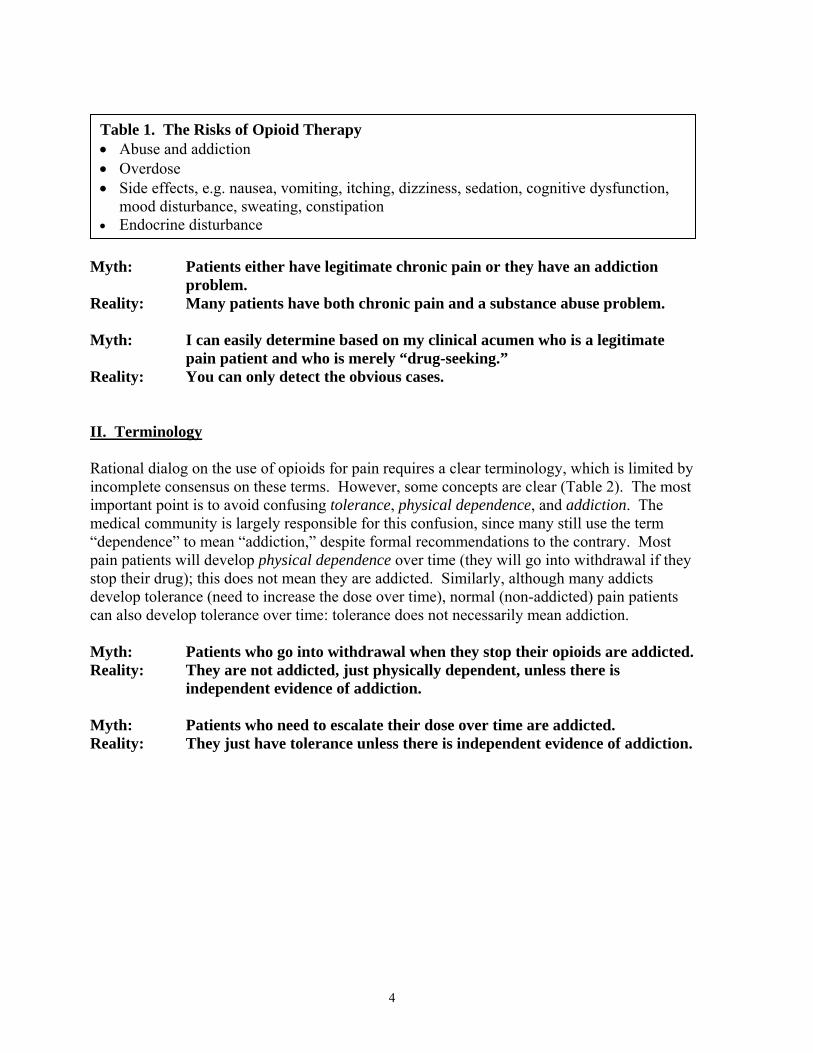
Table 1. The Risks of Opioid Therapy • Abuse and addiction • Overdose • Side effects, e.g. nausea, vomiting, itching, dizziness, sedation, cognitive dysfunction,
mood disturbance, sweating, constipation • Endocrine disturbance
yth: Patients either have legitimate chronic pain or they have an addiction problem.
eality: Many patients have both chronic pain and a substance abuse problem.
yth: I can easily determine based on my clinical acumen who is a legitimate pain patient and who is merely “drug-seeking.”
eality: You can only detect the obvious cases.
I. Terminology
ational dialog on the use of opioids for pain requires a clear terminology, which is limited by ncomplete consensus on these terms. However, some concepts are clear (Table 2). The most mportant point is to avoid confusing tolerance, physical dependence, and addiction. The edical community is largely responsible for this confusion, since many still use the term
dependence” to mean “addiction,” despite formal recommendations to the contrary. Most ain patients will develop physical dependence over time (they will go into withdrawal if they top their drug); this does not mean they are addicted. Similarly, although many addicts evelop tolerance (need to increase the dose over time), normal (non-addicted) pain patients an also develop tolerance over time: tolerance does not necessarily mean addiction.
yth: Patients who go into withdrawal when they stop their opioids are addicted. eality: They are not addicted, just physically dependent, unless there is
independent evidence of addiction.
yth: Patients who need to escalate their dose over time are addicted. eality: They just have tolerance unless there is independent evidence of addiction.
4
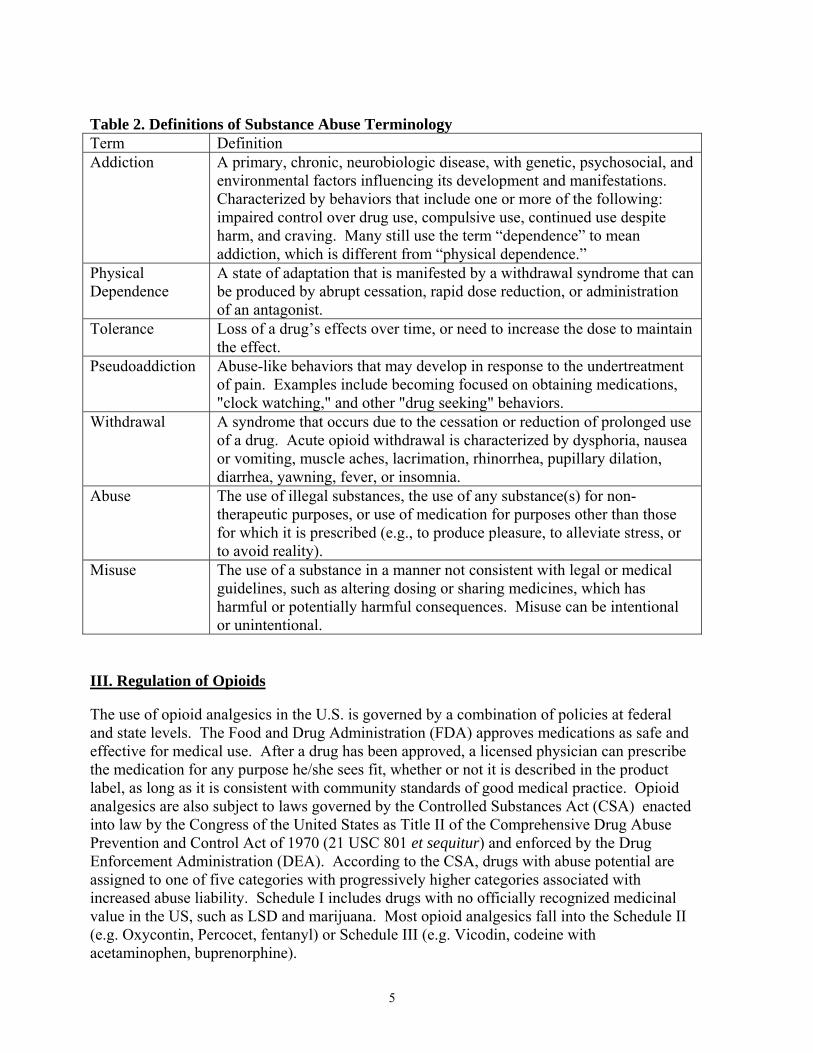
Table 2. Definitions of Substance Abuse Terminology Term Definition Addiction A primary, chronic, neurobiologic disease, with genetic, psychosocial, and
environmental factors influencing its development and manifestations. Characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving. Many still use the term “dependence” to mean addiction, which is different from “physical dependence.”
Physical Dependence
A state of adaptation that is manifested by a withdrawal syndrome that can be produced by abrupt cessation, rapid dose reduction, or administration of an antagonist.
Tolerance Loss of a drug’s effects over time, or need to increase the dose to maintain the effect.
Pseudoaddiction Abuse-like behaviors that may develop in response to the undertreatment of pain. Examples include becoming focused on obtaining medications, "clock watching," and other "drug seeking" behaviors.
Withdrawal A syndrome that occurs due to the cessation or reduction of prolonged use of a drug. Acute opioid withdrawal is characterized by dysphoria, nausea or vomiting, muscle aches, lacrimation, rhinorrhea, pupillary dilation, diarrhea, yawning, fever, or insomnia.
Abuse The use of illegal substances, the use of any substance(s) for non-therapeutic purposes, or use of medication for purposes other than those for which it is prescribed (e.g., to produce pleasure, to alleviate stress, or to avoid reality).
Misuse The use of a substance in a manner not consistent with legal or medical guidelines, such as altering dosing or sharing medicines, which has harmful or potentially harmful consequences. Misuse can be intentional or unintentional.
III. Regulation of Opioids The use of opioid analgesics in the U.S. is governed by a combination of policies at federal and state levels. The Food and Drug Administration (FDA) approves medications as safe and effective for medical use. After a drug has been approved, a licensed physician can prescribe the medication for any purpose he/she sees fit, whether or not it is described in the product label, as long as it is consistent with community standards of good medical practice. Opioid analgesics are also subject to laws governed by the Controlled Substances Act (CSA) enacted into law by the Congress of the United States as Title II of the Comprehensive Drug Abuse Prevention and Control Act of 1970 (21 USC 801 et sequitur) and enforced by the Drug Enforcement Administration (DEA). According to the CSA, drugs with abuse potential are assigned to one of five categories with progressively higher categories associated with increased abuse liability. Schedule I includes drugs with no officially recognized medicinal value in the US, such as LSD and marijuana. Most opioid analgesics fall into the Schedule II (e.g. Oxycontin, Percocet, fentanyl) or Schedule III (e.g. Vicodin, codeine with acetaminophen, buprenorphine).
5
All clinicians must be familiar with the rules regarding controlled substance prescribing in their states. Such regulations control activities such as calling in prescriptions, writing refills, calling in emergency supplies, etc. Prescribing opioids to patients with pain in the course of usual medical practice, and in the context of a legitimate doctor-patient relationship, is permitted. Moreover, the courts increasingly expect clinicians to attend to patients’ pain issues, including if this requires the use of opioid analgesics. It is rare for physicians acting in the context of appropriate medical practice, and maintaining adequate records, to be censured for prescribing opioids to patients with pain. One common source of confusion is whether physicians can prescribe to patients with addiction. The simple answer is that physicians with current licenses and DEA registrations can prescribe opioids, including methadone or buprenorphine, to patients with pain, whether or not the patient has an addictive disorder (although this may not always be advisable). In order to prescribe for the “maintenance treatment” of addiction, a physician must have a special license or waiver to prescribe maintenance treatment, whether or not the patient has pain. Of course, in the patient with co-morbid pain and addiction the medication does not know under which regulation it is being prescribed, or whether it is supposed to be treating the pain or the addiction. Nonetheless, physicians must be mindful of the applicable regulations. Unless specially licensed, physicians must be prescribing for pain, not addiction, even in patients with co-morbid addictive disorders, and the medical chart must reflect this practice. Myth: Physicians cannot prescribe opioids to patients with addictive disorders
unless they have a special license. Reality: Physicians can prescribe opioids to patients with addictive disorders as
long as the reason they are prescribing is for pain (and is so documented), and not for the treatment of addiction.
Myth: Physicians cannot prescribe methadone unless they have a special license. Reality: Physicians can prescribe methadone for pain just like any other Schedule
II opioid. However this must be for the treatment of pain and not for the treatment of addiction.
IV. Risk Minimization in Clinical Practice While there are no validated guidelines for the use of opioids in chronic pain, the following are a reasonable set of considerations and recommendations consistent with current thinking in the field. A. Comparison With Other Medical Conditions
The prescribing of opioids for the treatment of pain is no different than the prescribing of any medication for any disorder (Table 3). As in the example provided of insulin for diabetes, all therapies have complications, which are more likely to occur (by definition) in high-risk
6
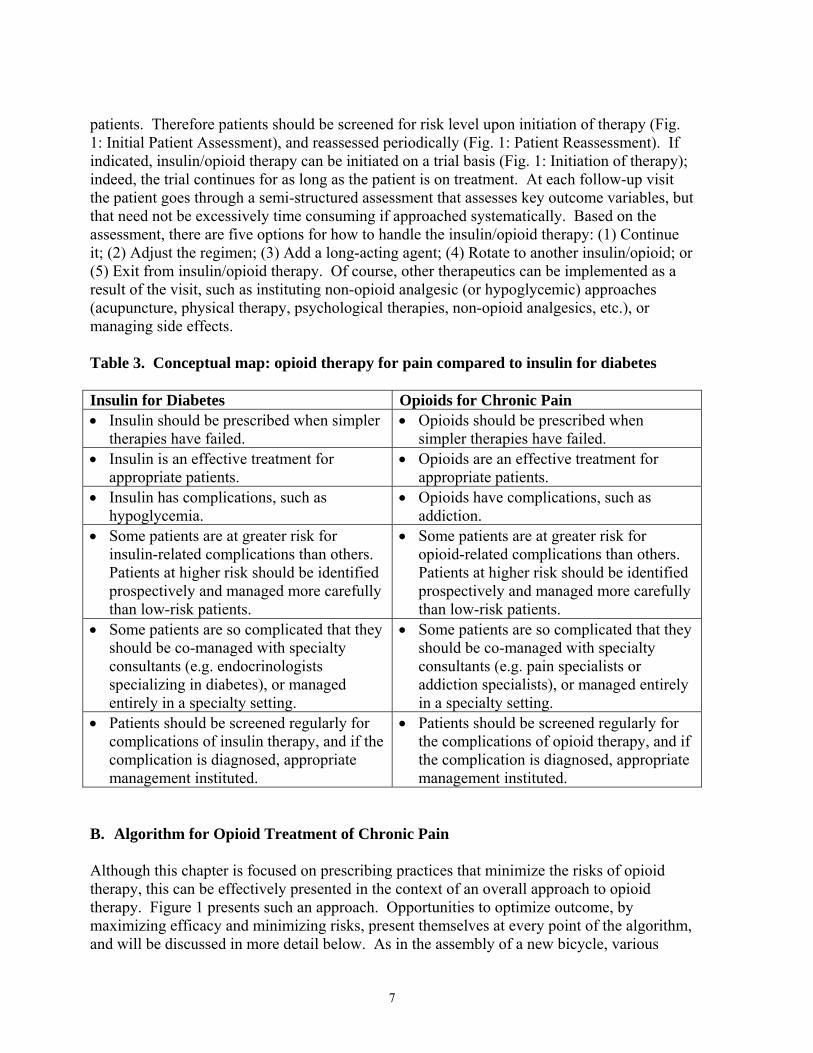
patients. Therefore patients should be screened for risk level upon initiation of therapy (Fig. 1: Initial Patient Assessment), and reassessed periodically (Fig. 1: Patient Reassessment). If indicated, insulin/opioid therapy can be initiated on a trial basis (Fig. 1: Initiation of therapy); indeed, the trial continues for as long as the patient is on treatment. At each follow-up visit the patient goes through a semi-structured assessment that assesses key outcome variables, but that need not be excessively time consuming if approached systematically. Based on the assessment, there are five options for how to handle the insulin/opioid therapy: (1) Continue it; (2) Adjust the regimen; (3) Add a long-acting agent; (4) Rotate to another insulin/opioid; or (5) Exit from insulin/opioid therapy. Of course, other therapeutics can be implemented as a result of the visit, such as instituting non-opioid analgesic (or hypoglycemic) approaches (acupuncture, physical therapy, psychological therapies, non-opioid analgesics, etc.), or managing side effects. Table 3. Conceptual map: opioid therapy for pain compared to insulin for diabetes Insulin for Diabetes Opioids for Chronic Pain • Insulin should be prescribed when simpler
therapies have failed. • Opioids should be prescribed when
simpler therapies have failed. • Insulin is an effective treatment for
appropriate patients. • Opioids are an effective treatment for
appropriate patients. • Insulin has complications, such as
hypoglycemia. • Opioids have complications, such as
addiction. • Some patients are at greater risk for
insulin-related complications than others. Patients at higher risk should be identified prospectively and managed more carefully than low-risk patients.
• Some patients are at greater risk for opioid-related complications than others. Patients at higher risk should be identified prospectively and managed more carefully than low-risk patients.
• Some patients are so complicated that they should be co-managed with specialty consultants (e.g. endocrinologists specializing in diabetes), or managed entirely in a specialty setting.
• Some patients are so complicated that they should be co-managed with specialty consultants (e.g. pain specialists or addiction specialists), or managed entirely in a specialty setting.
• Patients should be screened regularly for complications of insulin therapy, and if the complication is diagnosed, appropriate management instituted.
• Patients should be screened regularly for the complications of opioid therapy, and if the complication is diagnosed, appropriate management instituted.
B. Algorithm for Opioid Treatment of Chronic Pain Although this chapter is focused on prescribing practices that minimize the risks of opioid therapy, this can be effectively presented in the context of an overall approach to opioid therapy. Figure 1 presents such an approach. Opportunities to optimize outcome, by maximizing efficacy and minimizing risks, present themselves at every point of the algorithm, and will be discussed in more detail below. As in the assembly of a new bicycle, various
7
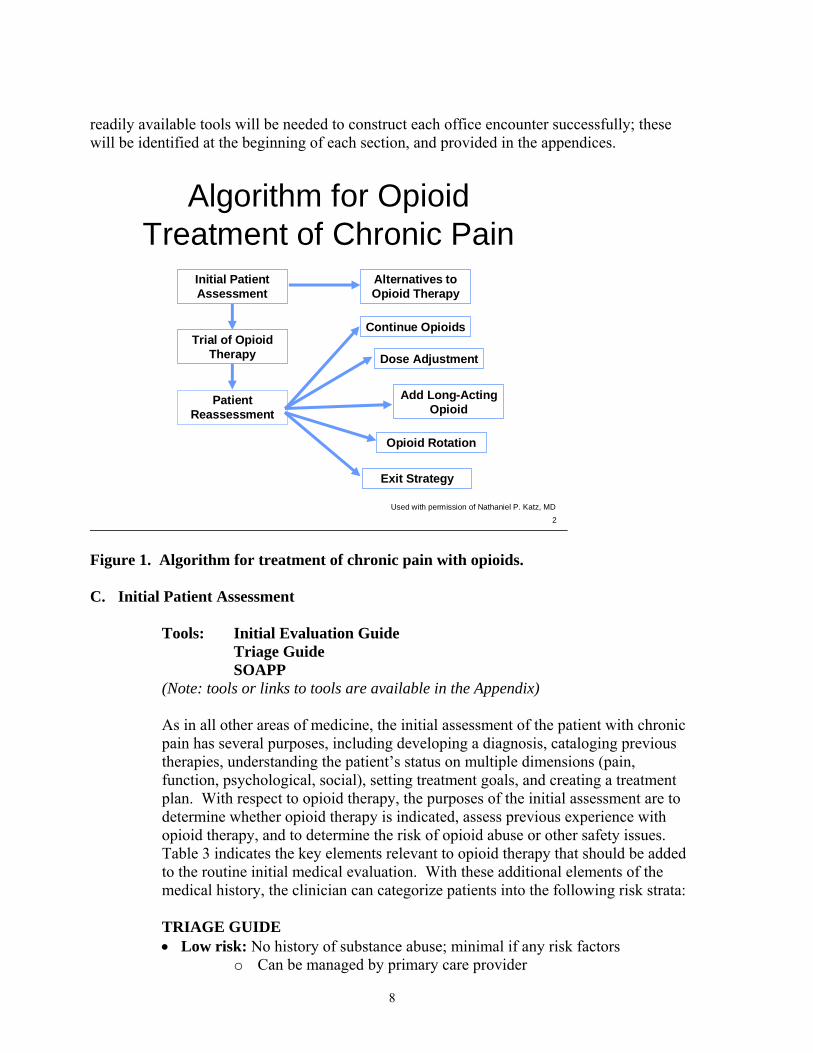
readily available tools will be needed to construct each office encounter successfully; these will be identified at the beginning of each section, and provided in the appendices.
Algorithm for Opioid Treatment of Chronic Pain
Initial Patient Assessment
Trial of Opioid Therapy
Alternatives to Opioid Therapy
Patient Reassessment
Exit Strategy
Opioid Rotation
2Used with permission of Nathaniel P. Katz, MD
Continue Opioids
Add Long-Acting Opioid
Dose Adjustment
Figure 1. Algorithm for treatment of chronic pain with opioids. C. Initial Patient Assessment
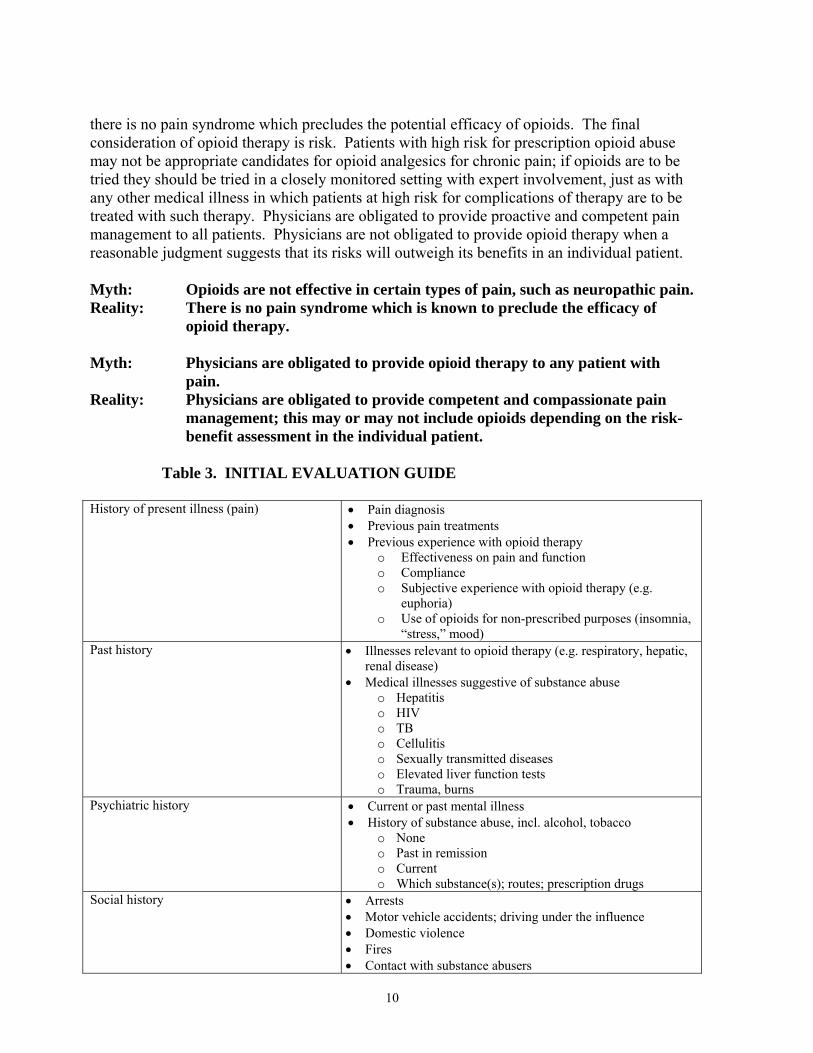
Tools: Initial Evaluation Guide Triage Guide SOAPP (Note: tools or links to tools are available in the Appendix) As in all other areas of medicine, the initial assessment of the patient with chronic pain has several purposes, including developing a diagnosis, cataloging previous therapies, understanding the patient’s status on multiple dimensions (pain, function, psychological, social), setting treatment goals, and creating a treatment plan. With respect to opioid therapy, the purposes of the initial assessment are to determine whether opioid therapy is indicated, assess previous experience with opioid therapy, and to determine the risk of opioid abuse or other safety issues. Table 3 indicates the key elements relevant to opioid therapy that should be added to the routine initial medical evaluation. With these additional elements of the medical history, the clinician can categorize patients into the following risk strata: TRIAGE GUIDE • Low risk: No history of substance abuse; minimal if any risk factors
o Can be managed by primary care provider
8
• Medium risk: Past history of substance abuse (not prescription opioid abuse); significant risk factors
o Co-manage with addiction and/or pain specialists • High risk: Active substance abuse problem; history of prescription opioid
abuse o Opioids may not be appropriate o Refer to center specializing in management of patients with co-
morbid pain and addictive disorders Assigning a patient into a risk category is a matter of clinical judgment and at the time of this writing has not been informed by evidence-based guidelines. However, broad consensus exists on several key points. An individual with a long life experience devoid of drug abuse problems or significant mental health issues is of very low risk for developing a prescription opioid abuse problem due to exposure to opioids for the treatment of pain. Such patients can be managed safely in primary care. However, even such patients are not immune to opioid addiction, and should undergo proper assessment and follow-up to ensure that negative outcomes of opioid therapy are not occurring. On the other hand, individuals with active substance abuse problems, or with a history of prescription opioid abuse, are highly likely to have problems if prescribed opioids outside a specialty setting (and even then). In general, the risk of opioid therapy outweighs their benefit in the primary care setting. The existence of these risk factors will often not be disclosed by the patient, and will need to be inferred by indirect sources of evidence, as provided in the Initial Evaluation Guide, or by review of “external sources of information” (e.g. urine toxicology results, prescription monitoring data, and outside medical records). Finally there is the middle: patients with a modest degree of risk. This requires the most judgment, and it is usually advisable to obtain some specialty input (or co-management) for these patients, and to always consider the risk categorization provisional. Special screening tests to estimate the risk of prescription opioid abuse in a patient starting opioid therapy have recently begun to appear. The most validated questionnaire at the time of this writing is the Screener and Opioid Assessment for Patients with Pain (SOAPP). By incorporating the SOAPP or another such tool into clinical practice, clinicians can obtain additional evidence to support the risk categorization of the patient. When is opioid therapy indicated? While complete consensus on this issue has not been achieved, there is broad agreement that opioids are indicated only after complete diagnostic assessments and primary treatment of the underlying painful disorder have been at least initiated, and when more conservative therapies have not been adequate. In general analgesic approaches should be implemented in parallel with efforts to diagnose and treat the underlying disorder; appropriate analgesia should not be postponed pending the diagnostic workup. It is also worth noting that therapies usually considered more conservative (acetaminophen, non-steroidal anti-inflammatory drugs, antidepressants, anticonvulsants, etc.) may in fact not be more conservative in certain subgroups of patients, such as those who have suffered NSAID-associated gastrointestinal bleeding, or who have had complications of antidepressant therapy. With respect to the underlying pain syndrome, opioids have been shown to be effective in essentially every pain syndrome in which they have been studied, at least in the short run;
9
there is no pain syndrome which precludes the potential efficacy of opioids. The final consideration of opioid therapy is risk. Patients with high risk for prescription opioid abuse may not be appropriate candidates for opioid analgesics for chronic pain; if opioids are to be tried they should be tried in a closely monitored setting with expert involvement, just as with any other medical illness in which patients at high risk for complications of therapy are to be treated with such therapy. Physicians are obligated to provide proactive and competent pain management to all patients. Physicians are not obligated to provide opioid therapy when a reasonable judgment suggests that its risks will outweigh its benefits in an individual patient. Myth: Opioids are not effective in certain types of pain, such as neuropathic pain. Reality: There is no pain syndrome which is known to preclude the efficacy of
opioid therapy. Myth: Physicians are obligated to provide opioid therapy to any patient with
pain. Reality: Physicians are obligated to provide competent and compassionate pain
management; this may or may not include opioids depending on the risk-benefit assessment in the individual patient.
Table 3. INITIAL EVALUATION GUIDE
History of present illness (pain) • Pain diagnosis • Previous pain treatments • Previous experience with opioid therapy
o Effectiveness on pain and function o Compliance o Subjective experience with opioid therapy (e.g.
euphoria) o Use of opioids for non-prescribed purposes (insomnia,
“stress,” mood) Past history • Illnesses relevant to opioid therapy (e.g. respiratory, hepatic,
renal disease) • Medical illnesses suggestive of substance abuse
o Hepatitis o HIV o TB o Cellulitis o Sexually transmitted diseases o Elevated liver function tests o Trauma, burns
Psychiatric history • Current or past mental illness • History of substance abuse, incl. alcohol, tobacco
o None o Past in remission o Current o Which substance(s); routes; prescription drugs
Social history • Arrests • Motor vehicle accidents; driving under the influence • Domestic violence • Fires • Contact with substance abusers
10
Family history • Substance abuse • Family support
D. Initiating an Opioid Trial
Tools: Patient Treatment Agreement Medication Flowchart Patient Education Brochure
(Note: Tools or links to tools are available in the Appendix) If a patient appears to be an appropriate candidate for opioid therapy it is appropriate to initiate a trial. This requires several steps and related documents as indicated above. In reality, many patients are prescribed opioids without a formal declaration of long-term opioid therapy. This occurs, for example, in a patient with chronic pain who receives a short-term opioid prescription for a pain flare, and continues to receive frequent refills before the clinician (and patient) realize that in fact the patient is now on long-term opioid therapy. While in principle these documentation steps will be initiated at the time of initiation of opioid therapy, in practice they will be initiated “when the light bulb goes off” and it becomes apparent that in fact the patient is on long-term opioid therapy. A written treatment agreement and the expressed informed consent of the patient is wise when managing chronic pain with long-term opioid therapy. The physician should discuss the risks and benefits of the use of controlled substances with the patient, persons designated by the patient, or with the patient's surrogate or guardian if the patient is incompetent. The written treatment plan should state objectives and goals as well as expectations regarding behavior, limits, consequences, and stipulations which may include (1) urine/serum medication levels screening when requested (2) number and frequency of all prescription refills and (3) reasons for which drug therapy may be discontinued (i.e. violation of agreement or lack of benefit). The contract should generally stipulate that the patient should receive prescriptions from one physician and one pharmacy. Treatment requires ongoing assessment and modifications of the treatment plan and agreed upon contract as appropriate.
Patients should be advised that opioid therapy is always considered a trial, and the advisability of continued opioid therapy, based on a risk-benefit assessment, is continually revisited for the duration of treatment, no matter how long. The spirit of these discussions is based on fundamental principles of medicine, and entered into as a collaboration with the patient to maximize pain relief, functional outcomes, and goal attainment. These goals may be enhanced by opioid therapy, or may be undermined by opioid therapy – determining this is the purpose of the opioid trial. If opioids are found not to be helpful to the patient, or the patient is
11
unable to comply with therapy, the opioids will be discontinued in an appropriate manner, since this is in the best interest of the patient. An important difference between opioid therapy and non-abusable drug therapies is in the role of patient self-report. As is well known in the addiction community, the patient’s self report in the context of opioid therapy must be taken with a grain of salt, since in a number of conditions, patient self-report loses its reliability; this applies to pain intensity, functional improvement, compliance with therapy, and substance abuse related issues. The physician accustomed to obeying the mantra of “always believe the patient” must learn to modify this approach in the setting of opioid therapy, and to consider self-report as one of many sources of information about the patient’s status. Again, this is done for the sake of the patient. Myth: In the context of opioid therapy, the patient’s self-report trumps all
other sources of information. Reality: The patient’s self report may be unreliable in the setting of opioid
therapy; self-report must be considered in the context of other sources of information.
A trial of opioid therapy is usually begun with as-needed (PRN) doses of a short-acting product combining an opioid and a non-opioid analgesic. Common choices include hydrocodone/acetaminophen, oxycodone/acetaminophen, oxycodone/ibuprofen, and codeine/acetaminophen. The non-opioid component maximizes the balance of analgesia and side effects of the regimen. The use of short-acting PRN doses allows the clinician and patient to assess the opioid requirement. Unfortunately, short-acting agents are the most widely abused opioids in the US. Long-acting products, with the exception of extended-release oxycodone products (e.g. Oxycontin, due to the ease with which the extended-release formulation can be converted to a high-potency immediate-release formulation), tend to be less abused than short-acting preparations. Also, individuals with addictive disorders tend to be able to comply better with medications that are taken at fixed doses round the clock rather than on an as-needed basis. Therefore, in a patient at-risk for substance abuse, an opioid trial at times may be more appropriately initiated with a transdermal opioid (such as fentanyl) or an extended-release oral formulation, although these products can certainly be abused as well. The patients’ pain profile should be taken into account as well: patients with a fairly consistent pain profile (pain intensity is more or less the same all the time) are more likely to succeed with a sustained-release-only regimen; patients with somewhat intermittent pain may not do well. A final consideration in the choice of opioid is tramadol. Tramadol is an analgesic that derives part of its pain relieving properties from an opioid effect (just like morphine), but part from non-opioid effects (inhibition of reuptake of norepinephrine and serotonin, like many antidepressants). Tramadol is far less
12
likely to be abused than other opioid analgesics, although it certainly can be abused. Tramadol is now available in an extended-release formulation as well. Patients with insufficient analgesia on tramadol can always be advanced to other opioid therapies. No discussion of minimizing the risk of opioid therapies would be complete without discussing the non-abuse risks of opioids, such as nausea, vomiting, and dizziness. These side effects are very common early in opioid therapy, and frequently cause patients to stop taking the prescribed or switch to another – a suboptimal result. Most guidelines call for implementing a prophylactic bowel regimen in all patients started on opioid therapy, although in patients at low risk for constipation, this can be held in reserve. Patients should be instructed to anticipate these side effects, and given instructions on how to deal with them should they occur, potentially including a prescription for an anti-emetic.
E. The Follow-Up Visit
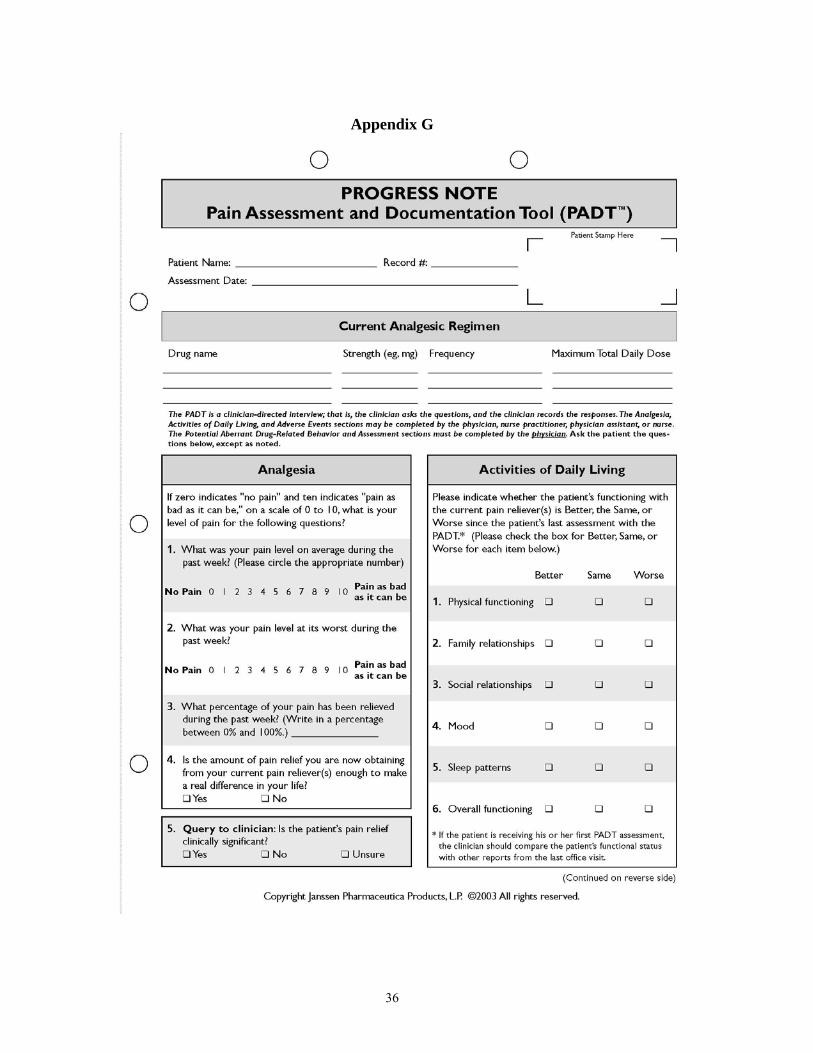
Tool: PADT (Note: Tools or links to tools are available in the Appendix)
It is helpful to follow a structured assessment in following patients on long-term opioid therapy. The PADT is a follow-up assessment that clinicians can use to assess such patients. The tool is based on the 4 A’s: • Analgesia: What is the patient’s average pain intensity? • Activities: How has the patient been functioning? • Adverse Events: Has the patient had side effects? • Aberrant Behavior: Has there been any evidence of abuse, misuse, or addiction? Based on capturing the above information, the clinician can develop two more “As”: Assessment and Action Plan. Each domain will now be discussed in a bit more detail. Analgesia. Patients on opioids for chronic pain rarely enjoy complete pain relief. In fact many patients live with pain in the “moderate” range – typically 4-7 on a 0-10 Numerical Rating Scale – despite the common perception that opioids are extremely “strong” medications. It is critical to manage patient expectations early, so that patients (and clinicians) are not disappointed with the result of partial pain relief and some functional restoration. In the assessment of Analgesia, at least partial pain reduction is necessary evidence for the appropriateness of continuing opioid therapy. Many clinicians are familiar with the type of patient who despite ongoing opioid therapy continues to have reports of severe pain (8-10/10), or even ratings that are “off the scale,” but who insist that the opioids are “taking the edge off.” These patients are at high risk for having psychosocial issues amplifying their pain perception, and may constitute an exception to the generally useful dictum that in making decisions about analgesic regimens the clinician should rely primarily on the patient’s self report. Patients with persistently high pain intensity ratings and no evidence of functional improvement should either have their dose
13
increased (as long as there are not significant side effects), have non-opioid analgesic approaches added (medical, rehabilitative, or psychosocial), or should be tapered off opioid therapy. Activities. A judgment that a patient indeed is benefiting from opioid therapy is more convincing if there has been some evidence of functional improvement. Function can be construed broadly and includes activities of daily living, psychological function, social function, sleep, employment, etc. Even a slight improvement in pain intensity accompanied by clear evidence of increased function is very persuasive of opioid benefit. On the other hand, a picture of persistently high pain scores and no functional improvement – or actual functional deterioration – generally suggests that an opioid taper is appropriate. Adverse Events. Patients have many more adverse effects of opioid therapy than they report. Therefore adverse effects should be elicited prospectively, as indicated on the PADT. Often patients fear that if they report side effects, the medication will be stopped. While switching opioids is often the most effective solution for opioid-induced side effects, a number of other approaches can be used to address side effects without changing medications, and thereby improving the patient’s outcome on opioid therapy. One underappreciated side effect of long-term opioid therapy is endocrine disturbance. Most men, and many women, on long-term opioid therapy will develop opioid-induced androgen deficiency (OPIAD), a form of central hypogonadism. In men this will be manifested by loss of libido, alteration in hair growth, mood disturbances, alteration of male role, loss of muscle strength and mass, and potentially osteoporosis and fractures. In women the manifestations have been less well defined but may include alterations in menses and infertility. It is appropriate to measure on an annual basis for all patients on long term opioid therapy: luteinizing hormone (LH), follicle stimulating hormone (FSH), total and free testosterone, sex-hormone binding globulin (SHBG), and prolactin, and to screen for symptoms of OPIAD. There is no consensus on the management of OPIAD. A reasonable approach would be to switch opioids if feasible (although there is no information on whether one opioid is less likely to cause OPIAD than another); if OPIAD persists, and opioids remain indicated, then to supplement testosterone, preferably under the guidance of an endocrinologist. Aberrant Behaviors. Many patients use their medication in a way that would not be condoned, or even anticipated by their clinicians. Non-compliance is ubiquitous in medicine, and may be unintentional (e.g. taking the wrong dose by mistake, forgetting a dose), intentional but not related to abuse (e.g. taking an extra Percocet to help sleep, unauthorized dose escalation for a pain flare), or intentional and related to abuse (taking extra to get high, faking pain to get opioids, using the medication in an out-of-control manner). The clinician seeing the patient for pain often does not have the luxury of the addiction specialist, whose patients all openly acknowledge their problematic drug use. The pain clinician will often see a
14

confusing and subtle pattern of behaviors, and will need to make a judgment as to whether the behaviors represent a pattern potentially indicating abuse, addiction, or criminal behavior, or whether the behaviors can be adequately explained by more benign causes: cognitive or language difficulties, administrative or insurance reasons, co-morbid psychological conditions, or pseudoaddiction. Research has shown that most patients will engage in a number of aberrant behaviors. How is the clinician to judge when these aberrant behaviors reach a high enough level to require recognition as an abuse-related or criminal phenomenon? How can clinicians take action when the diagnosis of addiction, or criminal behavior, can rarely be made with 100% certainty in the pain management setting? Table 4 provides a list of aberrant behaviors and a common-sense classification of their relative severity. Behaviors in the first column generally represent addiction or related phenomena; behaviors in the second column are less clear and indicate the need for review of the patient treatment agreement, limit setting, and enhanced monitoring to gain further clarity. Patients whose behaviors are felt to be most likely related to addiction or criminal behavior cannot generally be safely managed in the primary care setting, and cannot be managed safely in many pain management clinics either. The existence of a co-morbid addictive disorder does not necessarily mean that the patient cannot benefit from opioid therapy; indeed, many patients with co-morbid pain and addiction appear to benefit from methadone maintenance and other treatments. The issue is that opioids cannot be provided safely to many patients in medical settings not equipped to handle the needs of the substance abuser. Such patients should be tapered gradually off opioid therapy and/or referred to a center equipped to manage co-morbid pain and addiction. External Sources of Information: Urine Toxicology and Prescription Monitoring The difficulties of ascertaining the patient’s clinical status based only on the clinical assessment has made it essential to obtain “external” sources of information (information derived from outside the bedside assessment) in order to support safe opioid prescribing. Urine toxicology has grown in popularity as an external measure of drug abuse (see below). Some states (and payers) now share prescription monitoring data with physicians, which allows prescribers to review the prescription behavior of their patients for months or years into the past. Review of outside medical records should be done whenever possible especially for new patients. Finally, interviews with significant others, employers, school personnel, or others familiar with the patient’s behavior outside the office can also be helpful, although the issue of reliability of this input may create new complexities. There is no consensus at present about the role of external information in patient assessment. It is the opinion of this author, and consistent with the principle of “universal precautions,” to require that patients submit a urine specimen for
15
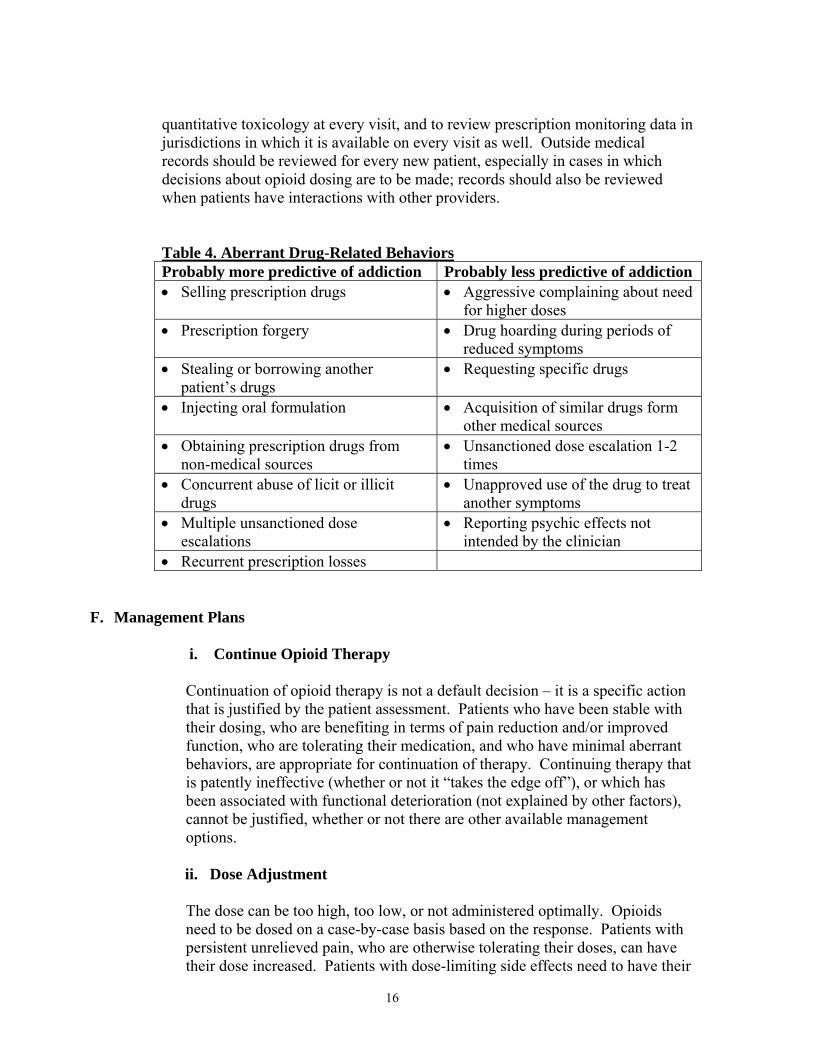
quantitative toxicology at every visit, and to review prescription monitoring data in jurisdictions in which it is available on every visit as well. Outside medical records should be reviewed for every new patient, especially in cases in which decisions about opioid dosing are to be made; records should also be reviewed when patients have interactions with other providers. Table 4. Aberrant Drug-Related BehaviorsProbably more predictive of addiction Probably less predictive of addiction • Selling prescription drugs • Aggressive complaining about need
for higher doses • Prescription forgery • Drug hoarding during periods of
reduced symptoms • Stealing or borrowing another
patient’s drugs • Requesting specific drugs
• Injecting oral formulation • Acquisition of similar drugs form other medical sources
• Obtaining prescription drugs from non-medical sources
• Unsanctioned dose escalation 1-2 times
• Concurrent abuse of licit or illicit drugs
• Unapproved use of the drug to treat another symptoms
• Multiple unsanctioned dose escalations
• Reporting psychic effects not intended by the clinician
• Recurrent prescription losses
F. Management Plans
i. Continue Opioid Therapy
Continuation of opioid therapy is not a default decision – it is a specific action that is justified by the patient assessment. Patients who have been stable with their dosing, who are benefiting in terms of pain reduction and/or improved function, who are tolerating their medication, and who have minimal aberrant behaviors, are appropriate for continuation of therapy. Continuing therapy that is patently ineffective (whether or not it “takes the edge off”), or which has been associated with functional deterioration (not explained by other factors), cannot be justified, whether or not there are other available management options.
ii. Dose Adjustment
The dose can be too high, too low, or not administered optimally. Opioids need to be dosed on a case-by-case basis based on the response. Patients with persistent unrelieved pain, who are otherwise tolerating their doses, can have their dose increased. Patients with dose-limiting side effects need to have their
16
dose decreased, or their side effects managed another way; the dose cannot be increased. For some patients, the therapeutic index can be improved by altering the mode of administration. For example, patients with side effects at the peak of exposure to a short-acting opioid, may do better with smaller more frequent doses, or with a long-acting opioid. In contrast, patients on long-acting opioids with side effects during periods of minimal pain may do better on intermittent doses of a short-acting opioid. Finally, some patients cannot find a dose that allows them to enjoy pain relief without significant side effects. Those patients are candidates for opioid rotation. If a therapeutic index cannot be found with a few opioids for an individual patient, that patient is probably not a candidate for opioid therapy, and should be moved to “exit strategy.”
iii. Add Long-Acting Opioid
There is little if any evidence that long-acting opioids are better in general than short-acting opioids for patients with chronic pain. However, there are particular types of patients for whom the addition of a long-acting opioid to a short-acting one, or even the substitution of long-acting for short-acting, may improve clinical outcomes. The clearest example is the patient who is taking substantial doses of short-acting opioids multiple times per day. Since tolerance is often first manifested by decreased duration of action, such patients may be forced to take their medication every three or even two hours. The addition of a long-acting agent may be extremely helpful. Another example is the patient with a compliance problem, due either to cognitive issues or abuse-related problems. Stopping the short-acting medication and substituting a long-acting medication may allow such patients to continue to benefit from opioid therapy in a manner that reduces risk. It is important for clinicians to realize that all currently marketed opioids can be abused, and substituting a long-acting opioid for a short-acting one may reduce risk in some circumstances but will not eliminate the risk. Furthermore, some long-acting opioids, such as extended-release oxycodone, are highly prized by abusers.
iv. Opioid Rotation
Tools: Opioid Rotation
(Note: Tools or links to tools are available in the Appendix) It has been observed that individual patients may do poorly on one opioid but better after switching to another. Various explanations have been offered for this phenomenon. One holds that since some opioids are associated with the accumulation of toxic metabolites after prolonged use (e.g. morphine, hydromorphone), switching to another allows for the clearance of metabolites accumulated from the first opioid. Another theory is that different opioids may bind in different patterns to subtypes of the opioid receptor, providing different profiles of efficacy and side effects. Regardless, if a patient can not seem to
17
find an effective and well tolerated dose of one opioid, it is reasonable to try one or two more opioids before giving up on opioid therapy or referring to a specialist for further management. It is of critical importance to note that switching patients who are on substantial doses of one opioid to another opioid can be tricky, and if done inappropriately can lead to under-dosing and severe pain flare or frank withdrawal, or to overdose and death, particularly with methadone. Guidelines for opioid rotation are presented elsewhere. Clinicians should have a clear sense of their comfort zone with opioid rotation and should get input as needed. v. Exit Strategy
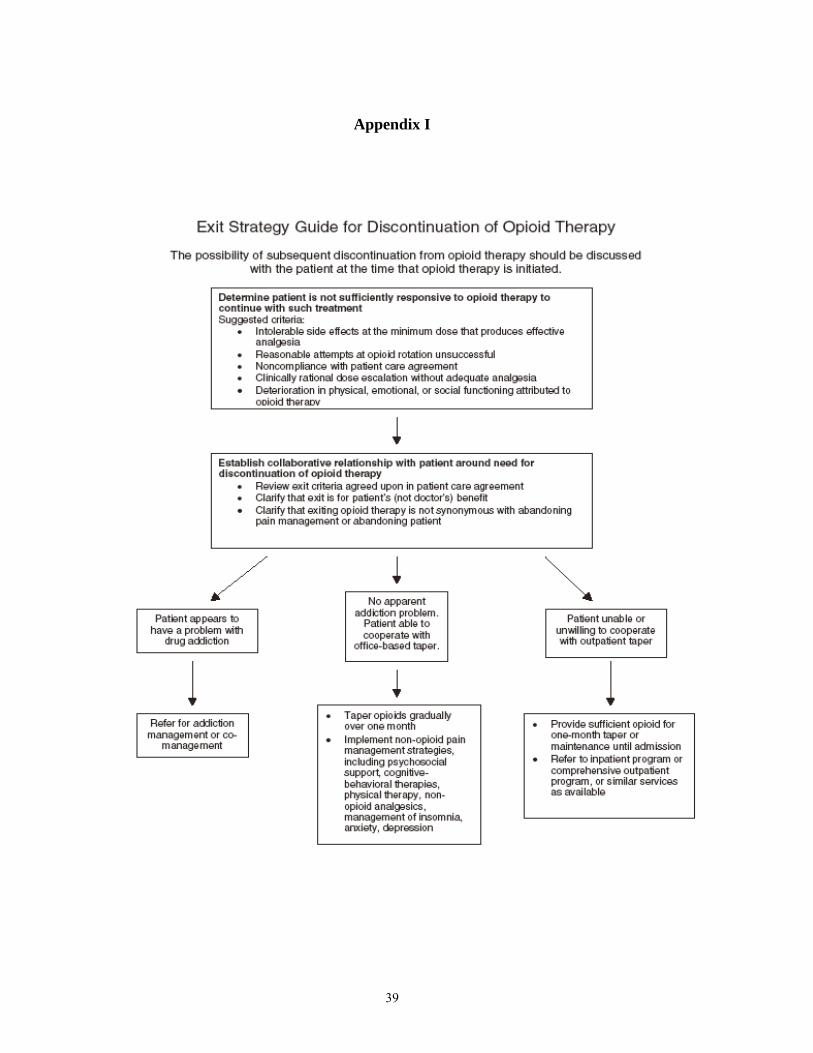
Tools: Exit Guide
(Note: Tools or links to tools are available in the Appendix) When is appropriate to give up on opioid therapy in an individual patient? While there has been little guidance on this issue, the following list of criteria are reasonable: • There has been no convincing benefit from opioid therapy despite
reasonable attempts at dose adjustment, management of side effects, and opioid rotation.
• Opioids cannot be tolerated at a dose that provides meaningful analgesia. • Persistent compliance problems despite a patient treatment agreement and
appropriate limit setting. • Presence of a co-morbid condition that makes opioid therapy more likely
to harm than help, such as an active substance abuse problem. (Note that the risk-benefit of opioid therapy depends as much on the treatment setting as on the patient and the medicine.)
It is critically important to distinguish between abandoning opioid therapy, abandoning pain management, and abandoning the patient. Exiting a patient from opioid therapy is often difficult for clinicians because of the failure to understand that when this decision is made, it is for the welfare of the patient, not for the welfare of the doctor. Approaching the need to taper off opioid therapy from the perspective of helping the patient helps avoid many (but not all) awkward confrontations. There are many other approaches to pain management than opioid therapy, and a patient can be tapered off from opioid therapy while alternative pain management approaches are aggressively pursued (albeit with reasonable expectations). Also, abandoning opioid therapy does not mean abandoning the patient. Often the most reasonable course is to offer the patient continued medical guidance (without opioid therapy), even in the case of an addicted patient who pursues co-management of the addictive disorder. Of course, in certain cases the patient’s behavior is so disruptive, or frankly criminal, that a productive clinician-patient relationship is no longer possible, and even that law enforcement personnel must be called in. In such cases, discharge from the practice, with appropriate
18

recommendations for alternative care, and sufficient opioids to taper off, is the best course of action.
Myth: Abandoning opioid therapy means you are abandoning the patient. Reality: It may be in the best interest of the patient to abandon opioid
therapy, and to continue aggressive but non-opioid pain management approaches.
Myth: Opioids should be provided if “nothing else works.” Reality: Opioids, like all other treatments, should be provided only when
they are helpful, and when their benefits outweigh their risks. There are as many different recipes for taking patients off opioids as there are physicians who have done it. From the perspective of the primary care physician the main issue is to decide who can be tapered in primary care, who needs consultation, and who needs the process conducted in specialty hands, inpatient or outpatient. While there are no hard and fast guidelines for how to determine which is the case, a few simple rules of thumb will be helpful. The patient who tends to taper well in primary care is the patient with a clear cut pain syndrome that is not severe or that is resolving spontaneously, who is willing to collaborate in the process of coming off opioids, and who has no significant past or present psychiatric or substance abuse problems. Such patients can simply be prescribed a tapering schedule of their current opioid with the plan of coming off over a 2-3 week period of time. Patients should be warned that due to opioid withdrawal, whether overt or subtle, they will likely experience mood disturbances, insomnia, lack of energy, irritability, aches and pains, bowel disturbances, and perhaps an increase in their pain. It is critical to educate the patient that any worsening of their pain syndrome during the taper may not reflect a benefit of the opioids, but may simply be a sign of coming off – the only way to know how their pain feels in the absence of opioids is to come off and stay off for a period of at least a few months. Patients (and physicians) often make the mistake of concluding that increased pain during the tapering process means that the opioid was actually helping the pain. While this is certainly possible, the worsening pain may in fact be a manifestation of subtle withdrawal, and the only way to find out is to stick with the taper. Many patients find that after a few months, their pain subsides to quite manageable levels in the absence of opioid therapy. However, it takes a great deal of hand-holding by the physician to get through the process. The physician can support the patient through the tapering process in many different ways. Frequent office visits, reassurance that things will get better, non-opioid pain management approaches (ice, heat, rest, acupuncture, physical therapy, non-opioid analgesics), and treatment for the symptoms that may emerge during opioid tapering (insomnia, anxiety, etc) will all help. Clonidine is a non-specific medication that can reduce the symptoms of withdrawal, which may be quite helpful. Although providing non-addicting medications during withdrawal is a wise course, a short course of
19
benzodiazepines during opioid tapering to help with anxiety, irritability, or insomnia is often worthwhile. Other symptoms may emerge during opioid tapering (such as depression) that may need to be managed directly. Some patients are less likely to do well during the outpatient opioid taper in primary care. These are patients with past or current addiction problems, somatoform pain disorders, or concurrent mental health issues. In these cases a consultation with a specialist in opioid tapering (either from an addiction perspective or a pain management perspective) is necessary. Often patients will do much better in an inpatient program, in which they can learn non-opioid pain management techniques during the taper, and where their access to medications can be controlled. There are also similar outpatient programs available.
G. Consultation and Referral
The physician should be willing to refer the patient as necessary for additional evaluation and treatment in order to achieve treatment objectives. Knowing that the management of pain in patients with a history of substance abuse or with a comorbid psychiatric disorder may require extra care, monitoring, documentation, and consultation with or referral to an expert in the management of such patients. Again, special attention should be given to those pain patients who are at risk for misusing their medications and those whose living arrangement pose a risk for medication misuse or diversion. Patients who are abusing alcohol, prescription medications, or illegal drugs should always be referred to substance abuse professionals or programs. Various options are available in different areas of the country and options may include inpatient or an outpatient treatment program, depending on the severity of dependence, availability of facilities, insurance coverage, and other considerations. Some facilities specialize only in detoxification or long-term treatment; others provide both. It is helpful to have a list of resources available, along with addresses and telephone numbers, so that referrals can be made quickly and easily. Alcoholics Anonymous and Narcotics Anonymous offer another option and provide ongoing support. Essential to the success of substance abuse referrals is willingness on the part of the patient to acknowledge that there is a problem. If the patient refuses the referral, he or she may be in denial about the substance abuse problem. Nevertheless, it is important for the physician to render an opinion on the matter and recommend treatment if it appears to be indicated. Some leverage can be gained by making ongoing treatment contingent upon the patient’s participation in a substance abuse program of some type. Treatment contracts are helpful in these situations. The physician has the option of refusing to prescribe drugs for a patient who is believed to be abusing substances, and if the patient continues to refuse to confront the substance abuse problem, the doctor may decide to terminate the relationship altogether. A multidisciplinary team is ideal for the management of substance abuse and misuse in the medical or pain treatment setting. A meta-analysis of 65 studies clearly demonstrated that multidisciplinary treatment for chronic pain is superior to no treatment, waiting list, and single-discipline treatments such as medical treatment or
20
physical therapy (Flor et al., 1992). A multidisciplinary pain management program combines medical management with physical and psychological treatment, education, and rehabilitation. Unfortunately the number of multidisciplinary pain programs in the country are limited and it can be difficult to obtain insurance approval for payment of this approach. In this case it may be necessary for a physician to make individual referrals to allied professionals. Managing patients with pain and substance abuse in isolation can be a frustrating experience and can lead to feelings of anger, defensiveness, and frustration. Building a network of colleagues and referral sources can help alleviate these feelings. It is beneficial for these physicians to establish a collective of complementary practitioners in their geographical locale with whom they can refer patients for the purpose of receiving supplementary services for pain control and maintain a modicum of team-based support. Mental health professionals with specialization in the area of addiction are usually instrumental in developing and executing strategies for behavioral management and treatment compliance. Physical and occupational therapists can also play a significant role in helping the patient to achieve goals and improve their quality of life. H. Documentation As in all cases, but especially when treating high risk patients and those with SUDs, the physician should keep accurate and complete records. Within the records the following information should be included: (1) the medical history and physical examination (2) diagnostic, therapeutic and laboratory results (3) evaluations and consultations (4) treatment objectives (5) discussion of risks and benefits (6) treatments (7) medications [including date, type, dosage, and quantity prescribed] (8) instructions and agreements and (9) periodic reviews. Records should remain current and be maintained in an accessible manner and readily available for review. I. Protecting Collaterals and the Community Unlike many other medications, prescribed opioids have the potential to harm not only the patient but members of the patient’s family and the community at large. Physicians fulfilling their obligation to relieve pain by prescribing opioids, which is a necessary part of clinical practice, cannot ignore their responsibility to minimize the negative impact of such prescribing on the community into which the prescription is directed. Physicians can also no longer ignore the reality that opioid prescribing appears to be a significant source of diverted prescription opioids. There are many pathways for such diversion. Patients themselves may abuse their own prescriptions, whether or not they have a pain problem. Patients may also share or sell their prescriptions with friends, family, acquaintances, strangers, or drug dealers. Burglars are known to seek prescription drugs with a level of interest matched only by cash, jewelry, and firearms. One of the major sources of prescription opioids by adolescents, the major demographic at risk for prescription opioid abuse, is the medicine cabinet of their own household or that of their friends and neighbors. While
21
these examples relate to intentional abuse, accidental ingestions are another safety issue for family and community. Among the pathways to accidental ingestion by children or others are the transfer of medications to non-childproof containers, leaving medicine bottles lying around, or leaving children in the custody of grandparents or other caretakers who do not take measures to secure their medications, often because they do not have children in the house.
The first step in protecting collaterals and the community involves practicing opioid management responsibly, by following the steps outlined throughout this document. The second step involves educating the patient around their own responsibilities to protect those around them from consequences of inappropriate opioids use. Following are a list of suggested points to be made in communicating about opioid prescribing with patients. These points can be delivered in one-on-one sessions, in signs and placards posted in the office, in patient education brochures, or by other means. These represent only key points that may not be covered in many educational brochures; there are a number of additional points that are generally covered in patient treatment agreements or educational materials and are not repeated here.
• Opioids are safe and effective when used as prescribed. However, the epidemic of
prescription opioid abuse requires that patients assume a level of responsibility with opioids that is different from most other medications, to avoid problems in their families and community.
• Prescription opioids should be secured like cash or jewelry, in a lock box or safe, not in a medicine cabinet or night table drawer.
• Transferring prescription opioids to non-childproof containers, such as pill reminder units, should be avoided whenever possible, to avoid accidental pediatric ingestion.
• Extra pills left over after they are no longer needed (such as for acute pain, flares of chronic pain, or after switching to another medication) should be disposed of (flushing down the toilet is the best method), and the disposal should be reported to and documented by the physician.
• Sharing of controlled prescription medications, even with the best of intentions for friends and family for legitimate needs, is a felony in the United States. Patients should be advised that this offense will be reported by the doctors’ office to the police.
• Patients who persistently violate their patient treatment agreement cannot be safely prescribed opioids, and will not be able to receive them.
• Patients must take responsibility for understanding what medications they are on, why they are on them, what dose they are on, and how they take them. This is best tracked on a written list that is updated whenever the prescription changes. Patients who are unable to comply with this requirement cannot be prescribed opioids (or anything else) safely.
Widespread adoption of guidelines such as these is the only way that the clinical community will be able to preserve its hard won right to relieve pain through the prescribing of opioids,
22

and is the only way to protect those of our patients who deserve continued access to this essential therapeutic agent.
V. Summary Pain patients with current, past, or potential for substance abuse can pose a management challenge for physicians. However, these patients’ pain can and should be treated with the same degree of efficacy and compassion as any other patient. The decision to implement a trial of opioid therapy should involve the physician’s clinical judgement, collateral input from multidisciplinary team members when possible, and data from available empirically sound assessment and screening tools which have been designed to aid in this process. Terms of a trial therapy period should be clearly outlined and expectations regarding behavior, limits, consequences, and stipulations should be clearly outlined and agreed upon at the outset. A behavioral or opioid contact may be helpful in establishing this agreement. This process should be clearly documented. Treatment requires ongoing assessment and modifications of the treatment plan and agreed upon contract as needed. Any violations of a contract must be addressed immediately and the consequences followed through without exception. While prescribing or dispensing chronic opioids, it is essential that particular attention is paid to the assessment of a patient’s clinical outcomes such as degree of pain relief, level of psychosocial and physical functioning, extent of medication side effects, and the presence of potentially problematic substance use behavior. Treatment agreements, behavioral contracts and contingency approaches should be tailored to address the nature, function, and severity of substance abuse or misuse. Fostering an environment of open and honest communication among all parties provides reassurance that guidelines are well established and will engender a focus on achieving shared treatment goals. VI. References American Pain Society. Definitions Related to the Use of Opioids for the Treatment of Pain: A consensus document from the American Academy of Pain Medicine, the American Pain Society, and the American Society of Addiction Medicine. 2001. Available at: http://www.ampainsoc.org/advocacy/opioids2.htm. Accessed January 6, 2006. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Text Revision. Washington, DC: American Psychiatric Press Inc; 2000. Brown RL, Patterson JJ, Rounds LA, Papasouliotis O. Substance abuse among patients with chronic back pain. J Fam Pract. 1996;43(2):152-160. Brown RL, Rounds LA. Conjoint screening questionnaires for alcohol and drug abuse. Wisconsin Medical Journal. 1995;94:135-140. Butler SF, Budman SH, Fernandez K, Jamison RN. Validation of a screener and opioid assessment measure for patients with chronic pain. Pain. 2004;112, 65-75.
23
Chabal C, Erjavec MK, Jacobson L, Mariano A, Chaney E. Prescription opiate abuse in chronic pain patients: clinical criteria, incidence, and predictors. Clin J Pain. 1997;13:150-5. Coambs RB, Jarry JL. The SISAP: a new screening instrument for identifying potential opioid abusers in the management of chronic nonmalignant pain in general medical practice. Pain Res Manage. 1996;1:15-162. Controlled Substances Act of 1970. Pub L No. 91513, 84 Stat 1242. Drug Abuse Warning Network. (2002). ED trends from DAWN: Final estimates 1995-2002. Acailable at: http://dawninfo.samhsa.gov/. Accessed December 14, 2005. Dunbar SA, Katz NP. Chronic opioid therapy for nonmalignant pain in patients with a history of substance abuse. Report of 20 cases. Journal of Pain and Symptom Management. 1996;11:163-171. Federation of State Medical Boards of the United States. Model Guidelines for the Use of Controlled Substances for the Treatment of Pain. Dallas, Tex: Federation of State Medical Boards; May 1998. Available at: http://www.fsmb.org. Accessed January 15, 2006. Fine PG, Portenoy RK. A clinical guide to opioid analgesia. Minneapolis, MD: The McGraw-Hill Companies; 2004. Fishbain DA. Treatment of pain in addicts. Paper presented at: National Institute of Substance Abuse Technical Review, 1993, Bethesda, Md. Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS. Validity of self-reported drug use in chronic pain patients. Clin J Pain. 1999;15(3):184-191. Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review. Pain. 1992;49(2):221-30. Fudin J, Levasseur DJ, Passik SD, Kirsh KL, Coleman J. Chronic Pain Management with Opioids in Patients with Past or Current Substance Abuse Problems. Journal of Pharmacy Practice. 2003;16;4:291-308. Gonzales GR, Coyle N: Treatment of cancer pain in a former opioid abuser: fears of the patient and staff and their influence on care. Journal of Pain and Symptom Management. 1992;7:246-9. Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being: A World Health Organization Study in Primary Care. JAMA. 1998;280:147-51.
24

Hays L, Kirsh KL, Passik SD. Seeking drug treatment for Ocycontin abuse: A chart review of consecutive admissions to a substance abuse treatment facility in Kentucky. Journal of the National Comprehensive Cancer Network. 2003;1:1-6. Hoffmann NG, Olofsson O, Salen B, Wickstrom L. Prevalence of abuse and dependency in chronic pain patients. Int J Addict. 1995;30:919-927. Jamison RN, Kauffman J, Katz NP. Characteristics of. methadone maintenance patients with chronic pain. Journal of Pain and Symptom Management. 2000;19:53-62. Kaiko RF, Foley KM, Grabinski PY, et al. Central nervous system excitatory effects of meperidine in cancer patients. Ann Neurol. 1983;13:180-5. Katz N, Fanciullo GJ. Role of urine toxicology testing in the management of chronic opioid therapy. Clin J Pain. 2002;18(suppl):S76-S82. Kouyanou K, Pither CE, Wessely S. Medication misuse, abuse and dependence in chronic pain patients. J Psychosom Res. 1997;43(5):497-504. Medina JL, Diamond S: Drug dependency in patients with chronic headaches. Headache. 1977;17:12-4. National Institute on Drug Abuse. Pain Medications: 13553. Available at: www.165.112.78.61/infofax/painmed.html. Accessed January 6, 2006. Ohayon MM, Schatzberg AF. Using chronic pain to predict depressive morbidity in the general population. Arch Gen Psychiatry. 2003;60:39-47. Ospina M, Harstall C. Prevalence of Chronic Pain: an Overview. Alberta Heritage Foundation for Medical Research, Health Technology Assessment. Edmonton, AB: 2002; Report No. 28. Passik SD, Kirsh KL. Assessing Aberrant Drug-taking Behaviors in the Patient with Chronic Pain. Current Pain and Headache Reports. 2004;8(4):289-94. Perry S, Heidrich G: Management of pain during debridement: a survey of U.S. burn units. Pain. 1982;13:267-80. Porter J, Jick H: Addiction rare in patients treated with narcotics. N Engl J Med. 1980;302: 123. Portenoy RK, Foley KM. Chronic use of opioid analgesics in non-malignant pain: report of 38 cases. Pain. 1986;25(2):171-86. Portenoy RK, Payne R. Acute and chronic Pain. In: Lowinson JH, Ruiz P, Millman RB, Landrod JG, eds. Substance Abuse: A Comprehensive Textbook, 3rd ed. Baltimore, MD: Williams & Wilkins; 1997:563-589.
25
Potter JS, Hennessy G, Borrow JA, Greenfield SF, Weiss RD. Substance use histories in patients seeking treatment for controlled-release oxycodone dependence. Drug and Alcohol Dependence. 2004;76:213-215. Rafii A, Haller D, Poklis A. Incidence of recreational drug use among chronic pain clinic patients. Abstract No. 33. Presented at the American Pain Society Ninth Annual Meeting. 1990. Reid MC, Engles-Horton LL, Weber MB et al. Use of opioid medications for chronic noncancer pain syndromes in primary care. J Gen Intern Med. 2002;17:173-179. Rosenblum A, Joseph H, Fong C, et al. Prevalence and characteristics of chronic pain among chemically dependent patients in methadone maintenance and residential treatment facilities. JAMA. 2003;289:2370–2378. Substance Abuse and Mental Health Services Administration. 2004: Latest National Survey on Drug Use & Health. Available at: http://www.oas.samhsa.gov/nhsda.htm. Accessed December 14, 2005. Weaver M, Schnoll S. Abuse liability in opioid therapy for pain treatment in patients with an addiction history. Clin J Pain. 2002;18(4 suppl):S61 –S69.
26
Appendix A
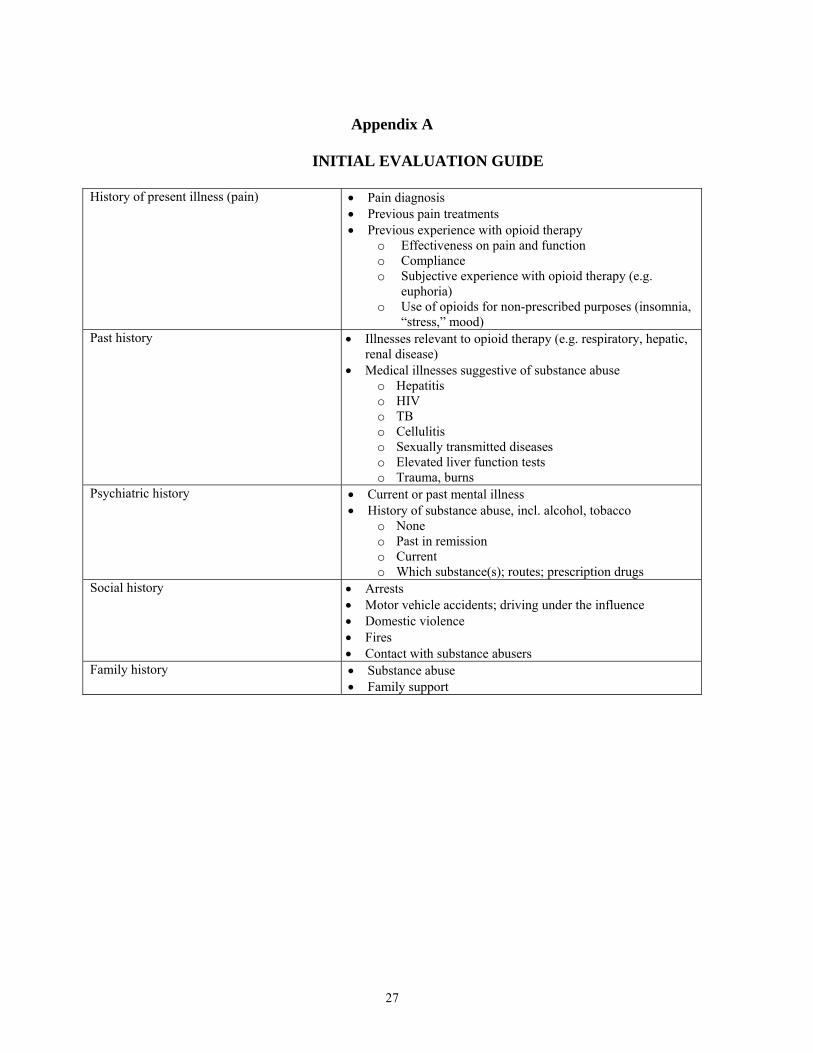
INITIAL EVALUATION GUIDE
History of present illness (pain) • Pain diagnosis • Previous pain treatments • Previous experience with opioid therapy
o Effectiveness on pain and function o Compliance o Subjective experience with opioid therapy (e.g.
euphoria) o Use of opioids for non-prescribed purposes (insomnia,
“stress,” mood) Past history • Illnesses relevant to opioid therapy (e.g. respiratory, hepatic,
renal disease) • Medical illnesses suggestive of substance abuse
o Hepatitis o HIV o TB o Cellulitis o Sexually transmitted diseases o Elevated liver function tests o Trauma, burns
Psychiatric history • Current or past mental illness • History of substance abuse, incl. alcohol, tobacco
o None o Past in remission o Current o Which substance(s); routes; prescription drugs
Social history • Arrests • Motor vehicle accidents; driving under the influence • Domestic violence • Fires • Contact with substance abusers
Family history • Substance abuse • Family support
27
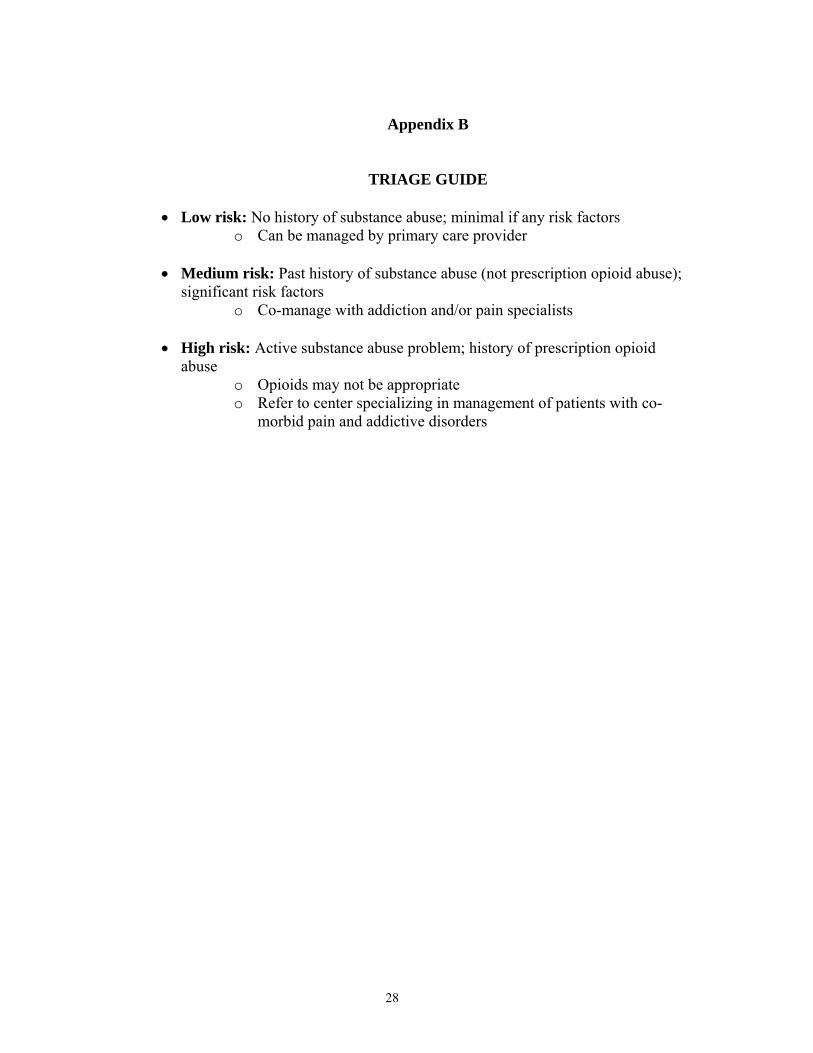
Appendix B
TRIAGE GUIDE
• Low risk: No history of substance abuse; minimal if any risk factors o Can be managed by primary care provider
• Medium risk: Past history of substance abuse (not prescription opioid abuse); significant risk factors
o Co-manage with addiction and/or pain specialists
• High risk: Active substance abuse problem; history of prescription opioid abuse
o Opioids may not be appropriate o Refer to center specializing in management of patients with co-
morbid pain and addictive disorders
28
Appendix C
Screener and Opioid Assessment for Patients with Pain (SOAPP®) Version 1.0
The Screener and Opioid Assessment for Patients with Pain (SOAPP) Version 1.0 is a tool for clinicians to help determine how much monitoring a patient on long-term opioid therapy might require. Physicians remain reluctant to prescribe opioid medication because of concerns about addiction, misuse, and other aberrant medication-related behaviors, as well as liability and censure concerns. Despite recent findings suggesting that most patients are able to successfully remain on long-term opioid therapy without significant problems, physicians often express a lack of confidence in their ability to distinguish patients likely to have few problems on long-term opioid therapy from those requiring more monitoring.
SOAPP version 1.0 is a quick and easy-to-use questionnaire designed to help providers evaluate the patients’ relative risk for developing problems when placed on long-term opioid therapy. Version 1.0 is:
• A brief paper and pencil questionnaire • Developed based on expert consensus regarding important concepts likely to predict which patients will
require more or less monitoring on long-term opioid therapy (content and face valid) • Preliminary reliability data (coefficient α) from 175 patients chronic pain patients • Preliminary validity data from 100 patients (predictive validity) • Simple scoring procedures • 24 items • 5 point scale • <10 minutes to complete • Ideal for documenting decisions about the level of monitoring planned for a particular patient or
justifying referrals to specialty pain clinic. • The SOAPP is for clinician use only. The tool is not meant for commercial distribution. • The SOAPP is NOT a lie detector. Patients determined to misrepresent themselves will still do so.
Other clinical information should be used with SOAPP scores to decide on a particular patient’s treatment.
• The SOAPP is NOT intended for all patients. The SOAPP should be completed by chronic pain patients being considered for opioid therapy.
• It is important to remember that all chronic pain patients deserve treatment of their pain. Providers who are not comfortable treating certain patients should refer those patients to a specialist.
29
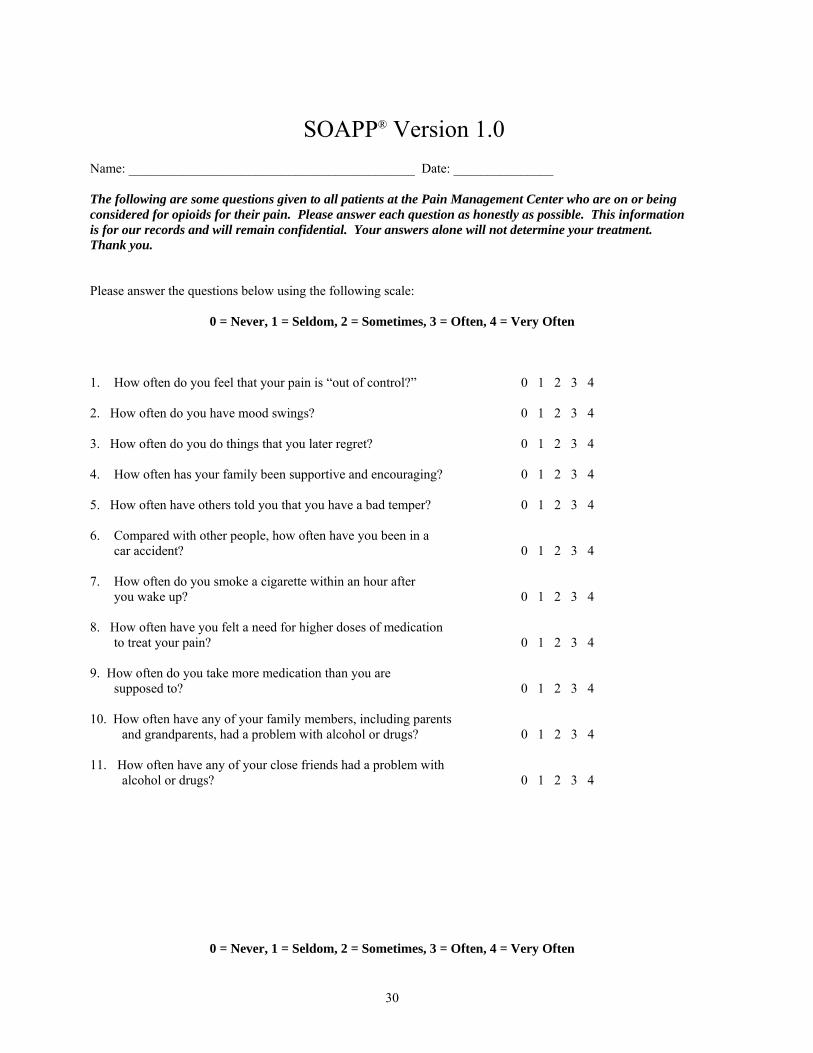
SOAPP® Version 1.0 Name: ___________________________________________ Date: _______________ The following are some questions given to all patients at the Pain Management Center who are on or being considered for opioids for their pain. Please answer each question as honestly as possible. This information is for our records and will remain confidential. Your answers alone will not determine your treatment. Thank you. Please answer the questions below using the following scale:
0 = Never, 1 = Seldom, 2 = Sometimes, 3 = Often, 4 = Very Often 1. How often do you feel that your pain is “out of control?” 0 1 2 3 4 2. How often do you have mood swings? 0 1 2 3 4 3. How often do you do things that you later regret? 0 1 2 3 4 4. How often has your family been supportive and encouraging? 0 1 2 3 4
5. How often have others told you that you have a bad temper? 0 1 2 3 4 6. Compared with other people, how often have you been in a
car accident? 0 1 2 3 4 7. How often do you smoke a cigarette within an hour after
you wake up? 0 1 2 3 4 8. How often have you felt a need for higher doses of medication
to treat your pain? 0 1 2 3 4 9. How often do you take more medication than you are
supposed to? 0 1 2 3 4 10. How often have any of your family members, including parents
and grandparents, had a problem with alcohol or drugs? 0 1 2 3 4
11. How often have any of your close friends had a problem with alcohol or drugs? 0 1 2 3 4
0 = Never, 1 = Seldom, 2 = Sometimes, 3 = Often, 4 = Very Often
30
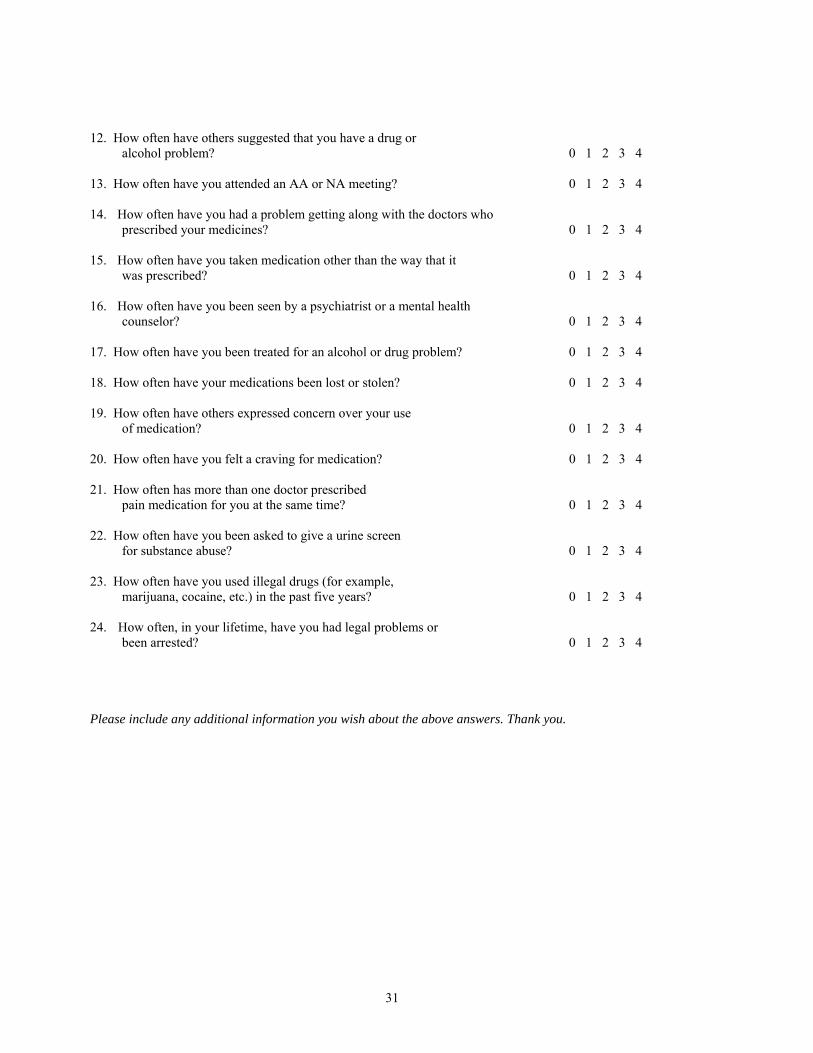
12. How often have others suggested that you have a drug or
alcohol problem? 0 1 2 3 4 13. How often have you attended an AA or NA meeting? 0 1 2 3 4 14. How often have you had a problem getting along with the doctors who
prescribed your medicines? 0 1 2 3 4
15. How often have you taken medication other than the way that it was prescribed? 0 1 2 3 4
16. How often have you been seen by a psychiatrist or a mental health
counselor? 0 1 2 3 4 17. How often have you been treated for an alcohol or drug problem? 0 1 2 3 4 18. How often have your medications been lost or stolen? 0 1 2 3 4 19. How often have others expressed concern over your use
of medication? 0 1 2 3 4
20. How often have you felt a craving for medication? 0 1 2 3 4 21. How often has more than one doctor prescribed
pain medication for you at the same time? 0 1 2 3 4 22. How often have you been asked to give a urine screen
for substance abuse? 0 1 2 3 4
23. How often have you used illegal drugs (for example, marijuana, cocaine, etc.) in the past five years? 0 1 2 3 4
24. How often, in your lifetime, have you had legal problems or
been arrested? 0 1 2 3 4 Please include any additional information you wish about the above answers. Thank you.
31
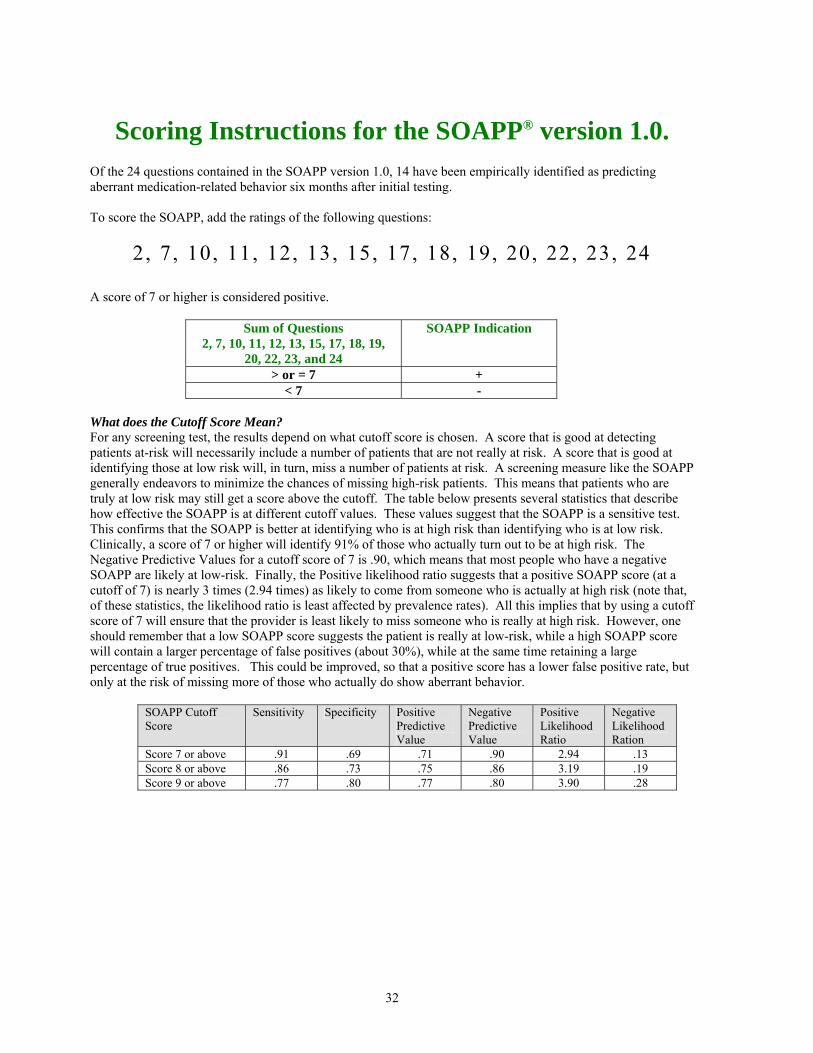
Scoring Instructions for the SOAPP® version 1.0. Of the 24 questions contained in the SOAPP version 1.0, 14 have been empirically identified as predicting aberrant medication-related behavior six months after initial testing. To score the SOAPP, add the ratings of the following questions:
2 , 7, 10, 11, 12, 13, 15, 17, 18, 19, 20, 22, 23, 24
A score of 7 or higher is considered positive.
Sum of Questions 2, 7, 10, 11, 12, 13, 15, 17, 18, 19,
20, 22, 23, and 24
SOAPP Indication
> or = 7 + < 7 -
What does the Cutoff Score Mean? For any screening test, the results depend on what cutoff score is chosen. A score that is good at detecting patients at-risk will necessarily include a number of patients that are not really at risk. A score that is good at identifying those at low risk will, in turn, miss a number of patients at risk. A screening measure like the SOAPP generally endeavors to minimize the chances of missing high-risk patients. This means that patients who are truly at low risk may still get a score above the cutoff. The table below presents several statistics that describe how effective the SOAPP is at different cutoff values. These values suggest that the SOAPP is a sensitive test. This confirms that the SOAPP is better at identifying who is at high risk than identifying who is at low risk. Clinically, a score of 7 or higher will identify 91% of those who actually turn out to be at high risk. The Negative Predictive Values for a cutoff score of 7 is .90, which means that most people who have a negative SOAPP are likely at low-risk. Finally, the Positive likelihood ratio suggests that a positive SOAPP score (at a cutoff of 7) is nearly 3 times (2.94 times) as likely to come from someone who is actually at high risk (note that, of these statistics, the likelihood ratio is least affected by prevalence rates). All this implies that by using a cutoff score of 7 will ensure that the provider is least likely to miss someone who is really at high risk. However, one should remember that a low SOAPP score suggests the patient is really at low-risk, while a high SOAPP score will contain a larger percentage of false positives (about 30%), while at the same time retaining a large percentage of true positives. This could be improved, so that a positive score has a lower false positive rate, but only at the risk of missing more of those who actually do show aberrant behavior.
SOAPP Cutoff Score
Sensitivity Specificity Positive Predictive Value
Negative Predictive Value
Positive Likelihood Ratio
Negative Likelihood Ration
Score 7 or above .91 .69 .71 .90 2.94 .13 Score 8 or above .86 .73 .75 .86 3.19 .19 Score 9 or above .77 .80 .77 .80 3.90 .28
32

Appendix D Sample Patient Treatment Agreement
Click on these links for sample patient treatment agreements
http://www.painmed.org/productpub/statements/index.html (American Academy of Pain Medicine);
http://www.painedu.org/components/Agreement.pdf
33
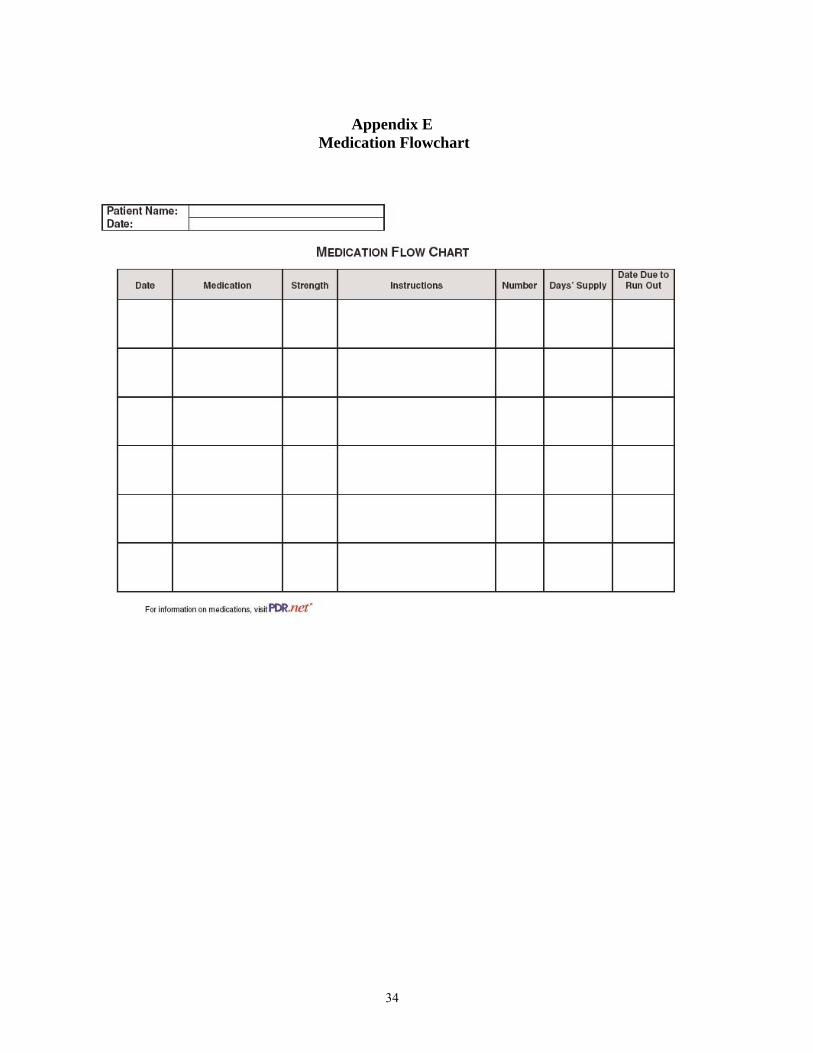
Appendix E Medication Flowchart
34

Appendix F
Patient Education
Click on this link for a patient education brochure http://www.endo.com/PDF/Understand_Pain_Opioid_Analgesics.pdf
35
Appendix G
36

37
Appendix H
Click on these links for information on opioid rotation
http://www.stoppain.org/pcd/content/forpros/individual.asp ; http://www.stoppain.org/pcd/content/forpros/EquianalgesicOpioidDoses.pdf http://www.stoppain.org/pcd/content/forpros/EmpiricalGuidelinesforOpioidRotation.pdf
38
Appendix I
39





























