Embed Size (px)
Citation preview
Accepted Manuscript
Title: Paediatric lung recruitment: a review of the clinicalevidence.
Author: Jacqui Jauncey-Cooke Chris E East Fiona Bogossian
PII: S1526-0542(14)00027-XDOI: http://dx.doi.org/doi:10.1016/j.prrv.2014.02.003Reference: YPRRV 965
To appear in: YPRRV
Received date: 11-8-2012Revised date: 13-2-2014Accepted date: 15-2-2014
Please cite this article as: Jacqui Jauncey-CookeChris E EastFiona BogossianPaediatric lung recruitment: a review of the clinical evidence. (2014),http://dx.doi.org/10.1016/j.prrv.2014.02.003
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

Page 1 of 18
Accep
ted
Man
uscr
ipt
Author Affiliations for paper submission: Paediatric lung recruitment - A review of experimental and clinical evidence (ID 34253)
1. Jacqui Jauncey-Cooke PhD Candidate, School of Nursing & Midwifery, The University of Queensland, Australia Master of Nursing, Grad Dip Crit Care Nursing, Grad Cert Health Professional Ed. [email protected] [email protected] Mobile - +61 418335634 Work - +61 7 3163 1143
2. Prof Chris E. East RN, RM, PhD Dept of Perinatal Medicine, The University of Melbourne, Royal Woman’s Hospital, Melbourne Dept of Obstetrics & Gynaecology, The University of Melbourne, Australia [email protected]
3. 3. A/Prof Fiona Bogossian RN, RM, PhD School of Nursing & Midwifery, The University of Queensland, Australia [email protected]
address(es):[email protected] Response:

Page 2 of 18
Accep
ted
Man
uscr
ipt
Abstract: Lung recruitment is used as an adjunct to lung protective ventilation strategies. Lung recruitment is a brief, deliberate elevation of transpulmonary pressures beyond what is achieved during tidal ventilation levels. The aim of lung recruitment is to maximise the number of alveoli participating in gas exchange particularly in distal and dependant regions of the lung. This may improve oxygenation and end expiratory levels. Restoration of end expiratory levels and stabilisation of the alveoli may reduce the incidence of ventilator induced lung injury (VILI). Various methods of lung recruitment have been studied in adult and experimental populations. This review aims to establish the evidence for lung recruitment in the pediatric population.
Keywords: paediatric; mechanical ventilation; lung recruitment; oxygenation; end expiratory lung volume

Page 3 of 18
Accep
ted
Man
uscr
ipt
Introduction
All mechanically ventilated paediatric patients are at risk of developing ventilator induced lung injury (VILI) and while mechanical ventilation may be lifesaving, a proportion of these children will acquire a degree of lung injury as a direct result of the ventilation strategies employed by the clinician.1 Mechanical ventilation strategies are continuously evolving but never more so than following the American‐European Consensus Conference, ARDSNet lung protective recommendations.2 These lung protective ventilation strategies (LPVS) were developed post large, multi‐site randomised trials in adults.2,3 Low tidal volumes, adequate PEEP, minimal peak pressures and minimal FiO2 are now considered standard practice.
2,3 These recommendations have been universally extrapolated to paediatrics, possibly due to the paucity of paediatric data. A retrospective cohort study by Halbertsma and colleagues in paediatrics did demonstrate a correlation between high tidal volume ventilation and a reduced oxygenation ratio (P/F) which is consistent with the findings of the ARDSNet study.4 Ultimately, irrespective of how gently we treat the paediatric lung, iatrogenic harm still occurs.1
Lung recruitment is considered an adjunct to LPVS and in part addresses the chronic derecruitment that occurs secondary to low tidal volume ventilation.5,6 This chronic derecruitment coupled with the acute derecruitment that occurs with each circuit disconnection contributes to the incidence of VILI. This review aims to assess the evidence for lung recruitment in mechanically ventilated paediatrics.
A literature search was undertaken in 2014. Databases searched included Medline, Embase, Lilac, Central register for Cochrane reviews and Cinahl. The search yielded 70 abstracts. Following a review of the abstracts 8 relevant, paediatric papers were identified. The paediatric literature is referred to in the first instance. In the absence of paediatric literature, adult and experimental literature is considered.
What is lung recruitment?
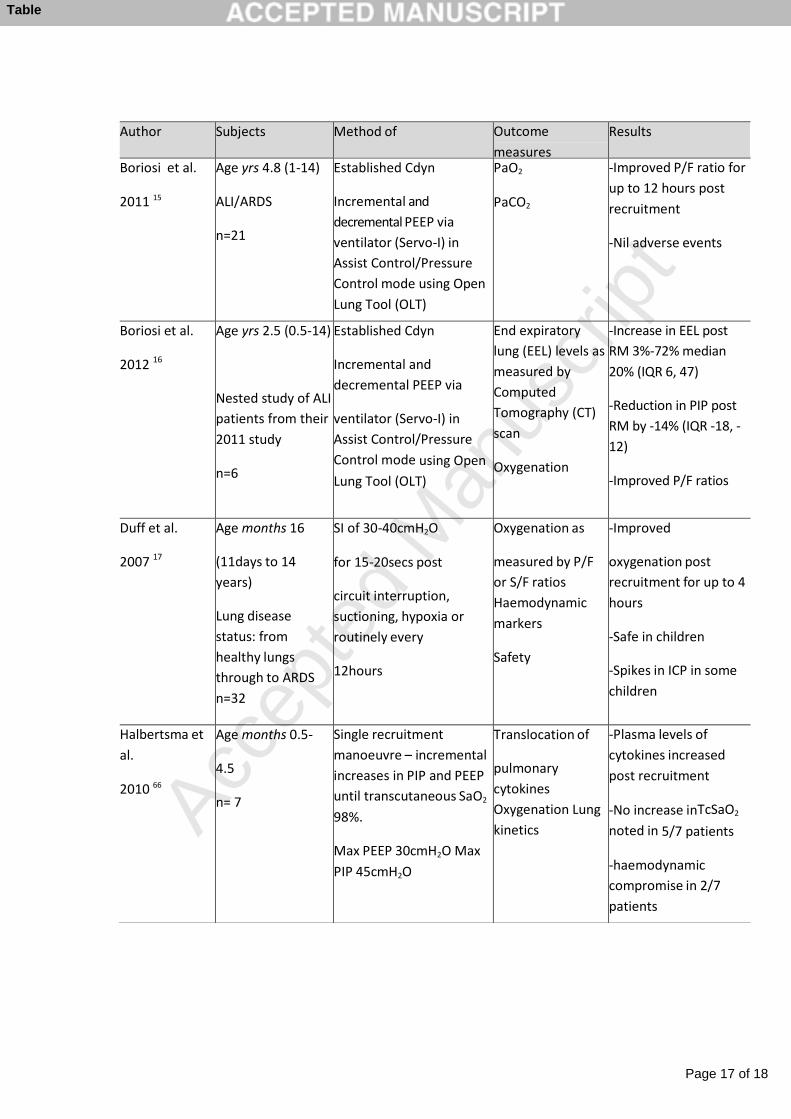
Lung recruitment is a deliberate strategy to increase transpulmonary pressure; to maximise the number of alveoli participating in gas exchange.7 The aim of lung recruitment is to recruit all recruitable alveoli and minimize atelectic regions of the lung. It can be achieved by either a sustained inflation (SI) or by briefly increasing positive end‐expiratory pressure (PEEP). These methods aim to overcome alveolar threshold opening pressures and/or overcome alveolar threshold closing pressures. Table 1 lists the current evidence of lung recruitment in paediatrics.
Table 1. Paediatric studies of lung recruitment

Page 4 of 18
Accep
ted
Man
uscr
ipt
Whose lungs do you recruit?
The process of lung recruitment is applicable to mechanically ventilated children and those undergoing general anaesthesia. Studies have been undertaken in both of these populations. Children, because of developmental differences may benefit most from lung recruitment; physiologically immature lungs differ significantly from adult lungs. At term, neonatal lungs possess only 25% of their alveolar potential with a rapid increase in number in the first two years of life and the interalveolar connections of Kohn’s pores are absent.8,9 Diaphragmatic muscle fibre fatigue is rapidly acquired as only 25% of muscle fibres are the fatigue resistant Type I – slow twitch fibres, compared to 50% at 8 months of age.9 Additionally, the diaphragmatic angle is almost horizontal rendering it less efficient in terms of contractility and oxidative capacity.9 By approximately two years of age, chest wall and lung compliance is similar to adults however, older infants and children continue to have a significantly smaller airway radius in proportion to their weight, less elastic retraction force, and a lower relaxation volume.10‐12 These factors all combine to predispose infants and children to atelectasis and hence an increased risk of VILI. Subsequently these populations show potential to benefit most from lung recruitment. In terms of lung disease severity, which patients do you recruit? Using clinically standard oxygenation ratios to crudely define the status of lungs; healthy lungs (PaO2/FiO2 {P/F} ratio) ≥300, acute lung injury (ALI) of 201‐300 and acute respiratory distress syndrome (ARDS) ≤200; which of these cohorts benefit from lung recruitment? Two studies have been undertaken on children with healthy lungs undergoing scheduled general anaesthesia.13,14 Both of these studies demonstrated the benefit of lung recruitment in the healthy lung in terms of improved compliance and a reduction in atelectasis.13,14 A study by Boriosi and colleagues using incremental PEEP in children demonstrated an overall improvement in oxygenation that was sustained for 12 hours in children with ALI/ARDS.15 Further subgroup analysis on the ALI population from this study demonstrated an improvement in EEL and P/F ratio post recruitment as well as a significant reduction in PIP.16 A study by Duff and colleagues in children with varied respiratory status demonstrated a significant and sustained reduction in FiO2 requirement for up to 6 hours post a SI manoeuvre.17 Another study using SI as a means to recruit lungs in combination with a stepwise recruitment manoeuvre reversed substantial atelectasis in dependant regions of the lung as measured by Electrical Impedance Tomography (EIT) which was also associated with improvements in gas exchange.18 No recruitment studies have been undertaken exclusively in children with ARDS however a study by Wolf and colleagues demonstrated the significant loss of global and regional lung volume post endotracheal suctioning in children with ARDS as measured by EIT.19 Potentially those children with ARDS have the most to gain from lung recruitment. In adults, a number of studies have demonstrated a positive benefit of lung recruitment in patients with ARDS. A clinical study by Dyhr and colleagues used two hyperinflations to 45cmH2O, held for 20s with an interval of 60seconds in patients with ARDS post‐suctioning.20 They found that the use of a recruitment manoeuvre, when combined with adequate ongoing PEEP, improved both oxygenation and EELV.20

Page 5 of 18
Accep
ted
Man
uscr
ipt
There is the potential that some children will be non‐responders to lung recruitment and that the lung recruitment may in fact simply overdistend already recruited alveoli particularly in proximal regions. This was demonstrated in the study by Wolf and colleagues as the reversal of atelectasis in dependant regions was accompanied by considerable overdistension in nondependent lung regions.18 This overdistension may contribute to barotrauma and subsequent VILI.18,19 Children may be more susceptible to overdistension than adults due to their compliant chest wall.21,22 In an experimental study, hyperinflated regions of the lung shifted to normally aerated areas at PEEP levels of 8cmH2O (mean of 30% decrease) and yet hyperinflated areas still appeared at zero end expiratory pressure.23 Hyperinflation of easily distensible regions of the lung is an acknowledged limitation of recruitment manoeuvres.18,20,22‐24
How to recruit lungs?
Various methods of lung recruitment have been studied in paediatrics but typically they involve either sustained inflations or manipulating PEEP. A recent study involved incremental increases in PEEP; an open lung strategy.15 PEEP is used to maintain alveolar patency and stability at end‐expiration but during tidal ventilation is usually set at a level insufficient to overcome the threshold opening pressure of atelectic alveoli.25‐27 Increasing PEEP effectively allows the clinician to manipulate the functional residual capacity (FRC) and thereby minimise physiological deadspace, improving ventilation/perfusion mismatch and decreasing shunt fraction.6,12,28‐30 Boriosi and colleagues chose this method of recruitment to assess the safety and efficacy of the open lung tool in paediatrics. Ultimately they used a modified version but found that oxygenation improved and peak inspiratory pressures were significantly reduced by 17% up to 12 hours post recruitment.15,16 Incremental increase in both Peak Inspiratory Pressure (PIP) and PEEP has been shown to result in improved gas exchange, tidal volume (Vt), EELV, oxygenation and lung compliance in ventilated adults.31‐34
Sustained inflations (SI) or inspiratory holds recruit alveoli via a combination of factors – the plateau pressure achieved and the duration of time maintained at that pressure. SI’s are reported within the literature as ranging from 25‐60cmH2O and held for a period of 10‐30 seconds.14,17,18,20,35‐37 This is achieved by using the Continuous Positive Airway Pressure (CPAP) setting on the ventilator, the ‘inspiratory hold’ feature or manually by using anaesthetic bagging circuits.17,18,34,36,37 Irrespective of technique, the purpose of the SI is to maintain an elevated plateau pressure for a period of time greater than that achieved with tidal breathing. A few studies have investigated the use of lung recruitment in paediatrics using the SI method. The safety and efficacy of using a SI of 30‐40cmH2O in paediatrics has been established in one study when the SI was maintained for 15‐20 seconds following circuit disconnection, suction, desaturation and/or routinely every 12 hours with positive results in terms of oxygenation.17 Another study in a PICU setting used a SI to 30cmH2O for 30 seconds post endotracheal suctioning.
36 The study design differed from similar studies in that there was a five‐ minute delay between suctioning and the lung recruitment manoeuvre and the SI was achieved using an anaesthetic bag which necessitated disconnection and then reconnection to the ventilator circuit.36 The authors concluded that the evidence did not support recruitment manoeuvres; that dynamic

Page 6 of 18
Accep
ted
Man
uscr
ipt
compliance was not improved post lung recruitment. The authors acknowledged that given the loss of EELV attributed to the disconnection of the circuit that any gains achieved from the recruitment manoeuvre could be reduced.36 Another clinical study in healthy children undergoing anaesthesia measured the extent of atelectasis induced by an FiO2 of 1.0 and the rate of recruitment with a single SI procedure.13 The results showed a significant re‐recruitment of atelectatic alveoli at pressures of 25‐30cmH2O.
13 This study used what they refer to as a TRIM – a timed re‐expansion inspiratory manoeuvre ‐ involving a constant pressure of 30cmH2O for 10seconds which resulted in significantly higher pulmonary compliance and lower airway resistance than the control group.(P<0.0001).13 Other studies have also demonstrated significant improvements in compliance post recruitment and in some instances oxygenation.33,34,37,38
An alternative lung recruitment strategy is to use the inflexion points of the Pressure‐Volume (P‐V) curve derived from ventilatory software. P‐V curves can be used as a tool to manage ventilation and recruitment as they describe the viscoelastic characteristics of the lung.13 There is a general consensus in the literature that opening of lung units occurs along the entire length of the inspiratory limb of the P‐V relationship.37‐40 The effectiveness of PEEP in recruiting alveolar tissue correlates with the value of the Lower Inflexion Point (LIP).13,40‐41 A range of ventilators have software suitable to measure P‐V curves. A method of determining an appropriate figure for SI was calculated by Qiu and colleagues based upon 5 X Mean Airway Pressure (MAP).42 This method provided optimal recruitment as measured by oxygenation, pulmonary dynamics, haemodynamics and lung histology in an experimental study by Lindgren and colleagures.42 Some clinicians use the Upper Inflexion Points (UIP) and LIP’s to establish optimal PEEP and/or optimal recruitment. Two studies have confirmed the effective use of PV loops to reflect recruitment above the LIP and below the UIP in adult populations.41‐42 However a study by Pestana and colleagues found that P‐V curves rarely reflected recruitment manoeuvres in ARDS patients which they suggest limits their application in the clinical setting as a measure of recruitment efficacy or as a guide to manage ventilation.43 Two studies caution clinicians against using inbuilt ventilator P‐V software as they had significant deleterious results in their research.44‐47 P‐ V loops may provide clinicians with data regarding lung aeration yet do not distinguish between hyperinflation and recruitment and provide no information in regard to distribution of ventilation.46
Due to the heterogeneity of the techniques used to conduct lung recruitment it is not possible to pool the data for further analysis.
When do you recruit lungs?
Paediatric patients rely heavily upon their FRC to maintain airway and alveolar patency; this FRC steadily diminishes with the use of LPVS.6,12 During positive pressure ventilation there is an inhomogeneous distribution of gas, although the distribution of alveolar opening pressures is deemed Gaussian.9 Duff and colleagues routinely conducted lung recruitment

Page 7 of 18
Accep
ted
Man
uscr
ipt
twice daily to address the progressive de‐recruitment associated with LPVS.17 Airway pressure release, subsequent to circuit disconnection, results in a sudden and profound loss of FRC.36,42 A number of studies have been conducted in adults demonstrating the significant losses associated with circuit disconnection and the application of suction to the airways.48‐50 One paediatric study compared open and closed suction and the impact on lung volume.51 Choong and colleagues demonstrated using inductive plethysmography that the greatest loss of lung volume is related to disconnection from the circuit and subsequently recommended the use of closed suction units.51 However a number of studies have cautioned clinicians about negative pressures associated with the use of closed suction units and a reduction in secretion clearance particularly in paediatrics.52‐54 Consequently, the use of closed suction systems, at least in the paediatric population, remains questionable. In addition, saline instillation exacerbates gas maldistribution and worsens de‐ recruitment by increasing threshold opening pressures.51‐52 Recent studies measured the impact of various suctioning methods and modes of ventilation and found that irrespective of ventilation mode, or whether open or closed suctioning was used, a significant loss of FRC occurred.48‐51 In a study by Lindgren et al, FRC as measured by EIT decreased by 58±24% of baseline after disconnection of the endotracheal tube and a further 22±10% during open suction itself.50 It is probable that some form of recruitment manoeuvre may be necessary to attenuate the impact of LPVS, particularly after circuit disconnection and the application of suction.
What benefit is there to using lung recruitment?
Oxygenation
A number of studies have explored the impact of lung recruitment on oxygenation in the paediatric population. Boriosi and colleagues noted a P/F ratio increase of 53% (p< .01) in children post lung recruitment that was sustained for up to 12 hours.15‐16 Duff and colleagues found a reduced oxygen demand for up to 6 hours post a sustained inflation lung recruitment manoeuvre.17 In adults several studies have demonstrated a beneficial effect on oxygenation assuming adequate baseline PEEP is present.7,20,34,44,55
Lung volume
Both CT and EIT have been used in studies to measure lung volume post recruitment in paediatrics. A study by Wolf and colleagues uses EIT to measure the impact of a combined SI and incremental PEEP manoeuvre on end expiratory lung volume in ventilated children diagnosed with ALI.18 In their analysis they clearly identified responders and non‐responders to lung recruitment.18 The children that responded to the recruitment were characterised by resolution of atelectasis in the most dependant regions of the lungs by 17% ± 4% (p = .016) plus an improvement in compliance across all regions of the lung.18 The non‐responders had no discernable reduction in atelectasis in the most dependant regions nor did they have a significant change in compliance.18 Overdistension was problematic with the incremental PEEP manoeuvre both the responders and non –responders.18
Three studies measuring lung volume in intubated paediatrics have been performed in anaethetised children with healthy lungs. One such study demonstrated a reduction in atelectic regions when a PEEP of 5cmH2O was applied compared to zero PEEP.56 Another

Page 8 of 18
Accep
ted
Man
uscr
ipt
study measured the impact of various inspiratory pressures on atelectic regions on children undergoing a CT scan.35 They found that those children ventilated with higher pressures (30cmH20) had significantly less atelectasis than those ventilated to pressures of 25cmH2O.35 A number of adult studies have measured lung volume using either computed tomography (CT) scans or EIT. A clinical study by Dyhr and colleagues used two hyperinflations to 45cmH2O, held for 20s with an interval of 60s in patients with ARDS post‐ suctioning.
20 They found that the use of a recruitment manoeuvre, when combined with adequate ongoing PEEP, improved EELV.20 Another study by Gattinoni used CT to measure the positive gains of increased PEEP in reducing atelectic regions and that these gains correlated with oxygenation increases.57
Lung water
The ALI and ARDS lung is typically oedematous.58‐59 No studies have measured the impact of lung recruitment on total lung water volume in children however a study by Toth and colleagues in adults did conclude that improvements in oxygenation post recruitment was independent of redistribution of extravascular lung water.60 Another study demonstrated a net alveolar fluid clearance post recruitment which the authors attributed to resorption of alveolar oedema.61
Compliance
Two studies have measured the impact of lung recruitment on compliance. Morrow and colleagues found no improvement in dynamic compliance with their lung recruitment technique using an open ended anaesthetic circuit post endotracheal suctioning in infants.36 Boriosi and colleagues also found no significant change in compliance.15‐16 However, Marcus and colleagues found a 30% increase in dynamic pulmonary compliance using Ventrak software post their TRIM manouvre (p <0.01).13
Morbidity
No studies to date have measured the short or long term impact of lung recruitment on morbidity in paediatrics.
Mortality
No studies to date have measured the impact of lung recruitment on mortality in paediatrics.
What harm can lung recruitment cause?

Page 9 of 18
Accep
ted
Man
uscr
ipt
Lung recruitment is considered by some clinicians to be controversial. Concerns include the potential for barotrauma, pneumothoraces and the possible contributory factor to both VILI and ventilator associated pneumonia (VAP).12,20,36,44,60 Other concerns include the potential to impact negatively on haemodynamics and intracranial pressure.17 By increasing the intrathoracic pressure during the recruitment manoeuvre an inevitable consequence is a commiserate reduction in venous return and subsequent cardiac output. Additionally, overdistension of alveoli will increase the regional pulmonary vascular resistance and subsequently will decrease regional perfusion.13 The method of recruitment and the pressures used obviously impacts on the degree of any deleterious impact. An experimental study by Odenstedt and colleagues measured the haemodynamic and lung mechanic side effects of three different recruitment manoeuvres; a vital capacity maneuver to 40cmH2O, a pressure controlled maneuver up to 40cmH2O with a PEEP of 20cmH2O and a slow recruitment with PEEP to 15cmH2O held for 7 seconds.62 They found that the slow, lower pressure manoeuvre produced less negative lung mechanic side effects and less circulatory depression.62 The higher pressure manoeuvres produced the greatest lung expansion but the slower, lower pressure manoeuvre produced the greatest improvement in oxygenation.62 Transient reduction in cardiac output have been noted in experimental studies.39,62‐65 There is the potential that lung recruitment may contribute to the barotrauma associated with mechanical ventilation. An experimental study by Frank and colleagues determined the degree of alveolar and lung endothelial injury post a sustained inflation recruitment manoeuvre.39 While oxygenation and compliance improved with the recruitment manoeuvre those in the recruitment group did appear to have a protected endothelium but there was no reduction in alveolar epithelial injury.39 One study investigating the potential of harm of lung recruitment has been conducted in paediatrics. Halbertsma and colleagues found that a single sustained inflation recruitment manoeuvre with inspiratory pressures up to ≤45cmH2O and PEEP pressures of ≤30cmH2O translocated cytokines into the circulation.66 Translocation of bacteria has been discovered in two studies using pressures in excess of 45cmH2O.
67‐68 An adult study investigated the potential of lung recruitment manoeuvres to reduce gastric mucosal perfusion.69 Measuring gastric mucosal perfusion with laser Doppler flowmetry they found that no significant reduction in perfusion occurred during lung recruitment.69 Another study produced a marked yet transitory impairment in splanchnic circulation for up to 8 minutes post‐manoeuvre.70
Conclusion
Recruitment manoeuvres may be useful in both restoring lung volume post circuit disconnection +/‐ endotracheal suctioning but also to minimise the chronic derecruitment subsequent to LPVS although insufficient evidence exists to support it’s universal application. The various methods of recruiting lungs have as their common goal the prompt restoration of EELV to improve respiratory compliance and oxygenation and to minimise alveolar shearing and subsequent VILI. Recruitment manoeuvres appear most effective when applied following disconnection of the ETT from the circuit and following airway suctioning. Various methods of lung recruitment have been tested. The current evidence does not enable us to reach a consensus as to which method is most effective, nor which patients are most receptive to lung recruitment manoeuvres. Haphazard application of recruitment manoeuvres may cause harm and as such should be individually assessed for

Page 10 of 18
Accep
ted
Man
uscr
ipt
each patient. Whether the consistent use of recruitment manoeuvres will reduce morbidity and mortality associated with mechanical ventilation is yet to be determined. Further research on the efficacy of various recruitment methods and the timing of recruitment in paediatrics is required to inform our clinical practice.

Page 11 of 18
Accep
ted
Man
uscr
ipt
References
1. Dahlem P, van Aalderen W, Hamaker M, Kijkgraaf M, Bos A. Incidence and short‐term outcome of acute lung injury in mechanically ventilated children. European Respiratory Journal, 2003. 22: 980‐5.
2. The ARDS Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The New England Journal of Medicine, 2000. 342: 1301‐1308.
3. Artigas A, Bernard G, Carlet J, Dreyfuss D, Gattanoni L, Hudson L, et al. The American‐European Consensus Conference on ARDS, Part 2 Ventilatory, Pharmacologic, Supportive Therapy, Study design strategies and issues related to recovery and remodelling. Intensive Care Medicine, 1998. 24: 378‐398.
4. Halbertsma F, Vaneker M, Pickkers P, Hoeven J. The oxygenation ratio during mechanical ventilation in children: The role of tidal volume and positive end‐ expiratory pressure. Journal of Critical Care, 2009. 24:220‐226.
5. Moran I, Zavala E, Fernandez R, Blanch L, Mancebo J. Recruitment manoeuvres in acute lung injury/acute respiratory distress syndrome. European Respiratory Journal, 2003. 22:S42‐37s‐42s.
6. Barbas C, et al. Mechanical ventilation in acute respiratory failure: Recruitment and high positive end‐expiratory pressure are necessary. Current Opinion in Critical Care, 2005, 11(1): 18‐28.
7. Lapinsky S. Recruitment and retention of lung volume. Critical Care, 2003.7(1):9‐10.
8. Priestley M, Helfaer M. Approaches in the management of acute respiratory failure in children. Current Opinion in Pediatrics, 2004. 16(3): 293‐298.
9. Taussig L, Landau L. 1999 Pediatric Respiratory Medicine, Mosby, Le Souef.
10. Papastamelos C, Panitch H, England S, Allen L. Developmental changes in chest wall compliance in infancy and early childhood. Journal Applied Physiology, 1995. 78:179‐184.
11. Suki B. Fluctuations and Power Laws in Pulmonary Physiology. American Journal Respiratory Critical Care Medicine, 2002. 166 : 133‐137.
12. von Ungern‐Sternberg B, Regli A, Schibler A, Hammer J, Frei F, Erb T. The Impact of Positive End‐Expiratory Pressure on Functional Residual Capacity and Ventilation Homogeneity Impairment in Anesthetised Children Exposed to High Levels of Inspired Oxygen. Anesthesia Analgesia, 2007. 104 : 1364‐8.

Page 12 of 18
Accep
ted
Man
uscr
ipt
13. Marcus R, van der Walt J, Pettifer R. Pulmonary volume recruitment restores pulmonary compliance and resistance in anaesthetized young children. Paediatric Anaesthesia, 2002. 12: 579‐584.
14. Tusman G, et al. Effects of Recruitment Maneuver on atelectasis in anesthetized children. Anesthesiology, 2003. 98: 14‐22.
15. Boriosi J, et al. Efficacy and safety of lung recruitment in pediatric patients with acute lung injury. Pediatric Critical Care Medicine, 2011. 12(4): 431‐6.
16. Borisosi J, et al. Lung aeration changes after lung recruitment in children with acute lung injury. Pediatric Pulmonology, 2012. 47: 771‐779.
17. Duff J, Rosychuk R, Joffe A. The safety and efficacy of sustained inflations as a lung recruitment maneuver in pediatric intensive care unit patients. Intensive Care Medicine, 2007. 33: 1778‐1786.
18. Wolf G, et al. Reversal of dependent lung collapse predicts response to lung recruitment in children with early acute lung injury. Pediatric Critical Care Medicine, 2012. 13(5): 509‐515.
19. Wolf G, et al. Regional lung volume changes in children with acute respiratory distress syndrome during a derecruitment manoeuvre. Critical Care Medicine, 2007. 35(8): 1972‐1978.
20. Dyhr T, Bonde J, Larsson A. Lung recruitment manoeuvres are effective in regaining lung volume and oxygenation after open endotracheal suctioning in acute respiratory distress syndrome. Critical Care, 2002. 7: 55‐62.
21. Neve V, Leclerc F, Dumas de la Roque E, Leteurtre S, Riou Y. Overdistension in ventilated children. Critical Care, 2001. 5(4):196‐203.
22. Papastamelos C, Panitch H, England S, Allen J. Developmental changes in chest wall compliance in infancy and early childhood. Journal of Applied Physiology, 1995. 78(1): 179‐184.
23. Carvalho A, Jandre F, Pino A, Bozza F, Salluh J, Rodrigues R, et al. Positive end‐ expiratory pressure at minimal respiratory elastance represents the best compromise between mechanical stress and lung aeration in oleic acid induced lung injury. Critical Care, 2007. 11(R86).
24. Grasso S, et al. Effects of recruiting maneuvers in patients with acute respiratory distress syndrome ventilated with protective ventilatory strategy. Anaesthesiology, 2002. 96:795‐802.
25. The ARDS Network. Effects of recruitment maneuvers in patients with acute lung injury and acute respiratory distress syndrome ventilated with high positive end‐expiratory pressure. Critical Care Medicine, 2003. 31(11): 2592‐2597.

Page 13 of 18
Accep
ted
Man
uscr
ipt
26. Halter J, et al. Effect of positive end‐expiratory pressure and tidal volume on lung injury induced by alveolar instability. Critical Care, 2007. 11(1).
27. Lim S‐C, et al. Intercomparison of recruitment maneuver efficacy in three models of acute lung injury. Critical Care Medicine, 2004. 32(12): 2371‐2377.
28. Gattinoni L, D’Andrea L, Pelosi P, Vitale G, Pesenti A, Fumagalli R. Regional effects and mechanism of positive end‐expiratory pressure in early adult respiratory distress syndrome. Journal of American Medical Association, 1993. 269(16): 2122‐2127.
29. Papadakos P, Lachmann B. The Open Lung Concept of Mechanical Ventilation: The role of Recruitment and Stabilization. Critical Care Clinics, 2007. 23(2) :241‐250.
30. Rimensberger P, Pache J, mcDerlie C, Frndova H, Cox P. Lung recruitment and lung volume maintenance: a strategy for improving oxygenation and preventing lung injury during both conventional mechanical ventilation and high‐frequency oscillation. Intensive Care Medicine, 2000. 26: 745‐755.
31. Tusman G, Bohm S, Suarezz‐Sipmanet F, Turchetto E. Lung recruitment improves the efficiency of ventilation and gas exchange during one‐lung ventilation anesthesia. Anesthesia Analgesia, 2004. 98: 1604‐9.
32. Povoa P, Almeida E, Fernandes A, Mealha R, Moreira P, Sabino H. Evaluation of a recruitment maneuver with positive inspiratory pressure and high PEEP in patients with severe ARDS. Acta Anaesthesiology Scandinavica, 2004. 48(3):287‐93.
33. Borges J, Okomoto V, Matos G, Caramez M, Arantas P, Barros F et al. Reversibility of lung collapse and Hypoxemia in Early Acute Respiratory Distress Syndrome. American Journal Respiratory Critical Care Medicine, 2006. 174: 268‐278.
34. Dyhr T, Nygard e, Laursen N, Larsson A. Both lung recruitment maneuver and PEEP are needed to increase oxygenation and lung volume after cardiac surgery. Acta Anaesthesiology Scandinavica, 2004. 48(2): 187‐197.
35. Sargent M, Jamieson D, McEachern A, Blackstock D. Increased inspiratory pressure for reduction of atelectasis in children anesthetized for CT scan. Pediatrics Radiology, 2002. 32:344‐7.
36. Morrow B, Futter M, Argent A. A recruitment manoeuvre performed after endotracheal suction does not increase dynamic compliance in ventilated paediatric patients: a randomised controlled trial. Australian Journal of Physiotherapy, 2007. 53: 163‐169.
37. Tugrul S, et al. Effects of sustained inflation and postinflation positive end‐ expiratory pressure in acute respiratory distress syndrome: focusing on pulmonary and extrapulmonary forms. Critical Care Medicine, 2003. 31: 974‐6.

Page 14 of 18
Accep
ted
Man
uscr
ipt
38. Almgren B, Wickerts C.‐J.. Hogman M. Post‐suction Recruitment Manoeuvre Restores Lung Function in Healthy, Anaesthetized Pigs. Anaesthesia and Intensive Care, 2004. 32(3): 339‐345.
39. Frank J, Matthay M. Mechanisms of ventilator‐induced injury. Critical Care, 2002. 7: 233‐241.
40. Henzler D, Hochhausen N, Dembinski R, Orfao S, Rossaint R, Kuhlen R. Parameters derived from the pulmonary pressure‐volume curve, but not the pressure‐time curve, indicate recruitment in experimental lung injury. Anaesthesia & Analgesia, 2007. 105(4): 1072‐1078.
41. Rothen H., Neumann P, Berglund JE, Valtysson J, Magnusson A, Hedenstierna G. Dynamics of re‐expansion of atelectasis during general anaesthesia. British Journal of Anaesthesia, 1999. 82(4): 551‐557.
42. Lindgren S, Odenstedt H, Olegard C, Sondergaard S, Lundin S, Stenqvsit O. Regional lung derecruitment after endotracheal suction during volume‐ or pressure‐controlled ventilation: a study using electric impedance tomography. Intensive Care Medicine, 2007. 33(1): 172‐180.
43. Pestana D, Hernandez‐Gancedo, Royo C, Perez‐Chrzanowska Criado A. Pressure‐volume curve variations after a recruitment manoeuvre in acute lung injury/ARDS patients: implications for the understanding of the inflection points of the curve. European Journal of Anaesthesiology, 2005. 22: 175‐180.
44. Lapinsky S, Aubin M, Mehta S, Boiteau P, Slutsky A. Safety and efficacy of a sustained inflation for alveolar recruitment in adults with respiratory failure. Intensive Care Medicine, 1999. 25(11): 1297‐1301.
45. Syring R, Otto C, Spivack R, Markstaller K, Baumgardner J. Maintenance of end‐expiratory recruitment with increased respiratory rate after saline‐lavage lung injury. Journal Applied Physiology, 2007. 102: 331‐339.
46. Maggiore S, Richard J‐C., Brochard L. What has been learnt from P/V curves in patients with acute lung injury/acute respiratory distress syndrome? European Respiratory Journal, 2003. 22: Suppl. 42, 22s‐26s.
47. Henzler D, Mahnken A, Dembinski r, Waskowiak B, rossaint R, Kuhlen R. Repeated generation of the pulmonary pressure‐volume curve may lead to derecruitment in experimental lung injury. Intensive Care Medicine, 2005. 31(2):302‐310.
48. Heinze H, Sedemund‐Adib B, Herinlake M, Gosch U, Eichler W. Functional Residual Capacity changes after different endotracheal suctioning methods. Anesthesia Analgesia, 2008. 107(3): 941‐44.
49. Cereda M, Villa F, Colombo E, Greco G, Nacoto M, Pesenti A. Closed system endotracheal suctioning maintains lung volume during volume‐controlled mechanical ventilation. Intensive Care Medicine, 2001. 27: 648‐654.

Page 15 of 18
Accep
ted
Man
uscr
ipt
50. Lindgren S, et al. Effectiveness and side effects of closed and open suctioning: an experimental evaluation. Intensive Care Medicine, 2004. 30: 1630‐1637.
51. Choong K, Chatrkaw P, Frndova H, Cox P. Comparison of loss in lung volume with open versus in‐line catheter endotracheal suctioning. Paediatric Critical Care Medicine, 2003. 4: 69‐73.
52. Stenqvist O, Lindgren S, Karason S, Sondergaard S, Lundin S. Warning! Suctioning. A lung model evaluation of closed suctioning systems. Acta Anaesthesiology Scandinavica, 2001. 45: 167‐172.
53. Copnell B, et al. A comparison of the effectiveness of open and closed endotracheal suction. Intensive Care Medicine, 2007. 33(9): 1655‐1662.
54. Kiraly N, Tingay D, Mills F, Morley C, Copnell B. Negative tracheal pressure during neonatal endotracheal suction. Pediatric Research, 2008. 64: 29‐33.
55. Schreiter D, et al. Alveolar recruitment in combination with sufficient positive end‐expiratory pressure increases oxygenation and lung aeration in patients with severe chest trauma. Critical Care Medicine, 2004. 32(4): 968‐975.
56. Serafini G, et al. Pulmonary atelectasis during paediatric anaesthesia: CT scan evaluation and effect of positive endexpiratory pressure (PEEP). Pediatric Anesthesia, 1999. 9(3): 225‐228.
57. Gattinoni L, et al. Relationships between lung computed tomographic density, gas exchange, and PEEP in acute respiratory failure. Anesthesiology, 1988. 69:824‐832.
58. Sibbard W, et al. Thermal dye measurements of extravascular lung water in critically ill patients. Intravascular Starling forces and extravascular lung water in the adult respiratory distress syndrome. Chest, 1985. 87: 585‐592.
59. Kirov M, et al. Extravascular lung water assessed by transpulmonary single thermodilution and post‐mortem gravimetry in sheep. Critical Care, 2004. 8:R451‐R458.
60. Toth I, et al. Hemodynamic and respiratory changes during lung recruitment and descending optimal positive end‐expiratory pressure titration in patients with Acute Respiratory Distress Syndrome. Critical Care Medicine, 2007. 35(3):787‐793.
61. Constantin J‐M, et al. Response to recruitment maneuver influences net alveolar fluid clearance in acute respiratory distress syndrome. Anesthesiology, 2007.106(5): 944‐951.
62. Odenstedt H, et al. Slow moderate pressure recruitment maneuver minimizes negative circulatory and lung mechanic side effects: evaluation of recruitment maneuvers using electric impedance tomography. Intensive Care Medicine, 2005. 31: 1706‐1714.

Page 16 of 18
Accep
ted
Man
uscr
ipt
63. Hansen L, et al. Selective recruitment maneuvers for lobar atelectasis: effects on lung function and central hemodynamics: An experimental study in pigs. Anesthesia and Analgesia, 2006. 102:1504‐10.
64. Lim S‐C, et al. Transient hemodynamic effects of recruitment maneuvers in three experimental models of acute lung injury. Critical Care Medicine, 2004. 32(12):2378‐2384.
65. Nielsen J, et al. Central hemodynamics during lung recruitment maneuvers at hypovolemia, normovolemia and hypervolemia. A study by echocardiography and continuous pulmonary artery flow measurements in lung‐injured pigs. Intensive Care Medicine, 2006. 32: 585‐594.
66. Halbertsma F, et al. A single recruitment maneuver in ventilated critically ill children can translocate pulmonary cytokines into the circulation. Journal of Critical Care, 2010, 25:10‐15.
67. Verbrugge S, et al. Lung overinflation without positive end‐expiratory pressure promotes bacteremia after experimental Klebsiella pneumonieae inoculation. Intensive Care Medicine, 1998. 24:172‐7.
68. Tremblay L, Valenza F, Ribeiro S, Li J, Slutsky S. Injurious ventilatory strategies increase cytokines and c‐fos m‐RNA expression in an isolated rat lung model. Journal Clinical Investigation, 1997. 99: 944‐952.
69. Claesson J, Lehtipalo S, Winso O. Do lung recruitment maneuvers decrease gastric mucosal perfusion? Intensive Care Medicine, 2003. 29(3): 1314‐1321.
70. Nunes S, Rothen H, Brander L, Takala J, Jakob S. Changes in splanchnic circulation during an alveolar recruitment maneuver in healthy porcine lungs. Anesthesia Analgesia, 2004. 98: 1432‐8.
Page 17 of 18
Accep
ted
Man
uscr
ipt
Author Subjects Method of
recruitment
Outcome
measures
Results
Boriosi et al.
2011 15
Age yrs 4.8 (1-14)
ALI/ARDS
n=21
Established Cdyn
Incremental and
decremental PEEP via
ventilator (Servo-I) in
Assist Control/Pressure
Control mode using Open
Lung Tool (OLT)
PaO2
PaCO2
-Improved P/F ratio for
up to 12 hours post
recruitment
-Nil adverse events
Boriosi et al.
2012 16
Age yrs 2.5 (0.5-14)
Nested study of ALI
patients from their
2011 study
n=6
Established Cdyn
Incremental and
decremental PEEP via
ventilator (Servo-I) in
Assist Control/Pressure
Control mode using Open
Lung Tool (OLT)
End expiratory
lung (EEL) levels as
measured by
Computed
Tomography (CT)
scan
Oxygenation
-Increase in EEL post
RM 3%-72% median
20% (IQR 6, 47)
-Reduction in PIP post
RM by -14% (IQR -18, -
12)
-Improved P/F ratios
Duff et al.
2007 17
Age months 16
(11days to 14
years)
Lung disease
status: from
healthy lungs
through to ARDS
n=32
SI of 30-40cmH2O
for 15-20secs post
circuit interruption,
suctioning, hypoxia or
routinely every
12hours
Oxygenation as
measured by P/F
or S/F ratios
Haemodynamic
markers
Safety
-Improved
oxygenation post
recruitment for up to 4
hours
-Safe in children
-Spikes in ICP in some
children
Halbertsma et
al.
2010 66
Age months 0.5-
4.5
n= 7
Single recruitment
manoeuvre – incremental
increases in PIP and PEEP
until transcutaneous SaO2
98%.
Max PEEP 30cmH2O Max
PIP 45cmH2O
Translocation of
pulmonary
cytokines
Oxygenation Lung
kinetics
-Plasma levels of
cytokines increased
post recruitment
-No increase inTcSaO2
noted in 5/7 patients
-haemodynamic
compromise in 2/7
patients
Table

Page 18 of 18
Accep
ted
Man
uscr
ipt
Tusman
2003 14
Age months 6-72
Children
undergoing
scheduled cranial
MRI
n=24
Manual SI to
40cmH2O + PEEP of
15cmH2O for 10 breaths
Compared to 5cm H2O of
PEEP alone and zero PEEP
% of atelectic
regions as
measured by MRI
- Children in the
recruitment group had
significantly less
atelectic regions
compared to those
managed with PEEP
alone or zero PEEP
Marcus et al.
2002 13
Age < 24 months
Children
undergoing
scheduled general
anaesthesia
n=20
Timed re-expansion
inspiratory manoeuvre =
30cmH2O CPAP for 10
seconds
Dynamic
compliance
Airway resistance
-TRIM maneuver
resulted in improved
dynamic compliance
-Airway resistance
changes insignificant
Morrow et al.
2007 36
Age yrs <1
n=48
SI up to 30cmH2O for 30
seconds using an
anaesthetic bagging circuit
post ETT suctioning
Dynamic
compliance
Oxygenation
Nil difference
between experimental
and control groups in
terms of oxygen
saturations or dynamic
compliance
Wolf et al.
2012 18
Age yrs 9.9 ± 4.2
ALI
n=10
Sustained inflation to
40cmH2O for 40 secs
using CPAP mode followed
by a stepwise RM,
escalating plateau
pressures by 5cmH2O
every 15mins
Regional
atelectasis, lung
compliance and
regional
overdistension as
measured by EIT
-small decrease in
reversible atelectasis
post SI RM
-physiological lung
recruitment achieved
in responders during
the stepwise
manoeuvre
-lung overdistension
proximally





























