Embed Size (px)
Citation preview

Older People in Acute Care Collaborative Evaluation
Pat O’Connor, Clinical Director R&D, NHS Tayside


Shetland
Grampian
Highland
WesternIsles
Borders
Fife
Lothian
GreaterGlasgow Clyde
Ayrshire & Arran
Orkney
Forth Valley
Lanarkshire
Dumfries &Galloway
Scotland’s Pop. 5.1 million
14 health Boards 150,000 staff
Tayside
And 7 Special Boards
NHS24NHS Education ScotlandNHS Health ScotlandNHS Healthcare Improvement Scotland Scottish Ambulance ServiceState HospitalNational Waiting Times Unit

Challenges
Increase in the elderly population NHS Tayside 60-70% of inpatients are over 65
Acute hospital care not set up or designed specifically for the elderly
Poor experience data older people and their carers of hospital care Patient population: 60-70% over 65 years 50% over 75 years 15-20% over 85 years

AimTo improve the experience of older people in acute care through the delivery of a person centred approach byNovember 2013
Goals:
• 95% of patient satisfaction scores are excellent
• 300 days between formal complaints
• 95% of appropriate patients receive a standardised screening

Public
• Mrs V died aged 80 in hospital on December 2008. Following her death an independent doctor (psychiatrist) raised concerns regarding aspects of Mrs V's care with the Mental Welfare Commission, in particular, her lack of nutrition during a sustained period.

Government Level • Improving the assessment of people who might
have dementia who are admitted to hospital; • Improving patient information systems• Patient centred -about the person, including their
likes, dislikes and routines; • Reducing unnecessary admissions of people
with dementia; facilitating timely discharge; • Better assessment, treatment and management
in hospital of frail elderly people• Improving access to telecare, intermediate care
services and re-ablement.

IHI Breakthrough Series
Select Topic (Develop Mission)
Planning
Group
Develop Framework & Changes
Participants
(14 Teams)
Prework
LS 1June 2012
P
S
A D
LS 3May 2013
LS 2January
2013
Expert Meeting
AP1 AP2 AP3
Holding the Gains
P
S
A D
P
S
A D
LS4December
2013

NHS Tayside/NHS Grampian Older People In Acute Care Collaborative
AimPerson centred assessment & plan of care by the multidisciplinary team
Delivery of patient family centred care
Collaborative multidisciplinaryteam and person centred Culture
Leadership framework to support improvement progress
To improve the experience of olderpeople in acutecare through the delivery of a person centred approach byNovember 2013
Goals:
1. 95% of patient satisfaction scores are > 4
2. 300 days between formal Complaints
3. 95%patients receive a standardised screening
Screening tool Reliable comprehensive assessment:
• Medical health (e.g. medicine reconciliation)• Functioning• Psychological• Social function
Risk identification
Increase family and carer involvement in careReview revise environment of care Optimise use of volunteer services
Promote open communication among MDT, patients, carers and familiesOptimise efficiency in handoffs and discharge process Promote use of patient, family, carer feedback to improve care Equip staff with the appropriate knowledge and skills to care for patients with dementia
Develop infrastructure to support teams QI workProvide oversight of collaborativealign position collaborative with widerorganisational agenda Develop infrastructure to work in partnership with teams across NHS Tayside and NHSGrampian

s

Collaborative Model
Ward Team leadPatient and carer
MedicalNursing
PharmacySupport services
PortersVolunteers
Leadership group Medical DirectorNurse Director
CEO Senior Manager
Dedicated locally developed change package of interventions

Evaluation
Aim
To critically evaluate the of the implementation of the older peoples collaborative in NHS Tayside
Mixed methods case study • Analysis of design and implementation plans and
arrangements -: local structure, minutes, actions and, reflective diaries
• Participation and observation in learning sets • Focus group and semi structured interviews with Tayside
attendees of learning sets (n= 70)• Analysis of measurement data recorded by frontline staff

Research Questions
• Is the programme or intervention in place reaching the people as intended?
• What are the challenges to implementing the programme?
• What appears to be working so far? • How satisfied are people with the delivery of the
intervention services? • What do they like most, and what are they concerned
about? • Cost and value considerations?• Leaders and mainstream managers views of OPAC?

Evaluation
– Being present, and seeing staff in action– Conducting the interviews with the teams – Listening to contributions that people were able
and willing to make in terms of their work and responsibilities
– Hearing the openness with which people spoke about their work and the Older People and thier families in their care
– Learning about some of the examples/innovations developed in response to OPAC

Staff Interviews
• “Something about this method(PDSA and collaboration for learning) that works”
• “Better communication” • “Improved environment” Large clocks coloured doors
picture signs toilet etc• “Improved handover”• “Faster and more complete patient assessments for our
most vulnerable patients” • “We’re making it better form the inside out”

Enhancing Care
– Cutting meal distribution down from 1½ hours to 12 minutes
– Weighing Older Persons on admission then settling them into bed rather than vice versa
– Domestic and Auxiliary Staffs’ role in risk assesment and safety briefing assisting Older Persons’ hydration and in pre-meal hand washing
– Increased use of “This is Me” and Butterfly Scheme

The Butterfly Schemereaching out to people with dementia

Planned Date of Discharge (PDD)
Synchronised PDD
0
20
40
60
80
100
120
Jun Jun Jul Jul Aug Aug Sep Sep Oct Oct Nov Nov Dec Dec Jan Jan Feb Feb
Pe
rce
nta
ge
PDD admission
synchronised PDD
Safety / patient info boards



OPACC – Ward Information Board

AMUPercentage of patients screened using a standardised screening tool
85
65
0
80
55 55
20
6965
70
85 85
9590 90
0
10
20
30
40
50
60
70
80
90
100Poster highlighting importance of screening for patients > 75 years of age on wall.
New nursing staff.
Education for nursing staff by by Senior Charge Nurse and Nurse Consultant

Arbroath-% of patients who have received an initial screening for a SAM assessment
0
10
20
30
40
50
60
70
80
90
100
43.47826087
64.9122807
82.6086956575.6756756799
998
63.8888888960
65.90909091
75
90.90909091
Less prompting from pharmacy staff
introduced screening form for self admin of medications
review of form
Embedded in clerk in document
Results shared with nursing staff so more on board
Team joins OPAC and starts testing
Testing 1-3-5 patients

MDT-Staff Involvement in Safety Briefs
15/0
7/20
13
22/0
7/20
13
29/0
7/20
13
05/0
8/20
13
12/0
8/20
13
19/0
8/20
13
26/0
8/20
13
02/0
9/20
13
09/0
9/20
13
16/0
9/20
13
23/0
9/20
13
30/0
9/20
13
07/1
0/20
130%
10%20%30%40%50%60%70%80%90%
100%
Nursing attendance Support Services OT
Weekly
Taped handover introduced including safety brief
Whiteboard-symbols introduced
Domestic support symbols introduced for safety brief

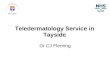
5 Wards are more than 300 days since their last complaint, one achieving > 500. All show improvement.
Jul-1
2
Aug
-12
Sep
-12
Oct
-12
Nov
-12
Dec
-12
Jan-
13
Feb
-13
Mar
-13
Apr
-13
May
-13
Jun-
13
Jul-1
3
Aug
-13
Sep
-13
Oct
-13
Nov
-13
Dec
-13
0
100
200
300
400
500
600
Ward 213
AMIA
Ward 110
Ward 102
Ward 7 DGH
Ward 11/303
Ward 12/304
Ward 209
Nu
mb
er o
f d
ays
sin
ce la
st c
om
pla
int
300 Days
543 Days
389Days
403 Days

Staff Feedback • “it’s brought back some of the personal elements”• “[it allows us] to take action rather than create action
plans”• “it provides an opportunity for deep reflection”• “support has been phenomenal”• “enjoying patient interaction”• “the [Ward] is relentlessly busy and…it’s difficult to step
back and consider BUT the collaborative has provided a structure for reflection on quality”
• “[we have] more sense of worth [as] part of the team”• “[we’re] seeing barriers breaking down”• “we can incorporate each other’s ideas”• “it’s infectious!”

How much did it cost?
• Local collaborative accommodation for learning sets
• Staff time out cost per day
• Additional funding for local environment and signage improvements £35K
• Evaluation £10K
Staff member Cost
Consultant £410.92
Pharmacist £195.88
Senior Charge Nurse £164.17
Physiotherapist £137.08
Staff Nurse £109.37
Nursing Assistant £71.60
Porter £71.60
Domestic £65.95

Conclusions
• Some evidence of improvement in all participating wards
• High level of patient experience scores in participating ward areas
• Sense of purpose and team vitality for participating staff groups
• Action oriented programme of work • Real ‘can do’ attitude for change and
improvement

Conclusions cont.
• Understanding of the programme and collaborative goals not widely understood senior leadership.
• Sustained change not yet evident in all areas for the goals set
• Some Middle and Senior managers often felt left out of the main stream collaborative work

The work continues
• Older peoples implementation groups operational changes at scale integrated health and social care
• More cohesive and inclusive approach
• Team vitality been maintained (pic) Quality award

Table Exercise
Find at your tables large post-it notes – some yellow, some blue – and take some of each color
Using the post-it notes, answer the following questions:– On the yellow post-it notes: What am I doing that is like this?– On the blue post-it notes: What would we like to do that
incorporates this idea and moves it forward?
At the break, place your post-it notes the driver diagram so people can walk around and read them