Embed Size (px)
Citation preview

Partnership working between the acute trust, community providers and adult social
care in Nottinghamshire
Productive NottsNottingham University Hospitals NHS TrustNottingham City Social ServicesNottinghamshire County Social ServicesNottingham CityCareNottinghamshire County Health Partnerships

In September, NUH provided an overview of Better for You: the approach to delivering
quality and efficiency
3 examples were shared:
This resulted in an invitation to return with colleagues to share the collaborative work across health and social care regarding transfers of care

Today we will cover
• The name of the project• The purpose and scope of the project• The activities and approach undertaken• Staff engagement• The redesign of processes• The new ways of working – and its challenges• Results from the work
– Views of staff– Data
• Next steps: our aims for further improvement

What’s in a name?
Nottingham University Hospitals NHS TrustNottingham City Social ServicesNottinghamshire County Social ServicesNottingham CityCareNottinghamshire County Health Partnerships
“External Waits”
“Integrated Health and Social Care Discharge Project”
Part of the “Productive Nottinghamshire”programme
“Integrated Discharge”

NUH data collection exercise
Summer 2010
All adult surgical and medical wards:
‘What is your patient waiting
for today?’
Over 100 patients waiting every day for a
service provided by NUH
Over 80 patients waiting every day for a
service provided by Social Care or
Community Health teams
NUH internal waits project
750 waits per week reduced to 260 in
12 months (66% reduction)
Integrated Care Transfers project
identified top 5 waits (now moving
into resolution phase)
What are our patients waiting for?

Project purpose and scope

Starting the project...Tendering process for external support to act as a workstream lead, bring external expertise and an independent view
All services provided a project lead (team leader level) to re-design processes and provide support to new ways of working
Completed the ‘discovery phase’ together to see the size of the problem as a whole group – ‘one view’and not ‘blame’
Staff engagement time out session for those staff not directly involved in re-design
4 weeks

Multi-agency engagement event for 100 delegates across health (acute and community) and social services
‘gained insight into how other
services work’
‘great to hear we all want the same
thing’
‘wish we had done this 20 years ago’
‘it feels different this time – hopeful
it’s going to change’
‘multi-agency tables worked so
well’
‘wish the senior people were present rather than on video’

Rapid progress covering a wide range of workOver 11 weeks we:
• Re-designed existing processes (4 day locked room event)
• Decided the measures
• Communicated with the wards
• Trained the team (NUH, City social care, County social care)
• Continuously improved and refined the process
• Continuously improved data quality
• Did group sessions with the discharge co-ordinators for continued engagement
• Sent out newsletters and FAQs
• Added to the wait codes for data accuracy
• Commenced new processes and daily health and social care meetings
• Wrote a manual
• Introduced flexible working to cover sickness and annual leave
• Weekly project steering group meetings
• Planned to roll out after evaluation

Existing processes were redesigned by front-line staff
“If you do what you've always done, you'll get what you've always gotten.”(Robbins)
•Blame culture•Delayed transfers of care•Medically stable patients in acute hospital beds•Queues for rehabilitation beds•End of life patients dying before getting home•Excessive admin processes
“We should work on our process, not the outcome of our processes.”(Deming)Numerous services 9 simple
pathways
7 standard steps (measured) in every pathway

These resulted in new ways of working to trial
Team daily routine:
• Collect ward folder with worksheets
• Attend daily boardround
• Proactively pick up new referrals (or
signpost)
• Action new referrals if able
• Update worksheets
• Continue with current case load
Team leaders meet 11am:
• Review worksheets
• Question delays between the steps
• Escalate delays
• Problem solve difficult cases
Admin inputs worksheets onto a database daily – themes of waits can
be reported in almost real-time

Immediate benefits
Patient quality
Relationships
Effectiveness
Efficiency
Patients are assessed by the right person first time (inappropriate cases are screened out at the boardround or signposted to another service)
• Social Workers feel part of the multi-disciplinary team again• Staff aren’t blaming each other• Daily communication of what stage of assessment/readiness the patient is at
• The duty line doesn’t get as many phone calls about when there will be an allocated worker• Assessments are responded to quicker (because we’ve reduced the inappropriate/not yet ready cases)
• No ‘chasing’ needs to be done. Time previously spent chasing progress is now spent on patient care.• Clear and timely escalation routes for issues/delays• Strong networks for working together opportunities

What’s gone well? – views of staffI can do my job
properly instead of fire fighting and answering complaints
It feels like we’ve turned a switch and things are starting to fall into place
We’re now allocating all County social care cases on referral across QMC
We’re receiving less inappropriate referrals across all services
Our teams can spend quality time with patients to get them the right service and we have better job satisfaction from building relationships
We feel we’re part of a multi-disciplinary team again My time is freed up
from chasing services so I can spend more time caring for patients

Ward staff like not filling in several referrals for each
patient needing a service
Trust and relationships are beingbuilt between the person attending
boardround from IDT/Social Services and the existing multi-disciplinary team
Ward staff like having the ‘signposting’ function of the person attending boardround – stops a lot of wondering where to try next
‘it used to feel like a battle zone, now its responsive and respectful’
What’s gone well? – views of staff

We now have quality data instead of anecdote
to 95% (169)50% (185) to 100% (22)
637 cases from seven wards in 10 weeks
Social Package of care and rehabilitation are the top two pathways for these patients
Mean age of patients is 85 years (59% female)
50% of patients leave NUH between 1-5 days after being medically stable, 45% leave between 6-22 days, 5% leave between 23-55 days
Services have delays in different steps of the process (some at the assessment stage, some at providing the care stage)
This enables an improved, shared understanding and an opportunity to improve

The data reinforces where benefits have already been achieved
As staff became used to the new process, they were able to increase the number of cases they dealt with – through process re-design and engagement with the wards
The team has increased the number of completed cases through a reduction of inappropriate cases, improved communication, right person involved at the right time
Improved predicted discharge dates to actual discharge date
Reduction in continuing care referrals through improved knowledge of the system with a similar conversion rate to actual assessment required

Maintaining the new process -challenges Buddy system introduced for health and
social care staff to initially work together on the boardround (use of medical terminology, understanding medical stability, knowing when to start an assessment and when to wait)
Data quality – requires daily remindersQuality of data requires constant prompts to make
sure we can continue to identify themes of waits and show improvements. Clinical staff often aren’t
aware of the importance of accurate and timely data
Shifting sands – nothing stays the sameNottingham City Social Services are reconfiguring their hospital based team, there’s been lots of staff movement and need for re-training and flexibility from all services. Nottinghamshire County Social Services are going out to consultation about reconfiguration

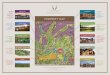
Our next challenges – reducing the top 5 waits
0.0 50.0 100.0 150.0 200.0 250.0 300.0 350.0
queue: community bedward to complete referral or checklist
queue: nursing homewait: funding decision
ad hoc funding (eg key safe)queue: transport
queue: Braywood rehabqueue: community bed Ilkeston
interim careout of area
queue: assessment bed Oaksqueue: assessment space Willows
social worker allocat ionreferral: ASC assessmentqueue: IMC at Braywood
queue: assessment space Braywoodreferral: physiotherapist assessment
wait : CCNA assessmentqueue: assessment bed
queue: assessment spacequeue: care home
self funderreferral: consultant other speciality
referral: capacity assessmentwait : geriatrician letter
referral: specialist nurse reviewqueue: assessment space Oaks
service declined pat ientqueue: assessment space Bramwell
referral: psychiat ric assessmentqueue: Bramwell rehab
queue: Oaks rehabreferral: IDT assessment
wait : diagnost ic testwait: diagnost ic result
queue: IMC at homeequipment: availabilityreferral: OT assessment
care home closed due to infectionfamily engagement
Safeguardingother
choicecare home: await ing assessment
queue: lings barpat ient medically unstable
queue: care package
Bed Days
Reas
on fo
r de
lay
Delays - once care in place1. Care package
availability2. Medically
unstable patient (after being stable)
3. Lings Bar rehab bed availability
4. Care home coming to NUH to assess a patient
5. Patient or family choice

0.0 50.0 100.0 150.0 200.0 250.0 300.0 350.0
queue: community bedward to complete referral or checklist
queue: nursing homewait : funding decision
ad hoc funding (eg key safe)queue: t ransport
queue: Braywood rehabqueue: community bed Ilkeston
interim careout of area
queue: assessment bed Oaksqueue: assessment space Willows
social worker allocat ionreferral: ASC assessmentqueue: IMC at Braywood
queue: assessment space Braywoodreferral: physiotherapist assessment
wait : CCNA assessmentqueue: assessment bed
queue: assessment spacequeue: care home
self funderreferral: consultant other speciality
referral: capacity assessmentwait : geriatrician let ter
referral: specialist nurse reviewqueue: assessment space Oaks
service declined pat ientqueue: assessment space Bramwell
referral: psychiatric assessmentqueue: Bramwell rehab
queue: Oaks rehabreferral: IDT assessment
wait : diagnost ic testwait : diagnost ic result
queue: IMC at homeequipment: availabilityreferral: OT assessment
care home closed due to infect ionfamily engagement
Safeguardingother
choicecare home: await ing assessment
queue: lings barpat ient medically unstable
queue: care package
Bed Days
Reas
on fo
r de
lay
Delays - once care in place
Our combined approach to resolve the waitsThe top 10 waits are now allocated to 10 ‘task and finish’groups led by members of Social Care, NUH and the Community Services
These groups are currently developing plans outlining:
- the size of the issue
- what options will resolve it and
- what can be achieved in 3 days, 1 month, 3 months and beyond 3 months
Progress is governed through a Productive Notts workstream.
Sponsor: David Pearson

Working together across health and social care
• An idea from one of our organisations• Productive Notts brought all the organisations together• Senior leaders from health and social care
commissioned the work• Frontline staff from health and social care designed the
change together• Managers from health and social care worked together
to support them• A Programme Board with senior managers from health
and social care is now overseeing the work to reduce delays
• David Pearson is Executive Sponsor for this Productive Notts workstream
Improvements for patients through collaborative working

Next steps• Roll out the new way of working across NUH and the hospital based social care teams (tailored to each new cohort of wards)
• Provide secure email for sharing information between services
• Reduce number of assessment forms in use and replace with a multi-purpose assessment
• Weekly data report showing themes of waits and improvements made
• Identify opportunities to reduce the number of patients directly admitted to a new care home from NUH
Work on the top waits:
• Review the success of improving throughput at Lings Bar and transfer successes to NUH
• Progress resolution of the top 10 waits through task and finish groups
• Weekly reporting of data to show improvements made

Thank you & questions