Embed Size (px)
Citation preview
Overview of the Disease Burden of Invasive Pneumococcal Disease in Asia
L.C. Bravoa*, the members of the Asian Strategic Alliance for Pneumococcal Disease Prevention
(ASAP) Working Groupb
a University of the Philippines Manila, Manila, Philippines
b Asian Strategic Alliance for Pneumococcal Disease Prevention (ASAP) Working Group—Brunei:
Hajah Roslin Haji Sharbawi, Elizabeth S.F. Chong; Hong Kong: Chok-Wan Chan, Kenneth K.C. Lee;
Macau: Kin-Man Lui; India: Nitin Shah, Shyam Kukreja; Indonesia: Cissy Kartasasmita, Sri Rezeki
Hadinegoro; Korea: Hoan-Jong Lee; Malaysia: Musa bin Mohd Nordin, Nik Khairulddin Nik Yusoff,
Zulkifli Ismail; Pakistan: Iqbal Ahmad Memon, Sajid Maqbool, Zulfiqar A. Bhutta; Philippines:
Anna Lisa Ong-Lim, Cecilia C. Maramba; Singapore: Chia-Yin Chong, Daniel Y.T. Goh; Sri Lanka:
Sanath P. Lamabadusuriya; Taiwan: Cheng-Hsun Chiu, Ping-Ing Lee; Thailand: Somsak Lolekha,
Usa Thisyakorn
This article was prepared based on the members’ presentations at the third meeting of
the Asian Strategic Alliance for Pneumococcal Disease Prevention (ASAP) on 15 December 2007
in Seoul, Korea. This meeting was sponsored by an educational grant from Wyeth. This article
was also presented as an abstract at the Asian Congress of Pediatric Infectious Diseases,
Surabaya, Indonesia, 2–5 July 2008 (Poster presentation number P-PNE-001).
* Corresponding author at: National Institute of Health, University of the Philippines,
Manila, 623 Pedro Gil Street, Ermita 1000 Manila, Philippines. Tel.: +632 5269167; fax:
+632 5262397
Email address: [email protected] (L.C. Bravo)
ABSTRACT
This paper represents a collaborative effort by the Asian Strategic Alliance for Pneumococcal
Disease Prevention (ASAP) Working Group to collate data on the disease burden due to invasive
pneumococcal disease (IPD) in participating Asian countries and territories; namely, Brunei,
Hong Kong, India, Indonesia, Korea, Macau, Malaysia, Pakistan, the Philippines, Singapore, Sri
Lanka, Taiwan and Thailand. A review of both published and unpublished data revealed that the
incidence of IPD in some countries is well documented by way of large, long-duration studies,
while in other countries, much of the available data have been extrapolated from international
studies or have come from small population studies of limited geographical coverage. This paper
confirms that data regarding the incidence of IPD in Asia are grossly lacking and reinforces the
need for urgent and more substantial studies.
Running title: Pneumococcal disease in Asia
Keywords: Asia, bacteremia, cost effectiveness, epidemiology, immunization, invasive
pneumococcal disease, pneumonia, meningitis, serotypes
Introduction
Pneumococcal disease can be regarded as a serious global problem based on the
number of deaths attributed to it. The World Health Organization (WHO) estimates that 1.6
million die every year from the disease, 0.7 to 1 million of which are children aged < 5 years [1];
while community-based studies of invasive pneumococcal disease (IPD) and vaccine efficacy
trials reveal that approximately 814,000 pneumococcal deaths occur each year in children aged
< 5 years in developing countries, most of them in Asia and Africa [2].
The Asian region is unique in that, while it consists of developed and newly emerging
markets, it is still home to 600 million children living in absolute poverty and large numbers of
children < 5 years old dying from malnutrition, diarrhea and acute respiratory infections (ARIs)—
mostly pneumonia, malaria and vaccine-preventable diseases [3]. Reducing healthcare
inequalities remains a challenge for the region, and substantial differences in health coverage
may exist between the poorest and wealthiest groups within a single country; for example, in
India and the Philippines, the wealthiest people are three times more likely to receive care than
the poorest [4].
Health authorities in the region have yet to act on the need to protect all young children,
regardless of social background, against the life-threatening pneumococcal disease. Although
pharmacological interventions such as antibiotics and vaccines are available for treatment and
prevention, policymakers cite the lack of data on pneumococcal disease as reason for indecision
[5,6].While the United Nations Children’s Fund (UNICEF) and WHO report provides
epidemiological evidence on the burden of pneumonia in children (Table 1) [7], information on
pathogen-specific etiology is lacking. The number of published data from the region to confirm
the impact of IPD and specific clinical presentations is also limited.
For this reason, many Asian countries still have not included pneumococcal vaccination
in their national immunization programs even though the rationale for vaccination has long been
supported by studies. In light of the additional benefits of herd immunity and with the threat of
widespread antibiotic resistance, the inclusion of this vaccine can become a cost-effective
intervention with long-term benefits [8,9].
1. Collation of available data on pneumococcal disease in Asia
The Asian Strategic Alliance for Pneumococcal Disease Prevention (ASAP) was organized
in 2007 to raise awareness of the morbidity and mortality caused by pneumococcal disease and
of the importance of preventing the disease through surveillance and advocacy. It is composed
of healthcare professionals from 13 Asian countries and territories; namely, Brunei, Hong Kong,

India, Indonesia, Korea, Macau, Malaysia, Pakistan, the Philippines, Singapore, Sri Lanka, Taiwan
and Thailand.
This paper represents the collaborative effort of ASAP members to gather local-level
data on pneumococcal disease, both published and unpublished, taking into account the
incidences of pneumococcal disease and its clinical manifestations (meningitis, pneumonia, otitis
media and septicemia) stratified according to age, mortality and case fatality rates, serotype
distribution and antibiotic resistance. With this collection of data, ASAP will then be able to
determine the importance of pneumococcal disease in the region and generate a regional
consensus on essential issues. This information will also provide an impetus for health officials
and policymakers to create strategies to manage anticipated cases and, more importantly, to
prevent disease. Summaries of data gathered by ASAP members are presented in this paper and
individual study objectives are outlined in Table 2.
2. Summaries of data from ASAP countries and territories
3.1. Brunei
The WHO reports that the mortality rate for < 5-year-olds in Brunei is 9/1000 live births.
Pneumonia and related meningitis, sepsis/septicemia and other infections are the highest causes
of neonatal deaths, contributing 7% to total deaths [10]. Records from Raja Isteri Pengiran Anak
Saleha (RIPAS) hospital, the main referral hospital in Brunei, indicate that most pneumococcal-
positive samples in children < 12 years old came from those with respiratory tract infections (268
out of the total 316 samples; RIPAS hospital, unpublished data, 2007).
3.2. Hong Kong
3.2.1. Epidemiology
A retrospective, population-based study, which included records dated between 1995
and 2004, showed that the annual incidence of IPD requiring hospitalization in children aged
≤ 2 years old was 18.3/100,000 [11]. The incidence rate was 15.6/100,000 in children aged
≤ 5 years old. More recent data from 2000 to 2005 showed that the hospitalization rate with IPD
for children ≤ 2 years old was 23.7/100,000 person-years [12] and 16.1/100,000 person-years in
children ≤ 5 years old. Based on laboratory results from the Hospital Authority in Hong Kong, the
average annual incidences among children aged < 2 years and adults aged > 65 years old were
both 7.7/100,000 (95% CI 2–13/100,000) from 2000 to 2004 [13].
2.2.2. Serotype distribution
A study conducted by Ho et al. in 79 daycare centers and kindergartens in Hong Kong
(December 1999–June 2000) determined the serotype distribution of Streptococcus pneumoniae
from both nasopharyngeal and invasive isolates in children aged < 6 years [14]. The most
common carriage serotypes found were similar to the invasive isolates—that is, 6B, 14, 19F and
23F. Furthermore, the serotypes in the 7-valent pneumococcal conjugate vaccine (PCV7)
accounted for 89.7% and 66.1% of the carriage and invasive isolates, respectively. The serotypes
in PCV7—4, 6B, 9V, 14, 18C, 19F and 23F—accounted for 89.8% of all serotypes found in invasive
isolates taken from children (age ≤ 5 years) in five Hong Kong hospitals between 1995 and 2001
[14,15].
3.2.3. Antibiotic resistance
As of 2000, the overall prevalence rate of penicillin resistance among pneumococci was
49% in Hong Kong [14]. Retrospective data gathered from patients aged ≤ 2 and ≥ 65 years
admitted to five Hong Kong hospitals with pneumococcal bacteremia between 1995 and 2001
determined that 37.4% of S. pneumoniae isolates were nonsusceptible to penicillin and 63.4%
were resistant to clarithromycin [15]. In the same study, 3.8% of S. pneumoniae isolates were
resistant to levofloxacin.
Of 383 nasopharyngeal isolates from the 79 centers in the Ho et al. study, 42.0% were
penicillin sensitive, 32.1% were intermediate and 26.1% were resistant [14]. The isolates had
high rates of resistance to cefotaxime and erythromycin at 42.8% and 77.0%, respectively. The
same study included 88 pneumococci isolated from children with IPD who were hospitalized in
five Hong Kong hospitals [14]. Isolates were obtained from the blood, cerebrospinal fluid or
brain tissue of children 0–6 years old. Among this group of isolates, 52.3% were penicillin
sensitive, 31.8% were intermediate and 15.9% were resistant. The rates of resistance to
cefotaxime and erythromycin were 33.0% and 85.2%, respectively.
More recent data from 519 S. pneumoniae isolates from nasopharyngeal aspirates of
3157 children (age < 16 years old) in Hong Kong in 2005 and 2006 were included in a surveillance
study [16]. Results showed that 64.9% and 37.2% of the isolates were not susceptible to
penicillin and cefotaxime, respectively.
3.3. India
3.3.1. Epidemiology
The Invasive Bacterial Infection Surveillance (IBIS) group and the International Clinical
Epidemiology Network (INCLEN) conducted a prospective multicenter hospital-based
surveillance study in India and reported that, of the 314 patients identified as having IPD, 32.8%
of cases occurred in children aged ≤ 5 years, including 22.6% in children ≤ 2 years and 10.2% in
2–5-year-olds [17]. Of the 304 IPD patients whose clinical outcome was known, the case fatality
rate (CFR) was 22% in children aged < 2 years, 10% in 2–12-year-olds, 26% in 13–50-year-olds
and 28% in adults > 50 years. Meningitis was found to cause approximately one-third (34%) of
the fatalities, while septicemia caused 21% and pneumonia 19%.
The IBIS group extended to other South Asian countries and established surveillance
systems in Nepal and Sri Lanka through the South Asian Pneumococcal Alliance (SAPNA) project
[18]. A semi-annual technical report from SAPNA revealed that there were 1273 enrollees to the
study from October 2006 to March 2007. S. pneumoniae has been identified as pathogen in 28 of
the participants, and 11 of them are from India [19].
3.3.2 Serotype distribution
A prospective observational study by Jebaraj et al. found 6, 19, 15, 14 and 23 to be the
most common serotypes isolated from the nasopharynges of 100 infants attending a well baby
clinic in Vellore. These serotypes comprise 55% of the pneumococcal isolates found by the study
[20]. While the IBIS–INCLEN study identified more than 25 serotypes in the total population, the
most common serotypes in children aged < 5 years were 6, 1, 19, 14 and 4 [17]. The more recent
study by the SAPNA group reported the most prevalent serotypes to be 6B, 20, 16 and 1 [19].
3.3.3. Antibiotic resistance
The IBIS–INCLEN group also performed antimicrobial susceptibility testing on 307 S.
pneumoniae isolates, finding that intermediate resistance to penicillin was noted in only 1.3% of
the isolates tested, but that resistance to cotrimoxazole and chloramphenicol was seen 56% and
17% of the isolates, respectively [17]. The Asian Network for Surveillance of Resistant Pathogens
(ANSORP), a multicountry collaborative group for antimicrobial research, has observed that India
still has the lowest pneumococcal resistance to penicillin and erythromycin in the region [21,22].
3.4 Indonesia
3.4.1. Epidemiology
Records obtained from six hospitals in Jakarta, Surabaya, Bandung, Bali, Padang, and
Makassar from January to December 2006 revealed that of the 1796 children aged < 5 years
admitted due to IPD, 1425 (79.3%) had pneumonia, 283 (15.8%) had sepsis (bacteremia) and 88
(4.9%) had meningitis. The CFR was 29.2% and 21.0% in infants aged 1–11 months and 12–23
months, respectively, while the overall CFR attributable to IPD was 23.5% (Hadinegoro, in
press),[23,24].
A hospital-based study involving pediatric patients with acute purulent meningitis
showed that in 155 cases confirmed by cerebrospinal fluid (CSF) culture, the most common
etiological agents were Salmonella sp. (12.9%), Acinetobacter sp. (7.1%), S. pneumoniae (5.8%)
and Hemophilus influenzae (5.2%) [25], whereas a more recent study showed that of the 177
positive nasopharyngeal specimens from 698 patients between 2 and 5 years of age with
nonsevere pneumonia, 120 (67.8%) had S. pneumoniae, 21 (11.9%) had Staphylococcus
epidermidis and another 21 (11.9%) had alpha-streptococcus [26].
A pneumococcal nasopharyngeal carriage study in neonates showed that 38.9% of the
108 assessed had positive isolates: 0.9% in newborns; 2.8% at 2, 4, 6 and 8 weeks; 9.3% at
10 weeks; 12.0% at 13 weeks; and 13.9% at 15 weeks. The most common sources of
transmission were siblings (57.1%) and mothers (11.9%) [27].
Records of Sanglah Hospital in Bali identified 25 cases of meningitis between 2000 and
2005; three of these patients died. Hydrocephalus, hemiplegia, monoparesis, deafness and
epilepsy were found to be the most common sequelae [28].
3.4.2. Serotype distribution and antibiotic resistance
A pneumococcal carriage study conducted in Lombok involving 484 healthy children
aged 0–25 months found pneumococcal isolates in 221 (48%) children. The most common
serogroups were 6, 23, 15, 33 and 12. Sixty-one percent of the isolates found are covered by the
current PCV7. Susceptibility testing revealed that 2.2% of the 221 specimens were
nonsusceptible to penicillin and 0% were nonsusceptible to cefotaxime [29].
3.5. Republic of Korea
3.5.1. Epidemiology
While there are no published data on the incidence rate of pneumococcal disease in
Korea, a survey of 13 hospitals found that S. pneumoniae (30%) is the most common invasive
pathogen among Korean children, especially among the immunocompromised and patients aged

3 months to 5 years (Lee HJ, unpublished data, 2007). In the same survey, the most common
clinical features of IPD in immunocompetent children were meningitis (39%) and bacteremic
pneumonia at 35%, whereas, in immunocompromised children, the most common clinical
features were bacteremia without focus (48%) and meningitis (18%).
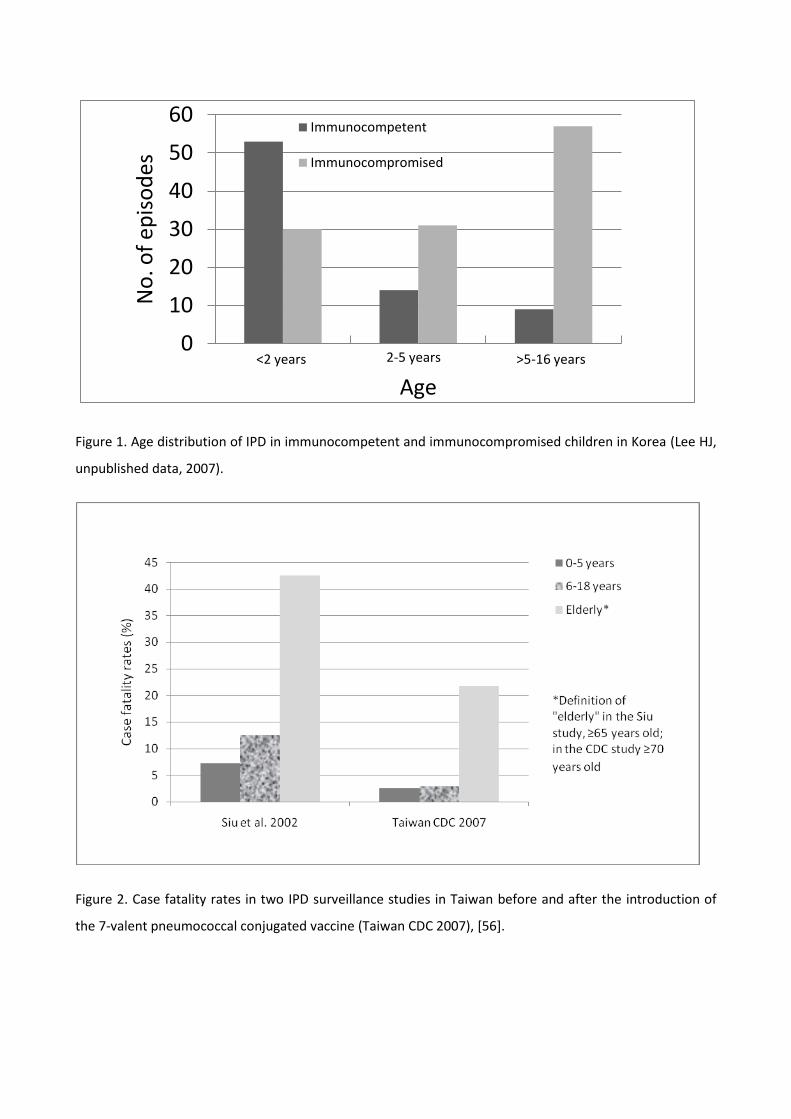
Among the immunocompetent children, IPD was most common in children aged
< 2 years, with incidence declining as age increased. In the immunocompromised children,
however, IPD episodes did not decrease with increasing age (Fig. 1). The CFR for children with
IPD was 12% (27/222): 13% (19/144) for immunocompetent children and 10% (8/78) for
immunocompromised children (Lee HJ, unpublished data, 2007).
3.5.2. Serotype distribution
A study evaluating serotype distribution among isolates from various clinical specimens
at Seoul National University Children’s Hospital from 1991 to 2006 showed that the most
common serotypes were 19F (21.0%), 23F (17.8%), 19A (10.8%), 6B (9.3%), 6A (8.0%), 14 (7.4%)
and 9V (4.5%) [30]. Between 1991 and 2003, it was observed that the proportion of 19A isolates
increased from 0 to 26% while 19F decreased during the same period. From 2001 to 2003, just
prior to the introduction of the pneumococcal vaccine, serotypes covered by the vaccine
accounted for 57% of isolates while vaccine-related serotypes accounted for another 24%.
Although the serotype distribution of isolates changed after the introduction of pneumococcal
vaccine in 2004, similar trends were observed, i.e. the proportion of serotypes covered by the
vaccine were decreasing and the increase of 19A became more evident from 2004 to 2006 [30].
3.5.3. Antibiotic resistance
The studies conducted by ANSORP showed that S. pneumoniae isolates from Korea have
a consistently high rate of penicillin resistance (1996–1997: 55.4%; 1998–1999: 31.3%; 2000–
2001: 54.8%) [21] and erythromycin resistance (1996–1997: 74.6%; 1998–2001: 85.1%) [22].
3.6. Macau
Macau is a small city south of China and Hong Kong with only two hospitals and no
serotyping facility. A review of records dated 2001–2007 from the public acute care hospital
Centro Hospitalar Conde Säo Januário found only one IPD case—a pneumococcal meningitis case
(Kin-Man Lui, personal communication, 2007). PCVs are provided free by the government for
high-risk groups: premature infants and those with complex heart diseases.
3.7. Malaysia
3.7.1. Epidemiology
Published studies on pneumococcal infection in Malaysia have shown pneumonia to be
its most common clinical presentation, with morbidity and mortality being highest in children
aged < 2 years [31,32]. A more recent hospital-based study confirmed this finding by showing
that majority of the cases occurred in patients aged < 2 years and that definite pneumonia,
probable pneumonia, meningitis, bacteremia without focus and septic arthritis were the most
common types of IPD in Malaysian patients. Those with meningitis had the highest rate of long-
term complications [33]. Earlier studies on childhood meningitis in Malaysia showed that most
cases occurred in those < 5 years of age and that H. influenzae and S. pneumoniae were the most
common causative organisms [34,35,36]. As the H. influenzae type b (Hib) vaccine was
incorporated in the country’s national immunization program in 2002, it is presumed that S.
pneumoniae is now the leading cause of meningitis in Malaysia.
However, there are no published data to date on the incidence of invasive
pneumococcal infection post-Hib vaccination except for a paper by Suhaimi, which reported on a
single-center retrospective study conducted at Queen Elizabeth Hospital in Kota Kinabalu
evaluating the incidence of childhood meningitis both before the introduction of Hib vaccine
(January 1999–December 2001) and afterwards (January 2004–December 2006). This study
showed that the incidence of pneumococcal meningitis increased following the introduction of

Hib vaccination (3.7 vs. 8.6/100,000 per year in children aged < 5 years) [37]. Larger studies
involving more centers in Malaysia are needed to confirm this finding.
3.7.2. Serotype distribution
Several studies have documented the serotype distribution in Malaysia with differing
results. Rohani et al. reported that the most common serotypes that cause IPD in children aged
< 2 years were 1, 5, 23B, 2, 8, 14, 20, 6A, 12A, 19B and 23B [32]. Cheong et al. looked at
pneumococcal serotypes isolated from children aged < 5 years presenting with ARI in three
centers in Malaysia and the most common serotypes isolated were 19F, 6A and 23F [38]. A 4-
year prospective study was also undertaken by Jamal and colleagues in Kuala Lumpur and, out of
43 isolates in children aged < 12 years with pneumococcal disease, the most common serotypes
were 6A (25.6%), 6B (16.3%) 14 (18.6%) and 19A (18.6%) [31]. Currently, a prospective
multicenter study is underway to evaluate IPD incidence and serotype prevalence in hospitalized
children (N.K. Nik Yusoff, personal communication, 2008).
3.7.3. Antibiotic resistance
The ANSORP study showed that pneumococcal disease serotypes prevalent in Malaysia
have a considerable degree of resistance to penicillin (29.5%) and erythromycin (34.1%) [21].
3.8. Pakistan
3.8.1. Epidemiology
A previous systematic review of all national published studies by Bhutta revealed that
pneumonia and meningitis account for over 85,000 childhood deaths and cases of disability in
infancy in Pakistan and that 33% of these are attributable to infections caused by S. pneumoniae
and H. influenzae [39]. These results have recently been updated and indicate that the
proportion of meningitis cases attributable to S. pneumoniae and H. influenzae may be higher in
recent studies (Bhutta et al. unpublished observations, 2008). The 2007 Pakistan Demographic
and Health Survey indicates that 25.7% and 9.1% of all postneonatal child deaths in Pakistan
were related to pneumonia and meningitis, respectively [40]. These figures are remarkably
similar to the estimates obtained earlier by Bhutta [39].
A number of community- and hospital-based studies provide an overview of the etiology
of ARIs among children < 5 years old in Pakistan. In a census conducted in four periurban
communities, Nizami et al. isolated S. pneumoniae in 3.7% of a total of 791 oropharyngeal swab
cultures and calculated the S. pneumoniae burden in these communities to be 3.0/1000 children
[41]. Using the same technique, Rehman and colleagues identified 139 positive cultures from
500 pediatric patients at Bahawal Victoria Hospital in Bahawalpur; 36 of the 139 (25.9%) were S.
pneumoniae positive [42]. Ghafoor et al. meanwhile reported that, of the 1331 blood specimens
included in their study, H. influenzae was the leading bacterial isolate (11% of the cases)
followed by S. pneumoniae (10%) [43].
3.8.2. Serotype distribution and antibiotic resistance
Serotypes 6, 9, 15, 16, 19 and 31 comprised 60% of the S. pneumoniae isolates found in
the study by Ghafoor et al. [43]. This finding was confirmed by Mastro and colleagues who
reported a year later that the most common serotypes detected were 19F, 31, 16, 19A, 9V, 15C
and 6A. They also tested 87 strains of S. pneumoniae isolates for antimicrobial susceptibility and
found that 97% had decreased susceptibility to at least one antimicrobial agent: 31% were fully
resistant to cotrimoxazole, 39% were resistant to chloramphenicol and 9% were moderately
resistant to penicillin [44]. Recent data on antimicrobial sensitivity patterns of respiratory
isolates of S. pneumoniae and H. influenzae also confirm increasing resistance to cotrimoxazole
and penicillin.
3.9. Philippines
3.9.1. Epidemiology
Statistics from the Philippines’ Department of Health (DOH) in 2000 attributed child
mortality rates of 37.8/100,000 to pneumonia, 4.7/100,000 to meningitis and 4.5/100,000 to
septicemia, although the statistics do not describe pathogen-specific causality [45].
A few hospital- and community-based studies have examined the etiology of infections
in children aged < 5 years with pneumonia, bacteremia and meningitis. In a study by Lupisan et
al., S. pneumoniae was found to be the leading isolate among blood cultures (1.3% of the total
from an overall culture positivity of 8.9%) [46]; while Capeding et al. documented S. pneumoniae
in 3.7% of acute lower respiratory tract infections and in 35.0% of patients with confirmed
bacteremia [47].
Data on the frequency distribution of bacterial meningitis from three tertiary hospitals in
Metro Manila have shown that S. pneumoniae and Hib are the most prevalent etiological agents
(Philippine General Hospital; Philippine Children’s Medical Center; University of Santo Tomas
Hospital, unpublished data, 2002–2006). The mortality rate in patients positive for S.
pneumoniae was 23.5% compared to 5.0% for patients with Hib.
3.9.2. Serotype coverage and antibiotic resistance
A study of nasopharyngeal samples from Filipino children with ARI showed serotypes 6,
14, 19 and 23 to be the most common [48], while in a recent study among children with IPD, the
most common serotypes were 6, 18, 14 and 5 [49]. Pneumococcal antibiotic resistance is low in
the Philippines at 1% for penicillin, 5% for chloramphenicol and 18% for cotrimoxazole [50].
3.10. Singapore
3.10.1. Epidemiology
A retrospective review of more than 4000 hospital records from 1995 to 2004 in
Singapore indicated that children aged < 5 years and adults aged ≥ 65 years were most
susceptible to pneumococcal disease, with hospitalization rates of 38.4/100,00 and
56.4/100,000, respectively [51]. Pneumococcal pneumonia was the most common disease

manifestation (97.9%), followed by septicemia (1.1%) and meningitis (0.7%). The CFR for all age
groups in this study was 3.2%. Cause of death was primarily attributable to pneumococcal
meningitis, followed by septicemia and pneumococcal peritonitis, and pneumococcal
pneumonia.
A retrospective survey among all pneumococcal-positive patients (n=146; aged 3 months
to 19.5 years) admitted to Kandang Kerbau Women’s and Children’s Hospital from 1997 to 2004
showed that 46.9% of these patients were between the ages of 2 and 5 years, with a mean age
of 45 months. Pneumonia (63.3%) was also the most common form of IPD, followed by
bacteremia (17%) and meningitis (15.6%). The morbidity rate was found to be 25.2% and the
mortality rate 6.1%. Using the country’s 2005 population estimates, IPD incidence was found to
be 13.6/100 000 in children < 5 years and 16.9/100,000 in children < 2 years [52].
3.10.2. Serotype coverage and antibiotic resistance
The four most common serotypes in the pediatric population were found to be 14
(21.8%), 6B (10.2%), 23F (10.1%), 19F (5.4%) and 6A (3.4%). Overall penicillin resistance was at
44.4%, most of which were observed in serotypes 14 and 19F, whereas resistance to ceftriaxone
was 15.0% [52].
3.11. Sri Lanka
3.11.1. Epidemiology
One of the largest Sri Lankan children’s hospitals, the Lady Ridgeway Hospital for
Children (LRH) in Colombo, reported 794 pneumonia cases and 295 meningitis cases in 2003, of
which 32 and 9 died, respectively (LRH, Annual Health Bulletin, 2003 unpublished), while SAPNA
reported in 2005 that of 228 patients from LRH, 75% had pneumonia, 8% had meningitis and 4%
had septicemia. Nine of these patients were found to have IPD [53]. In SAPNA’s semi-annual
technical report, 10 of the 28 participants identified with S. pneumoniae as pathogen were from
Sri Lanka [19]
Being one of the hardest hit countries by the December 2004 tsunami, Sri Lanka has data
available on the prevalence and transmission of ARIs caused by S. pneumoniae and H. influenzae
in the evacuation camps. Nasopharyngeal swabs were collected from 324 displaced people
staying in three different camps and 21 H. influenzae isolates from 20 people and 25
S. pneumoniae isolates from 22 were identified. It is suggested that some of these infections
may have been transmitted from person to person while staying in the camps [54].
3.11.2. Serotype distribution and antibiotic resistance
The most prevalent serotypes in Sri Lanka are 23F, 19F and 14 [53, 21]. Isolates have
shown markedly increased penicillin resistance (1996–1997: 0.0%; 1998–1999: 5.9%; 2000–
2001: 14.3%) in the course of the ANSORP studies [21]. Ciprofloxacin resistance is also high at
11.8%. The SAPNA study also revealed high penicillin resistance at 22% and cotrimoxazole
resistance at 67%.
3.12. Taiwan
3.12.1 Epidemiology
In 2006, data from the Bureau of National Health Insurance suggested that the overall
incidence of IPD in Taiwan was 216/100,000. Adults aged > 65 years old had the highest
incidence (1147/100,000), followed by children aged < 5 years (422/100,000). The incidence of
pneumonia showed a reversed trend, being highest among children aged < 5 years at
45,956/100,000 [55]. This differs substantially from UNICEF–WHO report where the incidence of
pneumonia among children aged < 5 years in East Asia and the Pacific was estimated to be
23,000/100,000 [7]. The incidences of septicemia and meningitis in children aged < 5 years were
1095/100,000 and 185/100,000, respectively. The IPD mortality rate was highest in the elderly
(> 65 years), mainly due to pneumonia (30,806/10,000) [55].

In a study conducted by Siu et al. from July 1998 to June 1999, the CFR for IPD was
highest among the elderly (≥ 65 years; 42.5%) and children ≤ 5 years (7.2%) [56]. A similar trend,
but reduced CFR, was observed in an island-wide IPD surveillance study conducted from January
to November 2007—two years after PCV7 was introduced in Taiwan. The CFRs were 21.7% in the
elderly (≥ 70 years) and 2.5% in children aged ≤ 5 years (Fig. 2) (Taiwan Center for Disease
Control and Prevention [CDC], unpublished data, 2007).
3.12.2. Serotype coverage and antibiotic resistance
Serotype 14 predominated in children aged ≤ 5 years with IPD, followed by 19F, 23F, 6B
and 19A. Penicillin susceptibility testing showed S. pneumoniae to be 65–70% resistant, while
resistance to ceftriaxone was 38% (Taiwan CDC, unpublished data, 2007).
3.13. Thailand
3.13.1. Epidemiology
Two studies have reported on the etiology of ARI in young Thai children. Sunakorn et al.
performed a study between 1988 and 1989 among children admitted to the Queen Sirikit
National Institute of Child Health (formerly known as the Children’s Hospital Bangkok) and found
that the most severe ARI cases were in children aged < 2 years. Most cases were caused by Hib
and few cases by S. pneumoniae [57]. In the second study, Ekalaksananan et al. reported that
pneumonia presented most frequently in children aged < 1 year, with S. pneumoniae and H.
influenzae contributing equally to the number of cases. Viral and bacterial co-infection was also
detected [58].
The Bureau of Epidemiology of the country’s Ministry of Public Health (MOPH) reported
that, from 1999 to 2005, the incidence rate of pneumonia among children aged < 5 years was
about 1500–2000/100,000 (Bureau of Epidemiology, MOPH, unpublished data, 2006).
A population-based survey in the provinces of Sa Kaeo and Nakhon Phanom, conducted
by the MOPH and the surveillance network of the International Emerging Infections Program
(IEIP) detected a minimum IPD incidence of 4/100,000 by blood culture. The highest IPD
incidence occurred in children aged < 5 years (8.8–12.3/100,000) and in the elderly ≥ 75 years
(26/100,000); this was compounded by substantial antibiotic resistance, with vaccine serotypes
found to be especially resistant (IEIP, unpublished data, 2007). Childhood meningitis was studied
by Chotpitayasunondh who found that Hib (42.3%) and S. pneumoniae (22.2%) were the leading
causative organisms [59].
3.13.2. Serotype coverage and antibiotic resistance
In a recent study, Phongsamart et al. found that the most common S. pneumoniae
serotypes were 6B (27.8%), 23F (20.0%), 14 (10.4%) and 19F (9.6%). Seventy-four percent of
these serotypes are covered by PCV7 and 88% are covered by the 13-valent PCV (PCV13).
Seventy percent were found to be penicillin resistant [60]. In another study, Levine et al. showed
that, among rural children aged < 5 years, nasopharyngeal colonization was 60%, with 6B, 19F
and 23F being the most common serotypes isolated. About 55% of the serotypes found were
covered by PCV7 and 68% were penicillin nonsusceptible strains [61].
3. Discussion
The collection of data from the ASAP members confirms that pneumococcal disease is
an important cause of morbidity and mortality in the Asian region. Overall CFRs resulting from
IPD, as reported by studies from India, Indonesia, Singapore and Taiwan, are illustrated in
Figure 3. In many of the studies, pneumonia was identified as the most common clinical
manifestation. Interestingly, four ASAP member countries, namely, India (with 44 million
pneumonia cases), Pakistan (7 million), Indonesia (6 million) and the Philippines (3 million) were
among the 15 countries identified by both UNICEF–WHO and Rudan et al. as accounting for

three-quarters of the total childhood pneumonia cases worldwide. Both reports identified S.
pneumoniae as the leading pathogen [7,62].
The high antimicrobial resistance of S. pneumoniae in Asia contributes to both the
treatment and economic burden caused by IPD [21,22,63]. In the ANSORP studies, Korea, Taiwan
and Thailand have consistently shown high rates of penicillin resistance [21]. The judicious use of
antibiotics and promotion of vaccination have been suggested as methods to control these
resistant infections [8]. However, pneumococcal vaccination is currently not part of the national
immunization programs of any of the ASAP member countries and territories, despite it being
projected to prevent around 260,000 deaths annually as well as having the potential to mitigate
widespread antibiotic resistance [64].
Rinaldi and Chong confirmed that vaccination of infants with PCV7 would lead to a
substantial reduction in the incidence of IPD, not only among children but also in adults due to
herd protection conferred by immunization [65]. Using a decision-analytic model previously used
in the United Kingdom, Lee et al. evaluated the clinical and economic benefits of routine infant
immunization with PCV7 in Hong Kong and found that 524 cases of IPD and over 2580 cases of
otitis media were potentially prevented over a 10-year period, leading to a reduction of at least
HK$35 million (US$4.5 million) in direct medical costs. The study also took into account the
additional cost savings from the indirect prevention of 919 adult cases of IPD during the same
period. Universal PCV7 vaccination was estimated to have an incremental cost per life-year gain
of HK$44,644 (US$5718) [66].
IPD incidences in Hong Kong, Singapore and Taiwan have been documented by way of
long-duration national studies, with the objective of understanding the epidemiology of invasive
S. pneumoniae. However, the primary objectives of the studies from other ASAP member
countries were to determine the bacterial etiology of ARI, pneumonia, or meningitis; to assess
antimicrobial sensitivity; to describe the dynamics of nasopharyngeal colonization; or to
determine serotype distribution of S. pneumoniae. Data from some countries were also obtained
from very small studies with limited geographic coverage or were extrapolated from results of
international studies. In addition, it is likely that the IPD incidence in some of the studies was
underestimated given the inherent limitation of blood cultures. Moreover, not all meningitis
cases were confirmed by CSF cultures and outpatient pediatric bacteremia cases were not
reported. These differences in study objectives, methodologies and reporting criteria, as well as
the limited coverage prevent comparative analysis and the estimation of regionwide burden of
disease.
IPD is currently not a notifiable disease in any of the ASAP member countries and
territories—with the exception of Taiwan—and no comprehensive and standardized laboratory
surveillance system for IPD has been established. A surveillance system is needed to provide
valuable data on serotype distribution, antibiotic resistance and the impact of vaccination. This
also has to be supported by statistical models and clinical trial results to be able to accurately
estimate disease burden [67,68]. Currently, several surveillance projects and clinical studies are
being conducted in Asia that will be able to provide a more accurate estimate of the
epidemiology and impact of IPD in the region [67].
4. Conclusion
This review of available data confirms the substantial burden of IPD and prevalence of
antibiotic resistance of pneumococci in the Asian region. High incidence is observed in both
children aged < 2 years and adults aged > 65 years. Incidence rates vary between countries.
More substantial and specific studies and continued surveillance are therefore needed to better
assess the incidence of IPD throughout Asia and be able to develop strategies for prevention and
management. The collection of studies also highlights the need to strengthen ARI management
programs. Lastly, the overview of disease burden due to IPD emphasizes the need to deliver
effective interventions, such as early recognition and treatment, prevention through vaccination
and methods to address increasing antimicrobial resistance.

Acknowledgements
This study was supported by an unrestricted educational grant from Wyeth to ASAP. Wyeth was
not involved in the editorial direction of this paper.
With the exception of Zulfiqar A. Bhutta, all authors have received honoraria, lecture fees and
travel grants from pharmaceutical companies involved in pneumococcal and invasive Hib disease
therapeutics, and have declared past funding from Wyeth for related work.
The authors thank Tina V. Garcia of In Vivo Communications Ltd for medical writing assistance.
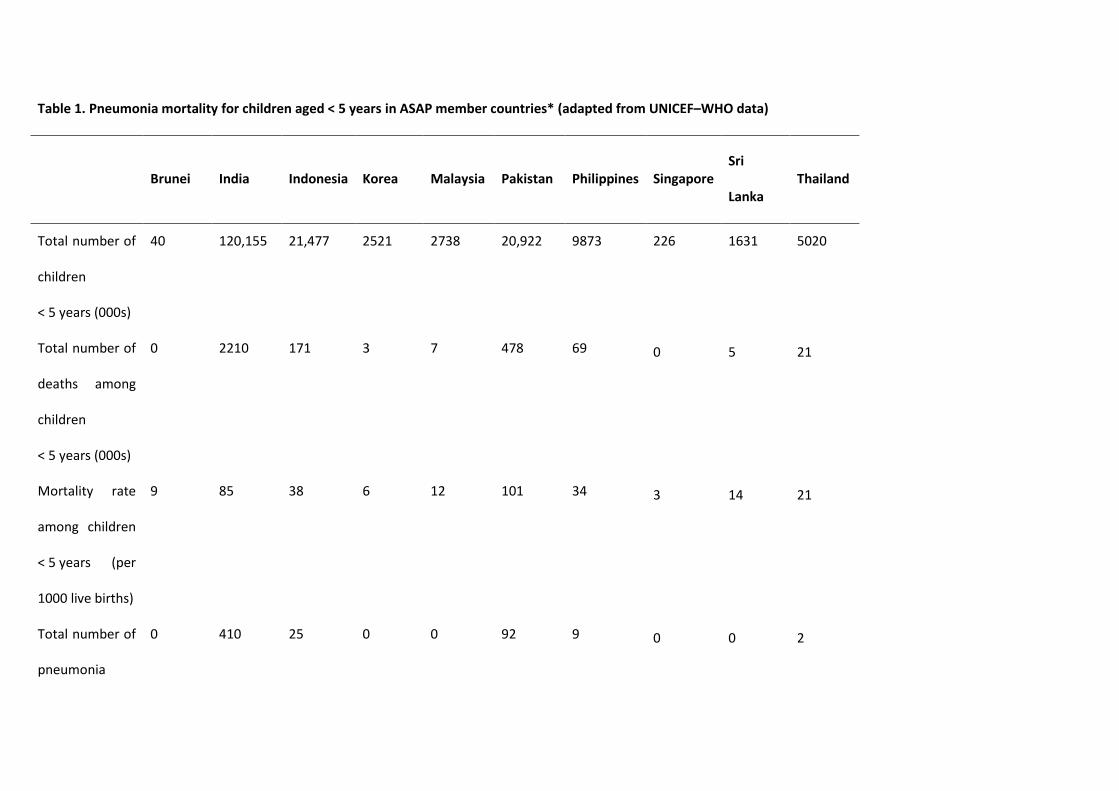
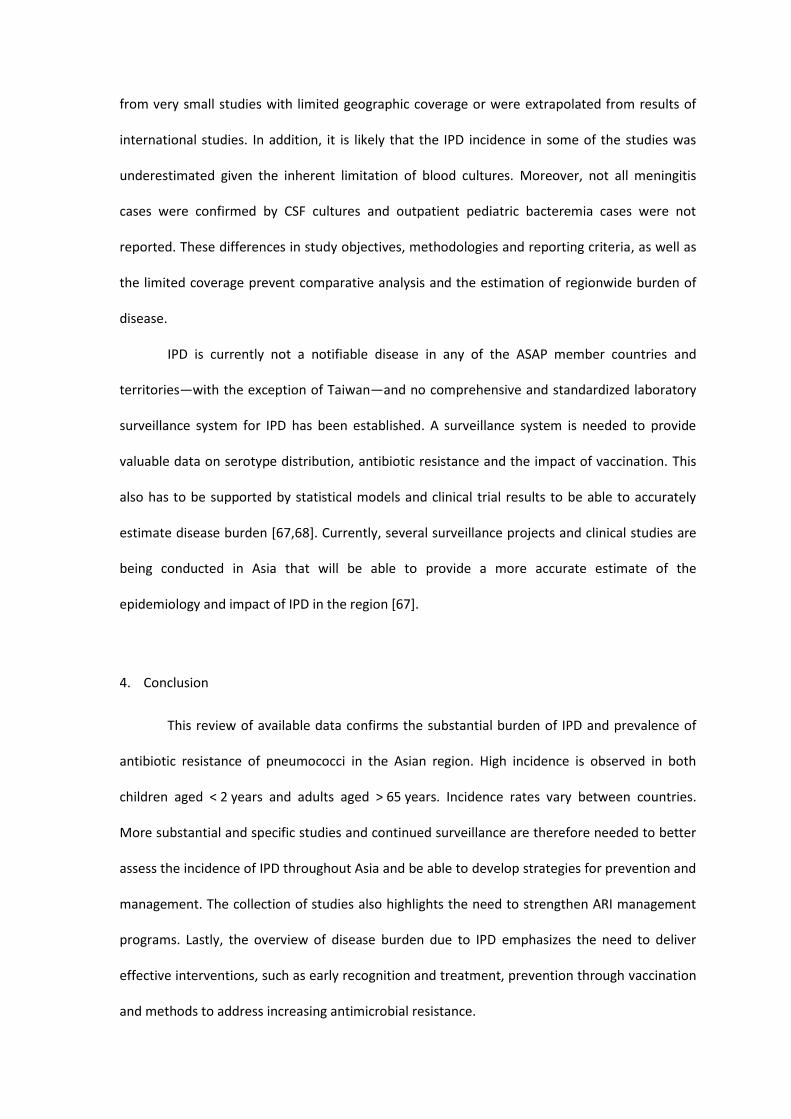
Table 1. Pneumonia mortality for children aged < 5 years in ASAP member countries* (adapted from UNICEF–WHO data)
Brunei India Indonesia Korea Malaysia Pakistan Philippines Singapore Sri
Lanka Thailand
Total number of
children
< 5 years (000s)
40 120,155 21,477 2521 2738 20,922 9873 226 1631 5020
Total number of
deaths among
children
< 5 years (000s)
0 2210 171 3 7 478 69 0 5 21
Mortality rate
among children
< 5 years (per
1000 live births)
9 85 38 6 12 101 34 3 14 21
Total number of
pneumonia
0 410 25 0 0 92 9 0 0 2
Brunei India Indonesia Korea Malaysia Pakistan Philippines Singapore Sri
Lanka Thailand
deaths among
children
< 5 years (000s)
Case fatality
rate in children
aged < 5 years
1% 19% 14% 2% 4% 19% 13% 9% 9% 11%
*Hong Kong SAR ceased to be a WHO member state in 1997 and thus was excluded from the world health reports. Taiwan and Macau are represented in the WHO system by China
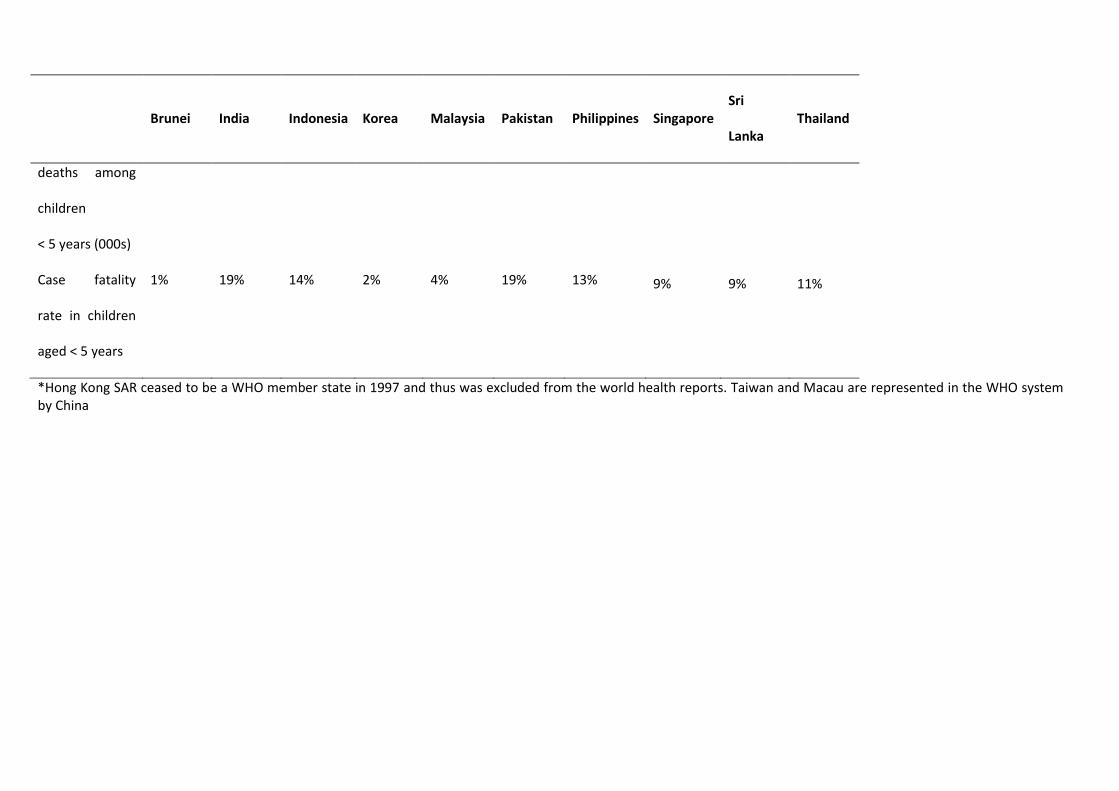
Table 2. Summary of sources
Objectives
Brunei
Raja Isteri Pengiran Anak Saleha
(RIPAS) hospital. Unpublished
hospital data. 2007
To document hospital admissions
WHO. Mortality country fact sheet
2006. Brunei Darussalam
To provide country-specific information on size of population, life
expectancy, under-5 mortality, adult mortality, and maternal
mortality
Hong Kong
Ho PL, Que TL, et al. 2004 [15] To evaluate activities of fluoroquinolones against invasive isolates
of S. pneumoniae
Ho PL, Lam KF, et al. 2004 [14] To determine vaccine coverage of prevalent carriage and invasive
pneumococci among children aged < 6 years in Hong Kong
Ho PL et al. 2006 [11] To estimate the age-specific incidence of IPD in Hong Kong from
1995 to 2004
Ho PL et al. 2007 [12] To estimate the hospitalization rates for pneumococcal disease
among children in Hong Kong from 2000 to 2005
Ip M et al. 2007 [16] To examine the serotypes and antibiotic susceptibility of S.
pneumoniae strains from nasopharyngeal aspirates of children aged
> 1 month to 15 years with ARI
Scientific Committee on Vaccine
Preventable Diseases. 2007 [13]
To provide scientific advice on vaccine use for the population
India
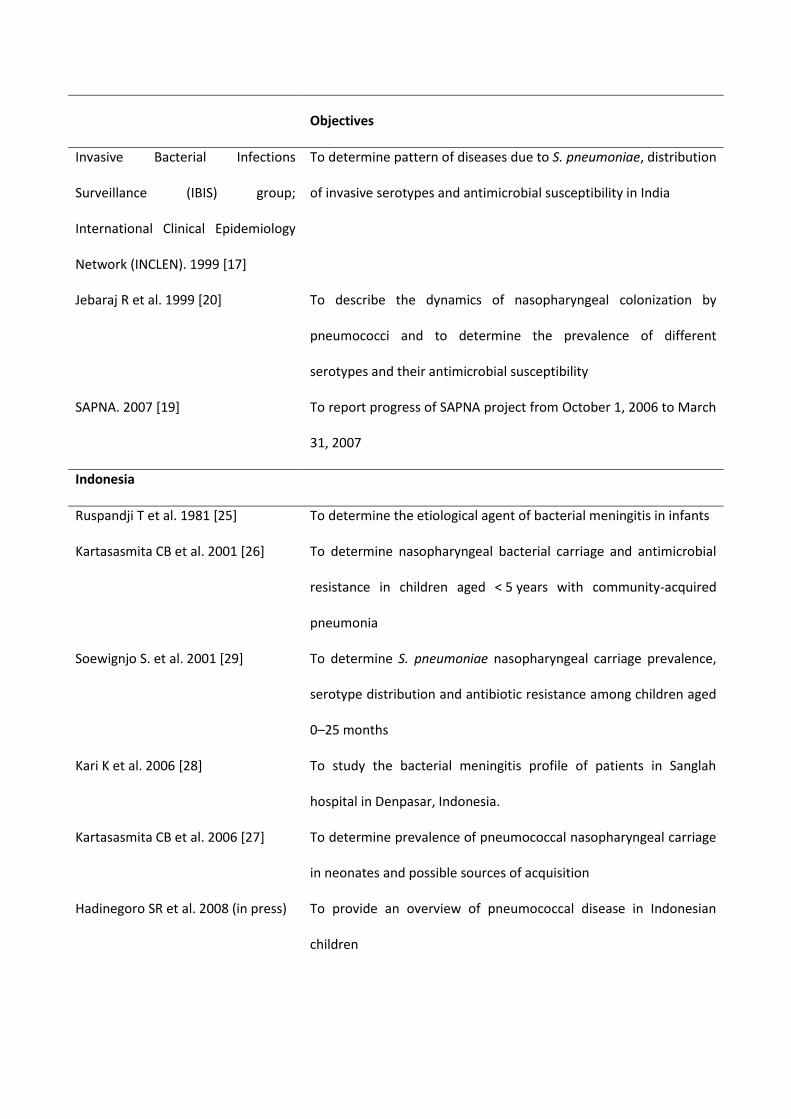
Objectives
Invasive Bacterial Infections
Surveillance (IBIS) group;
International Clinical Epidemiology
Network (INCLEN). 1999 [17]
To determine pattern of diseases due to S. pneumoniae, distribution
of invasive serotypes and antimicrobial susceptibility in India
Jebaraj R et al. 1999 [20] To describe the dynamics of nasopharyngeal colonization by
pneumococci and to determine the prevalence of different
serotypes and their antimicrobial susceptibility
SAPNA. 2007 [19] To report progress of SAPNA project from October 1, 2006 to March
31, 2007
Indonesia
Ruspandji T et al. 1981 [25] To determine the etiological agent of bacterial meningitis in infants
Kartasasmita CB et al. 2001 [26] To determine nasopharyngeal bacterial carriage and antimicrobial
resistance in children aged < 5 years with community-acquired
pneumonia
Soewignjo S. et al. 2001 [29] To determine S. pneumoniae nasopharyngeal carriage prevalence,
serotype distribution and antibiotic resistance among children aged
0–25 months
Kari K et al. 2006 [28] To study the bacterial meningitis profile of patients in Sanglah
hospital in Denpasar, Indonesia.
Kartasasmita CB et al. 2006 [27] To determine prevalence of pneumococcal nasopharyngeal carriage
in neonates and possible sources of acquisition
Hadinegoro SR et al. 2008 (in press) To provide an overview of pneumococcal disease in Indonesian
children

Objectives
Nyambat B, Purniti PS, et al. 2008
[23]
To conduct a hospital review of syndromes consistent with IPD in
children in Denpasar, Indonesia
Nyambat B, Dijanto I, et al. 2008 [24] To conduct a baseline assessment on the burden of IPD syndromes
in children by reviewing hospital records in a referral center in
Surabaya, Indonesia
Korea
Lee HJ. Unpublished hospital data.
2007
To identify major pathogens of invasive diseases in Korean children
Choi EM et al. 2008 [30] To describe S. pneumoniae serotype distribution changes, with an
emphasis on serogroup 19
Malaysia
Jamal F et al. 1987 [31] To describe the clinical features and outcomes of systemic
pneumococcal infection
Cheong YM et al. 1988 [38] To describe the antibiotic susceptibility pattern and serotypes of the
pneumococcal strains
Choo KE et al. 1990 [34] To study retrospectively pyogenic meningitis in hospitalized children
in Kelantan, Malaysia, with regard to etiology, clinical features,
investigation, treatment and outcome
Tee AC. 1993 [35] To determine the relationship of presenting features and outcome
in primary childhood meningitis among patients admitted to the
pediatric department of University Hospital Kuala Lumpur from
1980 to 1989
Hussain IHM et al. 1998 [36] To determine the pattern of post neonatal childhood meningitis in
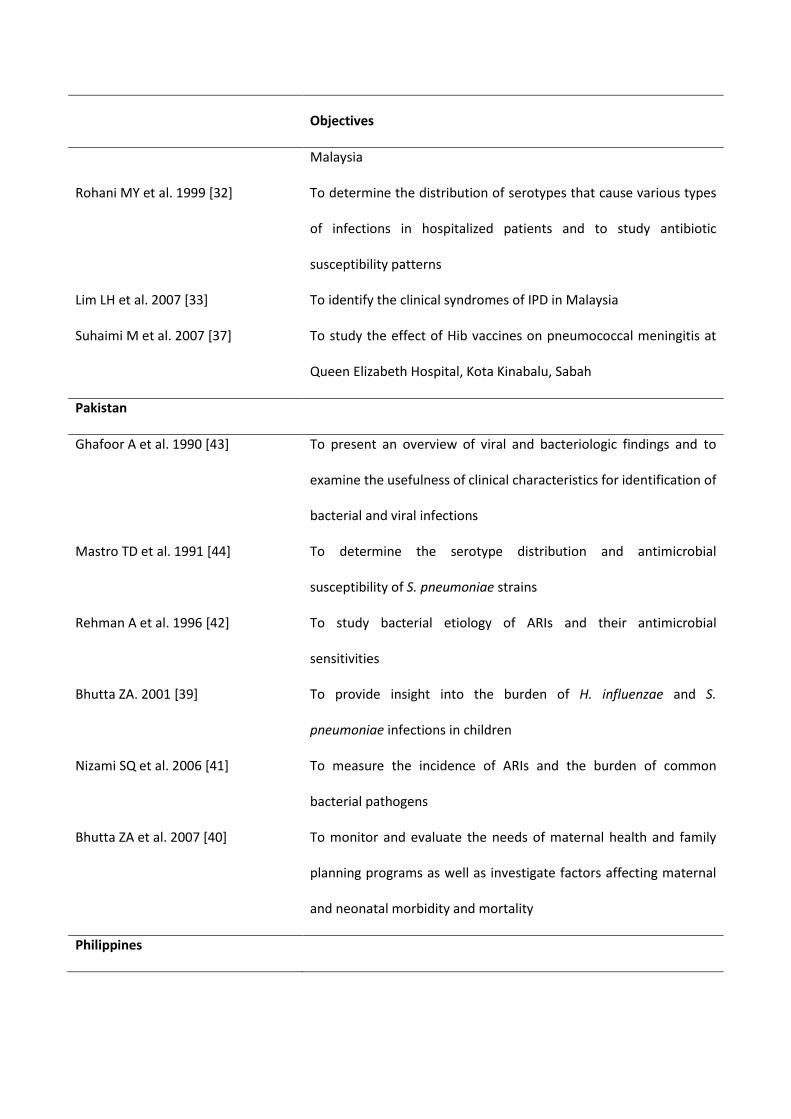
Objectives
Malaysia
Rohani MY et al. 1999 [32] To determine the distribution of serotypes that cause various types
of infections in hospitalized patients and to study antibiotic
susceptibility patterns
Lim LH et al. 2007 [33] To identify the clinical syndromes of IPD in Malaysia
Suhaimi M et al. 2007 [37] To study the effect of Hib vaccines on pneumococcal meningitis at
Queen Elizabeth Hospital, Kota Kinabalu, Sabah
Pakistan
Ghafoor A et al. 1990 [43] To present an overview of viral and bacteriologic findings and to
examine the usefulness of clinical characteristics for identification of
bacterial and viral infections
Mastro TD et al. 1991 [44] To determine the serotype distribution and antimicrobial
susceptibility of S. pneumoniae strains
Rehman A et al. 1996 [42] To study bacterial etiology of ARIs and their antimicrobial
sensitivities
Bhutta ZA. 2001 [39] To provide insight into the burden of H. influenzae and S.
pneumoniae infections in children
Nizami SQ et al. 2006 [41] To measure the incidence of ARIs and the burden of common
bacterial pathogens
Bhutta ZA et al. 2007 [40] To monitor and evaluate the needs of maternal health and family
planning programs as well as investigate factors affecting maternal
and neonatal morbidity and mortality
Philippines

Objectives
Capeding MRZ et al. 1994 [47] To determine the etiology of acute lower respiratory infection in
children under 5 years old
Lankinen KS et al. 1994 [48] To compare the sensitivity of pneumococcal culture with that of
antigen detection methods
Lupisan S. 2000 [46] To investigate the etiology of serious infections in children aged
< 5 years
admitted to a tertiary care government hospital in Bohol province
Philippine General Hospital;
University of Santo Tomas Hospital;
Philippine Children’s Medical Center.
Survey of bacterial meningitis.
Unpublished hospital data. 2002–
2006
To determine the etiology of bacterial meningitis
Capeding 2007 [49] To describe the pneumococcal serotypes seen among Filipino
children admitted in a tertiary care center in the Philippines due to
infectious diseases
Carlos C. 2007 [50] To determine the antimicrobial resistance patterns of common
pathogens in 2007
Singapore
Low S et al. 2007 [51] To describe the epidemiology of pneumococcal disease based on
hospitalization rates for all age groups for the evaluation of
prevention and control strategies
Chong CY et al. 2008 [52] To assess the adequacy of PCV7 and future expanded vaccine

Objectives
formulations in relation to the predominant IPD serotypes; to
determine the epidemiology of IPD, antibiotic susceptibility patterns
and the morbidity and mortality of children with community-
acquired IPD
Sri Lanka
Lady Ridgeway Hospital. Annual
Health Bulletin. Unpublished internal
hospital data. 2003
To provide hospital statistics on patient admissions
SAPNA. Newsletter. Jan–March 2005
[53]
To provide updates on the SAPNA project
SAPNA. 2007 [19] To report progress of SAPNA project from October 1, 2006 to March
31, 2007
Watanabe H et al. 2007 [54] To determine the status of ARIs caused by S. pneumoniae and H.
influenzae in tsunami evacuation camps in Sri Lanka
Taiwan
Siu LK et al. 2002 [56] To understand the epidemiology of invasive S. pneumoniae in
Taiwan
Department of Health Statistics;
Department of Health, Executive
Yuan, Republic of China. 2006 [55]
To collect essential information on several areas such as population,
economy, education, labor and healthcare among others.
Taiwan Centers for Disease Control
and Prevention (CDC). Unpublished
data. 2007.
To collect information necessary for the notification and control of
disease outbreaks, syndromes and communicable diseases
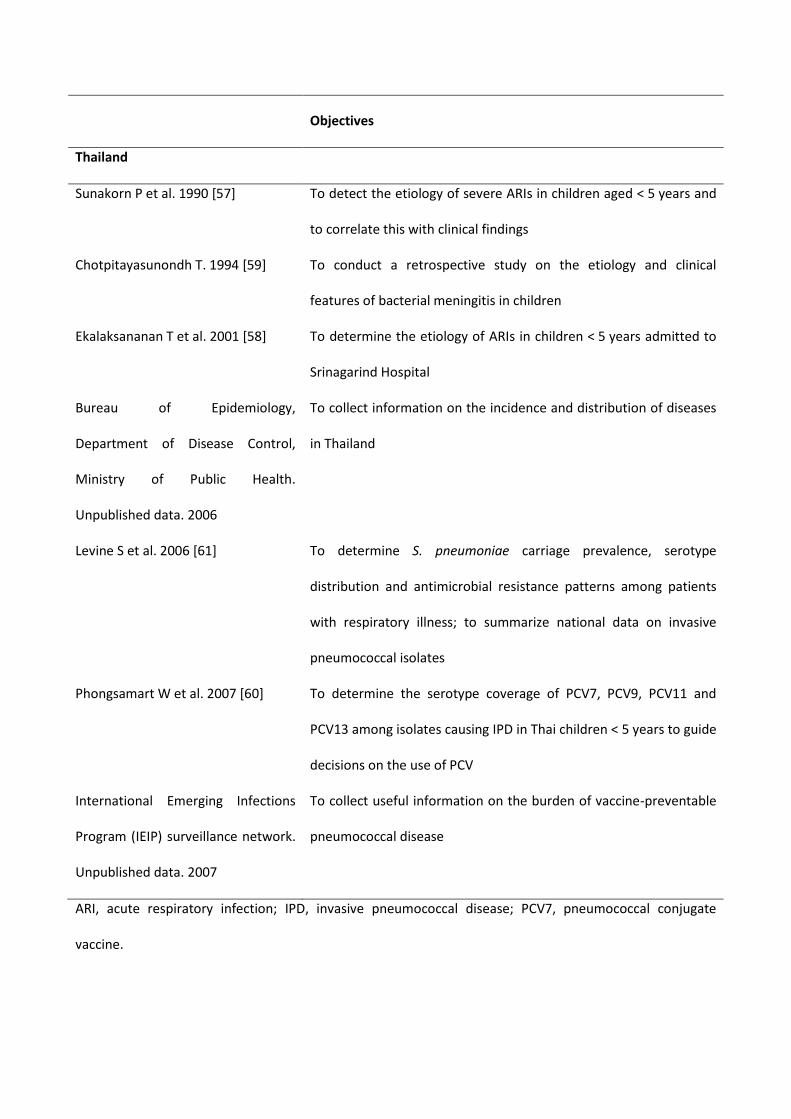
Objectives
Thailand
Sunakorn P et al. 1990 [57] To detect the etiology of severe ARIs in children aged < 5 years and
to correlate this with clinical findings
Chotpitayasunondh T. 1994 [59] To conduct a retrospective study on the etiology and clinical
features of bacterial meningitis in children
Ekalaksananan T et al. 2001 [58] To determine the etiology of ARIs in children < 5 years admitted to
Srinagarind Hospital
Bureau of Epidemiology,
Department of Disease Control,
Ministry of Public Health.
Unpublished data. 2006
To collect information on the incidence and distribution of diseases
in Thailand
Levine S et al. 2006 [61] To determine S. pneumoniae carriage prevalence, serotype
distribution and antimicrobial resistance patterns among patients
with respiratory illness; to summarize national data on invasive
pneumococcal isolates
Phongsamart W et al. 2007 [60] To determine the serotype coverage of PCV7, PCV9, PCV11 and
PCV13 among isolates causing IPD in Thai children < 5 years to guide
decisions on the use of PCV
International Emerging Infections
Program (IEIP) surveillance network.
Unpublished data. 2007
To collect useful information on the burden of vaccine-preventable
pneumococcal disease
ARI, acute respiratory infection; IPD, invasive pneumococcal disease; PCV7, pneumococcal conjugate
vaccine.
0
10
20
30
40
50
60N
o. o
f ep
iso
des
Age
Immunocompetent
Immunocompromised
<2 years 2-5 years >5-16 years
Figure 1. Age distribution of IPD in immunocompetent and immunocompromised children in Korea (Lee HJ,
unpublished data, 2007).
Figure 2. Case fatality rates in two IPD surveillance studies in Taiwan before and after the introduction of
the 7-valent pneumococcal conjugated vaccine (Taiwan CDC 2007), [56].
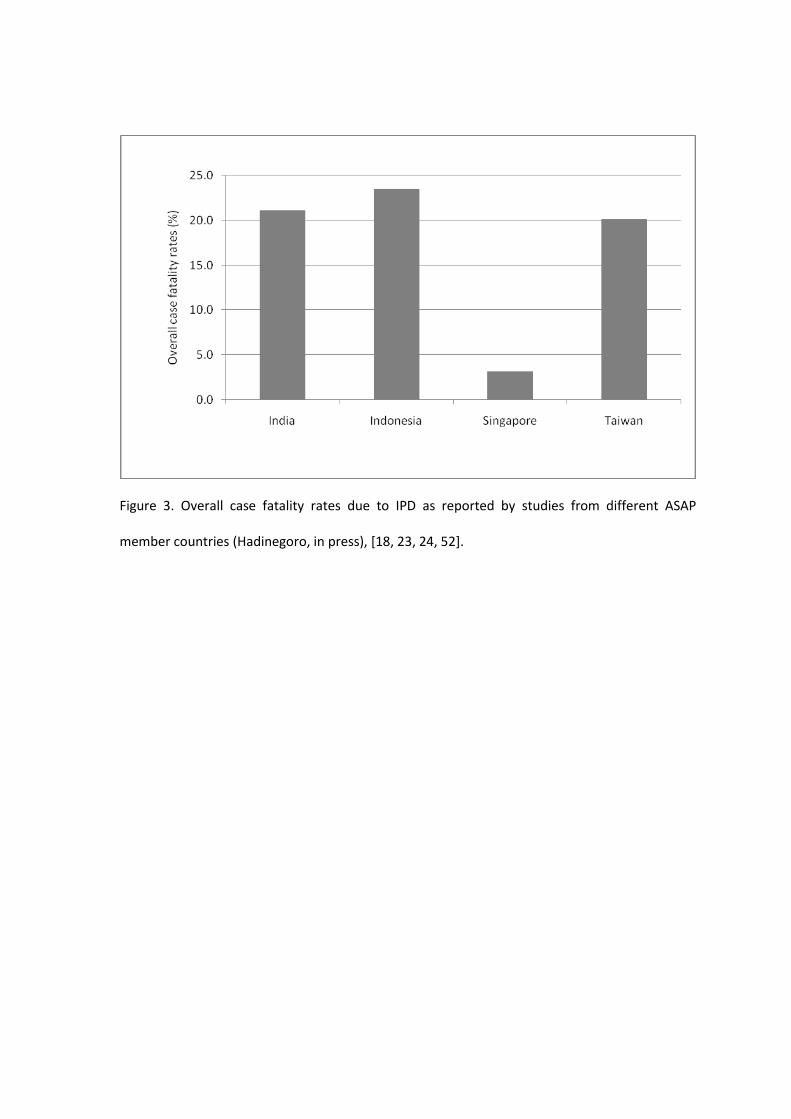
Figure 3. Overall case fatality rates due to IPD as reported by studies from different ASAP
member countries (Hadinegoro, in press), [18, 23, 24, 52].
References
[1] World Health Organization. Pneumococcal conjugate vaccine for childhood
immunization. March 2007 WHO Position Paper. Wkly Epidemiol Record
2007;12:93–104.
[2] Scott JA. The preventable burden of pneumococcal disease in the developing
world. Vaccine 2007;25:2398–405.
[3] Plan Asia. Growing up in Asia: Plan’s strategic framework for fighting child
poverty in Asia 2005–2015. Bangkok: Plan Ltd, 2005. Available at:
http://www.plan-international.org/pdfs/growingupinasia.pdf. Accessed 8 July
2008.
[4] World Health Organization. World health statistics 2008. Geneva: WHO, 2008.
Available at: http://www.who.int/whosis/whostat/EN_WHS08_Full.pdf. Accessed
30 July 2008.
[5] Knoll M. WHO global burden of Hib and pneumococcal disease in children.
Presented at the First Symposium on Pneumococcal Vaccination in the Asia-
Pacific Region, Seoul, Korea, December 13–14, 2007.
[6] O’Brien K. Global pneumococcal disease epidemiology [abstract S01-KS1] 6th
International Symposium on Pneumococci and Pneumococcal Diseases,
Reykjavik, Iceland, June 8–12, 2008. Available at: http://www.congress.is/ISPPD-
6/ISSPD-6-abstracts.pdf. Accessed 19 August 2008.
[7] United Nations Children’s Fund (UNICEF); World Health Organization.
Pneumonia: the forgotten killer of children. Geneva: WHO, 2006. Available at:
http://www.unicef.org/publications/files/Pneumonia_The_Forgotten_Killer_of_Ch
ildren.pdf. Accessed 30 July 2008.
[8] Kyaw MH, Lynfield R, Schaffner W, et al. Effect of introduction of the
pneumococcal conjugate vaccine on drug-resistant Streptococcus pneumoniae. N
Engl J Med 2006;354:1455–63.
[9] Klugman K. Pneumococcal resistance to antibiotics. Clin Microbiol Rev
1990;3:171–96.
[10] World Health Organization. Mortality country fact sheet 2006: Brunei
Darussalam. Available at:
http://www.who.int/whosis/mort/profiles/mort_wpro_brn_bruneidarussalam.pdf.
Accessed 30 July 2008.
[11] Ho PL, Chiu SS, Cheung CH, Lee R, Tsai TF, Lau YL. Invasive pneumococcal
disease burden in Hong Kong children. Pediatr Infect Dis J 2006;25:454–5.
[12] Ho PL, Chiu SS, Chow FKH, Mak GC, Lau YL. Pediatric hospitalization for
pneumococcal diseases preventable by 7-valent pneumococcal conjugate vaccine
in Hong Kong. Vaccine 2007;25:6837–41.
[13] Scientific Committee on Vaccine Preventable Diseases. Recommendations on the
Use of Pneumococcal Vaccines. Centre for Health Protection, Hong Kong.
October 2007.
[14] Ho PL, Lam KF, Chow FK, et al. Serotype distribution and antimicrobial
resistance patterns of nasopharyngeal and invasive Streptococcus pneumoniae
isolates in Hong Kong children. Vaccine 2004;22:3334–9.
[15] Ho PL, Que TL, Chiu SS, et al. Fluoroquinolone and other antimicrobial
resistance in invasive pneumococci, Hong Kong, 1995–2001. Emerg Infect Dis
2004;10:1250–7.
[16] Ip M, Nelson EA, Cheuk ES, et al. Serotype distribution and antimicrobial
susceptibilities of nasopharyngeal isolates of Streptococcus pneumoniae from
children hospitalized for acute respiratory illnesses in Hong Kong. J Clin
Microbiol 2007;45:1969–71.
[17] Invasive Bacterial Infection Surveillance (IBIS) Group; International Clinical
Epidemiology Network (INCLEN). Prospective multicentre hospital surveillance
of Streptococcus pneumoniae disease in India. Lancet 1999;353:1216–21.
[18] The INCLEN Trust. IndiaCLEN Invasive Bacterial Infection Surveillance (IBIS)
Study Group to extend pneumococcal surveillance to South Asia. INCLEN News
2004;25:14 Available at:
http://www.inclentrust.org/pdf/inclennews/July%202004/IBIS.pdf. Accessed 26
September 2008.
[19] South Asian Pneumococcal Alliance. Semi-annual technical report: SAPNA
Project. Available at: http://www.indiaclen.org/sapna/home/Semi-
annualTechnicalReport_May2007.doc. Accessed 26 September 2008.

[20] Jebaraj R, Cherian T, Raghupathy P, et al. Nasopharyngeal colonization of infants
in southern India with Streptococcus pneumoniae. Epidemiol Infect
1999;123:383–8.
[21] Song JH, Jung SI, Ko KS, et al. High prevalence of antimicrobial resistance
among clinical Streptococcus pneumoniae isolates in Asia (an ANSORP study).
Antimicrob Agents Chemother 2004;48:2101–7.
[22] Song JH, Chang HH, Suh JY, et al. Macrolide resistance and genotypic
characterization of Streptococcus pneumoniae in Asian countries: a study of the
Asian Network for Surveillance of Resistant Pathogens (ANSORP). J Antimicrob
Chemother 2004;53:457–63.
[23] Nyambat B, Purniti PS, Kim SW, et al. Invasive pneumococcal diseases-
associated syndromes in Denpasar, Indonesia, 2006 [abstract P1-089]. In: ISPPD-
6: 6th International Symposium on Pneumococci and Pneumococcal Diseases,
June 2008, Reykjavik, Iceland. Available at: http://www.congress.is/ISPPD-
6/ISSPD-6-abstracts.pdf. Accessed 11 September 2008.
[24] Nyambat B, Dijanto I, Atthyah AF, et al. The epidemiology of invasive
pneumococcal disease-associated syndromes among children in Surabaya,
Indonesia [abstract P1-090]. In: ISPPD-6: 6th International Symposium on
Pneumococci and Pneumococcal Diseases, June 2008, Reykjavik, Iceland.
Available at: http://www.congress.is/ISPPD-6/ISSPD-6-abstracts.pdf. Accessed
11 September 2008.
[25] Ruspandji T, Soedarmo SP, Wibisono C, Isnuhandojo B. Acute purulent
meningitis in infants and children. Modern Med of Asia 1981; 17:35–7.
[26] Kartasasmita CB, Duddy HM, Sudigdoadi S, Agustian D, Setiowati I, Ahmad TH,
Panigoro R. Nasopharyngeal bacterial carriage and antimicrobial resistance in
underfive children with community acquired pneumonia. Paediatr Indones
2001;41:292–5.
[27] Kartasasmita CB, Rifada M, Dewi NS, Yusnita S, Krishna E, Permatagalih V,
Murad, Sudigdo-Adi S, Simoes EAF. Pneumococcal nasopharyngeal carriage in
newborns and very young infants in Indonesia and possible source of acquisition.
Paed Respir Rev 2006;7(Suppl):S323–4.
[28] Kari KI, Suwarba IGN, Hartawan INB. Meningitis bacterial profile in Sanglah
hospital in Denpasar, Bali. Presented at Invasive Pneumococcal Disease
symposium. Bali 25 December 2006.
[29] Soewignjo S, Gessner BD, Sutanto A, et al. Streptococcus pneumoniae
nasopharyngeal carriage prevalence, serotype distribution, and resistance patterns
among children on Lombok Island, Indonesia. Clin Infect Dis 2001;32:1039–43.
[30] Choi EH, Kim SH, Eun BW, et al. Streptococcus pneumoniae serotype 19A in
children, South Korea. Emerg Infect Dis 2008;14:275–81.
[31] Jamal F, Pit S, Isahak I, et al. Pneumococcal infection in hospitalized patients: a
four-year study in Malaysia. Southeast Asian J Trop Med Public Health
1987;18:79–84.
[32] Rohani MY, Raudzah A, Ng AJ, et al. Epidemiology of Streptococcus
pneumoniae infection in Malaysia. Epidemiol Infect 1999;122:77–82.
[33] Lim LH, Lee WS, Parasakthi N. Childhood invasive pneumococcal disease: A
hospital-based study from Malaysia. J Paed Child Health 2007;43:366–9.
[34] Choo KE, Ariffin WA, Ahmad T, Lim WL, Gururaj AK. Pyogenic meningitis in
hospitalised children in Kelantan, Malaysia. Ann Trop Paediatr 1990;10:89-98.
[35] Tee AC. Childhood meningitis at University Hospital, Kuala Lumpur, 1980–89.
Dissertation for Master’s Degree in Medicine (Paediatrics), University Malaya,
1993.
[36] Hussain IHM, Sofiah A, Ong LC, et al. Haemophilus influenzae meningitis in
Malaysia. Pediatr Infect Dis J 1998;17(Suppl):S189–90.
[37] Suhaimi M, Asmiati AH, Soo TL. Pneumococcal meningitis in children aged 2–60
months at Queen Elizabeth (QE) Hospital, Sabah, Malaysia: before and after the
introduction of Hemophilus influenza type b vaccination [abstract 0345]. 5th
World Congress of the World Society for Pediatric Infectious Diseases, Bangkok,
Thailand, November 15–17, 2007. Available at:
http://www.kenes.com/wspid2007/program/session1.asp?SessionId=P10&SSessio
nDate=11/19/2007. Accessed 30 July 2008.
[38] Cheong YM, Jegathesan M, Henrichsen J, Wong YH, Ng AJ, Louis A. Antibiotic
susceptibility and serotype distribution of Streptococcus pneumoniae in Malaysian
children. J Trop Pediatr 1988;34:182–5.
[39] Bhutta ZA. Burden of H. influenzae and S. pneumoniae infections in Pakistan.
Journal of College of Physicians and Surgeons of Pakistan 2001; 10:346–54.
[40] Bhutta ZA, Cross A, Raza F, Zaheer Z. Infant and child mortality. In: National
Institute of Population Studies and Macro International. Pakistan Demographic
and Health Survey 2007.
[41] Nizami SQ, Bhutta ZA, Hasan R. Incidence of acute respiratory infections in
children 2 months to 5 years of age in periurban communities in Karachi,
Pakistan. J Pak Med Assoc 2006;56:163–7.
[42] Rehman A, Mazhar AU, Sarwar MSA, Ullah HH. Acute respiratory infections
bacteriology and antimicrobial sensitivity. Pakistan Pediatrics Journal
1996;20:71–6.
[43] Ghafoor A, Nomani NK, Ishaq Z, et al. Diagnoses of acute lower respiratory tract
infections in children in Rawalpindi and Islamabad, Pakistan. Rev Infect Dis
1990;12(Suppl 8):S907–14.
[44] Mastro TD, Ghafoor A, Nomani NK, et al. Antimicrobial resistance of
pneumococci in children with acute lower respiratory tract infection in Pakistan.
Lancet 1991;337:156–9.
[45] Department of Health Republic of the Philippines. Health indicators: ten leading
causes of child mortality. Available at:
http://www.doh.gov.ph/kp/statistics/child_mortality. Accessed 12 August 2008
[46] Lupisan S, Herva E, Sombrero L, et al. Invasive bacterial infections of children in
a rural province in the central Philippines. Am J Trop Med Hyg 2000;62:341–6.
[47] Capeding MRZ, Sombrero LT, Paladin FJ, Suzuki H, Numazaki Y, Saniel MC.
Etiology of acute lower respiratory infection in children under 5 years. Southeast
Asian J Trop Med Public Health 1994;25:684–7.
[48] Lankinen KS, Leinonen M, Tupasi TE, Haikala R, Ruutu P. Pneumococci in
nasopharyngeal samples from Filipino children with acute respiratory infections. J
Clin Microbiol 1994;32:2948–52.
[49] Capeding MRZ, Sombrero LT, Esparar GA, Mondoy MU, Taclibon AG.
Pneumococcal serotypes among Filipino children admitted to a tertiary care center
for infectious diseases in 2000–2005. Pediatric Infectious Disease Society of the
Philippines (PIDSP) Journal 2007;11:1–3.
[50] Carlos C. Antimicrobial Resistance Surveillance Program Progress Report,
January–December 2007. Research Institute for Tropical Medicine, Department of
Health. 2007.
[51] Low S, Chan FL, Cutter J, Ma S, Goh KT, Chew SK. A national study of the
epidemiology of pneumococcal disease among hospitalised patients in Singapore:
1995 to 2004. Singapore Med J 2007;48:824–9.
[52] Chong CY, Thoon KC, Mok YH, Tee WSN. Invasive pneumococcal disease in
Singapore children. Vaccine 2008;26:3427–31.
[53] South Asian Pneumococcal Alliance. SAPNA Newsletter. January–March 2005.
Available at: http://www.indiaclen.org/sapna/home/NewsLetterSAPNArev2.pdf.
Accessed 25 September 2008.
[54] Watanabe H, Batuwanthudawe R, Thevanesam V, et al. Possible prevalence and
transmission of acute respiratory tract infections caused by Streptococcus
pneumoniae and Haemophilus influenza among the internally displaced persons in
tsunami disaster evacuation camps of Sri Lanka. Intern Med 2007;46:1395–402.
[55] Department of Health, Executive Yuan, Republic of China. Health Statistics in
Taiwan, 2006. Taipei: ROC Department of Health, 2006.
[56] Siu LK, Chu ML, Ho M, Lee YS, Wang CC. Epidemiology of invasive
pneumococcal infection in Taiwan: antibiotic resistance, serogroup distribution
and ribotypes analyses. Microbial Drug Resist 2002;8:201–8.
[57] Sunakorn P, Chunchit L, Niltawat S, Wangweerawong M, Jacobs RF.
Epidemiology of acute respiratory infections in young children from Thailand.
Pediatr Infect Dis J 1990;9:873–7.
[58] Ekalaksananan T, Pientong C, Kongyingyoes B, Pairojkul S, Teeratakulpisarn J,
Heng S. Etiology of ALRTI in children at Srinagarind Hospital, Khon Kaen,
Thailand. Southeast Asian J Trop Med Public Health 2001;32:513–9.

[59] Chotpitayasunondh T. Bacterial meningitis in children: etiology and clinical
features, an 11-year review of 618 cases. Southeast Asian J Trop Med Public
Health 1994;25:107–15.
[60] Phongsamart W, Srifeungfung S, Dejsirilert S, et al. Serotype distribution and
antimicrobial susceptibility of S. pneumoniae causing invasive disease in Thai
children younger than 5 years old, 2000–2005.Vaccine 2007;25:1275–80.
[61] Levine S, Dejsirilert S, Sangsuk L, et al. Serotypes and antimicrobial resistance of
Streptococcus pneumoniae in Thailand 2002–2004. Pediatr Infect Dis J
2006;25:176–8.
[62] Rudan I, Boschi-Pinto C, Biloglav Z, Mulholland K, Campbell H. Epidemiology
and etiology of childhood pneumonia. Bulletin of the World Health Organization
2008;86:408–16.
[63] Bhutta ZA. Drug resistant infections in poor countries. A major burden on
children. BMJ 2008;336:948–9.
[64] Sinha A, Levine O, Knoll MD, Muhib F, Lieu TA. Cost-effectiveness of
pneumococcal conjugate vaccination in the prevention of child mortality: an
international economic analysis. Lancet 2007;369:389–96.
[65] Rinaldi F, Chong C. Predicted impact of a universal infant 7vPCV vaccination
program in Singapore [abstract P4-021]. In: ISPPD-6: 6th International
Symposium on Pneumococci and Pneumococcal Diseases, 12 June 2008,
Reykjavik, Iceland. Abstracts. Reykjavik: ISPPD, 2008:392. Available at:
http://www.congress.is/ISPPD-6/ISSPD-6-abstracts.pdf. Accessed 31 July 2008.
[66] Lee KC, Rinaldi F, Lee VWY, Hon EKL, So TMK Economic evaluation of
universal infant vaccination with 7vPCV in Hong Kong [abstract P4-022]. In:
ISPPD-6: 6th International Symposium on Pneumococci and Pneumococcal
Diseases, 12 June 2008, Reykjavik, Iceland. Abstracts. Reykjavik: ISPPD,
2008:393. Available at: http://www.congress.is/ISPPD-6/ISSPD-6-abstracts.pdf.
Accessed 31 July 2008.
[67] GAVI’s PneumoADIP comprehensive report with data. February 2007. Available
at:
http://www.preventpneumo.org/activities/surveillance_and_research/upload/RS-
Report-Final1207.pdf. Accessed 19 August 2008.
[68] Deloria-Knoll M, Wonodi CB, Moïsi JC, Grant L, Gilani Z, Levine O,
PneumoADIP-sponsored Surveillance Investigators. Surveillance for
pneumococcus: the PneumoADIP experience [abstract P1-047]. In: ISPPD-6: 6th
International Symposium on Pneumococci and Pneumococcal Diseases, 12 June
2008, Reykjavik, Iceland. Abstracts. Reykjavik: ISPPD, 2008:392. Available at:
http://www.congress.is/ISPPD-6/ISSPD-6-abstracts.pdf. Accessed 19 August
2008.





























