Embed Size (px)
Citation preview
Pathology Seminar Series: Implications of cytogenetic abnormalities in reactive lymphoid hyperplasia
Alia Nazarullah, MD Faculty: Russell Higgins, MD 01-30-11
• 53 year old male presented with right cervical lymphadenopathy(gross-3cm)
• Morphology - architecture distorted by a paracortical expansion comprised of lymphocytes, histiocytes and numerous eosinophils
• IHC - predominance of small T-cells (CD2+, CD3+, CD5+, CD43+, and BCL2+) and fewer small to intermediate-sized B-cells (CD20+ and PAX5+).
CLONAL CYTOGENETIC ABNORMALITIES IN REACTIVE LYMPH NODES:
INDICATORS OF AN OCCULT LYMPHOMA? Christina Mendiola, Russell A. Higgins, Maggie Zhu, Gopalrao Velagaleti
(AGT 5-31-2011)

Case 1
Initial biopsy – abnormal lymphoid hyperplasia

Case 1
• Flow cytometry - no abnormal lymphoid population
• Molecular – no clonal IgH or TCR rearrangements
• Cytogenetics - 47,XY,+add(1)(p31),t(3;14)(q27;q11.2)[11]/93,slx2[2]/46,XY[7] - BCL6 rearrangement
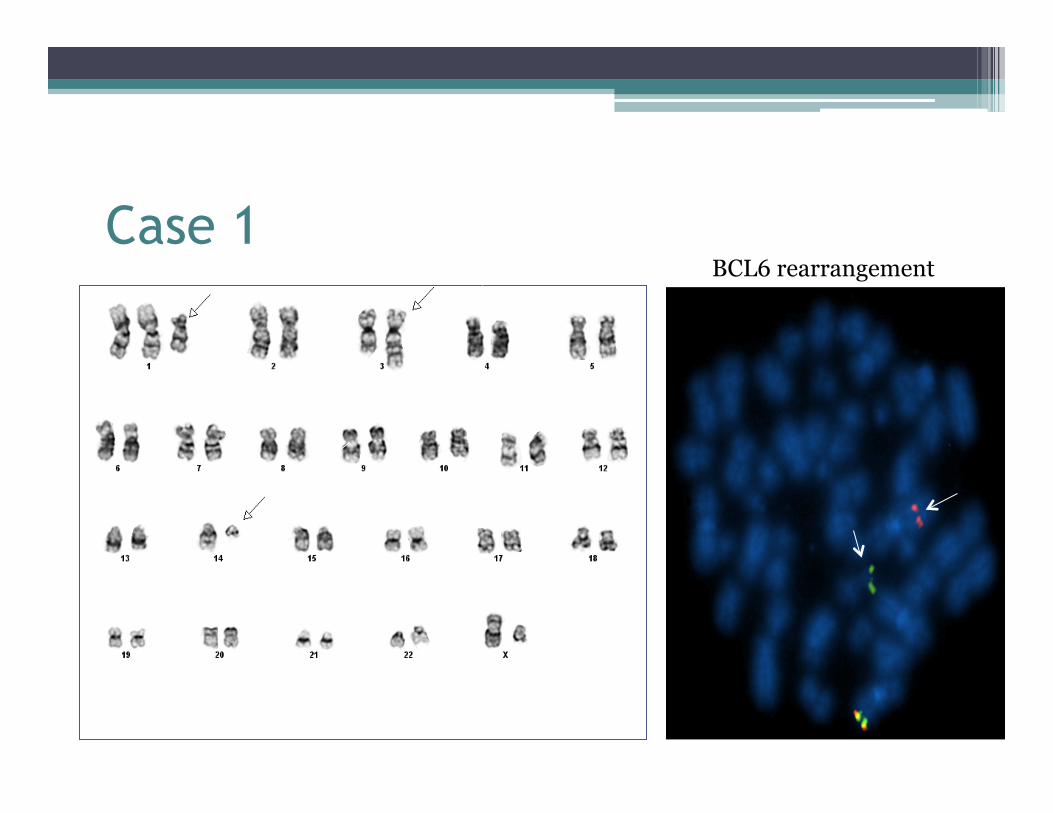
Case 1 BCL6 rearrangement

Case 1
• 6 months later – right inguinal lymph node

Case 1 • Morphology - diffuse infiltrate of large lymphoid
cells with anaplastic/pleomorphic features
• IHC – neoplastic B cells mark with BCL6, MUM1, CD30, OCT2 and BOB1
• Flow cytometry – no abnormal lymphoid population
• Molecular – no clonal IgH or TCR rearrangements
• Diagnosis – Diffuse large B cell lymphoma, NOS

Case 1

Questions to ponder • What is the significance of clonal cytogenetic
abnormalities in reactive/ non-neoplastic lymph nodes?
▫ Are they precursors/earliest indicators of development of malignancy?
▫ What frequency of these cases progress to lymphoma?
▫ What are the implications of their presence in non-neoplastic cells?

Overview • Background
• Review of basics ▫ B and T cell
� Normal development and germinal center reaction � Mechanisms of Ig gene remodelling � Aberrations in Ig gene remodelling
• “In situ / indolent” conditions
• Review of literature - cytogenetic abnormalities in ‘reactive’ tissues
• Summary

Background • Recurrent and clonal cytogenetic abnormalities are
described in B and T cell NHLs, some which are considered gold standard for specific entities
• Reactive clonal proliferations may occur in B and T cells in response to antigen stimulation
• Increased sensitivity of diagnostic methods have lead to identification of similar cytogenetic abnormalities in non-neoplastic tissues
• Few studies with clinical follow up exist on the consequences of these in reactive tissues

Overview • Background
• Review of basics ▫ B and T cell
� Normal development and germinal center reaction � Mechanisms of Ig gene remodelling � Aberrations in Ig gene remodelling
• “In situ / indolent” conditions
• Review of literature - cytogenetic abnormalities in ‘reactive’ tissues
• Summary

Early B and T cell development (Bone marrow)

Germinal center reaction
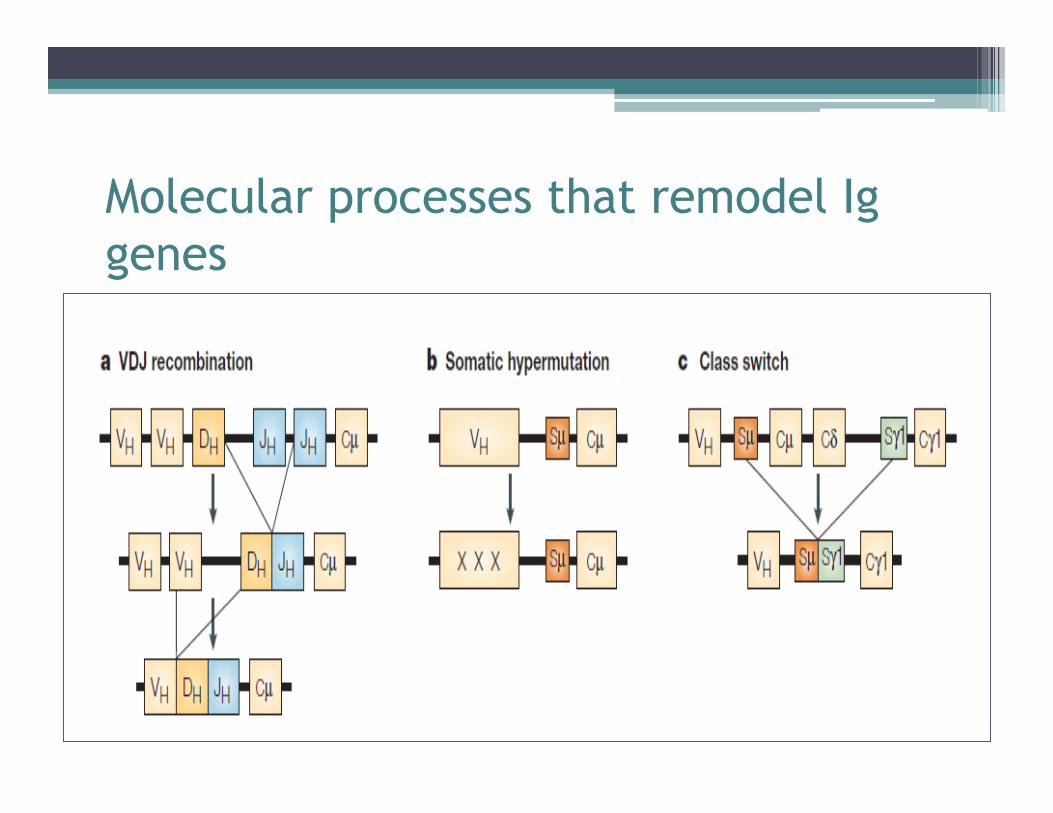
Molecular processes that remodel Ig genes

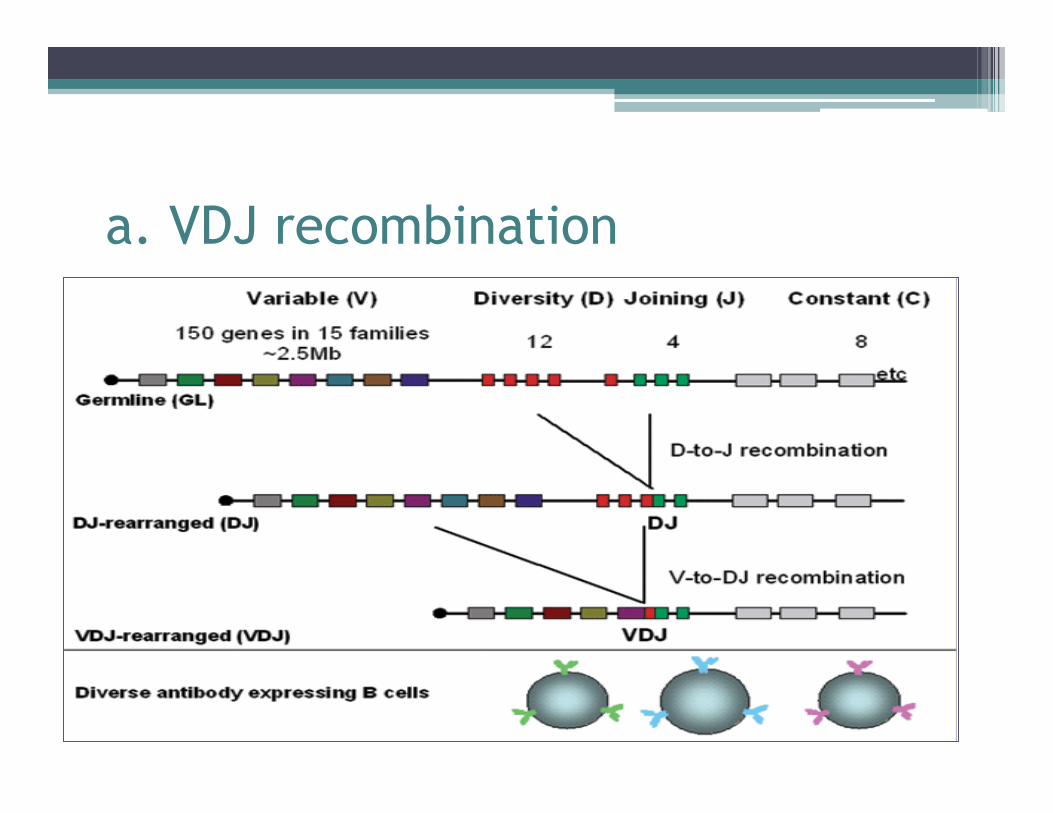
a. VDJ recombination
• Generation of a unique Ig variable region
• Ig heavy chains – V, D, J segments • Ig light chains – V, J segments
• Each developing B cell will assemble an immunoglobulin variable region by randomly selecting and combining one V, one D and one J gene segment

a. VDJ recombination
a. VDJ recombination

a. VDJ recombination
• V-D-J recombination errors?

b. Somatic hypermutation • Programmed mutation affecting variable region of Ig
genes (~1 million times higher than natural rate)
• Occurs in response to antigenic stimulation
• ‘Somatic’mutation – not transmitted to progeny
• Mutations at DNA hotspots – ‘hypervariable’ regions
• Single base substitutions, less commonly insertions and deletions
• Activation induced deaminase (AID) – cytosine to uracil

b. Somatic hypermutation • High fidelity DNA mismatch repair enzymes detect
change
• Error prone DNA polymerases introduce mutations
• B cell division – Ig variable region translated to B cell with varying antigen specificities
• Affinity maturation
• Highest affinity to antigen- plasma cell and memory B cell

c. Class switch • Isotype switching between Ig classes
• Involves constant region of Ig; variable region same – retains antigen specificity
• Naïve B cells – IgM and IgD
• DNA between ‘switch’ regions excised to produce IgG, IgA and IgD
• Constant region is same in antibodies of same isotype
• Variable region is identical in a single B cell or B cell clone

c. Class switch recombination

Transforming events • V-D-J recombination errors?
▫ t(14, 18) and t(11,14) translocations
▫ Breakpoints in IgH gene adjacent to JH or where DH joins JH
▫ loss of nucleotides around DH-JH and addition of non germline encoded nucleotides – typical features of normal VDJ recombination
▫ RAG nuclease activity in BCL2 – aberrant VDJ?
1. Jäger, U. et al. Follicular lymphomas’ BCL-2/IgH junctions contain templated nucleotide insertions: novel insights into the mechanism of t(14;18) translocation. Blood 95, 3520–3529 (2000). 2. Tsujimoto, Y., Gorham, J., Cossman, J., Jaffe, E. & Croce, C. M. The t(14;18) chromosome translocations involved in B-cell neoplasms result from mistakes in VDJ joining. Science 229, 1390–1393 (1985). 3. Tsujimoto, Y., Louie, E., Bashir, M. M. & Croce, C. M. The reciprocal partners of both the t(14; 18) and the t(11; 14) translocations involved in B-cell neoplasms are rearranged by the same mechanism. Oncogene 2, 347–351 (1988).

Transforming events • Somatic hypermutation of non-Ig genes?
▫ Genes encoding BCL6 and CD95 (Fas) were found to contain considerable fraction of mutations in normal GC and memory B cells
▫ 5’ end of BCL6 where hypermutation occurred, is also site for chromosomal translocation breakpoints
▫ In DLBCL, aberrant hypermutations of multiple oncogenes described
4. Pasqualucci, L. et al. BCL-6 mutations in normal germinal center B cells: evidence of somatic hypermutation acting outside Ig loci. Proc. Natl Acad. Sci. USA 95, 11816–11821 (1998). 5. Bross, L. et al. DNA double-strand breaks in immunoglobulin genes undergoing somatic hypermutation. Immunity 13, 589–597 (2000). 6. Papavasiliou, F. N. & Schatz, D. G. Cell-cycle-regulated DNA double-stranded breaks in somatic hypermutation of immunoglobulin genes. Nature 408, 216–221 (2000).

Transforming events
• Class switch recombination errors?
▫ Breakpoints in IgH constant region switch regions, in which DNA breaks are introduced
▫ Eg: C-myc translocations in Burkitt lymphoma
7. Goossens, T., Klein, U. & Küppers, R. Frequent occurrence of deletions and duplications during somatic hypermutation: implications for oncogene translocations and heavy chain disease. Proc. Natl Acad. Sci. USA 95, 2463–2468 (1998).

Transforming events • SHM and CSR in GC : most B cell lymphomas derive from GC or descendants • SHR and CSR do not occur in the DNA of T cells: B cells more prone to malignant transformation

Molecular and environmental factors in lymphomagenesis

Overview • Background
• Review of basics ▫ B and T cell
� Normal development and germinal center reaction � Mechanisms of Ig gene remodelling � Aberrations in Ig gene remodelling
• “In situ / indolent” conditions
• Review of literature - cytogenetic abnormalities in ‘reactive’ tissues
• Summary

In-situ follicular lymphoma • BCL2 overexpression in architecturally normal
follicles
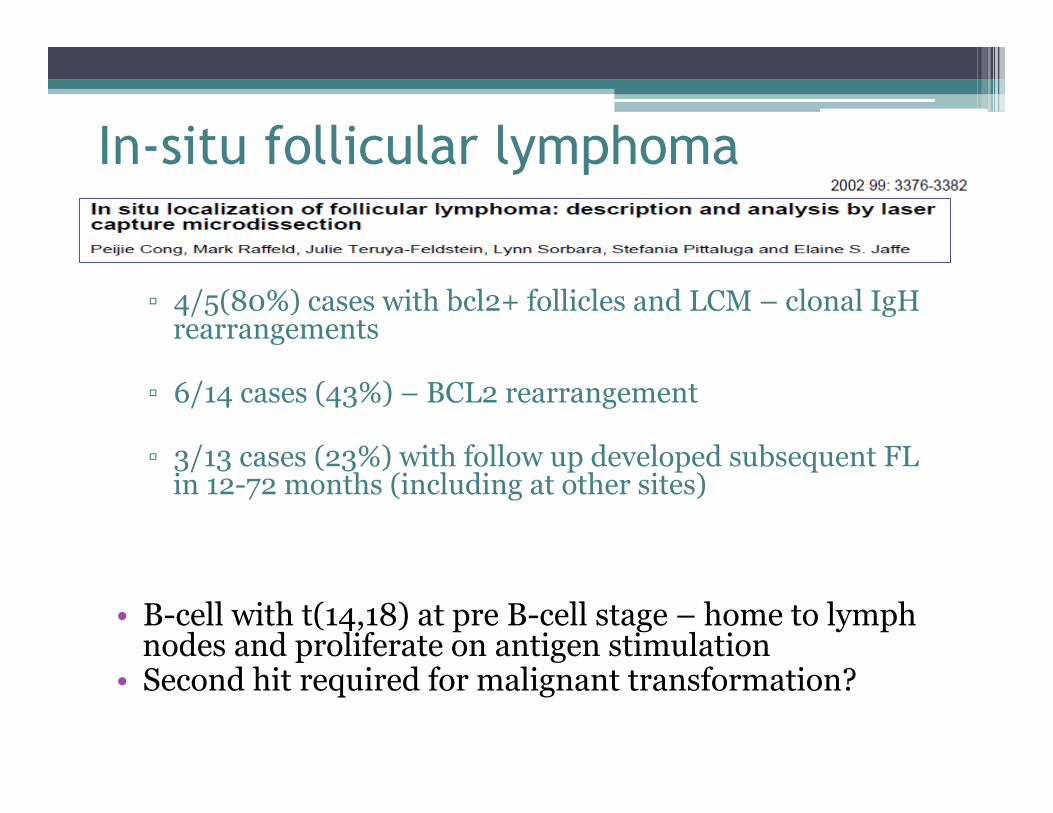
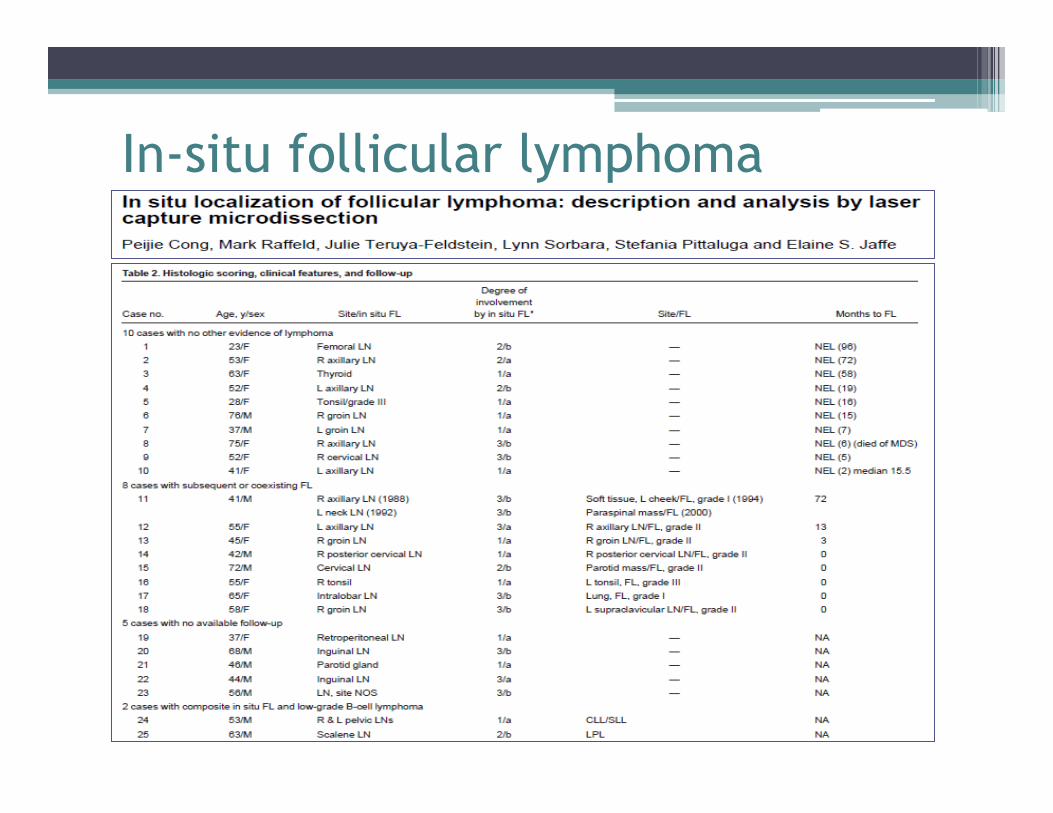
In-situ follicular lymphoma
▫ 4/5(80%) cases with bcl2+ follicles and LCM – clonal IgH rearrangements
▫ 6/14 cases (43%) – BCL2 rearrangement
▫ 3/13 cases (23%) with follow up developed subsequent FL in 12-72 months (including at other sites)
• B-cell with t(14,18) at pre B-cell stage – home to lymph nodes and proliferate on antigen stimulation
• Second hit required for malignant transformation?
In-situ follicular lymphoma

In-situ mantle cell lymphoma • Cyclin D1 positive B-cells in the mantle zones of
reactive lymphoid follicles

In-situ mantle cell lymphoma
▫ 9/9 cases (100%) were t(11,14) positive; 1/1 in cyclinD1 positive cell
▫ 1/13 (7%) cases with follow up developed overt MCL (4 years after diagnosis)
▫ Retrospective analysis of 7 cases of MCL had in-situ lesion in 7/7
previous specimens (2-15 years)
• Low malignant potential – low but definitive risk of progression
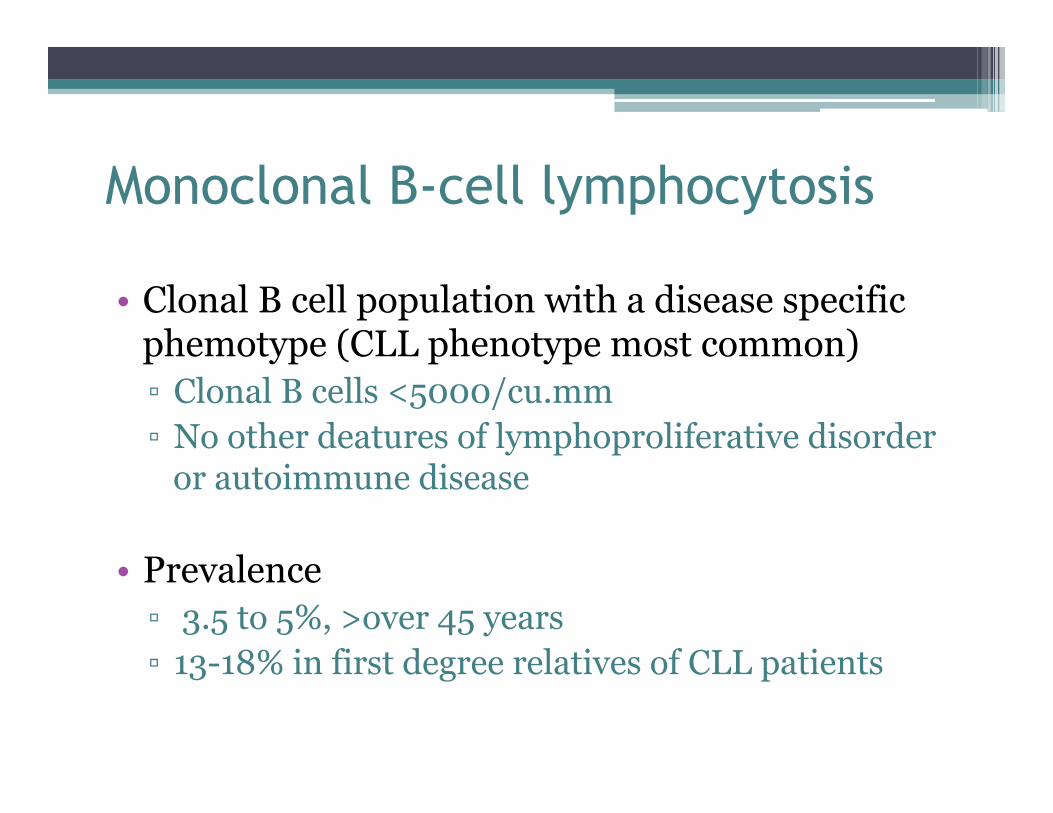
Monoclonal B-cell lymphocytosis
• Clonal B cell population with a disease specific phemotype (CLL phenotype most common) ▫ Clonal B cells <5000/cu.mm ▫ No other deatures of lymphoproliferative disorder
or autoimmune disease
• Prevalence ▫ 3.5 to 5%, >over 45 years ▫ 13-18% in first degree relatives of CLL patients

Monoclonal B-cell lymphocytosis
• Cytogenetic abnormalities
• Risk of malignant transformation – 1-2% per year
13q deletion Trisomy 12 11q deletion 17p deletion
CLL 54% 16% 18% 7%
MBL 36-58% 8-21% 0-6% 0-3%

Monoclonal gammopathy of unknown significance (MGUS)
▫ Serum M protein < 30g/L ▫ bone marrow clonal plasma cells < 10% ▫ no end organ damage ▫ no evidence of B cell lymphoma
• 3% of people over 50 yrs; >5% over 70 yrs
• ~50% have IgH translocations, t(11,14) – 15-25% • 13q deletion 40-50% (compared to 50% in myeloma) • Activating KRAS and NRAS mutations less frequent(~5%)
compared to myeloma(50%)
• Risk of malignant transformation – 1% per year

Overview • Background
• Review of basics ▫ B and T cell
� Normal development and germinal center reaction � Mechanisms of Ig gene remodelling � Aberrations in Ig gene remodelling
• “In situ / indolent” conditions
• Review of literature - cytogenetic abnormalities in ‘reactive’ tissues
• Summary

• Bcr-abl detected in blood of ▫ 22/73 (30%) adults ▫ 1/22 (4%) children ▫ 0/22 in umbilical cord blood
• Increase in incidence with age
• 2/23 cases had disappearance of transcript

• Presence of t(14, 18) breakpoints in 6/9 bood donors by PCR
• Almost exclusively in flow sorted B cells
• Estimated frequency – 1 in 105 or fewer circulating B cells
• 4/6 individuals harbored 2-5 unrelated t(14,18) carrying B cell clones
• Few cells with t(14,18) acquire additional oncogenic hits required for malignant transformation?
• Clones with t(14,18) increases with age (Liu et al, 1994)

t(11;14)-positive clones can persist over a long period of time in the peripheral blood of healthy individuals
• 5/71 (7%) cases had t(11,14) ▫ 7% in reference population ▫ 7% in cases exposed to pesticides
• 4/5(83%) of t(11,14) positive cases were also t(14,18) positive
• t(11,14) detectable in peripheral blood upto 9 years, some increased in levels 2-3fold; none developed lymphoma
Y Lecluse1, P Lebailly1,2, S Roulland3, A-C Gac1, B Nadel3 and P Gauduchon1 1Groupe Re´gional d’Etudes sur le Cancer, IFR146 ICORE, Universite´ de CAEN Basse-Normandie, CLCC Franc¸ois Baclesse, Caen, France; 2Registre ge´ne´ral des tumeurs du Calvados, CLCC Franc¸ois Baclesse, Caen, France and 3Laboratory Genomic Instability and Human Hemopathies, Centre d’Immunologie de Marseille-Luminy (CIML), CNRS-INSERM-Universite´ de la Me´diterrane´e, Marseille, France
Leukemia (2009) 23, 1190–1193

• 14/29 volunteer blood donors had NPM/ALK fusion sequence
• Frequency – 1 in 106 cells
• Proportion of abnormal cells very low – breakpoint specific bands very weak, 2/4 positive cases reproducible
• Presence of fusion gene in adjacent reactive lymphocytes may be responsible for t(2,5) in few cases of Hodgkin lymphoma?

• 22/31 reactive tissues showed NPM/ALK fusion sequence
• 1/31 showed ATIC/ALK fusion sequence
• Low proportion of cells compared to ALK+ cases of ALCL
A- ALK(+)ALCL; B- ALK(-)ALCL, Hodgkins lymphoma, Reactive

• 10/30 (33%) cases showed cytogenetic abnormalities; 5 of these 10 showed clonal IgH molecular abnormalities
• 10/10(100%) with clonal CG abnormalities subsequently developed lymphoma(0.3 – 37 months)
• 7/17 (41%) cases with normal/no metaphases developed lymphoma; 1 showed clonal molecular abnormality
• 3 cases (1HIV+) with non clonal abnormalities, including t(3,14) and t(3,22) – BCL6 rearrangement; none progressed to lymphoma in 4-6 year follow up


• 22/116(17%) reactive lymph nodes had cytogenetic abnormalities ▫ 14(70%) structural ▫ 6(55%) numerical
• 8 cases - chromosome 14 abberations; 7-IgH • 4 cases - chromosome 3 abberations; 3-BCL6 • 1 of 18 (5%) with clinical follow up developed
lymphoma


Overview • Background
• Review of basics ▫ B and T cell
� Normal development and germinal center reaction � Mechanisms of Ig gene remodelling � Aberrations in Ig gene remodelling
• “In situ / indolent” conditions
• Review of literature - cytogenetic abnormalities in ‘reactive’ tissues
• Summary
Summary • Clonal cytogenetic abnormalities may be seen in reactive lymph nodes–
increase with highly sensitive methods of detection
• These may pose a low but definitive risk for lymphomagenesis; median time variable
• Risk increases with age and with deregulated immunosurveillance – chronic antigen stimulation and genotoxic stress
• Additional oncogenic events necessary for malignant transformation
• Follow up to monitor for early morphologic or immunophenotypic evidence of lymphoma
• Important to consider while screening for stem cell transplant donors and monitoring minimal residual disease
• Further studies with larger series needed to describe the true implications of such findings – preventive therapy?

References • 1. Jäger, U. et al. Follicular lymphomas’ BCL-2/IgH junctions contain templated
nucleotide insertions: novel insights into the mechanism of t(14;18) translocation. Blood 95, 3520–3529 (2000).
• 2. Tsujimoto, Y., Gorham, J., Cossman, J., Jaffe, E. & Croce, C. M. The t(14;18) chromosome translocations involved in B-cell neoplasms result from mistakes in VDJ joining. Science 229, 1390–1393 (1985).
• 3. Tsujimoto, Y., Louie, E., Bashir, M. M. & Croce, C. M. The reciprocal partners of both the t(14; 18) and the t(11; 14) translocations involved in B-cell neoplasms are rearranged by the same mechanism. Oncogene 2, 347–351 (1988).
• 4. Pasqualucci, L. et al. BCL-6 mutations in normal germinal center B cells: evidence of somatic hypermutation acting outside Ig loci. Proc. Natl Acad. Sci. USA 95, 11816–11821 (1998).
• 5. Bross, L. et al. DNA double-strand breaks in immunoglobulin genes undergoing somatic hypermutation. Immunity 13, 589–597 (2000).
• 6. Papavasiliou, F. N. & Schatz, D. G. Cell-cycle-regulated DNA double-stranded breaks in somatic hypermutation of immunoglobulin genes. Nature 408, 216–221 (2000).

References • 7. Goossens, T., Klein, U. & Küppers, R. Frequent occurrence of deletions and duplications
during somatic hypermutation: implications for oncogene translocations and heavy chain disease. Proc. Natl Acad. Sci. USA 95, 2463–2468 (1998).
• 8.Küppers R. Mechanisms of B-cell lymphoma pathogenesis. Nat Rev Cancer. 2005 Apr;5(4):251-62. Review.
• 9.Jegalian AG, Eberle FC, Pack SD, Mirvis M, Raffeld M, Pittaluga S, Jaffe ES. Follicular lymphoma in situ: clinical implications and comparisons with partial involvement by follicular lymphoma. Blood. 2011 Sep 15;118(11):2976-84. Epub 2011 Jul 18.
• 10. Carvajal-Cuenca A, Sua LF, Silva NM, Pittaluga S, Royo C, Song JY, Sargent RL, Espinet B, Climent F, Jacobs SA, Delabie J, Naresh KN, Bagg A, Brousset P, Warnke RA, Serrano S, Harris NL, Swerdlow SH, Jaffe ES, Campo E. In situ mantle cell lymphoma: clinical implications of an incidental finding with indolent clinical behavior. Haematologica. 2011 Nov 4.
• 11. Trümper L, Pfreundschuh M, Bonin FV, Daus H. Detection of the t(2;5)-associated NPM/ALK fusion cDNA in peripheral blood cells of healthy individuals. Br J Haematol. 1998 Dec;103(4):1138-44.
References • 12. Au WY, Horsman DE, Connors JM, Klasa RJ, Gascoyne RD. Cytogenetic findings in
reactive lymphoid hyperplasia: Significance of non-clonal t(3;14) and t(3;22). Am J Hematol 2002;70:133-138.
• 13. Sevilla DW, Murth VV, Sun X-L, Nandula SV, Mansukhani MM, Alobeid B, Bhagat G. Cytogenetic abnormalities in reactive lymphoid hyperplasia: byproducts of the germinal centre reaction or indicators of lymphoma? Hematol Oncol 2011;29:81-90.
• 14. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. WHO Classification of Tumours of Haematopietic and Lymphoid Tissues, 4th ed. Lyon: WHO Press, 2008: 224-5.
• 15. Pasqualucci L, Neumeister P, Goossens T, Nanjangud G, Chaganti RS, Kuppers R, Dalla-Favera R. Hypermutation of multiple proto-oncogenes in B-cell diffuse large-cell lymphomas. Nature 2001;412:341-346.
• 16. Maes B, Vanhentenrijk V, Wlodarska I, Cools J, Peeters B, Marynen P, de Wolf-Peeters C. The NPM-ALK and the ATIC-ALK fusion genes can be detected in non-neoplastic cells. Am J Pathol. 2001 Jun;158(6):2185-93.





























