Embed Size (px)
Citation preview

CLINICIAN'S CORNER
Orthodontic occlusal reconstruction afterconservative treatment of unicysticameloblastoma in an adolescent patient:10-year follow-up
Yuko Tomita,a Shingo Kuroda,b Takumi Takahashi,c Ritsuko Ohura,d and Eiji Tanakae
Tokushima, Japan
FromaPostgdics, GbAssoInstitucSeniopedicdPostInstitueProfeInstituAll auPotenReprinOrthoSchootokusSubm0889-Copyrhttp:/
466
Conservative treatment of an ameloblastoma often requires an occlusal reconstruction. In this article, we reportthe successful interdisciplinary treatment of a 14-year-old girl with a unicystic ameloblastoma in the mandible.One year after the marsupialization, enucleation with bone curettage was performed with extraction of theimpacted third molar, but the proximal second molar could be maintained. The conservative treatment requiredlong-term use of an obturator, and it caused a total open bite. Additionally, the patient genetically had a Class IImalocclusionwith severe crowding. Consequently, orthodontic treatment was performed after 4 premolar extrac-tions. There was no recurrence of the ameloblastoma 10 years after the enucleation. (Am J Orthod DentofacialOrthop 2013;144:466-70)
An ameloblastoma is one of the most commonodontogenic tumors in the jaw.1,2 Trueameloblastomas are classified into 3 subtypes:
solid and multicystic ameloblastomas, unicysticameloblastomas, and peripheral ameloblastomas.2 Inthe treatment of ameloblastomas, surgical resectionwith surrounding tissues is still the mainstream approachbecause of its high recurrence rate.3,4 On the other hand,conservative treatment, defined as treatment without apartial or complete resection of the jaw such as anenucleation or a curettage, has been recentlyrecommended to treat unicystic ameloblastomas
the University of Tokushima, Tokushima, Japan.raduate student, Department of Orthodontics and Dentofacial Orthope-raduate School of Oral Sciences.ciate professor, Department of Orthodontics and Dentofacial Orthopedics,te of Health Biosciences, Graduate School.r assistant professor, Department of Orthodontics and Dentofacial Ortho-s, Institute of Health Biosciences, Graduate School.graduate fellow, Department of Orthodontics and Dentofacial Orthopedics,te of Health Biosciences, Graduate School.ssor and chair, Department of Orthodontics and Dentofacial Orthopedics,te of Health Biosciences, Graduate School.thors have completed and submitted the ICMJE Form for Disclosure oftial Conflicts of Interest, and none were reported.t requests to: Shingo Kuroda, Department of Orthodontics and Dentofacialpedics, Institute of Health Biosciences, University of Tokushima Graduatel, 3-18-15 Kuramoto-Cho, Tokushima 770-8504, Japan; e-mail, [email protected], February 2012; revised and accepted, June 2012.5406/$36.00ight � 2013 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2012.06.021
because they are thought to have recurrence potentialbut are less aggressive than other subtypes.5-10
After the enucleation, patients are sometimesrequired to wear an obturator to cover the fenestratedsite for several months. In many cases, teeth adjacentto the tumor should be extracted or are displaced bytumor growth, even with conservative treatment. As aresult, teeth move unpredictably, and patients with uni-cystic ameloblastoma often acquire a malocclusion. Insuch cases, orthodontic occlusal reconstruction canbe used.
However, there are few reports describing orthodon-tic treatment after conservative treatment of ameloblas-tomas in children and adolescents, since a tumor in ayoung person is considered a rarity, accounting forapproximately 10% to 15% of all reported cases of ame-loblastoma.9,11,12 Moreover, only a few reports haveshown the long-term observations after enucleation ofunicystic ameloblastoma in young patients.9
This case report shows 10 years of follow-up of con-servative treatment in a young patient with unicysticameloblastoma and the usefulness of orthodonticocclusal reconstruction.
DIAGNOSIS AND ETIOLOGY
A girl, age 14 years 10 months, consulted the univer-sity hospital with a chief complaint of swelling in themandibular angle and pain on biting. On the panoramic

Fig 1. Panoramic radiographs: A, before treatment, age 14 years 10 months; B, after nucleation, age15 years 11months;C, after orthodontic treatment, age 21 years 8months;D, after 4 years of retention,age 25 years 9 months.
Tomita et al 467
radiograph, the unicystic radiolucent area with theimpacted second molar was observed on the right sideof mandible (Figs 1, A and 2, A).
Under general anesthesia, a mucoperiosteal flap wasexfoliated along the mandibular right first molar, and asmall bone defect appeared at the distal region of thefirst molar. After aspiration, the pit was enlarged toapproximately 20 mm of diameter with a bone forceps.The part of the cyst wall over the second molar was re-sected, and the crown of the impacted tooth wasexposed into the oral cavity. At the same time, anocclusal-splint obturator was placed on the mandible.
After the biopsy, the lesion was diagnosed as unicys-tic ameloblastoma. The tumor tissues had proliferationof enamel organ-like structures with a follicular pattern.Neoplastic cells on the stroma looked like ameloblasts,which had cylindrical form with ovoid-shaped nuclei.Some stellate cells were also detected in the internalcapsule of the follicle. The stroma consisted of roughconnective tissue, and edematous and peripheral hyalinedegeneration was also observed. In addition, infiltrationof inflammatory cells was found in the stroma (Fig 3).
American Journal of Orthodontics and Dentofacial Orthoped
One year after the marsupialization, the radiolucentarea was significantly reduced. Then the enucleationwith bone curettage was performed with extraction ofthe impacted thirdmolar; however, the adjacent impactedsecond molar could be maintained (Figs 1, B and 2, B).
TREATMENT PROGRESS
Three years after the surgery, orthodontic treatmentwas initiated to improve the patient's genetic and iatro-genic malocclusion (Fig 4, A and B). She was diagnosedas having an Angle Class II malocclusion, with a skeletalClass II jaw-base relationship, severe crowding, and a totalopenbite fromthe long-termuse of theocclusal splint.Herocclusal contacts were only on the right first molars andthe left molars. The mandibular second molar on theaffected side was partially erupted with buccal dislocation.
After the placement of reinforced anchorage, a palatalbar, and a facebow type of headgear on the maxilla, themaxillary first and mandibular second premolars were ex-tracted. A multibracket appliance was placed in botharches. After 33 months of treatment, an acceptable Class
ics September 2013 � Vol 144 � Issue 3

Fig 2. Computed tomography images: A, before treatment, age 14 years 11 months; B, after enucle-ation, age 17 years 11 months.
Fig 3. Images of biopsy section stained with hematoxylin and eosin:A,magnified 100 times;B,magni-fied 400 times.
468 Tomita et al
I occlusion had been achieved with an ideal interincisalrelationship (Figs 1, C and 4, C). The dislocated mandib-ular second molar was aligned and participated in the oc-clusion. After 3 years of retention, the occlusion was quitestable. Therewere no indications of ameloblastoma recur-rence during the 10 years after the enucleation (Fig 1, D).
DISCUSSION
The patient was still in adolescence when thesymptoms appeared, and the radiographic examinations
September 2013 � Vol 144 � Issue 3 American
indicated the unicystic radiolucent area. The biologicbehavior of a unicystic ameloblastoma is consideredless invasive, and it responds more favorably to conser-vative treatment than does a multicystic ameloblas-toma.5-10 Therefore, conservative therapy with themarsupialization technique was performed in thispatient.
Unicystic ameloblastoma is most generally encoun-tered in the posterior mandible and commonly associ-ated with impacted teeth.8 Some adjacent teeth to thetumor should be extracted with the ameloblastoma to
Journal of Orthodontics and Dentofacial Orthopedics

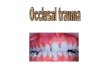
Fig 4. Intraoral photographs: A, at the start of orthodontic treatment; B, with the obturator; C, afterorthodontic treatment.
Tomita et al 469
prevent recurrence, and prosthodontic or orthodontictreatment is often necessary to reconstruct the occlu-sion, even though conservative treatments were cho-sen.13 In this patient, the eruption of the mandibularsecond molar on the affected side was disturbed by thetumor. Meanwhile, the impacted second molar naturallyerupted after the reduction of tumor volume from themarsupialization. Then we decided to keep the secondmolar, although the third molar had to be extracted.Ten years had passed since the enucleation of the ame-loblastoma; however, no recurrence was observed. As aresult, the conservative treatment of the ameloblastomamade it possible to maintain not only the jaw but alsothe molar.
On the other hand, the conservative treatmentrequired the use of the occlusal splint for more than ayear. This might have caused the patient's total openbite during the observation period after the surgery.Long-term application of such intraoral appliancesoccasionally induces an iatrogenic malocclusion.14,15
Additionally, the mandibular second molar on theaffected side was dislocated because of the
American Journal of Orthodontics and Dentofacial Orthoped
ameloblastoma. Moreover, the patient genetically hadan Angle Class II malocclusion with severe crowding.Therefore, orthodontic treatment was the only way tosolve these problems completely. Of course, aprosthetic approach was considered as an alternative,but it was a compromised process because it mighthave caused damage to her teeth.
Recent review articles have strongly suggested thatlong-term follow-up is important in conservative treat-ment of unicystic ameloblastoma because recurrencecan be years after tumor removal.7-9 Therefore,orthodontists should attend to this valuablesuggestion and observe the region where the primarylesion existed as part of interdisciplinary treatmentwhen the patient comes to the clinic during and afterthe retention phase.
CONCLUSIONS
Orthodontic occlusal reconstruction was useful in ayoung patient after conservative treatment of a unicysticameloblastoma.
ics September 2013 � Vol 144 � Issue 3

470 Tomita et al
ACKNOWLEDGMENTS
We thank Professor Naozumi Ishimaru of theTokushima University Graduate School for his helpfulcomments about the pathologic findings.
REFERENCES
1. Gorlin RJ, Chaudhry AP, Pindborg JJ. Odontogenic tumors. Classi-fication, histopathology, and clinical behavior in man and domes-ticated animals. Cancer 1961;14:73-101.
2. Robinson L, Martinez MG. Unicystic ameloblastoma: a prognosti-cally distinct entity. Cancer 1977;40:2278-85.
3. Carlson ER, Marx RE. The ameloblastoma: primary curative surgi-cal management. J Oral Maxillofac Surg 2006;64:484-94.
4. Mendenhall WM, Werning JW, Fernandes R, Malyapa RS,Mendenhall NP. Ameloblastoma. Am J Clin Oncol 2007;30:645-8.
5. Gardner DG, Corio RL. Plexiform unicystic ameloblastoma. Avariant of ameloblastoma with a low-recurrence rate after enucle-ation. Cancer 1984;53:1730-5.
6. Nakamura N, Higuchi Y, Mitsuyasu T, Sandra F, Ohishi M. Compar-ison of long-term results between different approaches to amelo-blastoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:13-20.
September 2013 � Vol 144 � Issue 3 American
7. Hong J, Yun PY, Chung IH, Myoung H, Suh JD, Seo BM, et al.Long-term follow up on recurrence of 305 ameloblastoma cases.Int J Oral Maxillofac Surg 2007;36:283-8.
8. Pogrel MA, Montes DM. Is there a role for enucleation in the man-agement of ameloblastoma? Int J Oral Maxillofac Surg 2009;38:807-12.
9. Zhang J, Gu Z, Jiang L, Zhao J, Tian M, Zhou J, et al. Ameloblas-toma in children and adolescents. Br J Oral Maxillofac Surg 2010;48:549-54.
10. Bisinelli JC, Ioshii S, Retamoso LB, Moys�es ST, Moys�es SJ,Tanaka OM. Conservative treatment of unicystic ameloblastoma.Am J Orthod Dentofacial Orthop 2010;137:396-400.
11. Keszler A, Dominguez FV. Ameloblastoma in children. J Oral Max-illofac Surg 1986;44:609-13.
12. Ueno S, Nakamura S, Mushimoto K, Shirasu R. A clinicopatho-logic study of ameloblastoma. J Oral Maxillofac Surg 1986;44:361-5.
13. Lim WH, Chun YS. Orthodontic treatment combined with auto-transplantation after removal of ameloblastoma. Am J OrthodDentofacial Orthop 2009;135:375-9.
14. Lew KK. Orthodontic finalization following therapy with an ante-rior repositioning splint. Int J Adult Orthod Orthognath Surg 1992;7:251-63.
15. Todd MA, Freer TJ. Case report—anterior open bite as a complica-tion of splint therapy. Aust Orthod J 1994;13:164-7.
Journal of Orthodontics and Dentofacial Orthopedics