Embed Size (px)
Citation preview

doi: 10.2522/ptj.20100421Originally published online October 27, 2011
2012; 92:236-250.PHYS THER. Michael J. ShoemakerMichigan: Challenges to Policy AdoptionDirect Consumer Access to Physical Therapy in
http://ptjournal.apta.org/content/92/2/236found online at: The online version of this article, along with updated information and services, can be
Online-Only Material 6.DC1.html
http://ptjournal.apta.org/content/suppl/2012/01/20/92.2.23
Collections
Professional Issues Policies, Positions, and Standards
Health Care System Direct Access
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

Direct Consumer Access to PhysicalTherapy in Michigan: Challenges toPolicy AdoptionMichael J. Shoemaker
Background. Despite the ability of consumers to receive treatment from a phys-ical therapist without a physician referral or prescription in 45 states, Michigancontinues to require a physician prescription. Given the impending primary careprovider shortage, direct access should be considered as a potential solution tobarriers that prevent patients from accessing timely musculoskeletal care.
Objective. The purpose of the present policy analysis was to analyze why anattempt in 2006 to remove the prescription requirement in Michigan was notadopted.
Methods. The Policy Analysis Triangle approach, which considers the relevantactors, processes, and context in which a policy must be considered, was used toanalyze why Michigan House Bill 5618 was not passed. Data sources includedposition statements from relevant stakeholders, state government documents, stake-holder analysis, and a systematic review of the literature.
Results. Multiple data sources, including a systematic review of the literature,revealed that direct access does not pose a risk to public safety and may result inbetter outcomes with regard to cost and quality of care. Failure of Michigan to adoptdirect access in 2006 was due to scope of practice conflicts and various politicalcontexts and processes.
Conclusions. Direct consumer access to physical therapy services appears to besound health policy that should be reconsidered by Michigan’s legislature to alleviatethe primary care provider shortage for those with musculoskeletal disorders.
M.J. Shoemaker, PT, DPT, GCS,Department of Physical Therapy,Cook-DeVos Center for Health Sci-ences, Suite 247, Grand ValleyState University, 301 MichiganNE, Grand Rapids, MI 49503-3314 (USA). Address all corre-spondence to Dr Shoemaker at:[email protected].
[Shoemaker MJ. Direct consumeraccess to physical therapy inMichigan: challenges to policyadoption. Phys Ther. 2012;92:236–250.]
© 2012 American Physical TherapyAssociation
Published Ahead of Print: October27, 2011
Accepted: September 19, 2011Submitted: December 14, 2010
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
236 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

The projected shortage of atleast 44,000 primary care pro-viders1 and the 32 million
newly insured individuals resultingfrom the federal Patient Protectionand Affordable Care Act of 2010(PL 111-148)2 will require that theUnited States closely examine thedeployment of the nation’s healthcare providers. A diverse and highlyspecialized workforce providesopportunities for a variety of disci-plines to function in primary careroles to improve access and reducecost by eliminating unnecessary pro-vider visits. However, redeploymentof a discipline may be limited insome states due to restricted scopesof practice. “Direct access” is theterm describing the ability of apatient to go directly to a physicaltherapist without a prescription orreferral from a physician. Physicaltherapists are trained to function asprimary care providers for musculo-skeletal problems, have the potentialto help mitigate the substantial pro-jected primary care provider short-age, and are able to currently func-tion in this role in 46 states.3,4
Michigan is 1 of 4 states that con-tinue to require physician prescrip-tion or referral, which prevents thepublic from directly accessing thecare of a physical therapist.
The purpose of the present analysisis to examine why the most recentattempts to pass direct access legis-lation in Michigan failed, in order todirect future legislative efforts. ThePolicy Analysis Triangle approach,developed by Walt and Gilson,5,6
was selected as the policy analysisframework because it is comprehen-sive in its consideration of the manyother factors beyond the merits ofa policy that influence its devel-opment and adoption. Walt and Gil-son based the framework on theirobservations that policy adoptionand implementation failure occursbecause most policy analyses focuson content of the proposed policy
rather than on the context, pro-cesses, and actors involved in pol-icy adoption and development. Thisanalysis, therefore, also will considerthose additional factors.
BackgroundHistory of Direct Accessin the United StatesIn 1973, the House of Delegates(HOD), as the decision-making bodyof the American Physical TherapyAssociation (APTA), resolved toestablish the necessary “guidelineswhich stipulate the professional andethical implications and responsibil-ities of [physical therapist] evalua-tion [of patients] without practitio-ner referral.”7 The HOD revised thisresolution in 1978 to “devise a planfor the development of physicaltherapy practice [evaluation andtreatment] independent of practitio-ner referral.”8 At that time, only 2states did not require practitioner/physician referral. Subsequently,APTA began a direct access initiativeto eliminate the physician referralrequirement in all jurisdictions in theUnited States.9 There also were pro-gressive changes in professional edu-cation standards to better prepareentry-level clinicians to be able toscreen for the presence of medicaldisease and to function in a directaccess environment as a point ofentry into the health care system.These efforts have resulted in 46states and the District of Columbianow permitting some degree ofdirect consumer access to physicaltherapy treatment. Seventeen stateshave unrestricted direct access, andthe other 29 states and the Districtof Columbia have a variety of pro-visions or restrictions on how a con-sumer can access and receive physi-cal therapy treatment.9 Examplesof these provisions or restrictionsinclude: (1) time limits that require areferral within a specified period oftime from the beginning of care,(2) referral to a physician if progressis not made within a specified time
frame or if the patient exhibitssigns or symptoms of a problem out-side of the physical therapist’s scopeof practice, (3) experience or con-tinuing education requirements, and(4) established diagnoses or priorreferral for physical therapy for thesame problem.
History of the Michigan PublicHealth Code and PhysicalTherapist Scope of PracticePhysical therapists in Michigan havebeen licensed since 1965 as a resultof Michigan Public Act (PA) 164. Theinitial scope of practice of physicaltherapy was restricted to being“under the prescription and direc-tion of a physician,” defined as adoctor of medicine, osteopathy, orpodiatry. The requirement for prac-tice under the “direction” of a phy-sician was removed as a result ofMichigan PA 368 of 1978. Doctors ofdentistry were permitted to pre-scribe physical therapy by MichiganPA 178 of 1982, but those with asubfield license (eg, physician’sassistant who is licensed as a subfieldof medicine) were prohibited fromdoing so. In 1987, Michigan PA 213permitted physical therapists toevaluate, educate, and consult with-out a prescription, but retained therequirement for treatment uponphysician prescription. Attempts toremove the physician prescriptionrequirement during several legisla-tive sessions were not successful(Michigan House Bill [HB] 5014/Senate Bill [SB] 620 of 2001–2002,HB 4176/SB 1174 of 2003–2004, andHB 5618 of 2005–2006).
Available WithThis Article atptjournal.apta.org
• Discussion Podcast with authorMichael Shoemaker, AngelaChasteen, and Rick Gawenda.Moderated by Linda Resnik.
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 237 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

Regulatory Policymakingand Policy AnalysisThe purpose of regulatory policy-making is to provide the neces-sary constraints on a group ofindividuals “to produce outcomesconsistent with citizens’ prefer-ences manifested by democraticallyaccountable representatives.”10(p411)
In the context of health professionalscope of practice under a state’s pub-lic health code, regulatory policy-making seeks to provide protectionto health care consumers receivingservices in that state.11 Lawmakersdeveloping and modifying policieswithin the public health code, there-fore, are acting as moral agentswho must understand how the pub-lic will be affected by such poli-cies.12 However, the philosophicalunderpinnings of policymaking ina democratic society are rooted inrationality and pragmatic philoso-phy, which seek to achieve a “work-ing harmony between diverse val-ues, desires, and their anticipatedconsequences.”13(p265) Indeed, mod-ern regulatory policymaking is notfree of special interest influence, nor
can the scientific evidence used inpolicymaking be apolitical.14
Policy analysis can be a retrospec-tive or prospective endeavor. Eithercan provide insight into the com-plex process of policy development,adoption, and implementation.5,6
Retrospective analysis can provideinsight into why a policy was orwas not adopted and, if adopted,how effectively a policy was imple-mented, whereas prospective analy-sis can provide concurrent and pre-dictive understanding and guidancein the policymaking process.5 Bestpractices in policy analysis utilizeframeworks to ensure that the con-clusions of an analysis are “clearand testable propositions.”6 Further-more, policy analysis can foster boththe development and utilization oftheories that explain the policymak-ing process.6 The present analysis isretrospective.
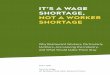
Methods ofReview and AnalysisWalt and Gilson’s Policy AnalysisTriangle15,16 (Figure) accounts for
additional factors beyond policycontent that affect policy develop-ment, adoption, and implementa-tion, including social and politicalcontexts, political processes, andprimary stakeholders or actors. ThePolicy Triangle framework, there-fore, can help explain why, in asocial and political system of com-peting interests, policy adoptionand implementation attempts havefailed and may help direct futurepolicymaking strategies. The presentanalysis utilized the Policy AnalysisTriangle approach to establish thecontent, context, processes, andactors relevant to direct access legis-lation in Michigan during the 2001–2002, 2003–2004, and 2005–2006legislative sessions.
Analysis of policy content includesnot only a description of the policy’sintent and provisions, but also anassembling and examination of theevidence regarding the anticipatedimpact of the policy.17 Therefore,in addition to describing the pro-posed changes to the Michigan Pub-lic Health Code introduced during 3different legislative sessions, thepresent analysis of policy contentsought to describe the potentialimpact of the direct access using theavailable research evidence and itseffect on access, cost, and quality ofphysical therapy services.
The analysis of the policy content ofdirect access legislation introducedduring each Michigan legislativesession included examination of theprovisions in each bill. This was sup-plemented by use of House and Sen-ate legislative analyses when avail-able. Michigan House and Senatelegislative analyses are written bynonpartisan House or Senate staff foruse in legislative deliberations andprovide a summary of the intent, pro-visions, and arguments provided bysupporters and opponents of a bill.Each bill and the associated analyses
Figure.The Health Policy Triangle.5,6
Direct Consumer Access to Physical Therapy in Michigan
238 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

are available on the Michigan Legis-lature Web site.18
Given that analysis of policy con-tent includes examination of thepotential impact of a proposedpolicy,16 the present analysis alsoincluded examination of the evi-dence regarding the potential impactof direct access that might havebeen available to legislators in theirdecision making during a given leg-islative session. This examinationincluded a literature search ofCINAHL and PubMed databasesusing the following key words:“physical therapist,” or “physicaltherapy” and “medical screening,”“medical referral,” “decision-making,”or “direct access.” Reference listsfrom articles found by these searcheswere utilized to discover additionalarticles. Articles were included ifthey specifically addressed some ele-ment of direct access or medicalscreening (identification of diseaseoutside of the physical therapistscope of practice) by physical thera-pists. There were no exclusion crite-ria. Articles were considered to be“available” for consideration by leg-islators if they were published by themidpoint of the legislative session inwhich the legislation had been intro-duced (eg, for legislation introducedduring the 2005–2006 legislative ses-sion, articles were considered to be“available” if published by 2005).
Analysis of the context of the pro-posed legislation included exam-ination of situational and culturalfactors that provide a better under-standing of how direct access legis-lation may have been perceived bylegislators and possible reasons whythe proposed legislation failed to beadopted. Situational factors weredefined as other specific legislativeevents or legislative precedentsrelated to the practice of physicaltherapy, as well as a description ofthe legislature in terms of politicalparty control. Cultural factors were
defined as general perceptions ofphysical therapy that may haveexisted at the time that each bill wasbeing considered. Therefore, analy-sis of context included:
• Consideration of the prevalence ofdirect access in other states usingdata from APTA about the numberof states that permitted directaccess during each legislativesession.
• Consideration of federal legislationknown to the author that sought toremove the physician prescriptionrequirement for physical therapyservices provided under Medicare.
• A search on the Michigan Legisla-ture Web site for other legislationduring each of the 3 legislative ses-sions that amended or proposed toamend the physical therapy prac-tice act. The search term used was“physical therapy.”
• Description of the legislature withregard to party control using histor-ical data from the Michigan Legisla-ture Web site.18
The analysis of processes included adescription of each bill’s progressand final disposition in the legisla-ture, analysis of legislator votingrecord on direct access, identifica-tion of relevant stakeholders, adescription of stakeholders’ positionon direct access, and an estimationof stakeholder influence. Bill prog-ress, disposition, and legislator vot-ing record were obtained using theMichigan Legislature Web site. Rele-vant stakeholders and their positionswere identified using the MichiganHouse and Senate legislative analy-ses, which identify supporters andopponents of the bill and describeeach group’s rationale for their posi-tion. An attempt also was made toexamine committee hearing atten-dance and written testimony; how-ever, Michigan law does not requirethis information to be retained fol-lowing the conclusion of the legisla-tive session. Thus, this information
was not available for analysis. There-fore, stakeholder position also wasdetermined using position state-ments from representative organiza-tions when available. Stakeholderinfluence was estimated by politicalaction committee (PAC) contribu-tions obtained from the MichiganCampaign Finance Reporting Search-able Database.
Additional sources of data were uti-lized to support the aforementionedanalysis strategies. First, a search formedia stories about direct consumeraccess in Michigan was conductedusing the MLive online news outletfor Michigan and the NewsBank data-base with the Michigan filterselected. Search terms were “physi-cal therapy” or “physical therapist”and “direct access,” “scope of prac-tice,” “referral,” or “prescription.”
The second additional source ofdata to support the planned analy-sis was consultation with 2 lobbyistsfrom a large, multiclient lobbyingfirm (Bret Marr and Terry Vander-veen from Muchmore, Harringtonand Smalley Associates, Lansing,Michigan; personal communication;February 14, 2011). The lobbyistswere selected based on authorconvenience. Both lobbyists cur-rently represent the Michigan Physi-cal Therapy Association (MPTA),although neither were involved inthe direct access efforts describedin this article. Multiclient lobbyingfirms represent a wide variety of spe-cial interest groups and have exper-tise in many different industries.Both lobbyists were very familiarwith direct access legislation, as onerepresented the Michigan Occupa-tional Therapy Association and theother represented the Michigan Col-lege of Emergency Physicians (nei-ther organization had a position onany of the bills analyzed in this arti-cle). The purpose of the lobbyistconsultation was to provide unbi-ased, expert insight into and confir-
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 239 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

mation of those elements in thepolitical process that are not docu-mented. Both lobbyists were pro-vided a draft of the article containingbackground, collected data, and pro-visional analysis in advance of a1-hour conference call. The discus-sion during the consultation wasunscripted, unrecorded, and focusedon the influence of stakeholder PACcontributions on political processesand possible reasons that directaccess legislation failed to progress(Appendix).
ResultsContentThe intent of and provisions in eachbill were obtained from the billsand the associated legislative analy-ses, which provided the followingcontent-related information (brieflyoutlined in Tab. 1). The primaryobjective of each bill was to removethe prescription requirement forphysical therapy intervention. Eachbill had additional provisions stat-ing that patients must be referred toa physician if they have problemsoutside of the physical therapistscope of practice or do not makereasonable progress. Other pro-posed changes to the Michigan phys-ical therapy practice act included theaddition of a continuing educationrequirement for license renewal, def-inition of the physical therapist assis-tant, endorsement of APTA’s pro-fessional Standards of Practice andCode of Ethics, and a requirementthat applicants for initial licensurepossess the Doctor of Physical Ther-apy degree by 2009. A final provi-sion in each bill stated that changesin the physical therapist scope ofpractice would not require nor pre-clude third-party payer reimburse-ment for services provided underdirect access. It should be noted thatHB 5618 of 2005 included consider-ably more restrictions on providinginterventions under direct access(Tab. 1).
With regard to the potential impactof direct access in Michigan, a liter-ature search sought to determinewhat research evidence was poten-tially available to legislators duringtheir deliberations in each legisla-tive session. The articles that wereavailable during each legislative ses-sion are summarized in Table 1. Dur-ing the 2001–2002 session, 11 arti-cles were available. All articlessupported direct access and sug-gested that direct access mayincrease access19–22 and reducecost.23 The articles also providedsome evidence that direct accesswould not compromise clinical out-comes24–26 and that physical thera-pists are able to screen for medicaldisease.27–29 During the 2003–2004legislative session, only an additionalcase report about the medicalscreening ability of physical thera-pists became available.30 However,by the 2005–2006 session, there wasa substantial increase in the numberof published articles that were avail-able to legislators. Fourteen new arti-cles provided further support ofdirect access: 1 article demonstratedthat physician prescription specific-ity was not related to outcome ornumber of visits,31 1 article demon-strated no adverse events or epi-sodes of litigation under directaccess,32 2 articles demonstratedadequate physical therapist perfor-mance on case-based tests and sce-narios,33,34 and 10 additional casereports demonstrated physical thera-pists’ ability to screen for medicaldisease.35–44 One article raised con-cern about physical therapists’ abil-ity to screen for medical disease bydemonstrating that physical thera-pists underestimated the probabilityof deep vein thrombosis in severalcase vignettes.45 Table 2 briefly sum-marizes all articles about directaccess that were available duringthe Michigan 2005–2006 legislativesession.
ContextA strength of the Policy Analysis Tri-angle approach is that it includes ananalysis of the context in which pro-posed changes in health policy mustbe adopted. The analysis revealedseveral situational and cultural fac-tors that may have contributed to thefailure of direct access legislationduring the three separate legislativeattempts (Tab. 1).
Situational factors. Several situa-tional factors may have negativelyinfluenced legislators’ perceptionsabout direct access. Despite theincrease from 36 to 43 states thatpermitted direct access to physicaltherapist intervention during the2001–2006 period, federal (Medi-care) policy continued to requirephysician referral for physical ther-apy provided to Medicare beneficia-ries. Federal legislation to repeal thisrequirement introduced in each con-gressional session failed to pass.
With regard to other legislationattempting to amend the physicaltherapy practice act in Michigan,several bills were found during theMichigan 2005–2006 legislative ses-sion that highlighted issues relatedto autonomous physical therapistpractice. Michigan PA 281 of 2005allowed physician assistants to pre-scribe physical therapy. This legisla-tion was unanimously adopted, withsupporters stating that because ofphysician oversight, physician assis-tants prescribing physical therapyposed no risk to patient safety. How-ever, Michigan HB 5288 of 2005, abill to allow nurse practitionersto autonomously prescribe physicaltherapy, was only introduced intothe House and did not progress fur-ther. No legislative analyses wereavailable for review, but accordingto lobbyists from a large, multi-client lobbying firm (Bret Marr, TerryVanderveen; personal communica-tion; February 14, 2011), the bill wasnot addressed by the legislature
Direct Consumer Access to Physical Therapy in Michigan
240 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

Table 1.Summary of Resultsa
Content
Legislative Session
2001–2002 HB 5014/SB 620 2003–2004 HB 4176/SB 1174 2005–2006 HB 5618
Key provisions The same provisions were included in 2000–2001 and 2003–2004:-Removal of prescription requirement-Requirement for referral to physician if signs or symptoms of problemoutside scope of practice or no reasonable improvement
-Establishment of continuing education requirement with commensurateincrease in licensing fee
-Endorsement of professional Standards of Practice and Code of Ethics-Definition of the PTA-Exemption of third-party payers from any requirement to pay for servicesunder DA
-Requirement for the DPT for eligibility for initial licensure after 2009
Same provisions as previous years, withadditional restrictions on practice underdirect access:-Allowed if service is for same diagnosisas previously treated within previousyear and one of the following:
1. Possesses the DPT2. Has 2 years of experience3. A physician is readily available in
the facility-Must inform primary health careprovider
-Must have additional continuingeducation in differential diagnosis
-Must be CPR certified-Must refer to physician for careexceeding 45 days or 20 visits
No. of published articles 11 12 27
Context
No. of states with DA 35 39 43
Relevant factors-Cultural
-Societal perspective of the need for physician oversight and direction of care-Failure of federal legislation seeking to permit DA under Medicare
-Situational -No other legislation related tophysical therapy
-No other legislation related tophysical therapy
-Physician assistants allowed to prescribephysical therapy under physicianoversight
-Failed attempt to allow nursepractitioners to prescribe physicaltherapy because it would be withoutphysician oversight
-Physical therapists prohibited fromperforming needle electromyography
Republican House, Senate, andgovernor
Republican House and Senate;Democratic governor
Republican House and Senate;Democratic governor
Processes
Legislative disposition -Introduced to House and SenateJuly 2001
-Referred to respective healthpolicy committees
-Passed House Policy Committeeand House; vote 65–33, withbipartisan support
-Senate Health Policy Committeedid not hold a hearing; senatorsponsor/physician/Health PolicyCommittee member did notadvocate for a hearing
-Introduced to the House February2003, Senate April 2004
-Referred to respective health policycommittees
-House Health Policy Committeehearing September 2004; no votetaken that day, nor during theremainder of the session despiterepeated requests by the Housesponsor
-Senate Health Policy Committee didnot hold a hearing
-Introduced to House-Referred to Health Policy Committee-No hearing was held-Senator/physician on Health PolicyCommittee strongly opposed
Stakeholder influence-Position-No. of licensees-Political action committeecontributions forrespective session
Supporting:-Michigan Physical TherapyAssociation, 6,765 licensees,$6,928
Opposed:-Michigan State Medical Society,32,554 licensees, $473,679
-Michigan Orthopedic Society,6,660 Licensees, $10,600
-Michigan Association ofChiropractors, 2,756 licensees,$59,725
Supporting:-Michigan Physical TherapyAssociation, 7,011 licensees,$12,190
Opposed:-Michigan State Medical Society,29,784 licensees, $169,815
-Michigan Orthopedic Society,6,260 licensees, $13,850
-Michigan Association ofChiropractors, 2,817 licensees,$66,620
Supporting:-Michigan Physical TherapyAssociation, 7,616 licensees, $11,995
Opposed:-Michigan State Medical Society,30,687 licensees, $199,748
-Michigan Orthopedic Society, 6,409licensees, $21,884
-Michigan Association ofChiropractors, 2,921 licensees,$70,120
a HB!Michigan House Bill, SB!Michigan Senate Bill, DPT!Doctor of Physical Therapy, PTA!physical therapist assistant, DA!direct access,CPR!cardiopulmonary resuscitation.
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 241 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

Table 2.Available Articles About Direct Access During the 2005–2006 Legislative Session
Author/Year Key Findings
Access
Durant et al, 198920 83% of patients attending 1 of 25 outpatient clinics in Indiana were supportive ofdirect access
Domholdt and Durcholz, 199222 Up to 10.3% of patients accessed physical therapy without physician referral inNorth Carolina, Utah, and Nevada
Crout et al, 199821 Up to 8.8% of patients accessed physical therapy without physician referral inMassachusetts
Snow et al, 200119 73% of South Floridians would go directly to a physical therapist
Cost
Mitchell and de Lissovoy 199723 Compiled claim data from Maryland Blue Cross Blue Shield showed 123% lowercosts and 60% fewer visits under direct access
Quality
Davenport et al, 200531 Physician prescription lacked sufficient specificity to guide treatment and was notrelated to clinical outcome
Moore et al, 200532 Retrospective review of 50,799 patients seen under direct access showed noadverse events or episodes of litigation
James and Stuart, 197524 Demonstrated feasibility and quality of care by a physical therapist in amusculoskeletal primary care provider role in the US Army
James and Abshier, 198125 Documented the proliferation of physical therapists as musculoskeletal primary careproviders in the US Army and found that care provided was “consistent withaccepted standards of medical care”
Daker-White et al, 199926 Randomized controlled trial of consultation and management by orthopedicsurgeons and physical therapists showed no differences in patient-reportedoutcomes, satisfaction, and cost
Riddle et al, 200445 Physical therapists underestimated the probability of the presence of deep veinthrombosis 49%–86% of the time
Moore et al, 200533 Physical therapist diagnoses were highly consistent with magnetic resonanceimaging results
Childs et al, 200534 Physical therapists outperformed all physician specialty groups except orthopedicsurgeons on a standardized knowledge test for management of musculoskeletalconditions
Robert and Stevens, 199729 Case reports demonstrating the ability of the physical therapists to screen for andidentify the presence of medical disease requiring referral to the physician forfurther medical evaluation and managementGreenwood et al, 199828
Gray 199927
Cleland and Venzke, 200330
Weishaar et al, 200535
Thien-Nissenbaum and Boissonnault, 200536
Sasaki, 200537
Ross and Bayer, 200538
Garber, 200539
Asavasopon et al, 200540
Browder and Erhard, 200541
Johnson and Abrams, 200542
Mamula et al, 200544
Stowell et al, 200543
Direct Consumer Access to Physical Therapy in Michigan
242 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

due to pressure from the MichiganState Medical Society (MSMS), whichhad aggressively opposed previousattempts at increased independenceof nurse practitioners on the prem-ise that only the physician is ableto independently diagnose healthconditions and develop an appro-priate plan of care. The assertionthat there must be physician over-sight of all health care providersand the acceptance of this premiseby legislators also was evidencedin PA 264 of 2005, which resultedin Michigan becoming 1 of only 2states that prohibited physical thera-pists from independently performingneedle electromyography. The legis-lation readily passed with over a two-thirds majority vote in both cham-bers and was opposed only by theMPTA.
With regard to political party controlduring the Michigan 2001–2002 leg-islative session, Republicans domi-nated the House and Senate under aRepublican governor. Both legisla-tive sessions during the 2003–2006period were presided over by aRepublican majority House and Sen-ate under a Democratic governor.
Cultural factors. A general soci-etal perception exists of the physi-cian as the health care provider whooversees and directs health care,46
and nearly all members of societyassociate the physician with diagno-sis and treatment of disease, illness,and injury. Physical therapy is notwell known to the public. To myknowledge, there has not been anymovement by the general publiceither for or against direct access totreatment by a physical therapist.
ProcessesThe analysis of processes soughtto identify to what extent stake-holder position and level of influ-ence impacted the progress and dis-position of direct access legislationbetween 2001 and 2006. The results
of these analyses are briefly outlinedin Table 1 and are discussed below.
Bill progress and disposition. Ineach of the legislative sessions inwhich direct access was attempted,the bills were introduced andreferred to each chamber’s respec-tive health policy committee. Duringthe 2001–2002 session, HB 5014passed the House with a two-thirdsmajority vote, but then did not pro-gress any further. Analysis of theonly voting record on direct accessin Michigan revealed that that Dem-ocrats and Republicans supportedthe bill in similar proportions. Dur-ing the 2003–2004 session, a hearingfor HB 4176 was held in the HouseHealth Policy Committee, but novote was taken despite requests bythe sponsor of the bill, who was amember of the committee. Two of16 Health Policy Committee mem-bers in the House and 3 of 7 mem-bers in the Senate had voted againstdirect access in 2002. Then, duringthe 2005–2006 session, no hearing ineither chamber was even scheduledfor HB 5618. Two of 17 Health PolicyCommittee members in the Houseand 3 of 5 members in the Senatehad voted against direct access in2002. Consideration of the stake-holders’ positions and their respec-tive levels of influence was con-ducted to provide insight into thereasons why direct access legislationfailed to progress during each legis-lative session. Stakeholder position isconsidered first, followed by an anal-ysis of stakeholder influence.
Relevant stakeholders and stake-holder position. Based on the leg-islative analyses, the MPTA wasthe only stakeholder in support ofdirect access legislation during eachof the 3 legislative sessions. TheMPTA asserted that the physicaltherapist is adequately trained toperform medical screening andidentify medical disease requiringphysician referral and that despite a
physician prescription, the physicaltherapist is responsible for ensuringthat the patient’s problem is onethat is appropriate for physical ther-apy. Furthermore, the MPTA statedthat the physical therapist mustexamine the patient and determinethe nature of the patient’s prob-lem to develop an appropriate treat-ment plan regardless of whether areferral is received. Therefore, theyargued, the physician visit results inincreased cost and delay of treat-ment. The MPTA cited research andother sources that demonstratedthe cost benefits of direct accessand the fact that there was noincrease in malpractice claims47 orvariations in liability insurance pre-miums between states with andwithout direct access48 and that themajority of other states permit directaccess. Regarding the requirementthat applicants for initial licensurehave the Doctor of Physical Therapydegree starting in 2009, the MPTAexpressed preference that the datebe changed to 2019, but there wasno indication of opposition to thisprovision by physical therapists’ orphysical therapy practices in the leg-islative analyses.
The MSMS and the MichiganOrthopedic Society offered 3 corearguments: threat to the physician–physical therapist relationshipwithin the health care team,increased utilization and cost, andpublic safety. They argued thatwithout the ability to diagnose med-ical disease, physical therapists areunable to safely decide on the natureor cause of the problem to be treatedand that there is a risk that seriousunderlying medical disease will notbe appropriately recognized andmanaged. The MSMS rejected theassertion that physical therapists aresufficiently trained to identify andmanage musculoskeletal problemsamenable to physical therapy treat-ment and that physical therapistscan effectively screen for conditions
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 243 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

not appropriate for physical therapyand make appropriate referrals. TheMSMS speculated that the reasonthere was no difference in liabilityclaims in states with direct accesswas that patient harm was notreported, but they offered no data tosubstantiate this conclusion. TheMichigan Chiropractic Society alsowas opposed to direct access, but nospecific arguments could be attrib-uted to their organization based onthe legislative analyses.
Although third-party payers werenot identified as having taken a posi-tion on direct access, the legislativeanalyses identified concerns aboutincreased health care cost and itsimpact on employers offering healthcoverage to their employees. There-fore, additional information wassought to determine how third-partypayers may have perceived directaccess. Blue Cross Blue Shield ofMichigan (BCBSM) Provider ClassPlan Summaries (biennial summariesof enrollment and cost data for reha-bilitation providers) reflect the orga-nization’s position on direct accessby stating that the requirement forphysician prescription and approvalof treatment plans for physical ther-apy services provided an effectivemechanism for controlling “costsassociated with unnecessary utiliza-tion.”49 No data were presented inthe summaries to substantiate thatconclusion. Additionally, the posi-tion of numerous third-party payers,including BCBSM, is representedby the Economic Alliance for Michi-gan (EAM), whose members believethat scope of practice expan-sions, including direct access tophysical therapy services, resultsin decreased quality of care andincreased costs.50 Although BCBSMand the EAM did not go on record inopposition to direct access legisla-tion, it was commonly understoodthat these organizations informallyexpressed concern about changes inscope of practice and the associated
fiscal impact (Bret Marr, TerryVanderveen; personal communica-tion; February 14, 2011).
Stakeholder influence. For thepurposes of this analysis, stakeholderinfluence was measured in terms ofPAC contributions. Table 1 outlinesthe financial political campaign con-tributions by the primary stakehold-ers. The opponents of direct accesswere in a position of considerablygreater influence than the MPTA,which was the sole advocate fordirect access.
During the analysis of processes,additional possible methods of stake-holder influence were noted. Twolegislators, both of whom were phy-sicians, may have played key roles inthe ultimate disposition of each leg-islative effort. During the 2001–2002session, the senate companion bill(SB 620) was sponsored by a senatorwho was also a physician and mem-ber of the Senate Health Policy Com-mittee. The second physician legis-lator served on the House HealthPolicy Committee during 2001–2002, then on the Senate HealthPolicy committee 2003–2006, andhad expressed strong opposition todirect access in a 2008 interview.51
This interview was the only newsmedia article found related to directaccess in Michigan.
DiscussionThe present analysis of several leg-islative attempts to allow directconsumer access to treatment byphysical therapists in Michiganconsidered the proposed policycontent, context, and legislativeprocesses that may have resultedin its failure to be adopted. Suchan analysis might inform futureattempts to implement direct accessin Michigan.
The 2 primary issues debated by thesupporters (the MPTA) and oppo-nents (physician groups) of direct
access were cost and safety. Physi-cian opponents argued that directaccess would jeopardize cost andsafety, but offered no evidence tosupport their position. Although noton record as opposed, the opposi-tion of third-party payer groups todirect access is without supportingdata as well. In contrast, the MPTAargued that research evidence sup-ports direct access with regard toboth cost and safety. Indeed, duringthe 2001–2006 time period, therewas a progressive increase in theresearch evidence supporting thesafety of direct access and anincrease in the number of states per-mitting direct access. However, theprogress of direct access legisla-tion in each legislative session wasprogressively less. Compared withthe nearly successful initial attemptduring 2001–2002, the 2005–2006attempt (HB 5618) did not evenreceive a hearing. This failure isironic because HB 5618 was muchmore conservative and placednumerous limitations on the circum-stances in which a physical therapistcould treat a patient under directaccess. In addition to these compro-mises with opponents, there were27 published articles refuting claimsthat direct access results in increasedcost and risk to patients, and directaccess was the prevalent pattern ofpractice in the United States. Thereason why direct access legislationmade no progress in 2005–2006 isunclear. However, the use of a com-prehensive policy analysis frame-work provides insight into the otherfactors that may have resulted inrepeated failures in direct access pol-icy adoption.
Several prominent contextual andprocess-related barriers to policyadoption became apparent afterconducting this analysis: (1) a lim-ited constituency supporting directaccess with regard to number of indi-viduals and their political influence,(2) a perception that only the physi-
Direct Consumer Access to Physical Therapy in Michigan
244 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

cian can independently diagnose andtreat patient problems, and (3) legis-lators in positions of power whooppose a bill.
First, with regard to a limited constit-uency, it would have been difficultfor legislators to see the potentialbenefit of direct access for Michi-gan’s citizens when only a relativelysmall group of individuals with lim-ited exposure (as measured by PACcontributions) were in support ofdirect access. Although PAC contri-butions may not directly influencelegislator activity or voting, financialcontributions, especially for attend-ing fund-raising events, do provide agreater amount of exposure to thelegislator during which the stake-holder’s views can be communi-cated (Bret Marr, Terry Vanderveen;personal communication; Febru-ary 14, 2011). This exposure is espe-cially important in states such Mich-igan that have term limits. Michiganlegislators are limited to 6 years inthe House and 8 years in the Senate.These term limits result in a heavyreliance by political parties and theircandidates on constant fund-raisingdue to the frequent turnover in eachdistrict, with significantly fewerelections that have well-established,long-term incumbents. Thus, thisconstant fund-raising increases theinfluence of lobbyists and their asso-ciated PACs. Furthermore, there isa shift of corporate, institutionalknowledge from legislators with rel-atively short tenures to relativelylong-term lobbyists (Bret Marr, TerryVanderveen; personal communica-tion; February 14, 2011).
Although the present analysis did notallow for quantification of grassrootsmember mobilization and activity, itis clear that consumer groups, third-party payers, policy experts, andother health care professionals werenotably absent in the efforts to pro-mote the adoption of direct access. Itis tempting to speculate that the pro-
vision requiring the Doctor of Phys-ical Therapy degree for initial licen-sure may have been controversialwithin the physical therapy commu-nity and, therefore, may have limitedgrassroots support and mobilization.However, all programs in Michiganwere expected to graduate studentswith the doctoral degree by 2009,and there was not any indication inthe legislative analyses that therewas dissent within the physical ther-apy community. Furthermore, thisprovision was included in the pro-posed legislation during each of the3 attempts and, therefore, does notaccount for the disparate progressmade in 2001–2002 compared with2005–2006.
With regard to the perception thatthe physician must direct and over-see all other health care providers,it is difficult to overcome physi-cian arguments that warn of patientharm if other health care providerswere to function autonomously. Theintent of the public health code is toensure the protection of the public,and the burden of proof is on theproponents of change to demon-strate that patient safety would notbe jeopardized. There was a consid-erable increase in the research evi-dence against the opponents’ claimsduring the 2001–2006 period, but itappears that the research evidenceavailable at the time was insufficientor was not adequately communi-cated to legislators to overcome theopponents’ arguments. Although it isnot possible to know which articles,if any, were considered by legisla-tors, the Michigan House and Senatelegislative analyses noted that theproponents of direct access citedliterature supporting the impact ofdirect access on cost, access, andquality. It also is not known howeffectively the MPTA’s grassrootsefforts were in communicating thisresearch evidence.
Additional barriers that prevented alimited constituency’s ability to over-come physician opposition includedthe failure of federal legislation seek-ing to allow direct access underMedicare and other state-level legis-lation reinforcing the perceptionthat the physician should direct andoversee physical therapy treatment.Given that federal legislators choseto not permit direct access to physi-cal therapy for Medicare beneficia-ries, state legislators may have beenmore reluctant to adopt a similar pol-icy at a state level. It should benoted, however, that several otherstates over that time period adopteddirect access despite this federalprecedent. Alternately, state-levellegislative precedents may have hada greater impact during the 2005–2006 Michigan legislative session.Legislators’ perceived need for phy-sician oversight of physical therapyservices may have been reinforcedby permitting physician assistants toprescribe physical therapy under aphysician’s supervision, eliminatingthe ability of physical therapists toperform needle electromyography,and not adopting legislation thatwould permit nurse practitioners toindependently prescribe physicaltherapy. Although these bills werenot considered during the 2001–2004 period, they may be reflectiveof many legislators’ perception ofthe need for physician oversight.
Although the aforementioned expla-nations are plausible, the failure ofHB 5014 during the 2001–2002 leg-islative session to continue its prog-ress and receive a hearing in theSenate Health Policy Committeeafter having passed the House with atwo-thirds majority vote is interest-ing because it suggests that theremay have been other factors unre-lated to the merits of the bill thatimpeded its progress. Possibilitiesinclude partisan conflicts, conflictsamong sponsors or other legislatorsfrom different chambers, and indi-
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 245 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

vidual biases or preferences exertedby those in leadership positions.
With regard to partisan conflicts, thevoting record in the House revealedthat it received bipartisan support,and both chambers and the gover-nor’s office were all Republican con-trolled. Thus, it is not likely that par-tisanship played a role in the failureof HB 5014 to progress.
Regarding conflicts among sponsorsor legislators from different cham-bers, there would not be any writtenrecord of such conflicts. However,no such conflicts were recalled bylobbyists familiar with the bill (BretMarr, Terry Vanderveen; personalcommunication; February 14, 2011).The fact that the sponsor of the Sen-ate companion bill to HB 5014 was aphysician and member of the SenateHealth Policy Committee shouldhave increased the likelihood thatthe bill would progress in the Senate.However, the fact that no hearingwas ever held despite requests ofthe House sponsor may indicate thathe was ultimately persuaded by theMSMS to not permit continueddeliberation about direct access(Bret Marr, Terry Vanderveen; per-sonal communication; February 14,2011).
During the 2003–2004 and 2005–2006 attempts, another physiciansenator on the Senate Health PolicyCommittee and who was stronglyopposed to direct access51 may havesignificantly influenced decisions tonot to allow deliberation on SB 1174in 2004 and may have influencedHouse leadership in 2003–2004 tonot spend time passing a bill thatwould not progress in the Senate(Bret Marr, Terry Vanderveen; per-sonal communication; February 14,2011). It should be noted that during2005–2006, 3 of the 5 Senate HealthPolicy Committee members, includ-ing the physician legislator, had pre-viously voted against direct access
in the House in 2002. With a major-ity of the committee either beingovertly opposed to direct access orhaving a history of being opposed todirect access, the House Health Pol-icy committee may have decided tonot allow a hearing on an ill-fatedbill.
In summary, there are a variety ofexplanations that could account forthe failure of direct access legislationin Michigan to be adopted during the2001–2006 period. Although it isdesirable to reach a definitive con-clusion, the cause of this failure islikely multifactorial. Furthermore,the purpose of the present analysiswas to direct future legislative effortsby identifying the most likely barri-ers to direct access policy adoption.Future attempts to remove the phy-sician prescription requirement inMichigan should consider the con-clusions provided by the presentanalysis. Grassroots efforts that effec-tively mobilize physical therapistsand physical therapist assistants toeducate their legislators about theprofession and direct access havebeen the mainstay of legislative advo-cacy in the physical therapy profes-sion dating back to the 1980s. Theadvent of online and electronicresources to identify physical thera-pists who are constituents of key leg-islators allows for more targetedmethods of communicating the mer-its of direct access. However, addi-tional strategies should be consid-ered. Advocates of direct accessshould develop a broader, moreeffective constituency of support fordirect access, directly address theroles of the physical therapist andphysician in diagnosis and patientmanagement and how they fit intohealth care reform, and considerpolitical tactics and strategies forovercoming legislators in positionsof power who oppose direct access.
First, with regard to developing abroader constituency of support, a
number of strategies can be utilized,such as facilitating a letter-writingcampaign by patients and by seekingsupport from other professionals,such as nurse practitioners andchiropractors, who may want to beable to refer patients for physicaltherapy. Additionally, increasingthe effectiveness of this constitu-ency can be accomplished throughaggressive PAC fundraising andutilizing those monies to increaseexposure to legislators through moreactive engagement in legislators’fund-raising campaigns. Increasedexposure to legislators allows for agreater opportunity to educate themabout the growing body of support-ing research evidence52–66 and pro-vide reassurance that direct accessdoes not endanger the public. Per-haps the most influential constitu-ency are legislators themselves.Finding legislators with prior posi-tive experiences with physical ther-apy who are willing to advocatefor direct access peer-to-peer isanother way to help build a broader,supportive constituency within thelegislature itself.
A second strategy that could be usedby states seeking direct access is todirectly confront the issue of diagno-sis by physical therapists and to rein-force their intent to continue collab-oration with physicians in patientcare. It should be made clear thatphysical therapists do not intend todiagnose and manage medical con-ditions that fall outside of theirscope of practice and that physicaltherapists will continue to collabo-rate with physicians and the healthcare team in the care of patients.However, confronting the issue ofdiagnosis by physical therapists andthe possible need for compromisemust be considered carefully. Forexample, 3 states currently requirethat a physician establish a diag-nosis prior to consumer access-ing physical therapy directly, andanother 7 states require that the
Direct Consumer Access to Physical Therapy in Michigan
246 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

diagnosis to be treated had beenpreviously referred to physical ther-apy by a physician. When Texasfirst gained direct access in 1991,physician opposition was removedwhen a provision requiring pre-vious physician referral to physicaltherapy was included67 (although itshould be noted that Texas is cur-rently seeking to remove this restric-tion). Other common compromisesinclude experience requirementsand time limits for patient treatmentunder direct access before a physi-cian referral is required. RhodeIsland obtained direct access withthese provisions in 1992 despite con-tinued physician opposition.68 How-ever, compromises may not resultin bill passage when there are influ-ential legislators who pose formida-ble barriers as evidenced by Michi-gan’s direct access bill in 2005–2006,which contained both of thesecompromises.
Therefore, although it is not likelythat any one constituency candirectly influence which legislatorsassume positions of power, it isimportant to consider other strate-gies that allow a bill to circumventindividual barriers. For example, itmay have been appropriate for directaccess legislation to be referred toan economic development–relatedcommittee, because there are finan-cial and business-related implicationsinherent in direct access. This strat-egy was effectively utilized by theMichigan Association of Chiroprac-tors in 2009 (PA 221) to revise theirscope of practice to include thetreatment of peripheral joints after30 years trying to overcome physi-cian opposition (Bret Marr, TerryVanderveen; personal communica-tion; February 14, 2011).69 Anotherstrategy utilized by this organiza-tion was to include language thatamended various parts of Michigan’sinsurance code that legally shieldedthird-party payers from any require-ments to pay for services that fell
within the expanded chiropracticscope. Although a similar intent wasincluded in Michigan’s previousdirect access attempts, the languagewas apparently insufficient to legallyachieve its intent. Thus, legal coun-sel or other expert consultation maybe necessary to develop languagethat will achieve the intended effect.
There are several limitations to thepresent analysis. First, it is a retro-spective analysis that relied uponpublicly available documents. Otherdocuments were not available thatmay have provided insight into otherstakeholders’ positions and a moredetailed description of the legislativedeliberations such as records ofattendance, verbal testimony, andwritten testimony from committeehearings.
Second, the reasons for whetherlegislation is heard and brought for-ward for a vote are not documentedand are likely mutlifactorial. Giventhat this analysis did not includeinterviews with representatives ofother stakeholder groups such asthe MPTA, MSMS, BCBSM, and theEAM, there may be other importantexplanatory variables that were notconsidered. Therefore, the presentanalysis required some speculationbased upon circumstantial evidenceand expert opinion from lobbyistswho were selected by the authorbased on convenience and whowere provided a draft of the col-lected data and preliminary analyses,which may have influenced theirresponses.
The third limitation of the presentanalysis is the method for determin-ing the role that research evidenceplayed in supporting the safety andcost benefits of direct access is diffi-cult, and this analysis can only offerspeculation as to what evidence leg-islators used in their deliberations.
Fourth, stakeholder influence wasdetermined by overall PAC contribu-tions for each legislative session anddid not account for the recipients ofsuch funding (eg, health policy com-mittee members), nor did the dataanalyzed allow for an estimate ofgrassroots activity. Unfortunately,electronic records of contributionsto individuals are difficult to searchand were incomplete for the periodprior to 2004, and many contribu-tions from special interest groupscome from individual contributionsfacilitated by the organization. Thus,accounting for all contributions froma given special interest is very diffi-cult and time consuming.
The fifth and most significant limita-tion is the potential for author bias.5
However, multiple sources of datawere used in the present analysis.
ConclusionsDespite an increasing number ofstates allowing direct access, severalstates continue to have provisionsthat restrict a consumer’s abilityto directly access physical therapytreatment. Removing these provi-sions may be considerably difficult.Analysis of 3 recent attempts atremoving the physician prescriptionrequirement in Michigan between2001 and 2006 with regard to con-tent, political and social context,legislative processes, and key stake-holders revealed that the success orfailure of direct access policy adop-tion is complex and multifactorial.Effectively articulating how diagno-sis is used by physical therapistsand communicating the evidencethat direct access does not result inincreased costs or decreased safetyfor the public may require: (1) alarger constituency of direct accesssupporters, including other profes-sions, consumer groups, and legis-lators; (2) a more influential con-stituency that effectively uses PACresources to gain exposure to legis-lators to communicate this evidence;
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 247 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

and (3) the creative use of legislativeprocesses and mechanisms to cir-cumvent legislators in positions ofpower who oppose direct accesslegislation.
The author thanks Kieran Fogarty, PhD,Nikola Nelson, PhD, CCC-SLP, and MaryLagerwey, PhD, RN, for their guidance,insightful comments, and suggestions forthe development of this article.
This article was completed in partial fulfill-ment of Dr Shoemaker’s pursuit of a PhD inInterdisciplinary Health Sciences at WesternMichigan University.
DOI: 10.2522/ptj.20100421
References1 Colwill JM, Cultice JM, Kruse RL. Will gen-
eralist physician supply meet demands ofan increasing and aging population?Health Aff (Millwood). 2008;27:w232–w241.
2 Congressional Budget Office. CBO’s Anal-ysis of the Major Care Legislation Enactedin March 2010. Available at: http://www.cbo.gov/ftpdocs/121xx/doc12119/03-30-HealthCareLegislation.pdf. Accessed May 9,2011.
3 Federation of State Boards of PhysicalTherapy. Jurisdictional licensure refer-ence guide. Available at: http://fsbpt.org/RegulatoryTools/ReferenceGuide/DirectAccess. Accessed March 21, 2010.
4 American Physical Therapy Association.Direct access map. Available at: http://www.apta.org/uploadedFiles/APTAorg/Advocacy/State/Issues/Direct_Access/DirectAccessMap.pdf. Accessed March 15,2011.
5 Buse K. Addressing the theoretical, practi-cal and ethical challenges inherent in pro-spective health policy analysis. Health Pol-icy Plan. 2008;23:351–360.
6 Walt G, Shiffman J, Schneider H, et al.“Doing” health policy analysis: method-ological and conceptual reflections andchallenges. Health Policy Plan. 2008;23:308–317.
7 House of Delegates stenotypist notes.Alexandria, VA: American Physical Ther-apy Association; June 1973.
8 House of Delegates stenotypist notes.Alexandria, VA: American Physical Ther-apy Association; June 1978.
9 Elliott J. Direct access and the profession’svision. Presented at: Texas Physical Ther-apy Association, Dallas/North Districtmeeting; January 25, 2011; Dallas, Texas.
10 Koski C. Regulatory choices: analyzingstate policy design. Law and Policy. 2007;29:407–434.
11 State of Michigan Public Act, 368 (1978).
12 Malone RE. Policy as product: morality andmetaphor in health policy discourse. Hast-ings Cent Rep. 1999;29:16–22.
13 Kuruvilla S, Dorstewitz P. There is no“point” in decision-making: a model oftransactive rationality for public policyand administration. Policy Sci. 2010;43:263–287.
14 Turner L. Politics, bioethics, and sciencepolicy. HEC Forum. 2008;20:29–47.
15 Walt G, Gilson L. Reforming the healthsector in developing countries: the centralrole of policy analysis. Health Policy Plan.1994;9:363–370.
16 Buse K, Dickinson C, Gilson L, Murray SF.How can the analysis of power and pro-cess in policy-making improve health out-comes: moving the agenda forward? ODIBriefing Paper No. 25. London, UnitedKingdom: Overseas Development Insti-tute; 2007.
17 Bardach E. A Practical Guide for PolicyAnalysis: The Eightfold Path to MoreEffective Problem Solving. 3rd ed. Wash-ington, DC: CQ Press; 2009.
18 Michigan Legislature Web site. Available at:http://www.legislature.mi.gov/(S(bu1pjbrhq1tkumy2urte3c45))/mileg.aspx?page!home.
19 Snow BL, Shamus E, Hill C. Physical ther-apy as primary health care: public percep-tions. J Allied Health. 2001;30:35–38.
20 Durant TL, Lord LJ, Domholdt E. Outpa-tient views on direct access to physicaltherapy in Indiana. Phys Ther. 1989;69:850–857.
21 Crout KL, Tweedie JH, Miller DJ. Physicaltherapists’ opinions and practices regard-ing direct access. Phys Ther. 1998;78:52–61.
22 Domholdt E, Durchholz AG. Direct accessuse by experienced therapists in stateswith direct access. Phys Ther. 1992;72:569–574.
23 Mitchell JM, de Lissovoy G. A comparisonof resource use and cost in direct accessversus physician referral episodes of phys-ical therapy. Phys Ther. 1997;77:10–18.
24 James JJ, Stuart RB. Expanded role forthe physical therapist: screening musculo-skeletal disorders. Phys Ther. 1975;55:121–131.
25 James JJ, Abshier JD. The primary evalua-tion of musculoskeletal disorders by thephysical therapist. Mil Med. 1981;146:496–499.
26 Daker-White G, Carr AJ, Harvey I, et al.A randomized controlled trial: shiftingboundaries of doctors and physiothera-pists in orthopaedic outpatient depart-ments. J Epidemiol Community Health.1999;53:643–650.
27 Gray JC. Diagnosis of intermittent vascularclaudication in a patient with a diagnosisof sciatica. Phys Ther. 1999;79:582–590.
28 Greenwood MJ, Erhard RE, Jones DL. Dif-ferential diagnosis of the hip vs. lumbarspine: five case reports. J Orthop SportsPhys Ther. 1998;27:308–315.
29 Robert G, Stevens A. Should general prac-titioners refer patients directly to physi-cal therapists? Br J Gen Pract. 1997;47:314–318.
30 Cleland JA, Venzke JW. Dermatomyositis:evolution of a diagnosis. Phys Ther. 2003;83:932–945.
31 Davenport TE, Watts HG, Kulig K, ResnikC. Current status and correlates of physi-cians’ referral diagnoses for physical ther-apy. J Orthop Sports Phys Ther. 2005;35:572–579.
32 Moore JH, McMillan DJ, Rosenthal MD,Weishaar MD. Risk determination forpatients with direct access to physicaltherapy in military health care facilities.J Orthop Sports Phys Ther. 2005;35:674–678.
33 Moore JH, Goss DL, Baxter RE, et al. Clin-ical diagnostic accuracy and magnetic res-onance imaging of patients referred byphysical therapists, orthopaedic surgeons,and nonorthopaedic providers. J OrthopSports Phys Ther. 2005;35:67–71.
34 Childs JD, Whitman JM, Sizer PS, et al. Adescription of physical therapists’ knowl-edge in managing musculoskeletal condi-tions. BMC Musculoskelet Disord. 2005;6:32.
35 Weishaar MD, McMillian DM, Moore JH.Identification and management of 2 femo-ral shaft stress injuries. J Orthop SportsPhys Ther. 2005;35:665–673.
36 Thein-Nissenbaum J, Boissonnault WG.Differential diagnosis of spondylolysis ina patient with chronic low back pain.J Orthop Sports Phys Ther. 2005;35:319–326.
37 Sasaki M. Cervical cord compression sec-ondary to ossification of the posterior lon-gitudinal ligament. J Orthop Sports PhysTher. 2005;35:722–729.
38 Ross MD, Bayer E. Cancer as a cause of lowback pain in a patient seen in a directaccess physical therapy setting. J OrthopSports Phys Ther. 2005;35:651–658.
39 Garber MB. Diagnostic imaging and differ-ential diagnosis in 2 case reports. J OrthopSports Phys Ther. 2005;35:745–754.
40 Asavasopon S, Jankoski J, Godges JJ. Clin-ical diagnosis of vertebrobasilar insuffi-ciency: resident’s case problem. J OrthopSports Phys Ther. 2005;35:645–650.
41 Browder DA, Erhard RE. Decision makingfor a painful hip: a case requiring refer-ral. J Orthop Sports Phys Ther. 2005;35:738–744.
42 Johnson MP, Abrams SL. Historical per-spectives of autonomy within the medicalprofession: considerations for 21st cen-tury physical therapy practice. J OrthopSports Phys Ther. 2005;35:628–636.
43 Stowell T, Cioffredi W, Greiner A, ClelandJ. Abdominal differential diagnosis in apatient referred to a physical therapyclinic for low back pain. J Orthop SportsPhys Ther. 2005;35:755–764.
44 Mamula CJ, Erhard RE, Piva SR. Cervicalradiculopathy or Parsonage-Turner syn-drome: differential diagnosis of a patientwith neck and upper extremity symptoms.J Orthop Sports Phys Ther. 2005;35:659–664.
Direct Consumer Access to Physical Therapy in Michigan
248 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

45 Riddle DL, Hillner BE, Wells PS, et al. Diag-nosis of lower-extremity deep vein throm-bosis in outpatients with musculoskel-etal disorders: a national survey study ofphysical therapists. Phys Ther. 2004;84:717–728.
46 Starr P. The Social Transformation ofAmerican Medicine. New York, NY: BasicBooks; 1982.
47 Lane M. Vice President of ProfessionalStandards and Assessment of Federation ofState Boards of Physical Therapy letter tothe American Physical Therapy Associa-tion; 2006.
48 Loughran MJ. Senior Vice President ofHealthcare Providers Service Organizationletter to the American Physical TherapyAssociation; 2006.
49 Rehabilitation Therapy Provider ClassPlan Annual Report. Provider Class Anal-ysis Dept, Regulatory Affairs Division;1990–2008.
50 EAM Brief. HB 4603: Expanding scope ofpractice to physical therapists. Novi, MI:Economic Alliance for Michigan; 2011.
51 Stevens L. Therapists question referrallaws. Business Review Western Michigan.May 01, 2008.
52 Holdsworth LK, Webster VS, McFadyenAK. What are the costs to NHS Scotlandof self-referral to physiotherapy: results ofa national trial. Physiotherapy. 2007;93:3–11.
53 Holdsworth LK, Webster VS, McFadyenAK. Are patients who refer themselvesto physiotherapy different from thosereferred by GPs: results of a National Trial.Physiotherapy. 2006;92:26–33.
54 Leemrijse CJ, Swinkels CS, Veenhof C.Direct access to physical therapy in theNetherlands: results from the first year incommunity-based physical therapy. PhysTher. 2008;88:936–946.
55 Brooks G, Dripchak S, Vanbeveren P, Alla-ben S. Is a prescriptive or an open referralrelated to physical therapy outcomes inpatients with lumbar spine-related prob-lems? J Orthop Sports Phys Ther. 2008;38:109–115.
56 Sandstrom R. Malpractice by physical ther-apists: descriptive analysis of reports inthe National Practitioner Data Bank publicuse data file, 1991–2004. J Allied Health.2007;36:201–208.
57 Boissonault WG, Badke MB, Powers JM.Pursuit and implementation of hospital-based outpatient direct access to physicaltherapy services: an administrative casereport. Phys Ther. 2010;90:100–109.
58 Leerar PJ, Boissonnautt W, Domholdt E,Roddey T. Documentation of red flags byphysical therapists for patients with lowback pain. J Man Manip Ther. 2007;15:42–49.
59 Cark DE. Screening for Medical Referral:Attitudes, Beliefs, and Behaviors of Phys-ical Therapists with Greater than 10Years Experience [dissertation]. Birming-ham, AL: University of Alabama; 2007.
60 Jette DU, Ardleigh K, Chandler K, McSheaL. Decision-making ability of physicaltherapists: physical therapy interventionor medical referral. Phys Ther. 2006;86:1619–1629.
61 Crowell MS, Gill NW. Medical screeningand evacuation: cauda equina syndrome ina combat zone. J Orthop Sports Phys Ther.2009;39:541–549.
62 Mintken PE, Boyles RE. Tarsometatarsaljoint injury in a patient seen in a direct-access physical therapy setting. J OrthopSports Phys Ther. 2009;39:28.
63 Neilson B, Boyles, RE. Osteochondraldefect of the medial femoral condyle.J Orthop Sports Phys Ther. 2009;39:490.
64 VanWye WR. Patient screening by a phys-ical therapist for nonmusculoskeletal hippain. Phys Ther. 2009;89:248–256.
65 Mechelli F, Preboski Z, Boissonnault WG.Differential diagnosis of a patient referredto physical therapy with low back pain:abdominal aortic aneurysm [erratum in:J Orthop Sports Phys Ther. 2008;38:648]. J Orthop Sports Phys Ther. 2008;38:551–557.
66 Sebastian D. Triangular interval syndrome:a differential diagnosis for upper extremityradicular pain. Physiother Theory Pract.2010;26:113–119.
67 Horn J. Texas becomes 25th state toapprove direct access. PT Bulletin. 1991;6:28–39.
68 Winter K. Rhode Island becomes 28thstate to legislate direct access to PT. PTBulletin. 1992;7:38, 39, 41.
69 Ahern LK. New rules let Michigan chiro-practors expand services. Lansing StateJournal. February 14, 2011.
Direct Consumer Access to Physical Therapy in Michigan
February 2012 Volume 92 Number 2 Physical Therapy f 249 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

Appendix.Lobbyist Consultation Topics
Recollection of direct access legislation
General impression of stakeholders’ positions:
—Physician groups (Michigan State Medical Society, Michigan Orthopedic Society)—Chiropractors—Blue Cross Blue Shield of Michigan—Economic Alliance for Michigan—Michigan Physical Therapy Association
General impression of legislators’ views on direct access and apparent loyalties to health care special interest groups
Potential factors that impeded the progress of direct access legislation:
—Stakeholder influence and the interaction of political action committee contributions and term limits—Legislative processes, including:
—Party control—Coordination of legislation (or conflicts) between chambers—Insights regarding health policy committee chair position on direct access, as well as potential external
influences or pressure—Health policy committee composition—Bill sponsorship
Direct Consumer Access to Physical Therapy in Michigan
250 f Physical Therapy Volume 92 Number 2 February 2012 at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from

doi: 10.2522/ptj.20100421Originally published online October 27, 2011
2012; 92:236-250.PHYS THER. Michael J. ShoemakerMichigan: Challenges to Policy AdoptionDirect Consumer Access to Physical Therapy in
References
http://ptjournal.apta.org/content/92/2/236#BIBLfor free at: This article cites 51 articles, 15 of which you can access
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtmlInformation for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
at APTA Member on February 2, 2012http://ptjournal.apta.org/Downloaded from












![Water shortage[1]](https://img.dokumen.tips/doc/110x75/556132e4d8b42a263b8b46da/water-shortage1.jpg)