Embed Size (px)
Citation preview
156
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 397, pp. 156–176© 2002 Lippincott Williams & Wilkins, Inc.
The purpose of the current study was to analyzethe long-term oncologic and functional resultsand complications associated with limb-sparingsurgery and endoprosthetic reconstruction for23 patients with osteosarcoma of the proximalhumerus. There was one Stage IIA lesion, 18Stage IIB lesions, and four Stage III lesions inthis study group. Twenty-two patients weretreated with an extraarticular resection that in-cluded the deltoid and rotator cuff and one pa-tient was treated with an intraarticular resec-tion that spared the shoulder abductors. In allthese patients, the proximal humerus was re-constructed with a cemented endoprosthetic re-placement that was stabilized via a technique ofstatic suspension (Dacron tapes) and dynamicsuspension (muscle transfers). At latest fol-lowup (median, 10 years), 15 patients (65%)were alive without evidence of disease. Therewere no local recurrences. Prosthetic survival
was 100% for the 15 survivors. The Muscu-loskeletal Tumor Society upper extremity func-tional score ranged from 24 to 27 (80%–90%).All shoulders were stable and pain-free. Elbowand hand function were preserved in all pa-tients. The most common complication was atransient neurapraxia (n � 8). En bloc extraar-ticular resection and endoprosthetic reconstruc-tion is a safe and reliable method of limb-sparing surgery for patients with high-gradeextracompartmental osteosarcoma of the proxi-mal humerus.
The proximal humerus is the third most com-mon site of origin for osteosarcoma22,44,49,51,52
(Fig 1). Before 1970, most patients with high-grade sarcomas arising in this location weretreated with a forequarter amputation.51 Theonly reported limb-sparing shoulder girdle re-sections were done for patients with low-gradescapular and periscapular sarcomas and weretermed Tikhoff-Linberg resections.16,38 Thisprocedure accomplished en bloc, extraarticu-lar resection of the entire scapula with the in-tracapsular portion of the proximal humerus,lateral 2⁄3 of the clavicle, and overlying deltoidand rotator cuff muscles.
The development of effective induction andadjuvant chemotherapy protocols prompted
Osteosarcoma of the Proximal Humerus: Long-Term Results With
Limb-Sparing Surgery
James C. Wittig, MD*; Jacob Bickels, MD**; Kristen L. Kellar-Graney, BS†; Frank H. Kim, MS†;
and Martin M. Malawer, MD†
From the *Department of Orthopedic Surgery, New YorkUniversity Medical Center and the Hospital for Joint Dis-eases, New York, NY; the **Tel-Aviv Sourasky MedicalCenter National Unit of Orthopedic Oncology; and the†Department of Orthopedic Oncology, Washington Can-cer Institute at the Washington Hospital Center, Wash-ington, DC.Reprint requests to Martin Malawer, MD, Department ofOrthopedic Oncology, Washington Cancer Institute,Suite C-2713, 110 Irving Street, N.W., Washington, DC20010.

Marcove et al50 to extend the indications forlimb-sparing shoulder girdle resections to in-clude high-grade sarcomas of the proximalhumerus and scapula. In 1977, they publishedthe first series of osteosarcomas of the proxi-mal humerus treated with wide, en bloc, ex-traarticular resection.50 This procedure, termeda modified Tikhoff-Linberg resection, entailedresection of the proximal humerus, intactglenohumeral joint, lateral 2⁄3 of the clavicle, ro-tator cuff muscles, and deltoid muscle. Surgi-cal margins and local tumor control rates weresimilar to those achieved with forequarter am-putation. Most important, survival did notseem to be compromised and a functional handand elbow were preserved. Limb-sparing re-section for patients with high-grade osteosar-
coma of the proximal humerus, in lieu of aforequarter amputation, subsequently becamewidely accepted.1,4,7,10,12,17,19,21,23,25,32,33,37,39,40,
43,46,48,53,54,61,67
The major obstacle after a limb-sparingproximal humerus resection is the restorationof shoulder girdle stability. During the earliestexperience with shoulder girdle resections,surgeons made no attempt at reconstruc-tion.13,17,25,50 Extremities were left flail, whichresulted in instability, traction neurapraxia,and the need to wear an orthosis. Subsequently,attempts were made to stabilize the remaininghumeral shaft to the clavicle or a rib, either viadirect attachment, using heavy nonabsorbablesutures or wires, or indirectly, by cementing aKuntscher rod or custom-made spacer into theremaining shaft and stabilizing its proximalend.4,33,50,67 Many surgeons were dissatisfiedwith these techniques because of the high inci-dence of failure of fixation, hardware failure,skin breakdown secondary to chronic rod irri-tation, and pain. Some surgeons advocated fu-sions using allografts from cadavers or freevascularized autogenous bone grafts to restorestability.10,19,37,54 These constructs requiredlong periods of immobilization and frequentlyfailed secondary to fracture, nonunion, and in-fection. Donor site morbidity also was a prob-lem. If a successful fusion was achieved, thepatient lost rotation below the shoulder level,where most activities of daily living are done.
In 1985, Malawer39 and Malawer et al48 re-ported results of nine patients with high-gradesarcomas of the proximal humerus (four os-teosarcomas) who were treated with en bloc,extraarticular resection (modified Tikhoff-Linberg resection; Malawer Type VB shouldergirdle resection).46 The goals were to do an on-cologically safe and reliable resection and toprovide a method of reconstruction that stabi-lized the shoulder, without compromising rota-tion and that preserved elbow and hand func-tion. Reconstruction was accomplished with anendoprosthetic proximal humerus that was sta-bilized to the remaining scapula and claviclewith nonabsorbable 3-mm Dacron tapes (staticsuspension) and various muscle transfers (dy-
Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 157
Fig 1. A plain radiograph shows a proximalhumerus osteosarcoma. The metaphyseal epi-center and extraosseous soft tissue componentthat is a common characteristic of most osteosar-comas arising in this location can be seen.

namic suspension). There were no local recur-rences. All shoulders were stable, and a func-tional elbow and hand were preserved in all pa-tients. Complications were minimal, and nopatients experienced pain or required an orthosis.
Since 1980, the senior author (MMM) hasdone limb-sparing surgery with endoprostheticreconstruction for 23 patients with osteosar-coma of the proximal humerus. The current au-thors report the indications, surgical technique,oncologic and functional results, and complica-tions associated with limb-sparing resectionand endoprosthetic reconstruction for osteosar-coma of the proximal humerus. Emphasis isgiven to en bloc, extraarticular resection in-cluding the deltoid and lateral portion of the ro-tator cuff (Type VB resection; Malawer’s clas-sification) for tumors with an extraosseouscomponent and endoprosthetic reconstructionusing static (Dacron tapes) and dynamic (mus-cle transfers) suspension to achieve stability.46
The authors summarize the results of that 20-year surgical experience. The strengths of thisstudy are that (1) it focuses on a relatively largenumber of patients, all with high-grade in-tramedullary osteosarcomas; (2) all surgerieswere done by one surgeon; (3) the same surgi-cal method for resection and reconstruction wasused for each patient; and (4) followup is rela-tively long, with a median of 10 years. Thisstudy is the largest series reported to date thatfocuses on limb-sparing surgery for osteosar-coma of the proximal humerus.
MATERIALS AND METHODS
A retrospective analysis was conducted on all pa-tients treated for osteosarcoma of the proximalhumerus, by the senior author, between 1980 and1998. Twenty-six patients were identified. Threepatients were treated with forequarter amputation.Twenty-three of the 26 patients were treated withlimb-sparing resection and endoprosthetic recon-struction. These 23 patients are the focus of thisanalysis.
Patient DemographicsTwenty-three patients, 10 to 77 years of age (me-dian, 18 years), had limb-sparing resection and en-
doprosthetic reconstruction for high-grade osteo-sarcoma of the proximal humerus (Table 1). Therewere 12 males and 11 females. The overall fol-lowup ranged from 6 months to 234 months (median,76 months). All survivors were followed up for atleast 2 years or until death (range, 24 months–234months; median 120 months). Biopsy was donethrough the anterior 1⁄3 of the deltoid in all patientsand confirmed the diagnosis of a high-gradeosteosarcoma.
One patient (4%) presented with a Stage IIA le-sion, 18 presented with Stage IIB lesions (78%),and four presented with Stage III lesions (17%).The primary tumors in all patients with Stage III le-sions extended extraosseously (extracompartmen-tal). All patients with Stage III lesions presentedwith pulmonary metastases only. Nine of 18 pa-tients with Stage IIB tumors had pulmonary metas-tases develop during their course of treatment.Three of these patients also had bony metastasesdevelop. All patients, except one (Patient 23), whopresented with or had pulmonary metastases de-velop had thoracotomy, pulmonary metastasec-tomy, and additional chemotherapy. The size of theprimary lesion was retrievable from the medicalrecords for 13 patients. The length varied from 5 to21 cm (median, 13 cm) and the width ranged from2 to 12 cm (median, 6 cm). Seven patients pre-sented with pathologic fractures (Patients 3, 4, 6, 7,9, 13, and 20). All extremities were immobilizedand treated with induction chemotherapy. All frac-tures healed and the patients were considered can-didates for limb salvage surgery.
Eighteen patients received induction chemother-apy before surgical resection. The induction che-motherapy regimen was based on cisplatin anddoxorubicin for the majority of patients. Five pa-tients (Patients 2, 10, 12, 17, and 23) did not haveinduction chemotherapy because they were partici-pants of an early protocol that randomized patientsto induction chemotherapy, surgery plus adjuvantchemotherapy, or immediate surgery followed byadjuvant chemotherapy. All patients received post-operative adjuvant chemotherapy per standard pro-tocols at the time of administration. Additional de-tails about dosages and deviations from protocolwere not available.
All patients with Stage IIB and Stage III tumors(n � 22) were treated with an extraarticular resec-tion encompassing the deltoid and lateral portionsof the rotator cuff (Type VB; Malawer classifica-tion46). The tumor was removed en bloc with the
Clinical Orthopaedics158 Wittig et al and Related Research

TA
BL
E 1
.D
emo
gra
ph
ics
and
Clin
ical
Dat
a o
n 2
3 P
atie
nts
Wit
h H
igh
-Gra
de
Ost
eosa
rco
ma
of
the
Pro
xim
al H
um
eru
s
Gen
der
T
um
or
Pat
ien
t A
ge
Siz
e P
ath
olo
gic
Ind
uct
ion
N
ecro
sis
Fo
llow
up
P
atie
nt
Nu
mb
er(y
ears
) S
tag
e(c
m)
Fra
ctu
reC
hem
oth
erap
y(p
erce
nt)
(mo
nth
s)M
etat
ases
Sta
tus
EC
om
plic
atio
n
1M
,15
IIA21
�2
�C
DD
P a
nd D
OX
95–1
0010
1—
AN
ED
MA
IN2
F,22
IIB—
�—
—21
6—
AN
ED
M—
3M
,77
IIB19
�7
�C
DD
P a
nd D
OX
80–8
521
—D
(C
VA
)M
RN
4F,
14IIB
—�
CD
DP
and
DO
X90
76—
AN
ED
M—
5M
,16
IIB20
�9
�C
DD
P a
nd D
OX
100
120
—A
NE
DM
—6
F,10
III—
�C
DD
P a
nd D
OX
100
122
PA
NE
DM
—7
M,1
8III
15�
6�
CD
DP
and
DO
X25
–50
48P
DC
Ski
n ne
cros
is8
M,1
2III
—�
HD
MTX
and
BC
D25
–50
24P
and
B (
18 m
onth
s)D
C—
9F,
19IIB
20�
12�
CD
DP
and
DO
X99
30—
AN
ED
CR
N a
nd U
N10
M,1
8IIB
—�
——
210
—A
NE
DC
—11
M,2
9IIB
—�
CD
DP
and
DO
X99
71P
(22
mon
ths)
AN
ED
M—
12F,
15IIB
12�
5�
——
234
—A
NE
DC
—13
M,2
0IIB
12�
5�
CD
DP
and
DO
X10
010
3—
AN
ED
MR
N a
nd U
N S
kin
necr
osis
14M
,17
IIB12
�6
—V
and
HD
MTX
25–5
012
P (
3 m
onth
s) a
nd B
(9
mon
ths)
DC
RN
/UN
15F,
24IIB
17�
4�
CD
DP
and
DO
X95
30P
and
B (
14 m
onth
s)D
M—
16F,
17III
—�
HD
MTX
and
BC
D?
203
PA
NE
DC
Frac
ture
(15
yea
rs)
and
AL
17M
,20
IIB—
�—
—19
0P
(24
mon
ths)
AN
ED
C—
18F,
30IIB
—�
CD
DP
and
DO
X?
18P
and
B (
8 m
onth
s)D
CR
N19
M,3
4IIB
8�6
�C
DD
P, D
OX
and
IFO
S50
19P
(8
mon
ths)
D (
CM
L)M
RN
and
UN
20F,
16IIB
6�4
�C
DD
P a
nd D
OX
1024
—A
NE
DM
—21
F,14
IIB17
�10
�C
DD
P a
nd D
OX
9013
9P
(10
mon
ths)
AN
ED
MA
IN22
F,16
IIB5�
3�
CD
DP
and
DO
X50
108
P (
8 m
onth
s)A
NE
DM
—23
M,2
0IIB
—�
——
6P
(3
mon
ths)
DC
—
P �
pulm
onar
y m
etas
tase
s, B
�bo
ny m
etas
tase
s, E
�en
dopr
osth
etic
type
, M �
mod
ular
pro
sthe
sis,
C �
cust
om p
rost
hesi
s, M
ST
S �
Mus
culo
skel
etal
Tum
or S
ocie
ty F
unct
iona
l Sco
re, C
DD
P �
cisp
latin
,D
OX
�do
xoru
bici
n, V
�vi
ncris
tine,
HD
MT
X �
high
-dos
e m
etho
trex
ate,
BC
D �
bleo
myc
in, c
yclo
phos
pham
ide,
act
inom
ycin
D, I
FO
S �
ifosf
amid
e, A
NE
D �
aliv
e w
ithou
t evi
denc
e of
dis
ease
, D �
dece
ased
,R
N �
radi
al n
eura
prax
ia,
UN
�ul
nar
neur
apra
xia,
AL
�as
eptic
loos
enin
g, A
IN �
ante
rior
inte
ross
eous
neu
rapr
axia
, �
�re
ceiv
ed in
duct
ion
chem
othe
rapy
, ?
�un
know
n or
not
ret
rieva
ble
from
cha
rt,
CV
A �
cere
brov
ascu
lar
acci
dent
, CM
L �
chro
nic
mye
loge
nous
leuk
emia

proximal humerus, intact glenohumeral joint, lat-eral 1⁄3 to 1⁄2 of the clavicle, overlying rotator cuff,and deltoid. The joint capsule was not violated andthe scapular osteotomy was made just medial to thecoracoid process. Extraarticular resection was fol-lowed with endoprosthetic reconstruction using amethod of static (3-mm Dacron tapes) and dynamic(muscle transfers) suspension of the prosthesis tothe clavicle and scapula for prosthetic stabilization,as described previously by Malawer39 and Malaweret al.48 The only patient with a Stage IIA tumor wastreated with an intraarticular resection that sparedthe deltoid and rotator cuff (Type IA resection;Malawer classification system46). A 40-mm wideGoretex aortic graft (WL Gore and Associates,Flagstaff, AZ) was used to statically stabilize theproximal humerus endoprosthesis to the glenoid.The rotator cuff muscles and deltoid were suturedto the prosthesis and Goretex graft for dynamic sta-bilization and reconstruction of the abductor mech-anism. Thirteen modular segmental prosthetic re-placements (after 1988) that permitted intraoperativesizing and 10 custom replacements (before 1988)were used for reconstruction. All endoprostheseswere cemented into the remaining distal humeralshaft.
Routine pathologic analysis was done on allspecimens after resection. The response of the pri-mary neoplasm to the induction chemotherapy reg-imen was determined by an experienced patholo-gist according to the system of Rosen et al59 andexpressed as the percentage of tumor necrosis inthe surgical specimen. The estimated percentage ofhistologic tumor necrosis was retrievable from themedical records for 16 of the 18 patients treatedwith induction chemotherapy.
Postoperatively, clinical examination, plain ra-diographs of the operative extremity, and com-puted tomography (CT) scans of the chest weredone approximately every 3 months for 2 years af-ter surgery, every 6 months from the secondthrough fifth years, and on a yearly basis thereafter.After the tenth year, a radiograph of the chest usu-ally was substituted for the CT scan of the chest.Function at latest followup was evaluated accord-ing to the Musculoskeletal Tumor Society func-tional evaluation system.14 This system evaluateseach of the following areas: pain, function, emo-tional acceptance, hand positioning, dexterity, andlifting ability. The greatest cumulative score that apatient could be assigned was 30 points and wasbased on a greatest possible score of 5 points in
each subcategory. Elbow and hand strength wereevaluated by comparing results of manual motortesting of the affected and unaffected extremities.Shoulder range of motion (ROM) was estimated byvisual inspection. All patients were questionedabout their ability to do activities of daily living andabout their participation in athletic or recreationalactivities.
Surgical TechniqueExtraarticular resection requires a combined ante-rior and posterior approach. An intraarticular re-section, by contrast, can be done solely through ananterior approach. In an extraarticular resection,the neurovascular bundle initially is explored andresectability determined through the anterior ap-proach. The neurovascular bundle is dissectedaway from the pseudocapsule of the tumor duringthis portion of the procedure. The posterior ap-proach is required for exposing the scapula and do-ing the scapular osteotomy.
The approach that is used is referred to as theutilitarian shoulder approach (Fig 2). The incisionconsists of three arms, each of which results in con-struction of a skin flap in which the base is at leastas wide as the flap is long. The incision results in alarge, medially based posterior skin flap that can beused for anterior coverage of the chest wall if aforequarter amputation is necessary at the time ofthe index procedure or postoperatively to treat a lo-cal recurrence or complication. For an extraarticu-lar resection of a proximal humerus osteosarcoma,incision A is used in entirety and a portion of inci-sion B. The incision can be extended into the axilla(incision C) for tumors with a large axillary com-ponent; however, this was not necessary in any ofthe patients in this study.
Anterior ApproachThe patient is positioned in a semilateral positionon a bean bag with the affected arm abducted andextended, and resting on a padded, sterile stand.The surgical incision extends distally from the mid-dle 1⁄3 of the clavicle, passes just medial to the cora-coid along the deltopectoral groove, and followsthe course of the neurovascular bundle, distallyalong the anteromedial aspect of the arm. Thebiopsy site is removed in an elliptical manner incontinuity with the skin incision and left attachedto the surgical specimen. Full-thickness, fasciocu-taneous skin flaps are developed medially and lat-erally. The deltopectoral groove is identified and
Clinical Orthopaedics160 Wittig et al and Related Research

the cephalic vein is ligated, divided, and resectedproximally and distally at the wound margins.
Exposure and Exploration of theNeurovascular BundleThe key step in exposing the neurovascular bundleis releasing the pectoralis major from its humeralinsertion followed by the strap muscles (coraco-brachialis, short head of the biceps, pectoralis mi-nor) from their insertions on the coracoid. The in-ferior border of the pectoralis major is identifiedand the fascia is opened. The pectoralis major in-sertion is released from the humerus using Boviecautery. The pectoralis major is retracted medially.The musculocutaneous nerve is dissected infero-medial to the coracoid in the interval between thepectoralis minor and coracobrachialis and short
head of the biceps insertions, where it enters theselatter muscles. With the musculocutaneous nerveprotected, the coracobrachialis and short head ofthe biceps complex is released from its coracoid in-sertion. This is followed by release of the pectoralisminor. At this point, the entire neurovascular bun-dle can be observed from the clavicle to the humerus(Fig 3). The axillary and radial nerves are dissectedup to their origins from the posterior cord of thebrachial plexus and are protected. The anterior andposterior humeral circumflex vessels are ligatedand divided to retract the neurovascular bundleaway from the tumor pseudocapsule (subscapularismuscle). For tumors with an extraosseous compo-nent, the axillary nerve is ligated. The musculocu-taneous nerve, radial nerve, remainder of the plexus,and vascular structures are retracted and protected
Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 161
Fig 2. This schematic shows the utilitarian shoulder girdle approach. The approach consists of threepotential incisions (A, B, C) all of which result in a skin flap in which the base is at least the same widthas the length of the flap. Incision A (anterior approach) permits exposure and exploration of the neu-rovascular bundle and osteotomy through the humerus. Incision B (posterior approach) exposes theposterior scapula and creates a wide medially-based posterior fasciocutaneous skin flap. Incision C(axillary extension) can be used for exposure of tumors with an extremely large axillary component. Allextraarticular resections in the current series were done through a combined anterior (incision A) andposterior (incision B) approach. The only intraarticular resection was done via an anterior approachonly (incision A). (Reprinted with permission from Wittig J, Kellar-Graney K, Malawer M, Bickels J,Meller I: Limb sparing surgery for high grade sarcomas of the proximal humerus. Tech Shoulder ElbowSurg 2:54–69, 2001.)

Clinical Orthopaedics162 Wittig et al and Related Research
Fig 3A–B. (A) This schematic shows exposureof the major neurovascular bundle to the upperextremity after release of the pectoralis major,short head of the biceps, coracobrachialis, andpectoralis minor (m � muscle; n � nerve; a.v. �artery and vein). (Reprinted with permission fromWittig J, Kellar-Graney K, Malawer M, Bickels J,Meller I: Limb sparing surgery for high grade sar-comas of the proximal humerus. Tech ShoulderElbow Surg 2:54–69, 2001.) (B) An intraopera-tive photograph shows exposure of the neu-rovascular bundle. B � short head of biceps; S �subscapularis (overlying tumor of the proximalhumerus); D � deltoid L � latissimus. The largestraight arrow points to the neurovascular bundlein axillary sheath; the large curved arrow pointsto the musculocutaneous nerve; and the smallwide arrow points to the axillary nerve and pos-terior humeral circumflex vessels.
A
B

for the remainder of the procedure. In all cases inthis study, it was possible to preserve the musculo-cutaneous, radial, ulnar, and median nerves and thevascular structures.
Extraarticular ResectionThe skin incision is extended posterolaterally overthe top of the shoulder to the scapular tip. A wide,medially based fasciocutaneous skin flap is raised.A distally based, lateral, fasciocutaneous skin flapalso is raised to expose to entire deltoid. The trapez-ius is released from its insertion on the clavicle,acromion, and scapular spine to the area just medialto the coracoid process where the scapular os-teotomy is done (Fig 4). The rotator cuff is incisedjust medial to the coracoid and an osteotomy ismade through this area with a high-speed burr orsagittal saw. A second osteotomy is made throughthe clavicle, usually at the junction of its middle 1⁄3and outer 1⁄3. The latissimus dorsi and teres majorare released from the humerus. The humeral os-teotomy is made 2 cm to 3 cm distal to the tumorextent to ensure a wide margin. Any brachialismuscle overlying tumor is resected en bloc. Thetendon of the long head of the biceps is resectedwhere it is juxtaposed to tumor. All margins, in-
cluding the distal intramedullary margin and axil-lary sheath, are sent for frozen section analysis. Theproximal humerus, intact glenohumeral joint, del-toid, and lateral portions of the rotator cuff andclavicle are removed en bloc.
Intraarticular ResectionThe anterior approach is done as described previ-ously; however, the axillary nerve is protected andpreserved. There is no need to extend the skin inci-sion posteriorly. The deltoid, long head of the bi-ceps, latissimus-teres major complex, rotator cuff,and glenohumeral joint capsule are released se-quentially from their insertions. The osteotomy ismade through the proximal humerus as describedfor an extraarticular resection. The trapezius inser-tion is not violated.
Extraarticular ReconstructionAn endoprosthetic proximal humerus is used. Theauthors currently recommend a modular system.The length should allow shortening of the arm by 2cm to 3 cm to prevent traction on the neurovascu-lar structures and to facilitate wound closure. Thecanal of the remaining distal humerus is reamed forplacement of the thickest possible stem, accommo-
Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 163
Fig 4. This schematic shows the posterior approach to the scapula for an extraarticular resection.(Reprinted with permission from Wittig J, Kellar-Graney K, Malawer M, Bickels J, Meller I: Limb spar-ing surgery for high grade sarcomas of the proximal humerus. Tech Shoulder Elbow Surg 2:54–69,2001.)
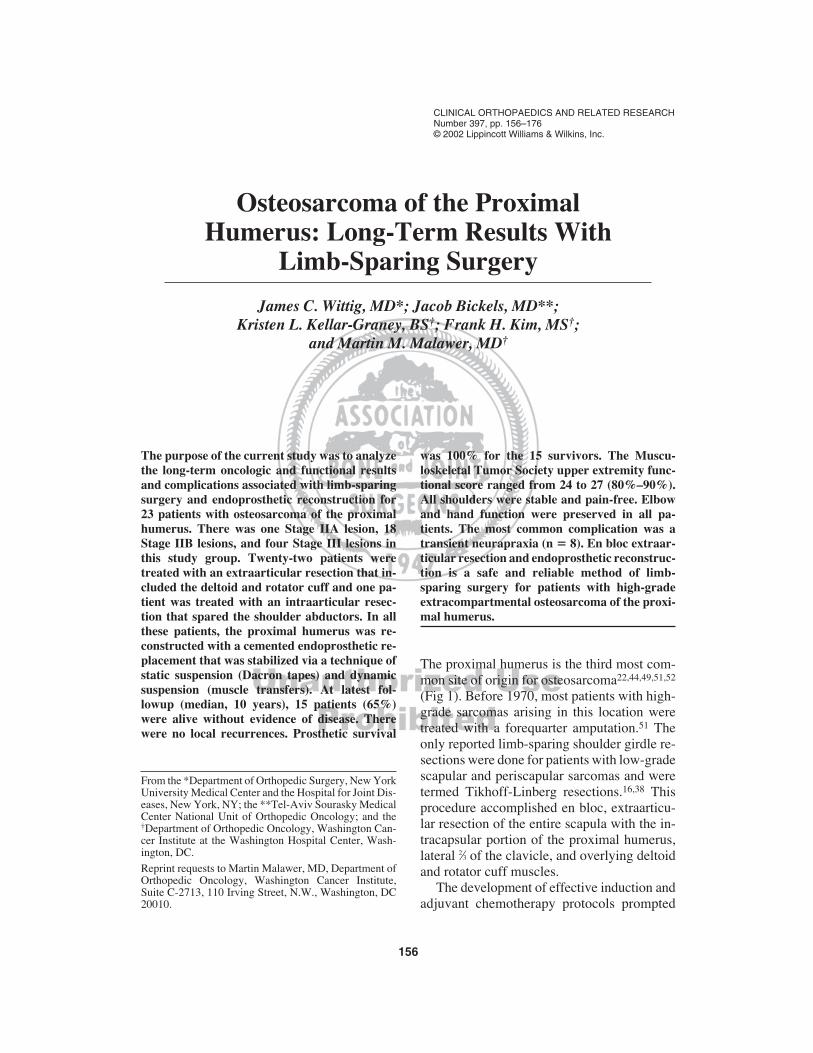
dating for a 2-mm cement mantle. The prosthesisis cemented in retroversion so the head of thehumerus faces the subscapular fossa. Static sus-pension is provided by Dacron tapes (3-mm) thatare passed separately through the scapula and clav-icle, and through holes in the neck of the proximalhumerus prosthesis (Fig 5). The proximal humerusis suspended vertically from the clavicle (verticalstatic suspension) and horizontally from the scapula(horizontal static suspension). The pectoralis minoris attached to the remaining subscapularis muscleso that it protects the neurovascular structures fromthe prosthesis. Dynamic prosthetic suspension,consisting of multiple muscle transfers, subse-quently is done. The short head of the biceps istransferred to the clavicle and tenodesed with a 3-
mm Dacron tape (dynamic vertical suspension).The trapezius is transferred distally over the head ofthe humerus and tenodesed to the prosthesis (dy-namic vertical suspension). The pectoralis major istransferred laterally so that it covers the entire prox-imal humerus. It is sutured to the holes in the neckof the prosthesis, any remaining infraspinatus mus-cles, the lateral border of the scapula, and the bor-der of the trapezius (dynamic horizontal suspen-sion). To restore external rotation and cover thedistal lateral aspect of the prosthesis, the latissimus-teres major complex is rerouted around the postero-lateral aspect of the prosthesis and attached in an an-terolateral position to the prosthesis and to adjacentmuscles. The long head of the biceps is reattachedto the pectoralis major with the forearm supinatedand the elbow in 45� flexion. The tension of the bi-ceps is set at 1⁄2 the distance of full stretch. All adja-cent muscle borders are sutured to each other usingnumber 0 braided nonabsorbable suture. At the con-clusion of all the muscle transfers, the entire pros-thesis is covered with muscle (Figs 6, 7).
Intraarticular ReconstructionA modular proximal humerus prosthesis is recom-mended. The canal is reamed and the prosthesis isimplanted while maintaining proper retroversion ofthe humeral head (30�–45� retroversion). Static cap-sular reconstruction is accomplished with a 40-mmdiameter Goretex aortic graft. The aortic graft is su-tured with Dacron tapes to the glenoid labrum andcapsular base, and its free end is pulled over thehead of the prosthesis where it is sutured to the holesin its neck. The aortic graft provides static stabilityuntil healing and scarring occur. It also facilitatesmuscle reattachment. The rotator cuff and deltoidare reattached to the prosthesis and Goretex aorticgraft. The short head of the biceps is reattachedproximally to the coracoid, and the long head of thebiceps is tenodesed to the pectoralis major.
Epineural AnalgesiaBefore doing muscle transfers, a 20-gauge silasticepidural catheter is threaded proximally within theplexus sheath and sutured to surrounding fasciawith 4-O absorbable suture.41 The free end isbrought through the skin using a 14-gauge angio-catheter. Bupivacaine (0.25% without epinephrine)is infused through the catheter postoperatively foranalgesia (a bolus of 10 cc, followed by 4 cc/hourcontinuous infusion). The dosage can be titrated formaximal pain relief.
Clinical Orthopaedics164 Wittig et al and Related Research
Fig 5. Static suspension of the prosthesis is ac-complished with 3 mm Dacron tapes. The pros-thesis is retroverted so that its articular surfacefaces the subscapular fossa. It then is suspendedvertically from the clavicle and horizontally fromthe lateral border of the scapula. AdditionalDacron tapes are passed through the lateral bor-der of the scapula for tenodesis of the pectoralismajor.

Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 165
ClosureClosed suction drains are placed. The wound isclosed in layers. A bulky soft dressing and elbowsplint are applied to reduce postoperative edemaand maintain the elbow in 45� flexion, respectively.
RESULTS
Local ControlThere were no local recurrences in any of the23 patients.
Overall SurvivalFifteen patients (65%) were alive without ev-idence of disease at a range of 24 months to
234 months (median, 120 months). This in-cluded two patients with Stage III lesions, 12with Stage IIB lesions, and one with a StageIIA lesion. Eight patients (35%) died at arange of 6 months to 48 months (median, 20months). Six of these patients died of tumor-related causes and two died of unrelatedcauses.
Prosthetic SurvivalProsthetic survival for the 15 survivors hasbeen 100% at a median followup of 120 months(range, 24 months – 234 months). No prosthe-sis required a revision in any of the survivors orpatients who died. There was one instance ofaseptic loosening that was detected radiograph-
Fig 6. Dynamic suspension of the prosthesis isaccomplished with multiple muscle transfers. Atthe conclusion, the entire prosthesis is coveredwith muscle. P � pectoralis major; T � trapezius;I � infraspinatus; B � biceps; L � latissimus-teres major complex. The arrow points to theepineural catheter in axillary sheath.
Fig 7. A radiograph taken after extraarticular re-section shows endoprosthetic reconstruction.

ically. It developed after a periprosthetic frac-ture and was asymptomatic (Patient 16).
ComplicationsComplications included eight transient nervepalsies (two anterior intraosseous nerve palsies;two radial nerve palsies; four combined radialand ulnar nerve palsies). All nerve palsies re-solved within 6 to 12 months after surgery.There were two instances of minor skin necro-sis that healed with dressing changes. Oneperiprosthetic fracture occurred distal to theprosthesis 15 years after surgery, secondary toa fall. The patient was treated with a brace un-til a stable union occurred. The patient waspain-free and function was unaltered after thefracture healed, although the patient subse-quently had radiographic signs of aseptic loos-ening. The patient was asymptomatic andtherefore a revision was not done. There wereno instances of prosthetic instability or dis-location, clinically or radiographically. Therewere no infections. No patients had late trac-tion neurapraxias develop from the weight ofthe upper extremity.
Functional OutcomeThe Musculoskeletal Tumor Society upper ex-tremity functional scores ranged from 24 to 27(80% to 90%). All shoulders were stable. Allpatients could do activities of daily living withthe involved extremity. Functional resultswere consistent and uniform among all pa-tients. All survivors received a score of 5 (bestpossible rating) in the areas of pain, hand dex-terity, and emotional acceptance. No patientcomplained of pain. All patients had normalfunctional use of the hand (normal sensation;Grade 5 motor strength) and all were emo-tionally accepting of the procedure and out-come. Patients lost points in the following ar-eas: function, hand positioning, and liftingability. Because the score for each of these ar-eas was subjective, a range was assigned as thescore. In terms of function, patients were as-signed a score of 3 to 4 points. All patients hadsome restrictions in activities but were capableof participating in some recreational activities.
Most restrictions were in high-level athletics,although one patient (Patient 1) wrestled forhis high school and college teams. Other pa-tients played tennis, lifted weights (withinlimits), rode bicycles, rowed boats, and swamregularly. All patients were assigned a score of3 to 4 for hand positioning. Hand positioningwas not unlimited, but all patients could placetheir hands above their shoulders, touch theback of their head and opposite shoulder, andfeed themselves. Active shoulder ROM variedslightly from patient to patient but was withinthe following ranges: forward flexion, 25� to45�; abduction, 25� to 45� (secondary to trapez-ius transfer and scapulothoracic motion); in-ternal rotation, 90�; external rotation, �15� toneutral. Passive shoulder motion was withinnormal limits for all patients. Lifting abilitywas graded 3 to 4 for each patient. All patientshad normal functional use of the elbow and el-bow motor strength was at least Grade 4 in allpatients. Patients did not have difficulty carry-ing objects with the arm adjacent to the body;however, they had difficulty carrying objectswith the arm away from the body because of alack of deltoid and rotator cuff function. Nopatients could lift objects significantly aboveshoulder level.
DISCUSSION
It is difficult to derive from the literature anexact approach to treating osteosarcomas aris-ing from the proximal humerus. Controversyexists concerning the indications for extraar-ticular versus intraarticular resection and re-garding the best method of reconstruction aftereach type of resection. Much of this difficultyhas arisen from the low incidence of osteosar-coma arising in this location. Although theproximal humerus is the third most commonsite of origin for osteosarcoma, only approxi-mately 15% of all osteosarcomas arise fromthis location.44 In the United States, this trans-lates into approximately 50 to 70 cases peryear. Given this incidence, it has been difficultfor individual surgeons to develop a large se-ries of patients; consequently, most surgeons
Clinical Orthopaedics166 Wittig et al and Related Research

report oncologic and functional results associ-ated with limb-sparing shoulder girdle resec-tions that are based on mixed groups of pa-tients. Reports have included patients withvarious types and grades of sarcomas (osteo-sarcoma, chondrosarcoma, Ewing’s sarcoma)and have combined results from patients withproximal humerus and scapular tumors. Pa-tients with metastatic carcinomas occasionallyhave been included in some series. Frequently,the type of resection (extraarticular versus in-traarticular) has not been specified for each tu-mor type, which causes difficulty in evaluatingthe oncologic results associated with the typeof resection, as assessed by local recurrencerates.12 Some reports have focused on resultsof reconstruction after limb-sparing surgeryand have included patients reconstructed viamultiple methods. Various systems, particu-larly the Musculoskeletal Tumor Society sys-tem14 and the system of Gebhardt et al19 havebeen used for functional evaluation by differ-ent authors. Therefore there has been difficultywith deriving statistically significant conclu-sions about functional results and complica-tions, and in comparing results among differ-ent institutions.
The current study reports excellent local tu-mor control, consistently good to excellentfunction, and excellent long-term prostheticsurvival for 23 patients with osteosarcoma ofthe proximal humerus who had limb-sparingresection (22 extraarticular, one intraarticular)and endoprosthetic reconstruction. The firstpriority of limb-sparing resection for a high-grade sarcoma is to achieve an oncologicallysafe resection. It has been proposed that theadequacy of a resection method can be evalu-ated by its associated local recurrence rate.12
Local tumor control in this region is essential,because patients with local recurrence fre-quently are treated with a forequarter amputa-tion and local recurrence of a high-grade lesionmay compromise survival.1,62 In the currentauthors’ opinion, the resection should not becompromised to improve functional results.The senior author has preferred extraarticularresection that includes the deltoid and overly-
ing rotator cuff musculature for high-grade os-teosarcomas arising from the proximal humerusthat extend extraosseously. Such was the casefor 22 of 23 patients in the current series. Thegoal has been to reliably achieve a wide surgi-cal margin and maximize local tumor controlwithout the need for a forequarter amputationor total scapulectomy combined with a proxi-mal humerus resection. The reliability of thismethod of resection is supported by the 0%local recurrence rate presented in the currentstudy. After resection, the goals of reconstruc-tion were to stabilize the proximal upper ex-tremity without compromising rotation belowthe shoulder level and to preserve a normallyfunctioning hand and elbow. All patients in thisstudy had reconstruction with an endoprostheticproximal humerus replacement that was stabi-lized with static and dynamic methods of softtissue reconstruction. Functional evaluationaccording to the Musculoskeletal Tumor Soci-ety System showed consistently good and uni-form results among all patients. These scoresranged from 24 to 27 (80% to 90% of the max-imum possible score). A score of at least 24 hasbeen considered by at least one author as an ex-cellent result.32
Local Sarcoma Growth, CompartmentalBorders, and Indications for anExtraarticular ResectionSeveral biologic reasons support performanceof an extraarticular resection that includes theabductor mechanism for high-grade sarcomasof the proximal humerus that extend beyond thecortices. Traditional teaching has emphasized apropensity for tumors in this location to conta-minate the glenohumeral joint or to spread tothe opposing glenoid and scapula, grossly andmicroscopically.13,39,40,46,48,61 The mechanismsof spread across the glenohumeral joint arebased on its unique anatomy. These mecha-nisms include: capsular extension, pathologicfracture hematoma, direct articular extension,spread along the long head of the biceps tendon,or through transarticular metastasis.
In discussion of local sarcoma growth, acompartmental border usually refers to any
Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 167

fascial boundary that resists tumor penetrationas described by Enneking.12 Sarcomas growalong the path of least resistance; therefore,any adjacent fascial border offers a boundaryto local growth. The current authors proposethat the important fascial boundaries surround-ing the proximal humerus consist of the invest-ing fascial layers of the deltoid, subscapularis,and remaining rotator cuff muscles and thatthese muscles form a compartment surroundingthe proximal humerus that contains and delin-eates the local spread of a high-grade bone sar-coma. An osteosarcoma that arises from theproximal humerus and extends extraosseouslywill grow to fill the compartment and will com-press the muscles that form the borders of thecompartment into a pseudocapsular layer (Fig8). By definition, a wide surgical margin in-cludes the pseudocapsular layer around the tu-mor, because this layer contains microscopictumor extension (satellite nodules). Therefore,for sarcomas of the proximal humerus, widesurgical resection entails en bloc resection ofthe deltoid and overlying rotator cuff. The axil-lary nerve and posterior humeral circumflexvessels pass along the inferior capsule and sub-scapularis muscle. They reside within the infe-
rior aspect of the pseudocapsule of any large tu-mor and, by strict definition, require resection.Because the glenoid is surrounded by the mus-cles forming the compartment, it resides withinthe same compartment as does the proximalhumerus. The intracompartmental locationplaces the glenoid at high risk of contamination,which lends support to concomitant glenoid re-section with the proximal humerus. In addition,retention of the glenoid confers no functionalbenefit after resection of the axillary nerve andabductor mechanism. Its resection permits me-dialization of the prosthetic construct, which fa-cilitates soft tissue coverage (Fig 9).
In a review of the literature (Table 2), theauthors were able to identify 106 patients withhigh-grade spindle cell sarcomas (Stage IIB orStage III) arising from the proximal humerusor scapula who were treated with an extraar-ticular resection encompassing the deltoid androtator cuff.1,7,17,19,33,37,48,50,53 Seven of thesepatients (7%) had a local recurrence develop.The authors also identified 51 patients withsimilar lesions who had intraarticular resec-tion, sparing the shoulder abductors.1,20,21,32
Nine patients (18%) in this group had a localrecurrence develop. The difference was statis-
Clinical Orthopaedics168 Wittig et al and Related Research
Fig 8 A–E. Local growth of an osteosarcoma from the proximal humerus is shown. (A) This schematicshows metaphyseal origin and extension beyond the cortices of the proximal humerus. The ex-traosseous component is crossing the glenohumeral joint. The deltoid, subscapularis, and remainingrotator cuff muscles form the compartmental boundaries around the tumor and are compressed into apseudocapsular layer. The axillary nerve and circumflex vessels enter this compartment. The majorneurovascular bundle is displaced by the tumor; however, the fascia overlying the subscapularis mus-cle and the axillary sheath usually protect the major neurovascular bundle from tumor involvement orencasement, in most instances. (Reprinted with permission from Wittig J, Kellar-Graney K, Malawer M,Bickels J, Meller I: Limb sparing surgery for high grade sarcomas of the proximal humerus. Tech Shoul-der Elbow Surg 2:54–69, 2001.) (B) A cross section through the glenohumeral joint shows extensionof the tumor across the glenohumeral joint and compression of the surrounding compartmental mus-cles into a pseudocapsular layer. The neurovascular bundle is protected by the subscapularis muscle.(Reprinted with permission from Wittig J, Kellar-Graney K, Malawer M, Bickels J, Meller I: Limb spar-ing surgery for high grade sarcomas of the proximal humerus. Tech Shoulder Elbow Surg 2:54–69,2001.) (C) A coronal MRI scan shows the metaphyseal origin and tumor crossing the glenohumeraljoint (straight arrow) and extending into the overlying deltoid muscle (curved arrow). (D) An axial MRIscan shows the extraosseous tumor extending beneath the subscapularis muscle (straight arrow) andcrossing the glenohumeral joint (curved arrow). The deltoid (D) is involved by the extraosseous com-ponent (G � glenohumeral joint). (E) The surgical specimen of a high-grade osteosarcoma of the prox-imal humerus is shown. The pathologic fracture and extraosseous extension across the glenohumeraljoint can be seen. A tumor nodule is evident in the deltoid muscle which forms part of the pseudocap-sular layer. The curved arrow points to the tumor nodule in deltoid muscle.

Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 169
A B
C
D
E

tically significant (p � .05 level). Several ofthese cited studies reported combined onco-logic results for proximal humerus and scapu-lar tumors; therefore, it was difficult, in manyinstances, to separate local control rates ac-cording to bone of origin. The current authorsrecommend extraarticular resection for high-grade spindle cell sarcomas (Stage IIB orStage IIIB) arising from either the proximalhumerus or scapula because of the propensityof these tumors to cross the joint in either di-rection. Definitive conclusions, however, shouldnot be derived from this review because it doesnot consider differences in length of followup,tumor size, specific histologic type of spindlecell sarcoma, patient survival, incidence ofpathologic fracture, and adjuvant treatment.However, the trend toward better local controlrates with extraarticular resection encompass-ing the shoulder abductors should prompt ad-ditional investigation.
SurvivalIn the current study, the survival rate of patientswith osteosarcoma of the proximal humerus didnot seem to differ significantly from survivalrates reported from large studies that includesimilar lesions arising at other anatomicsites, such as the distal femur or proximaltibia.2,3,56,57,62 Sixty-five percent of the patientsin the current study were alive without evidenceof disease at a median followup of 10 years(range, 2-19.5 years). There seemed to be atrend toward improved survival in patients whoachieved greater than 90% tumor necrosis withinduction chemotherapy, although the numberswere too small to do statistical analysis. Previ-ous reports have documented the prognosticvalue of the estimated percentage of histologictumor necrosis in the surgical specimen afterinduction chemotherapy.2,9,24,56,57
Functional ResultsFunctional results, as evaluated by the Muscu-loskeletal Tumor Society functional evalua-tion system, for all patients in this series weregood to excellent (range, 80%-90%) and re-sults were consistent among patients. Meller
et al53 reported on six patients treated with ex-traarticular resection who had reconstructionwith a modular prosthesis according to the samemethod as described originally by Malawer etal.48 The median Musculoskeletal Tumor So-ciety score was 75%. These results are similarto results reported by Asavamongkolkul et al1concerning intraarticular resection and endo-prosthetic reconstruction. They reported anaverage Musculoskeletal Tumor Society func-tional score of 76% for 17 of their patientswho had intraarticular resection and recon-struction with endoprosthetic replacement.1Preservation of the glenoid and abductor mech-anism does not seem to offer better functionalresults, as assessed by the MusculoskeletalTumor Society system, when compared withthe patients in the current report. All of the pa-tients in the current study had stable shouldersand all were able to do activities of daily liv-ing with the affected extremity, includingfeeding themselves, grooming, and personalhygiene. All patients could place their handabove the shoulder, touch the back of the head,and touch the opposite shoulder (Fig 10).
Some surgeons have advocated arthrodesisafter extraarticular resection to restore shoulderstability and improve abduction. Complicationsand failures have occurred frequently with thismethod of reconstruction and functional resultsdo not seem to be superior to those presented inthe current study. In 1991, Gebhardt et al19 re-ported on 12 patients treated with allograftarthrodeses. Five of 12 patients (42%) wereconsidered to have failed results. In 1994, Ku-mar et al37 reported on six patients who had re-construction via arthrodesis with a free vascu-larized fibula (n � 4) or free vascularizedscapular graft (n � 2). Two of the free vascu-larized fibula grafts became infected. One wasnot salvageable and the other was salvaged witha second free vascularized fibula graft. Threepatients had nonunions develop and requiredrepeat surgery. Two patients experienced ex-treme shortening of 8 to 10 cm. No patient wasable to do activities above shoulder level.
O’Connor et al54 recommended reconstruc-tion via arthrodesis with a combination of an
Clinical Orthopaedics170 Wittig et al and Related Research

Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 171
Fig 9. The concept of a compartmental resection of the proximal humerus is shown. All structures thatpotentially are involved by the tumor (overlying muscles that form the pseudocapsular layer and com-partmental borders, the glenoid, and the axillary nerve and circumflex vessels) are removed en bloc.N � nerve
TABLE 2. Local Recurrence Rates: Extraarticular Resection Versus IntraarticularResection of High-Grade Shoulder Girdle Sarcomas
Extraarticular Resection Intraarticular Resection
Number of Number of Number of Local Local Number of
Authors Patients Recurrences Percent Patients Recurrences Percent
Marcove et al50 1977 16 1 6 — — —Malawer et al48 1985 4 0 0 — — —Kaelin and Emans33 1985 7 0 0 — — —Capanna et al7 1990 20 1 5 — — —Frassica et al17 1987 8 1 13 — — —Gebhardt et al19 1991 13 2 15 — — —Meller et al63 1997 9 1 11 — — —Kumar et al37 1994 6 0 0 — — —Asavamongkolkul et al1 1999 1 1 100 33 5 15O’Connor et al54 1996** — — — — — —Wittig et al (current study) 2000 22 0 0 — — —Gebhardt et al20 1990 — 4 2 50Jensen and Johnston32 1995 — 8 2 25Getty and Peabody21 1999 — 6 0 0
Total 106 7 7% 51 9 18%
**unable to analyze data; surgical procedure not specified for histologic type and grade of tumor and local recurrences not specifiedaccording to type of surgical procedure

intercalary allograft and vascularized free fibulaconstruct for young patients treated with anextraarticular resection. They reported resultsfor five patients. All extremities were immo-bilized in a spica cast for an average of 14weeks. One patient had an infection developpostoperatively that required repeat surgeryand was salvaged with a second free vascular-ized fibula transfer. Two patients experiencedfractures and their extremities were immobi-lized in spica casts for 3 months; the fracturein one patient healed, and the other patient hada pseudarthrosis develop. Donor site morbid-ity was a frequent problem. Function accord-ing to the Musculoskeletal Tumor Society sys-tem averaged 66% for this group. These resultscompare inferiorly with those in the currentstudy. Complications also were more preva-lent and of greater magnitude.
The major goal after extraarticular resec-tion of a proximal humerus osteosarcoma is torestore stability to the proximal upper extrem-ity. The current authors accomplish this with amethod of static and dynamic and prostheticsuspension as opposed to an arthrodesis for thefollowing reasons: adequate stability can berestored; reconstruction is simplified and op-erating time is reduced; rotation is not re-stricted below the shoulder level, where most
activities are done; the procedure does not re-quire prolonged immobilization and is associ-ated with fewer complications, especially inthe early postoperative period when chemo-therapy is administered; functional results areuniform and reliable; and there is consistenthealing, fewer secondary procedures, and nodonor site morbidity. Most activities that re-quire use of the upper extremity (activities ofdaily living) are done below the shoulder leveland therefore motion in this region is more im-portant than overhead motion. Arthrodesis se-verely restricts rotation below shoulder level(internal rotation, external rotation, and forwardflexion). Complication rates and failures alsoseem greater in patients treated with arthrode-ses and have resulted in many secondary pro-cedures. Complications should be viewed se-riously because the major goal is to restore astable shoulder girdle and early functional useof the extremity, and to resume chemotherapyshortly after surgery.
Intraarticular resection has been preferredby some authors for treatment of select StageII and Stage III sarcomas of the proximalhumerus. This has been done in an effort tospare the articular surface and abductor mech-anism and improve function by reconstructingthe proximal humerus with an osteoarticularallograft or allograft combined with a pros-thetic replacement.20,21,32 In addition to poten-tially increasing the risk of local recurrencewhen done for high-grade extracompartmen-tal sarcomas, intraarticular resection with del-toid and rotator cuff preservation confers a du-bious functional benefit. One time proponentsof osteoarticular allograft reconstruction nolonger recommend its routine use because ofhigh complication and failure rates.20,21 Geb-hardt et al20 reported on 20 patients treatedwith osteoarticular allografts after intraarticu-lar resection of the proximal humerus (five hadhigh-grade tumors; 15 had low-grade or be-nign aggressive). Fifteen percent of patientshad an infection develop. Twelve complica-tions occurred in eight patients and 11 addi-tional procedures were needed for treatment.Patients rarely achieved shoulder abduction or
Clinical Orthopaedics172 Wittig et al and Related Research
Fig 10. Function after extraarticular resection andendoprosthetic reconstruction (3 years postopera-tively) is shown. The patient can place her handabove shoulder level with some external rotation.This is important for hair grooming and feeding.

forward flexion greater than 45� and only twopatients were able to abduct their shoulder 90�.Getty and Peabody21 also reported on 16 pa-tients who had intraarticular resection and re-construction with an osteoarticular allograft.The mean Musculoskeletal Tumor Societyfunctional score was 70%. Maximum abduc-tion in patients who were assessed was 40� andfour of nine patients who were assessed had noactive abduction. None of the patients coulddo activities above the shoulder or could abductagainst resistance. They had similar limita-tions in external rotation and forward flexion.Eleven patients (79%) had unstable gleno-humeral joints and five (36%) had revision forfracture or infection. In both of these studies,active shoulder ROM was not dissimilar to theactive shoulder motion presented in the cur-rent study.
Jensen and Johnston32 reported on 14 pa-tients who were treated with composite recon-struction of the proximal humerus (allograft orautoclaved autograft combined with a proximalhumerus Neer II prosthesis) after intraarticularresection. These authors reported a 25% localrecurrence rate. Active shoulder abduction wasbetween 70� and 90� in all the patients. Most pa-tients, however, had low- or high-grade tumorsthat were entirely intraosseous and therefore,the majority of resections were of smaller mag-nitude than those presented in the current study.Function according to the Musculoskeletal Tu-mor Society system was at least 24 (80%) in 12of the 14 patients. Overall function, as evalu-ated by the Musculoskeletal Tumor Societysystem, did not seem to be significantly differ-ent, despite preservation of the shoulder abduc-tors and glenohumeral joint.
Prosthetic SurvivalSurvivability of large segment proximalhumerus endoprostheses has been excellentafter limb-sparing resection, especially whencompared with the use of large segmentalprostheses at other anatomic sites, such as thedistal femur or proximal tibia.5,6,11,15,26,30,35,
36,58,60,63,64 In the patients in the current series,actual prosthetic survival was 100% at a me-
dian followup of 10 years (120 months). Onlyone patient in the current study had radio-graphic signs of aseptic loosening that wassecondary to trauma. Malawer and Chou43
previously reported 95% 5-year survival ratesfor proximal humerus endoprostheses after re-section for various types of tumor. Feruzzi etal15 reported on 33 patients followed up for atleast 10 years who were treated with proximalhumerus endoprosthetic reconstruction. Fiftypercent of these endoprosthetic devices wereplaced secondary to tumor resection. Therewere no instances of loosening or bone re-sorption. Asavamongkokul et al1 reported noinstances of aseptic loosening in 30 patientswho had cemented proximal humerus replace-ments after tumor resection. The low rate offailure secondary to aseptic loosening of largesegment proximal humerus endoprosthesesmay be related to many variables such as thelack of weightbearing forces across the joint;decreased angular and torsional forces sec-ondary to resection of the deltoid and rotatorcuff muscles; the nonconstrained nature of theprosthesis; the absence of a polyethylene ar-ticulation;18,28,65 the presence of porous coat-ing at the bone-prosthesis junction that facili-tates extracortical bone fixation and soft tissueingrowth;31,34,42,65 and the use of modern ce-menting techniques.55
Shoulder instability (prosthetic dislocation orsubluxation) is a potential complication after alimb-sparing procedure for a proximal humerussarcoma. None of the patients in the current se-ries had prosthetic instability develop. The au-thors think that the success is attributable to themethod of static (Dacron tapes) and dynamic(muscular) suspension of the prosthesis. TheDacron tapes probably function until sufficientsoft tissue scarring of the transferred musclesoccurs to stabilize the prosthesis. Other authorswho combine static and dynamic methods of re-straint also have reported a low incidence ofprosthetic instability.1,53
Infection has been a source of failure forendoprostheses and allografts.5,8,19,26,27,36,42
However, no patients in the current study hadan infection develop. The use of local muscu-
Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 173

lar rotational flaps (gastrocnemius flap) hasbeen beneficial in decreasing complications, es-pecially secondary infections, associated withproximal tibial and, occasionally, distal femo-ral reconstruction.11,29,45,47 The same conceptapplies to the shoulder girdle. The pectoralismajor is the key muscle used for covering theentire prosthesis with soft tissue. The pectoralismajor has an excellent blood supply and pro-vides a protective barrier for the prosthesis.Coverage by this muscle is facilitated by ex-traarticular resection, which permits medializa-tion of the entire construct.
The most common complication in the cur-rent patients was transient nerve palsy. Eightpatients had transient nerve palsies develop; inmany cases, it developed postoperatively, dur-ing the initial 24 hours after surgery. The mostlikely contributing factor was intraoperativetraction that was compounded by postopera-tive swelling. All of the neurapraxias occurredin patients who were treated with inductionchemotherapy. Chemotherapeutic agents usedin the treatment of osteosarcoma have knownneurotoxic effects that may have predisposedthis population to the nerve complications.66
The authors recommend extraarticular resec-tion encompassing the deltoid and rotator cuff(modified Tikhoff-Linberg resection; MalawerType VB resection) for all patients with high-grade osteosarcomas arising from the proximalhumerus that present with a significant ex-traosseous soft tissue component. This methodof resection is consistent with the basic biologicrules of sarcoma surgery, in that it accomplishesa compartmental resection of the tumor and re-moves all structures (pseudocapsule) potentiallycontaminated by tumor cells. The authors thinkthat this approach is the safest method forachieving a wide surgical resection and ob-taining local tumor control. This is importantbecause patients with a local recurrence in thisregion often are treated with a forequarter am-putation, which can have an adverse effect onsurvival. The authors recommend intraarticularresection that spares the rotator cuff and deltoidfor high-grade osteosarcomas that are entirelyintraosseous (Stage IIA). Reconstruction with
an endoprosthesis and static and dynamicmethods of soft tissue reconstruction should bestrongly considered. This method of reconstruc-tion consistently has achieved good functionalresults, is durable, and is associated with a lowrate of complications. Most patients have re-sumed chemotherapy promptly and have hadfunctional use of the extremity within 6 weeks.Shoulder stability has been restored withoutcompromising rotation below the shoulderlevel, where most activities are done. Patientshave been pain-free and have had normal func-tional use of the elbow and hand. Low-level ath-letic activities also are possible.
References1. Asavamongkolkul A, Eckardt JJ, Eilber FR, et al:
Endoprosthetic reconstruction for malignant upperextremity tumors. Clin Orthop 360:207–220, 1999.
2. Bacci G, Picci P, Ferrari S, et al: Primary chemo-therapy and delayed surgery for nonmetastatic os-teosarcoma of the extremities: Results in 164 pa-tients preoperatively treated with high doses ofmethotrexate followed by cisplatin and doxorubicin.Cancer 72:3227–3238, 1993.
3. Bacci G, Springfield D, Capanna R, et al: Neoadju-vant chemotherapy for osteosarcoma of the extrem-ity. Clin Orthop 224:268–276, 1987.
4. Badhwar R: Reconstruction following limb-sparingen bloc resection of the shoulder girdle-Tikhoff-Lin-berg procedure. Ind J Cancer 27:31–37, 1990.
5. Brien EW, Terek R, Healey JH, Lane JM: Allograftreconstruction after proximal tibial resection forbone tumors: An analysis of function and outcomecomparing allograft and prosthetic reconstructions.Clin Orthop 303:116–127, 1994.
6. Capanna R, Morris HG, Campanacci D, Del Ben M,Campanacci M: Modular uncemented prosthetic re-construction after resection of tumors of the distal fe-mur. J Bone Joint Surg 76B:178–186, 1994.
7. Capanna R, Van Horn JR, Biagini R, et al: TheTikhoff-Linberg procedure for bone tumors of theproximal humerus: The classical “extensive” tech-nique versus a modified “transglenoid” resection.Arch Orthop Trauma Surg 109:63–67, 1990.
8. Clohisy DR, Mankin HJ: Osteoarticular allograftsfor reconstruction after resection of a musculoskele-tal tumor in the proximal end of the tibia. J BoneJoint Surg 76A:549–554, 1994.
9. Davis AM, Bell RS, Goodwin P: Prognostic factorsin osteosarcoma: A critical review. J Clin Oncol12:423–431, 1994.
10. Damron TA, Rock MG, O’Connor MI, et al: Func-tional laboratory assessment after oncologic shoul-der joint resections. Clin Orthop 348:124–134, 1998.
11. Eckardt JJ, Matthews JG, Eilber FR: Endoprostheticreconstruction after bone tumor resections of the prox-imal tibia. Orthop Clin North Am 22:149–160, 1991.
12. Enneking WF: Natural History. In Enneking WF
Clinical Orthopaedics174 Wittig et al and Related Research

(ed). Musculoskeletal Tumor Surgery. Vol 1. NewYork, Churchill Livingstone 3–68, 1983.
13. Enneking WF: Shoulder Girdle. In Enneking WF(ed). Musculoskeletal Tumor Surgery. Vol 1. NewYork, Churchill Livingstone 378–410, 1983.
14. Enneking WF, Dunham W, Gebhardt MC, MalawerMM, Pritchard DJ: A system for the functional eval-uation of reconstructive procedures after surgicaltreatment of tumors of the musculoskeletal system.Clin Orthop 286:241–246, 1993.
15. Feruzzi A, Ruggieri P, Capanna R, Campanacci M:Prosthetic Replacement of the Proximal Humerus:Update of Cases Presented in 1981. In Brown KLB(ed). Complications of Limb Salvage. Prevention,Management and Outcome, Montreal, InternationalSociety of Limb Salvage 473–477, 1991.
16. Francis KC, Worcester JN: Radical resection for tu-mors of the shoulder with preservation of a func-tional extremity. J Bone Joint Surg 44A:1423–1430,1962.
17. Frassica FJ, Sim FH, Chao EYS: Primary malignantbone tumors of the shoulder girdle: Surgical tech-nique of resection and reconstruction. Am Surg53:264–269, 1987.
18. Friedman RJ: Advances in biomaterials and factors af-fecting implant fixation. Instr Course Lect 41:127–136,1992.
19. Gebhardt MC, Flugstad DI, Springfield DS, MankinHJ: The use of bone allografts for limb salvage inhigh grade extremity osteosarcoma. Clin Orthop270:181–196, 1991.
20. Gebhardt MC, Roth YF, Mankin HJ: Osteoarticularallografts for reconstruction in the proximal part ofthe humerus after excision of a musculoskeletal tu-mor. J Bone Joint Surg 72A:334–345, 1990.
21. Getty PJ, Peabody TD: Complications and func-tional outcomes of reconstruction with an osteoartic-ular allograft after intra-articular resection of theproximal aspect of the humerus. J Bone Joint Surg81A:1138–1146, 1999.
22. Glasser DB, Lane JM, Huvos AG, Marcove RC,Rosen G: Survival, prognosis and therapeutic re-sponse in osteogenic sarcoma: The Memorial Hospi-tal experience. Cancer 69:698–708, 1992.
23. Glynn MK, Quinlan W, Fennelly J: Endoprostheticreplacement of the proximal humerus for osteogenicsarcoma. Ir J Med Sc 151:285–287, 1982.
24. Goorin AM, Shuster JJ, Baker A, et al: Changing pat-tern of pulmonary metastases with adjuvant chemo-therapy in patients with osteosarcoma: Results fromthe multiinstitutional osteosarcoma study. J Clin On-col 9:600–605, 1991.
25. Ham SJ, Hoekstra HJ, Eisma WH, Koops HS, Old-hoff J: The Tikhoff-Linberg procedure in the treat-ment of sarcomas of the shoulder girdle. J Surg On-col 53:71–77, 1993.
26. Ham SJ, Koops HS, Veth RP, et al: Limb salvagesurgery for primary bone sarcoma of the lower ex-tremities: Long term consequences of endoprostheticreconstructions. Ann Surg Oncol 5:423–436, 1998.
27. Hornicek FJ, Mnaymneh W, Lackman RD, ExnerGU, Malinin TI: Limb salvage with osteoarticular al-lografts after resection of proximal tibial bone tu-mors. Clin Orthop 352:179–186, 1998.
28. Horowitz SM, Gautsch TL, Frondoza CG, Riley Jr L:Macrophage exposure to polymethylmethacrylateleads to mediator release and injury. J Orthop Res9:406413, 1991.
29. Horowitz SM, Lane JM, Healey JH: Soft-tissue man-agement with prosthetic replacement for sarcomasaround the knee. Clin Orthop 275:226–231, 1992.
30. Horowitz SM, Land JM, Otis JC, Healey JH: Pros-thetic arthroplasty of the knee after resection of a sar-coma in the proximal end of the tibia: A report of six-teen cases. J Bone Joint Surg 73A:286–293, 1991.
31. Hulbert SF, Cooke FW, Klawitter JJ, et al: Attach-ment of prostheses to the musculoskeletal system bytissue ingrowth and mechanical interlocking. J Bio-med Mater Res Symp 4:1–23, 1973.
32. Jensen KL, Johnston JO: Proximal humeral recon-struction after excision of a primary sarcoma. ClinOrthop 311:164–175, 1995.
33. Kaelin AJ, Emans JB: En-bloc resection for proxi-mal humerus osteogenic sarcoma. Z Kinderchir40:217–220, 1985.
34. Kaste SC, Neel MD, Meyer WH, Pratt CB, Rao BN:Extracortical bridging callus after limb salvagesurgery about the knee. Clin Orthop 363:180–185,1999.
35. Kawai A, Healey JH, Boland PJ, Athanasian EA,Jeon DG: A rotating hinge knee replacement for ma-lignant tumors of the femur and tibia. J Arthroplasty14:187–195, 1999.
36. Kawai A, Muschler GF, Lane JM, Otis JC, HealeyJH: Prosthetic knee replacement after resection of amalignant tumor of the distal part of the femur:medium to long term results. J Bone Joint Surg80A:636–647, 1998.
37. Kumar VP, Satku SK, Mitra AK, Pho RWH: Func-tion following limb salvage for primary tumors ofthe shoulder girdle. Acta Orthop Scand 65:55–61,1994.
38. Linberg BE: Interscapulo-thoracic resection for ma-lignant tumors of the shoulder joint region. J BoneJoint Surg 10A:344–349, 1928.
39. Malawer MM: Surgical technique and results of limbsparing surgery for high grade bone sarcomas of theknee and shoulder. Orthopedics 8:597–607, 1985.
40. Malawer MM: Tumors of the shoulder girdle: Tech-nique of resection and description of a surgical clas-sification. Orthop Clin North Am 22:73–75, 1991.
41. Malawer M, Buch R, Khurana JS, Garvey T, Rice L:Postoperative infusional continuous regional analgesia:A technique for relief of postoperative pain followingmajor extremity surgery. Clin Orthop 266:227–237,1991.
42. Malawer M, Canfield D, Meller I: Porous CoatedSegmental Prostheses for Large Tumor Defects. InYamamuro T (ed). New Developments for Limb Sal-vage in Musculoskeletal Tumors. New York, Springer247–255, 1989.
43. Malawer MM, Chou LB: Prosthetic survival andclinical results with use of large-segment replace-ments in the treatment of high grade bone sarcomas.J Bone Joint Surg 77A:1154–1165, 1995.
44. Malawer MM, Link MP, Donaldson SS: Sarcomasof Bone. In DeVita Jr VT, Hellman S, Rosenberg SA(eds). Cancer: Principles and Practice of Oncology.
Number 397April, 2002 Proximal Humerus Osteosarcoma Surgery 175

Ed 5. Philadelphia, Lippincott-Raven Publishers1891–1935, 1997.
45. Malawer MM, McHale K: Limb-sparing surgery forhigh grade malignant tumors of the proximal tibia:Surgical technique and a method of extensor mecha-nism reconstruction. Clin Orthop 239:231–248, 1989.
46. Malawer MM, Meller I, Dunham WK: A new surgi-cal classification system for shoulder girdle resec-tions: Analysis of 38 patients. Clin Orthop 267:33–44,1991.
47. Malawer MM, Price W: Gastrocnemius transposi-tion flap in conjunction with limb-sparing surgeryfor primary bone sarcomas around the knee. PlastReconstr Surg 73:741–750, 1984.
48. Malawer MM, Sugarbaker PH, Lampert M, BakerAR, Gerber NL: The Tikhoff-Linberg procedure:Report of ten patients and presentation of a modifiedtechnique for tumors of the proximal humerus.Surgery 97:518–528, 1985.
49. Marcove RC, Abou-Zahr K: En bloc surgery for os-teogenic sarcoma: Analysis and review of ninety op-erative cases. Bull NY Acad Med 60:748–758, 1984.
50. Marcove RC, Lewis MM, Huvos AG: En bloc upperhumeral interscapulo-thoracic resection: The Tikhoff-Linberg procedure. Clin Orthop 1124:219–228,1977.
51. Marcove RC, Mike V, Hajek JV, Levin AG, HutterRVP: Osteogenic sarcoma under the age of twenty-one. J Bone Joint Surg 52A:411–423, 1970.
52. Marcove RC, Rosen G: En bloc resections for os-teogenic sarcoma. Cancer 45:3040–3044, 1980.
53. Meller I, Bickels J, Kollender Y, et al: Malignantbone and soft tissue tumors of the shoulder girdle.Acta Orthop Scand 68:374–380, 1997.
54. O’Connor MI, Sim FH, Chao EYS.: Limb salvagefor neoplasms of the shoulder girdle: Intermediatereconstructive and functional results. J Bone JointSurg 78A:1872–1888, 1996.
55. Poss R, Brick GW, Wright RJ, Roberts DW, SledgeCB: The effects of modern cementing techniques onthe longevity of total hip arthroplasty. Orthop ClinNorth Am 19:591–598, 1988.
56. Provisor AJ, Ettinger LJ, Nachman JB, et al: Treat-ment of nonmetastatic osteosarcoma of the extrem-
ity with preoperative and postoperative chemother-apy: A report from the children’s cancer group. JClin Oncol 15:76–84, 1997.
57. Rha SY, Chung HC, Gong SJ, et al: Combined pre-operative chemotherapy with intraarterial cisplatinand continuous intravenous adriamycin for highgrade osteosarcoma. Oncol Rep 6:631–637, 1999.
58. Roberts P, Chan D, Grimer RJ, Sneath RS, Scales JT:Prosthetic replacement of the distal femur for primarybone tumors. J Bone Joint Surg 73B:762–769, 1991.
59. Rosen G, Caparros B, Huvos AG, et al: Preoperativechemotherapy for osteogenic sarcoma: Selection ofpostoperative adjuvant chemotherapy based on theresponse of the primary tumor to preoperative che-motherapy. Cancer 49:1221–1230, 1982.
60. Ross AC, Wilson JN, Scales JT: Endoprosthetic re-placement of the proximal humerus. J Bone JointSurg 69B:656–661, 1987.
61. Rubert CK, Malawer MM, Kellar KL: Modular en-doprosthetic replacement of the proximal humerus:Indications, surgical technique, and results. SeminArthroplasty 10:142–153, 1999.
62. Ruggieri P, De Cristofaro R, Picci P, et al: Complica-tions and surgical indications in 144 cases of non-metastatic osteosarcoma of the extremities treated withneoadjuvant chemotherapy. Clin Orthop 295:226–238,1993.
63. Shih LY, Sim FH, Pritchard DJ, Rock MG, Chao EYS:Segmental total knee arthroplasty after distal femoralresection for tumor. Clin Orthop 292:269–271, 1993.
64. Sim FH, Beauchamp CP, Chao EYS: Reconstructionof musculoskeletal defects about the knee for tumor.Clin Orthop 221:188–201, 1987.
65. Ward WG, Johnston KS, Dorey FJ, Eckardt JJ: Ex-tramedullary porous coating to prevent diaphyseal os-teolysis and radiolucent lines around proximal tibialreplacements. J Bone Joint Surg 75A:976–987, 1993.
66. Weiss RB: Miscellaneous Toxicities. In DeVita JrVT, Hellman S, Rosenberg SA (eds). Cancer: Prin-ciples and Practice of Oncology. Ed 5. Philadelphia,Lippincott-Raven Publishers 2799–2802, 1997.
67. Whitehall R, Wanebo HJ, Mabie KN, SchildwachterT, Rosenberger R: Reconstruction after the Tikhoff-Linberg procedure. Arch Surg 117:1248–1249, 1982.
Clinical Orthopaedics176 Wittig et al and Related Research


![Osteosarcoma of the Distal Tibia · Osteosarcoma more frequently occurs in children and adolescents, at the position of knee-joint and proximal humerus [1] (Figure 1). It is rare](https://img.dokumen.tips/doc/110x75/5fd415dc79ff91782318c086/osteosarcoma-of-the-distal-tibia-osteosarcoma-more-frequently-occurs-in-children.jpg)