Embed Size (px)
Citation preview

June 2012Issue 54
The international newspaper for vascular specialists BIBA Publishing
I N T E R N A T I O N A L
The first TASC group origi-nally reported in 2000;TASC II in 2007. There
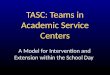
were reports that TASC IIb wasbeing worked on but it was neverpublished as the plan was tomove the discussions into TASCIII. Preparations for TASC III arenow underway. At CX, a seriesof questions were put to theaudience, and their opinionrevealed some of the difficultiesthat TASC III contributors willhave in achieving a workableconsensus.
To the question “Did youexpect TASC anatomical lesionsto change from 2000 to 2006?”,the majority of voters, 71%, said“yes”. To “How should TASC III
lesions be classified? Fixedanatomically, so that treatmentmodality changes over time?”68% voted yes. Fifty nine percent of the audience then said thiswould NOT determine to which
discipline a patient is referred. To the question “As treatment
urgency to intervene variesaccording to severity of presenta-tion, would this lead to a plethoraof TASC recommendations
according to presentation severi-ty?” 60% of the delegates votedyes.
Then, 73% voted that the indi-vidual clinician should determinemode of intervention. The vote tothe last question was particularlytelling: 75% voted yes to “Isthere a danger of TASC IIIattempting to consider too manyeventualities?”
“There is a clear request toTASC III authors to fix the anato-my and not constantly modifyTASC and to keep it simple,”Greenhalgh, London, UK, wrote.“My personal ‘take’ on this is thatit is expected that more of thedefined TASC anatomical lesions
The CX Symposium plenary session on the Inter-society Consensus for the Management of Peripheral ArterialDisease (TASC), under the chairmanship of interventional radiologist Johannes Lammer, Vienna, Austria, andvascular surgeon Roger Greenhalgh, London, UK, gathered the TASC co-chairs William Hiatt, Denver, USA, andLars Norgren, Örebro/Lund, Sweden. The panel also included Michael Jaff (internist, Boston, USA), Jim Reekers(interventional radiologist, Amsterdam, The Netherlands), Henrik Sillesen (vascular surgeon, Copenhagen,Denmark), Vincent Riambau (vascular surgeon, Barcelona, Spain), and Erich Minar (angiologist, Vienna,Austria). The plenary, which addressed problems with TASC IIb and preparations for TASC III, involved theaudience as an unofficial public focus group
Is the task for TASC IIIconsensus too great?
Continued on page 2
Profile:
Ross NaylorPage 20
Peter Schneider:
Dragons’ Den Page 16
William Hiatt Lars Norgren
“The superficial femoral arteryis a hostile environment forstents. Stents are subjected
to complex biomechanical stresses, andstent fractures and restenosis are prob-lematic. A bioabsorbable vascular scaf-fold has been long awaited,” Holdensaid.
The Stanza scaffold is the first self-
expanding bioresorbable technologybeing developed for treatment of ather-osclerotic disease in the superficialfemoral artery, Holden said. He addedthat “the scaffold design is a compositestructure of strong PLGA fibres in com-bination with an elastomer. This designenables the scaffold’s key attributes of
Continued on page 6
Gene linked to abdominalaortic aneurysms is foundAt the CX Symposium, Matt Bown, Leicester, UK, presented datafrom an international study that identified a gene linked to thedevelopment of abdominal aortic aneurysm. During the discussionsession, after the results were presented, the point was made thatthe interaction between the gene LRP1 and environmental factorswas key
“Abdominal aortic aneurysm isa genetic disease, with posi-tive family history found in
approximately 20% of patients. There isan increased risk, approximately 12-fold,in first degree relatives,” Bown said.
He told CX delegates that the investi-gators carried out a genome-wide associ-ation discovery study of 1,866 patients
with abdominal aortic aneurysm and5,435 controls and replication of promis-ing signals (lead single-nucleotide poly-morphism [SNP] with a p value<1×10−5) in 2,871 additional cases and32,687 controls and performed furtherfollow-up in 1,491 abdominal aorticaneurysms and 11,060 controls.
Continued on page 12
www.vascularnews.com facebook.com/vascularnews @VN_publishing
The first-in-man study results with a new bioresorbable scaffoldfor superficial femoral artery lesions were presented by AndrewHolden, Auckland, New Zealand, at the CX Symposium in London,UK. Holden described the Stanza Bioresorbable Scaffold Systemfrom 480 Biomedical and initial case experience from the firstpatients treated in the STANCE trial
World’s first experience with abioabsorbable stent for the superficialfemoral artery presented at CX
Page 29
CCSVI is an entity and a
subset of MS, 37% say at CX
GLIMPSE INTO THE FUTURE
Yes 68%No 32%
Yes 41%No 59%
Yes 60%No 40%
Yes 73%No 27%
Yes 75%No 25%
Voting resultsDid you expect TASCanatomical lesions tochange from 2000 to 2006?
How should TASC IIIlesions be classified? Fixedanatomically, so that treat-ment modality changesover time?
Would this determine towhich discipline a patient isreferred?
As treatment urgency tointervene varies accordingto severity of presentation,would this lead to a pletho-ra of TASC recommenda-tions according to presenta-tion severity?
Should the individual clini-cian determine mode ofintervention?
Is there a danger of TASCIII attempting to considertoo many eventualities?
Yes 71%No 29%

September 2010
BIBA Publishing
2 Lower limb June 2012
will move to the endovasculardomain. Nevertheless, this doesnot dictate mode of treatmentwhich is down to the clinicianresponsible. Also, if presenta-tional details and clinical dimen-sions are introduced, this wouldconstitute overload and the CXaudience 2012 would opposethat move. There was apprecia-tion from the audience and somesympathy that the ‘task’ ofTASC is a complex problem.”This year, the CX audience com-prised 56% vascular surgeons,21% interventional radiologists,9% interventional cardiology,10% other cardiovascular spe-cialists and 5% nursing or vascu-lar technology.
Balancing consensusand evidence
A theme that recurred was theissue of balancing consensus andscientific evidence. Lammersaid: “With TASC IIb, the chal-lenge really was the lack of evi-dence. The question is, and thisis a problem also for TASC III,how much should consensusoverrule evidence, or lack ofevidence?”
Hiatt, who spoke on the topic“Why was TASC initiated andwhat is achievable?”, said thegoal of TASC (2000) was toachieve a consensus in the“management of individualpatients with identical condi-tions. TASC (2000) aimed torepresent all relevant key vascu-lar disciplines… and identifyand represent minority views,”he said.
Hiatt noted that TASC wasthe first major vascular guide-line that represented all vasculardisciplines across Europe andNorth America and achievedconsensus on all but one recom-mendation. He said that it estab-lished TASC lesion classifica-tion to guide revascularisationdecisions.
Hiatt noted that the TASC IIIWriting Group represents adiversity of expertise, vasculardisciplines, societies, and geog-raphy. “Every reference isreviewed prospectively for qual-ity and relevance. The writinggroup had declared all industrydisclosures and there was appro-
priate separation from industrysupport,” he noted.
Hiatt also told CX delegatesthat the disagreements on spe-cific recommendations werenoted in final text with societiesin agreement and in disagree-ment listed.
He also outlined what wasachievable with TASC III atCX. “TASC III seeks to achievea consensus between surgicaland endovascular societies. Theresponse to TASC IIb was dis-appointing but current inter-societal engagement is encour-aging,” he noted.
On the question of whether itwas possible to create a moreintegrated and clinically-rele-vant classification of peripheralartery disease, he stated thatTASC III would include the keycomponents of: patient, limband lesions.
He added that TASC IIIwould establish new standardsfor regulatory approval andreimbursement of new therapies.For critical limb ischaemia, itwould expand on amputation-free survival to include healingof ischaemic ulcers, relief ofischaemic pain, avoidance ofadditional procedures andimprovement in functional sta-tus, he said.
Norgren then spoke on “Thepurpose of TASC II and TASCIIb; what is expected of TASCIII?” He said that while TASC(2000) was intended mainly forspecialists, TASC II aimed alsoat reaching referring physiciansfocusing on:n Key aspects on diagnosis and
managementn Updating and providing new
informationn Making graded recommenda-
tionsThe resulting TASC classifi-
cation was related to the appro-priate mode of revascularisationwith TASC A lesions beingappropriately treated byendovascular means, D appro-
priate for open surgery,endovascular revascularisationbeing preferred for TASC B andsurgical revascularisation for C.
“The outcome of TASC II
was >1,600 citations on
Google Scholar of which
some were critical.
Therefore TASC IIb set out
to update the TASC lesion
classification; add an
infrapopliteal classification
and clarify the role of
endovascular treatment (vs.
surgery) based on technical
developments and profes-
sional skill despite the lack
of level 1 evidence,” said
Norgren.
He told delegates that the prin-cipal conclusion of TASC IIbwas an endovascular firstapproach, with open surgery forcomplex lesions or endovascularfailure. “However, surgical soci-eties saw this conclusion asbeing weighted too much infavour of endovascular therapiesand the recommendations foropen surgery as too weak,” hesaid.
He also outlined some of thecontroversial issues pertainingto TASC IIb. “Scientificallyvalid rigorous guidelines areexpected, but the trials rarelyexist. The recommendationswere based on grade C evidencein line with practical handling.In TASC, TASC II, TASC IIb,the recommendations werebased on single lesion (anatomi-cal) management,” he said.“Consensus was not achieveddespite endorsement from mostsocieties, and the decision wasmade to move to TASC III,”Norgren added.
He told delegates that inpreparation of TASC III, “Allbasic information achieved forTASC IIb is set to be furtherdiscussed and included asappropriate. There is also amove to expand discussion fromprior TASC guidelines, which
were lesion-based to apatient/limb/lesion considera-tion. The point that critical limbischaemia differs from intermit-tent claudication was beinghighlighted and TASC III wouldconsider issues of experience,availability, and resources. Allstrategies (including endovascu-lar, surgery and hybrid) requireactive and honest individual andsocietal discussion for consen-sus,” he said.
What is expected ofTASC III?
Norgren told delegates thatTASC III is intended to satisfyall specialists, comply with tech-nical development, update theevidence grading, modify thechange in evidence, focus on rel-evant classification(s), increasereferencing, reflect the situationin developing countries and staytruly global.
“Currently, all societies arecommitted, relevant ChapterGroups have been formed, thereis an ongoing literature searchand details of evidence gradingare being worked out,” he said.
What were theproblems with TASCIIb?
Jaff said that TASC was a trueattempt to collaborate acrossnations and specialties to devel-op guidelines for the diagnosisand management of peripheralarterial disease.
“So, why TASC IIb?” heasked, and then outlined thatsignificant time had passedsince the publication of TASCII. There has been a rapidexpansion of endovascular tech-nologies to treat peripheral arte-rial disease and major practiceshifts to an “endovascular first”paradigm. He said that the goalof IIb was to update TASC II asan interim report and summarisepublished literature since TASCII. There was also a goal toupdate the anatomic recommen-
dations regarding treatmentstrategies and outline situationswhere an “endovascular first”approach is reasonable.
Jaff noted that VascularSurgery had been unwilling tosign off on TASC IIb, claimingthat the recommendations werebased on low quality literature.
“The Society for VascularSurgery could not endorse an‘endovascular first’ approach forany anatomic scenario,” Jaffnoted.
He said that vascular surgeonsidentified and emphasised theweakness of catheter-basedintervention, poor durability ininfrainguinal peripheral arterialdisease and said that surgicalpatency rates were far superior.They also said that catheter-based intervention could burnbridges to surgery down theroad, was costly and the datawere limited and of poor quality.
“So, why endovascular first?”he asked and outlined that it wasa low-risk procedure in skilledhands that was unlikely to“burn” the surgical bridges.Also, “Surgical revascularisa-tion is not without risk, cost,and need for repeat intervention,similar to percutaneous translu-minal angioplasty. The ideal sur-gical candidate is becomingharder to find due to older age,tissue loss and poor conduit.The ideal management willprobably be integrated/hybridon a background of comprehen-sive medical therapy.”
After the symposium,Norgren told Vascular News: “Iam pleased that the TASC dis-cussion went so well. WilliamHiatt and I feel that we havegood support for TASC III intrying to solve the problematicissues adequately with the col-laboration of so many devotedpeople.”
Read the full story on the TASC
plenary session at CX on
www.vascularnews.com
Is the task for TASC III consensus too great?Roger Greenhalgh, Johannes Lammer, Vincent Riambau, William Hiatt, Erich Minar and Jim Reekers
Continued from page 1
Michael Jaff




September 2010
BIBA Publishing
6 Updates June 2012
flexibility and radial stiffness, similar toself-expanding metallic stents.Preclinical animal studies demonstratebiocompatible resorption of the scaffoldover six to 12 months. The scaffold,which uses a conventional retractablesheath delivery system, is being tested inthe STANCE trial in target lesions up to100mm in length and diameters between4.6–6mm.”
The STANCE trial is a prospective,single-arm, multicentre trial of the Stanza
scaffold in patients with symptomaticatherosclerotic disease of the superficialfemoral artery. The primary endpoint ofthe trial is major adverse events at sixmonths, with evaluation of vessel paten-cy and other functional and quality of lifemetrics assessed three, six, 12 and 24months post-procedure. 480 Biomedicalexpects to enrol up to 60 patients in theSTANCE study at sites in New Zealand,Australia and Europe by the end of 2012.
Holden told delegates that, in theAuckland City Hospital experience with
nine patients treated to date, 100% proce-dural success was achieved with theStanza scaffold. He noted that the scaf-fold was accurately deployed in the tar-geted superficial femoral artery lesion
and blood flow was restored to the leg asevidenced by angiography and Dopplerultrasound.
“At Auckland City Hospital, treatedvessels were also imaged using opticalcoherence tomography (OCT), a modali-ty that has been used in coronary inter-ventions but never before used in clinicaltrials for superficial femoral artery treat-ment. Post-procedure OCT imagesshowed good vessel wall apposition withthe Stanza scaffold. Additional OCT andMR angiographic analysis of the treatedarea will be conducted at six and 12-months to enable visualisation of thescaffold as it dissolves over time,” hesaid. “Early follow-up is promising.Further case recruitment and follow-up isawaited.”
World’s first experience with abioabsorbable stent for the superficialfemoral artery presented at CXContinued from page 1
Andrew Holden
Ivancev described the evolution, from infra-renalaortic devices to aortic arch endovascularinterventions. “I am not quite sure that all of you
are clear over who was the man who started all ofthat – that was Nicholay Volodos. The world’s firstEVAR was performed in 1987 by him in Kharkov, inthe northern part of the Ukraine, and introduced in anarticle written in 1988,” Ivancev said. “He was thepioneer who started the endovascular stent graftrevolution.”
Roger Greenhalgh, London, UK and CX programmechairman, also praised the work of Volodos and askedpeople to stand if they thought it was worthwhilesending a message, via Ukranian delegates, to Volodosabout how much everyone appreciated Volodos’achievements – the entire audience stood up tocelebrate his work.
Volodos used the self-fixing syntheticendoprosthesis to perform his first transfemoralremote endosprothesis implantation in an iliac artery.This was in May 1985. Two years later, he performedan endovascular repair for an aneurysm in thedescending section of the thoracic aorta.
The first EVAR procedure reported in the literaturetook place on 7 September 1990, when Juan Parodi,Julio Palmaz and HD Barone at the InstitutoCardiovascular de Buenos Aires, Argentina, treated anabdominal aortic aneurysm patient. The aneurysm wasexcluded endoluminally with a Dacron graft that wasanchored at the proximal infrarenal neck with astainless steel balloon-expandable stent.
Ivancev said, “Volodos realised the mechanicalproperties required of a stent graft. He designed,manufactured and implemented the first stent graft andhis principles are still valid and exploited by ustoday.”
Volodos’ early experience was recorded in a papertitled “Experience with endovascular stent grafts forarterial disease from 1985 to present”, which waspresented at the 21st Annual Symposium on CurrentCritical Problems – New Horizons and Techniques inVascular Surgery in 1994.
He wrote: “Trying to realise more effectivelyCharles Dotter’s attractive idea of implanting aprosthesis in not easily approached vessels through asuperficially lying vessel, we developed a self-fixingsynthetic endoprosthesis in 1984. This endoprosthesis
received the national patent of the former USSR on 22May 1984. At that initial stage we called the method aremote endoprosthesis.”
“The design feature of the endoprosthesis was a
fixing element in the form of a radial zigzag
shaped cylindrical spring. The spring was made
from stainless steel wire 0.4–0.5mm in the diam-
eter. The height of the fixing element was about
18mm. As a rule, the number of rings was six or
seven,” Volodos reported.
The first animal studies with the endoprosthesiswere conducted in dogs, with the transfemoral prosthe-sis implanted in the thoracic aorta. “The results of thestudy showed good function of the endoprosthesis sixmonths after the operation,” Volodos said.
Volodos and colleagues used these results as the basisto perform endoprosthesis implantation in patients. “Thefirst operation of transfemoral remote endoprosthesisimplantation in the iliac artery in the clinic was per-formed on 4 May 1985. It was done in combination with
a simultaneous femorotibial bypass,” he wrote.In the first report, Volodos said that 19 patients had
been treated for stenosis and occlusions of the iliacarteries. “Positive results were achieved in 17 patientsimmediately after operation and in 15 patients in thelate period (from one to eight years).”
“Transfemoral remote endoprosthesis implantationwith the self-fixing synthetic endoprosthesis in case ofthe traumatic aneurysm of the descending section ofthe thoracic aorta was performed on 24 March 1987. Itwas performed in four patients, with positive results inall of them. At 7.5 years of follow-up, it has showngood function of the endoprosthesis.”
After that, Volodos performed endoprosthesis implan-tation of the abdominal aorta in five patients – two ofthem received a bifurcated synthetic endoprosthesis.
“The accumulated experience with the self-fixingsynthetic endoprosthesis permits us to consider thatremote endoprosthetics should have a place in thetreatment of patients with lesions of the aorta and mainarteries,” Volodos concluded in the paper.
As Nicholay Volodos, who developed a self-fixing synthetic endoprosthesis in the former Soviet Union in 1984, was unable to make CXSymposium, Krassi Ivancev, London, UK, spoke about the early history of endovascular repair on his behalf
Nicholay Volodos Krassi Ivancev
CELEBRATING THE PAST
Nicholay Vodolos’ work receives astanding ovation from CX delegates


September 2010
BIBA Publishing
8 Drug elution June 2012
Preliminary results from the 12-month follow-up of thePACIFIER trial presented at theCX Symposium in London, UK,showed significantly lowertarget lesion revacularisationwas needed for patients in thedrug-eluting balloon group vs.the percutaneous transluminalangioplasty group. Similarly,six-month follow-up fromFREEWAY demonstrated a lowertarget lesion revascularisationrate with the Freeway drug-eluting balloon and stent incomparison with plain oldballoon angioplasty and stent
Michael Werk, Berlin, Germany,presented the preliminary 12-month results of the PACIFIER
study, which is a randomised, multicentretrial that evaluated the prevention ofrestenosis with paclitaxel-coated angio-plasty balloons in stenosis or occlusionof femoropopliteal arteries.
Werk said that the In.Pact Pacificdevice (Medtronic) significantly reducedneointimal hyperplasia and restenosisrates compared with standard percuta-neous transluminal angioplasty in claudi-cants. He added that the six-month out-comes had shown that the drug-elutingballoon was associated with a -0.01mmlate lumen loss compared with 0.65mmfor standard percutaneous transluminalangioplasty (p=0.0014) – of the ran-domised controlled trials so far for drugeluting balloons, this is the best result forlate lumen loss.
The results showed that, for a groupof 83 completely analysed patients, tar-get lesion revascularisation was 7.7%with the drug-eluting balloon and 29.3%with angioplasty (p=0.02), there were noamputations in either groups, and therate of death was zero in the drug-elut-ing balloon group and 4.9% in theangioplasty group (p=0.49). The com-posite major adverse events rate was7.7% for the drug-eluting balloon groupand 34.1% for the angioplasty group(p=0.006).
Concluding, Werk said that the final12-month clinical results were awaitedand, so far, no coating-related adverseevents had been noted. He said: “PACI-
FIER confirms and reinforces the role ofdrug-eluting balloons as already seenfrom previous similar trials.”
FREEWAY study
Presenting the six-month results of theFREEWAY study, Stephan Duda, Berlin,Germany, said the study is investigatingthe inhibition of restenosis by stentingand angioplasty with a paclitaxel-elutingballoon (Freeway, Eurocor) postdilatation
compared with stenting and angioplastywith plain balloon postdilatation in thetreatment of superficial femoral artery orPI-segment lesions.
The multicentre, open, prospective ran-domised trial will enrol 200 patients withstenotic or occluded de novo lesions at15 German and Austrian centres. The pri-mary endpoint is the rate of clinicallydriven target lesion revascularisation atsix months. Forty six patients havereached six months of follow-up. Dudashowed cases of lesions treated with thedevice. The preliminary results, he said,demonstrated a low target lesion revascu-
larisation rate of 8.3% after Freewaydrug-eluting balloon and stent vs. 14%after plain old balloon angioplasty andstent at six months of follow-up.
Above- and below-the-kneelesions
Also at CX 34, Fabrizio Fanelli, Rome,Italy, presented the six-month results ofthe DEBELLUM trial. DEBELLUM(Drug-eluting balloon evaluation for
lower limb multilevel treatment) is a ran-domised, investigator-initiated trial thataimed to confirm the safety and efficacyresults of drug-eluting balloon vs. con-ventional angioplasty that have been seenin different studies assessing superficialfemoral artery and below-the-kneelesions. DEBELLUM included above-and below-the-knee lesions.
Fifty patients presenting with sympto-matic arterial disease due to claudicationor critical limb ischaemia were ran-domised to an IN.PACT drug-eluting bal-loon or standard angioplasty. The 122lesions were located in the superficial
femoral artery (72.1%), popliteal artery(3.3%) and infrapopliteal arteries (24.6%).Overall lesion length was 7.6±0.6cm inthe drug-eluting balloon group vs. 7.8±0.7cm in the angioplasty group.
In each arm – and exclusively for thesuperficial femoral artery portion – stentswere electively implanted at the discretionof the operator in 38.1% of the cases inthe drug-eluting balloon arm vs. 34.7% inthe angioplasty arm (p=ns) to deal withtypically long or calcified lesions. In caseof stent implantation, the drug-eluting bal-loon (or angioplasty in the control arm)was used for post-dilatation.
At six month follow-up, late lumenloss was significantly lower in the drug-eluting balloon arm vs. the angioplastyarm: 0.5±1.4 vs. 1.6±1.7 (p<0.01). Suchsignificant difference was maintained inthe sub-analysis of lesions treated withand without stents.
Fanelli, who is the principal investi-gator in the trial, told delegates that,although small, “this randomised studybuilds and contributes to raise confi-dence on the role of drug-eluting bal-loons within the variegate clinical andanatomical setting of lower limb periph-eral arterial disease. DEBELLUM offersconsistent results to what has beenobserved in other DEB-IN.PACT studiesand reveals new interesting signals onthe potential use of drug-eluting bal-loon,” he concluded.
In April 2012, Medtronic announced that it wouldinitiate the IN.PACT Global SFA Trial, a single-arm, real-world study of the In.Pact Admiral
drug-eluting balloon for revascularisation of femoral-popliteal arteries in patients with claudication and restpain.
The study will be part of the company’s drug-eluting balloon programme, which already includes
eight registries and 10 randomised controlled trials.The study, which will enrol 1,500 patients across
approximately 80 centres, represents the largest studyever conducted in superficial femoral arteryrevascularisation. The primary endpoint is clinically-driven target lesion revascularisation at 12 monthsand primary patency at 12 months for the “imagingcohort” with either in-stent restenosis or long lesions
>10cm. This controlled study will have independentmonitoring, corelab evaluation and Clinical EventCommittee adjudication to contribute to therobustness and reliability of results. Patients will befollowed up to five years.
“A single-arm study of this size offers unrivalledvalue in the assessment of real world population andpatient subgroups characterised by either isolated orcombined complexities such as long lesions, in-stentrestenosis, heavy calcifications, total occlusions etc,”said Gunnar Tepe, Rosenheim, Germany, chairman ofthe Study Steering Committee, at the Charing CrossSymposium.
Largest-ever superficial femoral arterydrug-eluting balloon study launched
First time presentation of one-year results fromPACIFIER reinforces role of drug-eluting balloons
Michael Werk Stephan Duda Fabrizio Fanelli
PACIFIER confirms and reinforces
the role of drug-eluting balloons
as already seen from previous sim-
ilar trials“ ”


September 2010
BIBA Publishing
10 Clinical trials June 2012
Ron Balm, Amsterdam, TheNetherlands, presented the AJAXresults, and Regula von Allmen,
London, UK, presented on the SWIFTstudy (Swiss ruptured aneurysmfavourable transport), which investi-gates whether the time from diagnosis tointervention relate to operative death ofruptured abdominal aortic aneurysm.
“Some excellent results have beenreported in Switzerland, which is a cir-cumscribed country where the centresperforming vascular surgery are clearlyidentified,” she said.
Von Allmen told delegates that thereare great variations between centres inthe country.
“Reports from Zurich show that
50% of the ruptured aneurysm
patients are managed by endovas-
cular means and 50% by open
repair. Zurich reports excellent
results for EVAR with a 30-day mor-
tality rate of 13.5%; open repair has
a mortality rate of 32.4%. But if
patients look anatomically unsuit-
able for EVAR, then this may not be
a fair comparison between open
and endovascular repair.
“However, when we look at data fromBern, there are only 4% who are treatedby endovascular means and the vastmajority, 96%, are treated with openrepair, and the overall 30-day mortality
is 15.3%.“From this we can see that there are
pockets of excellence in the treatment ofruptured abdominal aortic aneurysm inSwitzerland. As a consequence, it isclaimed by one centre that it is unethicalto carry out treatment other than EVARfor ruptured aneurysms, but there areobvious counter claims for open repairbased on the data from Bern. Disparitiesin views often point to uncertainty andthere is no proof that surgical approachis the key,” she said.
Close on the heels of this presentationcame the results of AJAX, whichshowed that indeed there was no differ-ence between EVAR and open repair inthe treatment of ruptured abdominal aor-tic aneurysms.
The primary endpoint of AJAX wascombined death and severe complica-tions at 30 days. The hypothesis wasthat EVAR would do better than openrepair with endpoint rate of 0.40 and0.65 for open repair, β=0.20, α=0.05 in asample size of 112 patients. Secondaryendpoints were length of hospital andintensive care unit stay, intubation/venti-lation and use of blood products.
“The trial area covered 1.2 millioninhabitants and three trial centres andseven regional hospitals contributeddata. All patients with rupturedaneurysms in the trial area were identi-fied and followed,” said Balm.
He told delegates that the preferredEVAR technique was use of an aorto-uni-iliac graft with contralateral occlud-er and femorofemoral crossover bypass.
“Between April 2004 and February2011, 520 patients with ruptured abdom-inal aortic aneurysms were enrolled inthe trial and 90% (466) were enrolled ina trial centre.”
Three hundred and ninety fivepatients were evaluated with CTA, and240 were found to have unfavourableanatomy for EVAR. Thirty nine patientswere excluded, of these 16 were unfitfor open repair, 11 were excluded forlogistical reasons, seven for haemody-namic instability following CT, and fivepatients refused surgery.
Balm said, “116 patients were ran-domised: 57 to EVAR and 59 to openrepair. The results showed that in termsof the primary endpoint EVAR had acombined and severe complications rateof 42% (24/57) at 30 days. In the openrepair group, this rate was 47% (28/59),(ARR 5.4% [95% CI -13 to +23]).
These results showed, said, Balm, thatthe hypothesis that EVAR is better thanopen repair, could not be confirmed.
With regard to the secondary end-points, ICU stay with open repair was 48hours while it was 28 hours with EVAR(p=0.14); hospital stay was nine dayswith EVAR and 13 days with open repair(p=0.57); 39 patients had to use amechanical ventilator with EVAR while52 did so with open repair (p=0.002).Balm said, “Blood loss with EVAR was500ml while it was 3,500ml with openrepair (p<0.001). Forty five EVARpatients needed blood during the surgerywhile 56 patients did so after open repair(p=0.01).
“EVAR performed a little better on the
secondary endpoints,” Balm said.He told CX delegates that death with
EVAR was 21% (12/57) while with openrepair it was 25% (15/59).
“Was there a selection of haemody-namically stable patients?” asked Balm,noting that 17% of the entire cohort washaemodynamically unstable (78/466). “Inthe randomised controlled portion, 20%was haemodynamically unstable(23/116),” he said.
Additionally, he also posed the ques-tion of whether the triallists had selectingsimple anatomy, by drawing attention tothe death rate following open surgery inpatients with unfavourable anatomy,which was 26% in the cohort (58/222).
The 30-day death rate of all consecu-tive patients who underwent surgery was30% (138/454) (95% CI 26–35%).
Balm cited data from Visser P et al thatwas published in EJVES in 2005. Thepopulation-based analysis showed a 41%in-hospital operative mortality in TheNetherlands (95% CI 40–42%)
Importantly, said Balm, “all comers”were consecutively enrolled in the analy-sis that this was a major strength ofthis study.
In conclusion, Balm said, “With
AJAX trial results showing that
EVAR vs open repair was ARR 5.4%
(95% CI -11 to +23), we saw that
open repair performed much better
than expected with low death rates
in the randomised controlled trial,
but also low death rates in the
entire cohort.”
He said, “This could be attributable tothe introduction of the trial with opti-mised logistics and patient care such asthe pre-operative CTA and centralisa-tion.”
RUPTURED ABDOMINAL AORTIC ANEURYSMS
AJAX confirms no differencebetween EVAR and open repair
Ron Balm
Regula von Allmen
CX Symposium delegates heard the results of the world’s firstmulticentre, randomised, controlled trial that compared EVAR andopen repair for ruptured abdominal aortic aneurysms. The DutchAJAX trial results demonstrated no difference between EVAR andopen repair in emergent cases. In the same session, the audiencealso heard an outline of the SWIFT study on the effect of transporton ruptured aneurysm treatment outcomes. While AJAX resultsshed some light on treatment for ruptured aneurysms, manyquestions still remain unanswered


BIBA Publishing
September 201012 Updates June 2012
“In the discovery study, nineloci demonstrated associationwith abdominal aorticaneurysms (p<1×10−5). In thereplication sample, the lead SNPat one of these loci, rs1466535,located within intron 1 of low-density-lipoprotein receptor-related protein 1 (LRP1)demonstrated significant associ-ation (p=0.0042),” Bown said.
“We confirmed the associa-tion of rs1466535 and abdomi-nal aortic aneurysm in our fol-low-up study (p=0.035). In acombined analysis (6,228abdominal aortic aneurysmsand 49,182 controls),rs1466535 had a consistenteffect size and direction in allsample sets. No associations
were seen for either rs1466535or the 12q13.3 locus in inde-pendent association studies ofcoronary artery disease, bloodpressure, diabetes, or hyperlipi-daemia, suggesting that thislocus is specific to abdominalaortic aneurysms.
“Our findings suggest amechanism contributing toabdominal aortic aneurysm for-mation via the LRP1 pathway,and exploration of this mecha-nism could provide future thera-peutic approaches to preventingthe development and/or progres-sion of abdominal aorticaneurysms,” Bown et al report-ed.
“This study identifies a bio-logical process that could bealtered using drugs and there-
fore treat aneurysms, either toprevent them completely or toprevent them growing,” Bownsaid.
“The key challenges are toidentify how the protein pro-
duced by this gene causes orprotects against aneurysms andthen work out ways to reduceor increase the activity of theprotein or pathway that thisprotein is involved in. The next
step is to find out how the pro-tein produced by this gene isinvolved in the development ofaneurysms,” he noted.
He concluded that the genewas aortic aneurysm specificand that it was biologicallyplausible.
In the discussion after hisstudy was presented, MartinBjörck, Uppsala, Sweden, askedBown about the possible inter-action between the LRP1 geneand environmental factors.Bown said their data were limit-ed and not powered to detectsuch an interaction. JanetPowell, London, UK, comment-ed: “The reason why we whitepeople get aneurysms must part-ly be because of our environ-ment and partly because of ourgenes.”
The research, funded by TheWellcome Trust, was publishedin The American Journal of
Human Genetics in November2011.
Three vascular trainees were rewarded for theirwork during a presentation at the end of the CXEuropean Vascular Surgeons in Training Prize
Session, which was held as part of the CX 34 TraineesProgramme on Tuesday 17 April 2012.
Fifteen trainees presented on varying topics, from,among many others, diagnostic dilemmas of late carotidpatch infection, to total aortic endovascular repair withstaged procedures, and hybrid procedure in an aortic archpenetrating ulcer.
In first place was Kathryn Griffin, Leeds, UK, for thepaper, “Stenosis & swelling: an unusual case of Sutton-Kadir Syndrome”. Awarded second place for the paper“Treatment of a ruptured-MRSA-infected thoracoabdom-inal aortic aneurysm with a cryopreserved arterial homo-graft and autologous great saphenous vein beats theodds”, was Theodosis Bisdas, Hannover, Germany.Finally, in third place was Faris Alomran, Creteil,France, for the paper “Augmented reality: Dislocation ofa branch of an endovascular branched device with chal-lenging vascular access treated under ‘image fusion’”.
New talentrecognised at CXSurgeons inTraining PrizeSession
From left to right: Christos Liapis, Theodosis Bisdas,
Kathryn Griffin, Faris Alomran and Vikas Pandey
Matt Bown
Gene linked to abdominalaortic aneurysms is foundContinued from page 1
GLIMPSE INTO THE FUTURE


September 2010
BIBA Publishing
14 Updates June 2012
At a session focusing onthe exercise programmefor intermittent claudi-
cation at the CX Symposium inLondon, UK, Andrew Gardner,Oklahoma, USA, said that aprimary goal for peripheralarterial disease patients withintermittent claudication is toregain lost physical functionthrough exercise rehabilitation.He also stated that medicallysupervised exercise pro-grammes are efficacious toimprove claudication onsettime and peak walking time.
Gardner presented data of astudy using a step activity moni-tor that quantifies daily ambula-tory activity in claudicants. “Wefurther explored its utility toaddress the primary flaw ofhome-based exercise pro-grammes by directly measuringexercise adherence and exercisevolume performed,” he said.“We compared changes in exer-
cise performance and dailyambulatory activity in peripher-al arterial disease patients withintermittent claudication follow-ing a home-based exercise reha-bilitation programme, a super-vised exercise programme, anda usual care control group.”
The control group, Gardnerexplained, was encouraged towalk more on their own but theydid not receive specific recommendations regarding anexercise programme during thestudy.
Gardner told delegates thatpatients in home-based exercise
completed 83% of their exercisesessions, averaging 42 minutesper session at a cadence of 37strides per minute. Home-basedexercise, he added, was effica-cious for increasing claudicationonset time, peak walking time,and daily ambulatory cadences.Increases in daily ambulatorycadences were also greatest fol-lowing home-based exercise.
The results, Gardner said,showed that a home-based exer-cise programme, quantified witha step activity monitor, had highadherence and was efficacious inimproving claudication meas-
ures, similar to that seen with astandard supervised exercise pro-gramme. “Home-based exerciseappears more efficacious inincreasing daily ambulatoryactivity in the community settingthan supervised exercise,” hesaid.
Ian Chetter, Hull, UK, saidthat exercise programmes forclaudication are effective withthe correct programme and aptsupervision. To the question doesthe exercise programme environ-ment influence outcome? Chetterexplained that there was conflict-ing evidence and vastly different
levels of supervision in the com-munity exercise programmes.
Jonathan Beard, Sheffield,UK, in the invited commentary,noted that current knowledgesuggested that unsupervisedexercise (advice) does not work;supervised exercise (classes) areeffective, but expensive andunavailable for most patients andthat home-based exercise withsupport seemed more cost-effec-tive. Beard added that new termi-nology is needed with regard tolocation, class (whether group orindividual), level of support,method of support, type of moni-toring and type of trainer. Healso highlighted that questionsremain regarding the level andduration of support required andabout which regime gave the bestlong-term compliance.
Roger Greenhalgh, London,UK, commented that supervisedexercise is a blanket term thatneeded to be broken down.
Supervised exercise needs to be defined more clearlySupervised exercise programmes have been proved to increase the walking distance of patients with intermittent claudication but howmuch and what kind of supervision is required?
Ross Naylor, LeicesterRoyal Infirmary, Leicester,UK, president of theVSGBI:
When I started my first vascular trainingpost in 1984, vascular procedures werealmost exclusively performed by generalsurgeons with a vascular interest. Thenext 28 years witnessed a growingawareness that outcomes were betterwhen procedures were performed by vas-cular surgeons and most general surgeonswere happy to withdraw from the provi-sion of elective and emergency vascularservices. However, despite this importantchange in the way consultants practiced(especially in the endovascular era), ourtrainees still had to fulfil a curriculumthat was heavily general surgery orientedand where countless training opportuni-ties were lost because of an obligation toparticipate in general surgery on call
rotas that increasingly involved shift-work and compensatory rest periods. Itwas no surprise that review after reviewfound that the UK was offering inade-quate training in the modern vascular erato the majority of its trainees.
That changed in March, when an Actof Parliament saw Vascular Surgerybecome a specialty independent ofGeneral Surgery in the United Kingdom.This was a landmark event and was theculmination of many years of hard workby members of the Vascular Society ofGreat Britain and Ireland. The new spe-cialty will recruit 20 trainees per yearthrough national selection, starting in2013, who will then enter a training pro-gramme that better reflects the challengesand vascular competencies of the 21stCentury. It is an exciting time for vascu-lar surgery and it is even more excitingfor new trainees entering our specialty.
Peter Lamont, Bristol RoyalInfirmary, Bristol, UK, past-president of the VSGBI:
The Vascular Society first started seriousmoves towards separate specialty statusfor vascular surgery in 2003 and it hasbeen a persistent aim of the officers andcouncil of the society ever since then.First there was the need to persuade theUK surgical community that this step wasnecessary to improve training and out-comes in vascular surgery, culminating ina vote at the society’s Annual GeneralMeeting, which was unanimously infavour of the development. John Black,then president of the Royal College ofSurgeons of England, lent his support andthe first of a two-stage application wentforward from the college to the UKDepartments of Health in 2009. Each ofthe two stages progressed slowly though aconsultation process to ensure that thedevelopment did not impinge on otherspecialties and that the proposed newtraining curriculum met the standards ofthe General Medical Council. The societywas particularly grateful for unreservedsupport from the Royal College ofRadiologists and the British Society forInterventional Radiology in this process.Approval from the Departments of Healthwas finally achieved in late 2011 and thenew specialty was formed on 16th March2012 when it entered the ParliamentaryStatute books.
Vascular trainees of the future will nolonger need to spend time training in
areas of general surgery that they willnever use as consultants. Instead they candevote their training time to developingthe full range of vascular surgical andendovascular skills needed of a currentday vascular surgeon. With recognitionof the new specialty comes an affirma-tion that there is a definite career path invascular surgery and experience fromother countries suggests that this willimprove recruitment into the specialty forthe future.
A new online training curriculum hasbeen written within the auspices of theIntercollegiate Surgical CurriculumProgramme and has been approved bythe GMC. A new specialty training com-mittee has been formed and is workingwith the Deaneries and Schools ofSurgery to develop future vascular train-ing programmes. A new exit examinationis being developed, which we hopetrainees of the future will find better fitfor purpose than the current general sur-gical version. Above all, vascular surgerynow has an independent voice within theprofessional surgical structures in theUK, with its own seat on the RoyalCollege of Surgeons of England Council,on the Joint Surgical Training andExamination Committees and on theFederation of Surgical SpecialtyAssociations and Surgical Forum. All ofthese developments will ultimately allowvascular surgery to provide an enhancedlevel of care to patients throughout theUK, with improved outcomes for thosesuffer from vascular disease.
COMMENT & ANALYSIS
ROSS NAYLORPETER LAMONT
Finally, vascular surgery recognisedas independent specialty in the UK
On 16 March 2012, the UK Parliament gave statutory approvalrecognising vascular surgery as a specialty independent fromgeneral surgery. Ross Naylor and Peter Lamont, respectivelypresident and past-president of the Vascular Society of Great Britain& Ireland (VSGBI), wrote to Vascular News about what this means forthe new specialty
Andrew Gardner Ian Chetter Jonathan Beard


September 2010
BIBA Publishing
16 Updates June 2012
The voting was at the end of session that saw Joostvan Herwaarden, Utrecht, The Netherlands,reviewing type II endoleaks. There is currently no
clear acceptance of whether type II endoleaks representa risk for the patient after EVAR. Treatment policies canrange from conservative to active intervention.
Van Herwaarden said, “Type II endoleaks are notalways ‘benign’. The annual rupture risk for type IIendoleaks and growing aneurysm sac is significant(about 2%). Treatment of type II endoleaks is probablyindicated in most of those patients. However, long-termresults from transarterial and translumbar embolisationare poor.”
EVAR was introduced over 15 years ago to treat theold and sick patients with abdominal aortic aneurysm.“The results were promising and in many centres EVARevolved to become the treatment of first choice for allpatients with suitable anatomy. However, there are stillsome concerns about EVAR,” he said.
Van Herwaarden told delegates that the causes of sacenlargement were: type I endoleak; type II endoleak;type III endoleak; type IV endoleak and endotension.
“There is debate about treatment for endotension, butall types of endoleak (ie I, III, IV) are treated excepttype II endoleak,” he said.
Van Herwaarden then reviewed the latest literaturewhich examined whether type II endoleaks were a har-binger of risk after EVAR. He told Vascular News thathe believed the treatment of type II endoleaks mayimprove with better imaging using magnetic resonanceangiography and blood-pool contrast agents. He addedthat his group is now focusing on research on this topic.
Aortic correction <5.5cm or outsideinstructions for use
In the same session on late performance of EVAR,Timothy M Sullivan, Minneapolis, USA, spoke on theconsequences, in the USA, of aortic correction either<5.5cm or outside the instructions for use.
He said, “The premise is that elective repair shouldnot be performed until a fusiform abdominal aorticaneurysm reaches the 5.5cm diameter and that an endo-graft should not be used outside the instructions for use.It is believed that adverse consequences that may bepatient-related, physician-related, and affect the health-care system may result.”
Sullivan stated that there were an estimated 525,000patients in the USA with aneurysms between 4 and5.4cm.
“The FDA-approved endografts in the US are Gore’sExcluder, Endologix’s AFX, Medtronic’s Endurant andCook’s Zenith. The US clinical trials for these endo-grafts typically utilise a minimum aneurysmal diameterof 5cm, but aneurysm diameter as low as 4.5cm wasreported. The instructions for use do not include a sizethreshold,” he said. “As such, we are asking US-basedphysicians to alter their practices and increase the size
threshold to 5.5cm following participation in an FDA-aproved trial where smaller aneurysms were treated; thisseems counter intuitive.”
Sullivan said that there was an association between“off label” use and type I endoleak and increasedaneurysm-related mortality. “The newer grafts makeanalysis a ‘moving target’ and long-term follow-up isnecessary.”
He also provided a financial analysis which could beused to shed some light on the matter.
For abdominal aortic aneurysm repair, hospital reim-bursement is US$24,000 and physician reimbursementis US$4,000. Twelve thousand repairs (5–5.5cm) xUS$28,000 = US$336 million, said Sullivan. He thenpointed out that if the threshold was lowered to 4cm, theequation would read 525,000 x US$28,000 = US$14.7billion, a real challenge for the US healthcare system,which is already financially strapped.
Type II endoleaks “not so benign” after allIn a vote that reflected a perceptible change in opinion from a few years ago, 75% ofvoters at the CX Symposium said “no” to the question “Are Type II endoleaks as innocent aswe thought?”
First-time Dragon’s Den winnerPeter Schneider (Honolulu, USA)beat off stiff competition with his
recently CE-marked device the Tack-ITendovascular stapler (Intact Vascular),which is designed to optimise peripheralangioplasty results for the treatment ofperipheral artery disease.
The other contenders were RalfKolvenbach, Düsseldorf, Germany, withthe BYFix Anastomic device (HDHMedical), which is used to mechanicallyconnect any standard vascular graft to theblood vessel; Claude Mialhe, Draguignan,France, with the Twister device – a newconcept of endovascular embolisation andocclusion; and James Coleman (Dublin,London) with a novel percutaneoustransapical closure device for structuredheart disease and aortic arch procedures.
Schneider said that the acute technicalsuccess with the endostapler device “wasgood”, the ability to place the device“right where we wanted it” was 96% intheir first-in-man series, and procedure
time was similar to a standard lowerextremity case. He added: “We got theacute stent-like result without a stentwhile addressing some of disadvantagesof stents.”
The Tack-it Endovascular Staplerdevice is a 6F multi-loaded catheter con-taining four self-expanding tacks. The6mm-length implant has six pairs ofanchors designed to optimise angioplasty
by creating tissue apposition to smooththe arterial lumen.
In a press release issued by IntactVascular, Schneider, who is the compa-ny’s co-founder and chief medical offi-cer, stated, “Right now, we are very lim-ited by the tools we have available. Wecan either do angioplasty, which oftenproduces a suboptimal result, or we canplace a stent, which looks good initiallybut often does not last and has a lot ofdownstream problems. We believe theTack-It technology will offer a new solu-tion to address this problem. One of thekey design features is that the device cantreat a range of diameters offeringtremendous versatility. This will enablephysicians to go down the leg afterangioplasty and spot-treat several areasusing a single device.”
A clinical trial was conducted in SouthAmerica on 11 patients in whom 50Tacks were placed. The patients were fol-lowed for 12 months.
“This is a first-in-man experience witha novel approach to superficial femoralartery revascularisation,” said William AGray, who serves as an advisor to IntactVascular. “The one-year results are veryencouraging, and the company is plan-ning to initiate a post-CE mark clinicalstudy within the next couple of months.”
Tack-IT endovascular stapler winsNew Technology Dragons’ Den
Peter Schneider (centre) with the judges (left to right) Frans Moll, Chas Taylor, Alan
Edwards and Eric Bielen
Joost Van Herwaarden
Timothy M Sullivan


September 2010
BIBA Publishing
18 Abdominal aortic aneurysms June 2012
Roger Greenhalgh, London, UK, who chaired thesession, addressed Alan Scott, Plymouth, UK, asthey were both instrumental in providing the evi-
dence on the 5.5cm threshold and basis of screening andsaid, “We made certain decisions at the time aboutthresholds and about screening based on information wehad at the time. We are hearing a story emerging andmay have to be very flexible, and re-look at thresholdsand screening intervals and find that they may not befixed intervals. They might be sliding scale intervals,”he said.
Scott replied that at the time they had been careful toset up the rescreening intervals so that they were safe,erring perhaps on the side of caution.
What is an optimum rescanning interval? SimonThompson, Cambridge, UK, presented data from a proj-ect called RESCAN indicating that much longer rescreen-ing intervals were likely to be safe and acceptable topatients.
National screening programmes in the UK, Swedenand Australia are observing a recent reduction in theprevalence of abdominal aortic aneurysms in 65-year-olds. CX delegates heard about each of them.
UK screening programme
Jonothan Earnshaw, Gloucester, UK, who opened thesession, took to the podium to speak about the NHSnational abdominal aortic aneurysm screening pro-gramme. In a CX exclusive, he shared draft data show-ing that between 2009 and 2012 the programme (with40% coverage) had screened 157,730 men. The uptakewas 80.17% and 2,494 (1.57%) abdominal aorticaneurysms larger than 3cm were detected. Four hundredand four men were referred for surgery.
“Perhaps the most interesting point is we were expect-ing, based on data from the MASS trial, to find approxi-mately 4% of 65-year-olds with aneurysms. In fact, wehave only found 1.57%. That is still a significant numberof men – we have now referred over 400 men with a largeabdominal aortic aneurysm for vascular opinion. I cannotgive you outcome data, but of the first 130 screen-detect-ed, 129 patients had survived the intervention.”
Earnshaw told delegates that the main issue in screen-ing in 2012 was the fact that “We are not finding asmany aneurysms as we thought we would. Twenty-yeardata from the Gloucestershire programme showed thatthe mean aortic diameter has reduced from 21mm in1991 to 17mm in 2009. There is something happening tothe 65-year-old male aorta in Gloucester. This reductionin the number of aneurysms is mirrored elsewhere, inScandinavia and Australasia, and does seem to be real.Aneurysms do seem to be going away, which is ironic,when we are starting a screening programme.”
On the issue of cost-effectiveness, Earnshaw told del-egates that ongoing research suggested that that it waslikely that aneurysm screening at the current prevalencewould remain cost-effective.
Swedish and Australian experiences
Anders Wanhainen, Uppsala, Sweden, who then took thestage, shared similar observations about the reduction ofaneurysms being observed.
He told delegates that Sweden had adopted a com-monly suggested screening design with a single ultra-sound examination of men at the age of 65. “The nation-al abdominal aortic screening programme has a nearlynationwide coverage today,” he said.
Wanhainen said that the prevalence of abdominal aor-tic aneurysms in the target population was lower thanexpected indicating a change in the epidemiology of thedisease, mainly attributed to a noticeable reduction insmoking frequency.
“We therefore need to continue to monitor and assessthe screening programmes already established andsimultaneously evaluate alternative screening strate-gies,” he said.
Describing the situation in Australia, Paul Norman,Fremantle, Australia, said that experts were adopting await and watch approach rather than implementing anational screening programme because the magnitude ofbenefit from screening is small. “Mortality from abdom-inal aortic aneurysm is falling without screening. Iwould question whether there is enough of a publichealth problem to warrant screening.”
Is the rupture rate falling?
Janet Powell, London, UK, told delegates that the rateand volume of aneurysm rupture is declining. She madethe point that smoking prevalence had decreased, anduse of lipid-lowering and antihypertensive drugs hadincreased in those who were 65+ years.
“The small aneurysm rupture rate is decreasing anddeaths from (and hospital admissions for) large rupturedaneurysms are decreasing. Since selection for repair andits mortality are unchanged, have cardiovascular riskprevention programmes pre-empted national aneurysmscreening programmes?” she asked.
Martin Björck, Uppsala, Sweden, told delegates thatan aneurysm screening programme should include asmoking cessation programme, promotion of exerciseand healthy diet and statin treatment prior to surgery.There should also be hypertension treatment, accordingto standard of care, he said.
“As we all know, screening elderly men for abdomi-nal aortic aneurysm, and repairing those who have orlater develop large aneurysms, reduce aneurysm mortali-ty by between 50 and 70%.
“Can we prevent growth of small aneurysms? Can weprevent cardiovascular events? Can we prolong life withsecondary prevention? Unfortunately, we lack specific
data on patients with screening detected aneurysms,” hesaid.
“Data on the possible effects of statins on aneurysmgrowth rates are contradictory, and there is no evidenceto support that growth is decreased. What is shown,however, in randomised trials, is that short-term statintreatment reduces perioperative cardiac events and mor-tality, by approximately 50%. Long-term statin treat-ment prevents events among patients with cardiovascu-lar disease, but there are no specific data on abdominalaortic aneurysm patients.”
Simon Thompson, speaking on behalf of the RES-CAN collaboration, told delegates that surveillanceintervals for small abdominal aortic aneurysms differedbetween surveillance programmes. “Some are based onscreening trials, but there is no good evidencebase/direct comparative data.”
The RESCAN Collaboration analysed smallaneurysms measuring 3–5.4cm, which came from indi-vidual patient data over time collated from surveillanceprogrammes/other longitudinal studies. Data were col-lated from 18 studies in the UK, Europe, North America,and Australia, involving 15,471 patients followed for upto eight years.
There were 228 ruptures, aneurysms were measuredmainly by ultrasound (external diameters) and there wasa 5.5cm threshold for surgery.
Results of the analysis showed that the averagegrowth rate is 2.2mm/year and the average rupture rateis 0.2% per year. “For each 0.5cm increase in aneurysmdiameter, the growth rate goes up by 0.5mm/year andthe rupture rate doubles. There is large heterogeneity inthese rates between studies, which is unexplained.Women have the same growth rates but four times therupture rates of men, at each abdominal aortic aneurysmdiameter.”
Thompson told delegates that the clinically acceptablesurveillance intervals for men are several years for 3–4cm aneurysms and six months for 5cm aneurysms.
“Intervals/threshold for surgery in women shouldreflect those for men with 0.5–1cm larger aneurysms,and the cost-effectiveness of different surveillance poli-cies needs to be formally assessed,” he said.
Is it time to reconsider abdominal aorticaneurysm screening programmes?
Roger Greenhalgh Alan Scott Jonothan Earnshaw Anders Wanhainen
Paul Norman Janet Powell Martin Björck Simon Thompson
CX delegates heard a variety of reasons why it might be time to question the very foundations on which national aneurysm screeningprogrammes are based. With a population that lives longer, smokes less and has lower cholesterol levels than in the past, it seems thatpeople are developing abdominal aortic aneurysms later in life. Do we need to raise the age threshold for screening? With all trial evidenceso far having studied abdominal aortic aneurysm in men between the ages of 65 and 74, is a policy selecting 65 as the age for screening stillvalid? Have cardiovascular risk prevention programmes pre-empted national aneurysm screening programmes?


September 2010
BIBA Publishing
20 Interview June 2012
Ross Naylor, Professor of Vascular Surgery, Department of Cardiovascular Sciences, University of Leicester, and consultant vascularsurgeon, Leicester Royal Infirmary, Leicester, UK, developed his interest in carotid endarterectomy back in 1979. Since then, he haspublished over 300 papers and book chapters on cerebral vascular disease. In this interview with Vascular News, Naylor spoke about hiscareer, controversies in carotid intervention, new technologies and objectives for his term as president of the Vascular Society of GreatBritain & Ireland 2011–2012. He also described his hobby of road cycling...
Profile Ross Naylor
How did you come to choosemedicine as a career and whyvascular surgery?I am embarrassed to admit that (aged 14) I decided on amedical career whilst sitting in my school CareersOffice. I had been told to attend with clear ideas aboutmy future, but had done absolutely nothing. I saw abrochure entitled “Why don’t you be a Doctor” and thatwas that! I was a third year student when I decided onsurgery (loved the buzz and activity) and fourth yearwhen vascular chose me. I had just watched someoneopen an abdomen and clamp a ruptured aortic aneurysmin what seemed like seconds and thought “that’s forme”! I have never regretted it.
Which innovations in vascularsurgery have shaped your career?
Improvements in medical therapy, the rise of evidence-based practice and the endovascular revolution. As atrainee in the 1980s, no one ever envisaged thataneurysm repair could almost become a day-case proce-dure.
Who were your mentors and whatadvice of their do you still remember?
Jetmund Engeset (Aberdeen) saw potential in the stu-dent who frequented his ward late at night and nurturedmy fledgling research interests. Second was VaughanRuckley (Edinburgh) who showed me you could be abusy NHS surgeon, still produce influential research andbecome a highly respected professor. Peter Bell(Leicester) influenced my career (both clinical andresearch) more than anyone else and was singularlyinfluential in persuading me to return to Leicester in1995 after I had moved back to join Jetmund inAberdeen as his consultant colleague in 1993.
Carotid endarterectomy is your mainarea of interest. How did you developthis interest? Do you still rememberthe first carotid procedure youperformed?
In 1979, I asked Jetmund to recommend a topic for myfinal-year student elective and he suggested a controver-sial operation called carotid endarterectomy, which wasapparently popular in the USA but rarely performed inthe UK. It was the beginning of a career-long interestand despite having published 300+ papers/book chapterson cerebral vascular disease, I still find the subject bothfascinating and enduringly controversial. I cannotremember my first operation, but I do recall my fourthor fifth. We had just introduced the quality control pro-gramme in Leicester, where we inspected the inside ofthe endarterectomy zone with an angioscope beforerestoring flow. Peter Bell was supervising me when the‘scope revealed a large luminal thrombus. Having previ-ously been sceptical about the merits of the project, hewas a rapid convert and (21 years later) we still useangioscopy for completion assessment.
You advocate early intervention insymptomatic carotid stenosispatients after the first onset ofsymptoms. Have you seen any
changes in clinical practice in recentyears or are somephysicians/decision makers stillresistant to this idea?Yes and yes! It is indisputable that the risk of stroke ishighest in the first few days after onset of symptoms andthat the longer you delay endarterectomy, the less thebenefit conferred to the patient. After many years of pro-moting the need to intervene early, this is now a keycomponent of the ESVS Guidelines and I am pleasedthat countries around the world are actively changingthe way they prioritise transient ischaemic attack/strokepatients. Sweden now has a median delay (symptom tosurgery) of 12 days. In the UK it is 15. Yes, there arestill those who close their ears to the evidence, but thatwill change. I suspect most surgeons/interventionists (ifasked) would want to be treated as soon as possible afteronset of symptoms. Shouldn’t we offer the same serviceto our patients?
At the recent CX Symposium, 61% ofthe delegates backed you and agreedthat “Randomised controlled trials forasymptomatic carotid diseasewithout a medical arm will beobsolete when published”.One of your argumentswas that the trialsshowed that over 90% ofthe interventions inasymptomatic patientsare “ultimatelyunnecessary”. What isyour key message onthis subject?
The world has moved on sinceACAS/ACST recruited patients,but despite compelling evidencethat the annual risk of stroke onmedical therapy is declining (alsoobserved in ACAS and ACST),ACAS data from 1995 are stillbeing used to model risk-benefitanalyses in contemporary guidelines.No one is seriously suggesting that allinterventions should cease, but we doneed to identify a smaller cohort of “highrisk for stroke” patients in whom to targetsurgery or stenting. Accordingly, randomised tri-als comparing carotid endarterectomy with stentingthat have not included a medical limb face the unfortu-nate prospect of being criticised following publication.It is no use hoping that lower procedural risks will great-ly increase the benefits of intervention so as to over-come the lack of a medical arm. Even if you could oper-ate (or stent) with a 0% risk, 93% of interventionswould still be unnecessary.
CREST continues to generate a lot ofdebate, with various interpretationswith regard to endpoints. At CX, theaudience voted against (93%)swinging the practice towardscarotid artery stenting. Do you forsee
a swing towards stenting in thefuture?If this had been a cardiology/radiology audi-ence, the result would have been different!It is inevitable that stenting will assumean increasing role, if only because theindications for stenting in “averagerisk” patients were liberalised inthe 2011 American HeartAssociation Guidelines. Oneconsequence of CREST hasbeen the debate about theinclusion of periopera-tive myocardial infarc-tion in the primaryendpoint. The popularinterpretation ofCREST was that peri-operative myocardialinfarction was asso-ciated with poorerlong-term survival,but at the 2011VEITHsymposium,
Tom Brott (CRESTprincipal investiga-
tor) stated that “itwas a myth to say
that myocardialinfarction in
CREST had abigger
impact on late mortality than did perioperative stroke”.Without the inclusion of perioperative myocardial infarc-tion, surgery would have been statistically superior tostenting in symptomatic patients. My personal opinion isthat the myocardial infarction issue has distracted atten-tion from the much more clinically important goal ofrapid treatment. Only 13/2,500 patients (0.5%) in CRESTdied prematurely following procedural myocardial infarc-tion (seven following endarterectomy, six following stent-ing). This must be compared with evidence that up to10% of patients will suffer a stroke within seven days oftheir index transient ischaemic attack. For now, surgery is

June 2012
BIBA Publishing
21Interview
Educationn Chapelpark Primary, Forfar, Scotland, UKn Merchiston, Edinburgh, Scotland, UK
Qualifications
1976–1981 Medical school, AberdeenUniversity, Aberdeen, UK
1981 MB, ChB with commendation,Aberdeen University
1986 Fellow of the Royal College ofSurgeons of Edinburgh
1990 MD, Aberdeen University1994 Certificate of Higher Surgical
Training1996 Fellow of the Royal College of
Surgeons of England (ad eundem)
Career
1981–1982 House officer, Aberdeen TeachingHospitals
1982–1983 Lecturer in Pathology, AberdeenUniversity
1983–1985 SHO in Surgery, Aberdeen TeachingHospitals
1985–1988 Surgical registrar, EdinburghTeaching Hospitals
1988–1990 Research fellow, EdinburghUniversity
1990–1991 Surgical registrar, Kirkcaldy1991–1993 Lecturer in Surgery, Leicester
University1993–1995 Consultant vascular surgeon,
Aberdeen Royal Infirmary1995–current Consultant vascular surgeon,
Leicester Royal Infirmary2002 Reader in Surgery2002 Hunterian Professor of Surgery
(RCSEng)2003 Professor of Vascular Surgery
Other appointments
2000–2005 Editorial Board; The British Journalof Surgery
2003–2008 Editorial Board; The Journal ofVascular Surgery
2006–current Council member, Vascular Societyof Great Britain & Ireland
2006–current Editorial Board, European Journalof Vascular & Endovascular Surgery
2007–2010 Associate editor, European Journalof Vascular & Endovascular Surgery
2010–current Council member, European Societyof Vascular Surgery
2011–2014 Senior editor, European Journal ofVascular & Endovascular Surgery
2011–2012 President, Vascular Society of GreatBritain & Ireland
2011–2012 Council member, Association ofSurgeons of Great Britain & Ireland
2012 Voted winner of “Pioneer inPerformance Award for Europe”
Fact File
probably the safer intervention in the hyperacute periodfor the majority of centres, but stenting will assumegreater importance as delays increase. Of course, someinterventionists may be able to offer comparably safeinterventions in the hyperacute period and stenting is thenentirely appropriate. However, it remains to be seen justhow generalisable that might be for practice as a whole.
It is still controversial whethercarotid stenosis patients undergoing
coronary artery bypass graftsurgery should undergo
carotid intervention.What is your opinion on
this matter?
How long have you got?Having been an advocateof synchronouscarotid/coronaryprocedures, I began toharbour doubts about its
role in
neurologicallyasymptomatic
patients, who make up>90% of those being
considered for intervention.There is now a growing body of
evidence that the vast majority ofperi-operative strokes after coronary
bypass (perhaps 95%) cannot beattributed to a previously asymptomatic
carotid stenosis. Most probably followatherothrombotic embolism from the aortic arch. My
own practice is to offer synchronous carotid/coronaryrevascularisation to the very small cohort of recentlysymptomatic patients who (because of their cardiacstatus) cannot undergo isolated carotid surgery. Iwould also offer a synchronous procedure to patientswith bilateral severe asymptomatic disease (<2% ofthose undergoing cardiac surgery). We do not offersynchronous procedures to anyone with a unilateralsevere asymptomatic carotid stenosis.
Can you describe a memorable case?
Six years ago, I was asked to see a lady in ourNephrology Unit. Ten days earlier, she had presented to
another hospital with anuria. Investigations showed shehad occluded her aorta from the iliac bifurcation upinto the mid-thoracic region (normally a fatal event).Every time she dialysed, she developed mesentericischaemia. If dialysis was withheld for any length oftime, she suffered flash pulmonary oedema. Our anaes-thetists advised that she would not survive a major tho-raco-abdominal reconstruction and when she suffered amore severe episode of mesenteric ischaemia, I and mycolleague Rob Sayers performed a left axillo-superiormesenteric artery bypass which resolved her symp-toms. We subsequently performed a right axillo-bifemoral bypass and she has since undergone success-ful renal transplantation. You just never know what isgoing to come through your door!
What are your other current topics ofresearch in cerebral vasculardisease?
Three projects. The first examines public awareness ofthe need to present early after onset of stroke/transientischaemic attack symptoms. We have shown that while90% are aware of the FAST symptoms (Facialweakness, Arm weakness, Speech problems), only50% know that leg weakness and visual loss areimportant warning symptoms. The second looks at theinteraction between biomarkers, gene profiling studies,plaque histology and computerised plaque analysis inpatients undergoing hyperacute carotid surgery. Thethird is my latest attempt to study the pathophysiologyof post-endarterectomy hypertension. Anyone who hastried to do this in the past will know just how difficultthis is.
What do you hope to achieve as2011–2012 president of the VascularSociety of Great Britain & Ireland?
I was honoured to be elected president for 2011–2012.This is an exciting time for UK vascular surgeons as wesecured independent specialty status through an Act ofParliament on 16 March 2012. Our absolute priority is toensure that the 20 trainees selected to enter the newnational programme each year from 2013 receive target-ed high-quality training, free from the rigours of cover-ing general surgery. This will, of course, involve a closerworking relationship with our interventional radiologycolleagues and I look forward to that. In Leicester, ourinterventional radiology colleagues have (for some yearsnow) provided our trainees (and visiting fellows) withhigh-quality interventional/endovascular training whichhas been much appreciated.
Which new techniques andtechnologies will you be watchingclosely in the future?
Innovative new methods for delivering medical therapy,totally endovascular solutions for the aortic arch, theemergence of nanotechnology, bioabsorbableimplantable devices and a desperate hope that someonewill finally tell me which acute thoracic aortic syn-dromes actually “need to be treated” rather than “can betreated”.
What are your interests outside ofmedicine?
Skiing and road cycling. After turning 50, I realised Ihad to stop finding excuses and get fit again. My wifehad already taken up road cycling and I joined her. Itwas very hard to keep up with her to begin with, but Ihave now tackled Mount Ventoux (securing Jean-PierreBecquemin’s respect), Alpe d’Huez and the Cold’Izoard. My target this year is the Stelvio Pass in Italywith its 48 hairpins.

Endovascular treatment for athero-sclerotic obstructions infemoropopliteal arteries is widely
used for patients with intermittent claudi-cation and critical limb ischaemia,although the optimal treatment of super-ficial femoral artery disease in thesepatients is a matter of continuing debate.
The femoropopliteal arterial segmentis known to be exposed to specialmechanical influences. The superficialcourse of the artery with crossing of flex-ion points as well as interaction with thesurrounding musculature, potentiallyexposes the artery to relevant externalforces, including compression, torsion,and elongation. This may have a negativeimpact on vessel patency after bothangioplasty and stenting. In fact, stentcompression has been identified as oneof the principal causes of restenosis, par-ticularly after implantation of balloon-expandable stents.
The use of percutaneous transluminalangioplasty to revascularise the superfi-cial femoral artery can result in initialtechnical success rates of more than 95%,with a low risk of complications.However, at one year, the rates ofrestenosis exceed 70% for lesions longerthan 100mm.
Endovascular stenting avoids the prob-lems of early elastic recoil, residualstenosis, and flow-limiting dissectionafter balloon angioplasty and can thus be
used for the treatment of long and com-plex lesions, even in heavily calcifiedarteries.
The problem of external stent com-pression was thought to be overcomewith the introduction of self-expandingstents and particularly with the clinicaluse of the new generation of nitinolstents.
A recent study (J Endovasc Ther.2010;17:767–776) compared seven dif-ferent superficial femoral artery nitinolstents during mechanical bending, com-pression, and torsion testing showing dif-ferences in the incidence of high strainzones, which indicates a potential forstent fracture.
The Zilver PTX drug-eluting stent is aself-expanding nitinol stent with a poly-mer-free paclitaxel coating; in the litera-ture there is only a single-arm clinicalstudy with a follow up of one year inwhich the results are promising but notdefinitive. The fracture percentage maybe considered in accordance with othernitinol stents.
A second generation stent designed toimprove the long-term superficialfemoral artery outcomes is the EasyFlype stent (CID). Two features of thisnitinol stent (Fig 1) make it unique. Themirror-like finishing of the stent surface,with rounded edge, and the integral coat-ing with iCarbofilm improve the metalsurface compatibility with blood and
arterial wall. The iCarbofilm is a highdensity carbon coating with turbostraticstructure characterised by high adhesionto the substrate, chemical inertness, ionimpermeability and very low thickness.
The compatibility of this carbon coat-ing has been extensively evaluated, andit has been demonstrated (Appl Bio-
mater 2009; 90B:338-349) that in con-tact with blood it strongly inhibits theactivation of the coagulative cascade,release of pro-thrombotic and pro-in-flammatory factors promoting a com-plete surface endothelialisation alreadyat seven days as observed in animalmodel (Fig 2).
In superficial femoral artery implants,the nitinol stents have negative outcomesrelated to the tissue response under thecyclic stimulation to the vessel wall. Inthis circumstances Easy Flype, thanks to
its mechanical performance and biocom-patible surfaces, minimises thromboticrisk and neointimal growth as observedin-vivo preclinical investigations (% areastenosis and neointimal thickness at 180days respectively 25.1±15.1% and0.27±0.25mm). Clinical evidence so farcollected includes the Casper study witha total of 60 patients with 70 lesions havebeen treated (98.6% de novo, 1.4%restenotic), most of them eccentric andcalcified with a mean length of25.6±12.3mm. In 70 % of lesions thestent was implanted using the directstenting technique. Post-dilatation wasnecessary in 94.3% of the Flype/HiFlypeCarbostent stent implants in order toobtain a satisfactory final angiographicresult. All lesions were successfully treat-ed, in all cases obtaining a residual vesselstenosis minor than 20%. In terms of pro-cedural performance, no complications oracute thrombosis phenomena wereobserved during the delivery phase.
The follow-up clinical assessmentsdid not reveal any sub-acute or delayedclinical events and patients’ statusimproved in 89.3% and 94.2% of thecases respectively at 30 days and at 180days. An important aspect of the of theEasy Flype/HiFlype Carbostent, is relat-ed with its cell’s elements’ structure:stresses induced by the main stent load-ing conditions occur in different areasthus avoiding elastic distortion andstress concentration on the vessel wallwhich, otherwise, can stimulate abnor-mal tissue response. In vitro, no yet pub-lished experiences, demonstrated fatigueresistance tests.
However, randomised controlled trialsare warranted to confirm these resultsbecause the effects of confounding fac-tors cannot be ruled out with certainty ina retrospective study.
Gianpaolo Carrafiello and Anna Maria
Ierardi are with the Interventional
Radiology Department, Unisubria,
Varese, Italy. They declared no conflict of
interest
September 2010
BIBA Publishing
22 Updates June 2012
GIANPAOLO
CARRAFIELLO
Can a new generation peripheralstent minimise thrombotic risk?
Fig 2
Fig 1
The prospectiveEndurant US inves-tigational device
exemption (IDE) study’scomplete results at twoyears continue to demon-strate durable clinical per-formance with strongsafety and efficacy inlong-term follow-up withthe Medtronic device.
“The Endurant StentGraft is performing just as
well at two years as it didat one year, with noaneurysm-related mortali-ties, migrations or conver-sions,” said the study’sprincipal investigator,Michel Makaroun, profes-sor and chief of vascularsurgery at the Universityof Pittsburgh School ofMedicine, USA. “Freedomfrom aneurysm-relatedmortality and secondary
interventions demonstratefavourable trends versusearlier generation devices.This finding will continueto play a critical role inimproving the minimally-invasive treatment ofpatients with abdominalaortic aneurysms.”
The Endurant US IDEstudy enrolled 150abdominal aorticaneurysm patients at 26US medical centres.Significant to clinicalpractice, the study includ-ed patients with “landingzones,” or healthy aorticneck lengths, as short as10mm, whereas most
other trials of aortic stentgrafts have required necklengths of at least 15mm.The study also monitoredchanges in aneurysm sizeand stent graft migration,a concern with currentendovascular treatment, aswell as the occurrence andtype of endoleaks.
The study found thatnearly all (97.6%) of theaneurysm sacs that weretreated with the Endurantstent graft decreased orremained stable in size attwo years post-procedure,with only 0.8% type Iendoleaks and no type IIIendoleaks.
Endurant stent graft shows durableperformance at two years in US study Two-year results from the US clinical studyof the Endurant abdominal aortic aneurysmstent graft system were presented at the 34thCharing Cross International Symposium inLondon, UK
Michel Makaroun
COMMENT & ANALYSIS
ANNA MARIA
IERARDI


While flow-diversion was acknowledged as afascinating concept, the ensuing discussionrevealed that there were still questions regard-
ing hard endpoints showing the device’s benefit, bail-outstrategies after implantation, and whether this technologywas ready to be implanted in patients yet… To the ques-tion “Is the multilayer stent a breakthrough?”, 56% ofvoters said “no” while 44% said “yes”.
Michel Henry, Nancy, France, told CX delegates thatthe Multilayer Flow Modulating (MFM) stent represent-ed an alternative to current devices to treat thoracoab-dominal and abdominal aortic aneurysms.
He explained that the key principles of the multilayerstent are: vortex velocity reduction, flow lamination inthe collaterals, flow acceleration, shear stress reductionat the aneurysm neck. The physiological exclusion leadsto the branches remaining patent, he said.
Henry reported that eight thoracoabdominal aorticaneurysms, five abdominal aortic aneurysms and threedissections were treated. He said that technical successwas 100% and that on an average between one and fourdevices were used. He said that 30-day outcomes showedthat there were no deaths, branch patency was 100% andthat there were no neurological complications. “These aregood outcomes if we compare them with currentendovascular procedures,” said Henry. “During the fol-low-up, we observed a progressive sac thrombosis andshrinkage depending on the importance of collaterals.”Henry added, “Despite the severity and complexity of thecases we treated, the preliminary clinical results are satis-factory and promising. We did not observe any neurologi-cal complications (these are usually to the level of 10–15% of the cases, with current techniques). Themultilayer stent leads to progressive sac thrombosis andshrinkage depending on the importance of collaterals.”
Henry told delegates “To have good results, it isimportant to have a perfect technique of implantationand to avoid endoleaks (type I or III.).” He made thepoint that the multilayer stent was not to be used fortreating ruptured aneurysms or mycotic aneurysms. “Donot oversize the stent by more than 20%,” he said.
He also noted that treating any branch stenosis beforecovering with the device was mandatory. He highlightedthe importance of one month of aspirin and clopidogreltherapy, as well as the importance of an early post-oper-ative CT scan to ensure proper device placement.“While greater experience and larger follow-up areneeded, multilayer flow modulation appears as a break-through to treat any aneurysm,” Henry said.
Charles McCollum, Manchester, UK, explained thatto answer the question of how safe it was to cover sidebranches, his team had looked at data from Italy andFrance where >300 vital side branches had been covered(brachiocephalic, carotid, subclavian visceral or renalarteries). There had been one early superior mesentericartery occlusion and one coeliac axis thrombosis show-ing the safety of the stent, he said. “In Manchester, wecovered 47 vital side branches and they are all patentwith no major complications,” he added.
The first 12 multilayer stents were implanted by iniliac or popliteal aneurysm, with follow-up ranging from4–16 months. One required revision but 11 fully throm-bosed to stent (median one week). All internal iliacarteries remained patent and there was no aneurysmgrowth. Three aneurysm sacs shrank >4mm,” he said.
“We also did eight compassionate cases and
these have not had a good outcome”, noted
McCollum. Among these cases, there was one
mycotic thoracoabdominal aneurysm (died of sep-
sis at five months) and one 10.8cms suprarenal
abdominal aortic aneurysm (rupture at two
months). “This stent cannot perform miracles.”
He also said “We have developed a protocol to do 40perirenal or thoracoabdominal aneurysms where theaneurysm involves or is very close to the important ves-sels either proximally or distally. These patients are notfit for open repair and standard EVAR is not possible,but they still have a life expectancy >12 months.”
McCollum said the investigators had been measuringthe patent sac diameter and had seen that the peripheralaneurysms thrombose very quickly to the aneurysm, butthat the larger abdominal and thoracoabdominalaneurysms were taking longer. “At this stage before wedo a proper clinical trial, we have to see that there is norupture and that the aneurysm begins to shrink, beforeyou could possibly say this technique is successful.However, our results so far are encouraging.”
Thomas Larzon, Örebro, Sweden, who presented theÖrebro experience, told CX delegates that the multilayerstent approach is not applicable for all types ofaneurysms. “Ruptured aneurysms are contraindicated,but the technology might be applicable in a sub-group.There are no hard endpoints that support that it really
works, but its use can be justified in compassionatecases,” said Larzon.
Investigators in Örebro began a study in November2010 and treated 13 patients with aortic aneurysm. Allof these were compassionate cases. Seven of these 13were non-symptomatic and four were symptomatic.There were also two cases of rupture. Eleven of the 13were thoracoabdominal aneurysms. Six patients had hadprevious aortic surgery.
Follow-up CTA was every third month and investiga-tors recorded overall/aneurysm-related death, aneurysmsize, branch vessel patency, thrombus formation, re-intervention and major adverse events.
“Three patients died due to non-aneurysm relatedcauses (two from cardiac infarction and one fromunknown causes). However, two other patients clearlydied from the aneurysms, one from a ruptured aneurysmand the other had a very rapidly expanding aneurysm(which was probably a mycotic aneurysm) and she diedtwo days after the intervention,” Larzon said.
In terms of size, the investigators observed that therewas no decrease in aneurysm size, and that this was over15-month follow-up period. In fact, two patients had asignificant increase in size,” noted Larzon. “No throm-bus was observed in three cases; there was partialthrombus in four cases and total thrombus formation inone case,” he added.
Larzon told delegates that in terms of vessel patency,28/29 of the major branch vessels were patent. A lumbarocclusion was also identified. The team also observed aspinal infarction with paraplegia (at 15 months).
September 2010
BIBA Publishing
24 New technology June 2012
44% of the CX audiencesee the MARS as apotential breakthroughOf the Multilayer Aneurysm Repair System (MARS), CX delegates heard early clinicalresults. In the discussion, it became apparent that the aim of the MARS approach is forthrombosis to form in the multilayers for strength, as well as branches to stay open aroundthe device. The indicator of success is the reduction of sac diameter and the consensus wasnot to use the device in ruptured aneurysms. The discussion at CX showed that expertsbelieved that the device was not suitable for elective repair, or ruptured aneurysms butsuitable for not very fit, high-risk patients. However, the ideal candidate to receive the MARSwas not clearly defined
Michel Henry
Thomas Larzon
Charles McCollum
CX chairman’s analysisRoger Greenhalgh wrote: “MARS is certainly receiv-ing very wide coverage. This is because many hopethat flow diversion can play a role in what is a com-pletely new concept and approach. As is expectedwith a new concept, there is doubt and this is proper.
Ted Diethrich, from the floor spoke vehemently infavour of MARS based upon his personal knowledgeof the introduction of this new technology. MichelHenry from the podium was very positive. ThomasLarzon spoke of deaths in patients in whom he hadused MARS. He introduced a doubt about this tech-nology. Charles Mc Collum spoke neither wholly foror against.
The vote taken on the multilayer stent was fairlybalanced and the reception by the audience was that itcould be an important new approach but some uncer-tainty prevailed. It became clear that it was unwise totreat a ruptured aneurysm with MARS. Uncertaintyemerged about which patient would be a candidate. Itseemed that MARS should be targeted towards high-risk but not emergency or fit elective patients at thisstage. More experience and data are awaited.”



June 2012
BIBA Publishing
27EVAR devices
“Generations of stentgraft systems havebeen developed for
the endovascular treatment ofabdominal aortic aneurysms.Most are designed to exclude theaneurysm from aortic blood pres-sure by achieving graft-vesselwall apposition at healthy arteryattachment sites proximal anddistal to the aneurysm. TheNellix Endovascular AneurysmSealing System has been devel-oped using an alternativeapproach. Nellix creates artificialflow lumens across the aneurys-mal segment of the aorta usingballoon-expanded stent graftsand fills the aneurysm space witha biostable polymer. The poly-mer solution is injected throughfill tubes and is contained inhighly conformable endobags.The polymer safely cross links insitu, and then the construct sealsand fixates across the entireaneurysm sac, rather than at onlya few discrete points as is typicalin state-of-the-art stent grafttechnology. This complete seal,from the renal arteries to thehypogastric arteries, is designedto provide a barrier, eliminatingbranch vessel perfusion of thesac. Further, this completeanatomical fixation is designedto mitigate lateral and transla-tional forces that contribute todevice migration and endoleaks,”Holden told delegates.
He demonstrated the currentsystem, which will soon be com-mercially available. “The systemnow includes an integrated oper-ator console that allows a singleoperator to easily use the device.Procedural simplicity (position-ing and deployment of “kissing”stents then the filling of
endobags) means potentiallytime consuming steps such ascontralateral limb cannulationare avoided. The procedure cannormally be completed wellwithin an hour,” he said.
Holden stated that 47 patientswith abdominal aortic aneurysmswere enrolled from 2008 to 2011.CT follow-up and clinical evalu-ation occurred at 30 days, sixmonths and annually up to fiveyears. The CT images were CoreLaboratory reviewed and anindependent Clinical EventsCommittee reviewed adverseevents. The mean age of thepatients was 72±7 years (89.4%were male). The mean aneurysmsac diameter was 5.6±0.8cm. Themean sac blood lumen diameterwas 4±0.5cm. The mean neckvessel diameter was 24±11mmand the mean neck length was22±7.1mm. Nearly 11% ofpatients had short necks(<10mm) and 34% had largeCIAA (>23mm).
Holden noted that there was100% procedural technical suc-cess. “The mean device implanttime was 57±27 minutes; themean fluoroscopy time was23±18 minutes, mean total proce-dure time was 109±34 minutes.The time to hospital dischargewas 3.6±2.4 days,” he said.
“The type IA endoleakresolved spontaneously within 60days. The type IB endoleak wasdue to improper device sizing(too short). A limb extension wasadded at 15 months and resolvedthe endoleak. The single type 2endoleak resolved spontaneouslywithin 60 days,” Holden said.
He concluded that the safetyand effectiveness of the NellixEndovascular Aneurysm Sealing
system observed to date has beenvery encouraging. “Specificallythe following observations arenoteworthy: absence of rupture,conversion, occlusion, or migra-tion; endoleak rate far lower thanany other device and allendoleaks have resolved; Lowrate of device-related secondaryprocedures, 0 at one year, one(4.3%) at 15 months; an abilityto treat a range of adverse proxi-mal neck anatomies; hypogastricpreservation with a single devicesimplifies procedural complexi-ty; simplified surveillance (eg,ultrasound) may be justifiedleading to reduced costs post-EVAR ,” he said.
Treovance
Chiesa told CX delegates that theADVANCE trial is a prospective,multicentre, non-randomisedstudy, primarily intended toassess the safety and perform-ance of the Treovance stent-graftin patients with infrarenalabdominal aortic aneurysms.
“This new abdominal aorticstent-graft, currently applying forthe CE mark, is a trimodular
Dacron-nitinol device with aproximal bare stent and a doublefixation system, ensured bysuprarenal and infrarenal barbs.The main body is premounted ina 18–19F outside diameter intro-ducing system, and leg exten-sions in 13F–14F sheaths,” heexplained.
In the study, from March toDecember 2011, 30 patients havebeen enrolled in five Europeancentres, including in SanRaffaele Scientific Institute inMilan, Italy, OspedaleSant’Agostino Estense inModena, Italy, Hospital Clinic deBarcelona, Spain, DeutschesHerzzentrum Berlin, Germanyand Hospital UniversitariGermans Trias i Pujol,Barcelona, Spain.
“The Treovance graft was suc-cessfully implanted in allpatients, and no 30-day deaths oraneurysm-related complicationswere recorded. Type II endoleakrate was 10%. No type I or IIIendoleaks were observed. Thedevice seemed to adapt well totortuous anatomies, with nocases of kinking, wire rupture ormigration. Investigating centresare currently collecting six-month follow-up data that will befully available from the end ofJune 2012,” Chiesa noted
“The early experience withthis new abdominal stent-graftwas largely satisfactory. Ofcourse, we still need follow-updata to draw conclusions ondevice safety and effectiveness,”Chiesa said.
Ovation
Manish Mehta, Albany, USA,presented 12-month results of
the Ovation Global PivotalTrial with the Ovation stentgraft (TriVascular). “TheOvation Abdominal Stent GraftSystem optimises the two mostimportant requirements forEVAR: access and seal. Theclinical trial has demonstratedexcellent one year resultsacross a clinically challengingcohort of patients,” Mehta said.
In the trial, the rate of majoradverse events was 2.5% at 30days and 3.8% at 12 months.There were no device-relatedmajor adverse events. Freedomfrom type I and III endoleakswas 100% at 12 months. Therewere no cases of migration orrupture.
Mehta added that, “with CEmark and FDA approval,Ovation’s 14F outer diametersystem is the lowest profilecommercially available deviceand expands the patient popula-tion suitable for EVAR.” Hesaid that “with over 800 patientstreated worldwide, Ovation rep-resents the next generationEVAR technology, today.”
INNOVATION trial
According to Giovanni Pratesi,Rome, Italy, the Incraft stentsystem (Cordis) is “easy to use,accurate in placement, andcomfortable.”
After six months (of datafrom 60 patients), Pratesi said,freedom from type I endoleakswas 98.2% and freedom fromtype III endoleaks was 100%.He added that rates of stentgraft patency, freedom frommigrations, freedom from frac-tures, freedom from sacenlargement, and freedom frommajor adverse events (eg,death) were all 100%.
Pratesi concluded: “Initialexperience and preliminary mid-term results with the new cus-tomisable, ultra-low profilestent graft system is encourag-ing.”
He added that more data onthe Incraft device was coming.The Inception trial, he reported,would enrol 150 patients at upto 25 sites in Europe, Australia,and New Zealand. He said aboutthe Inspiration trial, “90 subjectswill be enrolled at up to 50 sitesin North American and Japan.”
First data for the next generation ofEVAR stent grafts unveiled at CXThe first global data (presented by Andrew Holden, Auckland, New Zealand) on the Nellix device (Endologix), an investigationalendovascular aneurysm sealing system for the treatment of infrarenal abdominal aortic aneurysms, and the first-ever clinical trial results(presented by Roberto Chiesa, Milan, Italy), in the European Union, of Treovance (Bolton Medical), an abdominal stent graft with Naviteldelivery system that has been specifically designed for EVAR in patients with abdominal aortic aneurysms, were two examples of the firstdata on the next generation of abdominal aortic aneurysm devices that were presented at the CX Symposium
Table 1. Nellix resultsEvaluation 30 days Six months One year Two years
(n=47) (n=46) (n=32) (n=23)
Rate of secondary procedures (endoleaks) 0 0 0 4.3% (1)
Aneurysm rupture 0 0 0 0
Device migration 0 0 0 0
Sac expansion 0 0 0 0
Endoleak type IA 2.1% (1) 0 0 0
Endoleak type IB 2.1% (1) 2.2% (1) 3.1% (1) 0
Endoleak type II 2.1% (1) 0 0 0
Endoleak type III/IV 0 0 0 0
Stent occlusion 0 0 0 0
Fracture or fatigue 0 0 0 0
Roberto Chiesa


BIBA Publishing
Opening the debate, PaoloZamboni, Ferrara, Italy, statedthat CCSVI is an entity because
of the peculiar pathology. “According torecent data from Cleveland, CCSVI pres-ents with gross anatomy with an increasein significant intraluminal obstacles in theinternal jugular veins. This has been seenin cadavers of multiple sclerosis patients.Compared with a control, the histologyshowed abnormal type III collagenexpression in the vein wall,” he said.Zamboni also said he believed CCSVIwas a subset of multiple sclerosis because,despite a considerable variability of ultra-sound screening, “more abnormalities inthe extracranial veins are objectively doc-umented in multiple sclerosis patients thanwith other techniques.” He added,“Reduced venous outflow determineshypoperfusion, an important part of themultiple sclerosis pathogenesis; hypoper-fusion cannot be explained by autoimmu-nity and cannot be treated by current
immunomodulatory drugs. On the con-trary, brain perfusion can be improved inmultiple sclerosis by restorative vascularand endovascular procedures.”
Manish Mehta, Albany, USA, referredto the paper by Diaconu et al, wholooked at anatomical and histologicaldata from cadavers that had valvularaberrations and showed significantlyhigher prevalence in an multiple sclerosispopulation (seven abnormalities in fiveof seven patients) than a non-multiplesclerosis population (one abnormality insix patients). Then, Mehta showed datareporting improvement in symptomsamong multiple sclerosis patients afterangioplasty. “If you look at outcomemeasures that are objective and subjec-tive, following intervention, MS patientsreport significant improvement in termsof timed 25-foot walk in all multiplesclerosis types, as well as quality of life.If we look at a physical health compositescore, in multiple sclerosis communities
pre- and post- angioplasty there was sig-nificant difference, with 84% of patientsreporting improvement at a mean follow-up of 4.5 months. The same was seen interms of mental health (92%) and fatigue(82%) in a cohort of 125 patients weanalysed,” he said. “So yes, there aremany unanswered questions, and there isa lot more work to be done, but thereclearly is a connection between CCSVIand multiple sclerosis. What we need todo now is collaborate, move on and col-lectively find solutions.”
Complications
Speaking against the motion, Alun Davies,London, UK, pointed out that there is noevidence showing that CCSVI exists.Davies questioned the reliability of duplexscans and noted that complications havebeen documented after interventions tocorrect internal jugular stenosis.
“The reality is that there are complica-tions. We have published a review of pub-
lished complication (Phlebology 2011: 1-3) because the answer is that after theseinterventions thrombosis is observed.Studies get stopped; there is lack of fol-low-up and a reported death. Recommen-dations from CIRSE say that there is nosound basis to offer a new treatment, andif you are going to do it, please, do it aspart of a randomised controlled trial, notas an experiment,” he said.
In Imperial College, Davies continued,investigators have set up a blinded, age-sex matched cross-sectional ultrasoundstudy to look at differences in cerebralvenous outflow disturbance in multiplesclerosis patients and healthy controls.“Does the CCSVI phenomenon exist?Certainly, to date, we would suggest itdoes not,” he said.
Richard Nicholas, London, UK, arguedthat “we are unable to diagnose CCSVIcoherently, we can find it in healthy peo-ple and people with other neurological
At CX, majority of delegates say CCSVI is notan entity and a subset of multiple sclerosisIs chronic cerebrospinal venous insufficiency (CCSVI) an entity and a subset of multiple sclerosis? Sixty three per cent of the delegateswho voted in a session dedicated to CCSVI at the CX Symposium answered “no” to the question, backing the debaters Alun Davies andRichard Nicholas, who argued that there is no evidence that CCSVI exists or is a subset of multiple sclerosis. Speaking for the motion,Paolo Zamboni and Manish Mehta noted that some patients have improvement in symptoms after angioplasty/stenting in the internaljugular or azygos veins. Delegates also heard about the prevalence of jugular vein stenosis, endpoints to assess the effect of internaljugular vein correction and identified important questions to be answered by a randomised trial
CX chairman’s analysis
Roger Greenhalgh, CX Programme chairman, sum-
marised the CCSVI session at CX:
“The session proceeded in a fairly logical way. Itemerged that definition is as a subset of multiple scle-rosis in the opinion of most of the speakers but eventhis was not a unanimous view. Michael Dake includedthe existence of CCSVI outside of multiple sclerosis.There was a suggestion that the definition was madeonce a response to therapy was witnessed. If so, itwould be unlike other illnesses or entities which needto be recognised first so that a treatment (an interven-tion in this case) can be justified.
Another approach to an attempted diagnosis seemed
to depend on a multiple sclerosis patient being shown ohave a venous hold up in the internal jugular vein. Doesit have to be bilateral or can it be unilateral? The pre-cise duplex findings that define the condition did notseem absolutely clear. But symptomatic presumed ben-efit from correction of internal jugular vein hold upcorrection is claimed whilst others say it is a placeboeffect (the so-called nihilists frequently neurologists).
Sumaira Macdonald had looked carefully in the nor-mal population in the community to see if it can befound there. Her comments were equivocal but she saidshe “leaned towards CCSVI being an entity”.
It did not emerge what question should be asked forany randomised controlled trial although it was appre-
ciated that a randomised controlled trial would addimpetus if it could be performed. Definition of the keyquestion is move one and that did not appear and sothere was some uncertainty. What was quite certain wasthat every single clinician wishes to allow every chancefor a defined entity to appear and be recognised byeveryone especially if patients with multiple sclerosishad any hope of clinical benefit from internal jugularvein obstruction correction. Symptoms of headache,fatigue, depression and improvement in cognitive testsare reported.
At the end of a full discussion, the vote was takenand on the positive side, 37% see CCSVI as an entityand a subset of multiple sclerosis.
Alun Davies and Richard NicholasManish Mehta and Paolo Zamboni
June 2012
Continued on page 30

September 2010
BIBA Publishing
30 June 2012
diseases, CCSVI is uncommon in advanced multiple scle-rosis, and when you have central venous stenosis it doesnot predispose to multiple sclerosis. CCSVI needs furtherwork before we are to take it seriously as an entity inmultiple sclerosis”.
During the discussions, Davies noted that people whoare benefiting at the moment may be getting this benefitas a placebo-effect of having an intervention. Zamboniresponded pointing out that data that have been generatedby his group with blinded MRI showed a reduction of thelesion after the procedure, compared to non-treatedpatients. “There was also a trend in decreasing the brainoedema, so this means that an anti-inflammatory effect ofvenoplasty that cannot be denied.” Zamboni continued,“How long can a placebo effect last? In the next issue ofFunctional Neurology we are publishing a paper compar-ing our group of patients four years after the treatment,compared to two years before the treatment. We found asignificant decrease of the disabilities score and the num-ber of attacks. I do not think that in a serious disease likemultiple sclerosis a placebo effect can last four years.”
From the audience, Ian Franklin, London, UK, saidthat investigators from Glasgow reported a high level ofPCO2 concentration in the jugular venous blood in peo-ple affected with internal jugular vein stenosis. “Is thehigh PCO2 concentration in jugular venous blood partof the story or there is something completely different?”he asked. Zamboni answered: “We found that this is justhaemodynamics affecting the venous wall. Quite recent-ly in Geneva investigators published that interluminalstenosis cannot be found in normal people and also thatthere is no infiltration of these cells at all. This is veryinteresting, so it is not a secondary autoimmune phe-nomenon to multiple scleoris. And finally there is anabnormal content of type III collagen in these venouswalls. Something different from normal jugular veinsexists at the level of pathology.”
Then, Marian Simka, Katowice, Poland, spoke on thetopic “CCSVI is a recognisable syndrome, defined asthose within multiple sclerosis who have internal jugularvenous stenosis.” He told delegates that three mainquestions regarding hypothetical venous insufficiency inthe cerebral and spinal territory should primarily beanswered. “Does chronic cerebrospinal venous insuffi-ciency exist? If it does, is it exclusively associated withmultiple sclerosis? And if it is associated, does such aconnection have an impact on neurological pathology?”
Internal jugular vein stenosisprevalence
Sumaira Macdonald, Newcastle, UK, reviewed howoften internal jugular vein stenosis occurs in the com-munity through the literature. Macdonald, who clarifiedthat she does not treat patients with CCSVI, said that theprevalence is very variable in normal controls. “Thereare important positive controls that we have to think
about like patients on dialysis and patients with otherneurological disorders like transient global amnesia,”she said. She added that “There are a lot of limitations inthe assessment of the prevalence of internal jugular veinstenosis. We do not have any stringent postmortem dataor MR or duplex prevalence data on jugular or greatvein stenosis outside the CCSVI studies or good epi-demiological data on jugular vein issues in other rele-vant disease groups. We do need a good consensus onduplex. Zamboni et al are working on that in a multidis-ciplinary document, but there are still some unknowns.We have variability in the sensitivity and specificity ofvarious modalities used to image the great veins.
We have to accept that there are similar abnor-
malities as the Zamboni criteria for CCSVI in con-
trol populations. However, if you look, particular-
ly at the larger analyses, and patients with
clinically defined multiple sclerosis rather than
early multiple sclerosis (or clinically isolated syn-
drome) there are significant differences in these
findings between controls and multiple sclerosis
patients.”
Questioned by Greenhalgh as to whether she believedCCSVI was an entity, she said she leaned towards itbeing an entity but remained uncertain of the question ofcausation.
Endpoints of internal jugular veinstenosis correction
Michael Dake, Stanford, USA, spoke about what end-points should be chosen to assess the effect of internaljugular vein stenosis correction. He noted that to estab-lish the credibility and acceptance of CCSVI treatment,safety had to be established in mid- and long-term stud-ies, not just in short-term, and that efficacy had to beestablished in blinded, placebo-controlled phase I and IIstudies, before designing phase III studies. “We are justat the beginning of this whole story,” he said.
“If you are going to establish treatment benefit, thereare a number of efficacy outcomes you might want tolook at, depending on what you are claiming. In terms ofdisease modifications, you want to look at MRI, clinical
disability, relapses. You might want to look at quality oflife, but that is subjective. I think we should be lookingat symptom improvement, and a number of these can bequantified, some cannot,” he noted.
At Stanford, Dake said, “we use multiple sclerosisfunctional composite (MSFC), which looks at uppermotor, lower motor and cognitive measures. But we arealso supplementing that with a battery of exercise per-formance studies that include measured walking time,cognitive performance while exercising and temperatureregulation.” Dake told delegates he believed that CCSVIdoes exist and it is not unique to multiple sclerosis,because subjects with other neurologic and maybe non-neurologic diseases and healthy subjects also presentedwith the condition.
“What does CCSVI represent? It is characterised byclinical symptoms headache, sleep disturbances, sensa-tion of brain fog, fatigue etc that appear to improve, atleast transitorily, after angioplasty. What is the most sen-sitive, accurate diagnostic test for the detection ofCCSVI/venous anomalies? We have to admit, we do notknow yet. And the significance of CCSVI in relation toMS disease parameters and its clinical implications stillremains undetermined. We do not know, but we think itmay be a factor, along with other factors.”
Dake added that endovascular treatment of CCSVIshould only be performed under the auspices of a validclinical trial. “So where are we going? I am afraid to saythis is just the tip of the iceberg. We have got morequestions, and superabundance of questions than wehave answers. But the only way we are going to getthere is to have a spirit of collaboration,” he said.
Mark Meissner, Seattle, USA, was given the task toidentify “What is the important CCSVI question for anyrandomised controlled trial?”. He highlighted that multi-ple sclerosis trials are very complicated. “At least inNorth America, social pressures may prohibit a classicscientific approach. Trials are complicated by the fluctu-ating, long-term course of the disability and disagreementbetween neurologists about relevant outcomes,” he said.
“For patients, important outcomes are quality of lifeand long-term disability, which are obviously not goodmarkers for a randomised clinical trial. We need surro-gate endpoints, and disability scores are the best validat-ed surrogates for long-term outcome. Outcomes that areimportant, that cannot establish therapy, include techni-cal outcomes, relapse frequency and MRI. But we needto beware of the placebo effect.”
So what is the important question for CCSVI trials?Meissner answered: “In comparison to sham interven-tion, does active intervention for CCSVI in relapsing-remitting multiple sclerosis improve quality of life andprevent long-term disability (independently assessed bya neurologist) as reflected by validated surrogates?”
At the end of the session, most of the delegates werenot convinced that CCSVI is an entity and a subset ofmultiple sclerosis, and only 37% voted for the motion.
On 10 May 2012, the FDA released an alert
about injuries and death associated with
the use of balloon angioplasty devices or
stents to treat chronic cerebrospinal venous
insufficiency (CCSVI). The FDA stated that stud-
ies exploring a link between multiple sclerosis
and CCSVI are inconclusive, and the criteria
used to diagnose CCSVI have not been ade-
quately established.
“Because there is no reliable evidence from
controlled clinical trials that this procedure is effec-
tive in treating multiple sclerosis, FDA encourages
rigorously-conducted, properly-targeted research
to evaluate the relationship between CCSVI and
multiple sclerosis,” said William Maisel, chief sci-
entist and deputy director for science in the FDA’s
Center for Devices and Radiological Health.
“Patients are encouraged to discuss the potential
risks and benefits of this procedure with a neurolo-
gist or other physician who is familiar with multiple
sclerosis and CCSVI, including the CCSVI proce-
dures and their outcomes.”
The experimental procedure uses balloon
angioplasty devices or stents to widen narrowed
veins in the chest and neck. However, the FDA
has learned of death, stroke, detachment and
migration of the stents, damage to the treated
vein, blood clots, cranial nerve damage and
abdominal bleeding associated with the experi-
mental procedure. Balloon angioplasty devices
and stents have not been approved by the FDA for
use in treating CCSVI.
The FDA is notifying physicians and clinical
investigators who are planning or conducting clini-
cal trials using medical devices to treat CCSVI
that they must comply with FDA regulations for
investigational devices. Any procedures conduct-
ed are considered significant risk clinical studies
and require FDA approval, called an investigation-
al device exemption.
In February 2012, the FDA sent a warning letter
to a sponsor/investigator who was conducting a
clinical study of CCSVI treatment without the nec-
essary approval. The sponsor/investigator volun-
tarily closed the study.
The FDA has also announced that complica-
tions following CCSVI treatment can be reported
through MedWatch, the FDA Safety Information
and Adverse Event Reporting program.
The FDA said that it will continue to monitor
reports of adverse events associated with “libera-
tion therapy” or the “liberation procedure” and
keep the public informed as new safety informa-
tion becomes available.
FDA issues alert on potential dangers of intervention for CCSVI
Sumaira MacdonaldMichael Dake
Continued from page 29

BIBA Publishing
“Current techniques for endovenous ablationhave changed, but at the time we were onlyablating the above-the-knee great saphe-
nous vein regardless of whether there was above- andbelow-knee reflux or not. The follow-up was done withultrasound, Aberdeen Varicose Vein Severity Score(AVVSS) and CEAP grade,” Gough said.
He told delegates that the ultrasound findings showed“very satisfactory” results in the reduction of full above-knee great saphenous vein reflux and groin neovascular-isation.
“The commonest abnormality was persistent below-the-knee reflux. Nowadays that is easily dealt withbecause we would always ablate an incompetent below-knee great saphenous vein at the initial treatment. Sothat is not a problem. However, we did find that quite afew patients presented with segmental great saphenousvein reflux or with reflux at the sapheno-femoral junc-tion. These patients are more problematic” he noted.
In terms of varicose vein reflux, the ultrasound resultsshowed that 53% of limbs (42/79) had recurrent incom-petence. When looking at patients, the recurrent varicose
vein rate was lower, with 33% (21/63) reporting theirpresence. Seventy three per cent of the patients (45/62)considered the treatment successful and 80.6% (50/62)would have endovenous laser treatment again.
“In terms of the ultrasound recurrence, why hadpatients developed recurrent varicose veins? Most ofthem were because of progressive disease such as perfo-
rators, below-knee reflux, anterior or posterior thigh veinor pelvic varicosities. Nevertheless, a proportion were dueto a failure of the original treatment,” Gough said.
He added that, despite that, quality of life improve-ments persisted at six years. “So when we take into con-sideration patients’ views on their recurrence and onrepeat treatment, we have quite satisfactory results,” hestated. “Most recurrences were due to progressive dis-ease, and two-thirds of these were suitable to furtherendovenous therapy. Neovascularisation, as we alwayssuspected, was much less (14%) than with an equivalentgroup after surgery (54%) at five years.
The improvement in CEAP grade and quality of lifewas maintained.
“Persistent below-the-knee reflux was the commonestfinding and we now treat it from the outset as we knowthat it reduces the risk of residual varicose veins afterthe initial treatment. As far as the group with segmentalreflux and sapheno-femoral junction reflux is con-cerned, it is tempting to suggest that a 1470nm radialfibre may reduce the risk of this happening but of coursewe have to await further data.”
Satisfactory results with endovenouslaser ablation 6.5 years after treatmentMichael Gough, Leeds General Infirmary, Leeds, UK, presented long-term follow-up after endovenous laser ablation for great saphenous varicose veins at the CX Symposium in London, UK. The study reviewed a group of 63 patients (79 limbs), 6.5 years after above-knee laser treatment
Michael Gough
Swimming legend and Olympicgold medalist SummerSanders joined with the
Society for Vascular Surgery (SVS),American College of Phlebology(ACP) and American Venous Forum(AVF) to launch Rethink VaricoseVeins on 18 April 2012.
This educational campaignencourages those suffering fromvaricose veins to learn more abouttheir condition and speak to a veinspecialist about treatment options.
Only 1.9 million of the more than30 million Americans suffering fromvenous disease seek treatment annu-ally; the vast majority of sufferersremain undiagnosed and untreated.
As part of the campaign, Sandersis sharing her experience withvenous insufficiency. She alsodescribes how she improved follow-ing treatment.
“My legs were achy and heavy,especially after a long day. I thoughtthese symptoms were just a naturalpart of living an active lifestyle,being on my feet a lot and gettingolder,” said Sanders.
“I finally spoke with my vein spe-cialist, who told me that these symp-toms were due to venous insufficien-cy. He explained that if I did notseek treatment and my conditionprogressed to chronic venous insuf-ficiency, I could end up with moreserious symptoms like skin colorand texture changes, severe pain andeven leg ulcers.”
Patients are encouraged to visitwww.RethinkVaricoseVeins.com tolearn more about varicose veins,chronic venous insufficiency andtreatment options. Visitors to thewebsite also can assess their risk withan online tool, find vein specialiststrained in diagnosis and treatment,read more about Sanders’ experiencewith vein disease and treatment andshare an e-card with friends or familymembers to encourage them to learnmore about the condition.This educational campaign is spon-
sored by Covidien.
Rivaroxaban showscomparableefficacy to standardof care for inpulmonaryembolism patients
Results of the EINSTEIN-PE studyhave shown that the oral anticoagu-lant rivaroxaban (Xarelto, Janssen)
was comparable to today’s standard of carein treating patients with acute symptomaticpulmonary embolism and in preventingdevelopment of venous thromboembolism.The study also found rivaroxaban had a sim-ilar safety profile and significantly lower riskof major bleeding versus the current standardregimen. These data were presented as a latebreaking clinical trial at the AmericanCollege of Cardiology Annual ScientificSessions, and published in the New England
Journal of Medicine.The EINSTEIN-PE study compared
rivaroxaban to enoxaparin followed by vita-min K antagonist in the treatment of 4,833patients with acute symptomatic pulmonaryembolism for the prevention of recurrentvenous thromboembolism. Patients receivedtreatment for three, six or 12 months. In thestudy, rivaroxaban succeeded in demonstrat-ing non-inferiority to standard therapy forthe primary endpoint of recurrent sympto-matic venous thromboembolism, a compos-ite of symptomatic deep vein thrombosis andnon-fatal or fatal pulmonary embolism(2.1% vs. 1.8%, respectively [p=0.003 fornon-inferiority]). Rivaroxaban also demon-strated similar results compared to standardof care for the principal safety outcome
measuring a composite of major and non-major clinically relevant bleeding events(10.3% vs. 11.4%, p=0.23, respectively).Rivaroxaban treatment also resulted in a sig-nificant reduction in major bleeding events(1.1% vs. 2.2%, p=0.003, respectively) com-pared to standard therapy.
The treatment of venous thromboembolismcurrently requires a two drug regimen: a rap-idly acting, injectable anticoagulant followedby long-term treatment with an oral vitamin Kantagonist such as warfarin. Jack E Ansell,professor of Medicine at New YorkUniversity School of Medicine and chairmanof the Department of Medicine at Lenox HillHospital in New York, said “These resultsdemonstrate that a single-drug approach likeoral rivaroxaban could be an important addi-tion to our ability to simplify treatment byeliminating the need to transition to a differ-ent anticoagulant while preventing the occur-rence of secondary blood clots in patientswho have pulmonary emboli.”
“The average patient with venous throm-boembolism carries the risk of recurrence for ayear after the initial event and, for somepatients, the risk can persist beyond that,” saidPaul Burton, vice president, CardiovascularFranchise Medical Leader at Janssen. “Basedon the results seen in the EINSTEIN-PE study,rivaroxaban could provide an alternative,effective oral treatment that offers less risk ofmajor bleeding for patients who have beendiagnosed with a pulmonary embolism. Giventhat pulmonary embolism requires both acutemanagement in a hospital setting and long-term treatment at home, an oral, single-drugtreatment that does not require routine bloodmonitoring may be especially welcome.”
The company plans to file the EINSTEINstudies in a supplemental New DrugApplication with the FDA during the secondquarter of this year.
Olympic gold medalistkicks off RethinkVaricose Veins campaign
Summer Sanders
June 2012 31

September 2010
BIBA Publishing
32 Market watch June 2012
Product News
Zenith Fenestrated endograft
Initially introduced atthe RSNA 2011, theDiscovery system was
designed to address thetrade-off departmentshave historically neededto make between ceiling-and floor-mounted sys-tems, eliminating the needto compromise on patientaccess and image quality.It is neither floor- nor ceil-ing-mounted, but enablesfull patient access withoutthe need to suspend thesystem above the patient.It has the mobility of a C-arm with the power andimage quality of a fixedsystem. This laser-guided,motorised mobile gantrycreates an interventionalenvironment withoutboundaries. It allows com-plete access to the patientand unlimited parking
capability, or a flexibleand secure operating roomenvironment. The uniquegantry comes with a newwide bore design, whichallows for steep angles,ease in 3D acquisition,especially for largepatients.
GE also debuted its In-nova IGS 540 with operat-ing room option, to expandthe use of its Innova imag-ing system in the hybridOR setting. Thanks to aspecifically designed tableand accessories, the InnovaIGS 540 OR enables bothendovascular and open sur-gical procedures in the oneroom.
“In interventional radiol-ogy we are seeing a trans-formation, with both mini-mally-invasive andcomplex procedures being
performed in additionalsettings, including theOR,” said Chantal LeChat, general manager ofInterventional Radiologyfor GE Healthcare. “Thischange requires the devel-opment of technology thatis versatile and adapts tothe needs of the clinician –regardless of environment.We feel that with the avail-ability of the DiscoveryIGS 730 OR and now theInnova IGS 540 OR, weare opening up doors forour clinicians to haveaccess to cutting-edgeimaging in more settings.”
GE Healthcare alsohighlighted its OEC 9900Elite MD at CX 34. Withthe power, precision andperformance availablefrom the OEC 9900 EliteMD, this mobile C-arm is
an option for hybrid oper-ating rooms in whichcomplex interventionalprocedures are performed.
“When bringing open
and endovascular pro-
cedures into one room,
the GE Hybrid OR
makes it possible to
treat more cases with
great confidence,” said
Joe Shrawder, CEO, GE
Healthcare Surgery.
“From mobile to fixed
imaging systems, GE
Healthcare offers a
robust portfolio of prod-
ucts for healthcare
providers to choose
from.”
The OEC 9900 EliteMD has a unique X-raytube and cooling systemthat allows for full-resolu-tion imaging for longerperiods of time. With 22%more target cooling and upto 100% more housingcooling than previous OECC-arms, the 9900 Elite MDenhances procedural capa-
bilities. With the table-sideremote user interface ofthe OEC 9900 Elite MD,physicians have controlover their C-arm and theirprocedures. This motorisedC-arm allows 9 degreesper second orbital, lateral,and combo movementscontrolled from the remoteuser interface with an on-screen angle indicator.
“I think motorisation isreally the key to successwhen performing complexendovascular aorticrepairs (EVAR),” statedStephan Haulon. “I reallyhave complete control ofthe system. This hasdecreased the overall pro-cedure time and radiationof the procedure.” Haulonis the Vascular SurgeryDepartment chair atUniversity Hospital inLille, France, where the9900 Elite MD is used inthe hybrid OR. He says henow performs a regularEVAR in 45 minutes to anhour, where it used to take
almost an hour and a half.“The hybrid approach
of excellent angiographicimaging with road map-ping in a sterile environ-ment is the dream of allwho perform EVAR,TEVAR and FEVAR,”said Roger Greenhalgh,CX Symposiu m chair-man. “The hybrid systemssolve all that is expectedby demanding endovascu-lar surgeons and interven-tional radiologists.”
He added that “thelaunch of the alternativetype of hybrid by the GEDiscovery system contrastsmarkedly with existingsystems fixed in hybridsuits and takes a totallydifferent approach. It isbased upon the design ofthe French inventor,Bernard Bouvier. We aredelighted that it islaunched in Europe atCX34,” Greenhalgh stated.
Discovery IGS 730 andInnova IGS 540 with ORoption are not CE marked.
GE Healthcare unveils newimaging system for itsfamily of hybrid operatingroom solutions at CXGE Healthcare unveiled a new system for its family of hybridoperating room (OR) solutions at the Charing Cross Symposium inLondon, UK. Designed as a flexible environment with enhancedcapabilities, the GE hybrid operating room enables physicians toperform more complex procedures, which can improve patient care.Specifically, GE highlighted its recently FDA-cleared Discovery IGS730 system, with the operating room option, the first interventionalX-ray system designed to capture the advantages of both floor-andceiling-mounted systems
Discovery IGS 730
Cook Medical’sZenithFenestratedendograftapproved by theFDAThe FDA has approvedthe Zenith FenestratedAbdominal AorticAneurysm EndovascularGraft (with the adjunctiveZenith Alignment Stent)from Cook Medical foruse in the USA.According to the FDA,the device is indicated forthe endovasculartreatment of patients withabdominal aortic oraortoiliac aneurysmshaving morphologysuitable for endovascularrepair, including:n Adequate iliac/femoral
access compatible withrequired introduction
systemsn Nonaneurysmal
infrarenal aorticsegment (neck)proximal to theaneurysms with length≥4mm and unsuitablefor a non-fenestratedgraft; diameter ≤31mmand ≥19mm; angle <45degrees relative to longaxis of aneurysm;angle <45 degreesrelative to axis ofsuprarenal aorta
n Ipsilateral iliac arteryfixation site >30 mm inlength and between 9–21mm in diameter
n Contralateral iliacartery distal fixationsite >30mm in lengthand between 7–21mmin diameterThe Zenith Alignment
Stent is indicated for use
as an adjunct to theZenith Fenestratedendograft to securepositive alignment offenestrations or scallopswith the orifice of aorticbranch vessels havingdiameters ranging from 3to 8mm.
Cook has agreed toprovide a clinical updateto physician users at leastannually and conduct along-term follow-upstudy. This prospective,observational, single-armstudy will consist ofcontinued follow-up ofthe premarket cohort, aswell as newly enrolledsubjects, and patientswill be followedannually. The primaryendpoint of the study isaneurysm-relatedmortality at five years.
Covidienperipheralvascular stentsystem receivesFDA approvalCovidien has announcedthat the FDA hasapproved the EverFlexSelf-ExpandingPeripheral Stent Systemfor use in the superficialfemoral artery and/or theproximal popliteal artery.The EverFlex System,which has been approvedfor peripheral indicationin international marketssince 2006, is now avail-able in the United States,including a 200mm stentlength.
The clinical data sup-porting the FDA approvalof the EverFlex Systemfor use in the peripheralvasculature were obtained

through the DURABILI-TY II InvestigationalDevice Exemption trialthat enrolled patients atclinical sites within theUS and Europe. DURA-BILITY II is the firstclinical study to evaluatelesions up to 18cm and tospecifically test the per-formance of a singlelong, up to 200mm stent,in the superficial femoralartery and proximalpopliteal artery.Specifically, the studyresults show no majoradverse events at 30 daysand a low one-year stentfracture rate of 0.4%.Additionally, primarypatency at one year was67.7% when analysed bysimple proportions ofpatients patent; usingKaplan-Meier time-to-event analysis, it was77.2%.
“DURABILITY II is alandmark trial intended tostudy the patency andfracture resistance ofplacing a single nitinolstent in the superficialfemoral artery. It provid-ed the clinical evidencenecessary to demonstratethat you can successfullytreat long, complexlesions in the superficialfemoral artery with theEverFlex Self-ExpandingPeripheral Stent,” saidKrishna Rocha-Singh,director, Prairie VascularInstitute, Springfield,USA, and co-nationalprincipal investigator ofDURABILITY II.
Symplicity RenalDenervationSystem receivesHealth Canadalicence Medtronic has announcedthat it has received aHealth Canada licence forits Symplicity RenalDenervation System toreduce treatment-resistanthigh blood pressure inpatients unresponsive tothree or more anti-hyper-tensive medications.
“Decreasing a patient’ssystolic blood pressurefrom 160 to 130mmHgover a period of sixmonths, which renal den-ervation has been shownto do, could preventmany heart attacks andstrokes from ever hap-pening,” said BarryRubin, medical director,Peter Munk CardiacCentre, Toronto, Canada.“Our multidisciplinaryrenal denervation pro-
gramme, which includesinterventional radiolo-gists, vascular surgeons,cardiologists, hyperten-sion and kidney special-ists will treat many eligi-ble patients in the monthsahead.”
Results from the SYM-PLICITY HTN-1 trialhave shown sustainedsafety and effectivenessof renal denervation withthe system out to threeyears, and results fromthe SYMPLICITY HTN-2 trial showed safe, andstatistically significantreduction of blood pres-sure (-33mgHg systolicblood pressure) at sixmonths following theprocedure and sustainedto 12 months. These datawere recently presentedat the annual AmericanCollege of Cardiologyduring an oral session,which was dedicated torenal denervation.
In addition to thelicence from HealthCanada, the SymplicityRenal DenervationSystem has received CEmark and a listing withAustralia’s TherapeuticGoods Administration(TGA). The SymplicityRenal DenervationSystem is under investi-gational use in the UnitedStates.
Stille introducesthe new imagiQ2imaging table atCX
Stille introduced theimagiQ2 imaging table atCX 34 in London, UK.According to the compa-ny, imagiQ2 representsthe next generation of vas-cular imaging tables. Thecore technology of newimagiQ2 is based on anew proprietary, ultratransparent carbon fibretechnology that enablesreduced dosingand improvedimage qualityin endovas-cular proce-dures.
Stille nowintroducesimagiQ2, the secondgeneration vascularimaging table developedfor procedures such asendovascular repair ofabdominal aorticaneurysm.
“The new table is basedon patented and propri-etary technologies whichrepresents major innova-tion leaps in the imagingtable industry,” stated apress release issued by thecompany.
Among the many newfeatures, imagiQ2includes a new patentpending, ultra transparentcarbon fibre top that offersthe industry’s lowestattenuation which enablesreduced dosing for clini-
cians and patients,improved EVAR imagequality and ultimatelymore efficient procedures,according to the pressrelease.
”We are now settingnew industry standards toimprove patient safety andcreate more efficientendovascular procedures.The new imagiQ2 isdesigned based on clearcustomer needs with pric-ing, safety and featuresoptimised for both in- andoutpatient settings.imagiQ2 is the optimal C-arm complement in theHybrid OR,” said PhilipSiberg, president andCEO of Stille.
imagiQ2 is the succes-sor of imagiQ, Stille’stable that was introducedin the early 2000s andnow established as the oneof the leading endovascu-lar imaging tables in theUS, Japan and Europe.
imagiQ hasbeen
a key contributor to thetechnology shift fromopen to endovascularrepair.
The new imagiQ2 isintroduced as part ofStille’s new strategic planthat includes long-termgoals to leverage on thehigh-end mobile imagingtable market. First cus-tomer shipments areexpected in Q3–Q4 of2012.
Jotec receivesCE approval forE-vita thoracic3G stent graftsystem
Jotec received CE markapproval for E-vita tho-racic 3G in end of April2012 and has started tolaunch the system interna-tionally. E-vita thoracic
3G is Jotec’s third genera-tion of thoracic stent graftsystems and is approvedfor endovascular treat-ment of aneurysm, dissec-tion, penetrating aorticulcer as well as intramuralhaematoma of the thoracicaorta.
According to Jotec, E-vita thoracic 3G presentsmeaningful enhancementson the stent graft as wellas on the delivery system.The stent graft now fea-tures a unique spring con-figuration to achievehigher stent graft flexibil-ity without losing theappropriate longitudinalstiffness. The adaptedproperties allow best ves-sel adaption even in com-plex aortic anatomies.Stent graft sizes are avail-able from 24 to 44mm indiameter and from 130 to230mm in length.Different proximal anddistal stent graft designsplus straight and taperedconfigurations are avail-able for choosing theright product for individ-ual treatment of aorticdiseases. A uniquecatheter design with mul-tifunctional zones is usedfor the delivery systemand allows sheathlessapplication, excellentpushability and superiorflexibility without risk ofkinking. A hydrophilic
coating significantlyreduces friction
duringinsertion into the arterialvessel system. The deliv-ery system offers thesmallest crossing catheterprofile from 20 to 24F fora broad range of stentgraft versions comparedto other thoracic stentgraft systems in the mar-ket today.
E-vita thoracic 3G con-tinues the proven separateproximal spring fixationfor safe repositioning ofthe partially releasedstent graft as well as thepatented Squeeze-to-Release deploymentmechanism for stepwiseor continuous release ofthe stent graft whilefocusing on precise posi-tioning and safe handling.
June 2012
BIBA Publishing
33Market watch
Product News
EverFlex
Symplicity
E-vita 3G


Absolute Proreceives FDAapproval fortreatment of iliacartery disease Abbott has announced thatthe FDA has approved theAbsolute Pro VascularSelf-Expanding StentSystem for the treatmentof iliac artery disease.This approval was sup-ported by the MOBILITY(Omnilink Elite orAbsolute Pro stent used inthe iliac artery) study,which demonstrated thatAbsolute Pro is safe andeffective, even in patientswith complex disease.
“Iliac artery diseasegreatly impacts patients’overall quality of life,”said Tony S Das, director,Peripheral VascularInterventions, CardiologySection, PresbyterianHeart Institute in Dallas,USA, and co-principalinvestigator of theMOBILITY trial. “WithAbsolute Pro, US physi-cians now have an addi-tional option that isproven safe and effectiveto treat many patients withthis debilitating disease.”
Absolute Pro is a self-expanding nitinol stentsystem made of a flexiblematerial designed to allowthe stent to conform tochallenging lesions. Itincorporates advancedtechnologies for optimalstent visibility, with adelivery system that isdesigned to minimise fric-tion during stent deploy-ment and ensure precisestent placement at thelesion site.
The FDA approval wassupported by the results ofthe Absolute Pro arm ofthe MOBILITY trial, aprospective, non-ran-domised, two-arm, multi-centre study that evaluatedtwo Abbott stents,Absolute Pro andOmnilink Elite, in patientswith iliac artery disease.In the Absolute Pro arm,151 patients with iliacartery disease wereenrolled at 33 centres inthe United States. Thestudy met its primary end-
point, with a nine-monthmajor adverse event rateof 6.1% (p<0.0001). Thisresult was found to be sig-nificantly lower than theperformance goal of19.5%, which was devel-oped from published liter-ature on previous iliacartery stenting studies.The major adverse eventrate was defined as deathdue to any cause, myocar-dial infarction, clinicallydriven target lesion revas-cularisation and majoramputation on the treatedside(s). The results of theOmnilink Elite arm of thestudy will be availablelater this year.
PowerflexPro .035” PTAdilatationcatheterlaunched
Cordis has announced thelaunch of Powerflex Pro.035” percutaneous trans-luminal angioplasty (PTA)dilatation catheter, a newaddition to Cordis’ lowerextremity solutions port-folio.
Available through a tar-geted and limited release,Powerflex Pro deliversadvanced crossability andremarkable versatility totreat routine or challeng-ing cases in the lowerextremity; targeted specif-ically at Iliac and superfi-cial femoral artery dis-ease, according to a pressrelease issued by Cordis.
Vascops receivesCE approval forits A4clinicssoftware
Vascops has announced anew release and CEapproval for the A4clin-ics software. A4clinicsallows a patient-specificassessment of abdomi-nal aortic aneurysmrupture risk from stan-
dard clinical computertomography-angiographyimages together with basicpatient data such as age,gender, blood pressure,and others.
It is the first system forclinical use that providesphysicians with the PeakWall Rupture Risk(PWRR) index, stated thecompany. The PWRRindex reflects the abilityof the aortic wall to carrythe blood pressure for thegiven aneurysm anatomy.The clinical value of thePWRR index was estab-lished through clinicalstudies and its computa-tion is based on the samemathematical models thathave been applied formore than 50 years inother fields such asthe aviation
industry. ThePWRR index is
translated into a rupturerisk equivalent diameter,which is a powerful indi-cator with which to identi-fy high risk patients with-in the pre-operative rangeof up to 5.5cm.
A4clinics diagnosticoutput includes alsocolour-coded three-dimen-sional models of theaneurysm with which thephysician can easily identi-fy locations of high risk ofwall rupture. A list of othermeaningful patient-indi-vidual parameters includ-ing centerline-based maxi-mum diameter, aneurysmvolume, peak wall stressare also listed in therecently available analysisreport. A sequence of cen-terline-based diam-eter measure-ments all
along the aneurysm allowsa comprehensive monitor-ing of small aneurysms,which is clearly superior toa single diameter or vol-ume measurement. Apartfrom this additional func-tionality the new release isalso equipped with a fastpatient database. An opti-mised intern data structureprovides an unmatchedperformance and the intu-itive user interface sup-ports an effective handlingof patient cases.
Collaborations with nu-merous European hospitalsand universities guaranteea sound scientific basis forthe A4clinics software.First clinical experienceswith the software are nowavailable in the literature.Retrospective studies fromDepartment of Vascularand Endovascular Surgery,Ruprecht-Karls UniversityHeidelberg, Germany
(Journal of
Endovascular
Therapy,18(3):289–98, 2011)and the Department ofVascular Surgery, St Anto-nius Hospital, Nieuwegein,The Netherlands (Journal
of Vascular Surgery,55(2):326–330, 2012) re-ported high agreementamong observers of themeasurements taken withthe system, a key require-ment for its integration inthe clinical work flow.These studies verified alsothat physicians withoutany engineering back-ground could safely andeffectively handle the soft-ware tool within theiravailable clinical environ-ment.
“Abdominal aorticaneurysm repair is typical-ly performed for
aneurysms reach-ing
5.5cm, but a single thresh-old diameter is not appro-priate for every patient andthe indication for repairshould be individualised.Such an individual assess-ment is possible using theVascops software, whereknown risk factors likehigh wall tension, asym-metric abdominal aorticaneurysm geometry, highblood pressure, femalegender and other wallweakening phenomena, areall considered,” said JesperSwedenborg, former headof the Department of Vas-cular Surgery at Karolins-ka Hospital Stockholm,Sweden.
New Aorflexdelivery systemlaunched
Lombard Medical hasannounced the launch ofthe next generation oftheir delivery system. Thenew system, Aorflex,combines the clinicalexcellence of Aorfixstent graft with thenew Aorflex
delivery sys-tem
which offers a range ofclear clinical benefits suchas:n Greater deployment
control with exception-al one to one torque
n Ease of use withreduced deploymentforces
n Reduced risk of vesseldamage withhydrophilic coating The company says
extensive research anddevelopment, engineeringand bench testing datacombined with real lifeclinical use of Aorfix inover 2,000 patients world-wide give clinicians theconfidence to treat extremeabdominal aortic aneurysmanatomy without theunknown risks associatedwith off-label use.
Boston Scientificannounces FDAapproval and USlaunch of Epic
Vascular Stent
On 17 May 2012,Boston Scientific
announced FDA approvaland market launch of theEpic Vascular Self-Expanding StentSystem. The Epic Stent is
designed to open blockedarteries in patients withiliac artery stenosis.
“The Epic Stent Systemdemonstrates an excellentcombination of flexibility,radial force and deploy-ment accuracy – all impor-tant attributes when treat-ing challengingatherosclerotic lesions inthe iliac arteries,” saidThomas Shimshak, med-ical director atWheatonFranciscanHeart Care inRacine,USA. “Thecompre-hensivestent
sizematrix
should alsohelp meet a
variety ofclinical
requirementswhen treating iliac
arterial disease withno compromise in
deliverability or stentperformance.”The Epic Stent is a
self-expanding nitinolstent designed to sustainvessel patency, while pro-viding enhanced visibilityand accuracy during place-ment. It employs an inno-vative Tandem Architec-ture, which is engineeredto provide excellent stentflexibility while maintain-ing predictable radial forcecharacteristics and fractureresistance. The Epic Stentemploys distal and proxi-mal radiopaque markersand all stent sizes are com-patible with 6Fsheaths. The stent deliverysystem is offered in twoshaft lengths (75cm and120cm) for all sizes and iscompatible with 0.035”guidewires.
In January, BostonScientific announced thatthe ORION trial met itsprimary clinical endpoint.The Epic Vascular StentSystem demonstrated alow nine-month majoradverse events rate of3.4% in the intent-to-treatpopulation, which wassignificantly lower thanthe pre-specified perform-ance goal of 17%(p<0.001) based on histor-ical published outcomesfor iliac stenting.
The Epic Vascular Self-Expanding Stent Systemreceived CE markapproval and was launchedin Europe and other inter-national markets in 2009.
June 2012
BIBA Publishing
35Market watch
Product News
Absolute Pro
Aorflex


June 2012
BIBA Publishing
37Trials
Medtronicexpandsavailability ofValiant Captiviastent graft andannouncescompletion ofenrolment in theRESCUE trial
Medtronic is expandingavailability of the ValiantCaptivia Thoracic StentGraft System in severalcountries, includingChina, Japan and theUnited States. The deviceis approved by the FDAfor endovascular repair ofaneurysms and penetrat-ing ulcers of the descend-ing thoracic aorta inpatients with a non-aneurysmal aortic diame-ter in the range of 18–42mm andnon-aneurysmal aorticproximal and distal necklengths ≥20mm. Thedevice’s approved indica-tions in China and Japanare similar.
The Valiant Captiviasystem features an eight-peak crown that effective-ly secures the deployeddevice inside the aorta. Itis also more flexible andconformable through theelimination of the longitu-dinal connecting barfound in other stent grafts.
Medtronic alsoannounced in May thecompletion of enrolmentin an investigational clini-cal study of the ValiantCaptivia Stent GraftSystem as a minimallyinvasive treatment forblunt thoracic aorticinjuries. Data from thisFDA-approved clinicalresearch study, calledRESCUE, will be used toseek an expanded indica-tion for the device to treataortic transections. Thestudy’s principal investi-
gator is Rodney White,chief of vascular surgeryat Harbor-UCLA MedicalCenter in Los Angeles.
Fifty patients at 20 USsites were enrolled inRESCUE to investigatethe safety and effective-ness of stent grafts for thetreatment of blunt thoracicaortic injury. Early resultson the first 33 patientsenrolled in the study werepresented in late March atthe 2012 Annual ScientificMeeting of the Society ofInterventional Radiology.All-cause mortality at 30days, the study’s primaryendpoint, was 12% forthis patient group.
“Traditionally, the mor-tality rates associated withsurgical repair of blunt tho-racic aortic injuries rangefrom 15 to 20%,” saidAlan Matsumoto, profes-sor and chair of the depart-ment of radiology andmedical imaging at theUniversity of VirginiaHealth System in Char-lottesville, USA, and pre-senter of the data. “Withthis frame of reference, theearly data from RESCUEare very encouraging. Welook forward to reportingthe final results on all 50patients in the study at amajor upcoming scientificmedical meeting.”
Avinger enrolsfirst US patient inCONNECT IIglobal clinicaltrial
Avinger announced theenrolment of the first USpatient in the CONNECTII global clinical trial on 6March. Ian Cawich,Arkansas Heart Hospital,enrolled the first USpatient. The announce-ment came just two weeks
after Bernhard Reimersenrolled the first Europeanpatient in the CONNECTII trial at Ospedale diMirano in Mirano, Italy.
CONNECT II is a mul-ticentre, non-randomisedglobal clinical studydesigned to evaluate thesafety and efficacy ofOcelot, the first chronictotal occlusion crossingcatheter to use real-timeoptical coherence tomog-raphy (OCT). CurrentlyCE marked, Ocelot isdesigned for crossingchronic total occlusions inthe legs while simultane-ously using OCT to navi-gate inside the arteries.
“We are participating inCONNECT II because ourpatient, if treated withother current options onthe medical market, couldface amputation anddeath,” said Cawich.“With Avinger’s Ocelot,we believe this patient canbe saved right now fromboth. The timing of thistrial feels like a bit of mir-acle to our patient.”
CONNECT II is aprospective study that willevaluate 100 patients withfemoropopliteal chronictotal occlusion lesions at17 sites, including three inEurope, where Ocelotreceived the CE mark in2011.
Conditional FDAapproval to conduct thisstudy was received inJanuary. Co-principalinvestigators for the trialinclude Arne Schwindt, StFranziskus Hospital inMuenster, Germany, andMatthew Selmon, AustinHeart Hospital in Austin,USA.
Biotronikannouncespositive resultsfor the Passeo-18Lux PaclitaxelReleasingBalloon Six-month results fromthe BIOLUX P-I study,demonstrating excellentsafety and efficacy resultsfor the Biotronik Passeo-18 Lux PaclitaxelReleasing Balloon, werepresented on 17 May 2012at the EuroPCR 2012 con-gress by Andrej Schmidt,chief angiologist atHerzzentrum/Park-Krankenhaus, Leipzig,Germany.
The Passeo-18 LuxPaclitaxel ReleasingBalloon is a novelapproach for treating de
novo and restenoticfemoropopliteal lesions.The device is based on theproven Passeo-18 percuta-neous transluminal angio-plasty catheter, which isthen coated with a matrixof antiproliferative pacli-taxel and the biocompati-ble butyryl-tri-hexyl cit-rate (BTHC)
excipient—enabling anoptimal drug transfer tothe target lesion tissue. Inaddition, Passeo-18 Luxfeatures a unique, protec-tive insertion aid to facili-tate easier device intro-duction and handling.
BIOLUX P-I is a ran-domised controlled studyinvestigating the safetyand performance of thePasseo-18 Lux (n=30)versus an uncoatedPasseo-18 angioplastycatheter (n=30), for thetreatment of lesions in thefemoropopliteal segmentup to 200mm in length.Patients were enrolled atfive centres in Germanyand Austria.
Primary endpoint dataevaluated by an inde-pendent core-lab docu-mented significantlyreduced angiographic latelumen loss at six months(p=0.033) in the Passeo-18 Lux arm (in-segmentlate lumen loss0.51±0.72mm) vs. theuncoated angioplastycatheter (in-segment latelumen loss 1.04±1mm).Binary restenosis wasalso reduced (p=0.048) inthe Passeo-18 Lux armvs. the uncoated percuta-neous transluminal angio-plasty catheter (11.5% vs.34.6% respectively).
“The Passeo-18 Luxhas demonstrated excel-lent results in this studyand reinforces our confi-dence in drug-releasingballoons as a viable thera-py option forfemoropopliteal arterial
disease,” said DierkScheinert, chief clinicalinvestigator of BIOLUXP-I and Department Head,Herzzenturm/Park-Krankenhaus Leipzig,Germany. “This device isvery deliverable and easyto use compared withother technologies andtreatment options forthese demanding vessels.”
JuventasTherapeuticsenrols patients inphase IIa STOP-CLI trial
Juventas Therapeuticsreported that it isenrolling patients in aplacebo-controlled, ran-domised double-blindedphase IIa study evaluat-ing the safety and effica-cy for JVS-100 inpatients with RutherfordClass 4 or 5 critical limbischaemia (CLI). JVS-100, the company’s leadproduct, encodes stromalcell-derived factor 1(SDF-1) which has beenshown to repair damagedtissue through recruit-ment of circulating stemcells to the site of injury,prevention of ongoingcell death and restorationof blood flow.
Patients are enrolling atNorthwestern MemorialHospital, Cardiology PC,Minneapolis HeartInstitute Foundation, andSumma Health Systems.In addition, the companyis enrolling patients atthree leading cardiovas-cular institutions in India;Medanta the Medicity, SirGanga Ram, and FortisEscorts Heart Institute.
“We are excited to beparticipating in the STOP-CLI trial,” said MelinaKibbe, principal investi-gator for the study and theEdward G ElcockProfessor of SurgicalResearch at theNorthwestern UniversitySchool of Medicine.
Patient outcome meas-ures in the STOP-CLI trialinclude safety, time toamputation, wound clo-sure, TcPO2, ankle-brachial index and toe-brachial index.
Clinical News
Ocelot
Please visit www.vascularnews.com/register
Sign up now for afree subscription!
Passeo-18 Lux

September 2010
BIBA Publishing
38 Companies June 2012
7–9 June
Society for Vascular Surgery
Annual Meeting
Washington, USA
Gaylord National Resort &
Conference Center
T +1 (312) 334 2300
F +1 (312) 334 2320
W www.vascularweb.org
11–12 June
MEET 2012 – Multidisciplinary
Europen Endovascular Therapy
Rome, Italy
Crowne Plaza St Peter’s Hotel
T +33 (0)491 571960
F +33 (0)491 571961
W www.meetcongress.com
28–29 June
British Society of Endovascular
Therapy
Stratford-upon-Avon, UK
Walton Hall
W www.bset.co.uk
28–30 June
Annual Meeting of the
European Venous Forum
Florence, Italy
Palazzo dei Congressi
T/F +44 (0)20 8575 7044
E admin@europeanvenous-
forum.org
W www.europeanvenousforum.org
28–30 June
VIP (Vascular International
Padova) Congress
Padua, Italy
T +39 049 860 1818
F +39 049 860 2389
W www.vipcongress2012.org
1–5 July
XXV World Congress of the
International Union of
Angiology
Prague, Czech Republic
T +420 221 979 351
F +420 731 496 062
W www.iua2012.org
7 September
Thoracic Aortic Masterclass
2012 – New & Complex
Innovations
London, UK
Guy’s Hospital
T +44 (0)207 449 9172
F +44 (0)7736 771929
19–21 September
ESVS – The European Society
of Vascular Surgery Annual
Meeting
Bologna, Italy
Novo Polo Congressuale
T +45 2682 4869
W www.esvs.org
13–14 September
TOBI 2012 – Total Occlusion
and Bifurcation Interventions
Venice/Mestre, Italy
T +39 010 255146
F +39 010 255009
W www.tobionline.org
4–6 October
3rd International Meeting on
Aortic Diseases
Liege, Belgium
Palais de Congres
T +33 (0) 491 57 1960
F +33 (0) 491 57 1961
W www.chuliege-imaa.be
11–13 October
XXII MLAVS 2012 –
Mediterranean League of
Angiology and Vascular Surgery
Civitavecchia, Italy
T +39 06 330 531
F +39 06 330 53 229
W www.mlavs.org
9–12 October
VIVA – Vascular Interventional
Advances Meeting
Las Vegas, USA
Wynn Las Vegas
W www.vivapvd.com
31 October–3 November
EVF Hands On Workshop on
Venous Disease
Larnaca, Cyprus
T/F +44 (0)20 8575 7044
E admin@europeanvenous-
forum.org
W www.europeanvenousforum.org
Founder ofStraub Medicalpasses away Immanuel Straub, founderof Straub Medical, passedaway on 31 March at theage of 82. “Straub was anextraordinary engineerand entrepreneur. Thevariety of his activities,his technical innovations,his entrepreneurial visionand his provident leader-ship facilitated his globalsuccess in various indus-tries,” the company stated.
In the 1950s, accordingto a press release issuedby the company,Immanuel Straub mod-ernised technical springmanufacturing, whichsince the outbreak of theII World War had hardlyseen any advancement. Toa variety of industries,most notably the automo-tive industry, he providednewly designed machinesfor spring production,high-performance springs,and modern devices andproducts made possible bythe new components.
In 1967, he foundedStraub Kupplungen. In the1990s, Straub establisheda holding company tobundle his shareholdings.In 1998, he decided to
accept an internationalcorporate’s bid for hisgroup of companies. Heexcluded his most recentlyfounded company, StraubMedical, from this saleand made it an independ-ent company.
In the 15 years since itsfounding, Straub Medicalhas become a leadinginternational company inthe medical devices sectorwith the production anddistribution of its mini-mally invasive rotationalcatheters.
In 1998, ImmanuelStraub won the Lilienberg-Award. With its award, theLilienberg foundation hon-ours an entrepreneurialpersonality whose meritsare based on an outstand-ing personal entrepreneur-
ial achievement.“Immanuel Straub left
an impressive lifetimelegacy,” said Hans JakobNold, vice chairman of theSupervisory Board ofStraub Medical. “In his 58years of entrepreneurship,he has always looked forsolutions others have saiddo not exist. Mr Straubfound these solutions, andwith extraordinary entre-preneurial vision, madeeach of them a globalcommercial success.”
TriVascular hasnew chairman,CEO andpresident
On 12 April, the board ofdirectors of TriVascularappointed Christopher GChavez as chairman, CEOand president. Michael VChobotov, co-founder, for-merly president and CEO,has been appointed chieftechnology officer andwill continue to serve onthe board of directors.
Chavez joinsTriVascular with over 30years of leadership experi-ence in the medical deviceindustry. For the past sixyears, Chavez served aspresident of theNeuromodulation division
of St Jude Medical.Chavez joined St JudeMedical through its acqui-sition of AdvancedNeuromodulation Systems(ANS) in 2005. At ANS,he served as CEO, presi-dent and director leadingANS/NMD through 14years of profitable growthand innovation. Prior toANS, Chavez spent 17years at Johnson &Johnson. Chavez receivedhis MBA from the HarvardBusiness School and holdsa bachelors degree inaccounting from NewMexico State University.
Endologix selectsJohn McDermottas chairman ofthe board ofdirectors
Endologix has announcedthe appointment of JohnMcDermott, Endologix’spresident and CEO, to theadditional position ofchairman of the board ofdirectors. The transitionwas effective on 24 May2012, date of the compa-ny’s annual shareholder’smeeting. According toEndologix, Franklin DBrown announced hisdecision to retire as chair-man of the board at theend of his current term,“after a highly successfuland distinguished 15-yearcareer with the company”.He served in several exec-utive leadership positions,
including CEO from 1998to 2003 and the mostrecent, chairman of theboard from 1998 to 2012.
Sanofi to acquirePluromed
Sanofi and Pluromed haveentered into a definitiveagreement under whichSanofi is to acquirePluromed. Pluromed hasdeveloped a proprietarypolymer technology, calledRapid TransitionPolymers, pioneering theuse of injectable plugs toimprove the safety, effica-cy and economics of med-ical interventions. Sanofiwill commercialisePluromed’s LeGoo, a high-ly innovative FDAapproved and CE-markedgel for temporary endovas-cular occlusion of bloodvessels during surgicalprocedures.
“The acquisition ofPluromed underscoresSanofi’s commitment tostrengthen its Biosurgeryportfolio,” said AlisonLawton, senior vice presi-dent and general manager,Sanofi Biosurgery. “LeGoois a breakthrough technolo-gy with the potential tochange the paradigm ofvascular and cardiovascu-lar surgical procedures, byproviding fast, temporarycontrol of blood flowwhile avoiding vessel trau-ma associated with stan-dard of care.”
Industry News
Calendar of events
Editor-in-chief:
Roger Greenhalgh
Publisher:
Stephen Greenhalgh
Head of Publishing:
Marcio Brito
Editor:
Marcio Brito
Editorial contribution:
Urmila Doraswami
Design:
David Reekie
Layout:
Tim Parker
Advertising:
Nathalie Fortin
Subscriptions:
Sue Couch
Please contact the
Vascular News team
with news or advertising
queries
Tel: +44 (0)20 7736 8788
Published by:
BIBA Medical,
44 Burlington Road,
Fulham, London,
SW6 4NX, UK
Tel: +44 (0) 20 7736 8788
Fax: +44 (0) 20 7736 8283
Printed by:
Buxton Press
© BIBA Medical Ltd, 2010
All rights reserved.
Printed by Buxton Press.
Reprint requests and all
correspondence regarding the
newspaper should be addressed
to the editor at the above address.
Write to us!If you have comments on
this issue or suggestions
for upcoming editions,
write to
Vascular News
team
Make sure youget your copy of
Vascular News
Next issue
September
2012
Immanuel Straub





























![Tasc Basic[1]](https://img.dokumen.tips/doc/110x75/5449bfc5af795984188b45cc/tasc-basic1.jpg)