Embed Size (px)
Citation preview
Patient experiences of COPD: the impacts of interactions with
health professionals
Dr Cathy Bulley, Dr Lisa Salisbury,
Ms Suzanne Whiteford,
Prof Marie Donaghy,Ms Elaine MacKay
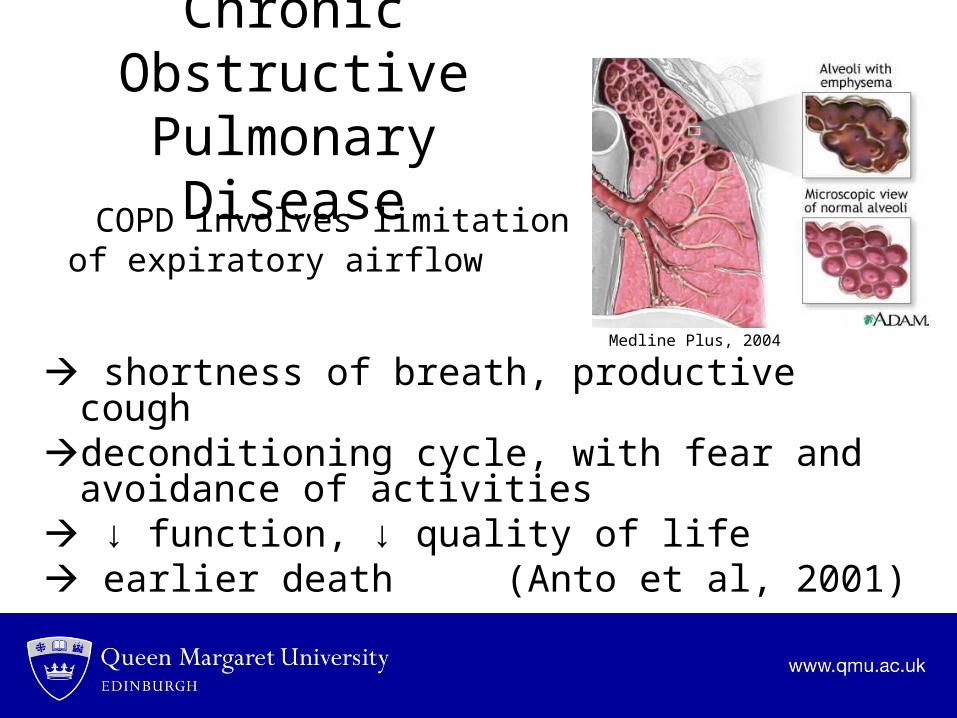
Chronic Obstructive Pulmonary Disease
COPD involves limitation of expiratory airflow
shortness of breath, productive coughdeconditioning cycle, with fear and avoidance of
activities ↓ function, ↓ quality of life earlier death (Anto et al, 2001)
Medline Plus, 2004
Extent of the Problem
• Global prevalence estimate: 9.3/1000 for men; 7.3/1000 for women
• Expected that in 2020 this will be the third most prominent cause of death (WHO, 1995; Murray & Lopez, 1997)
• Sub-optimal management over-reliance on acute care (Wouters, 2003)
Supporting Self-Management
• ↑ emphasis on management of long-term conditions
• Individuals can learn better ways of coping with COPD
• Pulmonary rehabilitation aims to maximise function using: (BTS, 2001)
exercise training, education and support in symptom control
Evidence and Participation• There is strong evidence of the
efficacy of pulmonary rehabilitation (Lacasse et al, 2006)
• BUT benefits depend on participation – varies from 40% to 66% (e.g. Young et al, 1999)
• Minimal research into patterns of participation
Greater understanding of decisions is needed
This study…Aim:
• to explore individuals’ experiences of COPD and its management PRIOR to attending pulmonary rehabilitation
Focus of this abstract:
• The impacts of interactions with health professionals on experiences and views about attending pulmonary rehabilitation
Study Design• Qualitative; Phenomenological • Interpretative Phenomenological Analysis (IPA)
(Conrad, 1987)Gain understanding of the patient’s perspective
through co-construction between the participant and researcher
• Single semi-structured person-person interview in participant’s home (Grbich, 1999): 50-90 minutes
Participants• Individuals with COPD accepting referral to
Pulmonary Rehabilitation during clinic visit
• Purposive selection to ensure men and women
• 10 participants sought, 9 participated (5 men, 4 women)
• White Caucasians living in Glasgow, aged 59-82
• Ethical approval granted (Multi-Centre REC)
Analysis
• Interpretative Phenomenological Analysis framework
Classification of views and experiences (themes)
Interrelationships between themesQSR N6 package for data management2 researchers to increase trustworthiness
Results: Positive Interactions
• Positive interactions with health professionals: Provision of effective advice on coping with
symptoms (paramedics, nurses, physiotherapists)Feelings of faith in health professionalsPositive expectations of further
management, including
pulmonary rehabilitation
Results: Negative Interactions
• Absence of advice (except about smoking) from medical staff
feelings of being dismissed perception that specialist
management is a waste of
time and energy The burden of pulmonary
rehabilitation may > benefit
Referral Practices: • views about attending pulmonary rehabilitation
were more positive when: Referrers stated how wonderful the results are
(non-specific…)
• views about attending pulmonary rehabilitation were more negative when:
Referrers were vague about content
(e.g. – “there’s exercise…”)
Follow-up…• Information on actual attendance – Non-attendance due to inappropriate referral (1) poor
referral coordination (1) and a clash with another research study (1) and for no stated reason (1)
Non-completion due to infection / co-existing conditions – mobility, depression (2)
Completion despite interruptions due to infection (3)This made follow-up interviews (6) of limited use
Conclusions• All our interactions impact on individuals’
beliefs and perceptions regarding management

What can we do? • Improve referral practices… Ideally: emphasise that pulmonary rehabilitation
aims to increase function and independence using education and advice, individually tailored and expertly supervised
exercise, and group supportconcerns about attending? At the very least – express enthusiasm!

Thank you for your attention!
• Acknowledgments:
School of Health Sciences, Queen Margaret University, Edinburgh
Centre for Integrated Healthcare Research, Edinburgh
References• Anto, J., Vermeire, P., Vestbo, J., & Sunyer, J. (2001). Epidemiology of chronic
obstructive pulmonary disease. Eur Respir J, 17, 982-994.• British Thoracic Society. (2001). BTS Standards of Care Subcommittee on Pulmonary
Rehabilitation. BTS Statement: Pulmonary Rehabilitation. Thorax, 56, 827-834.• Conrad, P. (1987). The experience of illness: Recent and new directions. Res Sociol
Health Care, 6, 1-31.• Grbich, C. (1999). Qualitative research in health: an introduction. London: Sage
Publications Ltd.• Lacasse, Y., Brousseau, L., Milne, S., et al. (2006). Pulmonary rehabilitation for chronic
obstructive pulmonary disease. The Cochrane Database of Systematic Reviews. (Issue 2, Art. No.: CD003793, DOI: 10.1002/14651858, CD003793)
• Medline Plus (2004) Medical Encyclopedia: Emphysema, National Library of Medicine (NLM). Online at: http://www.nlm.nih.gov/medlineplus/copyright.html [Accessed 19/03/2007].
• Murray, C., & Lopez, A. (1997). Alternative projections of mortality and disability by cause 1990-2020: Global burden of disease study. Lancet, 349, 1498-1504.
• World Health Organisation (WHO). (1995). World Health Statistics Annual. Geneva: WHO.
• Wouters, E. (2003). Economic analysis of the Confronting COPD survey: an overview of results. Respir Med, 97, S3-S14.
• Young, P., Dewse, M., Fergusson, W., et al. (1999). Respiratory rehabilitation in chronic pulmonary disease: predictors of nonadherence. Eur Respir J, 13, 855-859.





























