Embed Size (px)
Citation preview

1
Atherosclerosis is a chronic disease with features of inflammation across the distinct stages of development.1
Plaque rupture and erosion with ensuing thrombus formation and occlusion of the artery lead to acute clinical complica-tions comprising acute coronary syndrome (ACS),2 which constitutes one of the leading causes of death worldwide.3 Therefore, there is a great medical need to improve risk pre-diction in asymptomatic patients,4 to improve early diagnosis and risk stratification of patients with ACS5 and to monitor atherosclerotic burden during treatment.
Proteins that are secreted or released from atherosclerotic lesions or thrombi into the circulation may provide a direct and simple measure of the atherosclerotic burden in individual patients. This concept has already been examined in the diag-nosis and monitoring of other diseases, for example, several types of cancers by tumor markers.6
For the discovery of such biomarker candidates, we com-bined gene expression profiling of coronary thrombi versus peripheral blood mononuclear cells and proteomic analysis of secretomes derived from atherosclerotic plaques versus
© 2015 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org DOI: 10.1161/ATVBAHA.115.305365
Objective—Blood-borne biomarkers reflecting atherosclerotic plaque burden have great potential to improve clinical management of atherosclerotic coronary artery disease and acute coronary syndrome (ACS).
Approach and Results—Using data integration from gene expression profiling of coronary thrombi versus peripheral blood mononuclear cells and proteomic analysis of atherosclerotic plaque–derived secretomes versus healthy tissue secretomes, we identified fatty acid–binding protein 4 (FABP4) as a biomarker candidate for coronary artery disease. Its diagnostic and prognostic performance was validated in 3 different clinical settings: (1) in a cross-sectional cohort of patients with stable coronary artery disease, ACS, and healthy individuals (n=820), (2) in a nested case–control cohort of patients with ACS with 30-day follow-up (n=200), and (3) in a population-based nested case–control cohort of asymptomatic individuals with 5-year follow-up (n=414). Circulating FABP4 was marginally higher in patients with ST-segment–elevation myocardial infarction (24.9 ng/mL) compared with controls (23.4 ng/mL; P=0.01). However, elevated FABP4 was associated with adverse secondary cerebrovascular or cardiovascular events during 30-day follow-up after index ACS, independent of age, sex, renal function, and body mass index (odds ratio, 1.7; 95% confidence interval, 1.1–2.5; P=0.02). Circulating FABP4 predicted adverse events with similar prognostic performance as the GRACE in-hospital risk score or N-terminal pro–brain natriuretic peptide. Finally, no significant difference between baseline FABP4 was found in asymptomatic individuals with or without coronary events during 5-year follow-up.
Conclusions—Circulating FABP4 may prove useful as a prognostic biomarker in risk stratification of patients with ACS. (Arterioscler Thromb Vasc Biol. 2015;35:00-00. DOI: 10.1161/ATVBAHA.115.305365.)
Key Words: acute coronary syndrome ◼ atherosclerosis ◼ biological markers ◼ FABP4 protein, human ◼ follow-up studies
Received on: January 22, 2015; final version accepted on: May 29, 2015.From the Institute of Clinical Chemistry (H.R., D.H., S.C.-D., A.v.E., J.G.), Department of Cardiology, University Heart Center (R.K., N.F., A.A., U.L.,
C.M.M.), University Hospital Zurich, Zurich, Switzerland; Competence Center for Systems Physiology and Metabolic Diseases (CC-SPMD), Zurich, Switzerland (H.R., A.v.E.); Zurich Center for Integrative Human Physiology (ZIHP), Zurich, Switzerland (S.C.-D., U.L., C.M.M., A.v.E.); Bioinformatics, Genetic Diversity Center, Federal Institute of Technology (ETH), Zurich, Switzerland (S.Z.); Department of Internal Medicine (P.M.-V., P.V.), Institute of Social and Preventive Medicine, Department of Community Medicine and Public Health (H.M.S.), University of Lausanne, Lausanne, Switzerland; Institute of Social and Preventive Medicine, and Clinical Trials Unit, Department of Clinical Research (D.H.), Department of General Internal Medicine (N.R.), Department of Cardiology, Swiss Cardiovascular Center Bern (S.W., P.W.), University Hospital Bern, Bern, Switzerland; and Department of Cardiology, University Hospital Geneva, Geneva, Switzerland (F.M.).
*These authors contributed equally to this article.The online-only Data Supplement is available with this article at http://atvb.ahajournals.org/lookup/suppl/doi:10.1161/ATVBAHA.115.305365/-/DC1.Correspondence to Arnold von Eckardstein, Institute for Clinical Chemistry, University Hospital Zurich, Raemistrasse 100, CH-8091 Zurich, Switzerland.
E-mail [email protected]
Circulating FABP4 Is a Prognostic Biomarker in Patients With Acute Coronary Syndrome but
Not in Asymptomatic IndividualsHans Reiser,* Roland Klingenberg,* Danielle Hof, Seraina Cooksley-Decasper, Nina Fuchs,
Alexander Akhmedov, Stefan Zoller, Pedro Marques-Vidal, Helena Marti Soler, Dik Heg, Ulf Landmesser, Nicolas Rodondi, Francois Mach, Stephan Windecker, Peter Vollenweider,
Christian M. Matter, Thomas F. Lüscher, Arnold von Eckardstein, Joanna Gawinecka
Original Research
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

2 Arterioscler Thromb Vasc Biol August 2015
healthy tissue. The few differentially expressed transcripts and proteins identified by both approaches included fatty acid–binding protein 4 (FABP4). Its expression in atherosclerotic plaques of carotid arteries was previously found to predict cardiovascular outcome7 or naturally occurring genetic low-expression variant of FABP4 to promote plaque stability and to reduce the risk of cardiovascular events.8
We therefore selected FABP4 for clinical validation as a circulating biomarker and considered 3 different situations, where a novel cardiovascular biomarker may improve clini-cal management of coronary artery disease (CAD). In clini-cal routine, electrocardiography and cardiac troponins are the gold standards for making the diagnosis of ACS.9 As the trade-off of their high sensitivity, novel cardiac troponin assays have reduced specificity,10 what may be improved by the determi-nation of additional biomarkers reflecting plaque rupture. For this reason, we assessed in a cross-sectional study (designated as the diagnostic cohort) diagnostic performance of FABP4 by comparing circulating FABP4 levels of healthy individu-als with those of patients with stable CAD or ACS. Another medical need is an improvement of risk prediction toward optimized or personalized targeting of preventive measures.
Clinical risk prediction algorithms combining demographic, clinical, and biochemical measures are nowadays reference methods; however, they differ considerably in primary and secondary prevention settings. For instance, for primary pre-vention in an asymptomatic population, algorithms and scores, such as Framingham, Pooled Cohort Equations, or European Atherosclerosis Society/European Society of Cardiology score combine information on age and sex with risk factors, such as diabetes mellitus, blood pressure, and plasma lip-ids.11 For secondary prevention of symptomatic patients, the GRACE or thrombolysis in myocardial infarction scores com-bine data on age, cardiovascular, and renal function.12 In our study, we assessed the performance of circulating FABP4 as a prognostic biomarker for the incidence of cerebrovascular and cardiovascular events in 2 nested case–control studies: 1 with 5-year follow-up of asymptomatic individuals from the gen-eral population (designated as prospective population cohort) and another with 30-day follow-up of patients with ACS (des-ignated as prospective clinical cohort).
Materials and MethodsMaterials and Methods are available in the online-only Data Supplement.
ResultsIdentification of FABP4 as a Biomarker CandidateData sets from 2 independent approaches were combined to identify biomarker candidates for CAD. In the first approach, using gene array technology, mRNA expression levels isolated from coronary thrombi were compared with those of periph-eral blood mononuclear cells from patients with ACS. In the second approach, protein profiles of atherosclerotic plaque–derived secretomes were compared with those of healthy tis-sue secretomes from the corresponding endarterectomized
Nonstandard Abbreviations and Acronyms
ACS acute coronary syndrome
AUC area under the curve
BMI body mass index
CAD coronary artery disease
CI confidence interval
FABP4 fatty acid-binding protein 4
NT-proBNP N-terminal pro–brain natriuretic peptide
OR odds ratio
STEMI ST-segment–elevation myocardial infarction
Table 1. Characteristics of the Diagnostic Cohort
Characteristics Controls, n=313 CAD, n=68 NSTEMI, n=170 STEMI, n=269 P Value
Age, y 60±10 62±7 64±13 63±12 <0.001Sex, male* 214 (68%) 59 (87%) 137 (81%) 207 (77%) 0.001Hypertension* 159 (51%) 61 (90%) 136 (80%) 184 (68%) <0.001Hypercholesterolemia* 155 (50%) 58 (85%) 124 (73%) 179 (67%) <0.001T2DM* 38 (12%) 22 (32%) 52 (31%) 152 (57%) <0.001Current smoking* 103 (33%) 9 (13%) 73 (43%) 109 (41%) <0.001Body mass index, kg/m2 27±4 29±5 27±4 27±5 0.034Total cholesterol, mmol/L 5.8±1.0 4.1±1.1 4.9±1.2 5.1±1.2 <0.001HDL, mmol/L 1.6±0.4 1.1±0.4 1.1±0.4 1.2±0.3 <0.001LDL, mmol/L 3.6±0.9 2.3±0.8 3.1±1.1 3.4±1.6 <0.001Triglycerides, mmol/L† 1.3 (0.6–3.0) 1.0 (0.5–4.4) 1.3 (0.5–3.5) 0.9 (0.4–2.6) <0.001CRP, mg/L† 1.5 (0.3–8.3) 0.9 (0.3–15.0) 3.6 (0.5–43.5) 2.2 (0.4–35.7) <0.001hsTnT, µg/L† n.d. n.d. 0.47 (0.015–3.06) 0.22 (0.12–3.34) 0.002Glucose, mmol/L† 5.6 (4.6–8.1) 5.6 (4.3–11.2) 6.0 (4.6–11.7) 7.4 (5.2–17.2) <0.001FABP4, ng/mL† 23.4 (5.9–71.0) 22.5 (7.4–73.7) 20.3 (8.8–70.2) 24.9 (10.0–77.9) 0.029
CAD indicates coronary artery disease; CRP, C-reactive protein; FABP4, fatty acid–binding protein 4; HDL, high-density lipoprotein; hsTnT, high-sensitive troponin T; LDL, low-density lipoprotein; NSTEMI, non–ST-segment–elevation myocardial infarction; NT-proBNP, N-terminal pro–brain natriuretic peptide; STEMI, ST-segment–elevation myocardial infarction; and T2DM, diabetes mellitus type 2.
*n (%), χ2 test.†Median (5th–95th percentile), Mann–Whitney U test.
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

Reiser et al FABP4 as a Prognostic Biomarker in ACS 3
carotid arteries.13 Comparison of 325 upregulated mRNAs from coronary thrombi with 390 proteins from the secre-tomes (Table I in the online-only Data Supplement) yielded 8 common hits. The FABP4 was the only protein detected in the plaque secretomes, but not in the control secretomes, its mRNA expression in coronary thrombi was 55-fold higher than in peripheral blood mononuclear cells (Table II in the online-only Data Supplement). Moreover, increased FABP4 expression in atherosclerotic plaques of carotid arteries was found to predict forthcoming adverse cardiovascular events.7 Therefore, FABP4 was selected for clinical validation.
FABP4 Confounding Factors and Correlation With Other Diagnostic ParametersIn both the diagnostic and the prospective population cohort, bivariate analysis revealed weak to moderately positive cor-relations of circulating FABP4 with age, body mass index (BMI), glucose, and C-reactive protein. Notably, FABP4 in the diagnostic cohort showed stronger correlation with BMI in asymptomatic controls than in CAD patients (P=0.34 versus 0.22, both P value <0.001). There was no significant corre-lation of FABP4 with total cholesterol, high-density lipopro-tein, low-density lipoprotein, or triglycerides in either cohort (Table III in the online-only Data Supplement). In general, circulating FABP4 levels were significantly higher in women, in individuals with BMI >25 kg/m2, diabetes mellitus, or with hypertension when compared with men, normal weight, non-diabetic, and normotensive counterparts. Circulating FABP4 was lower in current smokers than in nonsmokers, but this
difference was only significant in the diagnostic cohort (Table IV in the online-only Data Supplement).
Furthermore, circulating FABP4 showed a very weak pos-itive correlation with high-sensitive troponin T (P=0.19 and 0.01) or C-reactive protein (P=0.16 and 0.04) in the diagnostic cohort. In the prospective clinical cohort, circulating FABP4 moderately correlated with the GRACE risk score for in-hospital death or myocardial infarction (P=0.41 and <0.001), with N-terminal pro–brain natriuretic peptide (NT-proBNP; P=0.35 and <0.001) and with creatinine (P=0.45 and <0.001; Table V in the Data Supplement).
Circulating FABP4 Levels Do Not Differ Remarkably Between Patients With ACS and Asymptomatic ControlsThe cross-sectional diagnostic cohort included 820 indi-viduals from both SPUM-ACS (n=553) and CoLaus studies (n=267). The SPUM-ACS participants were recruited at the University Hospital Zurich and included 46 healthy controls, 68 patients with stable CAD, 269 patients with ST-segment–elevation myocardial infarction (STEMI), and 170 patients with non–ST-segment–elevation myocardial infarction. Since the number of healthy controls was low in the SPUM-ACS study and these individuals were younger than patients with CAD (data not shown), additional controls were selected from the CoLaus study cohort. Detailed clinical and laboratory characteristics are shown in Table 1.
One-factorial ANOVA with Games–Howell correction was applied for multiple comparisons of circulating FABP4 in
Figure 1. Odds ratios (ORs) for associations of risk factors and circulating fatty acid–binding protein 4 (FABP4) with different clinical manifestations of acute coronary syndrome in the diagnostic cohort. Multivariate logistic regression models with adjustment for several confounding factors, such as sex (male), age (years), BMI (body mass index; kg/m2), hypertension, or diabetes mellitus, were used. Plots show odds ratios with corresponding 95% confidence intervals (CIs) and P values for the 1-SD changes in the log-transformed FAPB4, and 1-SD changes in the age and BMI (Wald statistics). Models for controls vs ST-segment–elevation myocardial infarction (STEMI; A and B) and non–STEMI vs STEMI (C and D). The vertical reference line indicates an OR of 1.0. T2DM indicates diabetes mellitus type 2.
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

4 Arterioscler Thromb Vasc Biol August 2015
asymptomatic controls, patients with stable CAD and patients with ACS, respectively. Circulating FABP4 was significantly higher (P=0.01) in patients with STEMI (median 24.9 ng/mL with 5th–95th percentile range, 11.0–77.9) compared with asymptomatic controls (median 23.4 ng/mL with 5th–95th percentile range, 5.9–71.0). Other groups did not differ signif-icantly from each other with respect to the circulating FABP4.
The difference in the circulating FABP4 between patients with STEMI and asymptomatic controls remained significant after adjustment for age, sex, and BMI (odds ratio [OR], 1.3; 95% confidence interval [CI], 1.1–1.6; P=0.004). However, this significance was lost after further adjustment for diabetes mellitus and hypertension (OR, 1.2; 95% CI, 1.0–1.5; P=0.1). In contrary, differences in the circulating FABP4 between patients with STEMI and non–ST-segment–elevation myocar-dial infarction became statistically significant in both adjusted models (OR, 1.4; 95% CI, 1.1–1.8; P=0.003 and OR, 1.4; 95% CI, 1.1–1.8; P=0.01). The details of logistic regression models are presented in Figure 1. No other differences in the circulat-ing FABP4 became statistically significant after adjustment for the confounding factors.
Circulating FABP4 Predicts the Occurrence of Adverse Cerebrovascular and Cardiovascular Events in Patients With ACSThe prognostic performance of circulating FABP4 for future cerebrovascular or cardiovascular events was assessed in a
nested case–control study of 200 patients with ACS from 4 hospitals participating in the SPUM-ACS study. These patients had a primary diagnosis of unstable angina (n=12), STEMI (n=106), or non–ST-segment–elevation myocardial infarc-tion (n=82). During 30-day follow-up, 70 patients developed adjudicated cerebrovascular and cardiovascular events: death (34 cardiac deaths and 3 unclear deaths), recurrent myocardial infarction (n=22), or stroke (n=11). Cases were matched for age, sex, and center with 130 patients who survived 30 days without any event (Table 2).
Circulating FABP4 was significantly higher in patients who developed adverse cerebrovascular and cardiovascular events during the follow-up compared with control patients without any event: 39.9 ng/mL (5th–95th percentile range, 15.0–307.7) versus 26.4 ng/mL (5th–95th percentile range, 13.8–97.9), respectively, P=0.001. These differences remained statistically significant after adjustment for age, sex, creatinine level, and BMI (OR, 1.7; 95% CI, 1.1–2.5; P=0.02; Figure 2).
The prognostic performance of FABP4 for predicting adverse cerebrovascular or cardiovascular events during the follow-up was further assessed by comparison with the GRACE risk score (predictor for in-hospital death or myocar-dial infarction) and NT-proBNP levels. On Cox proportional hazard analysis, FABP4 (hazard ratio, 1.40; 95% CI, 1.04–1.87; P=0.026), GRACE risk score (hazard ratio, 1.44; 95% CI, 1.08–1.92; P=0.014), and NT-proBNP (hazard ratio, 1.35; 95% CI, 1.02–1.81; P=0.039) almost equally contributed to
Table 2. Matching for Controls and Cases in the Prospective Clinical Cohort of Patients With Acute Coronary Syndrome During 30-d Follow-Up (n=200)
Characteristic Controls, n=130 Cases, n=70 P Value
Clinical presentation* UA 8 (6%) 4 (6%) 0.20 NSTEMI 59 (45%) 23 (33%) STEMI 63 (49%) 43 (61%)Age, y 71±12 72±11 0.71Sex, male* 91 (70%) 50 (71%) 0.83Hypertension* 95 (73%) 46 (66%) 0.28T2DM* 24 (18.5%) 21 (30%) 0.06Current smoking* 31 (24%) 23 (33%) 0.13BMI, kg/m2 27±4 27±5 0.26Total cholesterol, mmol/L 4.7±1.3 4.5±1.2 0.38HDL, mmol/L 1.2±0.4 1.2±0.3 0.59LDL, mmol/L 2.9±1.2 2.8±1.0 0.93Triglycerides, mmol/L 1.3±0.8 1.1±0.7 0.11CRP, mg/L† 2.9 (0.5–73.5) 5.8 (0.4–97.9) 0.04hsTnT, µg/L† 0.306 (0.012–3.008) 0.743 (0.018–5.323) 0.01NT-proBNP, ng/L† 797 (43–7314) 1340 (76–28 094) 0.01Creatinine, µmol/L† 77.0 (52.5–142.7) 88.5 (56.2–202.7) 0.001FABP4, ng/mL† 26.4 (13.8–97.9) 39.9 (15.0–307.7) 0.001In-hospital death or myocardial infarction GRACE score
212±50 248±68 <0.001
BMI indicates body mass index; CRP, C-reactive protein; FABP4, fatty acid–binding protein 4; HDL, high-density lipoprotein; hsTnT, high-sensitive troponin T; LDL, low-density lipoprotein; NSTEMI, non–ST-segment–elevation myocardial infarction; NT-proBNP, N-terminal pro–brain natriuretic peptide; STEMI, ST-segment–elevation myocardial infarction; T2DM, diabetes mellitus type 2; and US, unstable angina.
*n (%), χ2 test.†Median (5th–95th percentile), Mann–Whitney U test.
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

Reiser et al FABP4 as a Prognostic Biomarker in ACS 5
the prediction of adverse events during the 30-day follow-up. The receiver operating characteristic analysis of FABP4 as a prognostic marker revealed an area under the curve (AUC) of 0.65 (95% CI, 0.56–0.75; P=0.001), which was nearly identi-cal to that obtained for the GRACE risk score (AUC, 0.67; 95% CI, 0.57–0.76; P<0.001). The combination of FABP4 and GRACE scores did not further improve the prediction of the outcome (AUC, 0.67; 95% CI, 0.57–0.76; P<0.001). The AUC for NT-proBNP (AUC, 0.61; 95% CI, 0.53–0.71; P=0.045) was lower, but the combination of FABP4 and NT-proBNP reached the highest AUC of 0.68 (95% CI, 0.60–0.77; P=0.045; Figure 3).
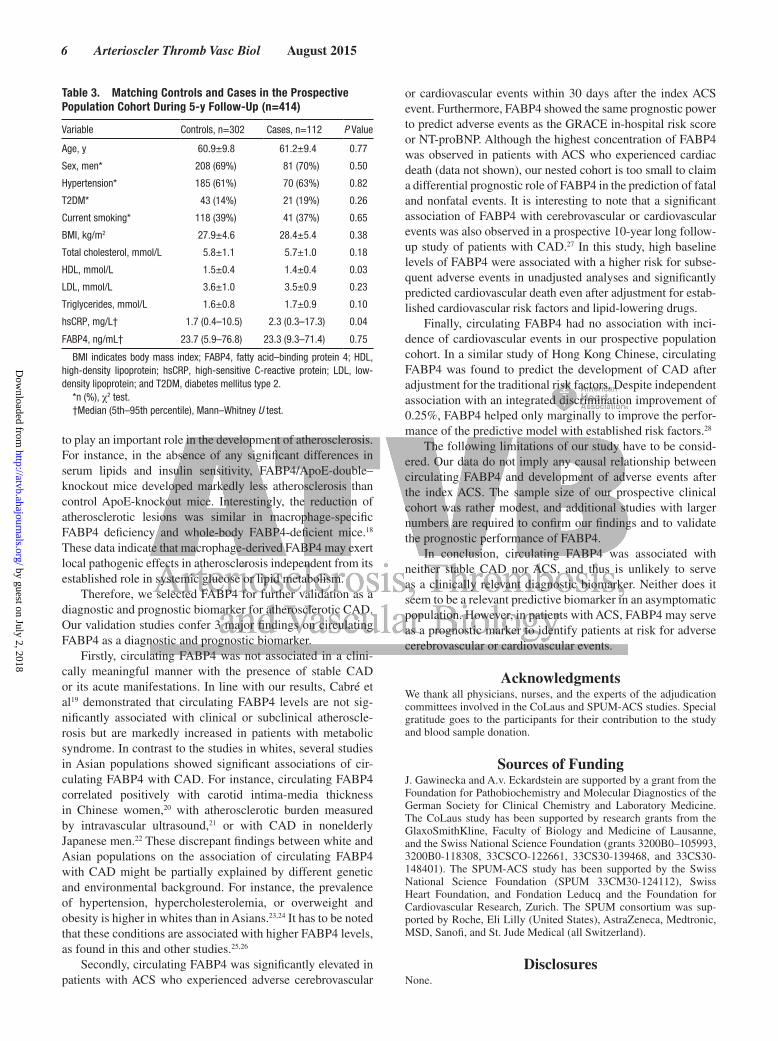
Circulating FABP4 at Baseline Does Not Predict the Development of Cardiovascular Events in the Asymptomatic PopulationThe prognostic performance of circulating FABP4 for future cardiovascular events was assessed in the prospective nested case–control cohort of 414 asymptomatic participants from the population-based CoLaus study. During 5-year follow-up, 112 individuals experienced an adjudicated cardiovascu-lar event: 22 cardiovascular deaths, 54 myocardial infarction, and 36 symptomatic CAD followed by percutaneous or surgi-cal revascularization. These cases were matched by sex, age, and health status with 302 controls who did not manifest any CAD event (Table 3). No significant difference in circulating FABP4 was found between individuals with or without inci-dence of cardiovascular event: 23.7 ng/mL (5th–95th percen-tile range, 5.9–76.8) versus 23.3 ng/mL (5th–95th percentile range, 9.3–71.4), P=0.75.
DiscussionThe purpose of this project was the identification of novel CAD biomarkers by integration of proteomic and gene expression profiling data sets obtained from atherosclerotic
plaque secretomes and coronary thrombi, respectively. The proteomic study aimed for the identification of proteins that are released from the plaque into the circulation during the progression or rupturing of atherosclerotic plaque. We previ-ously showed that the composition and phenotype of mononu-clear cells in coronary thrombi differ significantly from those of peripheral blood mononuclear cells obtained from patients with ACS.14,15 Therefore, differential gene expression profiling was performed to identify molecular characteristics of throm-bus-associated mononuclear cells that could also serve as ACS biomarkers. Comparison of both data sets revealed several common targets. One of them, FABP4 (also known as AFABP or aP2) was found in the plaque secretome but not in the con-trol secretome and its expression in coronary thrombi was 55-fold higher than in peripheral blood mononuclear cells.
FABP4 is abundantly produced in adipocytes, but sig-nificant amounts of FABP4 are also found in macrophages, which are pathogenic constituents of atherosclerotic plaques. Furthermore, a naturally occurring genetic low-expression vari-ant of FABP4 was found to promote plaque stability and reduce the risk of cardiovascular events.8 On the contrary, FABP4 expression is increased in vulnerable and ruptured plaques as shown by genome-wide expression analysis of isolated mac-rophages16 and quantification of FABP4 in vulnerable human plaques.7 Extensive studies in FABP4-deficient mice or FABP4 inhibitor–treated animals also demonstrated that FABP4 pro-motes insulin resistance and the development of diabetes melli-tus and modulates lipid metabolism.17 Moreover, FABP4 seems
Figure 2. Odds ratios (ORs) for associations of confounding factors and circulating fatty acid–binding protein 4 (FABP4) in patients with adverse cerebrovascular and cardiovascular events during 30-day follow-up after the index acute coronary syndrome event. Multivariate logistic regression model with adjustment for several confounding factors, such as sex (male), age (years), BMI (body mass index; kg/m2), and creatinine (μmol/L) were used. Plot shows ORs with corresponding 95% confidence intervals (CIs) and P values for the 1-SD changes in the log-transformed FAPB4 and creatinine values, and 1-SD changes in the age and BMI (Wald statistics). The vertical reference line indicates an OR of 1.0.
Figure 3. Fatty acid–binding protein 4 (FABP4) predicts adverse cerebrovascular and cardiovascular events during 30-day follow-up after an index acute coronary syndrome event. A, The calculated areas under the curve (AUCs) for FABP4, GRACE risk score, and their combination as predictors of adverse events was 0.65 (95% confidence interval [CI], 0.56–0.75; P=0.001), 0.67 (95% CI, 0.57–0.76; P<0.001), and 0.67 (95% CI, 0.57–0.76; P<0.001), respectively. B, The calculated AUCs for N-terminal pro–brain natriuretic peptide (NT-proBNP) was 0.61 (95% CI, 0.53–0.71; P=0.045) and for the combination of FABP4 and NT-proBNP was 0.68 (95% CI 0.60–0.77, P=0.045).
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from
6 Arterioscler Thromb Vasc Biol August 2015
to play an important role in the development of atherosclerosis. For instance, in the absence of any significant differences in serum lipids and insulin sensitivity, FABP4/ApoE-double–knockout mice developed markedly less atherosclerosis than control ApoE-knockout mice. Interestingly, the reduction of atherosclerotic lesions was similar in macrophage-specific FABP4 deficiency and whole-body FABP4-deficient mice.18 These data indicate that macrophage-derived FABP4 may exert local pathogenic effects in atherosclerosis independent from its established role in systemic glucose or lipid metabolism.
Therefore, we selected FABP4 for further validation as a diagnostic and prognostic biomarker for atherosclerotic CAD. Our validation studies confer 3 major findings on circulating FABP4 as a diagnostic and prognostic biomarker.
Firstly, circulating FABP4 was not associated in a clini-cally meaningful manner with the presence of stable CAD or its acute manifestations. In line with our results, Cabré et al19 demonstrated that circulating FABP4 levels are not sig-nificantly associated with clinical or subclinical atheroscle-rosis but are markedly increased in patients with metabolic syndrome. In contrast to the studies in whites, several studies in Asian populations showed significant associations of cir-culating FABP4 with CAD. For instance, circulating FABP4 correlated positively with carotid intima-media thickness in Chinese women,20 with atherosclerotic burden measured by intravascular ultrasound,21 or with CAD in nonelderly Japanese men.22 These discrepant findings between white and Asian populations on the association of circulating FABP4 with CAD might be partially explained by different genetic and environmental background. For instance, the prevalence of hypertension, hypercholesterolemia, or overweight and obesity is higher in whites than in Asians.23,24 It has to be noted that these conditions are associated with higher FABP4 levels, as found in this and other studies.25,26
Secondly, circulating FABP4 was significantly elevated in patients with ACS who experienced adverse cerebrovascular
or cardiovascular events within 30 days after the index ACS event. Furthermore, FABP4 showed the same prognostic power to predict adverse events as the GRACE in-hospital risk score or NT-proBNP. Although the highest concentration of FABP4 was observed in patients with ACS who experienced cardiac death (data not shown), our nested cohort is too small to claim a differential prognostic role of FABP4 in the prediction of fatal and nonfatal events. It is interesting to note that a significant association of FABP4 with cerebrovascular or cardiovascular events was also observed in a prospective 10-year long follow-up study of patients with CAD.27 In this study, high baseline levels of FABP4 were associated with a higher risk for subse-quent adverse events in unadjusted analyses and significantly predicted cardiovascular death even after adjustment for estab-lished cardiovascular risk factors and lipid-lowering drugs.
Finally, circulating FABP4 had no association with inci-dence of cardiovascular events in our prospective population cohort. In a similar study of Hong Kong Chinese, circulating FABP4 was found to predict the development of CAD after adjustment for the traditional risk factors. Despite independent association with an integrated discrimination improvement of 0.25%, FABP4 helped only marginally to improve the perfor-mance of the predictive model with established risk factors.28
The following limitations of our study have to be consid-ered. Our data do not imply any causal relationship between circulating FABP4 and development of adverse events after the index ACS. The sample size of our prospective clinical cohort was rather modest, and additional studies with larger numbers are required to confirm our findings and to validate the prognostic performance of FABP4.
In conclusion, circulating FABP4 was associated with neither stable CAD nor ACS, and thus is unlikely to serve as a clinically relevant diagnostic biomarker. Neither does it seem to be a relevant predictive biomarker in an asymptomatic population. However, in patients with ACS, FABP4 may serve as a prognostic marker to identify patients at risk for adverse cerebrovascular or cardiovascular events.
AcknowledgmentsWe thank all physicians, nurses, and the experts of the adjudication committees involved in the CoLaus and SPUM-ACS studies. Special gratitude goes to the participants for their contribution to the study and blood sample donation.
Sources of FundingJ. Gawinecka and A.v. Eckardstein are supported by a grant from the Foundation for Pathobiochemistry and Molecular Diagnostics of the German Society for Clinical Chemistry and Laboratory Medicine. The CoLaus study has been supported by research grants from the GlaxoSmithKline, Faculty of Biology and Medicine of Lausanne, and the Swiss National Science Foundation (grants 3200B0–105993, 3200B0-118308, 33CSCO-122661, 33CS30-139468, and 33CS30-148401). The SPUM-ACS study has been supported by the Swiss National Science Foundation (SPUM 33CM30-124112), Swiss Heart Foundation, and Fondation Leducq and the Foundation for Cardiovascular Research, Zurich. The SPUM consortium was sup-ported by Roche, Eli Lilly (United States), AstraZeneca, Medtronic, MSD, Sanofi, and St. Jude Medical (all Switzerland).
DisclosuresNone.
Table 3. Matching Controls and Cases in the Prospective Population Cohort During 5-y Follow-Up (n=414)
Variable Controls, n=302 Cases, n=112 P Value
Age, y 60.9±9.8 61.2±9.4 0.77
Sex, men* 208 (69%) 81 (70%) 0.50
Hypertension* 185 (61%) 70 (63%) 0.82
T2DM* 43 (14%) 21 (19%) 0.26
Current smoking* 118 (39%) 41 (37%) 0.65
BMI, kg/m2 27.9±4.6 28.4±5.4 0.38
Total cholesterol, mmol/L 5.8±1.1 5.7±1.0 0.18
HDL, mmol/L 1.5±0.4 1.4±0.4 0.03
LDL, mmol/L 3.6±1.0 3.5±0.9 0.23
Triglycerides, mmol/L 1.6±0.8 1.7±0.9 0.10
hsCRP, mg/L† 1.7 (0.4–10.5) 2.3 (0.3–17.3) 0.04
FABP4, ng/mL† 23.7 (5.9–76.8) 23.3 (9.3–71.4) 0.75
BMI indicates body mass index; FABP4, fatty acid–binding protein 4; HDL, high-density lipoprotein; hsCRP, high-sensitive C-reactive protein; LDL, low-density lipoprotein; and T2DM, diabetes mellitus type 2.
*n (%), χ2 test.†Median (5th–95th percentile), Mann–Whitney U test.
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

Reiser et al FABP4 as a Prognostic Biomarker in ACS 7
References 1. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease.
N Engl J Med. 2005;352:1685–1695. 2. Crea F, Liuzzo G. Pathogenesis of acute coronary syndromes. J Am Coll
Cardiol. 2013;61:1–11. doi: 10.1016/j.jacc.2012.07.064. 3. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional,
and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171.
4. Collinson P. The role of cardiac biomarkers in cardiovascular disease risk assessment. Curr Opin Cardiol. 2014;29:366–371. doi: 10.1097/HCO.0000000000000081.
5. Razzouk L, Fusaro M, Esquitin R. Novel biomarkers for risk stratification and identification of life-threatening cardiovascular disease: troponin and beyond. Curr Cardiol Rev. 2012;8:109–115.
6. Schwentner C, Stenzl A, Gakis G. Monitoring high-risk bladder cancer. Curr Opin Urol. 2012;22:421–426. doi: 10.1097/MOU.0b013e3283555d04.
7. Peeters W, de Kleijn DP, Vink A, van de Weg S, Schoneveld AH, Sze SK, van der Spek PJ, de Vries JP, Moll FL, Pasterkamp G. Adipocyte fatty acid binding protein in atherosclerotic plaques is associated with local vulnera-bility and is predictive for the occurrence of adverse cardiovascular events. Eur Heart J. 2011;32:1758–1768. doi: 10.1093/eurheartj/ehq387.
8. Saksi J, Ijäs P, Mäyränpää MI, et al. Low-expression variant of fatty acid-binding protein 4 favors reduced manifestations of atherosclerotic disease and increased plaque stability. Circ Cardiovasc Genet. 2014;7:588–598. doi: 10.1161/CIRCGENETICS.113.000499.
9. Amsterdam EA, Wenger NK, Brindis RG, et al; ACC/AHA Task Force Members. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:2354–2394. doi: 10.1161/CIR.0000000000000133.
10. Giannitsis E, Katus HA. Cardiac troponin level elevations not related to acute coronary syndromes. Nat Rev Cardiol. 2013;10:623–634. doi: 10.1038/nrcardio.2013.129.
11. Goff DC Jr, Lloyd-Jones DM, Bennett G, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascu-lar risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S49–S73. doi: 10.1161/01.cir.0000437741.48606.98.
12. Bawamia B, Mehran R, Qiu W, Kunadian V. Risk scores in acute coronary syndrome and percutaneous coronary intervention: a review. Am Heart J. 2013;165:441–450. doi: 10.1016/j.ahj.2012.12.020.
13. Cooksley-Decasper S, Reiser H, Thommen DS, et al. Antibody phage display assisted identification of junction plakoglobin as a potential biomarker for ath-erosclerosis. PLoS One. 2012;7:e47985. doi: 10.1371/journal.pone.0047985.
14. Wyss CA, Neidhart M, Altwegg L, Spanaus KS, Yonekawa K, Wischnewsky MB, Corti R, Kucher N, Roffi M, Eberli FR, Amann-Vesti B, Gay S, von Eckardstein A, Lüscher TF, Maier W. Cellular actors, Toll-like receptors, and local cytokine profile in acute coronary syndromes. Eur Heart J. 2010;31:1457–1469. doi: 10.1093/eurheartj/ehq084.
15. Klingenberg R, Brokopp CE, Grivès A, Courtier A, Jaguszewski M, Pasqual N, Vlaskou Badra E, Lewandowski A, Gaemperli O, Hoerstrup SP, Maier W, Landmesser U, Lüscher TF, Matter CM. Clonal restriction and predominance of regulatory T cells in coronary thrombi of patients with acute coronary syndromes. Eur Heart J. 2015;36:1041–1048. doi: 10.1093/eurheartj/eht543.
16. Lee K, Santibanez-Koref M, Polvikoski T, Birchall D, Mendelow AD, Keavney B. Increased expression of fatty acid binding pro-tein 4 and leptin in resident macrophages characterises atheroscle-rotic plaque rupture. Atherosclerosis. 2013;226:74–81. doi: 10.1016/j.atherosclerosis.2012.09.037.
17. Kralisch S, Fasshauer M. Adipocyte fatty acid binding protein: a novel adipokine involved in the pathogenesis of metabolic and vascular disease? Diabetologia. 2013;56:10–21. doi: 10.1007/s00125-012-2737-4.
18. Makowski L, Boord JB, Maeda K, Babaev VR, Uysal KT, Morgan MA, Parker RA, Suttles J, Fazio S, Hotamisligil GS, Linton MF. Lack of macrophage fatty-acid-binding protein aP2 protects mice deficient in apolipoprotein E against atherosclerosis. Nat Med. 2001;7:699–705. doi: 10.1038/89076.
19. Cabré A, Lázaro I, Girona J, Manzanares JM, Marimón F, Plana N, Heras M, Masana L. Fatty acid binding protein 4 is increased in metabolic syndrome and with thiazolidinedione treatment in diabetic patients. Atherosclerosis. 2007;195:e150–e158. doi: 10.1016/j.atherosclerosis.2007.04.045.
20. Yeung DC, Xu A, Cheung CW, Wat NM, Yau MH, Fong CH, Chau MT, Lam KS. Serum adipocyte fatty acid-binding protein levels were indepen-dently associated with carotid atherosclerosis. Arterioscler Thromb Vasc Biol. 2007;27:1796–1802. doi: 10.1161/ATVBAHA.107.146274.
21. Miyoshi T, Onoue G, Hirohata A, Hirohata S, Usui S, Hina K, Kawamura H, Doi M, Kusano KF, Kusachi S, Ninomiya Y. Serum adipocyte fatty acid-binding protein is independently associated with coronary athero-sclerotic burden measured by intravascular ultrasound. Atherosclerosis. 2010;211:164–169. doi: 10.1016/j.atherosclerosis.2010.01.032.
22. Doi M, Miyoshi T, Hirohata S, Nakamura K, Usui S, Takeda K, Iwamoto M, Kusachi S, Kusano K, Ito H. Association of increased plasma adipo-cyte fatty acid-binding protein with coronary artery disease in non-elderly men. Cardiovasc Diabetol. 2011;10:44. doi: 10.1186/1475-2840-10-44.
23. Liu J, Hong Y, D’Agostino RB Sr, Wu Z, Wang W, Sun J, Wilson PW, Kannel WB, Zhao D. Predictive value for the Chinese population of the Framingham CHD risk assessment tool compared with the Chinese Multi-Provincial Cohort Study. JAMA. 2004;291:2591–2599. doi: 10.1001/jama.291.21.2591.
24. Zheng Y, Ma W, Zeng Y, Liu J, Ye S, Chen S, Lan L, Erbel R, Liu Q. Comparative study of clinical characteristics between Chinese Han and German Caucasian patients with coronary heart disease. Clin Res Cardiol. 2010;99:45–50. doi: 10.1007/s00392-009-0076-3.
25. Bagheri R, Qasim AN, Mehta NN, Terembula K, Kapoor S, Braunstein S, Schutta M, Iqbal N, Lehrke M, Reilly MP. Relation of plasma fatty acid binding proteins 4 and 5 with the metabolic syndrome, inflammation and coronary calcium in patients with type-2 diabetes mellitus. Am J Cardiol. 2010;106:1118–1123. doi: 10.1016/j.amjcard.2010.06.028.
26. Tönjes A, Kralisch S, Lössner U, Kovacs P, Blüher M, Stumvoll M, Fasshauer M. Metabolic and genetic predictors of circulating adipocyte fatty acid-binding protein. Int J Obes (Lond). 2012;36:766–773. doi: 10.1038/ijo.2011.162.
27. von Eynatten M, Breitling LP, Roos M, Baumann M, Rothenbacher D, Brenner H. Circulating adipocyte fatty acid-binding protein levels and cardiovascular morbidity and mortality in patients with coronary heart disease: a 10-year prospective study. Arterioscler Thromb Vasc Biol. 2012;32:2327–2335. doi: 10.1161/ATVBAHA.112.248609.
28. Chow WS, Tso AW, Xu A, Yuen MM, Fong CH, Lam TH, Lo SV, Tse HF, Woo YC, Yeung CY, Cheung BM, Lam KS. Elevated circulating adipocyte-fatty acid binding protein levels predict incident cardiovascular events in a community-based cohort: a 12-year prospective study. J Am Heart Assoc. 2013;2:e004176. doi: 10.1161/JAHA.112.004176.
Blood-borne biomarkers reflecting atherosclerotic plaque burden have great potential to improve the clinical management of atherosclerotic coronary artery disease and acute coronary syndromes. Fatty acid–binding protein 4 was identified as a biomarker candidate using data inte-gration from gene expression profiling of coronary thrombi versus peripheral blood mononuclear cells and proteomic analysis of atheroscle-rotic plaque–derived secretomes versus healthy tissue–derived secretomes. In general, elevated fatty acid–binding protein 4 is associated with the incidence (of adverse secondary cerebrovascular or cardiovascular events during 30-day follow-up after the index acute coronary syndrome, independent of age, sex, renal function, and body mass index. Moreover, fatty acid–binding protein 4 predicts adverse events with similar prognostic performance as the GRACE in-hospital risk score or N-terminal pro–brain natriuretic peptide. Circulating fatty acid–binding protein 4 may prove useful as a prognostic biomarker in risk stratification of patients with acute coronary syndrome.
Significance
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

Christian M. Matter, Thomas F. Lüscher, Arnold von Eckardstein and Joanna GawineckaLandmesser, Nicolas Rodondi, Francois Mach, Stephan Windecker, Peter Vollenweider,
Alexander Akhmedov, Stefan Zoller, Pedro Marques-Vidal, Helena Marti Soler, Dik Heg, Ulf Hans Reiser, Roland Klingenberg, Danielle Hof, Seraina Cooksley-Decasper, Nina Fuchs,
but Not in Asymptomatic IndividualsCirculating FABP4 Is a Prognostic Biomarker in Patients With Acute Coronary Syndrome
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2015 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology published online June 11, 2015;Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/early/2015/06/11/ATVBAHA.115.305365World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2015/06/11/ATVBAHA.115.305365.DC1Data Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 2, 2018http://atvb.ahajournals.org/
Dow
nloaded from

FABP4 as a prognostic biomarker in ACS Reiser et al.
SUPPLEMENTAL TABLES Table I Number of identified proteins in secretomes n of proteins only
found in plaque secretome
n of proteins only found in
control secretome
n of proteins found in both secretomes
total n of proteins identified
Precipitates of specific antibodies (n=9) 18 21 66 105
Precipitate of irrelevant antibody (n=1) 0 36 6 42
All supernatants (n=10) 45 63 252 360
All measurements combined (n=10) 58 65 267 390
1

Table II Overview on proteins identified in both transcriptomic and proteomic approach. * PBMC - peripheral blood mononuclear cells
Protein name (gene name) Fold-change in
gene expression in coronary thrombi
vs. PBMC*
Identified in n of control secretome
measurements
Identified in n of plaque secretome
measurements Fibulin 3 (EFEMP1) 116 9/10 10/10
Fatty acid-binding protein 4 (FABP4) 55 0/10 5/10
Plastin 3 (PLS3) 50 9/10 10/10 Protein DJ-1 (PARK 7) 23 9/10 10/10
Cavin 1 (PTRF) 21 9/10 7/10 Complement C1s (C1S) 18 4/10 2/10
Glutathione peroxidase (GPX3) 9 4/10 6/10 Plasma protease C1 inhibitor
(SERPING1) 6 9/10 10/10
2

Supplemental Table III
Spearman rank correlations between circulating FABP4 and confounding factors or other diagnostic parameters in both the diagnostic and the prospective population-based cohort * - Correlation with troponin T was computed only for patients with MI.
Variable Diagnostic cohort Population-based cohort rho p-value rho p-value
Age 0.29 <0.001 0.18 <0.001 BMI 0.27 <0.001 0.35 <0.001 Glucose 0.15 <0.001 0.12 0.01 CRP 0.23 <0.001 0.20 <0.001 Total cholesterol -0.06 0.13 -0.06 0.21 LDL -0.06 0.19 -0.09 0.08 HDL -0.10 0.006 -0.05 0.28 Triglycerides 0.04 0.19 0.11 0.03 TnT* 0.21 0.001 n.d.
3
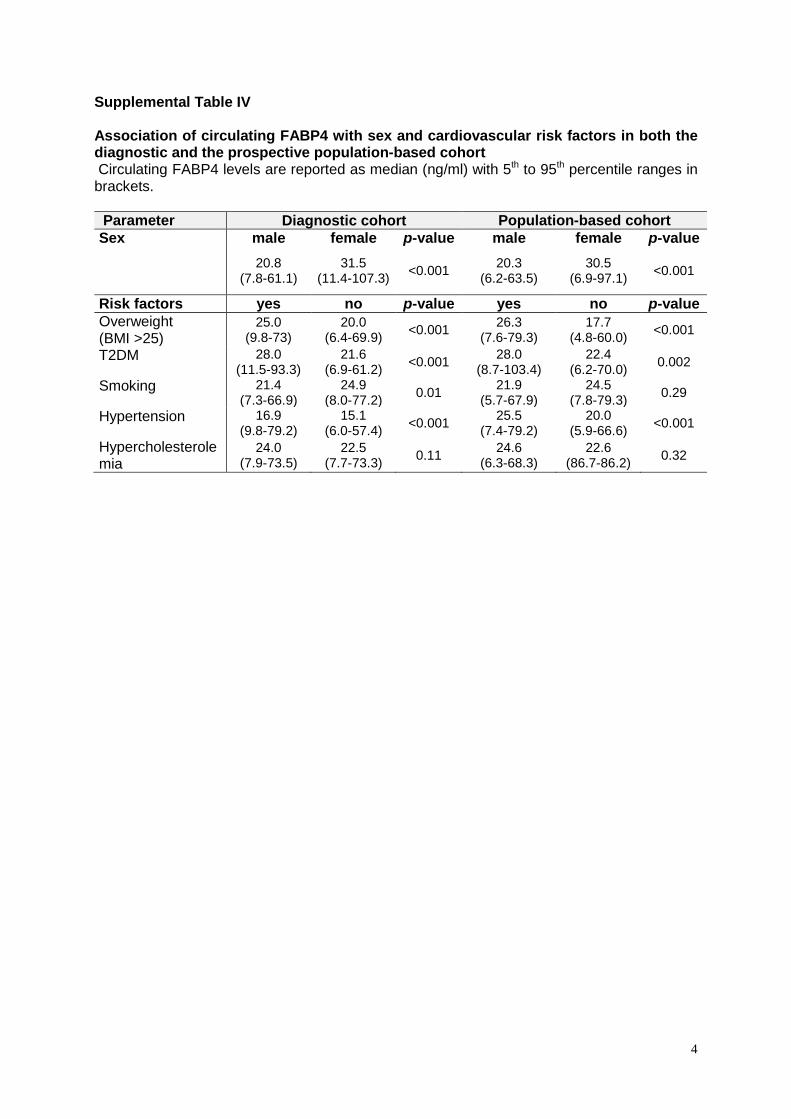
Supplemental Table IV Association of circulating FABP4 with sex and cardiovascular risk factors in both the diagnostic and the prospective population-based cohort Circulating FABP4 levels are reported as median (ng/ml) with 5th to 95th percentile ranges in brackets. Parameter Diagnostic cohort Population-based cohort Sex male female p-value male female p-value
20.8 (7.8-61.1)
31.5 (11.4-107.3) <0.001 20.3
(6.2-63.5) 30.5
(6.9-97.1) <0.001
Risk factors yes no p-value yes no p-value Overweight (BMI >25)
25.0 (9.8-73)
20.0 (6.4-69.9) <0.001 26.3
(7.6-79.3) 17.7
(4.8-60.0) <0.001
T2DM 28.0 (11.5-93.3)
21.6 (6.9-61.2) <0.001 28.0
(8.7-103.4) 22.4
(6.2-70.0) 0.002
Smoking 21.4 (7.3-66.9)
24.9 (8.0-77.2) 0.01 21.9
(5.7-67.9) 24.5
(7.8-79.3) 0.29
Hypertension 16.9 (9.8-79.2)
15.1 (6.0-57.4) <0.001 25.5
(7.4-79.2) 20.0
(5.9-66.6) <0.001
Hypercholesterolemia
24.0 (7.9-73.5)
22.5 (7.7-73.3) 0.11 24.6
(6.3-68.3) 22.6
(86.7-86.2) 0.32
4

Supplemental Table V Spearman rank correlations between circulating FABP4 and other diagnostic parameters in the prospective hospital-based cohort
Variable rho p-value hsTnT 0.19 0.01 CRP 0.16 0.04 NT-proBNP 0.35 <0.001 Creatinine 0.45 <0.001 GRACE score for in-hospital death or MI
0.41 <0.001
5
FABP4 as a prognostic biomarker in ACS Reiser et al.
MATERIAL AND METHODS
Ethics Tissue specimens and blood samples analyzed in this study were collected upon approval of the Ethics Committees in Bern, Lausanne, Geneva and Zurich. All participants provided signed informed written consent.
Study cohorts Serum samples for validation of circulating FABP4 as a potential biomarker were selected from the biobanks of two Swiss studies: a population-based cohort involving asymptomatic individuals to study epidemiology and genetic determinants of cardiovascular diseases (CoLaus, www.colaus.ch) and a clinical cohort involving patients with acute coronary syndrome (ACS), patients with stable coronary artery disease (CAD) and healthy individuals (SPUM-ACS, NCT01000701). The CoLaus (Cohorte Lausannoise) cohort is a single-center, epidemiological study including approximately 6000 individuals recruited between 2003 and 2006 in the city of Lausanne and followed for an average of 5.5 years. The rationale, sampling and follow-up procedures of the CoLaus study have been described previously1. Applied inclusion criteria included age between 35 and 75 years and willingness to the medical examination and to donate blood samples. Collected data include, but are not restricted to, demographic data, family history, cardiovascular risk factors and clinical data. To create the nested case-control cohort for this study, propensity scores based on age, sex, systolic blood pressure, lipid status, family history of cardiovascular events and menopausal status (for women) were calculated. These scores were then used to match cases (adjudicated cardiovascular death, myocardial infarction, symptomatic CAD followed by percutaneous or surgical revascularization) and controls (no cardiovascular event during five-year follow-up) at a 1:3 ratio. Consecutive patients with stable CADS and healthy individuals were enrolled between 2009 and 2012 into the SPUM-ACS study at the University Hospital Zurich. Healthy individuals were recruited from the local blood bank and presented for an ambulatory visit at University Hospital Zurich. All individuals aged ≥ 18 years were eligible if none of the exclusion criteria were found by history, clinical exam, blood analysis or echocardiogram. The following exclusion criteria were applied: use of cardiovascular medication, positive cardiovascular family history, smoking (including cessation of smoking within 2 years prior to study enrollment), history of hypertension, elevated total cholesterol (≥5.0 mmol/l), BMI > 30 kg/m2, history of diabetes mellitus, evidence of relevant valvular or structural heart disease and/or a reduced LV ejection fraction (LVEF; <55%) on echocardiogram and exclusion criteria as defined for patients with stable CAD. Patients with stable CAD were identified among patients referred for coronary angiography. All patients of both sex aged ≥ 18 years with angiographically documented coronary artery stenosis ≥50% were eligible. Exclusion criteria comprised ACS within the preceding six months, systemic infectious, inflammatory or autoimmune disease, known severe renal dysfunction (serum creatinine >220 μmol/l), known severe hepatic dysfunction (3x ULN for liver function tests), neoplasm or other life-threatening disease with a life expectancy less than one year, extended surgery in the preceding three months and/or evidence of valvular or structural heart disease and/or a reduced systolic LV function on echocardiogram or left ventricular angiogram.
1

Patients with a primary diagnosis of ACS referred for invasive management were enrolled at four Swiss university hospitals (Bern, Geneva, Lausanne and Zurich). Inclusion criteria comprised individuals aged ≥ 18 years presenting within five days (preferably within 72 hours) after pain onset with a main diagnosis of STEMI, NSTEMI or unstable angina. Exclusion criteria comprised severe physical disability, inability to comprehend study or less than one year of life expectancy for non-cardiac reasons. Follow-up was performed at 30 days with events adjudicated by independent experts. A nested case-control cohort for this study was constructed from patients with ACS, matching one case with two controls based on age, sex and medical center. Cases were defined as experiencing the endpoint cardiac death, recurrent myocardial infarction or stroke up to 30 days of follow-up, whereas controls did not experience this same endpoint up to 30-days of follow-up. The detailed patient characteristics of the diagnostic cohort are shown in Table 1. Matching for controls and cases in the prospective clinical cohort with 30-day follow-up and in the prospective population-base cohort with 5-year follow-up are shown in Table 2 and Table 3, respectively. GRACE risk score The GRACE risk score for in-hospital death or myocardial infarction was calculated using GRACE 2.0 ACS Risk Calculator (http://www.outcomes-umassmed.org/grace/) 2 and included the following parameters: age, heart rate, systolic blood pressure, Killip classification, blood creatinine, ST-segment deviation, cardiac arrest at admission, and positive high sensitive troponin T test (hsTnT).
Gene expression array of coronary thrombi Total RNA of freshly isolated thrombi and corresponding peripheral blood mononuclear cells from 15 patients with ACS was isolated using commercially available Qiagen RNeasy Mini Kit® (Qiagen) according to the manufacturer’s instructions. The concentration, purity and integrity of the isolated total RNA was determined using a NanoDrop® ND1000 (NanoDrop Technologies, Wilmington, USA) and a Bioanalyzer 2100 (Agilent Technologies, Basel, Switzerland). Quantitatively and qualitatively best RNA samples from a total of four patients were used for cDNA synthesis and analysis using Human Genome U133 Plus 2.0 Affymetrix Gene Chip® (Affymetrix, Inc. Santa Clara, USA). The microarray expression data were pre-processed with the statistics software R using the RMA method as implemented in the Affymetrix package. Differential expression analysis was performed with the moderated t-statistic and false discovery rate (FDR) multiple-test correction methods of the LIMMA package. Transcripts with a false discovery rate less than 0.1 and absolute linear fold-change of at least two were considered as significantly differentially expressed. The raw microarray expression data have been deposited in NCBI’s Gene Expression Omnibus and are accessible through GEO series accession number GSE19339 (http://www.ncbi.nlm.nih.gov/geo).
Proteomic analysis of plaque secretomes Proteomes were obtained by the combined application of antibody phage display and mass spectrometry to secretomes derived either from atherosclerotic plaques of endarterectomized carotid or iliac arteries or control arterial tissues were obtained as previously described3. In short summary, six independent and subtractive selections of single chain variable fragments (scFVs) from large synthetic human phage-displayed scFvs library, ETH-2-Gold, were performed using pairs of plaque and control secretomes obtained from six different patients. In subsequent ELISAs, nine of the 34 scFvs were found to react stronger with the plaque secretomes than with the respective control secretomes from at least three of four patients. Finally, these selected scFvs and one irrelevant control antibody as well as an
2

empty bead control were used as baits for immunoprecipitation and MS identification of their antigens in mixtures of two plaque and two control secretomes.The 140 microgram of both immunoprecipitated proteins and supernatants of each of the nine scFvs plus one control antiobody (together 10 experiments) were separated by standard 1D SDS-PAGE. After Roti-Blue-staining, each lane of the gel representing the proteome of either the immunoprecipitated material or the supernatant was cut into twelve segments each of which was transferred into individual wells of 96-well plates. Reduction with DTT, alkylation with IAA, followed by trypsin digestion was performed using a liquid handling robot (TECAN). Subsequently, samples were concentrated, purified using ZipTip-µC18 (Millipore) and analyzed on a LTQ-Orbitrap XL mass spectrometer (Thermo Fischer Scientific) coupled to an Eksigent-Nano-HPLC system (Eksigent Technologies, USA). Full-scan MS spectra (300-2’000 m/z) were acquired with a resolution of 60’000 at 400 m/z after accumulation to a target value of 500’000. Collision induced dissociation MS/MS spectra were recorded in a data-dependent manner in the ion trap from the six most intense signals. Mascot Deamon 2.3.0 (Matrix Science) was used to search the in-house FGCZ human decoy database. Data interpretation was done using Scaffold 3 (Proteome Software).The complete secretome proteome was therefore reconstructed by combining the immunoprecipitated proteins and the proteins identified in the respective supernatants (Supplemental Table 1).
ELISA measurements of FABP4 Serum samples were stored at -80°C until analyzed. Serum FABP4 concentrations were determined using a commercially available Adipocyte FABP4 Human ELISA kit from Biovendor (Laboratorni medicina a.s., Czech Republic). Assays were performed according to the manufacturer’s instructions. Samples were measured in duplicates. The intra- and inter-assay coefficients of variations were 3.4% and 5.6%, respectively.
Statistical analysis Statistical analyses were performed using SPSS 21.0 for Windows (IBM Software). Continuous variables that were not normally distributed, as determined using the D’Agostino test, were logarithmically transformed before analysis in order to resemble a normal distribution. One-factorial ANOVA with Games-Howell correction was used for multiple comparisons of circulating FABP4 between analyzed groups. Remaining bivariate analyses for continuous variables were performed using unpaired t-test for normally distributed data and Mann-Whitney rank test for non-normally distributed data. Results are reported either as mean ± SD or median with 5th and 95th percentiles for the corresponding calculations, respectively. Categorical variables were compared using χ2 test. Bivariate correlations between circulating FABP4 and other continuous variables were performed using Spearman rank correlation. All reported p-values are 2-tailed and p<0.05 indicates statistical significance. Models of binary logistic regression with adjustment for several confounding factors were used to determine the association of circulating FABP4 (effect of 1-SD of the log-transformed FAPB4 value) with CAD or incidence of secondary cardiovascular events during 30-day follow-up after initial ACS. The performance of binary logistic regression models were assessed by Hosmer-Lemeshow goodness-of-fit. Odds ratios (OR) are reported with 95% confidence intervals (95% CI). Cox proportional hazard model consisted of FABP4 or GRACE risk score was employed to analyze association of circulating FAPB4 (log-transformed FAPB4 value) with the incidence of death or myocardial infarction during 30-day follow-up. Hazard ratios (HR) are reported with 95% confidence intervals (95% CI).
3

References 1. Firmann M, Mayor V, Vidal PM, Bochud M, Pecoud A, Hayoz D, Paccaud F, Preisig M, Song KS, Yuan X, Danoff TM, Stirnadel HA, Waterworth D, Mooser V, Waeber G, Vollenweider P. The CoLaus study: a population-based study to investigate the epidemiology and genetic determinants of cardiovascular risk factors and metabolic syndrome. BMC Cardiovasc Disord 2008;8:6.
2. Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, Van De Werf F, Avezum A, Goodman SG, Flather MD, Fox KA, Global Registry of Acute Coronary Events I. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med 2003;163(19):2345-53.
3. Cooksley-Decasper S, Reiser H, Thommen DS, Biedermann B, Neidhart M, Gawinecka J, Cathomas G, Franzeck FC, Wyss C, Klingenberg R, Nanni P, Roschitzki B, Matter C, Wolint P, Emmert MY, Husmann M, Amann-Vesti B, Maier W, Gay S, Luscher TF, von Eckardstein A, Hof D. Antibody phage display assisted identification of junction plakoglobin as a potential biomarker for atherosclerosis. PLoS One 2012;7(10):e47985.
4





























