Embed Size (px)
Citation preview

Overview of Idiopathic Pulmonary Fibrosis:
Diagnosis and Therapy
Jeff Swigris, DO, MSDirector, ILD ProgramNational Jewish Health
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Disclosures
Speaker - Boehringer Ingelheim and Genentech
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Objectives
Describe how to diagnose IPF
Develop strategy to distinguish IPF from other ILDs
Comprehensive therapeutic approach to IPF
Patient education and taking aim at improving QOL
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

ILD
Inflammation and/or scar
In the INTERSTITIUM
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

To an ILD doc, the interstitium is located…
Along BV bundles
In interlobular septae
In the subpleural region
Within alveolar walls (largest area)Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Secondary Pulmonary Lobule
~1.5cmPropert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Etiology-based classification scheme
ILD
Exposure-relatedmold, bacteria, birds
medications XRT dusts
cigarette smoke
IdiopathicSarcoidosis
LAM IIP
GeneticFPF
Autoimmune-relatedRA
Systemic sclerosis PM/DM
Sjögren’s syndrome MCTD SLE IBD
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Idiopathic interstitial pneumonias (IIP)
Major IIP Major IIP Idiopathic pulmonary fibrosis (IPF) Idiopathic pulmonary fibrosis (IPF) Idiopathic nonspecific interstitial pneumonia (NSIP)Idiopathic nonspecific interstitial pneumonia (NSIP) Respiratory Respiratory bronchiolitisbronchiolitis--ILD (RBILD (RB--ILD)ILD) DesquamativeDesquamative interstitial pneumonia (DIP)interstitial pneumonia (DIP) Cryptogenic organizing pneumonia (COP)Cryptogenic organizing pneumonia (COP) Acute interstitial pneumonia (AIP)Acute interstitial pneumonia (AIP)
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

ILD ➙ IIP ➙ IPF
IPF: specific type of ILD within the IIP
IPF: specific type of pulmonary fibrosis UIP-pattern
IPF: Diagnosis of exclusion Rule out…
Exposure (environment, Rx, occupational) Connective tissue disease
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Histology-based classification scheme
S C ARFLAMMAT I ON
UIP‐pattern lives here
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Etiology-based classification scheme
ILD
Exposure-relatedmold, bacteria, birds
medications XRT dusts
cigarette smoke
IdiopathicSarcoidosis
LAM IIP
GeneticFPF
Autoimmune-relatedRA
Systemic sclerosis PM/DM
Sjögren’s syndrome MCTD
S C ARNFLAMMAT NI OI
S C ARNFLAMMAT NI OI
S C ARNFLAMMAT NI OI
S C ARNFLAMMAT NI OI
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Idiopathic disease + UIP-pattern
IPF
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What to do when you have a patient in front of you and you
are considering the possibility of IPF as the
clinical summary diagnosis
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Making the diagnosis of IPF You have to be a detective
History
Exam
Pulmonary physiology
Radiography
+/- surgical lung biopsy
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

History
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

History Typically…IPF presents with:
Dyspnea—subacute, insidious onset
“I thought it was just that I was a year older, 5# heavier, and out of shape”
+/- dry cough Fatigue/low stamina Not pain, swollen joints, rash
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Identify symptoms of rheumatologic illness Eyes/skin/joints/muscles
Family history Pulmonary fibrosis Rheumatologic illness
Exposures Smoking, dusts, M/M/B/B
History
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Physical Exam
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Physical examination
Hands Chest
Crackles ANY VELCRO CRACKLE IS ABNORMAL MAKE SURE YOU LISTEN AT THE BASES
Joints Skin Prop
erty o
f Pres
enter
Not for
Rep
roduc
tion

Laboratory
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Laboratory assessment
Serologies ANA RF/anti-CCP Scl-70 SSA/SSB Myositis panel
What to do with positive????Prop
erty o
f Pres
enter
Not for
Rep
roduc
tion

Pulmonary Physiology and Gas Exchange
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Pulmonary physiology
Pulmonary function testing
Measures of resting and exercise-related gas exchange
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Radiology
“ILD protocol” HRCT No IV contrast Supine and prone Inspiratory and expiratory images High-resolution reconstruction algorithm 1-1.5mm thick slicesProp
erty o
f Pres
enter
Not for
Rep
roduc
tion

Lung Biopsy
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Lung biopsy
Transbronchial biopsy Sarcoidosis Lymphangitic carcinomatosis Subacute HP
Surgical Thorascopic, multiple lobes When “classic” HRCT pattern absent
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Putting it all Together History
Exam
Labs ANA, RF, anti-CCP
Physiology Full PFTs
Gas exchange 6MWT
Radiology HRCT
Pathology
Integrate to get “summary diagnosis”
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Making the diagnosis of IPF
Suspected IPF
Identifiable causes for ILD?
HRCT
Consider VATSx Lung Biopsy
IPF or not IPFIPF Not IPF
Possible UIPIndeterminate UIP
Clin/Rad/Path
UIPProbable/Possible UIPNon-classifiable fibrosis
Yes
Not UIP
No
UIP-pattern
Other Dx
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Park et al. AJRCCM 2007
IPF
CTD
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Ann Intern Med. 2012;156(10):684-691
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

IPF: Cause of Death
Olson et al. Am J Respir Crit Care Med 2007
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What’s not IPF?
48 yo F with achey joints, cracked hands, Raynauds
and anti-PL-7 antibodiesProp
erty o
f Pres
enter
Not for
Rep
roduc
tion

What’s the Diagnosis?
69 yo M with anti-CCP positive RA, now with cough and exertional dyspnea
Propert
y of P
resen
ter
Not for
Rep
roduc
tion
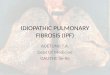
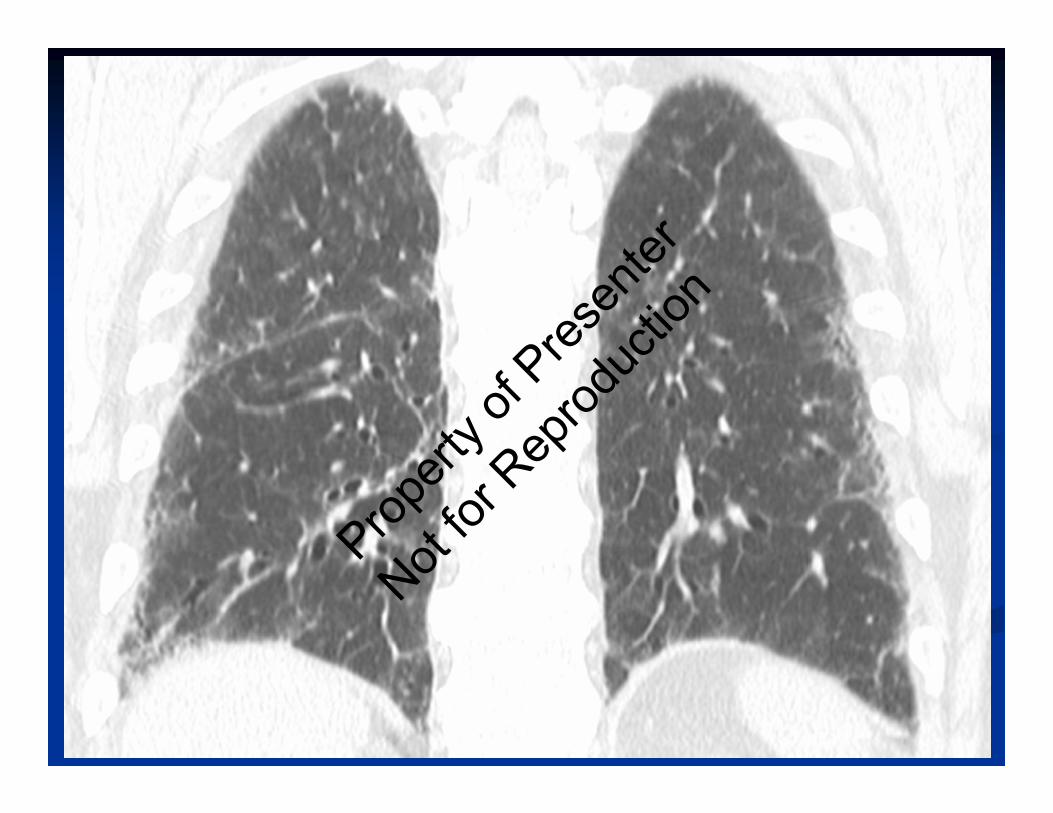
What’s not IPF?
69 yo M with parrot, exertional dyspnea and cough, VATSx bx = UIP-pattern with poorly-formed granulomas
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What’s not IPF?
73 yo F never-smoker, retired teacher, with chronic UTI on nitrofurantoin for > 4 years
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What’s not IPF?
53 yo F, executive secretary, uses her indoor hot tub daily, now with 4 months increasing dyspnea
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What’s the Diagnosis?
62 yo M former smoker, retired Air Force fighter pilot, no CTD symptoms, no exposures, VATSx bx with
UIP-pattern histologyProp
erty o
f Pres
enter
Not for
Rep
roduc
tion

Therapeutic Maneuvers
O2 – keep SpO2 > 89% regardless of activity level Improves fatigue, functioning, dyspnea
Pulmonary rehabilitation Improves fatigue, functioning, QOL
VaccinationsProp
erty o
f Pres
enter
Not for
Rep
roduc
tion

Therapeutic Maneuvers
Probably look for and treat GERD, OSA, PH
Education – knowledge is power
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Therapeutic Maneuvers
Anti-fibrotics
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Pathogenesis of IPF
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Anti-fibrotics work here
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Nintedanib or Pirfenidone
PlaceboPlacebo
0
‐100
‐200Placebo
Po
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

King TE, et al. N Engl J Med. 2014
Pirfenidone: adverse events
Adverse Event Pirfenidone (%) (N = 278)
Placebo (%) (N = 277)
∆ (%)
Nausea 36 13.4 22.6Rash 28.1 8.7 19.4Dyspepsia 17.6 6.1 11.5Anorexia 15.8 6.5 9.3GERD 11.9 6.5 5.4Weight Loss 12.6 7.9 4.7Insomnia 11.2 6.5 4.7Dizziness 17.6 13 4.6Vomiting 12.9 8.7 4.2
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Richeldi L, et al. N Engl J Med. 2014;370(22):2071‐2082.
Nintedanib: Adverse Events
Event
INPULSIS-1 INPULSIS-2
Nintedanib (n = 309)
Placebo (n = 204)
Nintedanib (n = 329)
Placebo (n = 219)
Any (%) 96 89 94 90
Diarrhea (%) 62 19 63 18
Nausea (%) 23 6 26 7
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Summary – Main Points
IPF = idiopathic + UIP
Thorough history, exam and HRCT
Therapeutic approach: anti-fibrotics
Simple things most important: Disease education O2 Pulmonary rehab
Propert
y of P
resen
ter
Not for
Rep
roduc
tion