Embed Size (px)
Citation preview

Outcomes Using Doxorubicin-Based Chemotherapy with orwithout Radiotherapy for Early-Stage Peripheral T-cell
Lymphomas
HOON K. LEEa, RICHARD B. WILDERa,*, DAN JONESb, CHUL S. HAa, BARBARA PROc, MARIA A. RODRIGUEZc, JORGEE. ROMAGUERAc, FERNANDO CABANILLASc, JOSE RODRIGUEZd and JAMES D. COXa
aDepartment of Radiation Oncology, Box 97, M.D. Anderson Cancer Center, 1515 Holcombe Blvd., University of Texas, Houston, TX 77030-4009 USA;bDepartment of Hematopathology, M.D. Anderson Cancer Center, University of Texas, Houston, TX USA; cDepartment of Lymphoma, M.D. Anderson
Cancer Center, University of Texas, Houston, TX USA; dHospital Universitario Son Dureta, Palma De Mallorca, Spain
(In final form 20 February 2002)
There is little information in the literature on outcomes using doxorubicin-based chemotherapy with orwithout radiotherapy for early-stage peripheral T-cell lymphomas. The purpose of this study was toanalyze The University of Texas M.D. Anderson Cancer Center results in such patients. From 1985 to1998, 39 patients with Stage I or II World Health Organization classification anaplastic large celllymphoma (ALCL; n ¼ 20), peripheral T-cell lymphoma, unspecified (PTCLu; n ¼ 11), or nasal-typeNK/T-cell lymphoma (NKTCL; n ¼ 8) were treated using doxorubicin-based chemotherapy (median, 6cycles) with ðn ¼ 24Þ or without ðn ¼ 15Þ radiotherapy (median dose, 40 Gy). Median age was 41years. Median follow-up of surviving patients was 85 months. Even though patients who presented withbulky disease or who achieved less than a complete response to chemotherapy were the ones typicallytreated with combined modality therapy rather than chemotherapy alone, there was no significantdifference in local control (5-year rates: 60 vs. 70%, p ¼ 0:49), progression-free survival (5-year rates:65 vs. 60%, p ¼ 0:62), or overall survival (5-year rates: 74 vs. 67%, p ¼ 0:47) between the groupstreated with combined modality therapy and chemotherapy alone. Fifteen (38%) patients relapsed.Twelve relapses were limited to the initial site of disease; two involved the initial site and new sites, andone involved only new sites. Based on the significant risk of relapse at the initial site of disease,different approaches, including chemotherapy with concomitant radiotherapy to doses $45 Gy, warrantinvestigation.
Keywords: T-cell lymphoma; Chemotherapy; Radiotherapy; Prognosis
INTRODUCTION
Most [1–5] but not all [6–8] groups have observed that
T-cell lymphomas have a worse prognosis than B-cell
lymphomas. Anaplastic large cell lymphoma (ALCL),
peripheral T-cell lymphoma, unspecified (PTCLu), and
nasal-type NK/T-cell lymphoma (NKTCL) are some of
the most common subtypes of mature peripheral
T-cell neoplasms [9]. In general, PTCLu and NKTCL
have a worse prognosis than ALCL [5,10]. Other
subtypes of mature peripheral T-cell neoplasms occur
rarely [11].
The diagnoses of ALCL, PTCLu, and NKTCL have
been made with increasing frequency based on improved
diagnostic methods [12]. No consensus has been reached
regarding optimal treatment. For example, the role of
involved-field radiotherapy remains unclear in patients
with early-stage disease. Considering that ALCL, PTCLu,
and NKTCL constitute only 12% of aggressive lympho-
mas [11], one cannot use Southwest Oncology Group
study 8736 [13], Eastern Cooperative Oncology Group
study E1484 [14], or Groupe d’Etude des Lymphomes de
l’Adulte study LHN93-1 [15] to determine the role of
radiotherapy in such patients. Since it is unlikely that a
prospective, randomized trial will be conducted specifi-
cally in patients with early-stage peripheral T-cell
lymphomas, we performed a retrospective analysis of
our results.
ISSN 1042-8194 print/ISSN 1029-2403 online q 2002 Taylor & Francis Ltd
DOI: 10.1080/1042819021000006277
*Corresponding author. Tel.: þ1-713-792-3400. Fax: þ1-713-745-6994. E-mail: [email protected]
Leukemia and Lymphoma, 2002 Vol. 43 (9), pp. 1769–1775
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.

MATERIALS AND METHODS
Prognostic Systems
The M.D. Anderson tumor score (MDATS) [16] and the
international prognostic index (IPI) [17] are presented in
Table I. MDATS differs from IPI in that bulky disease [18]
and serum beta-2 microglobulin [19,20] are taken into
consideration. Stage-adjusted scores were calculated in this
study since none of the patients had Stage III–IV disease.
The median stage-adjusted MDATS was 1 (range, 0–4) and
the median stage-adjusted IPI was also 1 (range, 0–2) for
the 39 Stage I–II peripheral T-cell lymphoma patients.
Patient Characteristics
Thirty-nine patients with Ann Arbor Stage I or II [21]
PTCLu ðn ¼ 11Þ; NKTCL ðn ¼ 8Þ; or ALCL (n ¼ 20 : 15
systemic and five primary cutaneous) were treated at The
University of Texas M.D. Anderson Cancer Center from
1985 to 1998. Because of their rarity, we did not include
other subtypes of peripheral T-cell lymphomas. Twenty-
two patients had Stage I disease, and 17 patients had Stage
II disease. Median age was 41 years. Table II lists patient
characteristics in terms of the treatment delivered, which
is described below.
Pathologic Evaluation
All cases were reviewed by pathologists at M.D.
Anderson. Hematoxylin and eosin staining was performed
in all cases. Immunophenotyping was done by cryostat or
paraffin-section immunohistochemistry or by a flow
cytometric panel of B- and T-cell markers. Cases were
diagnosed according to the World Health Organization
(WHO) classification [9] based on morphological features
and immunoreactivity for at least one NK- or T-cell
lineage-associated marker. Lymphoblastic tumors were
excluded. All cases diagnosed as ALCL demonstrated
positivity for CD30. Cases demonstrating positivity for B-
cell markers were excluded. Immunostains for the
anaplastic lymphoma kinase (ALK) protein (ALK1
mouse monoclonal antibody, Dako, Carpinteria, CA)
were performed on the 14 available ALCL specimens (six
of the ALCL specimens were no longer available). All
cases of NKTCL were positive for Epstein–Barr virus
(EBV) sequences detected by in situ hybridization with an
oligonucleotide probe for EBV-related RNAs.
Staging
All patients underwent routine laboratory studies and
computed tomography (CT) scans of the head and neck as
appropriate, chest and abdomen for staging. Twenty-two
TABLE I Prognostic systems
Variable Adverse Feature
(A) The University of Texas M.D. Anderson Cancer Center’s tumor score (MDATS) for aggressive lymphomas*Lactate dehydrogenase $ 1:1 £ upper limit of normal, i.e. $ 685 IU=l at M.D. AndersonAnn Arbor Stage III or IVSymptoms “B” ¼ (1) unexplained, recurrent or sustained fevers ðT . 388CÞ; (2) drenching night sweats; or
(3) weight loss . 10% over the 6 months prior to diagnosisTumor bulk† MassðesÞ $ 7 cm or a mediastinal mass visible on a standing, PA chest X-rayBeta-2 microglobulin‡ $ 1:5 £ upper limit of normal, i.e. $ 3:0 mg=l at M.D. Anderson
(B) International prognostic index{
Lactate dehydrogenase . normalAnn Arbor Stage III or IVZubrod performance status $ 2Extranodal involvement . 1siteAge . 60 years
* Each adverse feature is assigned one point. One point is assigned for each bulky mass. The sum of the points is the tumor score.† Cases with extranodal head and neck presentations, not measurable bidimensionally, are assessed using the 1992 American Joint Committee on Cancer staging systemwherein T3–T4 tumors are considered bulky. Other extranodal presentations such as in the stomach, kidneys or liver: if not measurable, are considered bulky if $ 2=3 of theorgan is involved.‡ For primary mediastinal lymphomas, $ 0:8 £ upper limit of normal for lymphomas arising at any site, i.e. $ 1:6 mg=l at M.D. Anderson.{ Each adverse feature is assigned one point. The sum of the points is the international prognostic index (IPI).
TABLE II Patient characteristics
Chemotherapyonly ðn ¼ 15Þ
Chemotherapy andRadiotherapy ðn ¼ 24Þ p value
HistologyALCL 10 10PTCLu 4 7NKTCL 1 7 0.18
StageI 7 15II 8 9 0.33
GenderFemale 4 9Male 11 15 0.49
Age, yearsMedian 39 48.5 0.52
MDATS0–2 11 183–4 4 6 0.91
IPI0–1 13 212 2 3 0.94
ALCL, anaplastic large cell lymphoma; PTCLu, peripheral T-cell lymphoma-unspecified; NKTCL, nasal-type NK/T-cell lymphoma; IPI, internationalprognostic index; MDATS, M.D. Anderson tumor score.
H.K. LEE et al.1770
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.

patients underwent lymphangiograms. Two patients
underwent staging laparotomies. Bone marrow biopsies
were performed in all but two patients. Gallium or
positron emission tomography scans were not routinely
obtained.
Treatment Modality
The chemotherapy was doxorubicin-based, and a median
of six cycles was administered (range, 1–9). The most
common chemotherapeutic regimen used was cyclophos-
phamide, doxorubicin, vincristine, and prednisone
(CHOP; n ¼ 26). The doses for each 3-week cycle of
CHOP were 750 mg/m2 cyclophosphamide intravenously
(i.v.) on day 1, 25 mg/m2/day doxorubicin i.v. by
continuous infusion on days 1 and 2, 1.4 mg/m2
(maximum, 2 mg) vincristine i.v. on day 1, and 100 mg
prednisone orally on days 1–5. The second most common
chemotherapeutic regimen used was doxorubicin, methyl-
prednisolone, cytarabine, and platinum (ASHAP; n ¼ 7).
Fifteen patients received chemotherapy as their sole
treatment (Table II). Response to chemotherapy was
assessed according to international working group
guidelines [22]. Twenty-four patients received chemother-
apy followed 3–4 weeks later by involved-field radio-
therapy. Total radiotherapy dose ranged from 5 to 60 Gy,
with a median of 40 Gy given in 20 daily 2-Gy fractions.
There was no significant difference in age, gender,
histology, stage, or prognostic scores between the groups
treated with chemotherapy alone or chemotherapy
followed by radiotherapy (Table II).
Statistical Analysis
Kaplan–Meier curves [23] were generated for local
control, progression-free survival, and overall survival.
Curves were compared using the log-rank test [24]. The
two-sided Fisher’s exact test and the Pearson chi-square
test were used to compare treatment groups. Patients with
stage-adjusted MDATS of 0–2 or IPI of 0–1 were
considered the low-risk group [16,17], whereas patients
with higher scores were considered the intermediate-risk
group.
RESULTS
The median follow-up of surviving patients was 85
months.
Histology and Stage
The 5-year local control, progression-free survival, and
overall survival rates for all 20 ALCL patients were 74, 74,
and 79%, respectively. Comparison of outcome by
whether immunohistochemical staining for ALK was
positive ðn ¼ 3Þ or negative ðn ¼ 11Þ showed no
significant difference in local control (5-year rates:
67 vs. 64%, p ¼ 0:99), progression-free survival (5-year
rates: 67 vs. 64%, p ¼ 0:99), or overall survival (5-year
rates: 100 vs. 82%, p ¼ 0:29), though the statistical power
was limited. There was no significant difference in local
control (5-year rates: 68 vs. 80%, p ¼ 0:59), progression-
free survival (5-year rates: 68 vs. 80%, p ¼ 0:59), or
overall survival (5-year rates: 78 vs. 80%, p ¼ 0:69) for
ALCL patients treated with chemotherapy and radio-
therapy vs. chemotherapy alone.
Eight of 11 (73%) PTCLu patients had a stage-adjusted
MDATS ¼ 0–2 and 9/11 (82%) had a stage-adjusted
IPI ¼ 0–1: The 5-year local control, progression-free
survival, and overall survival rates for all 11 PTCLu
patients were 64, 64, and 73%, respectively. Local control
(5-year rates: 86 vs. 25%, p ¼ 0:02) and progression-free
survival (5-year rates: 86 vs. 25%, p ¼ 0:02) were
significantly better in PTCLu patients who received
chemotherapy and radiotherapy as opposed to chemother-
apy alone. However, there was no significant difference in
overall survival between the two treatment groups (5-year
rates: 86 vs. 50%, p ¼ 0:41).
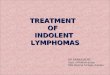
There was a trend towards inferior local control in
patients with NKTCL, with a 5-year local control rate of
50% compared to 70% for patients with ALCL or PTCLu
ðp ¼ 0:08Þ: Similarly, patients with NKTCL had inferior
progression-free survival compared to patients with ALCL
or PTCLu (Fig. 4; 5-year rates: 38 vs. 70%, respectively;
p ¼ 0:03). The 5-year overall survival rate for patients
with NKTCL was 50% compared to 77% for patients with
ALCL or PTCLu ðp ¼ 0:24Þ: In the six NKTCL patients
with a stage-adjusted MDATS ¼ 0–2; the 5-year local
control, progression-free survival, and overall survival
rates were 67, 50, and 67%, respectively. There was a
trend toward improved local control (5-year rates: 57 vs.
0%, p ¼ 0:08), progression-free survival (5-year rates: 43
vs. 0%, p ¼ 0:08), and overall survival (5-year rates: 57
vs. 0%, p ¼ 0:13) in NKTCL patients who received
chemotherapy and radiotherapy rather than chemotherapy
alone.
Treatment Modality
Patients with bulky disease as defined by the MDATS
(Table I) were typically treated with chemotherapy and
involved-field radiotherapy rather than chemotherapy
alone (75 vs. 33%, p ¼ 0:02). However, the percentage
of low-risk patients based on stage-adjusted MDATS or
IPI was not significantly different between the two
treatment groups (Table II). Even though patients with
mature peripheral T-cell neoplasms who achieved less
than a complete response to chemotherapy tended to be
treated with chemotherapy and radiotherapy rather than
chemotherapy alone (25 vs. 0%, p ¼ 0:06), there were no
significant differences in local control, progression-free
survival, or overall survival between the two treatment
groups (Table III).
EARLY STAGE PERIPHERAL T-CELL LYMPHOMAS 1771
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.

Prognostic Systems
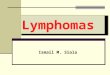
Local control for the low- and the intermediate-risk
patients based on stage-adjusted MDATS and IPI is shown
in Fig. 1. A significant difference in local control between
the two risk groups was observed when the MDATS
system was used ðp ¼ 0:007Þ: In contrast, no significant
difference in local control was observed using the IPI
system ðp ¼ 0:29Þ: Progression-free survival based on the
two prognostic systems is shown in Fig. 2. When MDATS
was used to assign score, progression-free survival was
significantly different ðp ¼ 0:01Þ between the low- and the
intermediate-risk groups. No significant difference in
outcome was observed if IPI was used to assign score
ðp ¼ 0:34Þ: In Fig. 3, overall survival is displayed based
on MDATS and IPI. Overall survival was significantly
different for the low- and intermediate-risk groups when
stage-adjusted MDATS was used as the prognostic system
ðp ¼ 0:001Þ: In contrast, stage-adjusted IPI did not predict
for significantly different outcomes ðp ¼ 0:40Þ; though the
conclusion is limited by the low statistical power.
Patterns of Failure
Fifteen (38%) patients relapsed. Local relapse was the
predominant pattern of failure, regardless of the WHO
diagnosis. In 12 of 15 (80%) patients, first recurrence was
limited to the initial site of disease. Seven of these patients
received chemotherapy followed by involved-field radio-
therapy and five received chemotherapy alone. In one
patient, whose primary tumor originated in the axilla,
recurrence was limited to a cervical lymph node. In two
patients, initial recurrences appeared in both local and
distant sites. Among the 24 patients who received
chemotherapy and involved-field radiotherapy, the
response to induction chemotherapy (complete vs. less
than complete) did not significantly affect local control (5-
year rates: 71 vs. 67%, respectively, p ¼ 0:84).
DISCUSSION
Most [10,25–27] though not all [19] groups have been
able to predict the outcome of patients with peripheral T-
cell lymphomas using the IPI [17]. The results from our
study ðn ¼ 39Þ suggest that, in the subgroup of patients
with early-stage ALCL, PTCLu, or NKTCL, MDATS may
be a better prognostic system than IPI. However, this
hypothesis needs to be tested prospectively.
The MDATS (Table I) was proposed as a prognostic
system for aggressive lymphomas in 1992 [16]. Most of
the factors that comprise the MDATS are tumor-dependent
rather than patient-related, e.g. factors such as age and
performance status were not included. In contrast, bulky
disease [18] and serum beta-2 microglobulin [19,20] were
included in an effort to reflect the biological character-
istics of the tumor. Our group [4] previously reported the
outcomes of 560 patients with aggressive lymphoma in
terms of MDATS and IPI. MDATS and IPI were
TABLE III Local control, progression-free survival, and overall survival based on treatment
5-year local 5-year progression-free 5-year overall
Treatment Control (%) p value Survival (%) p value Survival (%) p value
Chemotherapy only ðn ¼ 15Þ 70 60 67Chemotherapy and Radiotherapy ðn ¼ 24Þ 60 65 74
0.49 0.62 0.47
FIGURE 1 Local control in terms of the stage-adjusted M.D. Anderson tumor score (MDATS) and international prognostic index (IPI).
H.K. LEE et al.1772
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.

independent predictors of failure-free survival and overall
survival.
Adverse prognostic features such as an elevated serum
beta-2 microglobulin level or the presence of B symptoms
are commonly present in patients with PTCLu
[2,4,5,8,19,28,29]. Lopez-Guillermo et al. [10] reported
on 174 patients with PTCLu and observed that the
presence of B symptoms or an elevated serum beta-2
microglobulin level was associated with poor overall
survival. Lippman et al. [1] observed that the presence of
B symptoms was associated with poor disease-free
survival. Hatta et al. [29] studied 53 patients with
sinonasal tract lymphoma. Patients with B symptoms had
a poor prognosis. The usefulness of the MDATS in
patients with peripheral T-cell lymphomas may in part be
explained by the relatively high incidence of B symptoms
and an elevated beta-2 microglobulin level in such
patients.
Patients with PTCLu typically present with dissemi-
nated disease, including bone marrow involvement [5].
This study was limited to patients with early-stage disease
and included only 11 patients with PTCLu, most of whom
had #2 adverse prognostic features, which helps to
explain the relatively favorable 5-year progression-free
and overall survival rates of 64 and 73%, respectively.
Seven of the 11 PTCLu patients were treated with
consolidative radiotherapy, which resulted in a significant
improvement in local control and progression-free
survival. Based on the 5-year progression-free and overall
survival rates of only 26 and 24%, respectively, that have
been observed in peripheral T-cell lymphoma patients
with a MDATS . 2 [4], we are currently studying high-
dose chemotherapy and transplantation as the initial
treatment for these patients [30].
The patients with NKTCL in our study tended to
experience worse local control and overall survival and
experienced significantly worse progression-free survival
(Fig. 4) than the patients with ALCL or PTCLu. Poor
outcomes in patients with NKTCL has been described by a
number of groups [29,31–35]. In contrast, ALCL has a
relatively favorable prognosis, especially in ALK þ
patients [5,10,25,27,36]. Gascoyne et al. [27] reported
FIGURE 2 Progression-free survival in terms of the stage-adjusted M.D. Anderson tumor score (MDATS) and international prognostic index (IPI).
FIGURE 3 Overall survival in terms of the stage-adjusted M.D. Anderson tumor score (MDATS) and international prognostic index (IPI).
EARLY STAGE PERIPHERAL T-CELL LYMPHOMAS 1773
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.

5-year overall survival rates of 79% vs. only 46% in
patients with ALK þ vs. ALK 2 ALCL, respectively. In
support of these findings, Falini et al. [25] reported 5-year
overall survival rates of 71 and 15% in patients with
ALK þ and ALK 2 ALCL, respectively. While our
study had too few patients to make a meaningful
comparison between ALK þ and ALK 2 ALCL, we
observed a 5-year overall survival of 79% (95%
confidence interval: 57–92%) for all 20 patients with
ALCL (Table III), which is consistent with other
published reports [5,10].
Kim et al. [33] reported results in patients with NKTCL
of the head and neck who received involved-field
radiotherapy alone (median dose, 50.4 Gy). In their
study, 50% of patients developed a local recurrence and
25% relapsed in a distant site. Shikama et al. [37] reported
a 5-year disease-free survival rate of 83% using
radiotherapy (median dose, 49 Gy) with or without
chemotherapy in 25 stage IE patients with nasal
lymphoma. The most common recurrence site was local,
and 5/6 patients with a local recurrence received ,50 Gy.
Hence, doses ,50 Gy must be considered inadequate in
patients who receive radiotherapy alone. Kim et al. [31]
observed no relapses in 4 NKTCL patients who
completely responded to 4 cycles of CHOP chemotherapy
and then received radiotherapy to 45 Gy. Fifteen (38%)
patients in our study relapsed, with the majority (80%) of
the first relapses occurring only at the initial site of
disease. The median dose in our study was 40 Gy.
The patterns of failure described above suggest that
prevention of relapse in the initial site of disease is a
worthwhile goal in patients with peripheral T-cell
lymphomas. Adjuvant radiotherapy doses $45 Gy appear
to be warranted in patients with peripheral T-cell
lymphomas, even if a complete response to induction
chemotherapy is achieved. Since NKTCL is almost
universally associated with Epstein–Barr virus [38],
immunotherapy strategies targeting Epstein–Barr virus
antigens expressed by malignant cells are worth exploring
[34]. More effective systemic therapy, combined with
radiotherapy to $45 Gy, may improve local control. The
use of chemotherapy and concurrent radiotherapy, which
is effective in epithelial tumors, also warrants study. In
addition, high-dose chemotherapy followed by bone
marrow transplantation has been used in patients with
recurrent PTCLu and NKTCL with encouraging results
[30,35].
In conclusion, patients with NKTCL experienced
suboptimal results even when they presented with few
adverse features. The main pattern of failure was at the
initial site of disease after the delivery of doxorubicin-
based chemotherapy with or without involved-field
radiotherapy to a median dose of 40 Gy. Consequently,
we believe that systemic therapy and radiotherapy to doses
of least 45 Gy warrants investigation. We hope that new
approaches, such as cyclophosphamide, vincristine, and
prednisone chemotherapy with concomitant involved-field
radiotherapy to 45 Gy given in 25 daily 1.8-Gy fractions,
will improve the outlook for patients with peripheral T-
cell lymphomas.
Acknowledgements
This work was supported by grants CA 6294 and CA
16672 from the National Cancer Institute, National
Institutes of Health, U.S. Department of Health and
Human Services. Presented at the 2001 Pan Pacific
Lymphoma Conference, June 19–22, 2001, Wailea, HI.
References
[1] Lippman, S.M., Miller, T.P., Spier, C.M., Slymen, D.J. and Grogan,T.M. (1988) “The prognostic significance of the immunotype indiffuse large-cell lymphoma: a comparative study of the T-cell andB-cell phenotype”, Blood 72, 436–441.
[2] Coiffier, B., Brousse, N., Peuchmaur, M., Berger, F., Gisselbrecht,C., Bryon, P.A. and Diebold, J. (1990) “Peripheral T-celllymphomas have a worse prognosis than B-cell lymphomas: aprospective study of 361 immunophenotyped patients treated withthe LNH-84 regimen. The GELA (Groupe d’Etude des LymphomesAgressives)”, Annals of Oncology 1, 45–50.
[3] Slymen, D.J., Miller, T.P., Lippman, S.M., Spier, C.M., Kerrigan,D.P., Rybski, J.A., Rangel, C.S., Richter, L.C. and Grogan, T.M.(1990) “Immunobiologic factors predictive of clinical outcome indiffuse large-cell lymphoma”, Journal of Clinical Oncology 8,986–993.
[4] Melnyk, A., Rodriguez, A., Pugh, W.C. and Cabanillas, F. (1997)“Evaluation of the Revised European-American Lymphomaclassification confirms the clinical relevance of immunophenotypein 560 cases of aggressive non-Hodgkin’s lymphoma”, Blood 89,4514–4520.
[5] Gisselbrecht, C., Gaulard, P., Lepage, E., Coiffier, B., Briere, J.,Haioun, C., Cazals-Hatem, D., Bosly, A., Xerri, L., Tilly, H., Berger,F., Bouhabdallah, R. and Diebold, J. (1998) “Prognosticsignificance of T-cell phenotype in aggressive non-Hodgkin’slymphomas. Groupe d’Etudes des Lymphomes de l’Adulte(GELA)”, Blood 92, 76–82.
[6] Cheng, A.L., Chen, Y.C., Wang, C.H., Su, I.J., Hsieh, H.C., Chang,J.Y., Hwang, W.S., Su, W.C., Liu, T.W., Tien, H.F., et al., (1989)“Direct comparisons of peripheral T-cell lymphoma with diffuse B-cell lymphoma of comparable histological grades-should peripheralT-cell lymphoma be considered separately?”, Journal of ClinicalOncology 7, 725–731.
FIGURE 4 Progression-free survival for patients with early-stagemature T-cell lymphomas in terms of the WHO diagnosis.
H.K. LEE et al.1774
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.

[7] Kwak, L.W., Wilson, M., Weiss, L.M., Doggett, R., Dorfman, R.F.,Warnke, R.A. and Horning, S.J. (1991) “Similar outcome oftreatment of B-cell and T-cell diffuse large-cell lymphomas: theStanford experience”, Journal of Clinical Oncology 9, 1426–1431.
[8] Liang, R., Todd, D. and Ho, F.C. (1996) “Aggressive non-Hodgkin’slymphoma: T-cell versus B-cell”, Hematological Oncology 14,1–6.
[9] Harris, N.L., Jaffe, E.S., Diebold, J., Flandrin, G., Muller-Hermelink, H.K., Vardiman, J., Lister, T.A. and Bloomfield, C.D.(1999) “World Health Organization classification of neoplasticdiseases of the hematopoietic and lymphoid tissues: report of theClinical Advisory Committee meeting-Airlie House, Virginia,November 1997”, Journal of Clinical Oncology 17, 3835–3849.
[10] Lopez-Guillermo, A., Cid, J., Salar, A., Lopez, A., Montalban, C.,Castrillo, J.M., Gonzalez, M., Ribera, J.M., Brunet, S., Garcia-Conde, J., Fernandez de Sevilla, A., Bosch, F. and Montserrat, E.(1998) “Peripheral T-cell lymphomas: initial features, naturalhistory, and prognostic factors in a series of 174 patients diagnosedaccording to the REAL. Classification”, Annals of Oncology 9,849–855.
[11] “A clinical Evaluation of the International Lymphoma Study Groupclassification of non-Hodgkin’s lymphoma.” The non-Hodgkin’sLymphoma Classification Project. Blood, 89 (1997) 3909–3918.
[12] Morgan, G., Vornanen, M., Puitinen, J., et al., (1997) “Changingtrends in the incidence of non-Hodgkin’s lymphoma in EuropeBiomed Study Group”, Annals of Oncology 8, 49–54.
[13] Miller, T.P., Leblanc, M., Spier, C., Chase, E. and Fischer, R.I.(2001) “CHOP alone compared to CHOP plus radiotherapy forearly stage aggressive non-Hodgkin’s lymphomas: Update of theSouthwest Oncology Group (SWOG) randomized trial”, Blood 98,724a.
[14] Horning, S.J., Glick, J.H., Kim, K., Earle, J., O’Connell, M.J.,Habermann, T., Weller, E. and Gray, R. (2001) “Final report ofE1484: CHOP v CHOP þ radiotherapy (RT) for limited stagediffuse aggressive lymphoma”, Blood 98, 724a.
[15] Reyes, F., Lepage, E., Munck, J.N., Morel, P., Coiffier, B., Lederlin,P., et al., (2000) “Superiority of the ACVBP regimen over acombined treatment with three cycles of CHOP followed byinvolved field radiotherapy in patients (pts) with low risk localizedaggressive non-Hodgkin’s lymphoma: Results of the LNH93-1study”, Blood 93, 832a.
[16] Rodriguez, J., Cabanillas, F., McLaughlin, P., Swan, F., Rodriguez,M., Hagemeister, F. and Romaguera, J. (1992) “A proposal for asimple staging system for intermediate grade lymphoma andimmunoblastic lymphoma based on the tumor score”, Annals ofOncology 3, 711–717.
[17] “A predictive model for aggressive non-Hodgkin’s lymphoma.” TheInternational Non-Hodgkin’s Lymphoma Prognostic FactorsProject. New England Journal of Medicine, 329 (1993) 987–994.
[18] Wilder, R.B., Rodriguez, M.A., Ha, C.S., Pro, B., Hess, M.A.,Cabanillas, F. and Cox, J.D. (2001) “Bulky disease is an adverseprognostic factor in patients treated with chemotherapy comprisedof cyclophosphamide, doxorubicin, vincristine and prednisone withor without radiotherapy for aggressive lymphoma”, Cancer 91,2440–2446.
[19] Aviles, A., Diaz, N.R., Neri, N., Cleto, S. and Talavera, A. (2000)“Angiocentric nasal T/natural killer cell lymphoma: a single centrestudy of prognostic factors in 108 patients”, Clinical andLaboratory Haematology 22, 215–220.
[20] Johnson, P.W., Whelan, J., Longhurst, S., Stepniewska, K.,Matthews, J., Amess, J., Norton, A., Rohatiner, A.Z. and Lister,T.A. (1993) “Beta-2 microglobulin: a prognostic factor in diffuseaggressive non-Hodgkin’s lymphomas”, British Journal of Cancer67, 792–797.
[21] Carbone, P.P., Kaplan, H.S., Musshoff, K., Smithers, D.W. andTubiana, M. (1971) “Report of the committee on Hodgkin’s diseasestaging classification”, Cancer Research 31, 1860–1861.
[22] Cheson, B.D., Horning, S.J., Coiffier, B., Shipp, M.A., Fisher, R.I.,Connors, J.M., Lister, T.A., Vose, J., Grillo-Lopez, A., Hagenbeek,A., Cabanillas, F., Klippensten, D., Hiddemann, W., Castellino, R.,Harris, N.L., Armitage, J.O., Carter, W., Hoppe, R. and Canellos,G.P. (1999) “Report of an international workshop to standardize
response criteria for non-Hodgkin’s lymphomas”, Journal ofClinical Oncology 17, 1244–1253.
[23] Kaplan, E.L. and Meier, P. (1958) “Nonparametric estimation fromincomplete observations”, Journal of the American StatisticalAssociation 53, 457–481.
[24] Mantel, N. (1966) “Evaluation of survival data and two rank orderstatistics arising in its consideration”, Cancer Chemotherapy Report50, 163–170.
[25] Falini, B., Pileri, S., Zinzani, P.L., Carbone, A., Zagonel, V., Wolf-Peeters, C., Verhoef, G., Menestrina, F., Todeschini, G., Paulli, M.,Lazzarino, M., Giardini, R., Aiello, A., Foss, H.D., Araujo, I.,Fizzotti, M., Pelicci, P.G., Flenghi, L., Martelli, M.F. and Santucci,A. (1999) “ALK þ lymphoma: clinico-pathological findings andoutcome”, Blood 93, 2697–2706.
[26] Ansell, S.M., Habermann, T.M., Kurtin, P.J., Witzig, T.E., Chen,M.G., Li, C.Y., Inwards, D.J. and Colgan, J.P. (1997) “Predictivecapacity of the International Prognostic Factor Index in patientswith peripheral T-cell lymphoma”, Journal of Clinical Oncology15, 2296–2301.
[27] Gascoyne, R.D., Aoun, P., Wu, D., Chhanabhai, M., Skinnider, B.F.,Greiner, T.C., Morris, S.W., Connors, J.M., Vose, J.M., Viswanatha,D.S., Coldman, A. and Weisenburger, D.D. (1999) “Prognosticsignificance of anaplastic lymphoma kinase (ALK) proteinexpression in adults with anaplastic large cell lymphoma”, Blood93, 3913–3921.
[28] Armitage, J.O., Greer, J.P., Levine, A.M., Weisenburger, D.D.,Formenti, S.C., Bast, M., Conley, S., Pierson, J., Linder, J., Cousar,J.B. and Nathwani, B.N. (1989) “Peripheral T-cell lymphoma”,Cancer 63, 158–163.
[29] Hatta, C., Ogasawara, H., Okita, J., Kubota, A., Ishida, M. andSakagami, M. (2001) “Non-Hodgkin’s malignant lymphoma of thesinonasal tract-treatment outcome for 53 patients according toREAL classification”, Auris Nasus Larynx 28, 55–60.
[30] Rodriguez, J., Munsell, M., Yazji, S., Hagemeister, F.B., Younes,A., Andersson, B., Giralt, S., Gajewski, J., de Lima, M., Courie1,D., Romaguera, J., Cabanillas, F.F., Champlin, R.E. and Khouri, I.F.(2001) “Impact of high-dose chemotherapy on peripheral T-celllymphomas”, Journal of Clinical Oncology 19, 3766–3770.
[31] Kim, W.S., Song, S.Y., Ahn, Y.C., Ko, Y.H., Baek, C.H., Kim, D.Y.,Yoon, S.S., Lee, H.G., Kang, W.K., Lee, H.J., Park, C.H. and Park,K. (2001) “CHOP followed by involved field radiation: is it optimalfor localized nasal natural killer/T-cell lymphoma?”, Annals ofOncology 12, 349–352.
[32] Kwong, Y.L., Chan, A.C., Liang, R., Chiang, A.K., Chim, C.S.,Chan, T.K., Todd, D. and Ho, F.C. (1997) “CD56 þ NKlymphomas: clinicopathological features and prognosis”, BritishJournal of Haematology 97, 821–829.
[33] Kim, G.E., Cho, J.H., Yang, W.I., Chung, E.J., Sub, C.O., Park,K.R., Hong, W.P., Park, I.Y., Hahn, J.S., Roh, J.K. and Kim, B.S.(2000) “Angiocentric lymphoma of the head and neck: patterns ofsystemic failure after radiation treatment”, Journal of ClinicalOncology 18, 54–63.
[34] Rodriguez, J., Romaguera, J.E., Manning, J., Ordonez, N., Ha, C.,Ravandi, F. and Cabanillas, F. (2000) “Nasal-type T/NKlymphomas: a clinicopathologic study of 13 cases”, Leukemia andLymphoma 39, 139–144.
[35] Liang, R., Chen, F., Lee, C.K., Kwong, Y.L., Chim, C.S., Yau, C.C.and Chiu, E. (1997) “Autologous bone marrow transplantation forprimary nasal T/NK cell lymphoma”, Bone Marrow Transplan-tation 19, 91–93.
[36] Stein, H., Foss, H.D., Durkop, H., Marafioti, T., Delsol, G., Pulford,K., Pileri, S. and Falini, B. (2000) “CD30(þ) anaplastic large celllymphoma: a review of its histopathologic, genetic, and clinicalfeatures”, Blood 96, 3681–3695.
[37] Shikama, N., Izuno, I., Oguchi, M., Gomi, K., Sone, S., Takei, K.,Sasaki, S., Wako, T., Itou, N. and Ishii, K. (1997) “Clinical stage IEprimary lymphoma of the nasal cavity: radiation therapy andchemotherapy”, Radiology 204, 467–470.
[38] Jaffe, E.S., Chan, J.K., Su, I.J., Frizzera, G., Mori, S., Feller, A.C.and Ho, F.C. (1996) “Report of the Workshop on Nasal and RelatedExtranodal Angiocentric T/Natural Killer Cell Lymphomas.Definitions, differential diagnosis, and epidemiology”, AmericanJournal of Surgical Pathology 20, 103–111.
EARLY STAGE PERIPHERAL T-CELL LYMPHOMAS 1775
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
5/14
For
pers
onal
use
onl
y.