Embed Size (px)
Citation preview

Parenteral Nutrition in Critical Illness
Judy WONGDietitian
PMH
OverviewWhat is parenteral nutrition
Selection Criteria of parenteral nutrition
Parenteral nutrition access
Requirements of critically ill patients
Refeeding Syndrome
Parenteral Nutrition formulations & How to choose
Case Study

What is Parenteral NutritionParenteral nutrition refers to the infusion of
intravenous nutrition formula into the bloodstream
DAA, 2011

Selection Criteria for Parenteral Nutrition
Should be used in patients who are or will become malnourished, and
Who do not have sufficient gastrointestinal function to be able to restore / maintain nutritional status
McClave et al.,2009

Access of parenteral nutrition
Access of parenteral nutrition
Central parenteral nutrition (CPN)To large, high blood flow vein (e.g. superior vena
cava)
For long term parenteral nutrition
Central Parenteral Nutrition solution osmolarity can be > 900mOsm/L
More suitable for volume-sensitive patients (e.g. patients with heart, renal or liver problem)
Access of parenteral nutrition
Peripheral parenteral nutrition (PPN)Catheter tip placement in a small vein (e.g. forearm)
PeripherallParenteral Nutrition solution osmolarity < 900 mOsm/L
Usually do not fully meet nutrition requirements
Use as:Supplemental feedingTransition to oral/enteral feedingTemporary PN when central access has not been initiated

Energy requirementMacronutrient requirementsMicronutrient requirements
Requirements of critically ill patients
Requirements during metabolic stress
Adequate energy is essential for metabolically stressed patients
Avoidance of overfeeding in the critically ill patients is important
Excess calories can result in complications: hyperglycaemia hepatic steatosis excess CO2 production (exacerbate respiratory insufficiency /
prolong weaning from mechanical ventilation)
Krause’s, 2012

How much energy should critically ill patients receive?
ESPEN Guidelines 2009:
“as close as possible to the energy expenditure in order to decrease negative energy balance” (Grade B);
“in the absence of indirect calorimetry, ICU patients should receive 25kcal/kg/day increasing to target over the next 2-3 days” (Grade C)
Singer P et al (2009)
Calculations of requirementEstimation of energy requirement
= Basal Metabolic Rate (BMR) + Activity Factor
+ Stress Factor

Calculations of requirement
Estimation of energy requirementBasal Metabolic Rate (BMR) estimation
(Schofield Equation):
Age Male Female
18-29 15.1 x W + 692 14.8 x W + 487
30-59 11.5 x W +873 8.3 x W + 846
60-74 11.9 x W + 700 9.2 x W + 687
Over 75 8.4 x W + 821 9.8 x W + 624
W = body weight in kg; Calculated BMR in kilocalorie (kcal)Department of Health (UK), 1991

Activity FactorsActivity Level
Bedbound, immobile +10%
Bedbound, mobile or sitting + 15-20%
Mobile, on ward +25%
Todorovic and Micklewright (2004)

Stress FactorsCondition Stress factor (%
BMR)Brain Injury
Acute (ventilated and sedated)Recovery
0-305-50
Cerebral Haemorrhage 30
CVA 5
COPD 15-20
Infection 25-45
Intensive CareVentilatedSeptic
0-1020-60
Leukaemia 25-34
PancreatitisChronicAcute
310
Sepsis / Abscess 20
Solid Tumours 0-20
Transplantation 20
SurgeryUncomplicatedComplicated
5-2025-40
Todorovic and Micklewright (2004)
Macronutrients Requirements

Macronutrient requirements
Protein
depending on the baseline nutritional status, degree of injury and metabolic demand, or any abnormal losses (e.g. open wound or burned skin)
Varies between 0.9-1.5g/kg/day for various conditions
Krause’s, 2012

Macronutrient requirements
Carbohydrate
Ensures that protein is not catabolised for energy during metabolism
Excessive administration:hyperglycaemiahepatic abnormalities ventilatory drives
Maximum infusion rate of carbohydrate: <5mg/minute/kg body weight
DAA, 2011
Macronutrient requirements
Fat
~ 10% of calories/day from fat provide 2% to 4% of calories from linoleic acid (LA) in order to prevent Essential Fatty Acid Deficiency
Soybean and safflower oils: rich sources of LA
LA: pro-inflammatory & immunosuppressive
Maximum infusion rate of fat: <0.11g/hour/kg body weight DAA, 2011

Micronutrient Requirements

Micronutrient requirements
Ready-made Parenteral Nutritional Products are free of vitamins and trace elements
The addition of vitamins and trace elements are always required
ESPEN Guidelines 2009;Casaer & Van den Berghe,
2014

MicronutrientsVitamins and trace elements addition via
the addition of:
Soluvit® N
Vitalipid N® Adult
Addamel® N

Soluvit® Nprovide the daily requirement of water-
soluble vitamins
A vial (10ml) = normal daily requirement of water-soluble vitamins
Fresenius Kabi

Vitalipid N® Adultmeet the daily requirement of the fat-soluble
vitamins A, D2, E and K1 in adults & children aged 11 years or older
One ampoule (10ml) = daily intake of fat-soluble vitamins
Contraindications: hypersensitivity to egg protein / soybean / peanut protein
Fresenius Kabi

Addamel® Ncovers basal or moderately trace elements
needs
The recommended daily does for adult patients with basal or moderately elevated needs is 10ml (one ampoule)
Contraindications: in patients with blocked bile flow, and manganese levels must be checked if treatment lasts > 4 weeks
Fresenius Kabi
Refeeding Syndrome

Refeeding Syndrome1. What is refeeding syndrome?
A metabolic disorder as a consequence of too aggressive administration of nutrition after a prolonged inadequate nutrition supply
Characterized by hypophosphataemia, hypomagnesiumaemia and hypokalaemia; with excessive sodium and fluid retention
May cause potentially lethal electrolye flucatuations involving metabolic, haemodynamic & neuromuscular problemsStanga, Z et al (2008)
Krause’s (2012)Mehanna et al (2008)
Refeeding Syndrome2. Who is at risk?
Meet ANY of the criteria:
BMI < 16kgm-2
NPO ≥ 10 days (or with minimal nutrition intake > 10 days)
Weight loss > 15% in 3 to 6 months
Hypophosphataemia, hypokalaemia, hypomagnesaemia
Stanga, Z et al (2008)

Refeeding syndrome3. How to prevent?
Start feeding at < 50% of energy requirement, rate can then be if no refeeding problem detected
For high risk of refeeding: start with 10kcal/kg/day
For very malnourished patients, start with 5kcal/kg/day, with cardiac monitoring
NICE guideline (2006)
Refeeding syndrome3. How to prevent?
Vitamin supplementation: before and for the first 10 days of refeeding
Oral, enteral or IV supplements of K, PO4, Ca & Mg should be given unless blood levels are before refeeding
NICE guideline (2006)

PN formulations
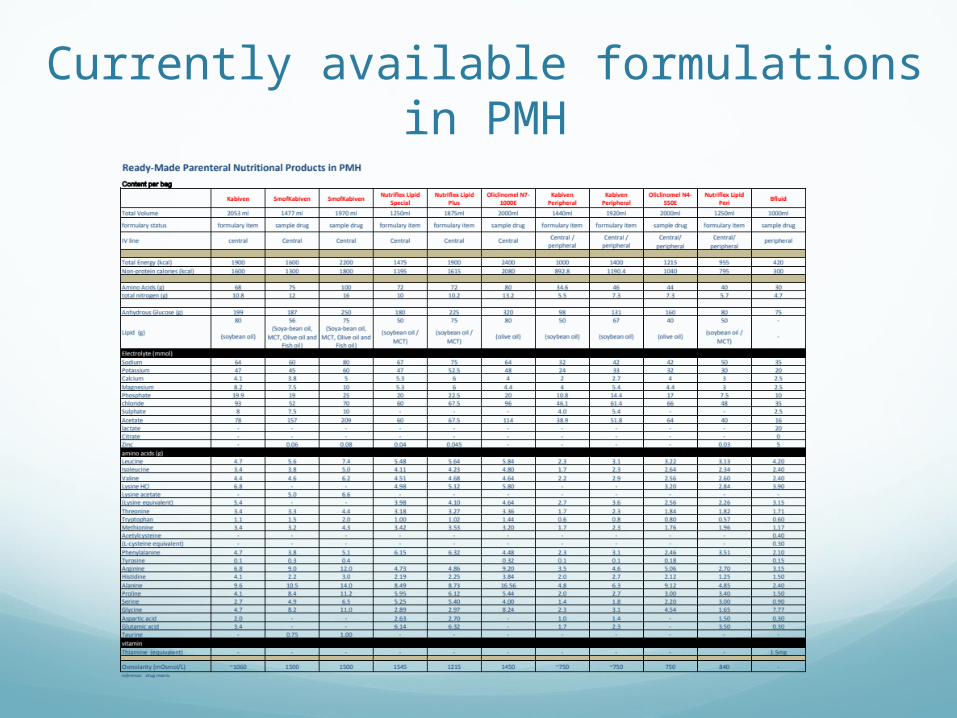
Currently available formulations in PMH
PN FormulationsBesides carbohydrate and protein content varies, type
of fat emulsions used also differ
Most commonly used is soybean oil based fat emulsion
Alternatively fat emulsions: Soybean oil + MCT Soybean oil + Olive Oil Fish oil other multi-lipids (a mixture of soy, MCT, olive and fish oil)
DAA, 2011ASPEN Position Paper, 2012

Soybean oil Examples: Kabiven Central, Kabiven Peripheral
The most commonly used fat emulsion type
Linoleic Acid (LA, n-6) comprise a 50% of total fatty acid profile
Alpha Linolenic Acid (ALA, n-3) about 10% of total fatty acid profile
omega 6 content drawback due to its pro-inflammatory potential
ASPEN Position Paper (2012)
Soybean oil + MCTExamples: Nutriflex Lipid Special, Nutriflex Lipid
Plus
Soybean oil : MCT = 50 : 50
MCT:readily oxidizableSafe source of lipidpro-inflammatory properties

Soybean oil + Olive oilExamples: Oliclinomel
Olive oil : soybean oil = 80 : 20
the content of omega 6 in formulation by ~ 75%
Higher vitamin E content for its anti-oxidating properties
ASPEN Position Paper (2012)

Multi-lipidsExamples: SMOF Kabiven
A mixture of soybean oil, MCT, olive oil and fish oil in a ratio of 30 : 30 : 30 : 10
Fish Oil:rich in omega 3 (anti-inflammatory properties)
ASPEN Position Paper (2012)

How to choose?
How to choose?1. Based on calculated energy / protein
requirements
2. Disease Specific:
Renal / Cardiac diseases Vs Fluid content of PN
BGA / pCO2 Vs CHO content

Initiation of parenteral nutrition

Initiation of Parenteral Nutrition
1. Ensure the selected formulation is compatible with the route of parenteral nutrition (central / peripheral)
2. Choice of parenteral nutrition regimenContinuous PN (Q24H)Cyclic / intermittent (Q16H/Q12H)
3. Ensure final infusion rate DOES NOT exceed the maximum infusion rate for fat and CHO

Case Study

Case StudyBackground Information
KC, 57 year-old male, admitted to PMH on 5 Aug 2013
Admission Diagnosis: Malnutrition
Past Medical History: HT, anaemia, Ca cardia with oseophago-gastrectomy, short bowel syndrome, CHB
Relevant Medications: Aminoleban EN (1 sachet), Entecavir, Vitamin K1, Slow K, Vitamin B complex

Case StudyAnthropometry:
Height 1.74m Weight 37.6kg BMI 12.4kgm-2 Ideal Body Weight: 56-69kg
Laboratory Values: Spot glucose 3.3 Alb 17 ALP 357 ALT 194
Wound x 1 (stage III)

Case StudyEstimated energy requirement:
~ 2000-2100kcal (bedbound + wound + weight )
Estimated protein requirement:
~56-69g per day
Route of nutrition:1. Oral (as much as tolerated)2. Peripheral parenteral nutrition
Case Study1. Formula selection:
Peripheral access = Kabiven Peripheral
Plan to start with small infusion rate and grade up as tolerated
Case Study2. Starting PN:
30ml/hr x 16hrs Kabiven Peripheral (+ Addamel N / Vitalipid N Adult / Soluvit N) (~333kcal, 11g protein)
Gradually stepped up to 100ml/hr x 16hrs (~1167kcal, 37g protein)
(Note: Maximum infusion rate: < 139ml/hr for 37.6kg)

One Month later (5 Sept 2013)

One month later Laboratory values: Spot glu 5.7, Alb 13, ALP/ALT normal
Wound healed
Oral intake: ~200ml/meal
Stool: BOx1 per day
PICC (central line) to be inserted the next day

One month laterPN consideration:
1. To central formula (for more nutrition to meet requirement)
2. Per case MO, patient cannot tolerate excessive volume
Nutriflex Lipid Special
(1250ml/1475kcal/72g protein)

One month laterRecommendation:
1. Nutriflex Lipid Special (+ Addamel N / Vitalipid N Adult / Soluvit N)
2. Start with 20ml/hr x 24hr, gradually step up to 52ml/hr x 24hr (~1475kcal, 72g protein)

10 months since first admission
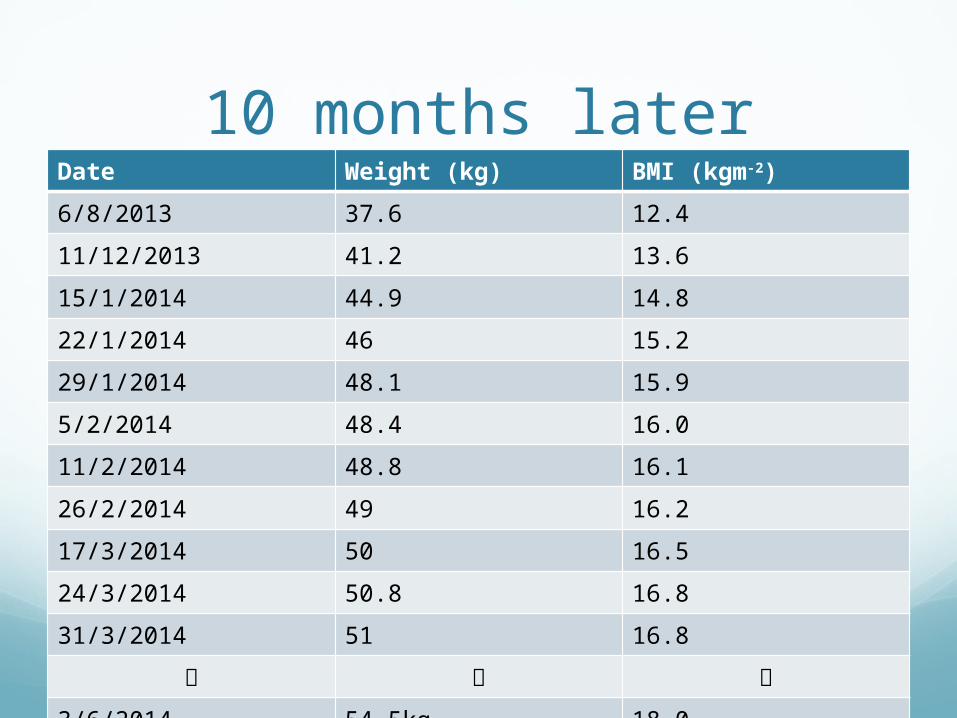
10 months laterDate Weight (kg) BMI (kgm-2)
6/8/2013 37.6 12.4
11/12/2013 41.2 13.6
15/1/2014 44.9 14.8
22/1/2014 46 15.2
29/1/2014 48.1 15.9
5/2/2014 48.4 16.0
11/2/2014 48.8 16.1
26/2/2014 49 16.2
17/3/2014 50 16.5
24/3/2014 50.8 16.8
31/3/2014 51 16.8
3/6/2014 54.5kg 18.0

10 months laterLaboratory Values: Alb 36, LFT normal, Cr 121
BO normal (once per day)
Oral Intake improved significantly: providing majority of nutrition orally (~1800kcal, 55g protein)

10 months laterPN:
Continuously titrating with oral intake
Previously: Nutriflex Lipid Special (+ trace elements) 300ml/day (354kcal, 17g protein)
Discussion with case MO: protein provision
Now: Kabiven Peripheral 1440ml (+trace elements) 500ml/day (347kcal, 12g protein)
Total: (oral + PN) = (~2100-2200kcal, ~67g protein)

Q & A Session

ReferencesStanga, Z et al. Nutrition in clinical practice – the refeeding syndrome: illustrative cases and guidelines for prevention and treatment. Eur J Clin Nutr 2008; 62: 687-94
Mehanna HM, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ 2008; 336: 1495-8
Singer P, Berger MM, Van den Berghe G, et al. ESPEN Guidelines on Parenteral Nutrition: Intensive care. Clin Nutr 2009: 28: 387-400
Casaer MP, Ven den Berghe G. Nutrition in the Acute Phase of Critical Illness. N Engl J Med 2014:370: 1227-35
Thomas B, Bishop J. Manual of dietetic practice, 4th edition.2007. Blackwell Publishing. P 71-79, p.858-860
A.S.P.E.N. Position Paper: Clinical Role of Alternative Intravenous Fat Emulsions. Nutr Clin Pract 2012 27: 150-192
Mahan L.K., Escott-Stump S., Raymond J.L. Krause’s Food and the Nutrition Care Process. 13th edition. 2012. Elsevier Saunders. p307-321
Parenteral Nutrition Manual for Adults in Health Care Facilities, DAA 2011

Ireton-Jones Energy Equations
Spontaneously breathing patients:
EEE(s) = 629 – 11 (A) + 25 (W) – 609 (O)
Ventilator-dependent patients:
EEE(v) = 1784 – 11 (A) + 5 (W) + 244 (G) + 239 (T) + 804 (B)
EEE = Estimated Energy Expenditure (kcal/day) s = spontaneously breathing v= ventilator-dependent
O = Presence of obesity: >30% above ideal body weight or BMI > 27 (0 = absent, 1 = present)
A = Age (years) W = Weight (kg) G = Gender (0 = female, 1 = male)
T = Trauma diagnosis (0 = absent, 1 = present) B = Burn diagnosis (0 = absent, 1 = present)





























