Embed Size (px)
Citation preview

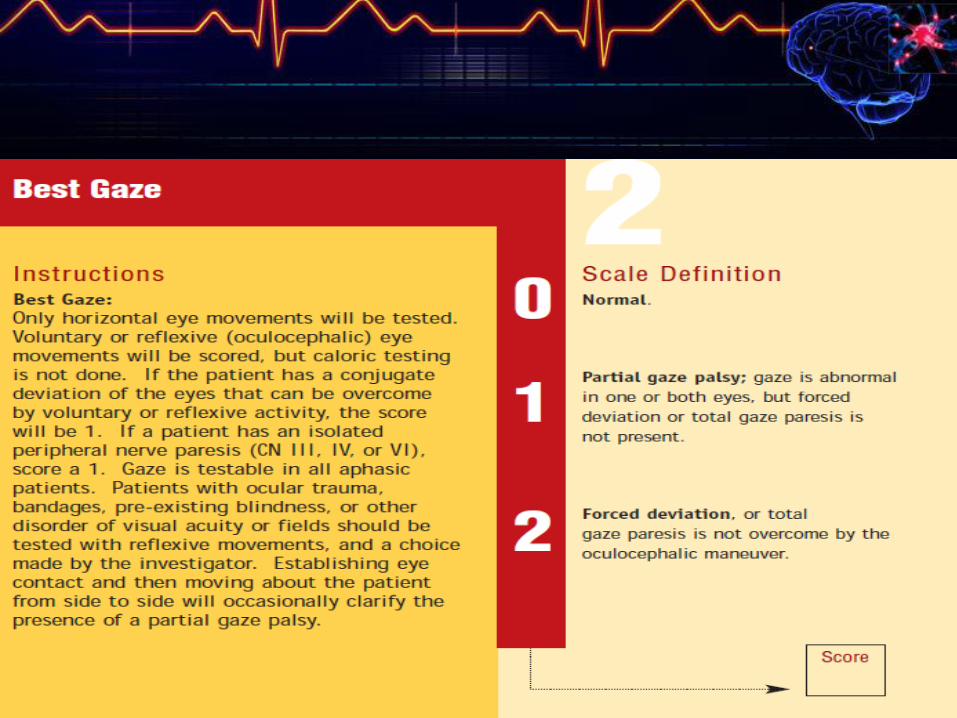
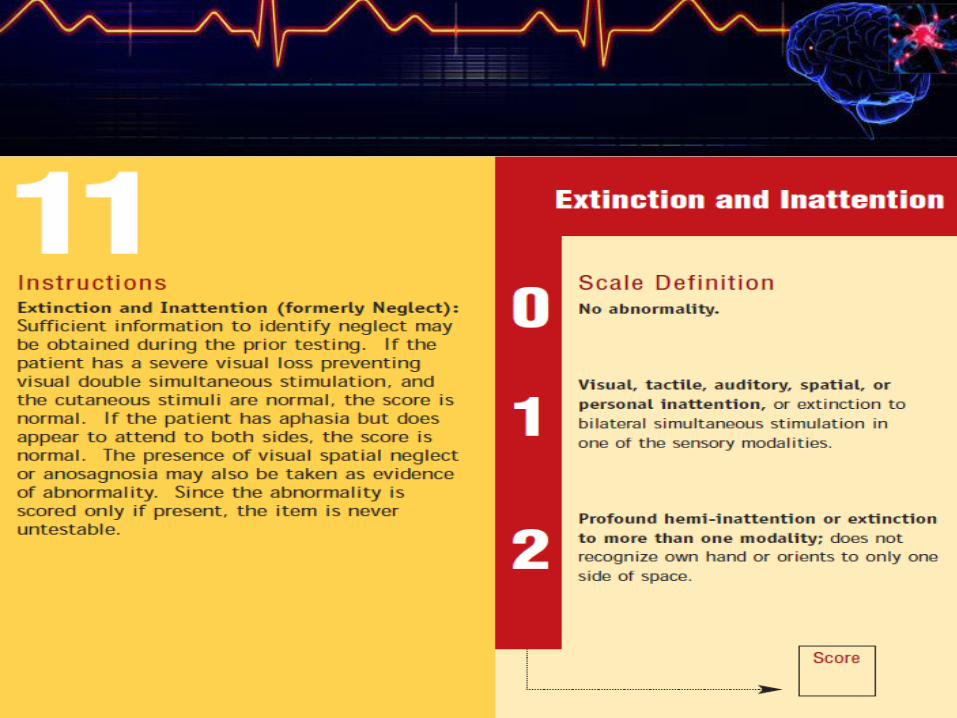
NIH Stroke
Scale &
Hospital
Management of
the Stroke
Patient
James Fleming, MD
Department of Neurology,
Erlanger Health System

NIH Stroke Scale














DO NOT NEED THESE!

Stroke CODE 1-2-3
• STROKE TEAM receive patient from EMS:
Accomplish upon arrival:
– Bedside Neuro exam (NIH Stroke Scale)
– Lab: CHEM 8, CBC, Coags, Type & Cross,
Pregnancy test and drug screen if appropriate
– Vital signs-(treat blood pressure if indicated: fever)
– 12 lead EKG (common problems w/ ICH and SAH)
– Evaluate for seizure activity at the scene or in the ED



Stroke Code
• If patient is candidate, then will proceed with
thrombolytic therapy (t-PA).
• Dosing: 0.9 mg/kg; maximum dose less than or
equal to 90mg.
– 10% of the total dose is administered as an IV bolus
over 1 minute.
– Remaining 90% is infused over 60 minutes
– Follow up: admit to ICU or Stroke Unit, monitor Vital
signs, Maintain < 180 mmHg if IV tPA given and < 160
after endovascular therapy or if ICH
– No anticoagulant therapy for 24 hours if received tPA

AFTER tPA - Complications
• Bleeding
– Initial signs may be obtundation,
headache, nausea, and vomiting
– Obtain STAT non-contrasted CT of
the brain
• Angioedema
– Medical emergency
– Treatment: Steroids, Histamine 1
and Histamine 2 blockers
– May require intubation
• At first sign of
complication, stop the
administration & call Neuro
Angioedema

General Stroke RN Management
1. Vital signs and Neuro checks (NIHSS) per protocol.
2. Titrate oxygen for Sat greater than 95%
3. Dysphagia Screen
4. Cardiac monitor
5. DVT prophylaxis (per stroke order set and tPA protocol)
6. GI prophylaxis
7. Euglycemia

8. I&O
9. Pressure Ulcer Prevention
10.Passive R.O.M. to prevent contractures or begin
mobility.
11.Pain management: H/A – tylenol is preferred, but for
SAH, opiates may be needed; antiemetics for N&V.
12.Activity per protocol
13.PT/OT to evaluate for discharge planning
14.GOAL: Prevent Falls and mobilize within 24-48
hours.

General Acute Stroke
Management
• DIAGNOSTIC TESTING – 24 hour needed
– Stroke Labs
– 2D Echo +- bubble study:
– Carotid Doppler not done typically
– 12 lead EKG: atrial fibrillation -
– MRI or MRA (if CTA not done)
– EEG if seizure activity noted
– 30 Day MCOT or LINQ may be ordered

Medical Acute Stroke
Management
• Antihypertensive management after 24 hrs
• Aspirin, if ischemic stroke (after 24 hrs if tPA)
• Anticoagulation if needed – time per Neurology
• Cholesterol lowering agents
• Strategies to control any seizure activity or
brain edema initiated in the ED will
continue: Mannitol-3% or AED.

General Management following
admission to the Hospital
• 10-20 % of all stroke
patients will
experience a
deterioration during
the first 24 hours and
outcomes in these
patients are worse.
• Neurological worsening can be due to:– Brain edema
– Acute hydrocephalus
– Seizures
– Progression of thrombosis
– Early recurrent embolization
– Vasospasm ->brain ischemia
– Continued bleeding
– Recurrent hemorrhage
– Medical Complications

In-House Stroke Alerts
RAPID RESPONSE TEAM
• For sudden changes in Level of Consciousness
or suspected stroke, Fire STROKE Pager (ICU)
or Rapid Response (for floor patients)
• Orders for Imaging (CT or CTA or CTP) will be
given by STROKE TEAM.

Complications of Stroke
• Brain edema
• Hydrocephalus
• Elevated ICP
• Seizures
• Hemorrhagic transformation of infarction
• Recurrent Hemorrhage
• Acute delirium
• Recurrent ischemic stroke
• Depression
• Aspiration
• Atelectasis
• Pneumonia
• AMI
• CHF
• DVT
• Pulmonary Embolism

EDUCATION IS KEY!
• Educate patients and family members
of stroke victims on modifiable risk
factors and lifestyle changes that will
prevent disability or death caused by
a second ischemic stroke.

EDUCATION TOPICS FOR THE PATIENT
• Stop Smoking
• Healthy Diet
• Manage Cholesterol
• Increase physical activity
• Lower blood pressure
• Limit alcohol, no illicit drugs
• Maintain good blood sugar
• Take antiplatelet agents as prescribed






























