Embed Size (px)
Citation preview
Palpitations in General Practice
Dr Jess Fletcher MBChB (Hons) MRCP MRCGP
What are Palpitations?
• Palpitations are a symptom characterised by awareness of the heartbeat, often described as a strong, skipping, fluttering, racing, pounding, thudding, or jumping sensation in the chest.
• Some patients describe a sensation of having to cough or their breath being taken away.
• However, patients occasionally mean something other than palpitations (eg. chest discomfort) which may need a different line of investigation.
Causes of palpitations
• List the common causes of palpitations you see in general practice
• Can you group the causes?
Evaluation and outcomes of patients with palpitations
Weber BE Kapoor WN Am J Med 1997
• Prospective cohort study presenting with palpitations
• 197 consecutive patients
• At Student medical centre
Outcomes
• Cardiac (43%)
• Psychiatric (31%)
• Miscellaneous (10%)
• Unknown (16%)
etiology of papitations
cardiac
psychiatric
miscellaneous
unknown
But please note….
• A large proportion of patients with palpitations are diagnosed as having panic, stress, or anxiety when, instead, they have an underlying arrhythmia
Unrecognised Paroxysmal Supraventricular Tachycardia. Potential for
misdiagnosis as panic disorder Lessmeier et al Arch Inter Med 1997
• Retrospective study • 107 consecutive pts with re-entrant pSVT • pSVT missed after initial medical evaluation in 55% • Remained unrecognised for median of 3.3 yrs • Ablation therapy 81% pts • Symptom resolution 86% • Post ablation, 4% met DSM-IV criteria of panic disorder
Cardiac Causes
• List
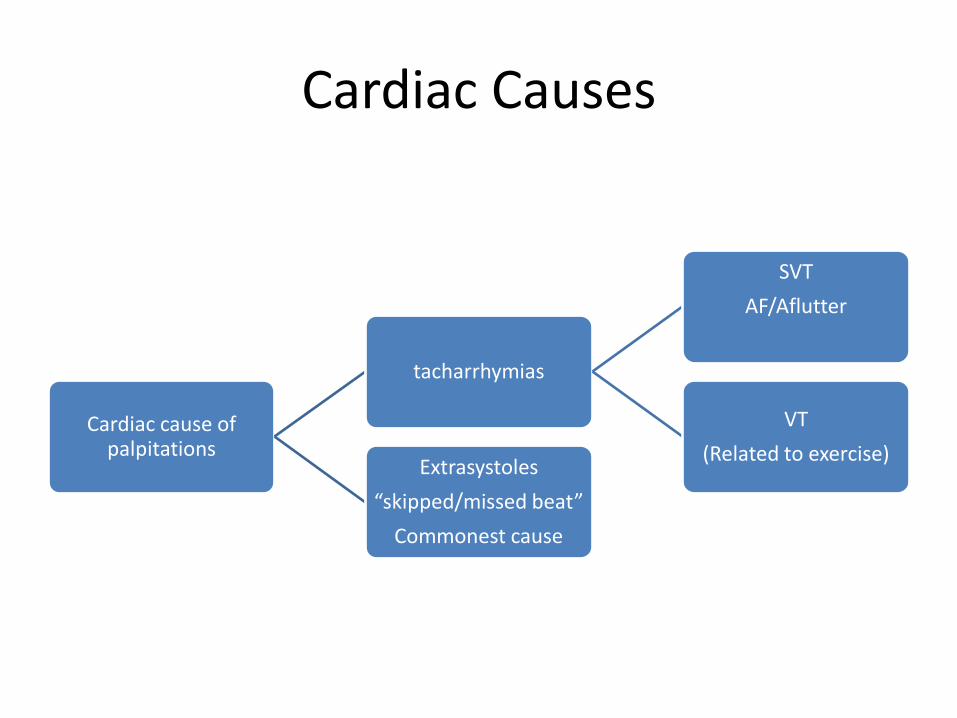
Cardiac Causes
Cardiac cause of palpitations
tacharrhymias
SVT
AF/Aflutter
VT
(Related to exercise) Extrasystoles
“skipped/missed beat”
Commonest cause
Extrasystoles
• Generally not associated with significant structural heart disease
• Common
• Frequent ventricular extrasystoles in >55 yr old more concerning (>30 per hr) might suggest underlying myocardial ischaemia
Paroxysmal supraventricular tachycardia
• Conduction abnormalities in atrio-ventricular node or bypass tracts
Atrial Fibrillation Atrial Flutter
• 5 commonest underlying causes?
Atrial Fibrillation Atrial Flutter
• Hypertension
• IHD
• Valvular heart disease
• DM
• Hyperthyroidism
• Chronic alcohol misuse
• Obesity
AF
• Classification, pathophysiology, and mechanisms of AF: key points • Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia
• AF is usually classified as paroxysmal, persistent, or permanent. • AF adversely affects cardiac haemodynamics because of loss of atrial
contraction and the rapidity and irregularity of the ventricular rate • AF causes significant symptoms in approximately two thirds of patients • AF is associated with a 1.5- to 2-fold increase in mortality • AF is associated with a 6-fold increase in risk of stroke • AF is initiated by rapid electrical activity, often arising from
arrhythmogenic foci located in the muscular sleeves of pulmonary veins. • After a period of continuous AF, electrical remodelling occurs, further
facilitating AF maintenance
Non cardiac causes
• Metabolic disorders (thyrotoxicosis, hypoglycaemia, pheochromocytoma)
• Medication induced (vasodilators, anticholinergic drugs)
• Central nervous system stimulants (caffeine, cocaine, amphetamines)
• Psychiatric disease (panic attacks, generalised anxiety disorder, depression)
History
• 7 key questions
History
1. What does the patient mean by palpitations? 2. Tap out rhythm on table 3. Duration/ Frequency 4. Severity ?have to sit down?collapse. If syncope urgent
referral 5. Associated chest pain or breathlessness (IHD associated
?fast AF)(“breath taken away” - extrasystoles 6. Exercise related? (urgent referral –
?cardiomyopthy/ischaemia/channelopathy) 7. How do they end? Can you stop them? (Valsalva/diving
reflex suggests SVT)
History continued
• Drug History –thoughts?
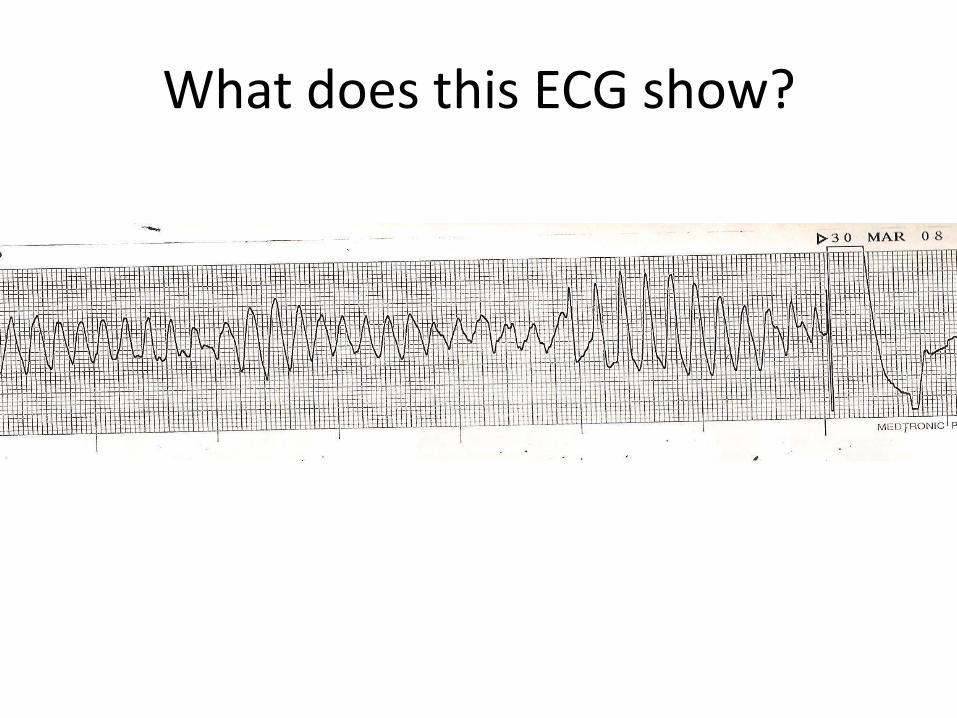
What does this ECG show?
Drugs that prolong the QT interval
• Erythromycin
• Moxifloxacin
• Haloperidol
• Amiodarone
• Amphetamines
Drugs associated with tachyarrhthymias
Drugs that are associated with tachyarrhythmias
• β agonists (salbutamol),
• antimuscarinics (amitriptyline),
• theophylline (phylocontin),
• dihydropyridine calcium channel blockers (nifedipine),
• class 1 anti-arrhythmics (flecainide, disopyramide),
Drugs
• Caffeine (sinus tachycardia )
• Alcohol (AF)
• Illicit drugs
History continued
• Fever or underlying infection (AF)
• History of Anaemia (sinus tachycardia)
• Family history sudden cardiac death <40 yrs
Brugada Syndrome
• Video BHF
Examination
• What do you look for?
Raised JVP Ankle oedema
Gallop rhythm Bi-basal crackles
Signs of heart failure
Tremor Goitre
Eye signs Thin
Thyrotoxicosis signs
Examination continued
• Listen for murmur
• Check for pallor
• Check BP for underlying hypertension
Tests
FBC
U+E
TFT
Case
• 40 yr old man
• Walk in -Asking for urgent GP appointment
• “Rapid fast palpitations and light headed”
• Told in past to see GP urgently if reoccurs for assessment while symptomatic
• What do you do?
• History:
• 3 previous episodes
• Self limiting after 10-15mins
• No chest pain
• No other significant history
• Examination
• P160bpm regular
• BP 98/50
• No sign of heart failure
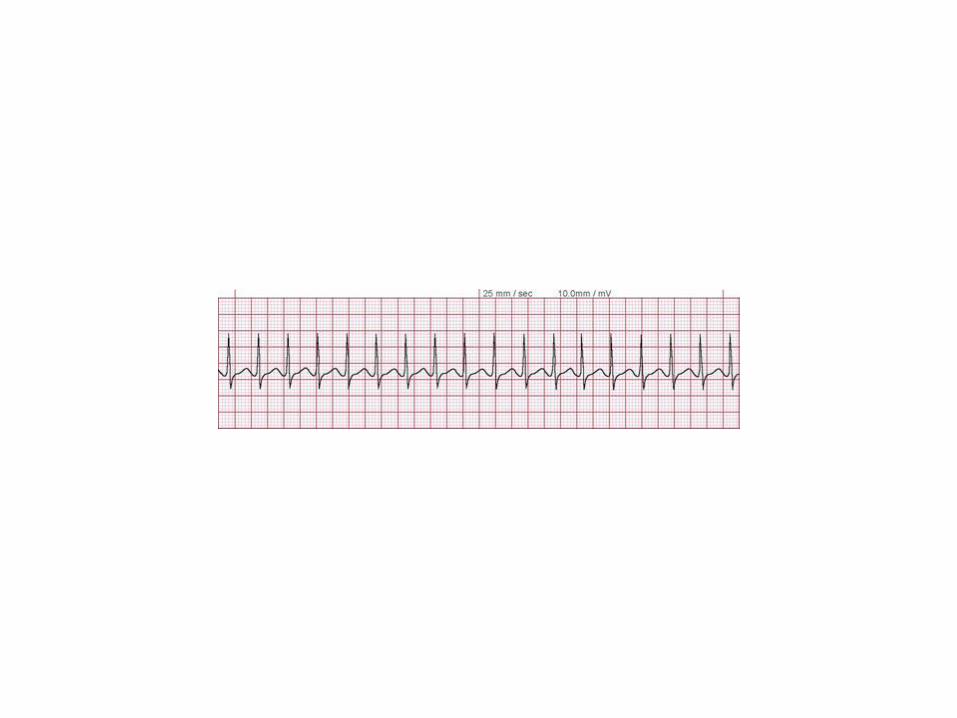
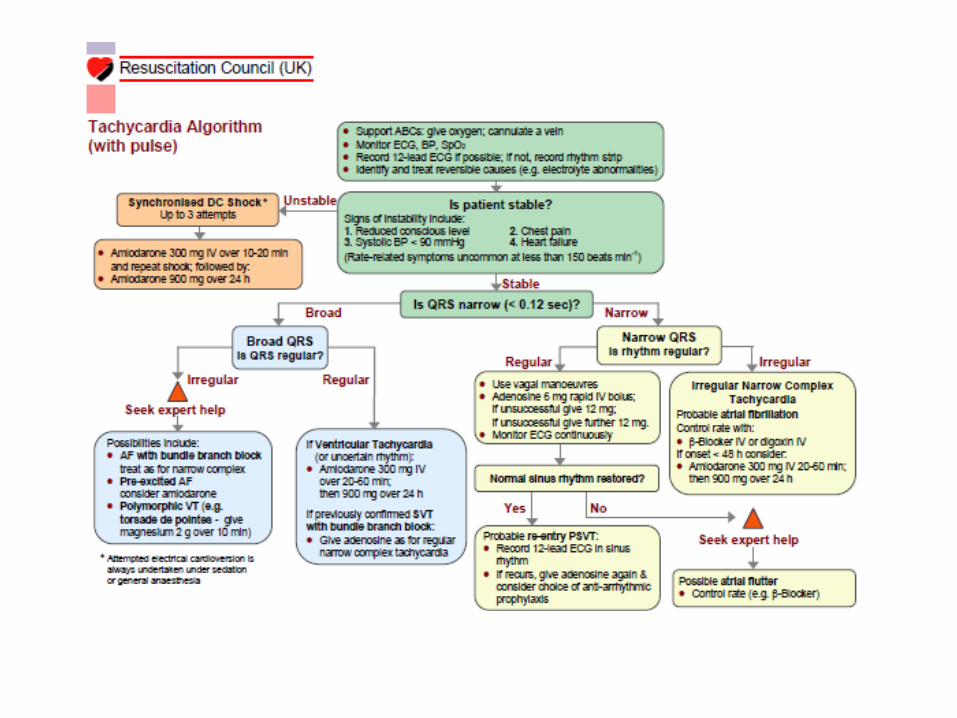
SVT
• Vagal manouvres, diving reflex
• Sinus rhythm restored
• Copy of ECG to patient to keep
• For patients with infrequent palpitations, asking them to attend your practice or the emergency department to have an electrocardiogram recorded during symptoms is not unreasonable.
ECG
• What are you looking for on ECG to give clues as to underlying cause?
12 lead electrocardiogram practice pointers for palpitations—when to consider specialist referral
• Atrial fibrillation or atrial flutter • Second degree atrioventricular block • Third degree atrioventricular block • Myocardial infarction • Left ventricular hypertrophy (with or without strain
pattern) • Left bundle branch block • Abnormal T waves and ST segments • Pre-excitation (Wolff-Parkinson-White pattern of a slow
rise in the initial portion of the QRS (delta wave)) • Abnormal QT/QTc interval
If ECG normal
• Guidelines from the American College of Cardiology
• Recommend Holter monitoring in patients with palpitations and syncope , near syncope (episodic dizziness or lightheadedness in patients with known cardiac disease), and recurrent palpitations if the resting ECG is normal.
Ambulatory Rhythm Monitors
• 24 hour Holter monitor to patients who have at least daily symptoms,
• a 48 hour Holter monitor to those with symptoms on most days,
• and a seven day monitor to those with weekly symptoms, even if the 12 lead electrocardiogram is normal.
• Inappropriate use of short periods of ambulatory monitoring for infrequent symptoms is cumbersome for patients, delays the diagnosis, and is costly.
Urgency of referral
• Low risk features for which referral is not mandatory • Isolated palpitations (described as skipped beats,
pounding, or short fluttering) that are not provoked by exercise and not associated with symptoms such as lightheadedness, syncope, persistent breathlessness, or chest pain;
• No history or signs of structural heart disease, heart failure, or hypertension and no family history of sudden cardiac death; and
• A normal 12 lead electrocardiogram. • In these cases, palpitations are generally due to
extrasystoles or sinus tachycardia.
Urgency of Referral
• Urgent cardiology referral
• Palpitations during exercise;
• Palpitations associated with syncope or pre-syncope;
• Family history of sudden cardiac death or inheritable cardiac conditions; or
• Second degree or third degree atrioventricular block on the 12 lead electrocardiogram.
Driving
• In the United Kingdom, the Driver and Vehicle Licensing Agency (DVLA) regulations state that if an arrhythmia has caused incapacity or is likely to cause incapacity, the patient must not drive.
• It is the clinician’s responsibility to notify the patient of this, document it in the case records, and advise the patient to contact the DVLA, who will make the final recommendation.
Citations
• Assessment of palpitations
• BMJ 2016; 352 doi: https://doi.org/10.1136/bmj.h5649 (Published 06 January 2016)Cite this as: BMJ 2016;352:h5649
• Markides V, Schilling RJ
• Atrial fibrillation: classification, pathophysiology, mechanisms and drug treatment
• Heart 2003;89:939-943





























