Embed Size (px)
Citation preview

Parkinson's diseaseParkinson's disease
Presented by
Abdulaziz .M. Al-Saad
Contents
• Definition & Pathophysiology .Definition & Pathophysiology .
• Static & Facts .Static & Facts .
• Causes & Stages .Causes & Stages .
• Strategy of treatment .Strategy of treatment .
• Drug therapy .Drug therapy .
• Surgical approach .Surgical approach .
• The future .The future .

What is Parkinson's disease ? Parkinson’s disease is a disorder of the extrapyramidal system .
Characterized by…
• It is progressive disease ??
• Imbalance between the excitatory neurotransmitter Acetylcholine and
inhibitory neurotransmitter Dopamine in the Basal Ganglia :
ACh
DA

Nonmotor symptoms
Cognitive impairment, dementia**
Psychiatric symptoms, particularly depression**
Autonomic disturbances**
» Urinary urgency and frequency
» Constipation
» Hypotension with orthostasis
» Sweating disorders
» Sexual dysfunction
Sleep disturbances**

Static and Facts
• Age at onset variable ( 50 – 80 years ) . Mean age 55 years
• Man and Woman are equally affected.
• Prevalence 100 case Per 100 000 Population .
• Incidence 20 case Per 100 000 People annually.

Static and Facts
• Progression highly variable. Within 10 – 20 years.
• Patient age at onset affect progression . ( high rate in older )
• Mortality not caused by disease itself , but, due to complications related
to immobility . Complication such as ( Aspiration Pneumonia ,
cardiovascular and cerebrovascular disease (

Drug induce PD :
1. Reserpine ------------ depletion of dopamine storage.
2. Halloperidole, phenothiazin , MPTP.
What is MPTP ?
Causes :1. Idiopathic due to exposure to :
• Neurotoxins.
• Oxidative reactions.
2. Genetic factors may be important.
3. Others :
1. Dopaminergic receptor antagonist ( Antipsychotic ) .
2. Destruction of dopaminergic neurons ( MPTP ) .

Stages of PD
• Stage 1 : Unilateral involvement Minimal or no functional impairment.
• Stage 2 : Bilateral involvement Without impairment of balance
• Stage 3 : Postural imbalance Some restriction of activity Mild – Moderate disability
• Stage 4 : Severely disable Cannot walk and stand
• Stage 5 : Restricted to the bed

Treatment of Parkinson’s Disease
Parkinson’s Disease
Pharmacological Treatment Non- Pharmacological Treatment
Education
Supportive service
Exercise
Nutrition
Neuroprotective( Selegiline ) Functional Impairment
Yes
Dopamine AgonistLD
+/- COMTIs
No
Dopamine agonist + LD+ / - COMTIs
Unaccepted Control Surgery

Two major categories
1. Dopaminergic agents :
» Promote activation of dopamine receptors
» Levodopa (Dopar)
2. Anticholinergic agents :
» Prevent activation of cholinergic receptors
» Benztropine (Cogentin)
Classification of Drug Therapy for Parkinson’s Disease

Mechanism of Action
• Promotion of dopamine synthesis
• Prevention of dopamine degradation
• Promotion of dopamine release
• Direct activation of dopamine receptors
Dopaminergic Agents
Anticholinergic Agents
Mechanism of action
Blockade of muscarinic cholinergic receptors in the striatum
Levo- dopa
– Immediate metabolic precursor of dopamine
– Dopamine not cross BBB.
– Levodopa cross BBB.
– After it cross BBB, decarboxylated to dopamine.
– Peripheral decarboxylation can be prevented by : Carbidopa
– This leads to decrease dose by 75 %
– Dose Sinemet ( 25 mg / 100 mg ) OR ( 25/ 250 ) OR Controlled release.
Side Effects1. GIT .
2. Cardiac abnormalities .
3. CNS .
4. Eye.
5. Behavior changes.
6. Fluctuations ------ Drug Holiday
7. Wearing off ------- Treatment
Contraindications :
» Psychotic Patients .
» Cardiac disease .
» Glaucoma .
» Peptic ulcer .
Drug Interactions
1. Pyridoxine ( Vit. B6 ) --------- Increase Periphral decarboxylations.
2. MAOIs type A ----------------- Hypertensive crisis.
Ergot Derivative
1- Bromocriptin :
- D2 agonist , widely used in PD.
2- Pergolide :
- D1, D2 agonist , widely used in PD .
Non-Ergot Derivative
Advantage :
1- Newer Agents
2- Effective against PD.
3- Approved by FDA.
4- Lower SE Than old group.
1- Ramipexole :
- D3 receptor
- Effective as monotherapy in mild cases
- Adjunctive + LD --------- decrease dose and fluctuation with LD.
2- Roprinil :- D2 receptor
- Effective as monotherapy in mild cases
- Adjunctive + LD --------- decrease dose and fluctuation with LD.
SE: ( fatiguge , insomnia , dyskinisia , confusion )

Mechanism of action ( Selegiline) :
Selective inhibitor of Monoamine Oxidase type B . ( what do you think about non-selective ? ) .
L -dopa Dopamine
MAO B
Reuptake
COMT
SelegilineSelegiline

Advantages of Selegiline :
1. Enhance and prolongs the anti-parkinsonism effect of Levo – dopa .
2. Reduce the dose of Levo – dopa .
3. Dose : ( 5 mg at break fast ) ( 5 mg at lunch )
4. SE : increase insomnia with LD.
5. Not used with TCAs.
L - dopa
70 %
GIT 29 %
Prephral tissuesBrain
1 – 3 %
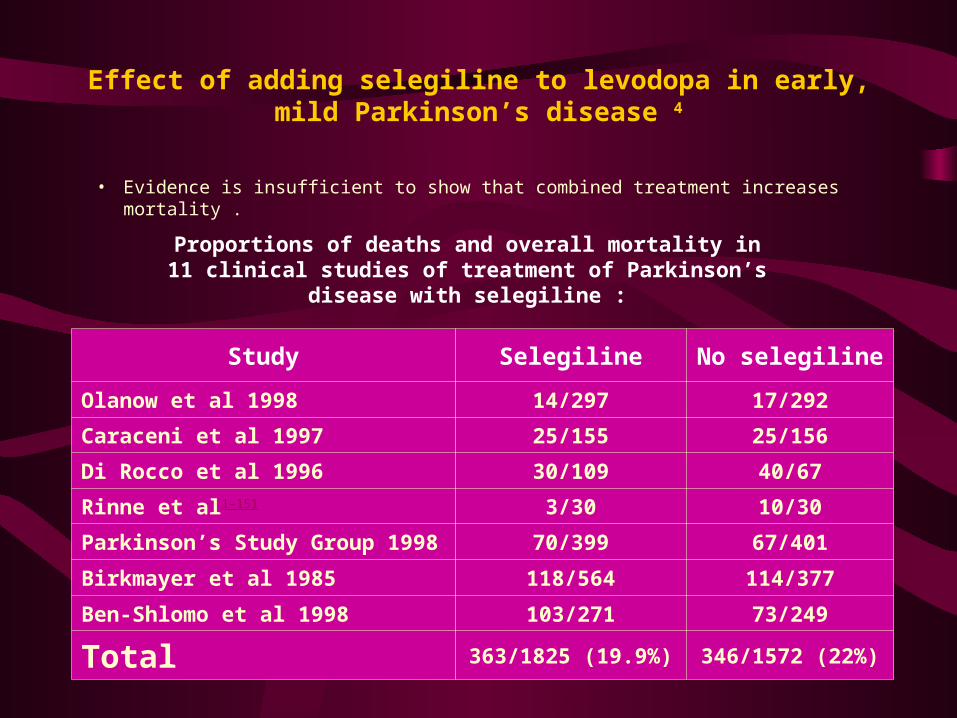
Effect of adding selegiline to levodopa in early, mild Parkinson’s disease 4
• Evidence is insufficient to show that combined treatment increases mortality .
Proportions of deaths and overall mortality in 11 clinical studies of treatment of Parkinson’s disease with selegiline :
Study Selegiline No selegiline
Olanow et al 1998 14/297 17/292
Caraceni et al 1997 25/155 25/156
Di Rocco et al 1996 30/109 40/67
Rinne et al1-151 3/30 10/30
Parkinson’s Study Group 1998 70/399 67/401
Birkmayer et al 1985 118/564 114/377
Ben-Shlomo et al 1998 103/271 73/249
Total 363/1825 (19.9%) 346/1572 (22%)

Catichol-O-Methyltransferase Inhibitor
( COMT )
1- Tolcapone & entacapone
– Prolong duration of action of LD.
– SE : Similar to LD .
2- Amantadine
– Antiviral agents.
– Potentiate action of DA by increase synthesis ,release and decrease reuptake.
– Therapeutic effect short – lived.
SE :
Restlessnes, agitation, depression , irritability ( CNS se )

Acetyl choline- blocking agents :
• Antimuscarinc Agents:
1. Bnzotropine , biperiden, orphenadrin.
– Effective against PD .
– SE :
– Drowsiness, hallucination , restlessness, depression
– Other : dry mouth , Mydriasis, urinary retention .
Experimental approach to treat PD
Vitamin E: Free radical scavenger.
Neurotropfic factor e.g. Glial –derived neurotropfic factor
Surgical Procedure :
Used in poorly responsive PD patients to pharmacotherapy ..
1. High Frequency Deep Brain Stimulation ( Thalamic Stimulation ).
2. Transplantation of Dopaminergic tissue
ConclusionConclusion • Patients with Parkinson's disease have a constellation of clinical symptoms that
evolve over the course of the condition.
• Patient management involves the accurate clinical diagnosis of the disease,
multidisciplinary management of clinical problems and the use of a number of
therapeutic options.
• Until disease-modifying drugs become available, we must focus on reducing the
burden of Parkinson's disease by treating the symptoms and helping our patients
cope with their disability by improving their quality of life.
The end
Pain Management in Patients with CA
CNS Pharmacology

Pain Management
• Pain– Unpleasant sensory and emotional
experience associated with tissue damage– Patient’s pain description is the
cornerstone of pain assessment
Types of Pain
• Nociceptive pain– Results from injury to tissues– Called somatic or visceral pain
Neuropathic pain
Results from injury to peripheral nerves
Responds poorly to opiods

Clinical Approach to Pain Management
• A- Ask and assess
• B- Believe
• C- Choose
• D- Deliver
• E- Empower and enable
Pain Assessment
• Assessment parameters of pain– Onset and temporal patterns– Location– Quality– Intensity– Modulating Factors– Previous treatment– Impact

WHO Analgesic Ladder
• Step 1- Mild to moderate pain– Nonopiod analgesic
• Step 2- More severe pain– Add opioid analgesic
• Step 3- Severe pain– Substitute opioid-morphine





![Parkinson's Disease[1] (1)](https://img.dokumen.tips/doc/110x75/55cf9295550346f57b97b1cc/parkinsons-disease1-1.jpg)























