-
Official reprint from UpToDatewww.uptodate.com 2015 UpToDate
AuthorsSassan Pazirandeh, MDClifford W Lo, MD, MPH, ScDDavid L
Burns, MD
Section EditorTimothy O Lipman, MD
Deputy EditorAlison G Hoppin, MD
Overview of water-soluble vitamins
All topics are updated as new evidence becomes available and our
peer review process is complete.Literature review current through:
Feb 2015. | This topic last updated: Sep 24, 2014.
INTRODUCTION Vitamins are a number of chemically unrelated
families of organic substances thatcannot be synthesized by humans
but need to be ingested in the diet in small quantities to prevent
disordersof metabolism. They are divided into water-soluble and
fat-soluble vitamins (table 1).
Many of the vitamin deficiency diseases, such as rickets
(vitamin D), scurvy (vitamin C), beriberi (thiamine),and pellagra
(niacin), have been almost completely eliminated in developed
countries. Great interest andcontroversy continues into whether
vitamin supplementation can prevent cancer, heart disease,
upperrespiratory infections, and other common diseases. (See
"Vitamin supplementation in disease prevention".)
The best dietary sources for most of the water-soluble vitamins
are fruits and vegetables; these also containmany related
substances such as flavins and carotenoids which are generally not
recognized as vitamins butmay have protective effects against
various diseases. This topic review will focus on the
water-solublevitamins excluding folic acid and vitamin B12, which
are discussed separately. (See "Etiology and clinicalmanifestations
of vitamin B12 and folate deficiency".)
Minerals and fat-soluble vitamins are also reviewed elsewhere.
(See "Overview of vitamin A" and "Overviewof vitamin D" and
"Overview of vitamin E" and "Overview of vitamin K" and "Overview
of dietary traceminerals".)
DEFINITIONS Several systems have been used to describe
nutritional requirements of a population.Dietary Reference Intakes
(DRIs) were developed by the Food and Nutrition Board of the
Institute ofMedicine to guide nutrient intake in a variety of
settings. Under this system, requirements can be expressedas a
Recommended Dietary Allowance (RDA), which is defined as the
dietary intake that is sufficient to meetthe daily nutrient
requirements of 97 percent of the individuals in a specific life
stage group. If there isinsufficient data to determine an RDA for a
given nutrient, requirements can be expressed as an AdequateIntake
(AI), which is an estimation of the nutrient intake necessary to
maintain a healthy state. These termsare described in greater
detail in a separate topic review. (See "Dietary history and
recommended dietaryintake in children".)
VITAMIN B1 (THIAMINE) Thiamine, first named "the antiberiberi
factor" in 1926, has a historical valuedue to the very early
description of Beriberi in the Chinese medical texts, as far back
as 2697 BC [1].Formerly known as vitamin B1, thiamine is soluble in
water and partly soluble in alcohol. Thiamine consistsof a
pyrimidine and a thiazole moiety, both of which are essential for
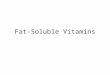
its activity (figure 1).
Sources Thiamine is found in larger quantities in food products
such as yeast, legumes, pork, rice, andcereals. Milk products,
fruits, and vegetables are poor sources of thiamine [1]. The
thiamine molecule isdenatured at high pH and high temperatures.
Hence, cooking, baking, and canning of some foods as well
aspasteurization can destroy thiamine [2].
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
1 de 32 3/7/15, 10:20 AM
-
Metabolism Thiamine is absorbed in the small intestine via both
passive diffusion and active transport.The maximal absorption of
thiamine is in the jejunum and ileum [3]. Thiamine passes through
the mucosalcells to enter the blood stream via a sodium and ATP
dependent pump. Bound to albumin, it is carried by theportal
circulation to the liver. Thiamine enters the red blood cells by
passive diffusion while its entry into othercells is via an active
energy requiring process [3]. The highest concentrations are found
in the skeletalmuscles, the liver, the heart, the kidneys, and the
brain. Thiamine's biologic half-life is approximately 10 to20 days;
due to limited tissue storage, continuous supplementation is
required [3]. Through a series ofmetabolic processes, thiamine is
incorporated into many phosphorylated esters, including
thiaminepyrophosphate (TPP) and thiamine monophosphate (TMP).
Thiamine and all of its metabolites are excretedin the urine.
Biliary excretion is a minor route of its homeostasis [4].
Actions Thiamine is an important cofactor for enzymes involved
in amino-acid and carbohydratemetabolism. Functioning along with
many coenzymes such as flavin and NAD, thiamine serves as a
catalystin the conversion of pyruvate to acetyl CoA, an oxidative
decarboxylation reaction mediated by pyruvatedehydrogenase:
Pyruvate + CoA + NAD Acetyl CoA + CO2 + NADH + H
Thiamine is also involved in many other cellular metabolic
activities such as the transketolation of thepentose phosphate
pathway [3]. Thiamine has a role in the initiation of nerve impulse
propagation that isindependent of its coenzyme functions [3].
Deficiency Thiamine deficiency can be assessed by measuring the
blood thiamine concentration,erythrocyte thiamine transketolase
(ETKA), or transketolase urinary thiamine excretion (with or
without a 5mg thiamine load) [5]. Most laboratories now measure
blood thiamine concentration directly, in preference tothe ETKA
method [6]. The ETKA method is a functional test and results are
influenced by the hemoglobinconcentration.
Thiamine deficiency has been associated with three
disorders:
Infantile beriberi Beriberi in infants becomes clinically
apparent between the ages of two and threemonths. The clinical
features are variable and may include a fulminant cardiac syndrome
with cardiomegaly,tachycardia, a loud piercing cry, cyanosis,
dyspnea, and vomiting [7]. A form of aseptic meningitis has
alsobeen described in which the affected infants exhibit vomiting,
nystagmus, purposeless movements, andseizure, despite a "normal"
cerebrospinal fluid [8].
In 2003, infantile beriberi was discovered in a series of
infants in Israel, due to feeding with a soy-basedformula that was
inadvertently deficient in thiamine [9]. Most of the infants with
severe symptoms at the timeof diagnosis, which included
cardiomyopathy and seizures, had severe permanent disabilities even
afterthiamine was replaced. Among infants with apnea or seizures at
presentation, all had moderate or severeintellectual disability
when reevaluated five and ten years later, and most had chronic
epilepsy [10,11]. A fewof the severely affected infants died. Many
other infants were asymptomatic or had nonspecific symptomswhile
being fed the thiamine-deficient diet (eg, vomiting, irritability
or failure to thrive). However, follow-uptesting revealed delays in
language and motor development [12].
Adult beriberi Adult beriberi is described as dry or wet. Dry
beriberi is the development of a
Beriberi (infantile and adult)Wernicke-Korsakoff syndromeLeigh's
syndrome
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
2 de 32 3/7/15, 10:20 AM
-
symmetrical peripheral neuropathy characterized by both sensory
and motor impairments, mostly of thedistal extremities. Wet
beriberi includes a neuropathy, as well as signs of cardiac
involvement withcardiomegaly, cardiomyopathy, congestive heart
failure, peripheral edema, and tachycardia [1].
Beriberi has been reported as a complication of weight loss
surgery, presenting as a polyneuropathy with aburning sensation in
the extremities, weakness, and falls [13-15]. Several of the case
reports have been inadolescents, but whether this nutritional
complication is more common in the adolescent age group ascompared
to adults undergoing weight loss surgery has not been established.
(See "Surgical managementof severe obesity in adolescents".)
Thiamine deficiency can occur as a complication of total
parenteral nutrition if adequate thiaminesupplements are not
provided. As an example, during the late 1990s, there were multiple
reports ofsymptomatic thiamine deficiency among recipients of
parenteral nutrition during a widespread shortage ofparenteral
multivitamins in the United States [16].
A number of studies have suggested that patients with heart
failure, especially those treated with loopdiuretics, may be
thiamine deficient and should be treated with 50 to 200 mg of
thiamine per day [17-19].However, this remains controversial
because of questions involving assay validity and a lack of
controlledtrials [20]. (See "Causes of dilated
cardiomyopathy".)
Wernicke-Korsakoff syndrome Wernicke-Korsakoff syndrome is the
best known neurologiccomplication of thiamine (vitamin B1)
deficiency. The term refers to two different syndromes,
eachrepresenting a different stage of the disease. Wernicke's
encephalopathy (WE) is an acute syndromerequiring emergent
treatment to prevent death and neurologic morbidity. Korsakoff's
syndrome (KS) refers toa chronic neurologic condition that usually
occurs as a consequence of WE. It is characterized by
impairedshort-term memory and confabulation with otherwise grossly
normal cognition. (See "Overview of the chronicneurologic
complications of alcohol", section on 'Korsakoff syndrome'.)
WE is a triad of nystagmus, ophthalmoplegia, and ataxia, along
with confusion. This combination is almostexclusively described in
chronic alcoholics with thiamine deficiency. The two entities are
not separatediseases, but a spectrum of signs and symptoms. There
may be a genetic predisposition for thedevelopment of WE since not
all thiamine deficient patients are affected. Impairment in the
synthesis of oneof the important enzymes of the pentose phosphate
pathway (erythrocyte transketolase) may explain such
apredisposition [21]. (See "Wernicke encephalopathy".)
WE is treated with thiamine supplementation. A range of
replacement doses have been used successfully,but large doses are
typically used because they appear to be safe. It is common
practice to delay givingdextrose to alcoholic patients until
thiamine supplementation has been initiated to avoid
precipitatingWernicke's encephalopathy. (See "Wernicke
encephalopathy", section on 'Treatment'.)
Leigh syndrome Thiamine deficiency has occasionally been
reported in infants presenting withfeatures of Leigh syndrome, a
progressive subacute necrotizing encephalomyopathy. This is a
sporadicmitochondrial disorder with a subacute neurologic course.
It is manifested with ataxia, dysarthria, movementdisorders,
areflexia, muscle atrophy, and weakness. (See "Hereditary
neuropathies associated withgeneralized disorders", section on
'Leigh syndrome'.)
Toxicity No real syndrome of excess thiamine exists since the
kidneys can rapidly clear almost all excessthiamine [22]. Its
half-life is 9.5 to 18.5 days.
Requirements The RDA for thiamine in the United States is 1.2 mg
daily for adult men and 1.1 mg dailyfor adult women (about 0.5
mg/1000 kcal), and 1.4 mg/day during pregnancy and lactation (table
2) [23].
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
3 de 32 3/7/15, 10:20 AM
-
Thiamine can be administered via intravenous and intramuscular
routes. For the treatment of patients withberiberi, the daily doses
range from 50 to 100 mg for 7 to 14 days. Then an oral dose of 10
mg per day isgiven until full recovery is achieved [1].
VITAMIN B2 (RIBOFLAVIN) Vitamin B2, or riboflavin, is a member
of naturally occurring compoundsknown as flavins. Flavins have a
critical role in numerous biochemical reactions. First identified
in the early1900s, riboflavin was isolated in 1935 [24].
Sources Riboflavin is supplied in many foods, including meats,
fish, eggs and milk, green vegetables,yeast, and enriched
foods.
Chemistry Riboflavin's chemical nomenclature is 7,8-dimethyl-10
(1'-D-ribityl) isoalloxazine (figure 1). Inthe free form, it is a
base, but in nature and in vivo, it is mostly found as a component
of flavin-adeninedinucleotide (FAD). The 5'-hydroxymethyl terminus
of the vitamin is phosphorylated to form a phosphateester, allowing
it to be incorporated into a different coenzyme [25].
Metabolism Dietary flavins are bound to albumin and other
riboflavin-specific carrier proteins and arereleased from their
protein-bound state via gastric acid and proteolytic enzymes [26].
In the proximal smallintestine, riboflavin is absorbed passively
along its concentration gradient across the intestinal mucosa.
Thisinvolves a saturable transport system that is passive and not
sodium dependent [27]. There also appears tobe some enterohepatic
circulation for riboflavin facilitated by bile salts [26].
Riboflavin eventually reaches thehepatocytes where its metabolism
into flavin mononucleotide (FMN) and flavin-adenine dinucleotide
(FAD)takes place.
The metabolic conversions of flavin take place in the cytoplasm
of cells of the body, particularly in the liver,heart, and kidney
[25]. Riboflavin is first phosphorylated to form FMN, which can
either be furtherphosphorylated into FAD, or become incorporated as
part of a certain coenzyme-flavin complex. Both of
thephosphorylation reactions are ATP dependent. As the more common
form of flavin in humans, FAD is oftencomplexed with other proteins
to form flavoproteins with oxidizing and hydrogenating abilities
[26]. Most ofthe riboflavin stores in the body are in the forms of
flavoproteins. Urinary levels of the vitamin only indirectlyreflect
dietary intake or riboflavin catabolism [28].
Actions Riboflavin is an essential component of coenzymes
involved in multiple cellular metabolicpathways, including the
energy producing respiratory pathways. Flavoproteins are catalysts
in a number ofmitochondrial oxidative and reductive reactions and
function as electron transporters [25].
Deficiency Riboflavin deficiency is more common than generally
appreciated. Many cases areundetected due to the mild nature and
nonspecific signs and symptoms of deficiency. Plasma
riboflavinconcentrations tend to reflect recent dietary intake.
Urinary riboflavin excretion and the erythrocyteglutathione
reductase assay are better functional indices of riboflavin
deficiency.
Significant deficiency syndromes are characterized by sore
throat, hyperemia of pharyngeal mucousmembranes, edema of mucous
membranes, cheilitis, stomatitis, glossitis (picture 1),
normocytic-normochromic anemia, and seborrheic dermatitis [28].
Whether all these changes are due to riboflavindeficiency is not
always clear since riboflavin deficiency is often accompanied by
other water-soluble vitamindeficiencies, which can cause similar
symptoms (table 3) [29]. Pure deficiency of riboflavin is rare,
althoughit has been described in areas of the third world where
starvation is prevalent and access to food is limited.Other
settings in which riboflavin deficiency may be noted include:
Patients with anorexia nervosa
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
4 de 32 3/7/15, 10:20 AM
-
Toxicity Excessive amounts of riboflavin are usually not
absorbed due to the limited water-solubility andthe inability of
the human gastrointestinal tract to absorb toxic doses of the
compound [25].
Requirements The RDA for riboflavin is 1.3 mg daily for adult
men and 1.1 mg daily for adult women(about 0.6 mg per 1000 kcal);
requirements rise to 1.4 mg daily during pregnancy and 1.6 mg daily
duringlactation (table 2) [23,32].
Some intramitochondrial beta-oxidation defects may respond to
riboflavin therapy. (See "Metabolicmyopathies caused by disorders
of lipid and purine metabolism".) In addition, patients with HIV
infection whoare treated with zidovudine or stavudine may develop
lactic acidosis that is reversed by riboflavin therapy[33]. (See
"Electrolyte disturbances with HIV infection".)
VITAMIN B3 (NIACIN) Pellagra (meaning "raw skin") was first
described in Spain and Italy in the mid 18thcentury. It is
characterized by a photosensitive pigmented dermatitis (typically
located in sun-exposedareas), diarrhea, and dementia. During the
early 1900s, pellagra was epidemic amongst the corn
eatingpopulation of southeastern United States. Pellagra is now
extremely uncommon in the western world exceptas a complication of
alcoholism, anorexia nervosa, or malabsorptive disease. Pellagra
due to dietarydeficiency can still be seen in India, in parts of
China, and Africa.
For centuries since its first description in 1735 by Spanish
physician Casal, it was thought to be an infectiousdisease [34].
However, in 1937, Elvehjen and his colleagues discovered that
nicotinic acid was effective inthe treatment of pellagra in dogs.
In the 1950s, tryptophan, a precursor of niacin, replaced it in the
treatmentof pellagra and research connected the low source of
niacin and tryptophan in corn-containing foods to thedevelopment of
pellagra [35]. Niacin had been isolated since 1867, but it was not
until 1937 that it becameknown as the anti-pellagra factor
[34].
Sources Niacin is widely distributed in plant and animal foods.
Good sources include yeast, meats(especially liver), cereals,
legumes, and seeds. It is theoretically possible to maintain
adequate niacin statuson a high protein diet of 100 g/day since
tryptophan can be converted to a niacin derivative in the
liver.
Chemistry Nicotinic acid and nicotinamide are the two common
forms of the vitamin most often referredto as niacin (figure 2).
Through a series of biochemical reactions in the mitochondria,
niacin, nicotinamide,and tryptophan form nicotinamide adenine
dinucleotide (NAD) and NAD phosphate (NADP). NAD and NADPare the
active forms of niacin.
Metabolism As the chief dietary forms of niacin, NAD and NADP
are first hydrolyzed in the intestinallumen by enzymes leading to
nicotinamide. Nicotinamide is converted by intestinal flora to
nicotinic acid. Thetwo forms of niacin are then absorbed and
released into plasma via passive and facilitated diffusion
[36].Through a passive process, niacin is rapidly taken up by the
liver, kidneys, and erythrocytes. Intracellularnicotinamide and
nicotinic acid are quickly converted to coenzyme forms NAD and
NADP, which are storedin tissues with high metabolic activities
(ie, muscle and liver).
Individuals who avoid dairy products (such as people with
lactose intolerance) since dairy products area good source of
riboflavin
Patients with malabsorptive syndromes such as celiac sprue,
malignancies, and short bowel syndrome
Rare inborn errors of metabolism in which there is a defect in
riboflavin synthesis [30]
Long-term use of phenobarbital and other barbiturates, which may
lead to oxidation of riboflavin andimpair its function [31]
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
5 de 32 3/7/15, 10:20 AM
-
Actions Many enzymatic reactions depend upon NAD and NADP. The
role of the niacin moiety is toaccept electrons or to donate
hydrogen ions. The majority of these NAD-dependent enzymes are
involved inreactions such as oxidation of fatty acids and other
reactions that yield chemical structures containing highenergy
bonds [37]. NADP is a cofactor in the reductive synthesis of the
fatty acids and steroids. As essentialcomponents of redox reactions
and hydrogen transport, NAD and NADP are crucial in the synthesis
andmetabolism of carbohydrates, fatty acids, and proteins [37].
Deficiency
Pellagra As mentioned above, pellagra is a rare entity in the
United States, but is still a commonmanifestation of niacin
deficiency in poorer countries where the local diet consists of
cereal, corn, orsorghum. In industrialized countries, pellagra
tends to occur in alcoholics, and has been reported as
acomplication of bariatric surgery or anorexia nervosa [38,39].
The most characteristic finding is the presence of a symmetric
hyperpigmented rash, similar in color to asunburn, which is present
in the exposed areas of skin (picture 2) [37]. Other clinical
findings are a redtongue and many non-specific symptoms, such as
diarrhea and vomiting. Neurologic symptoms includeinsomnia,
anxiety, disorientation, delusions, dementia, and
encephalopathy.
Niacin deficiency can also be seen in three other settings:
Toxicity The most documented and best known side effect of
niacin is the flushing reaction associatedwith the crystalline
nicotinic acid and not nicotinamide [43]. Symptoms are
dose-dependent yet variable fromperson to person. The flushing can
be experienced in a mild form while taking doses as small as 10 mg
perday [44]. Despite the inconvenience and the undesirability of
the reactions, there are no serious sequelaefrom flushing [43].
In pharmacological doses (eg, 1000 to 3000 mg/day), common side
effects of niacin are flushing, nausea,vomiting, pruritus, hives,
elevation in serum aminotransferases [45], and constipation. A
niacin-inducedmyopathy has also been described [46]. Caution should
be used in patients with a history of gout, sinceniacin is also
known to elevate serum uric acid concentration.
Severe toxicity reactions are reported in doses of 2 to 6 grams
per day [44]. At such high doses, the hepatic
Carcinoid syndrome, in which metabolism of tryptophan is to 5-OH
tryptophan and serotonin ratherthan to nicotinic acid. This leads
to the deficiency of active forms of niacin and the development
ofpellagra. (See "Clinical features of the carcinoid
syndrome".)
Prolonged use of isoniazid, since isoniazid depletes stores of
pyridoxal phosphate, which enhances theproduction of tryptophan, a
precursor of niacin. Several other drugs induce niacin deficiency
byinhibiting the conversion of tryptophan to niacin, including
5-fluorouracil, pyrazinamide,6-mercaptopurine, hydantoin,
ethionamide, phenobarbital, azathioprine, and chloramphenicol
[40].
Hartnup disease (MIM #234500), an autosomal recessive congenital
disorder [41]. Hartnup disease isassociated with a defect of a
membrane transport in the intestinal and renal cells normally
responsiblefor the absorption of tryptophan (one of the precursors
of nicotinamide-adenine dinucleotide). Throughthis pathway, around
50 percent of the daily niacin needs are synthesized. Due to the
resulting niacindeficiency, all the symptoms of pellagra can be
expected. The diagnosis is made by detecting anumber of neutral
amino acids in the urine, something that is not seen with dietary
pellagra. Thetreatment is aimed towards depleting stores and
supplementing the diet with niacin as well as proteinsand amino
acids [42]. (See "Overview of the hereditary ataxias", section on
'Aminoacidurias'.)
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
6 de 32 3/7/15, 10:20 AM
-
metabolism becomes saturated, and side effects of this drug can
be more frequently encountered. Whenless than 1 g of nicotinic acid
was ingested per day, only a handful of anecdotal cases of toxicity
has beenreported in the literature [47]. One clinical trial
assigned two groups of subjects to either a long or a short-acting
formula of niacin, each starting at 500 mg per day [48]. Subjects
were followed for several monthsduring which the dose of niacin was
raised every six weeks by about 500 mg. There was no
gastrointestinalor liver toxicity below 1000 mg of niacin per day.
The extent of the toxicity was minimal and mostlygastrointestinal
in the immediate release group, while mild liver enzyme elevation
was noticed only in theslow release group [48]. There is some
speculation that the metabolites of nicotinic acid in these
highconcentrations may lead to growth retardation in infants and
children [49].
Therapeutic roles In moderate to high doses (1 to 3 grams a day)
niacin is a well-establishedantihyperlipidemic agent, decreasing
total and LDL cholesterol [50]. The
Cholesterol-LoweringAtherosclerosis Study (CLAS II and II), for
example, showed that a combination of niacin and
colestipolsignificantly reduced the progression of atherosclerotic
related coronary artery complications (52 versus 15percent in the
control group). (See "Lipid lowering with drugs other than statins
and fibrates".) To reduce theflushing side effects, a
sustained-release formulation is available for these purposes.
However, these longeracting forms may be associated with more
gastrointestinal and hepatotoxic side effects [35]. Lower
startingdoses of crystalline niacin or premedication of the
patients with aspirin can attenuate these adverse effectsand side
effects. A more recent clinical role for nicotinic acid given in
high doses has been suggested fordelaying the onset of diabetes in
children [51].
Requirements The RDA for Niacin is 16 NEs (Niacin Equivalents)
daily for adult males, and 14 NEs dailyfor adult females, rising to
18 NE during pregnancy, and 17 NE daily during lactation (table 2)
[23]. One NEis equal to 1 mg of niacin, which is equal to 60 mg of
dietary tryptophan. These doses are far below
theanti-hyperlipidemic doses of niacin and are not associated with
toxicity. Requirements may be increased forindividuals on dialysis,
or for those with malabsorptive processes (eg, after bariatric
surgery, as discussedabove).
VITAMIN B5 (PANTOTHENIC ACID) Pantothenic acid (PA) was first
synthesized successfully in 1940[52]. It was not until 1947 when
its biologically active form, known as Coenzyme A (CoA), was
recognized[53]. PA is an essential cofactor in many acetylation
reactions in vivo including tricarboxylic acid cycle (TCA),fatty
acid synthesis and breakdown, as well as other mitochondrial and
cytosolic reactions.
Sources The major dietary sources of pantothenic acid are egg
yolk, liver, kidney, broccoli, and milk [52].Substantial
concentrations of pantothenic acid are also found in chicken, beef,
potatoes, and whole grains[23]. In the diet, pantothenic acid is
mainly in the form of CoA. Panthothenic acid is also produced
bybacteria in the colon [54].
Metabolism Once ingested and broken down, CoA is hydrolyzed in
the small intestine to formpantothenic acid (figure 2). It is then
absorbed in the jejunum and secreted into the bloodstream via
asodium-dependent transport system [55]. Most cells of the body
take up pantothenic acid via the samesodium-dependent mechanism.
Once inside the cell, pantothenic acid undergoes a number
ofATP-dependent phosphorylations to become CoA [56]. Excess
pantothenic acid is hydrolyzed and excretedas cysteamine and
pantothenate via the kidney [57].
Actions CoA has a crucial role in the synthesis of many
molecules, including vitamins A, D, cholesterol,steroids, heme A,
fatty acids, amino acids, and proteins. Coenzyme A also has an
essential role in the firststep of the TCA cycle, by binding with
oxaloacetate to form citrate and then succinyl-CoA. Other
biotin-dependent processes, such as beta-oxidation of fatty acids
and the oxidative degradation of amino acids
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
7 de 32 3/7/15, 10:20 AM
-
(which usually occur after mRNA translation) are important steps
for stabilization and activation of manyproteins in vivo. Many
peptide hormones, such as ACTH, undergo such acetylation in order
to becomebiologically active [58].
Deficiency Many animal models have been used to study the
deficiency of panthenoic acid [52]. In rats,growth failure,
hemorrhage, and necrosis of adrenal cortex, dermatitis, and
achromotrichia (gray hair) havebeen described [59]. In primates,
there is some evidence for impaired synthesis of heme, leading to
anemia[52]. Pantothenic acid deficiency is rare in humans. It has
been noted in severely malnourished individuals,usually in
situations of famine and war. Clinical manifestations can include
paresthesias and dysesthesias,referred to as "burning feet
syndrome." Human volunteers who were fed a pantothenate
antimetabolite forthree months developed burning, distal
paresthesias, and gastrointestinal distress. Because pantothenate
isessential to most living organisms, microbiologic assays have
been used to quantify concentrations in bloodand urine [60].
Toxicity There is no known toxicity for pantothenic acid. Excess
intake is excreted by the kidneys.
Requirements The recommended intake for pantothenic acid is
expressed as Adequate Intake (AI)rather than Recommended Dietary
Allowance (RDA) indicating that there is not adequate data to
specify thepercentage of individuals whose requirement is met by
this intake. The AI is 5 mg daily for adult men andwomen, 6 mg
daily for pregnant women, and 7 mg daily during lactation (table 2)
[23].
VITAMIN B6 (PYRIDOXINE) Paul Gyorgy separated a factor from the
antipellagra factor in the 1930s thathe named vitamin B6, or
pyridoxine. The related compounds, pyridoxal and pyridoxamine, were
later shownto have similar activity. Forms include pyridoxine,
pyridoxal, and pyridoxamine, as well as 5' phosphates(figure 1).
These forms are catabolized into 4-pyridoxic acid, which is
excreted in the urine and can be usedas a marker of pyridoxine
sufficiency, as outlined below.
Sources Pyridoxine and pyridoxamine are predominantly found in
plant foods; pyridoxal is mostcommonly derived from animal foods.
Meats, whole grains, vegetables, and nuts are the best
sources.Cooking, food processing, and storage can reduce vitamin B6
availability by 10 to 50 percent.
Actions Pyridoxal phosphate is used for Schiff base formation
during the transamination of amino acids.Pyridoxal phosphate is
also involved in decarboxylation of amino acids, gluconeogenesis,
conversion oftryptophan to niacin, sphingolipid biosynthesis,
neurotransmitter synthesis, immune function [61], and
steroidhormone modulation.
Deficiency and treatment Overt deficiencies of vitamin B6 are
probably rare. Marginal deficiencies maybe more common, manifested
as nonspecific stomatitis, glossitis, cheilosis, irritability,
confusion, anddepression. A number of genetic syndromes affecting
PLP-dependent enzymes such as homocystinuria,cystathioninuria, and
xanthurenic aciduria mimic vitamin B6 deficiency.
Depressed concentrations of PLP have been reported in asthma,
diabetes, alcoholism, heart disease,pregnancy, breast cancer,
Hodgkin lymphoma, and sickle-cell anemia [62]. Cystathionine
synthase is aPLP-dependent enzyme which produces cystathionine from
serine and homocysteine. As a result, vitaminB6 deficiency can lead
to elevations in plasma homocysteine concentrations, a risk factor
for thedevelopment of atherosclerosis and venous thromboembolism
[63]. (See "Overview of homocysteine".)
The following methods can be used to assess for vitamin B6
deficiency:
The mean plasma pyridoxal-5-phophate (PLP) concentration can be
measured (this is often reportedas pyridoxine or vitamin B6). The
normal ranges are from 27 to 75 nmol/L (6.7 to 18.5 ng/mL) for
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
8 de 32 3/7/15, 10:20 AM
-
Pyridoxine has been used to treat patients with Down's syndrome,
autism, gestational diabetes, carpaltunnel syndrome, premenstrual
syndrome, depression, and diabetic neuropathy, with variable
results [62].
Toxicity Cases of peripheral neuropathy, dermatoses,
photosensitivity, dizziness, and nausea have beenreported with
long-term megadoses of pyridoxine over 250 mg/day; a few cases of
neuropathy appear tohave been caused by chronic intake of 100 to
200 mg/day [66-68].
Requirements The RDA of pyridoxine is 1.3 mg daily for younger
men and women, and rises to 1.7 mgdaily for men older than 50
years, and 1.5 mg daily for women older than 50 years. The RDA is
1.9 mg dailyduring pregnancy, and 2.0 mg daily during lactation
(table 2) [69].
BIOTIN A number of growth factors found in yeast, originally
called "bios," were separated early in the20th century and
eventually identified as myoinositol, pantothenate, and biotin.
Biotin was also found in liverand variously called vitamin H,
coenzyme R, factor S, factor W, vitamin Bw, and protective factor
X, becauseit protected against a type of dermatosis and loss of
hair in animals that was associated with the intake ofraw egg
whites.
The characterization of biotin as a vitamin was based on its
role (deficiency) in carboxylase deficiencysyndromes. Biotin
functions as a cofactor to the carboxylase enzyme [70].
Sources Biotin can be found in a variety of plants, but is found
in highest levels in the liver, egg yolk,soybean products, and
yeast [71].
Chemistry Biotin consists of two cyclic molecules: a ureido and
a tetrahydro-thiophene ring (figure 2). Invivo, it is found in a
number of different isomers, not all of which are active
enzymatically [71]. D-biotin is theonly biologically active isomer.
Biocytin, bound with lysine, is also active. Many analogs of biotin
are actuallyantagonists.
Metabolism Other than the ingested forms of biotin, a number of
bacteria in the gut synthesize biotin as aby-product of their
proteolytic actions. Biotin is mostly absorbed in the proximal
small intestine, and to alesser degree in the cecum. Unabsorbed gut
biotin is excreted in the feces. Excess serum biotin is excretedvia
the kidney [72].
Actions Biotin is an essential component of several enzyme
complexes in mammals, all of which areinvolved in carbohydrate and
lipid metabolism. They include [73]:
males and 26 to 93 nmol/L (6.4 to 23 ng/mL) for females.
Erythrocyte transaminase activity, with and without PLP added,
has been used as a functional test ofpyridoxine status, and may be
a more accurate reflection of vitamin B6 status in critically ill
patients[64].
Urinary 4-pyridoxic acid excretion greater than 3.0 mmol/day can
be used as an indicator of adequateshort-term vitamin B6 status
(this is often reported as urinary pyridoxic acid) [65].
Urinary excretion of xanthurenic acid is normally less than 65
mmol/day following a 2 g tryptophanload.
Acetyl-CoA carboxylase (ACC)Pyruvate carboxylase (PC)Propionyl
CoA carboxylase (PCC)Beta-methylcrotonyl CoA carboxylase (MCC)
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
9 de 32 3/7/15, 10:20 AM
-
Biotin acts as a CO2 carrier on the surface of each enzyme. As a
result, it has an essential role in manyprocesses, including
protein and DNA synthesis and cell replication.
Deficiency Biotin deficiency was first noted in patients who
were on long-term parenteral nutrition prior toroutine biotin
supplementation [73]. It is now reported only rarely. Decreased
function of the biotin-dependentcarboxylases can have a number of
metabolic consequences. The enzyme pyruvate carboxylase,
forexample, is involved in converting pyruvate to oxaloacetate in a
number of tissues in which gluconeogenesisoccurs. Oxalate is later
converted to glucose. In the setting of biotin deficiency, pyruvate
levels rise and areconverted to lactic acid. Another example is the
synthesis of succinyl-CoA from several amino acids (ie,valine,
isoleucine, and methionine), which requires the enzymatic action of
propionyl CoA carboxylase.Biotin deficiency leads to build up of
propionyl-CoA, which gets metabolized into odd-chain fatty
acids.
The clinical manifestations of biotin deficiency may not be
solely due to decreased intake of biotin.Consumption of large
amounts of raw egg whites (which contain avidin, a substance that
binds to biotin andprevents its utilization), can also lead to
biotin deficiency. In addition, secondary biotin deficiency can
occurdue to lack of a specific enzyme (biotinidase), which is
required for recycling of biotin (see 'Multiplecarboxylase
deficiency' below) [74].
Symptoms of biotin deficiency are nonspecific and may include
changes in mental status, myalgia,dysesthesias, anorexia, and
nausea. Chronic deficiency can lead to a maculosquamous dermatitis
of theextremities [71]. Because of its role in lipid metabolism,
biotin deficiency can lead to defects in metabolism oflong-chain
fatty acids. The resulting deficiency of essential fatty acids is
often manifested by dermatologicchanges such as seborrheic
dermatitis and alopecia.
Normal serum biotin concentrations are around 1500 pmol/L.
Normal urine biotin excretion is around 160nmol/day, using biotin
bioassays measuring growth of Lactobacillus or other
microorganisms, or radioligandassays with labeled avidin.
Multiple carboxylase deficiency Multiple carboxylase deficiency
(MCD) refers to one of two inheriteddefects of biotin metabolism.
The infantile form is caused by a deficiency of holocarboxylase
synthetase(HCS) and presents in the first week of life with
lethargy, poor muscle tone, and vomiting [75]. A later-onsetform is
caused by biotinidase deficiency and is associated with a slow but
progressive loss of biotin in theurine, leading to organic aciduria
[76]; it is characterized by ataxia, ketoacidosis, dermatitis,
seizures,myoclonus, and nystagmus. (See "Overview of the hereditary
ataxias", section on 'Disorders of pyruvate andlactate
metabolism'.)
MCD is diagnosed definitively by studying enzymes from
lymphocytes. Screening for these deficiencies isincluded in the
newborn screen in most states (see "Newborn screening", section on
'Programs throughoutthe world'). Both infantile and late onset
multiple carboxylase deficiency can be treated with
pharmacologicdoses of biotin. Delayed treatment may fail to reverse
the neurologic sequelae and has been associated withneurologic and
developmental delay [60,76].
Toxicity No toxicity of excess biotin intake has been
described.
Requirements There are still no accurate data estimating dietary
requirements for biotin. Adequateintakes are approximately 30 mcg
daily for adults according to a report from the Food and Nutrition
Board of1998 (table 2) [69].
VITAMIN C (ASCORBIC ACID) Vitamin C (ascorbic acid) has a
prominent role in history. The clinicalmanifestations of scurvy
were well described in ancient Egyptian, Greek, and Roman
literature. British andEuropean explorers of the renaissance era
were ravaged by scurvy. Scurvy was a major cause of morbidity
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
10 de 32 3/7/15, 10:20 AM
-
and death amongst much of Europe during the great potato famine,
the United States Civil War, theexploration of the North Pole, and
the California gold rush. Captain James Cook was one of the first
todemonstrate that sailors who spent months at sea could avoid
scurvy by maintaining a diet rich invegetables [77]. James Lind, a
British naval surgeon, published his experiences and studies on
scurvyaboard ships in a book titled Treatise of the Scurvy [77].
During 1928 to 1931, Szent-Gyorgyi isolatedhexuronic acid from
cabbage, oranges, paprika, and adrenal glands. Hexuronic acid was
subsequentlytermed vitamin C and found to prevent the development
of scurvy [78,79].
Sources Important food sources of vitamin C are citrus fruits,
tomatoes, potatoes, brussel sprouts,cauliflower, broccoli,
strawberries, cabbage, and spinach [80].
Chemistry Ascorbic acid is the enolic form of an
alpha-ketolactone, and is closely akin to the glucosestructure
(figure 2). A number of compounds that exhibit the biologic
activities of ascorbic acid are generallyreferred to as vitamin
C.
Metabolism Ascorbic acid is absorbed in the distal small
intestine through an energy dependent process.Usual dietary doses
of up to 100 mg/day are almost completely absorbed [81]. As dietary
concentrationsincrease, a smaller fraction is absorbed;
pharmacologic dosing (>1000 mg/day) can result in
absorptionrates of
-
bleeding gums (picture 3), petechiae, coiled hairs,
hyperkeratosis (picture 4), Sjogren's syndrome,arthralgias, and
impaired wound healing. Generalized systemic symptoms are weakness,
malaise, jointswelling, arthralgias, edema, depression, neuropathy,
and vasomotor instability [83].
In the United States, ascorbic acid deficiency occurs mostly in
severely malnourished individuals, drug andalcohol abusers, or
those living in poverty or on diets devoid of fruits and vegetables
[91,92]. In children,breast milk provides an adequate source of
ascorbic acid for newborns and infants. In the
elderly,institutionalized, or chronically ill patients, scurvy can
be seen due to their poor dietary intake [93].Symptoms of scurvy
generally occur when the plasma concentration of ascorbic acid is
less than 0.2 mg/dL(11 micromol/L) [80]. Recent vitamin C intake
can normalize plasma ascorbic acid concentrations even iftissue
levels are still deficient. Measurement of ascorbic acid in
leukocytes is a better measure of bodystores but this test is not
widely available.
The treatment for scurvy is vitamin C supplementation and
reversal of the conditions that led to thedeficiency. A wide range
of replacement doses have been used successfully. For children,
recommendeddoses are 100 mg ascorbic acid given three times daily
for one week, then once daily for several weeks untilthe patient is
fully recovered [94]. Adults are usually treated with 300 to 1000
mg daily for one month [95,96].
Many of the constitutional symptoms improve within 24 hours of
treatment; bruising and gingival bleedingresolve within a few
weeks.
Therapeutic and prophylactic roles Several therapeutic and
prophylactic roles have been described forvitamin C, including
prevention of cardiovascular disease and cancer. However, current
evidence does notsupport the use of vitamin C supplementation for
disease prevention. Vitamin C may have a minor role inpreventing
the common cold. (See "Vitamin supplementation in disease
prevention", section on 'Cataractsand macular degeneration'.)
Toxicity A number of side effects of ascorbic acid have been
reported in the literature. Large doses ofvitamin C (in gram
quantities) can give false negative stool guaiac results [97] and
have been associatedwith diarrhea and abdominal bloating. There has
been some controversy in the literature regarding highintake and
increased oxalate production. Some reports conclude that excessive
use of vitamin C is a riskfactor for calcium oxalate
nephrolithiasis [98]. However, a prospective epidemiologic study
demonstratedthat consumption of high doses of vitamin C (1500
mg/day) lowered the relative risk of calcium oxalatestones compared
to 250 mg or less of vitamin C per day [99]. Thus, the relationship
of high-dose vitamin Cingestion and calcium oxalate stones is
tentative [100,101]. Patients with a predisposition to form
oxalatestones or those on hemodialysis should avoid excessive use
of vitamin C.
Ingestion of large quantities of ascorbic acid has been rarely
associated with fatal cardiac arrhythmias inpatients with iron
overload, presumably due to oxidative injury [102]. Thus, it may be
reasonable to advisepatients to avoid ascorbic acid supplements,
but there is no reason to discourage the consumption of freshfruits
or vegetables containing vitamin C. (See "Management of patients
with hereditary hemochromatosis".)
Requirements The RDA for ascorbic acid is 75 mg per day for most
women and 90 mg per day for men;pregnant or lactating women and the
elderly have requirements up to 120 mg/day (table 2) [80]. This
isbased upon the minimum requirement to prevent scurvy [83].
Requirements for smokers are increased by asmuch as 40 percent
[103].
OTHER VITAMINS AND PSEUDOVITAMINS Lecithin, choline (precursors
for acetylcholine), inositol,carnitine (long-chain fatty acid
transporter), lipoic acid, lutein, zeaxanthin, other flavonoids and
carotenoidsprobably could be classed as vitamins because humans
cannot synthesize them, but dietary sources usually
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
12 de 32 3/7/15, 10:20 AM
-
provide ample amounts and clinical deficiencies are extremely
rare. In addition, there are many substancesthat have been promoted
as vitamins in the popular press but have little support in the
scientific literature,including laetrile ("vitamin B17,"
amygdalin), pangamic acid ("vitamin B15,"
diisopropylaminedichloroacetate), and gerovital ("vitamin H3")
[104].
VITAMIN B12 AND FOLIC ACID These water-soluble vitamins are
discussed in detail in separate topicreviews. (See "Etiology and
clinical manifestations of vitamin B12 and folate deficiency" and
"Diagnosis andtreatment of vitamin B12 and folate deficiency".)
SUMMARY
Vitamins are a number of chemically unrelated families of
organic substances that cannot besynthesized by humans but need to
be ingested in the diet in small quantities to prevent disorders
ofmetabolism. They are divided into water-soluble and fat-soluble
vitamins (table 1). This topic reviewdiscusses the water-soluble
vitamins B1 (thiamine), B2 (riboflavin), B3 (niacin), B5
(pantothenic acid),B6 (pyridoxine), biotin, and vitamin C. (See
'Introduction' above.)
The following tables outline the requirements for each of the
water-soluble vitamins (table 2) andtypical symptoms of their
deficiency (table 3).
Thiamine (vitamin B1) is found in larger quantities in food
products such as yeast, legumes, pork, rice,and cereals. Thiamine
deficiency causes each of the following disorders:
Beriberi, characterized by peripheral neuropathy, with or
without edema and congestive heartfailure. (See 'Adult beriberi'
above.)
Wernickes encephalopathy, characterized by nystagmus,
ophthalmoplegia, and ataxia, along withconfusion, and
Wernicke-Korsakoff syndrome, a chronic neurologic condition. (See
'Wernicke-Korsakoff syndrome' above.)
Infantile beriberi, due to dietary deficiency, or Leigh syndrome
due to a sporadic mitochondrialdisorder. (See 'Infantile beriberi'
above and 'Leigh syndrome' above.)
Riboflavin (vitamin B2) is supplied in meats, fish, eggs and
milk, green vegetables, yeast, and enrichedfoods. Mild deficiency
is often undetected due to the mild nature and nonspecific signs
and symptomsof deficiency. Riboflavin deficiency is characterized
by sore throat, hyperemia of pharyngeal mucousmembranes, edema of
mucous membranes, cheilitis, stomatitis, glossitis,
normocytic-normochromicanemia, and seborrheic dermatitis. Risk
factors for riboflavin deficiency include anorexia
nervosa,malabsorptive syndromes, and chronic use of phenobarbital
and other barbiturates. (See 'Vitamin B2(riboflavin)' above.)
Niacin (vitamin B3) is widely distributed in plant and animal
foods.
Niacin deficiency causes pellagra, which is characterized by a
photosensitive pigmenteddermatitis (typically located in
sun-exposed areas (picture 2)), diarrhea, and dementia.
Inindustrialized countries, pellagra tends to occur in alcoholics
and has been reported as acomplication of bariatric surgery or
anorexia nervosa. (See 'Deficiency' above.)
In high doses (1 to 3 grams a day) niacin is a well-established
antihyperlipidemic agent,decreasing total and LDL cholesterol. Side
effects at these doses include flushing, nausea,vomiting, pruritus,
hives, constipation, and elevation in serum aminotransferases. (See
"Lipidlowering with drugs other than statins and fibrates", section
on 'Nicotinic acid (Niacin)' and
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
13 de 32 3/7/15, 10:20 AM
-
Use of UpToDate is subject to the Subscription and License
Agreement.
REFERENCES
Tanphaichitr V. Modern Nutrition in Health and Medicine, 9th,
Shils M (Ed), Lippincott, Philadelphia2000. p.381.
1.
Tanphaichitr V, Wood B. Thiamin. In: Present Knowledge in
Nutrition, 5th, Olson RE, Broquist CO, et al(Eds), Nutrition
Foundation, Washington, DC 1984. p.273.
2.
Gubler CJ. Thiamin. In: Handbook of vitamins: Nutritional,
biochemical, and clinical aspects, MachlinLJ (Ed), Marcel Dekker,
New York 1984. p.245.
3.
Davis RE, Icke GC, Thom J, Riley WJ. Intestinal absorption of
thiamin in man compared with folateand pyridoxal and its subsequent
urinary excretion. J Nutr Sci Vitaminol (Tokyo) 1984; 30:475.
4.
Sauberlich HE, Daude RP, Skala JH. Laboratory Tests for the
Assessment of Nutritional Status, CRCPress, Boca Raton, Florida
1974.
5.
Talwar D, Davidson H, Cooney J, St JO'Reilly D. Vitamin B(1)
status assessed by direct measurement6.
'Toxicity' above.)
Pantothenic acid (vitamin B5) in the diet is mainly in the form
of coenzyme A (CoA) and is supplied inegg yolk, liver, kidney,
broccoli, and milk. Pantothenic acid deficiency is rare in humans
but has beennoted in severely malnourished individuals. Clinical
manifestations can include paresthesias anddysesthesias, known as
"burning feet syndrome."
Pyridoxine (vitamin B6) is found in the diet in several forms,
including pyridoxine and pyridoxamine(from plants) and pyridoxal
(from animal foods). Meats, whole grains, vegetables, and nuts are
the bestsources. Overt deficiencies of vitamin B6 are probably
rare. Marginal deficiencies may be morecommon, manifested as
nonspecific stomatitis, glossitis, cheilosis, irritability,
confusion, anddepression. Toxicity has been reported with long-term
use of megadoses of pyridoxine (over 250mg/day), characterized by
peripheral neuropathy, dermatoses, photosensitivity, dizziness, and
nausea.(See 'Vitamin B6 (pyridoxine)' above.)
Biotin deficiency was first noted in patients who were on
long-term parenteral nutrition prior to routinebiotin
supplementation. Symptoms of biotin deficiency are nonspecific and
may include changes inmental status, myalgia, dysesthesias,
anorexia, and nausea. Chronic deficiency can lead tomaculosquamous
dermatitis of the extremities. (See 'Deficiency' above.)
Multiple carboxylase deficiency is a congenital disorder of
biotin metabolism, caused by deficiency ofbiotinidase or
holocarboxylase synthetase, enzymes crucial to the biotin
metabolism pathway. Thesedisorders are included in newborn
screening programs in the United States and can be treated
withpharmacologic doses of biotin. (See 'Multiple carboxylase
deficiency' above and "Overview of thehereditary ataxias", section
on 'Disorders of pyruvate and lactate metabolism'.)
Vitamin C (ascorbic acid) is essential for a variety of
processes including collagen synthesis. Vitamin Cdeficiency, known
as scurvy, is characterized by ecchymoses, bleeding gums (picture
3), petechiae,coiled hairs, hyperkeratosis (picture 4), Sjogren's
syndrome, arthralgias, and impaired wound healing,as well as
constitutional symptoms. However, current evidence does not support
the use of vitamin Csupplementation for disease prevention. (See
'Vitamin C (ascorbic acid)' above.)
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
14 de 32 3/7/15, 10:20 AM
-
of thiamin pyrophosphate in erythrocytes or whole blood by HPLC:
comparison with erythrocytetransketolase activation assay. Clin
Chem 2000; 46:704.
Chaitiraphan S, Tanphaichitr V, Cheng TO. Nutritional heart
disease. In: The international textbook ofcardiology, Cheng TO
(Ed), Pergamon Press, New York 1986. p.864.
7.
Tanphaichitr V. Epidemiology and clinical assessment of vitamin
deficiencies in Thai children. In: Childhealth in the tropics,
Eeckels RE, Ransome-kuti O, Kroonenberg CC (Eds), Martinus Nijhoff,
Dordrect1985. p.157.
8.
Fattal-Valevski A, Kesler A, Sela BA, et al. Outbreak of
life-threatening thiamine deficiency in infants inIsrael caused by
a defective soy-based formula. Pediatrics 2005; 115:e233.
9.
Fattal-Valevski A, Bloch-Mimouni A, Kivity S, et al. Epilepsy in
children with infantile thiaminedeficiency. Neurology 2009;
73:828.
10.
Mimouni-Bloch A, Goldberg-Stern H, Strausberg R, et al. Thiamine
deficiency in infancy: long-termfollow-up. Pediatr Neurol 2014;
51:311.
11.
Fattal-Valevski A, Azouri-Fattal I, Greenstein YJ, et al.
Delayed language development due to infantilethiamine deficiency.
Dev Med Child Neurol 2009; 51:629.
12.
Towbin A, Inge TH, Garcia VF, et al. Beriberi after gastric
bypass surgery in adolescence. J Pediatr2004; 145:263.
13.
Chaves LC, Faintuch J, Kahwage S, Alencar Fde A. A cluster of
polyneuropathy and Wernicke-Korsakoff syndrome in a bariatric unit.
Obes Surg 2002; 12:328.
14.
Lawson ML, Kirk S, Mitchell T, et al. One-year outcomes of
Roux-en-Y gastric bypass for morbidlyobese adolescents: a
multicenter study from the Pediatric Bariatric Study Group. J
Pediatr Surg 2006;41:137.
15.
Hahn JS, Berquist W, Alcorn DM, et al. Wernicke encephalopathy
and beriberi during total parenteralnutrition attributable to
multivitamin infusion shortage. Pediatrics 1998; 101:E10.
16.
Shimon I, Almog S, Vered Z, et al. Improved left ventricular
function after thiamine supplementation inpatients with congestive
heart failure receiving long-term furosemide therapy. Am J Med
1995; 98:485.
17.
Seligmann H, Halkin H, Rauchfleisch S, et al. Thiamine
deficiency in patients with congestive heartfailure receiving
long-term furosemide therapy: a pilot study. Am J Med 1991;
91:151.
18.
Rieck J, Halkin H, Almog S, et al. Urinary loss of thiamine is
increased by low doses of furosemide inhealthy volunteers. J Lab
Clin Med 1999; 134:238.
19.
Leslie D, Gheorghiade M. Is there a role for thiamine
supplementation in the management of heartfailure? Am Heart J 1996;
131:1248.
20.
Singleton CK, Pekovich SR, McCool BA, Martin PR. The
thiamine-dependent hysteretic behavior ofhuman transketolase:
implications for thiamine deficiency. J Nutr 1995; 125:189.
21.
Food and Nutrition Board, National Research Council Recommended
dietary allowances. 10th edition.Washington DC: National Academy
Press, 1989. p.125.
22.
Food and Nutrition Board-Institute of Medicine. Dietary
reference intakes. Thiamin, riboflavin, niacin,vitamin B6, folate,
vitamin B12, pantothenic acid, biotin, and choline, National
Academy Press,Washington DC 1998.
23.
McCormick DB. Metabolism of riboflavin. In: Riboflavin, Rivlin
RS (Ed), Plenum press, New York 1975.p.153.
24.
McCormick DB. Riboflavin. In: Present knowledge in nutrition,
6th, Brown ML (Ed), International LifeSciences Institute Nutrition
Foundation, 1990. p.146.
25.
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
15 de 32 3/7/15, 10:20 AM
-
Merrill AH Jr, Lambeth JD, Edmondson DE, McCormick DB. Formation
and mode of action offlavoproteins. Annu Rev Nutr 1981; 1:281.
26.
Said HM, Ma TY. Mechanism of riboflavine uptake by Caco-2 human
intestinal epithelial cells. Am JPhysiol 1994; 266:G15.
27.
Wilson JA. Vitamin deficiency and excess. In: Harrison's
Principles of Internal Medicine, 14th, FauciAS, Braunwald E,
Isselbacher K (Eds), McGraw-Hill, New York 1998. p.481.
28.
Nichoalds GE. Riboflavin. Symposium in laboratory medicine. In:
Symposium on laboratoryassessment of nutritional status. Clinics in
laboratory medicine, Labbae RF (Ed), WB Saunders,Philadelphia 1981.
Vol 1, p.685.
29.
DiDonato S, Gellera C, Peluchetti D, et al. Normalization of
short-chain acylcoenzyme Adehydrogenase after riboflavin treatment
in a girl with multiple acylcoenzyme A dehydrogenase-deficient
myopathy. Ann Neurol 1989; 25:479.
30.
Ohkawa H, Ohishi N, Yagi K. New metabolites of riboflavin appear
in human urine. J Biol Chem 1983;258:5623.
31.
Food and Nutrition Board, National Research Council. Riboflavin.
In: Recommended dietaryallowances, 10th ed, National Academy Press,
Washington, DC 1989. p.132.
32.
Fouty B, Frerman F, Reves R. Riboflavin to treat nucleoside
analogue-induced lactic acidosis. Lancet1998; 352:291.
33.
Weiner M, Van Eys J. The discovery of nicotinic acid as a
nutrient. In: Nicotinic acid: Nutrient-cofactor-drug, Clinical
pharmacology, Weiner M (Ed), Marcel Dekker, New York 1983. p.3.
34.
VILTER RW, MUELLER JF, BEAN WB. The therapeutic effect of
tryptophane in human pellagra. J LabClin Med 1949; 34:409.
35.
Kim H, Jacobson EL, Jacobson MK. Position of cyclization in
cyclic ADP-ribose. Biochem Biophys ResCommun 1993; 194:1143.
36.
Cervantes-Laurean N, McElvaney G, Moss J. Niacin. In: Modern
Nutrition in Health and Medicine,Shils M (Ed), Lippincott,
Philadelphia 2000. p.401.
37.
Ashourian N, Mousdicas N. Images in clinical medicine.
Pellagra-like dermatitis. N Engl J Med 2006;354:1614.
38.
Prousky JE. Pellagra may be a rare secondary complication of
anorexia nervosa: a systematic reviewof the literature. Altern Med
Rev 2003; 8:180.
39.
Wan P, Moat S, Anstey A. Pellagra: a review with emphasis on
photosensitivity. Br J Dermatol 2011;164:1188.
40.
Elsas LS, Longo N, Rosenberg LE. Inherited defects of membrane
transport. In: Harrison's Principlesof Internal Medicine, 14th,
Fauci AS, Braunwald E, Isselbacher K, et al (Eds), McGraw-Hill, New
York1998. p.2203.
41.
Levy HL. Hartnup disorder. In: The Molecular and Metabolic Basis
of Inherited Disease, 7th, Scriver S,et al (Eds), McGraw-Hill, New
York 1995. p.3629.
42.
Bean WB. Some aspects of pharmacologic use and abuse of water
soluble vitamins. In: Nutriton anddrug interrelations, Hathcock JN,
Coon J (Eds), Academic Press, New York 1978. p.667.
43.
Hathcock JN. Vitamins and minerals: efficacy and safety. Am J
Clin Nutr 1997; 66:427.44.
DiPalma JR, Thayer WS. Use of niacin as a drug. Annu Rev Nutr
1991; 11:169.45.
Gharavi AG, Diamond JA, Smith DA, Phillips RA. Niacin-induced
myopathy. Am J Cardiol 1994;46.
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
16 de 32 3/7/15, 10:20 AM
-
74:841.
Rader JI, Calvert RJ, Hathcock JN. Hepatic toxicity of
unmodified and time-release preparations ofniacin. Am J Med 1992;
92:77.
47.
McKenney JM, Proctor JD, Harris S, Chinchili VM. A comparison of
the efficacy and toxic effects ofsustained- vs immediate-release
niacin in hypercholesterolemic patients. JAMA 1994; 271:672.
48.
Petley A, Macklin B, Renwick AG, Wilkin TJ. The pharmacokinetics
of nicotinamide in humans androdents. Diabetes 1995; 44:152.
49.
ALTSCHUL R, HOFFER A, STEPHEN JD. Influence of nicotinic acid on
serum cholesterol in man.Arch Biochem Biophys 1955; 54:558.
50.
Elliott RB, Pilcher CC, Stewart A, et al. The use of
nicotinamide in the prevention of type 1 diabetes.Ann N Y Acad Sci
1993; 696:333.
51.
Robinson FA. The vitamin co-factors if enzyme systems, Pergamon
Press, Oxford 1966. p.406.52.
Plesofsky-Vig N. Pantothenic acid. In: Modern nutrition in
health and disease, Shils ME, Olson JA,Shike M, et al (Eds),
Lippincott, Philadelphia 2000. p.423.
53.
Said HM, Ortiz A, McCloud E, et al. Biotin uptake by human
colonic epithelial NCM460 cells: a carrier-mediated process shared
with pantothenic acid. Am J Physiol 1998; 275:C1365.
54.
Fenstermacher DK, Rose RC. Absorption of pantothenic acid in rat
and chick intestine. Am J Physiol1986; 250:G155.
55.
Robishaw JD, Berkich D, Neely JR. Rate-limiting step and control
of coenzyme A synthesis in cardiacmuscle. J Biol Chem 1982;
257:10967.
56.
Wittwer CT, Burkhard D, Ririe K, et al. Purification and
properties of a pantetheine-hydrolyzing enzymefrom pig kidney. J
Biol Chem 1983; 258:9733.
57.
Plesofsky-Vig N, Brambl R. Pantothenic acid and coenzyme A in
cellular modification of proteins. AnnuRev Nutr 1988; 8:461.
58.
HODGES RE, BEAN WB, OHLSON MA, BLEILER R. Human pantothenic acid
deficiency produced byomega-methyl pantothenic acid. J Clin Invest
1959; 38:1421.
59.
Sander JE, Packman S, Townsend JJ. Brain pyruvate carboxylase
and the pathophysiology of biotin-dependent diseases. Neurology
1982; 32:878.
60.
Rall LC, Meydani SN. Vitamin B6 and immune competence. Nutr Rev
1993; 51:217.61.
Leklem JE. Vitamin B6. In: Handbook of Vitamins, 2nd, Machlin LJ
(Ed), Marcel Dekker, New York1991.
62.
Rimm EB, Willett WC, Hu FB, et al. Folate and vitamin B6 from
diet and supplements in relation to riskof coronary heart disease
among women. JAMA 1998; 279:359.
63.
Burtis CA, Ashwood ER, Bruns DE. Vitamins and trace elements.
In: Tietz Textbook of ClinicalChemistry and Molecular Diagnostics,
5e, Saunders/Elsevier, St. Louis, MO 2012. p.895.
64.
Leklem JE. Vitamin B-6: a status report. J Nutr 1990; 120 Suppl
11:1503.65.
Schaumburg H, Kaplan J, Windebank A, et al. Sensory neuropathy
from pyridoxine abuse. A newmegavitamin syndrome. N Engl J Med
1983; 309:445.
66.
Silva CD, D'Cruz DP. Pyridoxine toxicity courtesy of your local
health food store. Ann Rheum Dis 2006;65:1666.
67.
Katan MB. [How much vitamin B6 is toxic?]. Ned Tijdschr Geneeskd
2005; 149:2545.68.
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
17 de 32 3/7/15, 10:20 AM
-
Food and Nutrition Board-Institute of Medicine. Dietary
reference intakes. Thiamin, riboflavin, niacin,vitamin B6, folate,
vitamin B12, pantothenic acid, biotin, and choline, National
Academy Press,Washington DC 1998. www.nap.edu (Accessed on June 06,
2008).
69.
Dupuis L, Campeau E, Leclerc D, Gravel RA. Mechanism of biotin
responsiveness in biotin-responsivemultiple carboxylase deficiency.
Mol Genet Metab 1999; 66:80.
70.
Mock D. Biotin. In: Modern Nutrition in Health and Disease, 9th,
Shils M (Ed), Lippincott Williams andWilkins, Philadelphia 2000.
p.459.
71.
Kopinski JS, Leibholz J, Bryden WL. Biotin studies in pigs. 3.
Biotin absorption and synthesis. Br JNutr 1989; 62:767.
72.
Mock DM. Biotin. In: Present knowledge in nutrition, Ziegler EE,
Filer LJ Jr (Eds), International LifeSciences Institutes Nutrition
Foundation, Washington DC 1996. p.220.
73.
Cole H, Reynolds TR, Lockyer JM, et al. Human serum biotinidase.
cDNA cloning, sequence, andcharacterization. J Biol Chem 1994;
269:6566.
74.
Mock DM, Mock NI, Dankle JA. Secretory patterns of biotin in
human milk. J Nutr 1992; 122:546.75.
Baumgartner ER, Suormala T. Multiple carboxylase deficiency:
inherited and acquired disorders ofbiotin metabolism. Int J Vitam
Nutr Res 1997; 67:377.
76.
Carpenter KJ. The History of scurvy and vitamin C, Cambridge
University Press, New York 1986.77.
Szent-Gyorgyi A, The function of hexuronic acid in the
respiration of the cabbage leaf. Biochem J1931; 90:385.
78.
Svirbely JL, Szent-Gyrgyi A. The chemical nature of vitamin C.
Biochem J 1933; 27:279.79.
Food and Nutrition Board - Institute of Medicine. Dietary
reference intakes for Vitamin C, Vitamin E,Selenium, and
Carotenoids, National Academy Press, Washington DC 2000 www.nap.edu
(Accessedon April 07, 2009).
80.
Kallner A, Hornig D, Pellikka R. Formation of carbon dioxide
from ascorbate in man. Am J Clin Nutr1985; 41:609.
81.
Glatthaar BE, Hornig DH, Moser U. The role of ascorbic acid in
carcinogenesis. Adv Exp Med Biol1986; 206:357.
82.
Jacob R. Vitamin C. In: Modern nutrition in health and disease,
Shils M, Olson J, Shike M, Ross AC(Eds), Lippincott, Philadelphia
2000. p.467.
83.
Bigley RH, Stankova L. Uptake and reduction of oxidized and
reduced ascorbate by humanleukocytes. J Exp Med 1974; 139:1084.
84.
Schorah CJ. The transport of vitamin C and effects of disease.
Proc Nutr Soc 1992; 51:189.85.
Rebouche CJ. Renal handling of carnitine in experimental vitamin
C deficiency. Metabolism 1995;44:1639.
86.
Ronchetti IP, Quaglino D Jr, Bergamini G. Ascorbic acid and
connective tissue. In: Subcellularbiochemistry Ascobic acid:
Biochemistry and biomedial cell biology, Harris JR (Ed), Plenum
Press,New York 1996. p.41.
87.
Katsuki H. Vitamin C and nervous tissue. In: Subcellular
biochemistry Ascobic acid: biochemistry andbiomedial cell biology,
Harris JR (Ed), Plenum Press, New York 1996. p.293.
88.
Horrobin DF. Ascorbic acid and prostaglandin synthesis. In:
Subcellular biochemistry Ascorbic acid:biochemistry and biomedial
cell biology, Harris JR (Ed), Plenum Press, New York 1996.
p.109.
89.
Millar J. The nitric oxide/ascorbate cycle: how neurones may
control their own oxygen supply. Med90.
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
18 de 32 3/7/15, 10:20 AM
-
Hypotheses 1995; 45:21.
Reuler JB, Broudy VC, Cooney TG. Adult scurvy. JAMA 1985;
253:805.91.
Smith A, Di Primio G, Humphrey-Murto S. Scurvy in the developed
world. CMAJ 2011; 183:E752.92.
Monget AL, Galan P, Preziosi P, et al. Micronutrient status in
elderly people. Geriatrie/Min. Vit. AuxNetwork. Int J Vitam Nutr
Res 1996; 66:71.
93.
American Academy of Pediatrics. Water-soluble vitamins. In:
Pediatric Nutrition, 7th ed., Kleinman RE,Greer FR. (Eds), American
Academy of Pediatrics, Elk Grove Village 2011. p.527.
94.
Hirschmann JV, Raugi GJ. Adult scurvy. J Am Acad Dermatol 1999;
41:895.95.
Weinstein M, Babyn P, Zlotkin S. An orange a day keeps the
doctor away: scurvy in the year 2000.Pediatrics 2001; 108:E55.
96.
Jaffe RM, Kasten B, Young DS, MacLowry JD. False-negative stool
occult blood tests caused byingestion of ascorbic acid (vitamin C).
Ann Intern Med 1975; 83:824.
97.
Urivetzky M, Kessaris D, Smith AD. Ascorbic acid overdosing: a
risk factor for calcium oxalatenephrolithiasis. J Urol 1992;
147:1215.
98.
Block G. Vitamin C and cancer prevention: the epidemiologic
evidence. Am J Clin Nutr 1991; 53:270S.99.
Hatch GE. Asthma, inhaled oxidants, and dietary antioxidants. Am
J Clin Nutr 1995; 61:625S.100.
Seddon JM, Ajani UA, Sperduto RD, et al. Dietary carotenoids,
vitamins A, C, and E, and advancedage-related macular degeneration.
Eye Disease Case-Control Study Group. JAMA 1994; 272:1413.
101.
McLaran CJ, Bett JH, Nye JA, Halliday JW. Congestive
cardiomyopathy and haemochromatosis--rapidprogression possibly
accelerated by excessive ingestion of ascorbic acid. Aust N Z J Med
1982;12:187.
102.
Smith JL, Hodges RE. Serum levels of vitamin C in relation to
dietary and supplemental intake ofvitamin C in smokers and
nonsmokers. Ann N Y Acad Sci 1987; 498:144.
103.
Cody MM. Substances without vitamin status. In: Handbook of
Vitamins, 2nd, Marcel Dekker, NewYork 1991.
104.
Topic 5367 Version 15.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
19 de 32 3/7/15, 10:20 AM
-
GRAPHICS
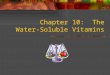
Clinical symptoms of selected vitamin deficiencies
Function Deficiency syndrome
Water-soluble vitamins
Vitamin B1(thiamine)
Thiaminepyrophosphate
Beriberi - congestive heart failure (wet beriberi),aphonia,
peripheral neuropathy, Wernickeencephalopathy (nystagmus,
opthalmoplegia,ataxia), confusion, or coma
Vitamin B2(riboflavin)
Flavine adeninedinucleotide
Nonspecific symptoms including edema of mucusmembranes, angular
stomatitis, glossitis, andseborrheic dermatitis (eg, nose,
scrotum)
Niacin(nicotinic acid)
Nicotinamideadeninedinucleotide
Pellagra - dermatitis on areas exposed to sunlight;diarrhea with
vomiting, dysphagia, mouthinflammation (glossitis, angular
stomatitis, cheilitis);headache, dementia, peripheral neuropathy,
loss ofmemory, psychosis, delirium, catatonia
Vitamin B6(pyroxidine,pyridoxal)
Transaminasecofactor
Anemia, weakness, insomnia, difficulty walking,nasolabial
seborrheic dermatitis, cheilosis, stomatitis
Vitamin B12(cobalamin)
One carbontransfer
Megaloblastic anemia (pernicious anemia). Peripheralneuropathy,
with impaired proprioception, andslowed mentation.
Folate One carbontransfer
Megaloblastic anemia
Biotin Pyruvatecarboxylasecofactor
Nonspecific symptoms including altered mentalstatus, myalgia,
dysesthesias, anorexia,maculosquamous dermatitis
Pantothenate Coenzyme A Nonspecific symptoms including
paresthesias,dysesthesias ("burning feet"), anemia,gastrointestinal
symptoms
Vitamin C(ascorbate)
Antioxidant,collagensynthesis
Scurvy - fatigue, petechiae, ecchymoses, bleedinggums,
depression, dry skin, impaired wound healing
Fat-soluble vitamins
Vitamin A(retinol,retinal, retinoicacid)
Vision, epithelialdifferentiation
Night blindness, xerophthalmia, keratomalacia,Bitot's spot,
follicular hyperkeratosis
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
20 de 32 3/7/15, 10:20 AM
-
Vitamin D(cholecalciferol,ergocalciferol)
Prohormone forcalciumregulation
Rickets, osteomalacia, craniotabes, rachitic rosary
Vitamin E(tocopherols)
Antioxidant Sensory and motor neuropathy, ataxia,
retinaldegeneration, hemolytic anemia
Vitamin K(phylloquinone,menaquinone,menadione)
Clotting factors,bone proteins
Hemorrhagic disease
Graphic 63827 Version 7.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
21 de 32 3/7/15, 10:20 AM
-
Chemical structure of vitamins B1, B2, B6 and B12
Graphic 77100 Version 2.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
22 de 32 3/7/15, 10:20 AM
-
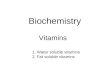
Dietary Reference Index (DRIs) of water soluble vitamins
Lifestagegroup
Thiamin(mg/d)
Riboflavin(mg/d)
Niacin*(mg/d)
Pantothenicacid
(mg/d)
VitaminB
(mg/d)
Biotin(mcg/d)
RDA*/AI
ULRDA/
AIUL
RDA/AI
ULRDA/
AIUL
RDA/AI
ULRDA/
AIUL
Infants
0 to6 mo
0.2 ND 0.3 ND 2 ND 1.7 ND 0.1 ND 5 ND
7 to12mo
0.3 ND 0.4 ND 4 ND 1.8 ND 0.3 ND 6 ND
Children
1 to3 y
0.5 ND 0.5 ND 6 10 2 ND 0.5 30 8 ND
4 to8 y
0.6 ND 0.6 ND 8 15 3 ND 0.6 40 12 ND
Males
9 to13 y
0.9 ND 0.9 ND 12 20 4 ND 1.0 60 20 ND
14 to18 y
1.2 ND 1.3 ND 16 30 5 ND 1.3 80 25 ND
19 to30 y
1.2 ND 1.3 ND 16 35 5 ND 1.3 100 30 ND
31 to50 y
1.2 ND 1.3 ND 16 35 5 ND 1.3 100 30 ND
51 to70 y
1.2 ND 1.3 ND 16 35 5 ND 1.7 100 30 ND
>70y
1.2 ND 1.3 ND 16 35 5 ND 1.7 100 30 ND
Females
9 to13 y
0.9 ND 0.9 ND 12 20 4 ND 1.0 60 20 ND
14 to18 y
1.0 ND 1.0 ND 14 30 5 ND 1.2 80 25 ND
19 to30 y
1.1 ND 1.1 ND 14 35 5 ND 1.3 100 30 ND
6
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
23 de 32 3/7/15, 10:20 AM
-
31 to50 y
1.1 ND 1.1 ND 14 35 5 ND 1.3 100 30 ND
51 to70 y
1.1 ND 1.1 ND 14 35 5 ND 1.5 100 30 ND
>70y
1.1 ND 1.1 ND 14 35 5 ND 1.5 100 30 ND
Pregnancy
14 to18 y
1.4 ND 1.4 ND 18 30 6 ND 1.9 80 30 ND
19 to30 y
1.4 ND 1.4 ND 18 35 6 ND 1.9 100 30 ND
31 to50 y
1.4 ND 1.4 ND 18 35 6 ND 1.9 100 30 ND
Lactation
14 to18 y
1.4 ND 1.6 ND 17 30 7 ND 2.0 80 35 ND
19 to30 y
1.4 ND 1.6 ND 17 35 7 ND 2.0 100 35 ND
31 to50 y
1.4 ND 1.6 ND 17 35 7 ND 2.0 100 35 ND
RDA: recommended dietary allowance; AI: adequate intake; UL:
upper tolerable level; d: day; mo:months; y: years.* The RDA is the
level of dietary intake that is sufficient to meet the daily
nutrient requirements of97 percent of the individuals in a specific
life stage group. The AI represents an approximation of the average
nutrient intake that sustains a definednutritional state, based on
observed or experimentally determined values in a defined
population. The UL is the maximum level of daily nutrient intake
that is likely to pose no risk of adversehealth effects in almost
all individuals in the specified life-stage or gender group.
Dietary Reference Intakes: The Essential Guide to Nutrient
Requirements. Otten JJ, Hellwig JP,Meyers LD (Eds), The National
Academies Press, Washington, DC 2006. pp.530-541. Reprinted
withpermission from the National Academies Press, Copyright 2006,
National Academy of Sciences.Sources: Dietary reference intakes for
Thiamin, Riboflavin, Niacin, Vitamin B , Folate, Vitamin B
,Panthothenic acid, Biotin, and Choline (1998); Dietary reference
Intakes for Vitamin C, Vitamin E,Selenium, and Carotenoids (2000).
These reports may be accessed via www.nap.edu.
Graphic 69963 Version 12.0
6 12
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
24 de 32 3/7/15, 10:20 AM
-
Atrophic glossitis
A smooth tongue that has lost its papillae and is often sore
suggest adeficiency in riboflavin, niacin, folic acid, vitamin B12
or iron. Thispatient had vitamin B12 deficiency.
Reproduced with permission from: Berg D, Worzala K. Atlas of
Adult PhysicalDiagnosis. Philadelphia: Lippincott Williams &
Wilkins, 2006. Copyright 2006 Lippincott Williams &
Wilkins.
Graphic 54472 Version 4.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
25 de 32 3/7/15, 10:20 AM
-
Physical signs of selected nutritional deficiency states
Signs Deficiencies
Hair Alopecia Protein-energy malnutrition
Brittle Biotin, Protein-energy malnutrition
Color change Protein-energy malnutrition
Dryness Vitamins E and A
Easy pluckability Protein-energy malnutrition
Skin Acneiform lesions Vitamin A
Follicular keratosis Vitamin A
Xerosis (dry skin) Vitamin A
Ecchymosis Vitamin C or K
Intradermal petechia Vitamin C or K
Erythema (especially where exposed tosunlight)
Niacin
Hyperpigmentation Niacin
Seborrheic dermatitis (nose, eyebrows,eyes)
Vitamin B2, Vitamin B6, Niacin
Scrotal dermatitis Niacin, Vitamin B2, Vitamin B6
Eyes Angular palpebritis Vitamin B2
Corneal revascularization Vitamin B2
Bitot's spots Vitamin A
Conjunctival xerosis, keratomalacia Vitamin A
Mouth Angular stomatitis Vitamin B12, Vitamin B2, Vitamin B6
Atrophic papillae Niacin
Bleeding gums Vitamin C
Cheilosis Vitamin B2, Vitamin B6
Glossitis Niacin, folate, vitamin B12, VitaminB2, Vitamin B6
Magenta tongue Vitamin B2
Extremities Genu valgum or varum, metaphysealwidening
Vitamin D
Loss of deep tendon reflexes of thelower extremities
Vitamins B1 and B12
Vitamin B1: thiamine; Vitamin B2: riboflavin; Vitamin B3:
niacin; Vitamin B6: pyridoxine; Vitamin
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
26 de 32 3/7/15, 10:20 AM
-
B12: cyanocobalamin.
Adapted from: Bernard MA, Jacobs DO, Rombeau JL. Nutrition and
Metabolic Support ofHospitalized Patients. WB Saunders,
Philadelphia 1986.
Graphic 78426 Version 2.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
27 de 32 3/7/15, 10:20 AM
-
Chemical structure of folate, vitamin C, pantothenate,biotin and
niacin
Graphic 57133 Version 4.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
28 de 32 3/7/15, 10:20 AM
-
Pellagra dermatitis
Dermatitis due to niacin deficiency (pellagra). The term
"pellagra"derives from the Italian words for "rough skin". The
condition ischaracterized by an erythematous, blistering rash that
may be pruriticor painful. The rash occurs in areas of sun
exposure, and is thereforeoften seen around the neck ("Casal's
necklace"), arms, hands, or malararea.
Reproduced with permission from: www.visualdx.com. Copyright
LogicalImages, Inc.
Graphic 69889 Version 6.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
29 de 32 3/7/15, 10:20 AM
-
Gingival abnormalities in scurvy
The gingival swelling and dusky color just above two of the
teethindicate hemorrhage into the gums of this patient with poor
dentition.The gingival abnormalities of scurvy occur only in the
presence of teeth,which presumably provide portals of entry for
microbes into the gums.One hypothesis suggests that vitamin C
deficiency impairs neutrophil-mediated killing of bacteria, leading
to chronic gingivitis, which is thencomplicated by bleeding from
the fragile vessels characteristic of scurvy.
Reproduced with permission from: Hirschmann JV, Raugi GJ. Adult
scurvy. JAm Acad Dermatol 1999; 41:895. Copyright 1999
Elsevier.
Graphic 76282 Version 3.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
30 de 32 3/7/15, 10:20 AM
-
Perifollicular abnormalities in scurvy
In this example, the perifollicular hyperkeratotic papules are
quiteprominent, with surrounding hemorrhage. These lesions have
beenmisinterpreted as "palpable purpura," leading to the mistaken
clinicaldiagnosis of vasculitis.
Reproduced with permission from: Hirschmann JV, Raugi GJ. Adult
scurvy. JAm Acad Dermatol 1999; 41:895. Copyright 1999
Elsevier.
Graphic 64172 Version 2.0
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
31 de 32 3/7/15, 10:20 AM
-
Disclosures: Sassan Pazirandeh, MD Nothing to disclose. Clifford
W Lo, MD, MPH, ScD Nothing to disclose. David L Burns, MDNothing to
disclose. Timothy O Lipman, MD Other Financial Interest: GI Board
Review Lecturer [Clinical nutrition]; Audio JournalClub Practice
Reviews in Gastroenterology [Clinical nutrition, gut microbiome,
complementary and alternative medicine, criticalreading skills].
Alison G Hoppin, MD Employee of UpToDate, Inc.Contributor
disclosures are reviewed for conflicts of interest by the editorial
group. When found, these are addressed by vettingthrough a
multi-level review process, and through requirements for references
to be provided to support the content. Appropriatelyreferenced
content is required of all authors and must conform to UpToDate
standards of evidence.Conflict of interest policy
Disclosures
Overview of water-soluble vitamins
http://www.uptodate.com/contents/overview-of-water-soluble-v...
32 de 32 3/7/15, 10:20 AM