Embed Size (px)
Citation preview

O R I G I N A L A R T I C L E S
Out-patient antihypertensive drug utilizationand stroke mortality
An ecological study
JUAN MERLO, LENNART RASTAM, JONAS RANSTAM, ANDERS WESSUNG, ARNE MELANDER •
Directly age-standardized rates of out-patient utilization of antihypertensive drugs (antlhypertenstves, diuretics andbeta-blockers) and stroke mortality in men and women (40-79 years of age) were compared over 4 years(1987-1990) In a mid western (Varmland) and a southern (Skane) province of Sweden and in their 49 (16 + 33)municipalities. In both genders, the stroke mortality and utilization rates of the 3 antihypertensive drug groups,both combined and separate, were higher in Varmland and there were positive correlations between these rateswhen all 49 municipalities were compared. On the other hand, for each province and each drug group there weremunicipalities with every possible combination of stroke mortality and antihypertensive drug utilization rates. Inaddition, antihypertensive drug utilization rates were similar in men and women even though the stroke mortalityrates were much lower among the latter. The findings cast doubt on the effectiveness of antihypertensive drugtreatment in common practice.
Key words: drug utilization, effectiveness, hypertension, stroke, ecological study, regional differences
Hypertension is the most common drug-treated cardio-vascular condition in out-patient care.1 One of the al-leged effects of antihypertensive pharmacotherapy is re-duction of stroke morbidity and mortality, and this hasbeen documented in several clinical trials.2"5 However, ithas been questioned whether an effect of similar magni-tude is also achieved in common practice.6'7
Comparisons of drug utilization and mortality or morbid-ity in different areas may be valuable in the evaluation ofdrug effectiveness in common practice.8"16 It is knownthat cardiovascular drug utilization and cardiovascularmortality are higher in midwestem than in mideastern17
and southern14 Sweden. Therefore, the aim of this studywas to compare out-patient antihypertensive drug utiliza-tion and stroke mortality among men and women in onemidwestern and one southern Swedish province and intheir 49 municipalities. The comparison was based ondirectly age-standardized data of mortality and drug util-ization as recently described.18
MATERIAL AND METHODSProvinces, counties and municipalities
The county of Varmland consists of the province ofVarmland, less one municipality, and is situated in mid-
• J. Merlo1, L Rijtam1. J. Raratam1, A. Wealing1, A. MeUnder1
1 Department of Community Medicine. Und Unlvenrty, Malmo Unh/enltyHojpital, Malmo, Sweden2 The NEPI Foundation. Malmo and Stockholm. Sweden3 The National Corporation of Pharmacies, Stockholm. Swed«nCorrespondence: Or J. Merlo, Department of Community Medicine,Medical Research Centre. Malmo University Hospital, S-205 02 Malmo,Sweden, tel +46 40 332064, fa* +46 40 336215
western Sweden. More than 70% of its area is forestterritory and forestry is a major occupation in the rural areas.Its population on 31 December 1990 was 283,110 inhabit-ants, 5% of whom were >79 years of age and 50% of whomwere women. The county comprises 16 municipalities.The province of Skane, which was part of Denmark until1658, is divided into 2 counties, Kristianstad andMalmohus, and constitutes the soudiemmost part of theScandinavian peninsula, surrounded by the Baltic sea andthe strait of Oresund. Most (90%) of the area is farmlandand fanning is a major occupation outside the urban areas.The Kristianstad county population on 31 December1990 was 289,278 inhabitants, 5% of whom were >79years of age and 50% of whom were women. The corres-ponding figures for Malmohus county were 779309 in-habitants, 5% of whom were >79 years of age and 51% ofwhom were women. Kristianstad county comprises 13municipalities and Malmohus county comprises 20 muni-cipalities. The demographic figures were obtained fromStatistics Sweden, Stockholm.
Out-patient annhypenensiveFour years (1987-1990) of out-patient antihypertensivedrug utilization data at the county and municipality levelswere obtained from the Continuous Recording of DrugPrescribing in Sweden, run since 1974 by the NationalCorporation of Pharmacies (Apoteksbolaget), Stock-holm, Sweden," which records all sales made at all Swed-ish pharmacies. The computerized survey is based onevery twenty-fifth prescription and provides informationabout die dispensing pharmacy, type of prescription, year
Dow
nloaded from https://academ
ic.oup.com/eurpub/article/6/2/113/596411 by guest on 28 January 2022
EUROPEAN JOURNAL OF PUBLIC HEALTH VOL 6 1996 NO. 2
and month of dispensing, year of birth and sex of thepatient and the trade name, quantity and price of die drug.Non-standardized drug utilization data were obtained in5-year age groups for the entire age span, but the agegroups studied after standardization were restricted tothose of 40-79 years. The data were expressed in defineddaily doses (DDD) per 1,000 inhabitants per day. Thedrug categories studied were i) antihypertensives (Ana-tomical Therapeutical Chemical Classification system20
code C 02), i.e. methyldopa, clonidine, alpha-blockers,labetalol, hydralazine, calcium antagonists (recently re-classified as C 08) and ACE inhibitors, ii) diuretics (C 03),i.e. diiazides and thiazide-like diuretics, loop diuretics andpotassium-retaining diuretics and iii) beta-blockers (C 07).The Swedish Diagnosis and Prescription Survey (SwedishDrug Statistics 1987-1990) has shown that the propor-tion of beta blockers (C 07), for treatment of essentialhypertension in the region (1.5 million inhabitants)which Varmland belongs to was 72% and in the region(1.9 million inhabitants) which Skane belongs to was76%. The corresponding figures for diuretics (C 03) were3 7 and 43% respectively and for antihypertensives (C 02),59 and 56% respectively. Hence, it is reasonable to assumethat the utilization rates of these drug groups give a fairreflection of the extent of antihypertensive drug utiliza-tion.
Stroke mortalityData on the causes of deadi of every subject residing inSweden at his/her time of death are entered in the Na-tional Mortality Register. Causes are categorized accord-ing to the International Classification of Diseases (ICD).The eighdi revision was used for deaths during 1987 and
the ninth for 1988-1990. Data on stroke mortality (ICDcodes 430-438) in each municipality were obtained dur-ing 1987-1990 for men and women aged 40-79 years.
Standardization and statisticsTo adjust for geographical differences in age distribution,direct age standardization wirh equal weights for all 5-yearage groups in bodi genders from 40 to 79 years was carriedout by the equivalent average rate (EAR) techniqueproposed by Yule21 and by the cumulative rate (CR)technique proposed by Day22, as recently described fordrug utilization studies.1" These 2 methods give essen-tially the same results; EAR is based on averages of ratesand CR is based on sums of rates, CR equalling EAR* \* vi,where 1 is the number of age groups and if is the width ofthe ith class.18 Statistical testing of differences and cor-relations was performed on data aggregated at the muni-cipal level. The Mann-Whitney test was used to assessbetween-county and between-gender differences in drugutilization and stroke mortality. Spearman rank correl-ation coefficients were used for correlation analyses. Allgiven p values are two-sided and those lower than 5%were considered as denoting statistical significance.
RESULTSStroke mortalityBy both direct age-standardization techniques, strokemortality rates (40-79 years range) were significantlyhigher in men dian in women (table I). In both genders,the rates were significantly higher in Varmland than inSkane (MalmohusandKristianstadcounties) (table l).lnVarmland, male stroke mortality rates were S200/100,000individuals in 12 of the 16 municipalities, whereas only 2
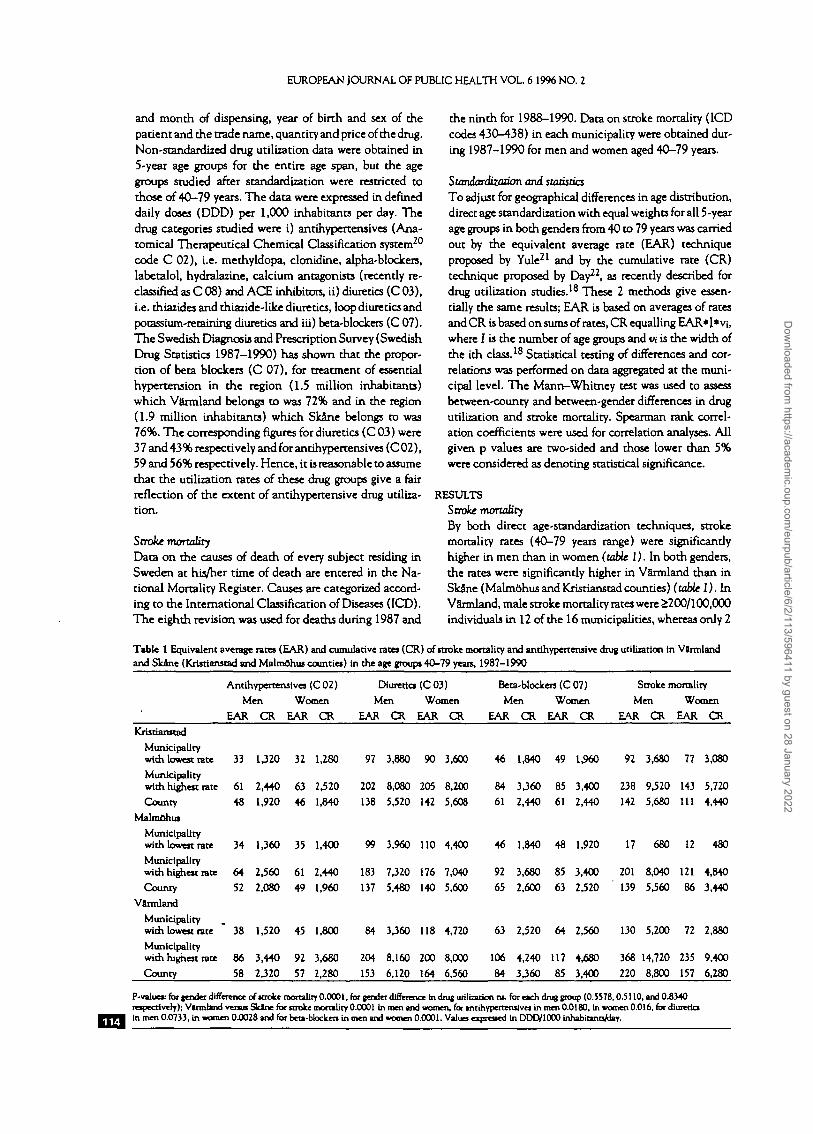
Table 1 Equivalent average rates (EAR) and cumulative rates (CR) of stroke mortality and antihypertensive drug utiliiarion tn Varmlandand Skane (Kristianstad and Malmohus counties) in the age groups 40-79 years, 1987-1990
Antihypertensives (C 02)
Men Women
EAR CR EAR CR
Diuretics (C 03)Men Women
EAR CR EAR CR
Beta-blockers (C 07)Men Women
EAR CR EAR CR
Stroke mortality
Men Women
EAR CR EAR CR
Kristianstad
Municipalitywith lowest rate
Municipalitywith highest rateCounty
Malmohus
Municipalitywith lowest rate
Municipalitywith highest rate
County
Varmland
Municipalitywith lowest rate
Municipalitywith highest rate
County
33 1,320 32 1,280 97 3,880 90 3,600 46 1,840 49 1,960 92 3,680 77 3,080
61 2,440 63 2,52048 1,920 46 1,840
202 8,080 205 8,200138 5,520 142 5,608
84 3,360 85 3,40061 2,440 61 2,440
238 9,520 143 5,720
142 5,680 111 4,440
34 1,360 35 1,400 99 3,960 110 4,400 46 1,840 48 1,920 17 680 12 480
64 2,560 61 2,440
52 2,080 49 1,960183 7,320 176 7,040
137 5,480 140 5,600
92 3,680 85 3,400 201 8,040 121 4,84065 2,600 63 2,520 139 5,560 86 3,440
38 1,520 45 1,800 84 3360 118 4,720 63 2,520 64 2,560 130 5,200 72 2,880
86 3,440 92 3,680
58 2320 57 2,280204 8,160 200 8,000
153 6,120 164 6,560
106 4.240 117 4,680
84 3360 85 3,400
368 14,720 235 9,400
220 8,800 157 6,280
P-valuec for lender difference of stroke mortality 0.0001, for gender difference In drag utilization ns. for e»ch drag group (0.5578,0.5110, and 0.8340respectively); Vlnnhnd rain Skint for stroke morality 0.0001 In men and women, for tntihypertetuivei in men 0.0180, tn women 0.016, for diureticsin men 0.0733, in women 0.0028 and for ben-btocken in men and women 0.0001. Values -r |v""^ in DDD/1000 InhabitanrVday.
Dow
nloaded from https://academ
ic.oup.com/eurpub/article/6/2/113/596411 by guest on 28 January 2022
Drug utilization and stroke mortality
j
oefc^y
200
Antihypertensives(C02)
of the 33 Skane municip- ...•; Antihypertensives
alities had correspondingly (C02)high rates in men (figure I).The female stroke mortalityrates were £150/100,000 in-dividuals in 9 of the 16 g-'soVarmland municipalities, ^whilst no Skane municip- Bality had such a high rate in js 120
women (figure 2). ~oo
Anahypenensive drug 3utilization ^ ®°The directly age-stand-ardized rate of utilization(40-79 years range) of anti-hypertensives (C 02), diuret-ics (C 03) and beta-blockers(C 07) together was signi-ficantly higher in Varmlandthan in Skane in both menand women (table I). Eventhe separate utilization ratesof antihypertensives (bothgenders), diuretics (womenonly) and beta-blockers(bodi genders) were signi-ficantly higher in Varmlandthan in Skane. Beta-blockersshowed the highest geo-graphical difference in util-ization rates (table 1). Therewere no significant differ-ences between men andwomen in drug utilizationrates (table 1).
Relations between stroke
mortality and
anakypertensive drug
utilizfltion
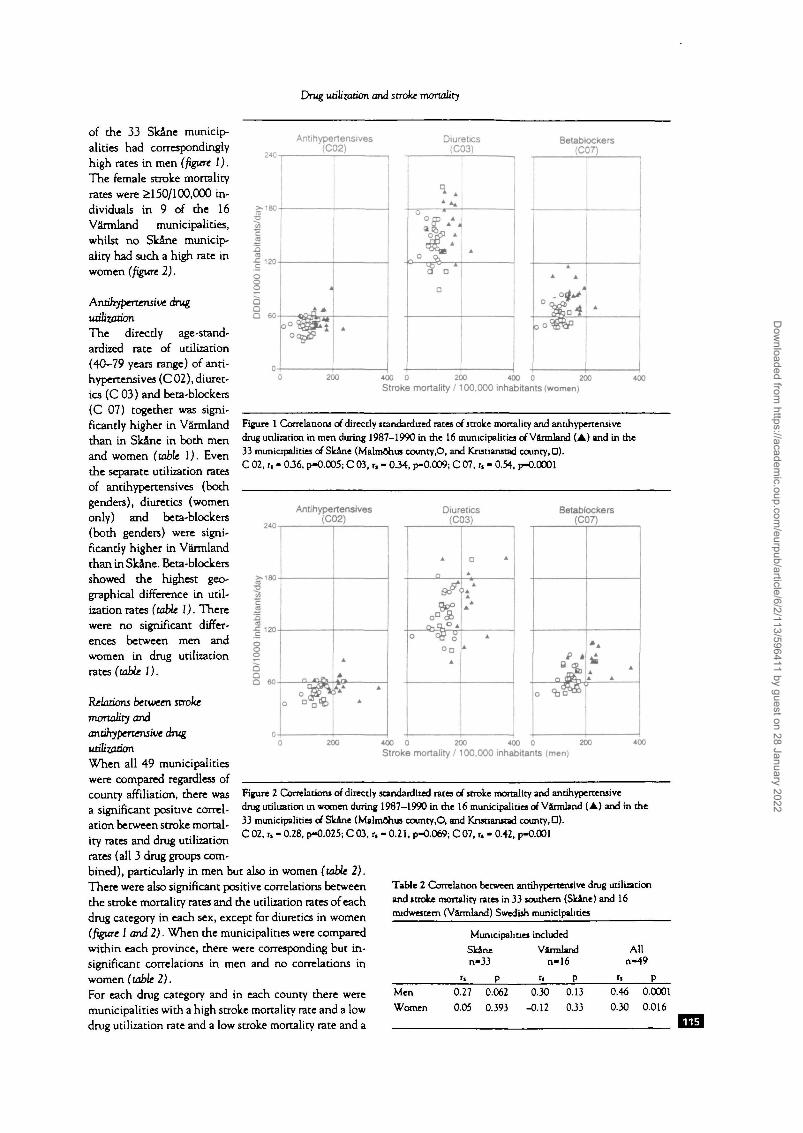
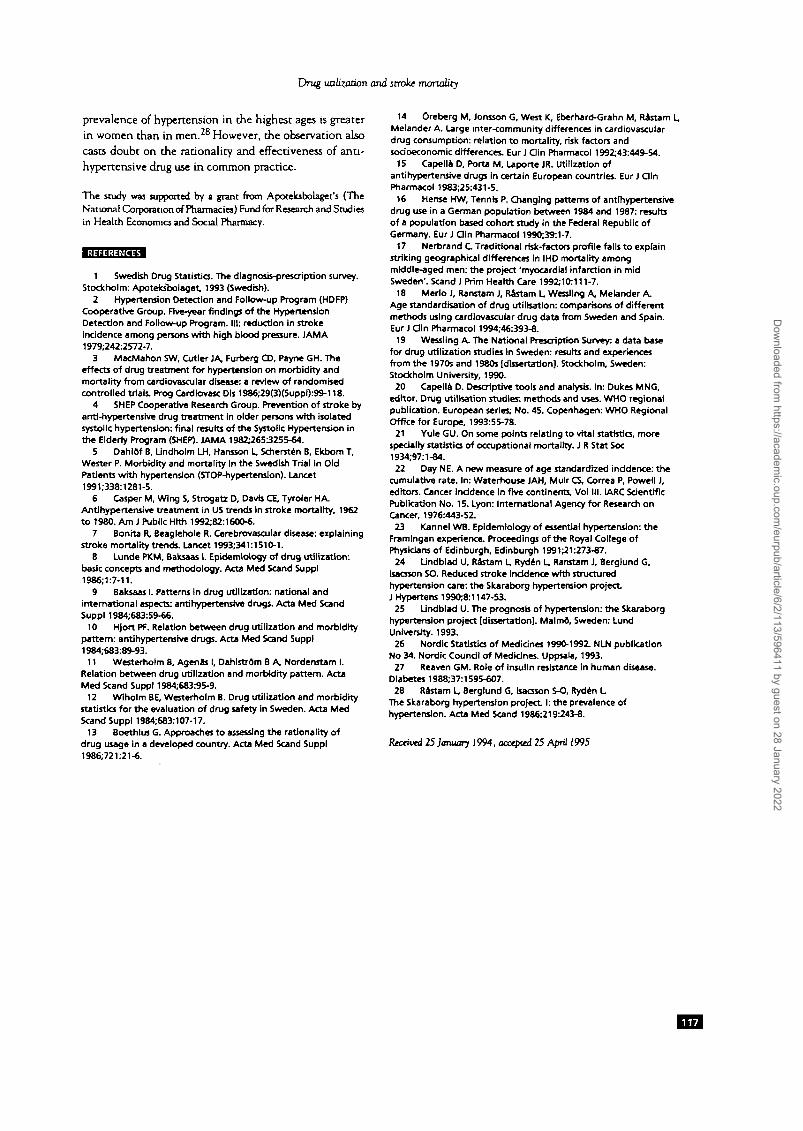
When all 49 municipalitieswere compared regardless ofcounty affiliation, there wasa significant positive correl-ation between stroke mortal-ity rates and drug utilizationrates (all 3 drug groups com-bined), particularly in men but also in women (table 2).There were also significant positive correlations betweenthe stroke mortality rates and the utilization rates of eachdrug category in each sex, except for diuretics in women(figure 1 and 2). When the municipalities were comparedwithin each province, there were corresponding but in-significant correlations in men and no correlations inwomen (table 2).For each drug category and in each county there weremunicipalities with a high stroke mortality rate and a lowdrug utilization rate and a low stroke mortality rate and a
Diuretics(C03)
AA ^
0 *O rp A
0 ° %
O
A
Betablockers(C07)
• • • JA
•00 0 200 400 0 200Stroke mortality /100,000 inhabitants (women)
Figure 1 Correlations of directly standardized rates of stroke mortality and annhypertensivedrug utilization in men during 1987-1990 in die 16 municipalities of Varmland (A) and in the33 municipalities of Skane (Malmohus county,O, and Krutianstad county, D).C 02, r, - 0.36, p-0.005; C 03, r. - 034, p-0.009; C 07, r, - 0.54, p-0.0001
•£ 120
SaQ
o ^Q
A
A
A
Diuretics(C03)
A
n
o SB ooa
A
a *A
A
A
A
Betablockers(C07)
e *
O u O"^^
* A
AA
A A
400 0 200 400 0Stroke mortality /100,000 inhabitants (men)
Figure 2 Correlations of directly standardized rates of stroke mortality and antihypertensivedrug utilization in women during 1987—1990 in die 16 municipalities of Varmland (A) and in die33 municipalities of Skane (Malmohus county.O, and Knsaanstad county, D).C 02, r, - 0.28, p-0.025; C 03, r, - 0.21, p-0.069; C 07, r, - 0.42, p-0.001
Table 2 Correlation between antihypeTtensive drug utilizationand stroke mortality rates in 33 southern (Skane) and 16midwestem (Varmland) Swedish municipalities
MenWomen
Municipalities included
Skanen-33
r, p
0.27 0.062
0.05 0.393
Varmlandn-16
u P0.30 0.13
-0.12 0J3
Alln-49
ri P
0.46 0.0001
0.30 0.016
Dow
nloaded from https://academ
ic.oup.com/eurpub/article/6/2/113/596411 by guest on 28 January 2022

EUROPEAN JOURNAL OF PUBLIC HEALTH VOL. 6 1996 NO. 2
high drug utilization rate, as well as high and low rates ofboth parameters (figure 1 and 2).
DISCUSSIONThe current study confirmed that stroke mortality ishigher in men than in women.23 It also indicated thatdirectly age-standardized stroke mortality, both in menand in women, was considerably.higher in the midwestemSwedish province of Varmland dian in the southernprovince of Sk3ne. This was further emphasized aftercomparison of die municipalities; die majority of Varm-land municipalities had stroke mortality rates of 200 per100,000 men and 150 per 100,000 women, whereas few(men) or no (women) Slcine municipalities had corres-pondingly high mortality rates. A previous study has alsoshown that the mortality of coronary heart disease ishigheT in Varmland than in Skane.14 The latter studyfurther suggested that there are both genetic-ethnic, en-vironmental and socioeconomic reasons for this differ-ence. It is likely that similarly complex factors are in-volved in the corresponding geographic differences instroke mortality rates.
Hypertension is the major risk factor for stroke,23 andstroke prevention is a main reason for the use of anti-hypertensivc drugs. The current data could be interpretedto mean that hypertension is more prevalent in Vannlandthan in Skane, but there are no actual prevalence data tocorroborate this assumption. Furthermore, it is not knownwhether stroke morbidity is higher in Varmland, norwhether the case/fatality ratios for stroke differ betweenVarmland and Skane.
Clinical trials2"5 and community-based interventions2*125
indicate that antihypertensive drug treatment may reducestroke mortality considerably. If this were so, even incommon practice, one should expect a negative correl-ation between stroke mortality and antihypertensive drugutilization, provided that hypertension is appropriatelydiagnosed, that doctors prescribe rationally, that thera-peutic compliance is high and that demographics, healthsystem resources and case/fatality ratios in areas of com-parison are similar. When all 49 municipalities werecompared regardless of county affiliation, positive insteadof negative correlations were found both for each druggroup and for the 3 groups combined. Also, both strokemortality and antihypertensive drug utilization rates werehigher in Varmland than in Skane although diere wereno significant wirhin-province correlations between the2 parameters. While raising doubts concerning the degreeof effectiveness of antihypertensive treatment in commonpractice, the findings need not signify inefficacy; rather,they indicate that a number of the assumed provisions donot apply.
Two recent reports have suggested that the long-termtrend of reduced stroke mortality in the US may be dueto better care of stroke cases, i.e. a decreased case/fatalityratio, rather than to increased antihypertensive drugtreatment.617 Varmland is generally less affluent thanSkane and has fewer hospitals and longer distances tohealth care centres and hospitals.14 Accordingly, the
higher stroke mortality rate in Varmland could at least inpart be due to less efficient stroke care in Varmland, i.e.an increased case/fatality ratio. Furthermore, previouslydemonstrated genetic-ethnic differences between (north-ern) Varmland and Sk3ne14 may influence the prognosisof hypertension and stroke. The medicosocial and eco-nomic disadvantages of Varmland may also signify thathypertension is less appropriately diagnosed and treated,dius reducing the stroke-preventive effectiveness of pre-scribed antihypertensive drugs. In this context, \hc parti-cularly high antihypertensive drug utilization in someVarmland municipalities known to have vacancies filledby doctors on very brief assignments could be an expres-sion of overtreatment, and lower dierapeutic complianceamong patients in Varmland is a related possibility.Assuming diat there is a steady state in the treatment ofhypertension in Sweden,26 we found it justified to performa cross-sectional study using parallel observations on drugutilization and stroke mortality. A 4-year period wasregarded necessary to minimize the influence of year toyear random variations.
It must be emphasized that this study was based on rathercrude data. This, together with the cross-sectional design,limit the possibility of making firm conclusions.The proportions of each of the 3 drug groups that wereused to treat hypertension differed only marginally be-tween the 2 health care regions in which the provinces ofSkane and Varmland are located (Swedish Diagnosis andPrescription Survey). However, because the health careregion was the lowest level of information in this respectthere is no way of adjusting for differences in the thera-peutic profiles between municipalities. The same is truefor age and gender.
A major confounding factor is that different types ofstroke have different causes. There is increasing evidencethat thromboembolic macrovascular diseases, such as oc-clusive stroke and myocardial infarction, are promoted bymetabolic-endocrine dysfunction, such as hypercholes-terolaemia and the insulin-resistance syndrome (the me-tabolic syndrome),27 rather than by hypertension; thelatter would be secondary or coincidental, rather thanprimary and causal, in this common syndrome. In con-trast, hypertension may be a primary cause in haemor-rhagic stroke.23 Accordingly, antihypertensive drug treat-ment would reduce the risk of haemorrhagic stroke butwould have a less preventive effect against thromboem-bolic stroke. As thromboembolic stroke is more commonthan haemorrhagic stroke in Sweden and most orherWestern countries, the relation between stroke mortalityand antihypertensive drug utilization should be weak, inaccordance with the present findings. It is also possiblethat the rate of haemorrhagic versus rhromboembolicstroke differs between Varmland and Skane, thus con-founding further the relation between stroke mortalityand antihypertensive drug utilization.An interesting observation was that antihypertensivedrug utilization rates were similar in men and women,even though the stroke mortality rate was much loweramong the laner. This may relate to the fact that die
Dow
nloaded from https://academ
ic.oup.com/eurpub/article/6/2/113/596411 by guest on 28 January 2022
Drug utilization and stroke mortality
prevalence of hypertension in the highest ages is greaterin women than in men.2 However, the observation alsocasts doubt on the rationality and effectiveness of anti-hypertensive drug use in common practice.
The study was supported by a grant from Apoteksbolaget's (TheNational Corporation of Pharmacies) Fund for Research and Studiesin Health Economics and Social Pharmacy.
1 Swedish Drug Statirtia. The diagnosis-prescription survey.Stockholm: Apoteksbolaget, 1993 (Swedish).
2 Hypertension Detection and Follow-up Program (HDFP)Cooperative Group. Five-year finding! of the HypertensionDetection and Follow-up Program. Ill: reduction in strokeIncidence among persons with high blood pressure. JAMA1979,242:2572-7.
3 MacMahon SW, Cutler JA. Furberg CD, Payne GH. Theeffects of drug treatment for hypertension on morbidity andmortality from cardiovascular disease: a review of randomisedcontrolled trials. Prog Cardlovasc Dis 19S6;29(3)(SuppO.-99-U8.
4 SHEP Cooperative Research Group. Prevention of stroke byanti-hypertensive drug treatment In older persons wtth isolatedsystolic hypertension: final results of the Systolic Hypertension inthe Elderly Program (SHEP). JAMA 1981265:3255-64.
5 Dahlof B, Undholm LH, Hansson L, Schersten B, Ekbom T,Wester P. Morbidity and mortality in the Swedish Trial in OldPatients with hypertension (STOP-hypertensJon). Lancet1991;338:1281-5.
6 Casper M, Wing S, Strogatz D, Davis CE. Tyroler HA.Antihypertensive treatment in US trends In stroke mortality, 1962to 1980. Am J Public Hlth 1992:82:1600-6.
7 Bonha R, Beaglehole R. Cerebrovascular disease: explainingstroke mortality trends. Lancet 1993:341:1510-1.
8 Lunde PKM, Baksaas I. Epidemiology of drug utilization:basic concepts and methodology. Acta Med Scand Suppl1986:1:7-11.
9 Baksaas I. Patterns In drug utilization: national andinternational aspects: antihypertensive drugs. Acta Med ScandSuppl 1984;683:59-66.
10 HJort PF. Relation between drug utilization and morbiditypattern: antihypertensive drugs. Acta Med Scand Suppl1984:683:89-93.
11 Westerholm S, Agenas I, Dahlstrom B A, Nordenstam I.Relation between drug utilization and morbidity pattern. ActaMed Scand Suppl 1984:683:95-9.
12 Wlholm BE, Westerholm B. Drug utilization and morbiditystatistics for the evaluation of drug safety in Sweden. Acta MedScand Suppl 1984:683:107-17.
13 Boethlus G. Approaches to assessing the rationality ofdrug usage in a developed country. Acta Med Scand Suppl1986:721:21-6.
14 Oreberg M, Jonsson G, West K, Eberhard-Grahn M, Rastam L,Melander A. Large inter-community differences in cardiovasculardrug consumption: relation to mortality, risk factors andsodoeconomic differences. Eur J din Pharmacol 1992:43:449-54.
15 Capella D, Porta M, Laporte JR. Utilization ofantihypertensive drugs in certain European countries. Eur J dinPharmacol 1983;25:431-5.
16 Hense HW, Tennis P. Changing patterns of antihypertensivedrug use in a German population between 1984 and 1987: resultsof a population based cohort study In the Federal Republic ofGermany. Eur J din Pharmacol 1990:39:1-7.
17 Nerbrand C Traditional risk-factors profile fails to explainstriking geographical differences in IHD mortality amongmiddle-aged men: the project 'myocardial Infarction in midSweden'. Scand J Prim Health Care 1992:10:111-7.
18 Merio J, Ranstam J, Rastam L, Wessling A, Melander A.Age standardisation of drug utilisation: comparisons of differentmethods using cardiovascular drug data from Sweden and Spain.Eur J din Pharmacol 1994:46:393-8.
19 Wessling A. The National Prescription Survey: a data basefor drug utilization studies In Sweden: results and experiencesfrom the 1970s and 1980s [dissertation]. Stockholm, Sweden:Stockholm University, 1990.
20 Capella D. Descriptive tools and analysis. In: Dukes MNG,editor. Drug utilisation studies: methods and uses. WHO regionalpublication. European series; No. 45. Copenhagen: WHO RegionalOffice for Europe, 1993:55-78.
21 Yule GU. On some points relating to vital statistics, morespecially statistics of occupational mortality. J R Stat Soc1934:97:1-84.22 Day NE. A new measure of age standardized incidence: the
cumulative rate. In: Waterhouse JAH, Mulr CS, Correa P, Powell J,editors. Cancer Incidence In five continents, Vol III. IARC ScientificPublication No. 15. Lyon: International Agency for Research onCancer, 1976:443-52.
23 Kannel WB. Epidemiology of essential hypertension: theFramingan experience. Proceedings of the Royal College ofPhysicians of Edinburgh, Edinburgh 1991:21:273-87.
24 Undblad U, Rastam L, Ryden L, Ranstam J, Berglund G,tsacsson SO. Reduced stroke Incidence with structuredhypertension care: the Skaraborg hypertension projectJ Hypertens 1990:8:1147-53.
25 Undblad U. The prognosis of hypertension: the Skaraborghypertension project [dissertation]. Malmd, Sweden: LundUniversity. 1993.26 Nordic Statistic of Medicines 1990-1992. NLN publication
No 34. Nordic Council of Medicines. Uppsala, 1993.27 Reaven GM. Role of Insulin resistance in human disease.
Diabetes 1988:37:1595-607.28 Rastam L, Berglund G, Isacsson S-O, Ryden L
The Skaraborg hypertension project I: the prevalence ofhypertension. Acta Med Scand 1986:219:243-8.
Received 25 January 1994, accepted 25 April 1995
Dow
nloaded from https://academ
ic.oup.com/eurpub/article/6/2/113/596411 by guest on 28 January 2022




























