Embed Size (px)
Citation preview

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 1
SUCCESS THROUGH TEAMWORK
OVERCOMING BARRIERS TO SPEAKING VALVE USE Disclosure Statement
• Passy-Muir, Inc. has developed and patented
a licensed technology trademarked as the
Passy-Muir® Tracheostomy and Ventilator
Swallowing and Speaking Valve. This
presentation will focus primarily on the biased-
closed position Passy-Muir Valve and will
include little to no information on other
speaking valves.
Presenter
Nicole Riley, MS CCC-SLP Director of Clinical Education
Passy-Muir Inc.
(949) 783-3755
Disclosure: Financial — Employee of Passy-Muir Inc.
Nonfinancial — No relevant nonfinancial relationship exists.
Course Outline
1. Evidence for Passy-Muir Protocols
2. Common barriers and practical strategies to overcome barriers to
Passy-Muir® Valve Use
3. How to implement a Passy-Muir protocol
4. Forming a tracheostomy team
5. Outcomes and Case Studies
My Story at Barlow
Why make the Passy-Muir® Valve a standard of care?
Benefits of the valve:
• Voice/Speech Production
• Improved swallowing
• Secretion management
• Restores positive airway pressure
• Restores PEEP
• Weaning
• Decannulation
• Quality of Life

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 2
Goal Common Barriers to this Goal
• Myths, misconceptions and ex cuses
• Sociological Issues
Barrier 1: “We can’t deflate the cuff because
the patient will aspirate”
VENTILATOR APPLICATION OF THE PASSY-MUIR® VALVE
Cuff Deflation Benefits
• Reduced aspiration1, 2 • Improved laryngeal
elevation 2, 3 • Weaning time was shorter-
average of 3 days vs 8 days3
• Fewer respiratory infections including ventilator associated pneumonia (20% vs. 36%) 4
• Swallowing better in cuff deflated group and improve more from baseline4
1. Davis, et al. (2002). Journal of Intensive Care Medicine. 17(3): 132-135. 2. Ding, R. & Logeman, J. (2005). Head & Neck. 27(9):809 -13 3. Amathieu, R., et al. British journal of anaesthesia109.4 (2012): 578-583. 4. Hernendez, et al. (2013). Intensive Care Medicine. 39(6):1063-70
One Way Valve Reduces Aspiration Further
• Improved scores on
penetration-aspiration scale1
• Restores expiratory airflow2
• Improves laryngeal
clearance2
• Improved secretion rating
scale3
• Maintains lung volumes4
• Restores subglottic air
pressure5
1. Suiter, D. Head and Neck. 2005. Sep;27(9):809-13
2. Pr igent, Helene. Intensive Care Med. 2012 June38(1):85-90.
3. Blumenfeld, L. Oral Abstract Presented at Dysphagia Research Society Annual Meeting 2012 4. Gross, R., et al. (2006). The Laryngoscope, 116:753-761
5. Eibling, D., & Gross, R. (1996). Annals of Otology, Rhinology, & Laryngology, 105(4):253-8.
Barrier 2: “The patient has too
many secretions”

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 3
Before Passy-Muir Valve
After Passy-Muir Valve
Barrier 3: “We need to wait until the
patient is on a trach collar” Disuse Atrophy
• Mechanical ventilation
can cause atrophy, and
injury of diaphragmatic
muscle fibers
• “Patients in intensive
care lose about 2% of
muscle mass a day
during their illness.”1
• Muscle weakness
predicts pharyngeal
dysfunction2
1. Jaber, S.et al, 2011; Griff iths, BMJ, 1999
2. Mirzakhani, H. et al Anesthesiology . 2013
Passy-Muir Valve facilitates weaning
• Greater tolerance of weaning attempts leading to
independent breathing
• Patients have reported that breathing is easier and
have been able to tolerate trials of CPAP longer
• Multidisciplinary teams incorporating the valve
have had improved outcomes
1 . Fre y, J. & Wo o d , S. We an in g fro m M e ch an ical Ve n ti latio n Au gme n te d b y th e P assy-M u ir Sp e akin g Valve (1 9 9 1 ). Ab stract at th e In te rn atio n al C o n fe re n ce o f
Ame rican Lu n g Asso ciatio n an d Ame rican Th o racic So cie ty
2 . B lack, C . e t al . (2 0 1 2 ). A M u ltid iscip l in ary te am ap p ro ach to we an in g fro m p ro lo n ge d me ch an ical ve n ti latio n . B ri ti sh Jo u rn al o f Ho sp ital M e d icin e . Au g;,
7 3 (8 ): 4 6 2 -4 6 6 .
3 . Ati to -Narh , E. e t al (2 0 0 8 ). Slo w ve n ti lato r we an in g afte r ce rvical sp in al co rd in ju ry. B ri ti sh Jo u rn al o f In te n sive C are . 9 5 -1 0 2 .
4 . K o b ak, J. & De an , L. (2 0 1 1 ). Use o f th e P assy-M u ir Valve fo r we an in g in lo n g te rm acu te care h o sp ital . R e sp irato ry Th e rap y. 6 (4 ):4 4 , 5 7
5 . Win d h o rst, C ., e t al (2 0 0 9 ). P atie n ts re q u irin g trach e o sto my an d me ch an ical ve n ti latio n : a mo d e l fo r in te rd iscip l in ary d e cisi o n makin g. Th e ASHA Le ad e r, 1 4
(1 ), 1 0 -1 3 .
6 . Gu rn ari , D. & M artin , C . (Octo b e r, 2 0 1 1 ). Early co l lab o ratio n o f re sp irato ry an d re h ab i l i tatio n d e p artme n t imp ro ve s ve n ti lato r we an i n g rate s. P o ste r
p re se n te d at th e C o n fe re n ce o f th e Natio n al Asso ciatio n o f Lo n g Te rm Ho sp itals, Ne w Orle an s, LA.

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 4
Use of the Passy-Muir can facilitate weaning
Barrier 4: “The patients are too sick”
Patients should be medically stable
Barrier 5: “The Ventilator will
continuously alarm”
0 cm H20
PEEP
.30 FiO2
PIP 10cm H2O
VT
500cc
0cc
500cc
Set your pressure alarms appropriately Barrier 6: “Tracheostomy tube is too large”

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 5
Downsizing the Tracheostomy
• Improves expiratory
pressures1
• Improves speaking valve and capping recommendations,
comfort and tolerance1
• Associated with earlier oral intake and reduced length of stay2
• Improves weaning for spontaneous breathing trials3
1. Johnson , JD et al. (2009). The Clinical Respiratory Journal 2009; 3: 8–14.
2. Fisher, D. et al. (2013). Respiratory Care. 2013 Feb;58(2):257-63. 3. H ernandez , G . et al. (2013). Intens ive Care Medicine. Jun;39(6):1063-70
Not all Trach Sizes are Equal!
Size 6.0 Tracheostomy
ID OD L
Portex 6.0 8.3 55.0
Bivona 6.0 8.8 70.0
Shiley 6.4 10.8 74.0
SCT 6.0 8.3 67.0
Other Recommendations to Increase Airflow
• Cuffless
• Fenestrated
• Consider ENT consult
Barrier 7: “Absence of a Team”
Tracheostomy Teams
• Affordable Care Act
• Joint Commission
Tracheostomy Teams
• Increased speaking valve use
• Improved decannulation time
• Reduce Length of Stay (LOS)
• Reduced costs
Speed, Lauren, and Kather ine E. Harding. Journal of Cr itical Care (2012).

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 6
Tracheostomy Team
Role of Speech-Language Pathologist
• Help assess airway
patency
• Assess swallow ability and diet recommendations
• Assess vocal ability
– Speech/swallow exercises
• Monitor tolerance
• Recommend wear time
• Educate caregivers
Role of Respiratory Therapist
• Help assess airway
patency
• Adjust and monitor
ventilator
• Technical
troubleshooting
• Monitoring of pt status
• Cough/breathing
techniques
Barrier 8: Lack of Knowledge/Inconsistency
Educate
• Be a leader
• Physician support is KEY!
• Pulmonologists, RTs, SLPs,
nursing
• U se Passy-Muir
webinars/inservices
Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 7
Performance Improvement
• Protocol to assess all tracheostomy patients for Passy-Muir Valve within 72
hours of admission
• Criteria:
– Tolerate cuff deflation
– Patent upper airway
– 48-72 hrs post trach
– Medically stable
• FiO2<60%
• PEEP<10
• PIP<40
Competency
Name Watched vent application webinar
Verbalized understanding of protocol
Performs procedure for placing Passy-Muir
Valve
John Doe ❑ ❑ ❑
Matt Smith ❑ ❑ ❑
Jane Jones ❑ ❑ ❑
Henry Cooper ❑ ❑ ❑
Andrea Thompson ❑ ❑ ❑
Margaret Miller ❑ ❑ ❑
Dave Parker ❑ ❑ ❑
Track your compliance
• SLP completes Passy-Muir Valve evaluation form
within 72 hours of admission OR states reason
patient was not a candidate.
• 98% compliance for PMV assessment at Barlow
Barrier 9: No Protocol
VENTILATOR APPLICATION OF THE PASSY-MUIR® VALVE
Multi-disciplinary Tracheostomy Weaning Protocols
• Increase amount of
patients decannulated
• Reduce time to
decannulation
• Assign clear
responsibilities
• “The tracheostomy tube
decannulation process is
well suited for therapist-
implemented
protocols.”
Christopher, KL. (2005). Respiratory Care, Vol 50
http://passymuir.com/policiesandprocedures
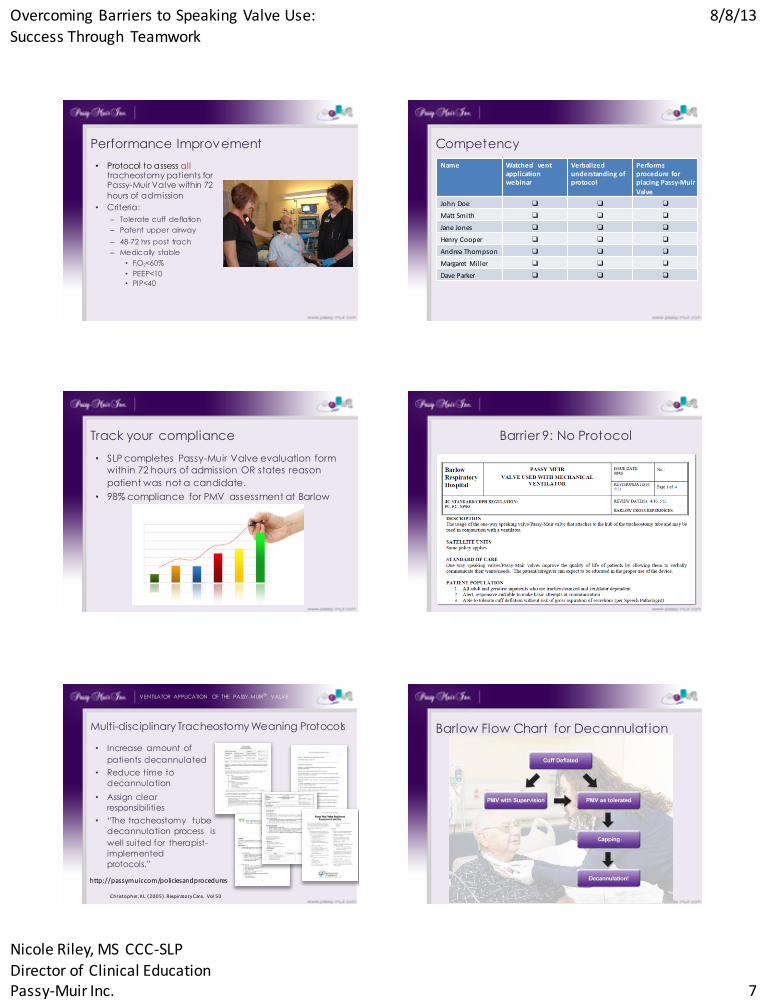
Barlow Flow Chart for Decannulation

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 8
Cuff Deflation as Tolerated
• Stop Criteria:
– Respiratory rate greater than 35
– Heart rate changes by
20 bpm
– SpO2 less than 90%
– FiO2 greater than 60%
– Pt complains of
difficulty breathing 6/10
Stop criteria present:
YES: Re-inflate cuff and
reassess patient before
progressing
NO: Advance to One-Way
Valve
Speaking Valve as Tolerated
Stop Criteria:
• Respiratory rate over 35
• Heart rate changes by
20 bpm
• SpO2 less than 90%
• FiO2 greater than 60%
• Pt complains of difficulty
breathing 6/10
Stop criteria present:
• YES: Remove valve and
consult physician for
possible downsizing
• NO: Advance to One
Way Valve as Tolerated
Capping as Tolerated
Stop Criteria:
• Respiratory rate greater
than 35
• Heart rate changes by
20 bpm
• SpO2 less than 90%
• FiO2 greater than 60%
• Pt complains of difficulty
Breathing 6/10
Stop criteria present:
• YES: Reassess patient to
determine barriers.
Patient may need
additional trach tube
downsizing.
• NO: Consider
recommendation for
decannulation from
physician after 24-48hrs
Decannulation!
• Requires an order
Candidates for Decannulation
• Have the indications for trach resolved or
improved?
• Weaned from mechanical ventilation, effective
coughing, no significant upper airway lesion1
• Absence of distress, stable arterial blood gases,
hemodynamic stability, absent fever1
• A peak cough flow of 160 liters/minute2
• Survey: patient’s level of consciousness, cough
effectiveness, secretions, ox ygenation3
1. Christopher, K.(2005). Respiratory Therapy. 50(4):538 –54. 2. Bach & Saporito, (1996). Chest. 110(6): 1566 -71. Stelfox, H. et al (2009). Respiratory Care. 54(12): 1658 -68.
Success!
• Earlier decannulation times
• Reduced restraint use as patients were less anx ious
• Individual success stories

Overcoming Barriers to Speaking Valve Use: Success Through Teamwork
8/8/13
Nicole Riley, MS CCC-SLP Director of Clinical Education Passy-Muir Inc. 9
Summary
Be a leader
Provide research to support your information
Educate the clinicians and MDs
-U se Passy-Muir webinars
-Consider live webinars or inservices
Implement a protocol
Competencies
Build your team!
Q and A
Presenter
Nicole Riley, MS CCC-SLP Director of Clinical Education
Passy-Muir Inc.
(949) 783-3755
Disclosure: Financial — Employee of Passy-Muir Inc.
Nonfinancial — No relevant nonfinancial relationship exists.