Embed Size (px)
Citation preview

QUALITY OF LIFE OF COMMUMTY-DWELLING, OLDER PERSONS THE CNnLIENCE OF OPTIMISM, SELF-EFFKACY, AND SOCIAL SWPORT
by Elisabeth J. Wheab le
Faculty of Nursing
Submîtted in partial fùltillment of the requirements for the degree of
Master of Science in Nurshg
FacuIty of Graduate Studies The University of Western Ontario
London, Ontario June i997

- Nationa L Libmry BibMh' u s nationale a du Cana a
Acquisitions and Acquisitions et Bibliograp hic Semices setvices bibliographiques 395 Weliïngton Street S, rue Wellington Ottawa ON K1AONQ ûttawaON K1AON4 Canada Canada
The author has granted a non- exclusive licence ailowing the National Library of Canada to reproduce, loan, distri'bute or seli copies ofthis thesis in microform, paper or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the thesis nor substantial extracts fiom it may be printed or othmCse reproduced without the author's penmission.
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque nationale du Canada de reproduire, prêter, distri'buer ou vendte des copies de cette thèse sous la forme de microfiche/fh, de reproduction sur papier ou sur format électronique.
L'auteur conserve la propriété du droit d'auteur qui protège cette thése. Ni la thèse ni des edts substantiels de celieai ne doivent être imprimés ou autrement reproduits sans son autorisation.

AB STRACT The purpose of this study was to examine the relationships among quality of Iife,
dispositionai optimism, self-efficacy, and perceived social support for comrnunity-
dwelling, older persons. The relationships arnong personai characteristics, health and the
primary study variables were also examined. Carver and Scheier's (1982) mode1 of
behavioural self-regulation provided the conceptuai frarnework for this descriptive
correlational study of 39 women aged 65 years and older. Quality of life was correlated
positively with dispositional optimism (1 = 3 3 to .65) and with perceived social support
(r = .36 to .4 1). In addition, subjects who were more optimistic reponed greater
adequacy of perceived support (1 = -3 8). The impact that heaith had on daily activities
was associated with lower quality of life (E= 4.0 to 7.0) and the number of health
problems was associated with lower optimism (1 = -.32). Generdized self-efficacy was
not associated with any variable. Greater understanding of the quaiity of Iife of older
persons and its correlates can help nurses become better prepared to meet their needs.

DEDICATION
This thesis is dedicated to the women who gave of their time and of themselves to
be part of this research study.
1 wish 1 could
gather the
woman essence
I have met here
into a small, beautitiilly
crafted basket
and take it home
with me-
To have in that basket
aii the wisdom and tmth saying
1 have heard here-
An essence to draw on, to bathe in
and to l e m fiorn-
Rather though-
t will take with me
a few words, many miiles
and glimpses of
sparkiing, knowhg eyes.
Mary Martha Muck
The Enduring Spint Conference
Apd, 1995

t would like to acknowledge and thank severai peopie who supported me through
the completion of this endeavour. First of dl, t would like to thank my chief advisor,
Dr. Janet lefiey, for her wisdom, caring and support throughout this project. Her
patience and sense of humour, dong with her extensive knowledge of nursing research
were instrumentai in assisting me to finish this work. Thank you ako, to Elsie McMaster
for her timely feedback and encouragement.
I would also like to thank my family for their ongoing encouragement and love.
Special thanks to my husband, Alan, for his gentle hints, his computer knowledge, and
constant support. Thank you to my daughter Remy, €or her enthusiastic help in searching
out library resources and her attention to detail. Thank you to my son Robert, for his
knowledge of the workings ofe-mail, and his patient attempts to teach his "old" mother
new cornputer skiIis. Thank you to my son Geo$ for his timely words of wisdom and for
building me my own computer. Also, thank you to rny mom and dad for their ongoing
support and for "just iistening".
Recognition must go as well to all of my colleagues at work who patiently saw
me through the tuid days. Thank you for your help and much needed suppon.

TABLE OF CONTENTS
CERTZFICATEOFEXAMINATION~~~~..~~~~..~..~ .. * . . * .w* * * * . * * ABSTRACT .................................................. DEDICATION ................................................ ACKNOWLEDGMENTS ........................................ TABLE OF CONTENTS ........................................ LISTOFTABLES .......m..D.................................. LIST OF FIGURES . . . . . . . . . . . . . .m. . . . . . . . . . . . . . . . . . . . . . . . . . . . . LIST OF APPENDICES ......................................... CHAPTERI -INTRODUCTION ..........m......................
1 . Purpose ........................................... 2 . Significance of the Study ................................
................................. 3 . Conceptual Framework Application of the Conceptual Frarnework to the Study ....
4 . Research Questions ...........................CD...C.. Definition of Terms ..............................
................................ Quality of Life ........................ Dispositional Optimism
................................ SeEEfficacy Perceived Social Support ....................... Persona1 Characteristics ........................
...................................... Kealth Community-Dwelling Older Persons ...............
5 . Assumptions ......................................... CHAPTERIC -REVIEWOFTHELITERATURE ....m...........mm..
....................................... . 1 QualityofLife Quality of Life and Keafth .......................... Quality of Life and Personal Characteristics ............. Summ ary ........................................
2 . Dispositional Optirnism ................................. Optirnism and Quality of LXe ................... ....
Optimism and Psychological WeU-Being ........... Optimism and Heaith .............................. Optimism and Personai Characteristics .................
....................................... Summary 3 . Self-Efncacy .........................................
Self-EEcacy and Quality of LZe ...................... Self-EEcacy and Optimïsm ......................... Self-Efncacy and Health ........................... SeLf-Efficacy and Personai Characteristics ..............
....................................... Summary . ........................................ 4 Social Support
.................... Social Support and Qu* of Life ........................ Social Support and Optimism
Page . . 1 1
i i i i v
v v i i x
X
xi

Social Support and Self-Efficacy ..................... Social Support and HeaIth .......................... Social Support and Personal Characteristics ............. Summary .......................................
5 . Conclusion .......................................... CHAPTERIII -METHODOLOGY ................................
.............................................. . 1 Design 2 . Setting .............................................. 3 . Sample Design ........................................
.................................. Sample Critena Recruifment .....................................
............................... . 4 Data Collection Procedure 5. Instrumentation .......................................
........................... Background Information ......................... Health Status Questionnaire
.............................. Quality of Life Index ................................. Development
........................ Description and Sconng ................................... Reliability
..................................... Validity .............................. Life Orientation Test
................................. Development ........................ Description and Sconng
................................... Reliability Vdidity .....................................
................................ Self-Efficacy Scale ................................. Development
........................ Description and S c o ~ g ................................... Reiiability
Vaiidity ..................................... .................... Personal Resources Questionnaire
Development ................................. ........................ Description and Scoting
................................... Retiabilny ..................................... Validity
. 6 Data Analysis Plan ....................................
. ............................. 7 Protection of Human Rights
...................................... . CHAPTERIV RESULTS 1 . Personai Characteristics of CommunÏty-Dwehg OIder Persons .
.............................................. 2- Hedth ........................... Specific Kealth Problems
. .... 3 Summary ofDescriptive StatistÏcs for Major Study Vanables .............................. Quality of Life Index .............................. LifieOrÏentationTest

Self-Efficacy Scale ................................ Personal Resources Questionnaire ....................
. 4 Research Question One ................................
. 5 Research Question Two ................................ 6 . Research Question Three ............................... . 7 Research Question Four ................................ . 8 Research Question Five ................................ . 9 Research Question Six ................................. . 10 Research Question Seven ...............................
Quaiity of Life and Health .......................... Dispositional Optimism and Heaith .................... Self-Efficacy and Kealth ........................... Perceived Social Support and Kealth ..................
. I l Research Question Eight ............................... Quality of Life and Persona1 Characteristics ............. Dispositional Optimism and Personai Characteristics ...... Self-Efficacy and Personal Characteristics .............. Perceived Social Support and Personal Characteristics .....
. ........................................... 12 Summary Research Questions One to Six ....................... Research Question Seven ...........................
........................... Research Question Eight CHAPTERV .DISCUSSION ....................................
1 . Characteristics of the Sarnple ............................ Characteristics of the Subjects ....................... Prirnary Study Variables ............................
2 . Research Question One ................................ . 3 Research Question Two ................................
4 . Research Question Three ............................... 5 . Research Question Four ................................ . 6 Research Question Five ................................ . 7 Research Question Six .................................
8 . Research Question Seven ............................... . 9 Research Question Eight ...............................
LO . Limitations of the Study ................................ . I 1 hplications of the Smdy ...............................
Nursing Practice .................................. Nursing Administration ............................ Nursing Education ................................
12 . Suggestions for Future Research ......................... . 13 Su m a r y ...........................................
...... APPENDICES . . . . . . . . . . . . . . . . . . . . . . .C . . . .C .C. . . . . . . . . . . . ................................................ -CES
VITA. ...*...*........................*.........*.*...*..*.

LIST OF TABLES
Table Description
Type and Frequency of Available Help from Family and Fnends ..... Type of Health Problems and Arnount of Influence on Daily Activities
Page
54
55
Mean, Standard Deviation, and Range of Scores for the Primary Study Variables: Quaiity of Life, Dispositional O ptimism, Self-Efficacy, and Cerceived Social Support .................................. 57
Correlations among Quality of LXe, Dispositionai Optimism, Selfi Efficacy, and Perceived Social Suppon ........................ 59
Mean, Standard Deviation, and Analysis of Variance for the Primary Study Variables by Rating of Overd Health .................... 6 L
Mean, Standard Deviation, and Analysis of Variance for the Primary Study Variables by Rating of Impact of Health Problems on Daily Activities.. ............................................. 62
Mean, Standard Deviation, and t-Test for the Primary Study Variables and Maritai Status ...........m......................e..... 64
Mean, Standard Deviation, and Analysis of Variance for the Pnmary Study Variables by Level of Formal Education ....................... 65

Figure
I
LIST OF FIGURES
Description
Scheier and Carver's View of Influences on Behaviour towards ......................................... goal attainment
Adapted Conceptual Mode1 for this Study ....................
Page

LIST OF APPENDICES
Appendix
Appendix A
Appendk B
Appendix C
Appendix D
Appendix E
Appendix F
Appendix G
Appendix H
Appendix I
Appendix I
Appendix K
Appendix L
Appendix M
Appendk N
Appendix O
Quality of LXe Index ............................... Life Orientation Test ............................... SelGEfficacy Scale ................................. Persona1 Resources Questionnaire ..................... Background tnforrnation ............................ Health Status Questionnaire .......................... Information Poster .................................
Letter of Consent .................................. Combined LXe Orientation Test ....................... Approval by the University of Western Ontario Review Board For Research Involving Human Subjects ................ Permission to Use the Quality of Life index .............. Permission to Use the Life Orientation Test and Revised Life Orientation Test ................................... Permission to Use the Self-EtFcacy Scale ................
.... Permission to Use the Personai Resources Questionnaire
Page
88
92
93
94
96
97
98
99
100
101

C W T E R I
INTRODUC~ON
The quality of life of older persons living in the community has received [idle
research attention despite the fact that approximately 9 1% of al1 Canadians over the age of
65 years live in independent households in the community (Novak, 1993). Research on
the quality of life of older persons has focussed on individuals living in institutional
settings or individuals who have undergone medical or surgical treatment These studies
may not be relevant to community-dwelling, older persons (Baltes, 1994; Foreman &
Kleinpell, 1990).
Quality oflife studies of younger populations living in the community cannot be
translated to community-dwehg, older persons. Community-dwelling, older persons
form a diverse group which differs significantly from any other age group. By the time
individuals reach 65 years of age or older, they have encountered and integrated a wide
variety of lie's events. As they age, oider persons expenence many changes including:
(a) changes in social support and relationships, secondary to iliness and death; and (b) loss
of role and function, secondary to retirement and changes in physical ability. As well, the
likelihood of havhg a chronic illness with associated physical hpairments increases
sigdicantly. Approximately 85% of cornmunity-dwelling people over the age of65 years
have at least one chronic heaith problem (Osbers McGiis, DeJong & Seward, 1987).
in addition to these chronic heaith problems, there is a decüne in physical tùnction and
central nervous system tùnction includiig: (a) decrease in bone strength, (b) alteration in
mobiiity, (c) decline in sensory fùnction, and (d) reduction in reaction tirne (Staab &
Hodges 1995). In light of the rapidly Uicreasing size of the diverse population of
community-dwehg, older persons, it is important that research be conducted to provide a
better understanding of what constitutes qua@ of Ke for these individuals.
Quality of life is a comple~ multidimensional concept which has been dif?ïcult to
define and measure (Ferrans & Powers, 1992; Peariman & Uhlmann, 1991; Stewart &
King, 1994). Researchers have used a vacïety of approaches to study quality of Life
including: (a) various subjective appraisals both of life in generai and of specific
components oflife; and (b) various objective appraisds of extemai circumstances, such as

liestyle and standard of living which infer quaiity. QuaIity of Iife is iduenced by many
factors including health, fiinctiond ability, psychological welt-being, income, social
environment, aspects of personality, and availability and perception of social supports
(Larson, 1978). Given that most current research does not accurately reflect the quality of
life of most older persons and that understanding quality of life is important to determining
health care support for the older population, the aim of this study was to examine the
quaiity of Iife of community-dwellhg, older persons and factors which are related to
quality of Iife, specifically dispositional optimism, self-efficacy, and perceived social
support.
Scheier and Carver (1992) described dispositional optimism as a relatively stable
and important characteristic of personality in which individuals have a generaiized
expectancy for positive outcomes. Dispositional optimism has been found to have
beneficial effects on physical weii-being, psychological well-being, and quaiity of He, in a
variety of populations (Scheier & Carver). However, the relationship between
dispositional optimism and quaiity of lifte ofolder persons has not been studied.
SeKefficacy, the confidence which one has in oneselfto successnllly achieve a
desired outcorne, may also be iduenced by changes in health, and perceived social
support and thus seif-efficacy may be related to quaiity of life (Taal, Rasker, Seydal, &
Wiegrnan, 1993). Aithough extensive literature is available whîch iinks self-efficacy to
heaith and positive health behaviours (Allen, Becker, & Swank, 1990; OZeary, 1992;
Moore, L990; Rodin & McAvay, 1992), information about the relationship between self-
efficacy and quality of life is very limited for conununity-dweiiing, older persons.
Social support is the method by which individuals obtain materîai aid and personai
resources, such as affection, information, feedback. and encouragement, necessary for the
enhancement of life and the continuation of human development (Piazza, et al., 199 1).
Social support changes dramatically in Iater years. Major life events such as retirement,
death, loss of health or mobility, and relocation, often occur during this t h e (Kahn,
L994). A substantiai body of research has documented the importance of social support
and social networks for heaith and quality of Iife (Auslander & Litwin, 199 1; Caiiaghan
& Morrissey, 1993; Maton, 1989; Matt & Dean, 1993; Muikler & Langhauser, 1988;

Revicki & Mitchell, 1986; Thornpson, 1989; Wilcox, Kasl, & Berkman, 1994). However,
much of the research linking quaiity of life to social support has focussed on social
network size, network density, types of social support, and specific support behaviours
(Ailoway & Bebbington, 1987; Kahn, L994). Little consideration has been given to the
relationship between perceived social support and quality of Me in community-dwelling,
older persons.
Purpose
The purpose of this study was to examine the quality of life of community-
dwelling, older persons and the relationships among quaüty of life, optimism, self-efficacy,
and perceived social support. In addition, the relationships among health and the primary
study variables, quality of life, ooptimism, self-efficacy, and perceived social support, were
examined. As well, relationships arnong personal characteristics and the primary audy
variables were considered.
S ignificance of t he S tudy
Quality of life of older persons is an important concept and outcome for
gerontologicai nursing that has received little research attention. The potential
significance ofthis study is in the information gained about the relationships among older
persons' quality of We, dispositional optimism, self-efficacy, and perceived social support.
These relationships have not been examined in the community-dwelling, older population.
Monnation gained fiom this study has implications for nursing practice, nursing
education, and nursing administration.
Current geronto [ogical nursing care is prharily provider focussed and determîned
by heaith problerns, dependency, and Iongevity (Gooding, Sloan, & Amsel, 1988).
Knowledge of what quality of Ke means to older persons wüi assist nurses to provide care
that is consumer focussed rather than sirnply providing care that is medicaily or
technoiogicdy detennined. Quality of Life must be considered when planning and
hplementhg any nursing care. Quaiity of care can be provided only when qua@ of Life
is addressed by care providers (George & Bearon, 1980; Williams, 1990).
As heaith care doUars are shifted fiom hospitai care to provision of support for
older persons within their comrnunity and as the number of older persons living wÏthin the

community increases, it is essential that nursing services be designed to maintain and
promote quality of life. Nurses working with older persons in the comrnunity need to be
knowledgeable about what quality of life means tu older persons. Quality of life is often
the detennining factor which influences decisions about health care for older persons.
As people age, factors which influence the quality of their lives change in both
importance and impact (Abeles, Gift, & Ory, 1994). Determinhg what is important to
support older persons' quality of lifè will result in appropriate and effective utilkation of
nursing resources (Faden & Gerrnan, 1994; Oleson, l99Oa). identification OF factors
which support the quality of life of cornmunity-dwelling, older persons supports the
initiation ofnuning interventions direaed towards maintaining or improving that quality
of life. Identification of factors which impede individuals' quality of life can Iead to
identification of those at risk of lower quality of life. Greater awareness of factors which
place individuais at this risk could support the implementation of nursing strategies to
maintain or improve quality of Me in a timely and cost-effective manner.
In younger populations, dispositional optimism has been found to be associated
with lower levels ofpsychologîcal distress, feelings of subjective well-being, and higher
quality of life (Scheier & Carver, 1987). Ifdispositional optimism is related to quality of
Life of older persons, ident6ng individuals who have lower levels of optimism would
promote identification of individuals at risk for lower quality of We. individuals with
lower levels of optimisrn are more likely to give up on activities towards goal-attainment
than individuals with higher levels of optirnism Since Scheier and Carver believe that
dispositionai optimisrn is a relatively stable trait of personaiity, nursing interventions
wouId need to be directed toward counteracting the negative influence of lower levels of
optimism. Development and implementation of nursing interventions which wouid
support continued behaviour towards activities necessary to maintain quality of life would
be essentiai for those individuais,
Individuais with weaker self-efncacy beliefs generdy tend to put forth less effort,
persevere in activities for shorter periods of tirne, and @ive up much sooner than
individuais with stronger self-efficacy (Bandura, L982). Nurses need to assess the oIder
persons' self-efficacy For persons who demonstrate Iower Ievels ofself-etticacy, eearly

nursing interventions may increase their efficacy expectations to prevent decline in health
and quality of Iife.
Nurses must have knowledge of the sources of self-efficacy in order to develop
and implement effective nursing interventions to enhance efficacy expectations. Skills
mastery is an effective way to enhance self-efficacy. Fostenng mastery is best
accomplished by encouraging older persons to set goals for themselves in areas that are of
particulai importance to them (Gonzales, Goeppinger, & Long, L990). When nurses
encourage older individuals to set their own goals, they support incentive for action or
change. This action should promote quality of life since quality of life is determined
through subjective satisfaction with those things that are important. Nurses can aiso
promote the enhancernent of se6efficacy through: (a) provision of timely and age-
appropriate information; (b) listening to and leamhg more about older persons' beiiefs
and concerns; (c) encouraghg networking with other older persons; and (d) gentle
persuasion, which encourages individuals to believe in themselves and their abilities
(Gonzalez et al.). Quaiity of life could be maintained through nurshg interventions which
promote and support self-efficacy.
It is important that nurses gain more knowledge about the infiuence of perceived
social support on quality of We. A relationship between quality of life and social support
should prompt nurses to include assessment of older persons' social support perceptions
and neh~orks as a regular and necessary part of data collection. Consistent and
purposefiil data collection wiii support obtaùùng Uiformation which wiil be usefbl in
determinhg a plan of care specinc to the needs of the individual.
Perceived social support is amenable to change, yet nursing interventions
developed to influence sociai support have met with rnixed success. Many nursing
interventions designed to promote support for older persons have been unsuccessfiil in
achieving expected outcomes (Avom & Langer, 1982). Learning more about the
relationship between perceptions of social support and quaiity of üfe may promote
development of interventions which will meet the sociai suppoa needs of older persons.
Thus gaining information about the relationship among the four primacy study
varÎables, q u e of Hie, dispositional opnmism, self-eficacy, and perceived sociai support

for community-dwelling, older persons wü1 be of value in planning care and developing
interventions for individuals who might otherwise be at risk for declining quaiity of Iife.
Conceptual Framework
The conceptual framework used to guide this study was based on Carver and
Scheier's (1982) model of behavioural self-regdation. According to this model, al1 human
behaviour is goal-directed and controlled by an internal guidance system which is
intluenced by a process of seKregulatory feedback control. In other words, people's
actions are greatly intluenced by theu expectations or beliefs about the outcome of their
actions as weU as by past experiences, personaiity dispositions, and perceptions of
informational and environmental factors. Within this self-regulation view of behaviour,
individuals' goals and values are of central importance.
SeEreguIatory processes are continuous and have no real beginning or end.
Behaviour is continually adjusted to refiect acquisition of goals and changes in goals and
intentions. Existing conditions are compared to previously known conditions. If there is a
discrepancy between what is and what is desired then actions are directed towards
decreasing this discrepancy. Experiences are schematicaiiy organized in memory as
cognitive structures which are then used to understand, recognize, predict, and deal with
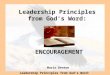
new events or activities. The model that Scheier and Carver (1987) published depicts this
behavioural self-regdation, includœmg some of the factors which influence behaviour (see
Figure 1).
Behaviour becomes ùiherentiy purposefiil or goal diected in an attempt to
correspond with reference values in memory. Behaviour continues towards the desired
goal whenever the person believes that he or she can attain the goal. Even when it
becomes very dEcult, individuais wiii continue to strive for a desired outcome or goai
when it is seen as attahable. When outcomes are seen as unattainable, attempts towards a
desired outcome are terminated,
Scheier and Carver (1987) labelied this subjective expectation of goal attaùunent
as outcome expectancy. In their view, outcome expectancy is the major detenninant in
goal attainment. Outcome expectancy is formdated tiom the individuai's evaluation or
reff ection of hidher ability to overcome mterruptions or obstacles encountered during

7
Figure 1 Scheier and Carver's View of Infiuences on Behaviour towards Goal Attainment
Constraints, Environmental hpediments or Facilitators
Knowledge of Behaviour's
Outcome Expectancy
Efficacy
Pnor Accomplishments Vicarious Expenences,
From Scheier, M & Carver C. (1987). Dispositionai optirnism and physical well-being:
The infiuence of generalized outcome expectancies on health. Journal of Personalip and
Social Psvcholosy., p.199.
attempts to reach a goal. Outcome expectancy is innuenced by many factors:
(a) knowledge of the consequences of the behaviour, (b) efficacy expectancy, and(c)
various extemal factors such as t h e constrahts and environmental facilitators or
hpediments.
Although not depicted in this mode4 the continuous nature of the self-regdatory
process is implied through the influence of knowledge about the consequences of
behaviour on outcome expectancy. Knowledge of behaviour is derived nom reference
schemata in memory which have resulted fkom previous expenences in goal anainment
or goal relinquis hing.
EtFcacy expectancy or self-efficacy is an important influencing component in
behavioural self-regdation (Scheier & Carver, 19 87). Self-efncacy expectations are

determined by various sources including pnor accomplishments, vicarious expenences,
and verbal instructions. Pnor accompiishments are the most intluential, with successful
experiences raising self-efficacy expectations and f~lures decreasing them (Carver &
Scheier, 1990).
When a goal and outcome expectancy for that goal are very specific, self-efficacy
is often the most important influence on the decision to engage or not engage in goal
directed behaviours. This has been shown to be especially true in research related to
specific heaIth behaviour or activities (O'Leary, 1985; Rabinowitz & Melamed, 1992;
Taal, Rasker, & Wiegman, 1996). In situations where more generalized goals are desired,
other factors are aiso influentid in the formation of outcome expectancies.
Outcome expectancies are often subject to other important influences in addition
to one's self-efficacy (Carver & Scheier, 1990). As depicted in Figure 1, integration of
information from a varïety of sources, including evaluation of physical and social
impediments and consideration of the depth and extent of one's resources are some of
these additional factors which will influence outcome expectancy formation.
&dication of the Concq&gal Frarnework to the StuQ
This research study was designed to examine quality of Life and factors that are
related to the quality of iife of community-dwehg, older penons. Scheier and Carver's
(1987) conceptual model of goal oriented behaviour was modiied to include the study
variables dispositional optimîsm, self-efficacy, perceived social support, personai
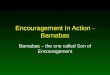
characteristics, and heait h (see Figure 2).
Quality ofiife was conceptuaüted in this applied model as the goal of human
behaviour based on the assumption that aiI persons are working towards a better quality of
Bee This is a goai that Carver and Scheier (1990) would describe as a higher level,
generaiized goai.
Quality of üfe is a generai goai which is determined by each person fiom many
dEerent factors that are important to that person. When dealing with a general goal,
specinc outcome expectancies cannot be defhed, since acquisition of a generai goai will
occur over time and wiIl result fkom the accumulation of a multitude of varÏed outcome
expectancies. As well, specific behaviour requïred for goal attainment c m o t be measured

b r e 2 Adapted Conceptual Mode1 for this Study
Efficacy Expectancy (SeIf-Eflcacy ScuIe)
t Personal C haracteristics 11.
œ--m-mw-œ--œœ11œ9-œ
HeaIt h 4
i Generaiized Expectancy Dispositionai Optimism (Zife Orientation Test)
v ( Perceived Social Support
1 (Personai Resourcrs Questionnaire) 1
when a goal is non-specific. Therefore, outcome expectancy and behaviour toward goal
attainment were excluded fiom the adapted conceptual rnodel for this study in which
quality of Life was the goal.
According to Scheier and Carver's theory of behaviourai self-regdation, perceived
internai and various extemai resources innuence individuds' expectancies toward
attainment of goals (Carver & Scheier, 1990; Scheier & Carver, 1985). Ofthe many
internai and extemai factors that innuence the process of attaining the goal of quality of
me, dispositionai optimism, seEefficacy, and perceived social support were studied.
Personai characteristics and heaith were also considered as they have been recognized as
variables which influence quality of Life.
Over the, individuals begin to hold generalized expect ancies for either favourable
outcomes or unfiavourable outcomes. These generalized exp ectancies have been
uifluenced by a wide variety of factors includùig past experience, personal abüïty, luck,
and feelings of support (Scheier & Carver, 1985). Scheier and Carver coined the term
dispositÎonai optimisrn as the generalized expectancy that good things, rather than bad,

will occur in one's We. Scheier and Carver (1993) proposed that dispositional optimism is
an important dimension of penonality and that it remains fairly stable over t h e and
context. They ascertained that individuals who have an optimistic outlook on life are
more likely to persist towards attaining goals than individuais with a less optimistic
outlook (Scheier, Weintraub, & Carver, 1986). Thus, if individuals have an optimistic
outlook on life, they are more ke ly to report a higher quality of life.
In Carver and Scheier's (1982) self-regdation theory, self-efficacy is seen as an
intra-personal varîable which dong with various extra-personai variables will infiuence an
individuals' decisions to continue towards goal attainment (Scheier & Carver, 1 987).
Scheier and Carver believe that self-efficacy expectations are important in goal attainment
especially when a specific goal is targeted. When quality of life is the goal, self-efficacy
remains important to goal attainment but Scheier and Carver proposed that it will not be
the only determinhg factor.
Many environmental ùripediments or facilitators influence behaviours toward goal
attainment. Perceived social support was included in the adapted model, for this study, as
an extra-personal factor which may Unpede or facilitate attainment of the goal of quality of
life. Numerous researchen have ünked strong social support systems to well-being for
comrnunity-dwelling older individuais (Krause, 1987; Ploeg & Faux, 1989; Rickelman,
Gallman, & Parra, 1994; Roberts, Anthony, Matejczyk, & Moore, 1994).
Unfortunately, as ind~duals age they often experience drarnatic changes in their
sociai support structure and in theu perceptions of available social support. Social
isolation, which may result fiom changes in social structure, has been recognized as an
important problem for community-dweiling older pesons and has been associated with
risk of premature institutionalization, poor heait h, loneliness, and decreased well- being
(Foxall, Barron, VonûoUen, Shuii, & Jones, 1994; Korte & Gupta, 199 1). Thus changes
in social support could negatively impact on quality of life.
Two other variables, health and personal characteristics, were aiso included in the
mode[ as their relationship with the other variables, quality of Hie, dispositionai opùmism,
self-efficacy, and perceived sociai support is uncertain. As weU as being a notable factor
in reported quality of We, heaith has been reported to be related to ai i of the study

variables, to some degree (Abeles et al., 1994; Callaghan & Morrissey, 1993; OZeary,
1995; Scheier & Carver, L992). Many relationships have also been reported among
personal characteristics and the study variables.
Research Questions
The following research questions guided this study:
1. What is the relationship between quality of life and dispositional optimism for
comrnunity-dwelling, older persons?
2. What is the relationship between quality of life and self-eficacy for comrnunity-
dwelling, older persons?
3. What is the relationship between quality of life and perceived social suppon for
comrnunity-dwelling, older persons?
4. What is the relationship between dispositional optimism and self-efficacy for
community-dwelling, older persons?
5. What is the relationship between dispositionai optimism and perceived social
support for community-dwelling older persons?
6. What is the relationship between self-etficacy and perceived social support for
community-dweliing, older persons?
7. What are the relationships among healt h for community-dwellingy older persons
and the primary study variables of quaiity of He, dispositional optimism, self-efficacy, and
perceived social support?
8. What are the relationships among personal characteristics of comrnunity-
dweüïng, dder persons and the primary study variables of quality of We, dispositional
optimism, self-efficacy, and perceived social suppon?
Definition of Tema
Quaiity of Hie is "a person's sense of weü-being that stems fiom satisfaction or
dissatisfaction with the areas of life that are important to W e r " (Ferrans, L990a, p. L5).
QuaIity of life was measured using the Quality of L'de Index (Ferrans & Powen, 1985)
which was designed to measure both perceived satisfaction with and importance of various
Ke domains (see Appendix A).

Dispositional optimism was defined by Scheier and Carver (1985) as the tendency
to believe that one will generally experience good versus bad outcornes in life. Optimism
is considered to be a personal resource variable which remains stable over time. The Life
Orientation Test (LOT) developed by Scheier and Carver was used to measure optirnism
(see Appendix B).
Self Efficacy
Seif Efficacy was defined for this study as the self-assessecf personal capability
that one c m successfiilly perfonn certain behaviours (Bandura, 1977). Self-efficacy was
measured using the Self-Efficacy Scale (Seeman, Rodin, & Albert, 1993) which was
designed to assess self-efficacy perceptions in nine Life domains relevant to older perçons
(see Appendk C).
Perceived Social SUD DO^ Perceived social support was defined as the perception by the individual of the
adequacy of necessary personai and material resources nom other individuals (Callaghan
& Morrissey, 1993). Socîai support was measured using part 2 of the Personal
Resources Questionnaire (PRQ8 5) which was designed by Weinert ( 1987) to measure
perceived social support as a composite of attachent and intimacy, social htegration,
numirance, worth, and availability of help (see Appendii D).
Personal Characteristics
Personai Characteristics are those demographic characteristics which describe the
sample and which may be related to the primary variables ofthe study. Monnation on
personal characteristics coiiected Eom subjects included: sex, age, marital status,
education, and availability of family andfor fkiend (see Appendix E).
Healt h
Information coiiected fiom subjects related to heaith included: (a) self-rating of
curent health (Statistics Canada, L987); (b) self-rating ofcurrent health as compared to
previous heaith (Statistics Canada); (c) self-rating of the Muence of hedth problems on
desired actMties of daily living (ADLs); and (d) Iisting of heaith problems and subjective
appraisai of their influence on abüity to perform desired ADLs (Canadian Study on Health

and Aging Working Group, 1994). Health pmblems were defined as any change in health
which the individual perceived as a problem (see Appendk F).
Communitv-Dwelline Older pers on^
Community dwelling, older persons were defined as individuals aged 65 years or
older who lived in a non-institutionai setting.
Assumptions
The following assumptions were made to conduct this study:
I The experiences of older persons provide a unique perspective which is not the
same as that ofyounger persons.
2. Quality oflife is individually detemined.
3. Recruiting subjects &om diverse settings would result in a heterogeneous
sarnple of older persons.
4. OIder persons are able to complete Iengthy self-report measures related to
the abstract concepts of the study.
5. Completing the self-report measures in older persons' homes would facilitate
taking time to reflect and answer questions about abstract concepts of the study.
6. Completing the questionnaires with the indivîduals would reduce the likelihood
of missing data.

CHAPTER tI
REVlEW OF THE LITERATUliE
The numbers and proportion of people aged 65 years and older is steadily
increasing and is expected to continue to increase over the next 40 years. By the year
203 1, approximately 25% of the Canadian population will be over 65 years of age (Novak,
1993), the majority of whom wiii reside in the cornmunity. However, the quality of Me of
community-dwelling, older persons has received little research attention. Until more is
known about quality of life and factors which influence quality of life, uncertainty will
remain regarding interventions to support and prornote quality of life of this population.
To detennine the care requirements of these older individuals, an accurate assessment of
their needs must include identification of those factors which determine their perceived
quality of life (Vanicchio, IWO).
The review of pertinent literature has been organited using the conceptual model,
that guides this study, adapted 6om Scheier and Carver's (1987) model. Quality of life
was conceptualized within this conceptual model as the goal towards which al1 individuals
are working. First, research related to quality of life is reviewed. The correlates,
dispositional optirnism, self-efficacy, perceived social support, personal characten'stics,
and health are considered individually as weil as in relation to quality of life and to one
anot her.
Quality of Life
Quality of life is a multidimensionai concept that encompasses many other
concepts Uicluding weli-behg, happiness, contentment, fiilnlment, health, and life
satisfaction (Abeles et al, 1994; Chan, 1987; Ferrans, 1 WOb; Grant, Padiiia, Ferreli, &
b e r , 1990). There is some general agreement about the factors which contniute to
quality oflife, but shce quality of life is subjectively determineci, agreement about its
definition has not been reached (Faden & German, 1994; George & Beamn, 1980;
Stewart & King, 1994).
Quality of life has been measured both by extemal or objective measures, wkch
are considered to uifer quaüty, and by subjective appraisal (Abeles et ai., 1994; Ferrans &
Powers, 1985). Objective measures commoniy used ïnclude income, physical health

status, tùnctionai ability? independence, standard of living, social status, goal achievement,
longevity, and recovery from illness or surgery (Ferran & Powers, 1985; Foremen &
KleinpeU, 1990; Jalowiec, 1990). These objective measures contribute to quality of life
but do not capture individuals' perceptions of their overall quality of life (Oleson, 1990b).
In addition, some of these objective measures, such as occupation, income, social status,
housing, and work, may not be as relevant for older persons as they are for younger
persons. Stewart and King (1994) suggested that infemng quality fiom external factors
dernonstrates an inability to clearly distinguish between actual quality of life and those
factor that rnight simply be predictive of quality of life.
Quality of lise is best determined by a subjective assessrnent which focuses on the
individuals' perceptions of satisfaction with dornains of Me which are important to each
individual (Ferrans & Powers, 1985; George & Bearon, 1980; Oleson, 1990b; Pearlman &
Uhlmann, 199 1; Peplau, 1994). Perceived quaiity of life of community-dwelling, older
persons has not been studied to any great extent. An exhaustive iiterature search
produced Iïmîted description of perceived quality of life of this population. In this study,
perception of quality of üfe of communi~dwehg, older persons was measured using the
Quality of Life Index (Ferrans & Powers, 1985).
Quality of life has ofien been equated with heaith or physical functioning. There
exias a subaantial body of research which provides evidence that health is one of the
arongest predictors of quaüty of life for older persons (Ginadas, Counte, Glandon, &
Tancredi, 1993).
m i i t v of Life and HeaIth
Many researchers have reported that health and quality of life are related
(Bradbury & Catanzaro, 1989; Gu-radas, et ai., 1993; Harvey, Bond, & Greenwood, 1991;
Rickelman, Gallman, & Parra, 1994). Larson (1978) who reported on a collection of 30
years of research on the subjective well-being of older Americans, found hedth to be the
strongest Îndicator of weli-beîng. Gooding, Sloan, and Ansel (1 988) undertoo k a
secondary anaiysis of data 6om 2724 individuals over the age of 65 years, who were
Uicluded in the 1978-1979 National Canada Health Survey (Hedth and Weffire, 198 I).
They aiso found that p hysicd heaith status was the most signincant factor in predicting

well-being for these older persons. These findings were supported by Ruchlin and Moms
(199 1), who found that self-assessed good health and functionai independence were
associated with higher quaiity of Iife ratings in a study of 3 10 individuals aged 65 to 74
years.
Ginadas et a1.k (1993) findings also supported the relationship between health
status and quaiity of Ise. They studied 402 adults, age 62 years and older. Three
measures of heaith status were used including functional health, historical health, and
~e~assessed health. Quality of Life was measured using a single life satisfaction question
which the researchers agreed was oniy a crude approximation of the cornplex, quality of
Me constnict. The researchen found a strong positive relationship between the health
status of older persons and their life satisfaction, with the fùnctional heaith status having
the strongest association.
Aithough many researchers have detennined that better heaith is related to greater
perceived quality of Ire, how health idluences quality of life is not known. Rodin and
McAvay (1992) studied factors which uinuenced change in perceptions of health for 25 1
Engiish-speaking, comrnunity-dwelling penons in South Central Connecticut, aged 62
years and older. Data were colected nine tirnes over a 3-year penod of time. Subjects
were placed into groups according to their self-rated health and perceived changes in
health were captured during each interview. Many (Sa%, = 145) reported a decline in
perceived health between any two consecutive interviews. Life satisfaction was measured
using items from the Life Satisfaction Index (Neugarten, Havighurst, and Tobin, 196 1).
Rodin and McAvay found that individuais who were categorked at the initial hteMew as
having low to moderate levels of Ke satisfaction were twice as iikely as other subjects to
report a subsequent deche in perceived heaith. Accordimg to Carver and Scheier's
(1982) theory of behavioural self-regdation, used to guide the curent study, these
hdings support the notion that factors, such as heaith, c m infiuence qudity of life and
that quaiîty of life cm also influence heaith.
A relationship between quaiïty oflife and health has been reported by researchers
who have used the Quaiity of Life Index (QLI) in various populations. Biiiey and Ferrans
(1993) used the QLI to measure perceived quality oflife of 40 patients, aged 39 to 73

years, who were undergoing percutaneous transluminal coronary angioplasty (PTCA).
Data on perceived general health were collected the evening before surgery and again 4 to
6 weeks later. Perceived health improved significantly after PTCA as did mean overall
QLI scores. Bliley and Fetrans reported that this improvement in overall quality of life
scores was due to increased satisfaction with health and hnction rather than changes in
other aspects of life. [n JeRey's (1989) examination of the relationships between quality
of life and severity of rheumatoid arthritis, better funetion, less pain severity, and fewer
problems related to arthritis were associated with better quality of life.
Perceived health status for older persons has been found to be related to objective
measures of health status (Rodin & McAvay, 1992). Older persons may, however, rate
their health as good or excelient even when they have chronic health problems (Barron,
Foxall, Von Dollen, Shull, & Jones, 1992). Recall of episodes that were better or worse
and cornparisons with peers ofien affects how individuals perceive their current health
status. They have a lüé-the of expenences and adaptations to other problems which
serve as resources to their ingenuity to overcome the limitations of the disability
(Verbrugge, 1994).
Fhdings dEer when objectively measured functional status is used rather than
perceived health. Osberg et ai. (1 987) studied quality of life and life satisfaction among 97
moderately to severely disabled adults, aged 60 to 95 years. Using the Barthel Index
(Mahoney & Barthei, 1965) to objectively measure tiinctional heaith status, older persons
who were more active and who had high fûnctional levels reported higher quaiity of We
regardless of disability. These findings support the use of both questions which ask the
individual to rate their perceived heaith status and questions which elicit information about
the acnial health problerns ofthe W d u a l and their duence on fùnctionai ability, as was
done in thîs study.
Quality of Life and Persona1 Characteristics
Although personai characteristics such as se7 age, marital status, education, and
availabiiity of supports have been found to be related to quality of Sie, reported
relations hips among these varÏables have been inconsistent for the community-dwelIing,
older penons (Larson, 1978). This inconsistency is, in part, because the dive* for this

population is greater than for any other age group. This diversity in the community-
dwelling, older population is because of: (a) the three decade age range fiom as young as
65 years to as much as 95 years or more, @) differences in earlier life experiences,
(c) differing numbers and degrees of changes and losses expenenced, and (d) wide
variations in health status tiom individuals with no chronic hedth problems to individuals
with three or four such problems (Hughes, 1993; Stewart & King, 1994).
In some studies, hcreasing age has been shown to be related to higher quality of
l ie (Campbell, Converse, & Rodgers, 1976; Hicks, Larson, & Ferrans, 1992). Medley
(1980) examined Lie satisFdcton across four stages of adult Me. Using two measure to
determine overall Life satisfaction, Medley found that life satisfaction increased for men as
they aged but remained relatively constant for women.
Marital status has generaiIy been found to be positively associated with quality of
life (Girzadas et al., 1993). Girzadas et ai. found that individuals who were married were
more satisfied with their iives than t hose who were not married. It is not clear in their
study of older men (n = 150) and women (fi = 252) if this association held for both sexes.
ln this study quality of Me was assessed through the use of a single question about current
Iife satisfaction which does not reflect the multidimensionai nature of quality of lie as it
was conceptuaiized in the current study.
Larson (1978) reviewed studies of older people fiom over a 30-year period. He
concluded that marrïed persons tend to have greater weh-being and wîdowed divorced,
and separated persons tend to report poorer well-being- Weli-being of single individuals
was found to be similar to that of mm*ed persons.
G o o d i i et al. (1988) studied the relationship among several hedth and lifestyle
factors and the weU-behg of Canadians over the age of 65 years a = 2746). Weii-being
was measured using a singie measure, a self-rating of happiness. Subjects also completed
the Bradbum Affect Balance Scaie (1969) which asked for responses in terms of
fiequency of the foIIowing feeüngs: on top of the world, very Ionely, excited, depressed,
pleased, bored, proud, restiess things going my way, and upset Gooding et al. reported
that age, sex, Iiving arrangements, psycho-socid health, and Hiestyle factors were
relatively unimportant to weli-beiag.

Summarv Studies of the quaiity of üfe of older community-dweiiing individuals generally
report that they experience a quality of life that is equivalent or better than the quality of
life of younger persons (Gooding et al., 1988; Johnson, 1995; Larson, 1978; Medley,
1980). These results have been consistent despite the diversity of conceptuai and
operational definitions of quality of life in studies of the older persons.
Dispositional Optimism
Dispositional optimisrn has been detined as the general expectancy that good
things rather than bad things will happen in one's lie (Scheier & Carver, 1993). Scheier
and Carver believed that the generalized expectancy of optimism is an important
dimension of personaiity and remains fairly stable over time and events.
This conceptuaikation of optimism as a stable dimension of personality was
supported by Guamera and Williams' (1987) study of optimism of 92 mentally alert,
elderly adults ranghg in age fiom 69 to LOO years. Using the LXe Orientation Test (LOT)
to measure dispositionai optimism, Guarnera and Williams found that the mean score for
their sample was generally equivalent &l=20.74) to those from a much younger sample
&f = 2 1 .O3 for men and M = 2 1.4 1 for women). This midy is of interest since it is the
only snidy found in which dispositional optimism was measured for persons older than 65
years of age. Consistent with the current study, Guarners and Williams used the LOT to
measure O ptirnism.
Dispositional optimism has also been reported to be stable in other studies where
scores obtained on the LOT have remained consistent for test-retest over penods ofup to
3 years even when major changes in life events occurred (Bromberger & Matthews 1996;
Carver & Gaines, 1987; Schult, Thompkins, & Rau, 1988). These studies lend support to
the conceptuaiîzatîon of dispositional optïmism as a stable trait of personality.
Scheier and Carver (1987) reasoned that ifdispositionai optimism is a generafized
expectancy for fàvourable outcomes, then individuais who are optimisùc should have a
greater sense of confidence than Iess optimistic ind~duals. Therefore, optimistic persons
shouid deal more readiiy with obstades which they encounter in day-to-day Ee.
Optimistic individuais would be more iikeIy to continue to work towards attaùunent of

goals than individuals who were less optimistic.
Optirnism and Oualitv of Life
As proposed in the conceptual fiamework guiding this study, dispositional
optirnism was examined as it relates to quaiity of life. The limited research about this
relationship for older persons has been described. Thus, research which links these
concepts in other populations is also reviewed.
Individuals who have an optimistic disposition have been found to have
consistently higher levels of subjective well-being and quality of life than individuals who
are less optimistic. Scheier et al. (1989) examined dispositional optimïsm and qudity of
Ire of 5 1 relatively healthy patients undergoing cardiac bypass surgery. Optimism was
measured using the Life Orientation Test (LOT) on the day of surgery. Quality oflife was
measured 6 months d e r surgery by an abbreviated (3 1-item) version of Andrews and
Withey's (1976) Perceived Quality of Life Scale. This scale measured a wide spectnirn of
indicaton of quality of life similar to the items on the Quaiity of Life [ndex used in this
current study. Fitzgerald, Tennen, Afneck, and Pransky (1993) also studied 39
individuals, aged 38 to 77 years, who were undergoing bypass surgery. Quality of life was
measured by: (a) rating severity o f angina pain; @) the 10-item Positive and Negative
Affect Schedule (Watson, Clark, & Tellegen, 1988) which measured negative affect; and
(c) a 3-item scale of life satisfaction hcluding satisfaction with activity level, satisfaction
with sexual fùnctioning, and general satisfaction. Dispositional optirnism was measured
using the LOT. Measurements were taken pcïor to surgery and 8 months after surgery.
in both studies higher levels of dispositional optimism prior to surgery were found
to predict higher levels of quality of üfe d e r surgery (Scheier et al., 1989). The results of
these mdies have been supported by numerous other studies in various populations Eom
which researchers have reported ünks between optirnism and psychological weli-behg
and physical weli-being Given that weii-being is closely related to quaiity of We and Eom
which quaiity of life might be infened, bnefconsideration is given to these findiigs. It
must be noted that the populations sarnpled were not over the age of 65 years and so it is
unknown whether the same relationships hold tme for the older population.

Q ~ t i ~ s m and Psycholpgical Well-being
The tems psychological well-being and subjective well-being are often used
interchangeably as evaiuative tems to describe individuals' menta1 health (Abeles ei
21
al.,
1994). Psychologicai well-being is one of many dimensions which have been used to
assess quality of l i k
The effeas of dispositional optimism on psychological well-being have been
examined through a nurnber of studies using the LOT. Findings have been consistent.
Persons who are more optimistic generaily report higher level of psychological well-being
than Iess optimistic persons during stresshl periods of time. Components of psychologicai
well-being that have been identified as correlates with optimism include: (a) resistance to
the development of depressive symptoms and higher Ievels of reported well-being at 3
weeks postpartum (Carver & Gaies, 1987); @) better adjustment and lower distress
levels in coiiege students 3 months afker entering their first semester (Aspinwall & Taylor,
1992); (c) better adjustment to arthritis for 205 individuals with rheumatoid and
osteoarthritis (Long & Sangster, 1993); (d) greater satisfaction with tnends and subjective
well-being in cardiac patients 5 years d e r surgery (Scheier & Camer, 1992); (e) less
negative moods in HIV positive, gay men (Taylor et ai., 1992); and ( f ) less mxiety in
seeking care for symptoms of breast cancer (Lauver & Tak, 1995). In al1 of these studies
the Life Orientation Test (LOT) was used to measure optimism.
In the ody study found which looked at optimism and perceived wel-being in the
cornrnunity-dwelluig, older population, Reker and Wong (1985) found that optimism was
positively related to perceived well-being. Thïrty-one cornmunity-dwelling individuals,
aged 70 to 93 years completed the Future Orientation Survey (FOS) to measure optimism.
Data coiiected on the FOS included subjectively measured anticipated events, timing of
events, locus of initiation, and the confidence that these events would take place. Reker
and Wong reported that expectations about long-term events (events occurring a year or
more later) and self-initiated events were responsible for the significant relationship
between optimism and perceived weU-being. Since Iong-term expectation of events
requires greater optimism, Reker and Wongys study Iends support that the relationship
between optimism and quality of life exists for older persons.

Optimism and Health
Optimism has also been found to confer benefits to physical health for various
populations (Hamid, 1990; Scheier & Carver, 1985), although there is little information on
the relationship between optimism and health for comrnunity-dwelling, older persons.
However, since dispositional optimisrn is believed to be a trait of personality that remains
fairly constant over the, then its relationship with hedth might also be fairly constant over
time. In other words, reported relationships between dispositional optimism and health in
younger populations may be consistent with those in older populations, although this
needs to be determined.
A positive relationship between optimisrn and health has been found in many
studies of younger, hedthy and unhealthy penons @amid, 1990; Lauver & Tak, 1995;
Schulz, Bookwala, Scheier, Knapp, & Williamson, 1996). In one study, illness symptoms
experienced by college students during the last 4 weeks of an academic semester were
examined. High levels ofoptimism were associated with low levels of physical syrnptoms
(Scheier & Carver, 1985). Measurements taken from L41 college midents before and
after the final 4 weeks showed that optimism was negatively associated with physical
syrnptoms across time (Scheier & Carver).
The effea of optimism on recovery from cardiac bypass surgery a = 5 1) was
studied by Scheier et al. (1 989). Using the LOT to measure dispositional optimism,
Scheier et ai. found that those who were optimists recovered more quickly, were more
ükely to resume physical and recreationai activities and retum to work, and were less
likely to have two clinicdy signincant hdicators for subsequent myocardiai infàrctions.
In generai, O ptimistic subjects returned to their "normal" tives more readïiy than less
optimistic subjects. Data collected Eom these same subjects 5 years later showed that
benefits in physicai heaith status continued for optimists. . . Personal Characteristics Dttmrsm and
Few studies have examined the relationships between dispositionai optirnism and
penonai characterïstics, such as age, se% maritat status, and education. In studies where
these associations have been addressed, oniy one significant correlation was reported.
Lauver and Tak (1995) found a positive reIationship (1 = -32, p < -00 1) between education

and scores on the LOT in their study of 135 women, aged 19 to 76 years.
Summarv Dispositional O ptimism involves holding positive expectancies about one's future,
that good will happen rather than bad. Not surprisingly, optimism has been found to be
positively associated with quality of life and this association is believed to be influenced in
part by the use of adaptive coping mechanisms (Scheier et al., L989). People who are
more optimistic adapt more readily to life circum~tances~ they report less stress, and they
report higher levels of subjective psychological and physical weli-being than those who are
less optirnistic.
SeKEfficacy
In the conceptual Framework used to guide this study, Scheier and Carvet (1987)
pro posed that efficacy expectations influence decisions towards goal att ainment . Self-
efficacy has been measured typically through subjective assessrnent of one's capacity to
perform specific behaviours. Self-efficacy is based not on the actud skills that individuals
possess but rather on the judgement which individuals make about what they can do
(Gonzalez et al., 1990). Scheier and Carver believed that efficacy expectations operate at
various levels of specificity, nom the very specific to the very generai.
Generalized self-efficacy is deterrnined by assessùig individuais' beliefs in their
general ability to deal with various situations. The Self-Efficacy Scale which was used in
this study was developed to capture generalized efficacy within nine domains of living
including health, transportation, farnily relationships, marital relationships, finance, safety,
fiÏend relationships, living arrangements, and p roductivity (Rodin & McAvay, 1 992).
Since the goal measured for this study was the generalized goal of quality of Ise, situation
specific measures of self-efficacy were not appropriate. The globai goal of quality of life is
broad and abstract and use of specific seIf-efficacy questionnaires would not be
approprÎate since no single specinc behaviour can achieve quaIity of life.
The largest body of self-efficacy research is task specific. This research about self-
efficacy is limited for the older population. Generaiked self-efficacy, congruent with the
conceptuai h e w o r k has been studied in older people. However, Kttle is known about
the relationship between self-efncacy and the other variables of interest in this study for
communÎty-dweiiing older persons.

Self-Eficacv and quality of Life
The relationship between selliefficacy and quality of life for aii populations has
received little research attention. Much of the research which links quality of life to self-
efficacy, uses health as an indicator of qudity of life (Abler & Fretz, 1988; Moore, 1990).
Health-related quality of life does not appropriately reflect the subjective assessrnent of
quality of Sie (Oleson, 1 WOb). In addition, the self-efficacy perspective for much of the
available research has been specific to a particular behaviour and has not been studied as
perceptions of generalized self-efficacy. No data were found which described the
relationship between generalized self-efficacy and quality of life for community-dwelling,
older persons.
Some of the researchers who have examined the relationship between self-eficacy
and quality of life have done so through addressing the concept of control. It is often the
individuals' perceptions of their ability to enact coping strategies that determines
behaviour rather than the more global sense of control. In these situations, self-efficacy
was perceived to be one of the main sources of control and control was dehed as the
subjective determination that one is taking charge of what happens in one's life. in these
studies, a sense of control was found to be an important predictor of psychologicai weii-
being (Rodin, L986; Rowe & Kahn, L987).
Only one study was found which specificaily addressed the relationship between
quality of life and self-efficacy. Cunningham, Lockwood, and Cunningham (199 1) studied
the relationship between perceived self-efficacy and quality of life of 270 cancer patients
aged 30 to 60 years, before and after a psycho-educational program designed to enhance
their sense of control over their mental and emotional aates. Quality of Life was rneasured
ushg the Functional Living Index - Cancer, a 22-item scaie designed to assess generai
quality of Life in cancer patients (Schipper, Chch, McMunay, & Le* 1989). Affective
state was aiso measured, as it was perceived to be an important contributor to quality of
We. Using the ProfXe of Mood States (POMS) ( McNair, Lorry & DroppIeman, 1971)-
mood disturbance scores were obtaÏned for six negative mood States. Self-efficacy was
measured using the Stanford Inventory of Cancer Patient Adjustment, a 38-item scaie
which assesses individuais' beliefs regardhg their abüity to ded with specinc situations
(TeIch & Telch, 1986). Cunningham et ai. found strong correlations between quality of

Life and self-efficacy scores (c = -67 to .69) and strong negative correlations between
negative mood state scores and self-efficacy (1 = -63 to -.70) even after controlling for
personal, disease, and demographic characteristics. Also of note in this study were the
improvements in both perceived self-efficacy, quaiity of life, and mood measures which
occuned after the 7 week, coping skiiis training intervention. Although this was a
correlation study, these results do suggest that training can influence self-efficacy which in
tum can positively influence mood and perceived quaiity of life.
Self Efficacy and Optimism
Scheier and Carver (1992) recognized that self-efficacy and dispositional optimism
have some sirniladies, and that both concepts may be intluential in detennining behaviour.
However, they are very dierent constructs. Self-efficacy expectations are usually
determined by the person's assessrnent of hidher ability to perfom act-specific or domain-
specific behaviours successfully. Self-efficacy theory emphasizes the use of specific
cognitive or performance strategies ( G o d e z et ai., 1990). Dispositional optimism is
conceptuaiïzed as a generalized expectancy that has developed over time becomes an
important part of penonaiity, and remains relatively stable over time and context (Scheier
& Carver, 1985). Unl ie dispositional optimism, self-efficacy is not a characteristic of
personality or a global trait. Instead, self-efficacy expectations tend to vary across
behaviours and contexts (Bandura 1977). Dispositional optimism is a personality trait
which cannot be significantiy iduenced whereas self-efficacy can be enhanced through
modelling, persuasion, skills mastery, and emotional adaptation (Moore, 1990).
Results ofresearch demonstrate that both self-efficacy and optimism are usefùl in
predicthg behaviour (Scheier et ai., 1989). In their study of 51 post-operative heart by-
p a s surgery patients, Scheier at ai. found that for some specïfîc outcomes, such as
resumption of semai activities and expectations around work and socializing, specinc
expectancies were better predictors of behaviour than optimism. For other specific
outcomes, both specinc expectancies and generalized expectancies for positive outcomes
predicted behaviour. In the case of resumption of vigorous p hysicai exercise, the
individuais' relevant specific expectancy was not a predictor. Instead optimism was a
signincant predictor of behaviour.

These findings were supported by Friedman, Nelson, and Webb (1994) in their
cross-sectional study which examined the reiationship between predictors of breast self-
examination, dispositional optimism and self-efficacy in 427 rniddle-aged women. They
found that self-efficacy, (c = .45, Q c -00 1) not optimism, was one of the strongest
correlates for breast seKexam*nation. This is consistent with Carver and Scheier's (1982)
theory of self-regulation where self-efficacy plays a major role in determining behaviour
when there is a specific goal, in this case breast self-examination. These hidies support
the belief that both generalized and specific expectancies are usefil in predicting behaviour
with each containhg predictive power that is not available from the other (Scheier &
Carver, L992).
The relationship between self-efficacy and dispositional optimism has not been
extensively studied. In the oniy study found which addressed this relationship Friedman et
al. (1994) reported a positive, weak correlation of y = -13 (p < .O 1). Aithough individuals
who were more optimistic did not practice breast self-examination more often than Iess
optimistic women, Friedman et al. proposed that a more optimistic attitude about the
outcome of self-examination increased the likelihood of greater self-efficacy in performing
breast examination.
Self-Efficacv and Health
Efficacy expectations have been tinked to health-relevant behaviours such as
smoking cessation, pain management, controhg weight, and adherence to exercise and
preventative health programs in a variety of populations (Domelas, Swencionis, & Wylie-
Rosett, 1994; OZeary 1992; Strecher, DeVeüis, Becker, & Rosenstock, L986).
Individuals with hîgher IeveIs of self-efficacy are also more like1y to recover better from
ilinesses, rate their health as better, require Iess medicai interventions, and report fewer
sicknesses and feelings of depression (Fitzgerald, 199 1; Gecas, 1989; Grembowski et aL,
1993; Taal et al., 1993).
Men et ai. (1990) studied 125 male patients, aged 35 to 65 years following
coronary artery bypass surgery. Self-efficacy for activities of daily Iiving and for social
and leisure activities was measured jus prior to hospital discharge on a iikert-type scaie
ranghg h m "defKteLy cannot do" to "defitely can do". Men et ai. found that high

~e~eff icacy ratings at the time of hospital discharge significantly predicted physicai,
social, and Ieisure fitnctional status 6 months later.
Few researchers have studied the relationship between self-efficacy and health in
the community-dwelling, older population. However, two studies of older cornrnunity
dwelling persons were found which demonstrate consistency with study results of younger
populations. Grembowski et al. (1993) studied the relationship between ~el~efficacy,
health behaviour and health status in a large sample = 2,524) of adults over the age of
65 years, living in north-western United States. SeKefficacy data were obtained using a
l 0-item scale, ranging fiom "not at al1 sure" (0) to "very sure" ( LO), on which subjects
rated their perceived ability to control five specific health behavioun: exercise, fat intake,
weight control, alcohol intake, and smoking. Health status was determined through data
collected on: (a) the Quality of WelCBeing scale (Kaplan, Bush, & Berry, L976); (b) the
10-item Centre for Epidemiological Studies Depression scaie (Radlott; 1977); and (c) a
selfkaring on five health scales. Grembowski et al. found that those reporting higher seK
efficacy had better overail health status, reported fewer physician visits, and had Iower
health risk in the five health behaviours studied,
Rodin and McAvay, (1992) along with various colleagues have provided much of
what is known about the relationship between generaiized health and a generalized
measure of self efficacy for older persons. Rodin and McAvay studied the influence of
self-efficacy on perceptions ofheaith in 264 individuals, age 62 years and older, over a
perïod of 3 years. An Uiitial h t e ~ e w and 7 absequent intemîews were conducted. At
each interview individuals were placed into one of two groups dependîng upon their rating
of their perceived health. niose with a change in health perception were placed in one
group and those without a change were placed in the other group. Self-efficacy was
assessed at each interview ushg the SeFEfficacy Scaie which the authors of the study
developed. This is the same questionnaire that was used for the current study.
Rodin and McAvay (1992) found that subjects had signincantly lower feelings of
segefficacy when negative changes in perceived heaith occurred secondary to an increase
in the number of pre-existhg medical conditions. This change in self-efficacy was
reported to be signiscant oniy for those individuais who were over 75 years and who had

higher feelings of self-efficacy at their initiai assessment. Interestingly, changes in
preexisting conditions were not associated with perceived decliie in heaith for those
individuais who were categorized as having a low self-efficacy. at the initial interview.
Self-efficacy appeared to be a moderator variable which affiected the relationship between
changes in perceived heaith and changes in objective health. It seemed that for those who
had high levels of self-efficacy, changes in actual health status had greater impact than for
those who had lower perceptions of self-efficacy. Whether perceptions of health
influenced self-efficacy or self-efficacy iduenced health could not be concluded from this
study, since changes to both occurred at the same time.
Self-Efficacy and Personal Characteristics
Wonnation regarding the relationship of self-efficacy to personal characteristics
such as age, education, marital status, and proximity of social support is ümited for older
persons. As individuals age they experience many personal and social challenges as well
as physical decline which influence their independence and feelings of control. One
can thus speculate that older individuals may not be as able to cope with these changes
and that self-efficacy would more readily be negatively infiuenced and thus be found to be
lower in the older-population. However, research results are contradictory as to whether
self-efficacy increases or declines with advancing age.
In their study, cited in the previous section, Grembowski et al. (1993) found that
self-efficacy did not decline wîth age. In Rodin and McAvayYs (1992) snidy, the
relationship between lower reported self-efficacy and negative changes in perceived heaith
was only present for the subjects over the age of 75 years, and not for the group aged 62
to 75 years.
Summarv Self-efficacy expectations have been found to be associated with positive health-
related behaviours in a variety of populations* SeEefficacy has also been associated with
lower levels of depression and stress (Stevenson, 1990). Since health and emotional States
are important factors which affect qudity of We, it is probable that self-efficacy
expectations are related to perceptions of overaii quality of Life for the older person.

Social Support
A lack of consensus exists arnong researchers concerning what constitutes social
support, how social support should be measured, and what makes it supportive (Alloway
& Bebbington, 1987; Kahn, 1994). According to Weiss (1974), social support is made up
of five dimensions: (a) the availability of help (emotionai, informational, and material);
@) indication of individual worth and role accomplishments; (c) oppominity for
numtrance; (d) social integration; and (e) provision for attachent and intimacy. This
conceptuaiization of support is consistent with the social suppon measure, the Personal
Resource Questionnaire (PRQgS), used in the current study.
Changes in the social network for older persons may stem fiom decreases in
network size secondary to death, illness, and losses in îùnctional status. Even when social
network size remains constant, older persons rnay perceive a shift in available sociai
support and express dissatisfaction with support. This perception of social support
avaiiabiiity may stem from changes in the older persons' ability to access support or fiom
changes in the suppon relationship. Engaging in reciprocal relationships and feeling
needed by others are important aspects of social support. Decünes in physical or
functional health may alter the usual social relationship, and cause individuais to feel
dissatistied with their social suppon status (Kahn, Wethington, & Ingersoii-Dayton, 1987;
Stoller & Pugliesi, 199 1).
Older persons rnay report satisfaction with available suppons even when network
size decreases. Barron et al.'s (1992) study supported the growing belief that it is the
subjective perception of social support, rather than the amount of social support, that is
important to the individuai. They found that the subjects in their study reported high
levels of satisfaction with social supports even though the mean network size was only 2
persons.
Two aitemative mechanisms have been proposed to expIain the intluence of sociai
support on weii-behg One model suggests that social support butfers or protects
individuais Eorn the negatîve infiuence of stressfiil events (Alloway & Bebbuigton, 1987;
Cohen & Wfis, 1985). The other model proposes that social support chectly benefits
hdiviciuds, regardiess of stressors, through various avenues such as boIstering feeiings of

control, increasing ~e~efficacy, hope, coping mechanisms, and improvement of self-
esteem (Krause, 1987; P i n a et al., 1991; Ploeg & Faux, 1989). Regardless of
ditFerences in measurement and concept of support, there is agreement that social support
is necessary for well-being, health maintenance, and life extension (Kahn, 1994; Levitt,
Clark, Rotton, & Fidey, 1987; Revicki & Mitchell, 1986).
Social SUD DO^^ and Oualitv of life
Major determinants of quality of life include human relationships, interactions with
other people, and supportive environments (Peplau, 1994). The nature and significance of
social support are common indicators to much of the research on quality of Iife (Abeles et
ai., 1994; Bury & Holme, 1990). "The power to manage one's own life efectively, that is,
to be able to cope with day-to-day experiences, including unexpected and unfiortunate
events, is both a personai ability essential to quality of life and an expected outcome of
social support." (Peplau, 1994, p. 14). Research findings support the notion that
perceived attachent to others significantly impacts on perceived quality of life
(Rickelman, Gaiiman, & Parra, 1994).
A national study in the ünited States of 4,734 people over the age of 65 years by
Newsom and Schulz ( 1996) which looked at the relationship among physical fbnctioning,
social support, depressive syrnptoms, and Ke satisfaction, supported the beliefthat social
support infiuences quality of life. To measure social support, subjects in the study
completed the Lubben Social Network Scale, a LO-item scaie that assesses social
networks. They also completed a 6-item version of the interpersonal Support Evaluation
List (ISEL) which is used to measure perceived social support. The 6-item [SEL
measured tangible, betongùig, and appraisai support with statements such as "If1 were
sick, [ could easily h d someone to help me wÏth daily chores", "When 1 feel lonely there
are several people 1 c m talk to", and "Men 1 need suggestions on how to deal with a
persond problem, 1 know someone 1 can Nm to". To measure quality of life, two
questions were asked regarding satisfaction with and fèehg about Ee. These questions
were answered on IO and six-point scales, respectively, with responses from extremely
dissatisfied to extremely satisfied and temole to delighted. Newsom and Schulz found
that the strongest predictor of quality of life was perceived social support with greater
perceived support associated with higher quality of Mie. These hdings have been

supponed by other studies with older persons (Levitt et al., 1987). Turner, Frankel, and
Levin (1983) studied the relationship between social support and well-being of 989
physicaily disabled individuals aged 18 to 92 years. They found a modest association
between sociai support and psychological well-being, with well-being measured through
such symptoms as mm-ety, depression, and anger. Revicki and Mitchell's (1 986) study of
cornmunity-dweliing, older persons @ = 2 IO), aged 65 years and older supported this
relationship. Using various social support measures to measure the quantity and affective
dimensions of social support and the 13-item Life Satisfaction Index (Wood, Wylie, &
Schafer, 1969) to measure quality of life, Revicki and Motche1l found a significant
relationship b e ~ e e n social support and Sie satisfaction.
Only two studies were found in which the relationship between quality of life and
perceived social support was exarnined using the PRQ8S to measure social support.
Findings fiom these studies were consistent with the findings of other snidies cited above.
One study examined the relationship of social support and well-being in a sample
of99 adolescents aged 15 to 17 years. Using the 39-item Adolescent Generd Well-Being
Questionnaire (Columbo, 1986) to assess psychological, physical, and social dimensions of
well-being and the PRQIS to measure social support, Yarcheski, Scoloveno, and Mahon
(1994) found a significant positive correlation (1: = -55, p < .001) between perceived social
support and weN-being.
The other cross-sectional study exarnined the relationship between psychological
weii-behg and perceived social support in 50 cornrnunity-dwelling, older persons, aged 65
to 80 years (Ploeg & Fawc, 1989). Psychological weii-being was measured by the Affect
Balance Scaie (Bradbum & CaploviU, 1965), a 10-item scaie which assesses positive and
negative affect. Positive affect includes feeling of being excited, pleasure, and pride.
Negative affect related to feelings such as depression and amiety- Ploeg and Faux found
that sociai nippon was moderately associated with psychological weli-behg (1 = -54,
p < .O 1) and negatively correlated to negative affect (1 = --43, p < .O 1).
Although a relationship is known to exist between sociai support and quaüty of
We, the direction of the effects has not yet been determined. T t is possible that the
relationship is ceciprocal and that older persons who have higher levels O ~ S O ~ support

perceive that they have a better quality of Iife It is also possible that older persons who
perceive themselves as havhg a higher quality oflif'ie are more Iikely to develop close
relationships (Ploeg & Faux, 1989).
Social Swaort and Optimism
Researchers generally agree that a positive relationship exists between social
support and optllnism although the direction of the relationship is not known. Barron et
al. (1992) studied loneliness in 56 women, aged 75 to 94 years, who had poor vision.
Optimism was measured using the LOT while sociai support was measured by the Social
Support Questionnaire (SSQ). The SSQ is a 6-item questionnaire which addresses social
support network and social suppon satisfaction. Optimism and social support satisfaction
explained approxirnately 43 percent of the variance in degrees of Ioneliness in this nudy
sample. Barron et al. (1992) found that women who had Iower levels of optimism and
who reported less satisfaction with their social support, experienced higher levels of
loneliness. Optim*sm was found to be direaly related to loneliness and to be related
indirectly through sociai suppon satisfaction.
Optimisrn was also found to be significantly related to both social network
(1 = -26, = .OS) and to social satisfaction (1 = .38, p = -003). Optimistic individuals
reported Iarger social networks and greater satisfaction with the identified networks.
Although social suppon networks were smaii (141 = L.94), satisfaction levels with nippon
were high. This Iends support to the use of a satisfaction rneasure to determine social
support. Results of Scheier, Weintraub, and Carver's (1985) study supported hdligs
reported by Barron et a1 (1992). Scheier et ai. proposed that optimists would use
cornple>~ problem-sohg coping mechankms to deal with stresstùl situations.
Undergraduate students &i = 100) were asked to write down in a fiee response format
what they would do in five, hypothetical, and moderately stressflll, but potentially
controllable situations. Optimism was measured using the LOT and social support was
defined as the extent to which subjects sought out other people. Scheier et ai. reported
that optimists demonstrated utilization of active complex coping strategies hcluding the
seeking out of sociai supports.
Billingsley, Waehier, and Kardin (1993) lent additional support to these findings.

They assessed dispositional optimism and coping strategy in 82 univenity students at two
times of measurement over a period of 4 weeks. They found that optimism was associated
with seeking out social supports for emotionai and for instrumental reasons.
Social Support and Self-Efficacy
Consistent with the conceptual model used to guide the current study, the choices
which individuals make are greatly influenced by their seE-efficacy expectations as well as
by their social environments (Kahn, 1994). Whether individuals engage in certain
behaviours or take certain actions is often dependent on the perception that others have of
their seiCefficaciousness (Taal, Rasker, & Wiegrnan, 1996). This relationship bas been
exarnined in a number of studies which looked at the infiuence of social support on
behaviour. In one longitudinal study, individuals with rheumatoid arthritis, whose spouses
joined them in a self-management education program, reported significantly higher self-
efficacy regarding pain control, self-management, and exercise than individuals who did
not have spousal support (Taal et al.).
Nthough social support has received extensive research smtiny, idormation
about the relationship between social support and self-efficacy is limited. Only one study
was tound which specincaiiy addressed the relationship between these two variables.
Barlow, Williams, and Wright (1996) studied the relationship between self-efficacy and
social support in 80 people who had arthritis. The mean age of this group was 68.4 years
(m = 8) although some participants were as young as 50 years of age. The Generaked
Self-Efficacy Scale (Jerusalem & Schwarzer, 1992), a IO-item scaie which measures
global confidence across a range of situations was used to measure self-efficacy. Social
support was measured using the Social Support Swey, a short questionnaire which
focuses on assessing satisfaction with support received fkom various sources (Funch,
Marshall, & Gebhardt, 1986). Resuits of the study showed a positive relationship between
social support and self-efficacy (c = -25,g = -024). Lower generaiized seIf-efficacy was
associated with lower social support satisfaction.
Social S w ~ o r t and Hedth
Many researchers have studied the iink between social support and health. Sociai
support has been found to have a signincant infiuence on health and this relationship has

been well documented (Audander & Litwin, 199 1; Berkman, Oxman, & Seeman, 1992;
Callaghan & Morrissey, 1993; W e r & Langhauser, 1988; Revicki & Mitchell, 1986).
Despite this consistency in research results, it is not known how social support actually
works to protect the health of individuals. It has been proposed that social support
provides a buffering effect from stress, decreasing the vulnerability of individuals to stress-
related illnesses. It has also been proposed that social support may positively influence
health through encouraging cornpliance with health prornoting behaviours.
Some researchers have also found that the influence of social support on health is
even more significant for older persons who are at greater nsk than younger individuals
for health problerns and for changes in social support (Blazer, 1982). Minkler and
Langhauser's (1985) study of the relationship between social support and health of 280
cornmunity-dwelling persons, aged 60 years and older concluded that social support may
even be predictive of individuals subsequent health status as much as 5 years later.
Lubben (1988) studied the relationship of social support to health of community-
dwelling persons, aged 65 years and older, in Califom*a m= [,O3 7). The Lubben Social
Network Scde (LSNS), a 10-item questionnaire which addresses network size, social
interactions, fiequency of contact with family and ûïends, and interdependent social
supports, was used to measure social support. Three health indicators were used to
measure heaith status including: (a) hospitalization length within a particular 6-month time
tiame; @) the revised Life SatSiaction Index (Adams, 1969), a measure of mental hedth;
and (c) the BeUoc-Breslow checkiist of seven health practices. Lubben found that al1 three
health measures correlated weakly with the LSNS aithough this relationship was arongea
with the revised Life Satisfaaion Index (1 = .2L,g < -00 1).
Ploeg and Faux (1989) studied the relationship between social support and health
of50 community-dwehg older persons, aged 65 to 80 years. Social support was
measured using the PRQ8S-Part II. Heaith was measured thmugh subjects rating their
current hedth on a Cpoint Likert-type scale ranging fiom "very poor" to "very good" and
by subjects comparing their health to others their age using a 3-point Likert-type scde
ranging Eom "worse than average" to "better than average". Lzestyie behaviours were
measured using the 24-item Personai LXestyIe Questionnaire which measures the extent to

which individuals engage in certain lifestyle behaviours in the categories of exercise,
nutrition, relaxation, safety, substance use, and general promotion. Subjects rated the
fiequency of practising each iifestyle behaviour on a +point Likert-type scale ranging
from "never" (1) to cbalm~n alwaysy' (4). Ploeg and Faux (1989) found that social support
had a strong, direct relationship with heakh and a positive relationship with health through
lifestyle behaviours. These results suggest that older persons with higher levels of
perceived social support engage in lifestyle behaviours which are health enhancing and
thus social support may be a vital component in the maintenance ofhealth in older
persons. However, Ploeg and Faux also suggeaed that older persons who participate in
positive lifestyle behaviours and perceive themselves to be in good health, may develop
more social relationships. Thus, the direction of the relationship between heaith and sociai
support may be reciprocal rather than unidirectional.
in the? study of 1 58 women, aged 20 to 86 years, who had diabetes, White,
Richter, and Fry (1992) concluded that social support was important to psychosocial
adjustment to iUness and to health outcornes. Using the PRQ85-Part II to measure
perceived social support, White et al. found that the greater the perceived sociai support,
the better the psychosociai adjustment to iiiness. They also found that those subjects with
poorer health had lower levels ofperceived social support and wondered whether poor
health status and chronic illnesses rnight lirnit the development and maintenance of social
networks. The reciprocal effect might also occur where lack of social support rnay
influence health deterioration.
Social Support and Personal CharacteristQ 1
Social support is influenced by various personal characteristics although reports of
the influence of age, marital status, and education on perceived social support for
CO mmhty-dwehg, older persons have been hco nsistent. Typicaliy, as individuals age,
sociai network contact decreases as a consequence of death, iliness, and mobility problems
(Kahn, Wethington, & Dayton, 1987). Average network size of 7 to 10 penons have
been reported for those under age 65 years and this range typicdy decreases by one
person for those over age 75 yean (Antonucci, 1990). Generaiiy women have Iarger
network sùes and more fiequent contact wnh network members than men (Kahn et ai.).

In addition, those who are married and widowed have larger network sizes and more
frequent contacts than those who were never maded or divorced persons (Kahn et ai.).
Since social support is derived from sociai network, this slight decrease in network
size as well as decline in fünctional health of many network supporters may influence older
persons' perceptions of available support and oldet persons may be especially vulnerable
to social isolation (Minkler & Langhauser, 1988). The main source of support for married
women are generally farnily and fnends while husbands rely on their wives to be their main
source of support (Kahn, 1994; Preston & Grimes, 1987). Therefore, widowed men are
more vulnerable to inadequate social support than wornen. Higher income, marriage, and
better education have al1 been Iinked to greater sociai support in older populations
(Weinberger, Hiner, & Tiemey, 1987).
Summarv The importance of social support to quality of life and heaith for cornmunity-
dwelling, older persons has been well-documented. Agreement and consistency in
measurement of social support by researchers will enhance the acquisition of accurate
information about oider persons' sociai support needs.
Conclusion
The current study examines the relationships among the variables quality of We,
dispositional optimism, self-efficacy, and perceived social support for community-
dwehg, older persons. Numerous msearcher have reported relationships between some
of the variables of the current study in a wÏde variety of populations. However, this study
provides information about these relationships that have nat been previously reported.
Quality of life for the agi% cornrnunity-dwelling population is important for the
determination of health care.

CHAPTER rn METHODOLOGY
The methodology used for this study is detailed in this chapter. This includes the
design, sample, the data collection procedure, instrumentation, plan for data analysis, and
ethical considerations.
Design
The purpose of this study was to determine the relationships among the primary
study variables of quality of me, dispositional optimism, self-efficacy, and perceived social
support for community-dwelling, older persons. A descriptive, correlational design was
used to examine these relationships. This type ofnonexperimentai design was appropriate
because the intent of this research was not to determine the predictors of quality oflife of
cornmunity-dweiiing, older persons, but to understand relationships arnong variables (Polit
& Hungier, 1993). An advantage of nonexperimental research is that it is often high in
reaiism (Polit & Hungler). It provides a description of a situation as it happens naturally,
and thus advances understanding of what the worId is like (Polit & Hungler). In addition,
since the relationships among the four primary study variables have not been reported,
establishing such relationships is requisite to determinhg the potential value of an
intervention to be evaluated in experimental research.
Setting
Subjects for this study were remited in a southwestern Ontario city Eom a
recreationai centre, a seniors centre, two churches, and through "word of mouthn
referrals. The recreationai centre, seniors centre, and churches were selected as places
where older personscongregated. Use of several sites increased access to different
groups of older persons thereby increasing the Likeiihood that the sample would be
diverse. Subjects were also recniited through discussions with nursing coiieagues who
had contact with cornmunity-dwehg, older persoos.
Data were coiieaed by i n t e ~ e w over an 18 month period between Iune 1995 and
December L996. [ n t e ~ e w s were conducted in the homes of each subject, at a t h e
chosen by the individuai.

Sample Design
A convenience sarnple was selected for this study by recruiting subjects from a
variety of settings to obtain a diverse group of community-dwelling, older persons.
Sample size, inclusion criteria, and recruitment methods are descnied.
Sam~le Sim
Sample size was detennined based on a moderate effect size for Pearson Product
Moment Correlation Coefficient as the primary test statistic (Cohen, 1988). Since
correlations among quaiity of life, dispositional optimism, self-efficacy, and social support
have not been reported in any one study, correlations of related concepts were used to
provide the estimate for effect size.
Scheier et al. (1989) reported a correlation r = .60 between optimism and quality
of life for 5 1 men r e c o v e ~ g nom coronary artery bypass surgery, although quality oflife
was not measured with the same questionnaire that was used for this study. IefEey (1989)
reported correlations r = .35 to -5 1 between quality of life and social support for adults
with rheumatoid arthritis, using the questio~aires that were used in this study.
Thus, given that similar moderate correlations could be expected for this study,
sample size was estimated using a moderate eEect size (r = -40). According to Cohen
(1988, table 3.4.1, p. 101), wth alpha of .OS, and power of .8O,37 subjects were required
to obtain a s m d to moderate effect of -40. Thus, 39 subjects were recniited to account
for missing data.
SampIe Cntenê * .
The inclusion criteria for the study were adults who were: (a) aged 65 years or
older, (b) living in the community, and (c) able to read and understand English. Since data
coiIection involved compIeting questionnaires, individuals with O bvious cognitive
impairment or IUnited fadity with English were excluded. Since aU i n t e ~ e w s were to be
conducted in the individualsr homes, con.hnation that individuals resided within the
community was obtained when individuals s h e d theu addresses with the researcher. No
subjects were excluded based on this criterion. One man was excluded fiom the study,
when Ï t became apparent that aU of the other participants in the study were femaie. Two
other men had initiaiIy agreed to participate in the study, but ilines for one and a move for

the other necessitated withdrawal of their agreement.
Recruitment
Potential subjects were recruited using several strategies to increase the sample
diversity: (a) the Uiformation poster (see Appendix G) was posted at a recreation centre;
(b) the Letter of uifomtion (see Appenduc EX) was given to participants in a pool
program, by the activity direaor at a recreational centre; (c) the Letter of IRfonation was
given to individuals at a seniors' complex by the pastoral care worker, (d) the Letter of
Information was given to older individuais at a church by the rninister's wife; (e) a
colleague provided verbal information about the study to members of her church; and
( f ) other colieagues who had contact with indbiduals within the community who met the
study criteria. The Letter of Information was given to penons who expressed an interest
in participating in this study by the individuals who recruited subjects in each setting.
individuals who wished to participate in this study gave their names and phone
nurnbers to the contact person in each agency or to the contact person identitied above.
These names and phone numbers were then given to the researcher who telephoned each
prospective subject and reviewed the purpose of the study, age criterion, and what was
expected of them. Potential subjects were invited to ask questions about the research and
information was shared in response to those questions. Individuais who agreed to
participate in the shidy were screened for obvious cognitive impairment during this phone
contact by the researcher who has extensive experience working with older persons and
with the cognitively irnpaired.
Data Collection Procedure
Interview t h e and place were arranged by tetephone with each individual who
agreed to participate in the study. At the beginnùig of each interview, the Letter of
Information (Appendu H) was reviewed with each subject, questions were answered and
the Letter of Consent was signed (see Appendix I).
Data collection instruments were completed in the same order for all subjects.
Background idormation was collected fïrst, Îollowed by the Health Stahts Questionnaire.
The Quality of Life Index (QLI) was the next questionnaire completed. Suice quality of
life was the focus of thÏs study, and the QU was the Iongest questionnaire, the QLI was

completed eariy in the interview to decrease the effects of fatigue. Following the QLI, the
questionnaires were completed as follows: the Life Orientation Test (LOT-C), the Self-
Efficacy Scale (SES), and the Personai Resources Questionnaire (PRQ85). Before
completing each of the questionnaires, instructions for completion were reviewed with
subjects.
Data collection interviews took from 2 to 3 hours per subject with the exception of
two subjects who took only about one hour each. Subjects were given the choice of
cornpleting the questionnaires on their own or having the researcher read aloud the
questions or statements in the questionnaires and writing in participants' responses. At
the request of moa subjects, the researcher read each question or statement out loud and
then wrote down subjects' responses. Subjects who used this method of completing the
questionnaires did so because of poor vision, poor writing skiils, andlor perceived greater
ease of providing data. Subjects were given a copy ofeach rating scaie, identical to the
one on each questionnaire, to assist them in selecting their responses to each item put to
them by the researcher.
In ail interviews, except for one, the researcher remained with the participant
during the completion of the questionnaires. One subject, because of unexpected events
related to her husband at the tirne of the planned i n t e ~ e w , asked that the researcher leave
the questionnaires with her for completion. The researcher retumed a few days Iater to
pick up the completed questionnaires.
Instrumentation
This section includes descriptions of the questionnaires used to coiiect the study
data. Ali of the instruments have been used in previous studies. A description of each
instrument follows in order ofcompletion by the study participants.
Backmound Information
The content of the Background Infionnation questionnaire (see Appendix E)
focused on usuai personai demographic characteristics including: sex, age, marital aatus,
education, and living arrangements. Demographic data were coliected to describe the
sample and to idente additional variables which may be related to the ptunary study
v ~ b l e s Some of the variables measured by items on this questionnaire have been

related to quality of life for older persons in previous research; for example age and
education (Flanagan, 1978; Solar, MacEntee, & Hill, L 993).
Four additionai questions asked subjects about the proximity of niends and
relatives and the help which those individuais could provide for subjects. These questions
were supported by a nation-wide study in which Antonucci (1985) noted geographical
proximity of social network supports "within an hour drive" as important.
Health Status Ouestionnaire
Health status was measured because of its known relationship to quaiity of life and
perceived social support. The Health Status Questionnaire consisted of two parts (see
Appendk F). Part A, Overall Health, included two questions fiom the General Health
Survey (Statistics Canada, L 987). Question I asked subjects to rate their overall health
nom poor (1) to excellent (4). Question 2 asked subjects to compare their current health
to their health 6 months before tom worse (1) to better (3). Question 3, fiom the
Canadian Study of Health and Aging Working Group (1994) asked subjects to rate the
extent to which their overall health problems affected their daily activities tom not at al1
(O) to a great deal (2).
Part B, Long-term Health Problems, focused on subjects' chronic health problems
and asked subjects to rate the extent which these specific heaith problems interfered with
activities on a 3-point scale nom not at au (O) to a great deal (2). This approach adapted
Eom the CSHA (see question 3 above) provided a more specific information about the
impact of health aatus on daily living. No information is avdable regarding the validity
and reiiability of these questionnaires. However, among the oIder population, perceived
health is considered to be a valid and reliable measure of generai heaith status (Speake,
C o w a & Pellet, 1989)- High correlations have been found between global measures of
perceived health and objective heaith indicators such as number of illnesses or level of
disability (Minkfer & Langhauser, 1988).
Quality of Life Index
Quaiity of life was measured ushg the genenc version of the Quality of Lifk Index
(QLI) deveioped by Ferrans and Powers (1985, see Appendoc A). The QLI is a
comprehensive questionnaire which addresses both satisfacton with and importance of

various life domains identined by experts in quality of Sie measurement (Ferrans &
Powers). This questionnaire was chosen because it captured the global nature of quality
of life as it was defined for this study. Disease specinc tools were not appropriate for a
diverse sample of seniors, some of whom have no significant health problems and some of
whom have a variety of different medical conditions. In addition, the QLI has been used
in both hedthy and ill populations.
Development
The initial version of the QLI was developed by Ferrans and Powers (1985) to
measure individuals' subjective well-being which is derived from satisfaction or
dissatisfaction with domains of life of seifrated importance. Items in the questionnaire
were derived from extensive literature review and inte~*ews (Ferrans, 1990). The life
dornains addressed in this instrument included "hedth care, physicd health and
functioning marriage, family, fiiends, stress, standard of living occupation, education,
Ieisure, friture retirement, peace of mînd, personai faith, life goais personal appearance,
self-acceptance, generd happiness, and general satisfaction" (Ferrans & Powers, 1985,
p. 17). Factor analysis of the QLI resulted in four subscdes: (a) health and fùnctioning,
(b) socioeconornic aspects, (c) psychologicaVspirituai aspects, and (d) farniiy (Ferrans
& Powers, 1985).
The generic version of the QLI was developed to measure quaiity of Iife in the
general population. Several subsequent versions of the QLI have been developed for
specific ihess populations. In al1 cases revision has consisted of mod-g and adding
oniy two to four additional items to the generic version of the QLI.
Descn~tion and Sconng
The QLI consists oftwo parts. The fkst part of the questionnaire asks
respondents to rate theu satisfaction with 34 various life domains on a 6-point scde from
very dissatisfied (1) to very satisfïed (6)- The second part asks respondents to rate the
importance of these same domains on a 6-point scaie nom very unimportant (1) to very
important (6).
To more accurately reffect perceived puality of Mie? scores for the QU are
deter-ed by adjustuig the satisfaction responses to reflect the value or importance that

each domain has to the individual. This adjustment results in the highest score being
awarded to the items which were rated high satisfactiodhigh importance and lowest score
given to items rated high dissatisfactionhgh unimportance. The rationale for this
adjustment was that individuals enjoy better quality of life if they are very satisfied with
things that are important to them (Ferrans & Powers, 1985). Scores can be calculated for
overall quality of life and for each of the four main subscales. AI1 scores have possible
range of O to 30 with higher scores indicating greater quality of life.
Reliabilie
The overall QLI and subscales have demonnrated reliability in a variety of
populations. Intemal consistency dunng initial testing of the generic version of the QLI
with 88 graduate nursing students was supported by Cronbach alpha of .93 (Ferrans &
Powers, 1985). The dialysis version of the QLI also achieved Cronbach alpha of -90.
These high alphas were supported in later findings of hi& interna1 consistency in various
versions of the QLI. For the QLI-Cardiac version, alpha coefficients of 36, prior to
coronary angioplasty and .96 following angioplasty were obtained (Bliley & Ferrans,
1993) and in the QLI-Cancer version, alpha coefficients of -95 were achieved (Ferrans,
1990).
Alpha coefficients have also been deterrnined for each of the four subscales with
the health and functioning subscale consistently receiving the highest alpha and the family
subscale receiving the lowest The alpha range for each of the subscales have been as
follows: (a) heaith and functioning fiom -87 to -90; @) socioeconomic aspects Rom -82 to
-89; (c) psychologÎc~spirîtuai aspects from .84 to .93; and (d) family h m -66 to -79
(Ferrans, 1990; Ferrans & Powers, 1992; Papadantonaki, Stons, & Paul 1994; Searle,
1992).
Test-retest correlations of -87 d e r a 2-week intervai were obtained in Ferrans and
Power's (1985) study of 69 graduate students. Correlations of -81 were achieved at a
L-month interval with 37 dialysis patients (Ferrans & Powers). These resdts support the
stability of the QLI, as -80 is the acceptable level for established instruments (Frank-
Stromberg, 1988).

Vaüdity
As previously described, the QLI was developed after extensive review of the
literature. Content validity of the QLI for use in research of older persons was evaluated
by Oleson (L990a). A seven-member panel of experts in the subject matter was selected
to rate the relevance of each item in the QLI using the theoretical definition and content
domain of quality of üfe. This panel rated 27 of the 3 1 items (87%) in the QLI as content
valid. This finding supported the use of this instrument in research of older persons.
Criterion validity was first established using an overall satisfaction with Iife
question as the criterion measure of quality of life (Ferrans & Powers, 1987). The
correlation between a single item rie satisfaction question and the scores ftom the
graduate nursing students = 88) who participated in the initial testing of the QLI was
-75 (Ferrans & Powers, 1985). The validity has been ftrther substantiated in diverse
populations with a correlation of -77 between the same measures for a randorn sample of
349 haemodialysis patients (Ferrans & Powers, 1992), and .89 for liver transplant patients
(Hicks et al., 1992). A study of 40 patients, pre and post coronary angioplasty, supponed
concurrent validity with correlations of -6 1 and -93 respectively between the overail score
of the QLI and a measure of Sie satisfaction developed by Campbell et al. (1976) (Briey &
Ferrans, 1993).
ife Onentation Teg
The Life Orientation Test (LOT) developed by Scheier and Carver (L985, see
Appendi 9) and the revised Life Orientation Test (LOT-R) developed by Scheier,
Carver, and Bridges (1 994) measure dispositional O ptirnism. niese self- report mesures
do not focus on any specific content domah but rather were intended to reflect persons'
generalized expectations. These instruments are highly congruent with the fiamework for
this research as they were developed by the same authors who developed the theoretical
fiamework that guided this study.
Develo~men~
The LOT was developed by Scheier and Carver (1985) to measure generaüzed
expectancy of optimism. Other avaiiable memes that potentidy meaçure optimism were
inadquate as they tended to ïnclude other refated variables such as affect, motivation,

satisfaction, and morde. The LOT was designed so that it did not include any efficacy-
based or attniution-based content (Scheier et al., 1989). Revisions were made to the
LOT as a result of hdings ofrelatively high correlations between: (a) optimism and trait
amciety, (b) optimism and self-mastery, and (c) optimism and neuroticism (Scheier et al.,
1994). In the LOT-R two items were eüminated as neither item explicitly referred to
positive outcome expectations: "1 aiways look on the bright side of things," and "Pm a
believer in the idea that "every cloud has a siiver Iining" (Scheier, et al., 1994). Since
etidnation of these two items ieft only IWO positively worded items, making it difficuit to
compute separate scores, one new positively worded expectancy item was added. A
negatively worded item was then elirninated so that an equal number of positively and
negatively worded items were left on the d e . * *
escnotion and Sconng
The LOT, which consists of L2 statements, is short and easy to complete. Four of
these statements are phrased optimisticalIy, four are phrased pessimisticaily, and four are
filer statements. The fïiier statements were constructed to disguise the purpose of the test
(Scheier & Carver, 1985). The LOT and the LOT-R are similar except that the LOT-R
has oniy 10 statements, with three statements phrased optimistically, three phrased
pessimisticdy, and the four Wer statements.
The response format of the LOT and the LOT-R is a 5-point Likert scale ranging
Eom arongiy disagree (0) to arongly agree (4). Mer reversai of the responses to the
pessimisticaliy phrased statements, a total score is caiculated. Responses to mer
statements are not hcluded in the finai score. Scores can range f?om O to 32 for the LOT
and from O to 24 for the LOT-R Higher scores hdicate greater optimism (Scheier &
Carver, 1992). For this study, aU of the items £tom the LOT as weli as the new item fiom
the LOT-R were combined into the Cornbined Life Orientation Test (see Appendix J) to
d o w for computation of both the LOT and LOT-R scores. This was done for two
reasons: (a) ümÎted reiiabiliv and vaiidity data for LOT-R are avdabIe; and (b) Lamb
(1996) used the LOT based on Cronbach aipha = -77 rather than the LOT-R which was
not intemally consistent (Cronbach aipha = -43).

Reliability
The LOT has been used extensively to determine optimism in younger individuals
but has rarely been used with older adults. Therefore, reliability and validity of this tool
across age span are not well documented.
The LOT has been reported to be intemaüy consistent, with Cronbach alpha
ranging from -75 to .87 in various populations (Carver et al., 1993; Friedman et al., 1994;
Scheier & Carver, 1985; Shifien & Hooker, 1995). Cronbach alpha was -78 for the
LOT-R when it was used in a population of 20% undergraduate students (Scheier,
Carver, & Bridges, 1994).
The LOT has acceptable test-retest reliability: (a) -75 and -79 after 4 weeks
(Scheier & Carver, 1985: Strack, Carver, & Blaney, 1987); @) -72 afler 13 weeks
@i = 182) (Carver & Gaines, 1987); (c) .74 after 12 months for 59 women (Carver et al.,
1993); and (d) -69 after 3 years with a sample of 460 middle-aged woman (Bromberger &
Matthews, 1996).
In the only study of older persons, the test-retest results of 90 frai1 elderly wornen
is not as supportive of the stability of optimism for the older population (Sharpe, Hickey,
& WoK 1994). Test-retest correlations -59 and .68 over two 6-week intervals are much
lower for older persons than for younger subjects (see above). Sharpe et al. suggested
that due to the instability of major Life events such as potential for ihess, disability, and
loss of loved ones, this remlt may be quite reasonable for this age group. Kowever,
S harpe et al. replaced the 5-point rating format of the LOT with an agree-disagree format.
This change may have afected the psychometric property results.
Test-retest correlations for the LOT-R 'ui different smples of undergraduate
students over dEerent time intervals were: (a) -68 after 4 months &i = 96); (b) -60 after
12 months a = 96); (c) .56 a£ter 24 months @ = 52); and (d) -79 afîer 28 months
a = 2 L) (Scheier, Carver, & Bridges, 1994). The test-retest correlations for the LOT-R
are lower than correlations ofthe LOT and suggest that the LOT-R is not as stable over
Ume as the LOT. More research is needed for the LOT-R across diffierent populations.
VaIidÎty
The LOT.was developed by Scheier and Carver (1985) after searching the

Iiterature and not finding any measure that focused exclusively on optimism. The initial
factor anaiysis of item responses combined indicated that the LOT items formed a factor
distinct tiom the items of the other scales (Scheier & Carver). The LOT can, therefore, be
considered unidimensional in nature.
Convergent and discriminant vaiidity for the LOT have been reported. Scores on
the LOT have been found to correlate with a number of related concepts in the expected
direction. Correlations between scores on the Beck Depression Inventory and the LOT in
a large sample of undergraduate students a = 624) were 4 7 for women and -.40 for
men (Scheier & Carver, 1985). These correlations suggest that although there is a good
deal of overlap between optimism and depression, the two are not seen to be the same
concept. Convergent and discriminant validity was determined for the LOT using a
hopelessness measure (Beck, Weissman, Lester, & Trexler, 1974) in the same sample:
(a) 1 = 4 8 for women, and (b) 1 = -.35 for men. Correlations with other related concepts
were: (a) self-esteem (women 1 = .60, men 1 = .33); (b) perceived stress (women r = -.5 1,
men L = -.60); and (c) intemal-extemai control (women r = -42, men g = -24).
By correlating scores on the LOT-R with other similar and contrasting concepts
convergent and discrimant validity for the LOT-R was aIso determined. The LOT-R
correlated in the expected direction with: (a) self-esteem (1: = -50); (6) self-mastery
(1 = -48); (c) trait amiety (1 = 4 3 ) ; and (d) neuroticism (1 = - 3 6 and -.43). Correlation
between the LOT-R and the LOT (g = .95) for 2055 men and women support the
simiiarity of the questionnaires. (Scheier et al., 1994)
Self-Etncacv S c a l ~
Self-efficacy was measured ushg the SeLf-EfEcacy Scaie (SES) developed by
Rodin and McAvay (1992, see Appendk C). This measure was chosen because it was
short, easy to complete, and it had been used in several studies with older persons
(Seeman, Rodin, & Albert, L993). The SES was aiso the only available, generaüzed self-
efficacy measure found that was relevant to older persons.
Development
The SES was developed to assess self-efficacy, at nine points in the, in a
3-year longmiduid study of 264 community-dweiiing, individuals over the age of 62 years

(Rodin & McAvay, 1992). The original questionnaire assessed efficacy in eight domains
of living. A ninth domain, related to spousal relationship, was added in subsequent use of
the questionnaire. The original questionnaire also had a 1-month time hune attached to
each statement. Statements have since been revised to reflect current feelings of efficacy
(Seeman et al., 1993).
Description and Sc~nnq
The SES was developed to assess the extent to which respondents feel effective in
dealing with people and events in their lives and the degree to which they feel able to
influence things in life (Seeman et al., 1993). The SES addresses nine life domains of
particular relevance to older adults: health, transportation, finance, living arrangements,
productivity, safety, fiuniiy, fiiends, and spouse. Responses to the 9-item SES are
recorded on a Cpoint Likert scaie ranging fiom strongiy agree (1) to strongly disagree
(4). A score is obtained by summing the responses. Scores could range h m 8 (since the
ninth item is only included if the respondent is married) to 36, with lower scores reflecting
higher levels of self efficacy.
When the nine domains of the SES were correlated, two summary measures were
created. lnterpersonal efficacy was one summary measure derived Eom items dealing with
interpersonal relationships including family, Friends, and spouse. The other summary
measure, named instrumental efficacy, was derived from the items related to instrumental
activities such as transportation, safety, iïlivig arrangements, and productivity (Seernan, et
ai., 1993). Two items in the SES were excluded h m the 2 summary measures. The
question related to finances was excluded because it was found to relate equally to both
instrumentai and interpersonai efficacy. The question related to hedth efficacy was
excluded to minimize confounding with the heaith-related outcomes which the authon
were researching when they initialiy used the SES.
ReliabiIity
Reported use of the SES is lunited. The only infDrmation provided about
reliability was interitem correIations. Since the SES was developed to assess perceptions
of self-efficacy in nine life domains, and these domains were expected to be unrelateci,
interitem correlations were low, ranghg Eom -10 to -25. In addition, when the nine items

were categorized into two groups, correlations between the two "subscales" were Iow:
.42 and .58. Stability was suppoaed by test-retest correlations over 2 weeks of .74 and
.87. (Seeman et al., 1993)
Validity
Items used to develop the SES were reported to be valid by the Rodin and
McAvay (1992) as they are particularly relevant to older persons. However, specific
idormation about validity has not been published.
Persona1 Resources Questionnaire
Social support was measured by Part II of the Penonal Resources Questionnaire
(PRQIS) (Brandt & Weinert, 1985, see Appendk D). The PRQ85 is a widely-used,
nom-referenced measure of perceived availability of support.
DeveIo~ment
The original Personai Resources Questionnaire (PRQ) was a two-part measure
designed by Brandt and Weinert (198 1). Weiss's (1974) mode1 of relational fùnctions
provided the basis for the development of the PRQ. Weiss suggested that sociai
relationships had multiple fùnctions. Five of these were integrated in the development of
the PRQ: (a) opportunity for numirant behaviour, (b) social integration; (c) provision for
attachment/intimacy, (d) reassurance of worth; and (e) availability of iflormational,
emotional, and materiai help. The PRQ was modified in 1982 and refined in 1985 after
use in a vatiety of research projects.
Description and Scot-ing
The PRQ8S-Part LI, was used for this study because revisions to the wordiig of
items in the original instrument broadened the? appiicability to seniors and because of its
fit to the conceptualization of support for this study. The 25 items measures subjects'
perception of their social support as a composite of the dimensions of intimacy/assistance,
socîai integration~afikmation, and reciprocity (Weinert, 19 87). Responses are reco rded on
a %point Likert scaIe fiom strongiy disagree (1) to strongiy agree (7). After reversai of
the responses to negatively worded statements, a total score is calculated by adding the
scores of the 25 items. Scores can range fiom 25 to 175 with higher scores indicating
higher Ievels of perceived sociai support.

Reliability
Coefficient alpha reported for the PRQ8S-Part iI have been consistently over .80
(Lee, Graydon, & Ross, 199 1; Mahon & Yarcheski, 1988, 1992; Ploeg & Faux, 1989;
Weinert, 1987; Weinert & Brandt, 1987; Weinert & Tilden, 1990; White, Richter, & Fry,
1992; Yarcheski, Mahon, & Yarcheski, 1992; Yarcheski et al., 994). Thus internai
consistency has been well substantiated.
Stability was supponed by test-retest correlation of .72 over a 4 to 6 week interval
for the PRQ8S-Part L I in 100 adults, aged 30 to 37 years (Weinert & Brandt, 1987).
Vaddity
Content validity of the PRQ-Part II was initiaiiy established through evaluation of
the tool by experts in the area of sociai support who critiqued its content for clarity and
adequate representation of content domain. The content items were then categorized by a
group of graduate-prepared individuals with health or sociai science backgrounds and
items were deleted that were not categorized consistently.
Construct validity is Unponant when there is no accepted universal criterion or
content that entirely defhes the attribute to be measured (Weinert & Tilden, 1990).
Accumulation of support From many studies combine together to indicate that an
instrument measures what it proposes to measure. Construct validity was measured using
the 1982 version of the PRQ (PRQ82). The strength of correlations between the scores
obtained nom the Trait Anxiety Scale, the Beck Depression Inventory, and the PRQ82
demonstrated that the PRQ82 was measuring a construct consistent with that
conceptualized to be social support (Weinert, 1987).
Criterion validity was reported by Wehert and Tilden (1990) who examùied the
relationship between scores on the PRQSS-Part II to the Coa and Reciprocity hdex
(CRI) in two samples, 33 3 middle-aged adults and 99 adults. The CRI is a 3 8-item, self-
report questionnaire based on social exchange and equity theory (Tilden, Nelson, & May,
1992). The strength of the correlations were -58 and -53 respectively providhg support
that both instruments were measuring a sunilar constnrct (Weinert & TiIden, 1990). As
we& convergent validity was supported by correlations of -37 to -55 between scores on
the PRQ8S-Para and two memres of famiiy weil-beÏng, the Famiiy APGAR (Smilkstein,

1978) and the Spanier Dyadic Adjustment Scale (Spanier, L976), in the sarnple of 3 3 3
adults.
Data Analysis Plan
The data from the questionnaires were andyzed using the Statistical Package for
the Social Sciences (SPSS/PC+). Scores on each questionnaire were calculated according
to the instructions of the authors of each questionnaire and descriptive statistics were
displayed in table form. Interna1 consistency and distribution of questionnaire data were
evaluated before conducting data analysis.
Pearson Product Moment Correlation Coefficients (PPMCC) were computed to
determine the relationship among questionnaire scores in order to answer the first 6
research questions. To answer question # 7, PPMCC were computed arnong
questionnaire scores and personal characteristics that were interval level data (eg., age,
educational level). T-test and analysis of variance (ANOVA) were used to detemine
relationships arnong questionnaire scores and persona1 characteristics and heaith status
that were at nominal and ordinal levet of measurement-
Protection of Human Rights
This study was approved by The University of Western Ontario Review Board for
Health Sciences Research involving Human Subjects (see Appendix K). Approval was
granted by the directors of the participating centres to recruit potential participants within
their facilities. This approvaf was verbal at their preference, since formai processes for
approval did not exist in these facilities. AU potentiai participants received either verbal or
written Uiformation about the snidy prior to agreeing to participate. At the face-to-face
meeting to coUect data, the Letter of Monnation (see Appendix H) was reviewed and
subjects signed the Letter of Consent (see Appendix I). There were no identifîed risks
involved with participating in this study. However, given that the Iength of time required
to complete aii of the questionnaires may have caused fatigue for some older persons, they
were given the option of meeting more than once with the researcher to complete the
questionnaires.
AU ÏnteMews were held in the subjects' homes to maintain their privacy Names of
subjects did not appear on any questionnaire to maintah anonymrCty. Identification

numbers were assigned to each subject and aii data colIections forms were labelled with
the correspondhg number. The Est of subjects' narnes, addresses, phone numbers, and
code numbers was known oniy to the researcher and was destroyed at the end of data
collection. Actual data were reviewed oniy by the researcher and her advisor and were
entered into a cornputer using only the identification number. Oniy group data were used
in the analysis.

CHAPTER IV
RESULTS
The descriptive statistics including the characteristics of the sample and the means,
standard deviations, and range of scores calculated for instruments representing the major
study variables are described in this chapter. Subsequently, the results of the inferential
statistical analysis are reported for each research question.
Personal Characteristics of Community-Dwelling, Older Persons
The sarnple consisted of 39 community-dwelling, older women. They ranged in
age €tom 65 to 9 1 years with the mean age being 76.2 years of age (m = 6.1). Of the
sample 56.4% (IJ = 22) were widowed, 33.3% (a = 13) were mmied, 7.7% (a = 3) were
divorced, and 2.6% (Q = 1) were single. Slightly more that half of the sample had post-
secondary education (5 1.3%, n = 20), 4 1% (n = L6) had completed highschool, and only
7.7% (a = 3) had achieved public school education. The majority of the sample (66.7%.
n = 26) lived alone, while 28.2% (fi = L L) lived with their spouse. One person lived with
both her spouse and daughter and a second person lived with her daughter. Subjects who
lived alone were similar in age = 76.4 years, = 6.4) to subjects who lived with their
spouses and/or daughters a = 75.7 years, = 5.7).
Thirty-two ofthe 39 subjects (82.1%) reported available help nom family within a
one-hour drive. Sons, daughters, or daughters-in-law were named most often (87.5%.
n = 28) as the source of fimily help by those who had f d y available, followed by
nieceshep hews (6.3%, = 2) and sibhgs (6.3%, Q = 2). Younger subjects &f = 75.3,
se = 5.2) were more likely to have available f d y help wîthin a one-hour dnve than
older subjects (M = 80.1 years, = 8.6), but this diïerence for age was not significant
(l= 1.4, p= -19).
Thuty-eight of the 39 subjects (97.4%) reported that help was available Eom
friends who iived withùi a one-hour drive. Ten ofthe 38 subjects (26.3%) reported having
many fnends. 1 L (29%) narned a neighbour as the fiend who would help them out, and
13 (34.2%) subjects narned specinc Gends. The 4 (10.5%) remaining subjects did not
identify their tiiend.
The types of a&tles which the family and fnends "could do" for the subjects are
reported in Table 1. Over one-halfof the subjects with nearby family and just over

Table 1
Type and Frequency of Available KeIp fiom Farnil
Type of Help Family
Percent - n
Fnend
Percent ri
Do anything required
Do chores andlot home repairs
Assist with ADLs
Provide transportation
Run errands
Able to come if needed
Givdget immediate or needed help
Provide companionship
Wouldn't ask for help
one-quarter with nearby Eends reported that these individuais could do anything that
needed to be done. More than one-quarter of nearby fiiends and a few family memben
did chores andior home repairs. Other commonly reported things which both families and
%end could do were providing transportation, and running errands. Subjects dso
reported that some family (12.5%) and fiiends (26.2%) were also able to come ifneeded,
and give immediate or emergency help. Oniy a few subjects said that they had family
(a = 3) or fnend (a = 1) avdable but that they would not ask them for help
Heaith
The majority of subjects (56.4%, n = 22) rated their health as good, one-third rated
it as excellent (33.3%- n = 13)' while four subjects (10.3%) rated it as fair. No one rated
their heaith as poor. Most (69.2%, = 27) rated their curent health as unchanged from 6
months before the interview. Eight subjects (20.5%) rated it as better, and four (10.3%)
rated it as worse. Haif of the subjects @ = 19) reported that their health problems "did
not at aiin stand in the way of theu ddy actlvities or things which they wanted to do.

Fourteen subjects (36.8%) reported that their heaith problems interfered "a Utle" and 5
subjects (12.8%) reported "a great deai" of interference.
Specific Heaith Problems
Subjects reported a variety of health problems in their own words. These
problems included recognized medical diagnoses (e.g., gout) as well as description of
problematic symptoms (e.g., pain). The number of health problems per subject ranged
from O to 7 = 2.6. m= 1.5). Over one-haif of the subjects (53.9%, = 21) reported
two problems or less and 23% of the subjects (n = 9) reported four or more heaith
problems. The fiequency and type of health problems are reported in descending order by
fiequency in Table 2. In addition, the subjeas' perceptions of the amount of influence that
Table 3
Type of Health Problems and Amount of Influence on Dailv Activities
Type of Frequency of Amount of Influence
Heaith Problem Health Problem Not at al1 A little A great deal
Percent (4) Percent (n) Percent (n) Percent @)
Rheumatic
Cardiovascular
Vision or Kearing Loss
Gastro intestinal
Pain"
Recent surgeqdfiactures
~ndocnne"
41.7 (10) 20.8 (5)
18.8 ( 3) 25.0 (4)
44.4 ( 4) i L - i (L)
25.0 ( 2) 12.5 (1)
66.7 ( 4) 16-7 (1)
50.0 ( 3) 16.7 (1)
25.0 ( 1)
75.0 ( 3)
42.9 ( 6) 7.1 (1)
*generalized pain, headaches, backaches
bdiabetes, t hyroid condition C psoriasis, shingies, kidney Stones, weight ioss claustraphobia, depression, leukemia,
environmentai ilInas, breast lumps, "fiozenn shoulder. numbness in hands, prosthetic,
cholesterol osteo porosis

these problems had on their daily activities are reported in Table 2. The two most
cornmon types of health problems were various forms of rheumatic conditions (including
arthritic, bursitis, and gout) and cardiovascular problems (such as phlebitis, high blood
pressure, and edema). The rheumatic conditions interfered a little or a great deal with
activities for almost two-thirds of the subjects (62.5%) while just over one-third (37.5%)
reported no interference on their activities 60m their rheumatic conditions. Subjects with
cardiovascular problems reported sirnilar impact on activities. Overall, subjects reported a
total of 91 heaith problems of which only 15.5% @= 14) interfered a great deal with
subjects' activities.
Summary of Descriptive Statistics for Major Study Variables
The means, standard deviations, and range of scores for the Qudity of Life Index
(QLI) and its subscales, the Life Orientation Test (LOT), the Seff-Efficacy Scale (SES),
and Part il of the Personal Resource Questionnaire (PRQ85) are reported. Interna1
consistency of the questionnaire data was measured using Cronbach d p ha to deterrnine
reliability (see the following sections for each questionnaire). In addition, the data were
evaluated for nomd distribution to determine ifpararnetric statistical tests were
appropnate.
The distribution of participants' responses to the questionnaires was evaiuated by
calculation ofthe Pearson Skewness Coefficient using the formula reported by Munro and
Page (1 993). AU data were normdy distributed with the exception of the heaithlfunction
subscale of the QLI. Pearson Product Moment Correlation Coefficients, independent
t-tests, and analysis of variance were used for aIi nomaiiy distributed data Skewed data
were anaiysed using non pararnetric statistical tests; for exarnple, Kendali's tau for
correlations and Mann-Whitney U for t-tests.
Q&y of Life Index
Interna1 consistency of the QLI was evaiuated using Cronbach aipha to rneasure
reliability for the overaii scaie as weii as for the QLI subscales. Cronbach aipha for the
QLI was -75 meeting the criteeri of -70 for intemal consistency (Frank-Stromberg,
L988). Retiabiüty of two ofthe four subscaies was aIso acceptable, -82 for
psychologicai/spinhiai and -88 for heait6 Cronbach aipha for the socioeconomic subscaie

was .64 which fdls below the bits of acceptability. However, this subscaie was used for
subsequent analysis since .64 was close to the criterion for acceptability. Since Cronbach
alpha for the famiiy subscale was -.O 13 and, therefore, unacceptable, no findings related to
this subscaie are reported. Of note for al1 of these reliability estimates, the sample size
was less than the fil1 sample completion since some subjects did not answer al1 questions.
This is not uncornmon given the questions on the QLI are not applicable to al1 subjects.
For example, unrnanied or widowed subjects do not routinely answer questions regarding
their spousal relationship or sex Ise.
The rneans, standard deviations, and range ofscores for the overall QLI and its
subscales are reported in Table 3 : (a) health and functioning, @) socioeconomic,
and (c) psychologicaVspintuai. The reported means for the overail QLI and its subscales
were in the upper third of the possible range of scores. The socioeconornic subscale had
the smallest range of scores.
Table 3
ean. Standard Deviation. and Range of Scores for the Prima? Studv Variables: Oualitv
p f Life. Disoositional O~t~rnrsm. Se If Efficacy, and Perceived Social SUD DO^ . *
Variables Mean SD Range of Possible
Scores Range
Quality of Life Index
Overd 24-1 3 -0 14.3 - 28.4 O - 30
Subscales
Heaith 23.1 4.6 LO-9 - 28.6 O - 30
Socïoeconomic 25-2 2.9 18-4 - 39-6 O - 30
Psycho logical 24-0 4-1 10.4 - 30.0 O - 30 Life Orientation Test 22-5 4.2 11-0 - 31.0 O - 32
Self-Eficacy Scale 22.1 2.0 18-0 - 26.3 8 - 36
Personai Resource Questionnaire 142.5 6 108-0 - 172-0 25 - 175

Life Orientation Test
Cronbach alpha for the LOT-R was not acceptable (.34) and was weil below that of
the LOT. Therefore, the LOT-R was not used in any fùrther statistical analysis. Cronbach
alpha for the LOT was .69 just below the acceptable limit. AIthough the LOT was just
below the criterion of -70, it was used in the analyses because coefficients of -60 to .70 are
often acceptable for newly developed tools (Frank-Stromberg, 1988) and because
dispositional optimism as measured by the LOT was a major variable in the study.
The mean, standard deviation, and range of scores for the LOT are reported in
Table 3. The reported means for the LOT were in the upper half of the possible range
of scores.
Self-Efficacv Scale
Cronbach alpha for the SES was -28, well below the acceptable lirnit. This result
is slightly higher than previously reported intentem correlations which ranged fiom -10
to .25 (Seernan et ai., 1993), but was not unexpected since this questionnaire was
develoged to assess perceptions of self-efficacy in nine unrelated life domains. Since
~el~efficacy was a major variable in this study and resuits of the cronbach alpha are as
expected, the SES was used in the analyses.
The mean, standard deviation, and range of scores for the SES are reported in
Table 3. Ail of the reported scores for the SES were in the upper haif of the possible
range of scores.
Personal Resources Questionnaire
Cronbach alpha for the PRQ8S was -82, weli above the IeveI of acceptability.
This is consistent with the weil-substantiated reliability scores reported in the îiterature
and exceeds the -80 cntenon for reliability for established instruments (Frank-Stromberg,
1988).
The mean, standard deviation, and range of scores for the PRQ are reported in
Table 3. AU of the reported means were within the upper third of possible range of
scores. AU of the reported scores were weii within the upper halfof possible range of
scores.

Research Question One
The relationship between quaiity of lifie and dispositionai optimism for comrnunity-
dwelling, older persons was exarnined by caiculating Pearson Product-Moment
Correlation Coefficients between scores on the overali and three subscales of the QLI and
scores on the LOT (see Table 4). The correlation between the health subscale of the QLI
and the LOT were calculated using Kendall's tau. Statistically significant positive
correlations were found between scores on the overall QLI and the three subscales and
scores on the LOT. Those who reported higher quaiity of life were more optirnistic.
These findings suggest that overall quality of life is arongly associated with optimism.
Table 4
Correlations amo . . ne Ouality of Life. Disoositional Ootimism. Self-Efficacv. and Perceived
Social S u p p o ~
- - - -
Optimism SeEEfficacy Social Support
Quality of Life
Overd -63"" -12 -3 6*
Subscales
Heal t ha .33** .O3 - 33 -- Socioeconomic .4L* -14 -16
Psychological -65*** . L7 -41"
Optimism -,2 1 -3 8*
SeIf-Efficacy -00
*p c .os **g ' -0 1 ***a < .O00 1
%endall's tau used hstead of Pearson Product Moment Correlation.
Research Question Two
The relationship between quaiity of life and self-eficacy for comrnunity-dweiüng,
older persons was examhed using the appropriate correlation coefficients (see Table 4).
There was no statisticdy signincant relationship between quallty of Ee and seff-efficacy.

Research Question Three
The relationship between quality of life and perceived social support was examined
using the appropriate correlation coefficients (see Table 4). A statistically significant,
positive relationship was found between scores on the overall QLi and the PRQ85, and
between scores on the psychologicdspirituai subscaie and the PRQ8S. hdividuais who
reported higher quaiity of life had higher levels of perceived social suppon. Correlation
between the wo other quality of life subscales, healtWfùnction and socioeconomic, and
the PRQ8S were not significant.
Research Question Four
The relationship between dispositional optimism and self-efficacy was examined by
calculating the Pearson Product Moment Correlation Coefficient between scores on the
LOT and scores on the SES (see Table 4). There was no statistically significant
relationship between dispositionai optimism and selGefficacy found in this study.
Research Question Five
The relationship between dispositional optimism and perceived social support was
examined by calculating the correlation coefficient between scores on the LOT and scores
on the PRQSS (see Table 4). A significant positive relationship was found between
optimism and perceived social support. Individuals who were more optimistic reported
higher levels of perceived social support.
Research Question Six
The relationship between self-efficacy and perceived social support was examined
by calculating the correlation coefficient between scores on the SES and scores on the
PRQSS (see Table 4). No relationship was found between self-efficacy and perceived
social support.
Research Question Seven
The relationship among health and the primary study variables of quality of life,
dispositional O ptimism, seEefficacy, and perceived social support were examined. Healt h
data obtained fiom subjeas included: (a) overaii heaith rathg as excellent, good, fur, or
poor; @) rathg of health changes over the previous 6 months as better, about the same, or
worse; and (c) rating of impact of health on daily activities as not at aii, a iittle, or a great

deal. Analysis of variance (ANOVA) was used to examine the relationship arnong health
ratings and the four major study variables. Kendall's tau was used to determine the
relationship between the number ofhealth problems and the four major variables of the
study, since data on the number of heaith problems were not nomally distributed.
Findings are organized by the major study variables.
@di@ of Life and Health
The means and standard deviations obtained fiom the overall QLI and its
subscales, are reported in Table 5 by subjects' rating oftheir health as fair, good, or
excellent. Results of ANOVA are also reported in this table. AIthough there was a trend
for subjects who rated their health as excellent to report higher quality of life overall and
for the health subscale as compared to those who rated their health as good or fair, these
findings were not statisticaiiy significant (E = 2.4, p = -10). No relationship was found
between perceived changes in health status and quality of tif&
Table 5
Mean. Standard Deviation. and Analvsis of Variance for the Prirnanr Studv Vanables by
Ratine of Overall Kealth
Variables Ratings of Overail Health
Fair" (300db Excellentc F
M (Sie) M (SP) M (SPI Quality of Life
Overaii 22.9 (2.5) 23 -4 ( 2.9) 25.4 ( 2.9) 2-4
Subscales
Soc5oeconomic 26. 1 (2.8) 24.7 (3.0) 25.8 ( 2.7) 0.9
Psychological 21 -4 (2.8) 23.7 (4.1) 25.3 ( 4.1) L -6
Self-Efficacy 23.1 (2.3) 22.4 ( 1.6) 2 1 -7 ( 2.4) Q -9
Social Support 126.5 (3 -9) 145.8 (15.7) 142.3 (17.7) 2-5 O a=4 bn=22 'n= 13 AUgvaiues>.OS

The means and standard deviations obtained fiom the QLI and its subscales are
reported in Table 6 by subjects' rating of the impact which their general health problems
had on them doing their ddy activities. ANOVA are also reported in this table. A
significant relationship was found between overall quality of life scores and perceived
impact of health on activities. The greater the impact of heaith problems on subjects' daily
activities, the lower the overall quality of life. For the health subscale, this relationship
was even more significant (F = 7.0, = -003). These differences did not hold for the other
two subscaies.
On examination of the relationship of number of health problems to quality of life
oniy one of the relationships approached statistical significance. Subjects who reported a
greater number of health problems reported a lower quality of life for the
psychologicaVspi~tua1 subscale (u = -.22, p = .07).
Table 6
Mean. Standard Deviation. and Anal~sis of Variance for the Prima S t ~ d y Variables b~
Rating: of Impact of Health Problems on Dailv Activitie~
Variables Rating of Health Problem impact
Not at alla A ~ i t t l e ~ A Great ~ea l ' - F
M (SP) M (SPI M (se>
Overail 25.4 ( 2.5) 23.2 ( 3 -2) 22.3 ( 2.6) 4.0 * S ubscales
O ptimism 23.5 ( 3 -6) 22.6 ( 4.3) 19.4 ( 5.8) 1.9
Social Support 143.4 (14.3) 145.9 (19.6) 135.5 (10.6) -8 b n = 1 9 n=14 'Q=S - *p<.o5 **p<.OI.

Disoositionai Optimkm and Heaith
Although overd ratings of heaith were not related sigm*ficantly to dispositional
optimism (see Table 5), there was a trend for subjects who rated their heaith as excellent
to report greater optimism than those who rated their health as good or fair @ = 2.6,
9 = -09). There was no significant relationship between LOT scores and changes in health
status over the previous 6 rnonths (see Table 6). There was ais0 no relationship between
LOT scores and ratings of impact of health problems on daily activities. Subjects who
reported greater numbers of health pmblems reported significantly lower scores on the
LOT (m = -.33, g < .01). In other words, subjects with more health problems were less
optimistic than those with fewer heaith problems.
Self-Efficacy and Healtb
No significant relationships were found between self-efficacy and any health
ratings.
Perceived Social S ~ D O ~ and Health
No significant relationships were found between perceived social support and
various ratings of health. However, one interesting trend was observed. Subjects who
rated their health as excellent or good reported higher mean scores on the PRQ8S than
subjects who rated their health as fair (E = 2.5, p = -10; see Table 5). There was no
relationship between perceived social support and ratings of health changes in the previous
6 months. There was aiso no relationship between impact of health problems on daity
activities and perceived social support. However, subjects who had more health problems
had lower levels of perceived social support and this relationship almoa attained a level of
aatistical significance (m = -.22, p = -06).
Research Question Eight
nie eighth research question addressed the relationship among the nibjects'
persond characteristics and the prirnary study variables of quality of Ke, dispositionai
optùnism, self-efficacy, and perceived sociai support. Personal characteristics addressed
were age, marital status, Ievel of education, living arrangement (living alone or with some
one), and avaiiabihy o f f d y or fiiends.
Pearson Product-Moment Correlations were calculated between age and di scores
on the QLI, the exception of the hedth subscaie), the LOT, the SES, and the

PRQ85. Since data were skewed on the heaith subscaie of the QLI, Kendall's tau was
used to determine correlation. Independent t-tests were used to examine the daetences
berneen marital status, living arrangement, and availability of farnily and the major study
variables. ANOVA was calculated to test for âiierences in the major study variables for
level of education. Findings are organized by the four major study variables, quality of
We, dispositional optimism, self-efficacy, and perceived social support.
Quality of Life and Penonal Charactensttc~ * .
Marital status and education were the only two persona1 characteristics which were
found to be related to quality of life. Married subjects reported lower scores on the
overall QLI than not married subjects (see Table 7). Although the relationship between
maritai status and overaii quaiity of 1Ze was not statisticaily significant, it was significant
with the health subscale of quality of We. No relationship was found between the
socioeconornic and psychoIogicai/spintuaI subscaies of the QLI and marital status.
Individuais with higher levels of education reported a greater quality of life with the
Table 7
Variables Marriedu Not ~ ~ e d ~ 1 P
Mean Mean Sp
- - - - - --
Quality of Life
Overaii 22.9 3 -4 24.7 2-7 1.9 .O7
Subscaies
Health" 20.9 5 .O 24.1 4-0 2 2 -04
Socioeconornic 25-0 3 -2 25.4 2.8 0-4 -68
Psycho logical 22.7 5 .O 34-7 3.4 L-5 -15
Optimisrn 32-9 5-4 22-9 3.6 0-7 -48
Seif-Eficacy 22.5 2-0 22.1 1-9 -0-6 -55
Socid Support 142-5 17-5 142.5 16.3 0-0 1.00

65
exception of the public school group (see Table 8). Since, the number of individuals who
made up the public school group was smail, it was not as representative oflevel of
education as the other three groups. For the subscales of the QLI this relationship
between education and quality of iife was significant only for the socioeconomic subscale.
Table 8
ean. Standard Deviation. and Analvsis of Variance for the Prim Study Variables by
Level of Forma1 Education
Vanab les Education
~ublic' EIighb Post HighC universityd E School School Certificate Degree
M (ml M(Se) M M (Sol
Quality of Life
Overail
Subscaies
Mealt h
Socioeconomic
Psychological
Optimism
Self-Efficacy
Social Support
- --
a n=3 bn=16 'n=6 dfi=14. *p<.05
Age, living situation, and availability of family were not found to be related to
quality of Ke. Andysis for data for subjects with nlends versus no friends was not done
because only one subject reported have no fiend avaiiable. Aithough subjects who lived
alone reported overaii higher scores on the QLI than subjects who h e d with thei.
husbands d o t daughter, this dierence was not signincant

. . Dispositional Optimism and Personai Characteristics
No significant relationships were found between dispositional optimism and any of
the persond characteristics.
SelCEfficacv and Persona1 Characteristics
No significant relationships were found between self-efficacy and any of the
personal characteristics.
Perceived Social Suport and Persona1 Charactenstic~ * *
A significant, negative relationship existed between subjects' perceived
sociai support and their age (1 = 0.52, p = .O0 1). Older subjects reported lower perceived
social support t han younger subjects.
Several other observations are worth noting but none of them reached statistical
significance. There was a trend for subjects with poa high school education to report
higher levels of perceived sociai support than those with only public and high school
education (E = 1.7, p = -19; see Table 8). Subjects who did not [ive alone also tended to
report higher levels of perceived support than those who lived alone (t = 1.3, p = -19). As
well, subjects who reported family availability wth a one-hour drive reported higher
perceived social support than subjects without family but this difFerence was also not
significant (t = 1.3, a= -19). There was no reported difference between perceived social
support for married and not manied subjects.
s-ary There were several significant results reported for al1 of the study van-ables except
self-efficacy. Findings are summarired for research questions one through six, research
question seven and research question eight.
Research Ouestions One to Six
Research questions one to six addressed the relationship among the major study
variables, quality of life, dispositional op timism, self-efficacy, and perceived socid
support- A strong positive relationship was found between dispositional O ptimism and
overali quatity of Key and for the psychologicaVspiritual subscale. A positive relationship
was also found between dispositionai optimism and the health/function and socioeconornic
subscales for quality oflife- Perceived adequacy ofsocid support was aiso related to

overail quality of We and the psychological/spiritual subscale. Correlations between
quality of life and social support strengthened slightly when partial correlations were
computed controüing for age. In addition, the relationship between dispositionai optimism
and perceived sociai support was found to be signincant: Subjects who reported higher
levels ofoptimism reported higher levels of perceived social support.
Research Ouest ion Seven
There were two significant relationships found arnong heaith and the study
variables quality of life, ddispo sitional op timism, self-efficacy, and perceived social support.
First, a signincant relationship was found between the perceived impact of health problems
on subjects' ability to carry out their daily activities and their reported quality of life. The
less that the health problems were reported to have an impact on daily activitieq the higher
the subjects' overall quality of life, more specitically the health subscale.
Secondly, pesons who reported greater number of health problems had
significantly lower optimism than subjects who had fewer health problems. Subjects who
reported more health problems aiso reported a lower quality of life and lower perceived
social support than subjects with fewer health problems although these relationships only
approached statistical significance. No significant relationships were found between self-
efficacy and heaith, and perceived social support and heaith.
esearch Ouestion E i ~ h t
Higher quality of life was found to be related to f o n d education- Subjects who
had achieved higher levels of education reported better quality of life in both the overall
and socioeconomic domains. Marital status was also found to be related to quality of life,
but the reIationship between marital status and quaiîty of life oniy reached signifïcance for
the heaith/fÙnction subscaie. Subjects who were not m h e d reported higher quality of life
than those who were married.
Perceived social support was found to be negatively correiated to age. Younger
subjects tended to reported higher levels of social support than older subjects. No other
statisticaliy significant relationships were found between the major study variables and
personai c haracteristlcs.

CHAP'rERv
DISCUSSION
In this chapter the results, meaning, implications, and limitations of the study are
discussed. Comparisons are made between the characteristics of the sample for this study
and other study samples of community-dwelling, older persons. The examination of the
study results is organized according to the research questions. The remainder of the
chapter is organized as follows: (a) limitations of the study; (b) implications for nursing
practice, administration, and education; and (c) suggestions for future research.
Characteristics of the Sample
Comparisons are made between the characteristics of subjects in this study and
available information about the characteristics of the older, Canadian, community-
dwelling, population. This study examined four pnmary variables: quality of life,
dispositionai optimism, self-efficacy, and perceived social suppon. Since no other study
was found in which al1 of these variables were addressed, cornparisons are made for each
of these variables with findings in other studies.
Characteristics of the current sample were found to be similar to previous studies
for age, number of health problems, and rating of health. The current sample was
dissimilar to many other relevant samples for sex, marital status, level of formal education,
and living arrangements.
The average age of the women in this study, 76 years, was consistent with a large,
representative sample of community-dweiiing, older Canadian women in a study ofwell-
behg by Gooding et al. (1988). Aithough moa other studies of older persons over the
age of 65 years included both men and women, the average age of the women in this study
was consistent with many of these other studies (Foxali et ai., 1994; Girzada et al., L993 ;
Sharpe et al., 1994).
Fewer subjects in this study (one-third) were married than reported in moa other
studies. Although the proportion of those who were mamed was similar to that in studies
by Medley (1980) and Ploeg and Faux (1989), in most other studies, approlùmately two-
thirds of the sample were married (Goodhg et al., 1988; Grembowski et aL, 1993;
Newsom & Schuh, 1996).

The average number of years of fonnai education of this study sample tended to be
much higher than found in the majority of studies of older persons (Ausiander & Litwin,
199 1 ; Krause, 1987; Ploeg & Faux, 1989; Stoller & Pugliesi, L99 1). In this study, most
subjects had finished high school and over one-haif of the subjects had some poa high-
school education. In other studies of older persons (noted above), subjects had an average
of 10 years of formai education and less than one fifth had attended university.
Living arrangements of subjects in this sample also dEered significantly from those
of subjects in other samples. Slightly more than one-quarter of the sample in the study by
Gooding et al. (1988) lived alone compared to a rnuch larger proportion, two-thirds, of
the sample in this study.
The number of health problems reported by the women in this study was consistent
with the reported rates for older Canadian women (Novak, 1993). Although many of the
women in this study reported health problems, most of them rated their health as either
good or excellent. This report of good health was comparable to that reported by
Lindgren, Svardsudd, and Tibblin (1994) in their study of the health of 959 individuals
aged 75 years and older where the majority of subjects (87%) rated theû heaith as good,
even though they reported a variety of health problems. The rating was also similar to a
study of older women reported by Barron et ai. (1992), in which most ofthe 56 women
who had chronic health problems rated theù overall health as either good or excellent.
Prirnarv Studv Variables
Scores obtained on the Quality of Life Index (QLI), SeEEfficacy Scale (SES), and
Personal Resource Questionnaire (PRQIS), in this sarnple, diered somewhat from those
obtained in other related sarnples. Scores obtained on the Life Orientation Test (LOT) in
this sample were sirniiar to those obtained fiom a varîety of other studies.
Aithough there is no sampIe of community-dweüing, oIder persons with which to
compare quaiity of Ke, scores reported on the QLI in thîs audy were higher than those
reported in other studies using the QU (Belec, 1992; BiiIey & Ferrans, 1993; Dunn,
Lewis Borner, & Meize-Grochowski, L994; Htcks et ai., 1992). As weli, standard
deviations were not as large in this study as h other studies. Differences in age and heakh
status between sarnpIe groups is likely the reason for differences h reported quality of We.

Subjects in the other studies represented a wkie vaciety of age groups and were either
undergoing or recovering fiom major *hesses or surgical events. Since age and health
can infiuence quaiity of Me significantly, lower quality of life and greater fluctuation in
scores would be expected for this sample (Abeles et al., 1994; Lawson 1978). However,
quality of Life scores obtained in this study may be typical for the older, healthy,
community-dwelling population, but confirmation wiii require fùrther exploration.
Scores obtained on the LOT for this study were similar to those obtained by
Guarnera and Williams (1987) in their study ofcomrnunity-dweüing, older persons. LOT
scores were also similar to those in other studies in which dispositional optimism was
measured even though the samples in the other studies differed significantly from the
current study (Barron et al., 1992; Guarnem & Williams, 1987; Long & Sangster, 1993 ;
Scheier & Carver, 1985). This finding supports the beliefof Scheier and Carver (1987)
that dispositional optUnism is a relatively stable personality trait. If dispositional optimism
is a trait which remains stable across tirne. scores on the LOT should be consistent across
vanous age groups.
The generalized self-efficacy betiefs of the women in this study were lower than
the self-efficacy of wornen in a large, longitudinal study of comunity-dwelling, older
persons in which the same questionnaire, the SES, was used to measure generalized self-
efficacy (Seeman et al., 1993). Tho results obtained on the SES for this study may not be
a true reflection of the self-efficacy betiefs of the sarnple. Early in the data collection
process, it became evident that the responses which many of the women were rnaking to
specinc questions on the SES were not consistent with their verbal anecdotes and
explanations. This concem about the validity of the SES is explained in greater detail in
the discussion on limitations of the study.
Scores obtained on the PRQSS for this study were siightly higher than those
obtained in other studies of similar and diverse populations (Conn, Taylor, & Hayes, 1992;
Ploeg & Faw, 1989; Weinert & Long, 1993; Yarcheski et ai., 1994). These sightiy
higher scores indicate that the sample in this study perceived their satisfaction with soàd
support to be greater than reported typicaiiy. Since subjects in this study dso rated theu
quaiity of Me as higher than subjects in many other similar hidies, findings of higher

perceived social support are not surprising, since social support has been shown to be
related to quality of life (Newsom & Schulz, 1996; Rickelman et al., 1994).
Research Question One
The first research question considered the relationship between quality of life and
dispositional optimism. Subjects with higher levels of optirnism reported significantly
higher overali quality of lie and this relationship held for the three quality of life domains,
psychologicaVspintual, heaithlfunction, and socioeconom*c. These findings support those
of other studies in which dispositional optimism was found to be associated with higher
levels of subjective well-being and lower levels of psychological distress in a variety of
populations (Scheier â: Carver, 1987, 1 992).
tn the current study, quality of life was conceptualized as the goal, which is both
intluenced by and influences factors which determine behaviour. Dispositional optimism is
an important factor in goal attainment in that optimistic individuals strive towards goal
attainment even when faced with adversity. The positive relationship between quality of
Life and dispositionai optimism found in this study supports this conceptualization.
Aithough the reason optimistic people have a higher quality of life is not known,
Scheier and Carver (1987) have suggested that this may happen because these individuais
are able to develop more effective coping mechankms which assist them in dealing with
the stress and difncult situations they encounter in their iives. In general, more optimîstic
people have been found to use coping strate@ that are active and problem-focuseci.
Optimists are much less likely to use strategies such as deniaf or withdrawal or to become
preoccupied wit h negative emotions secondary to the stress (Carver et ai., 1993; Friedman
et al., 1992; Fontaine, Manstead, & Wagner, 1993; Scheier et ai., 1986). It is beyond the
scope of the current study to speculate about the coping stytes of the subjects who were
intem-ewed, however, consideration that there are Merences in how persons manage
their every day lives warrants fiirther investigation.
Consideration shouid dso be &en to the possibiiity that optimïsrn distorts the
recall of events. It is possible that more optirnistic îndividuals recaii more positive events
and thus report higher quality of Life while those who are Iess optimistic recail more
negative events and report Iower quality of Life-

Anecdotal Uiformation provided by the women in this study supported both of
these explanations for the relationship between quality of Iife and optimism. Coping
strategies described by the women in this group included: (a) f i th in God; (b) reliance on
good fiiends; (c) accepting what life offered including Ioss of spouse, and health
limitations; and (d) focusing on what one could still do rather than what had been lost.
Other comments expressed frequently during interviews were: feeling blessed, feeling
gratetiil, feeling lucky, wanting for nothg, and being satistied with what was since things
"could be a lot worse".
Research Question Two
No relationship was found between quality of life and self-efficacy in this study.
Aithough research addressing the relationship between these two variables is limited,
studies in which self-efficacy and components of quality of life have been examined have
reported strong correlations (Cunningham et al., 1991; Dornelas et al., 1994).
The lack of any relationship between quality of life and ~e~eff icacy in this study
may stem eorn the foiiowing considerations: (a) data obtained on the Self-Efficacy Scaie
(SES) in this study rnay not have accurately reflected the efficacious beliefs of the
subjects, (b) self-efficacy can only be reliably measured for specinc behaviours, and (c) the
generaiized measure of self-efficacy used in this study did not relate to areas of satisfaction
and importance that were addressed in the quaiity of life measure. The vaiidity and
retiabiiity of the data obtained on the SES in this study have been questioned. As
mentioned previously, concems about the SES are further discussed under Limitations of
the study.
The relationship between self-efficacy and quality of life has been found to exist
when specific self-efficacy behaviours were measured and their relationship to select
components of quality of life was studied* Finding a relationship between self-efficacy
and specific outcomes is consistent with Bandura's (1982) conceptuaiization of self-
efficacy. He proposed that individuals have efficacy expectancies about their abüity to
perform certain behavioun in order to achieve specifïc outcomes. Ifindividuals judge
themselves to be competent and capable of achieving certain outcomes in specinc
situations, then they wiii initiate specinc behaviours dïrected towards attainùig those

outcomes.
In their conceptual framework, Scheier and Carver (1987) agreed to some extent
with Bandura's conceptuaikation of self-efficacy but only in specific situations. They
agreed that seIf-efficacy was an important factor in the development of favourable
outcome expectancies for succesfiI goal attainment when the goal is very specific.
However, they proposed that when a goal is more generalized, that generalized
expectancies would be better predictors ofgoai attainment. They acknowledged that
attempts to study the predictive power of generalized expectancies have not met with
much success. This lack of success may result h m the specifics of the expectancy not
matching the specüics of the goal.
In this study, the Quality of Lüe Index (QLI) was used to determine global quality
of life through the subjective evaluation of the satisfaction with and importance of 1 8 areas
of Me. The SeKEfficacy Scale (SES) was used to determine subjects' generalized self-
efficacy perceptions in nine tife domains. It is possible that domains addressed by the SES
were not matched to areas of satisfaction and importance addressed by the QU. In other
words, judgernents of self-efficacy in areas addressed by the SES, such as arranging
transportation, being productive, and controllhg living arrangements, may not have been
relevant to areas of satisfaction and importance addressed by the QLI for women in this
study. It may be that self-efficacy which is considered to be act-specinc can oniy be
measured as part of act-specific behaviour towards specific outcomes and that atternpts to
use a generalized measure to capture self-efficacy prove ineffective.
Research Question Three
The third research question considered the relationship of quality of lûe and
perceived sociai support. As expected, a moderate, positive relationship was found
between overall quaiity of life and perceived sociai support. Individuals in this study who
repo rted greater quality of Life aiso reported greater perceived social support. This
relationship heId for one specinc puality of We domain, psychologicaVspintua1, but not for
the O ther two domains, healthlfùnctîon and socioeconomic. The relationship between
qualÏty of Iife and sociai support is consistent with hdings ofother studies of ofder
persons in which thÏs relationship was exarnined (Newsom & Schuiz 1996; Ploeg & Faux,

L989). Adequate social support is an important component in the maintainence of quality
of lik
This finding is congruent with the conceptual model used in this study. In this
model, many factors, including extemal circumstances can influence behaviour toward
goal attainment. Two-thirds of the women in this study had been widowed, many had
undergone dramatic changes in their health status, and in their living arrangements, yet
they reported a relatively high quality of life. The relationship found between social
support and quality of lie indicates that adequacy of their social support was likely one of
the factors which contributed to their ability to maintain their quality of Me. As well,
their high qudity of lie rnay have provided them with opportunities to maintain adequate
social support.
Research Question Four
In this study, no relationship was found between dispositional optimism and self-
efficacy. As mentioned previously, hdings with the SES must be questioned based on
problems with measurement. Only one other study was found in which the relationship
between these two variables has been reponed. Friedman et al. (1994) studied the
relationship among predictors of self-efficacy regardiig breast self-examination and
dispositionai optimism for a large number of middle-aged women. Moderate correlations
were found between self-efficacy and breast examination, whereas no relationship was
found between optimisrn and breast examination.
in Friedman et al.'s (1994) study, self-efficacy, not optimism, was the strongest
predictor of the behaviour to engage in self-breast examination. Findings Corn their study
are congruent with Scheier and Carver's (1987) view of the roie of self-efficacy in act-
specEc situations. in act-specific situations, self-efficacy may be the determining factor in
the decision to engage in a behaviour. In situations that are more globaî, dispositional
optllnism may be the detemiinllig factor. It is also possible that a number of factors, in
combination, influence behaviour towards a goal.
Friedman et ai. (1994) found a very weak relationship between self-efficacy and
dispositional O ptimisrn which indicates that a sense of O ptimisrn may be imposant for
greater self-efficacy It may also be that individuals who experience greater self-efncacy

may be more optimistic. Although women in Friedman et al's study were on average 30
years younger than in the current study, age should not have a bearing on the results, since
neither dispositional optimism or self-efficacy have been found to be related to age
(Grembowski et ai., 1993).
Research Question Five
A significant positive relationship was found between dispositional optimisrn and
perceived adequacy of social support. Subjeds who were more optimktic reponed higher
levels of perceived social support. Similady, subjects who were less optimistic reported
lower levels of perceived support. This fhding is consistent with that reported by Barron
et al. (1992) in a study of comrnunity-dwelling, older women with similar personal
characteristics to the cunent study. Barron et al. found a relationship between both
dispositional optirnism and social network size, and between dispositional optimism and
satisfaction with social support.
In the conceptual mode1 which guided this study, Scheier and Carver (1987)
described dispositional optimisrn as a relatively stable personaiity trait. Optirnists tend to
continue to work towards attainment of goals even when faced with difiïculties and
adversities. One of the ways in which optimists deal with stressful situations is to seek out
social support (Billingsley et al., 1993; Scheier et al., 1985). ifoptimias have a greater
tendency to seek out social support, then as long as they remain optirristic, their feelings
of adequacy and satisfaction with this support is likely to be high.
Severai reseatchers have questioned the stability of optimism, specificaliy in older
persons and have proposed that optimism can be infhenced, either positiveIy or
negatively, b y various factors in individuals üves or environment (Marshail, Wortman,
Kusulas, H e ~ * g , & Vickers, 1992; Shinen, 1996; Shifien & Hooker, 1992; Sharpe et al.,
1994). Health, emotionai fluctuations, and daily life events or stressors have been
identified as factors which cm inauence optimism. Sharpe et ai. found that measuring
optimism ofolder persons at two times was not as stable as found in younger populations.
They suggested that this greater inaabiiïty in optimism mÏght occur because of decreased
overaii stabüïty in üfe events hcluding such things as mess, Ioss of fûnctionai ability, and
death ofloved ones. Knowing that a relationship exists between s o d support and

optirnism, and given that the stability of optimism is questionable, suggests that social
support may be as important to maintaining optirnism as optimisrn is to maintaining social
support.
Research Question Six
No relationship was found between self-etticacy and perceived adequacy of sociai
support in this study. Only a few studies have been conducted in which the relationship
between self-efficacy and social support was examined (Barlow et al., 1996; Taal et al.,
1996).
Barlow et al. (1996) reported the ody positive relationship between satisfaction
with social support and generalized ~e~efficacy. Unlike the generalized self-efficacy tool
used in the current study, the generalized self-efficacy tool used in the study by Barlow et
al. did not focus on various domains of life but instead focused on feelings of efficacy such
as problern solving, confidence, coping, and resourcefùlness. This difference in approach
to generalized self-efficacy may explain the variation in outcome between the study by
Barlow et al. and the current study.
It would be reasonable to expect to h d a relationship between feelings of
generaiized self-efficacy and perceived social support. The behaviours of persons with
arong global feelings of self-efficacy would promote acquisition of sociai support
necessary to meet their needs. Lack of fhding this relationship in the current study may
be because of the previously mentioned concerns regarding : (a) the accuracy of the
questionnaire used to measure self-efficacy beliefi of the women in this study, and (b) the
possibility that the areas measured on the SES did not correspond to areas measured on
the sociai support questionnaire.
Research Question Seven
nie relationships among health and the major study variables were addressed in
the seventh research question Health was measured ushg four single qum-ons which
addressed: (a) rating of current heafth, @) cornparison of current health to previous health
stattq (c) rating of impact of heaith on daiiy activities, and (d) number of hedth problems.
Women with better selfrated heakh reported greater quality of We, opptimism, and
adequacy of social support than women wïth poorer health In addition, the more that

health had an impact on the daily activities in these womens' lives the lower they rated
their quality of life. Examination of the relationship between the number of health
problerns which these women reported and their quality of lEe reveaied that, although
women who reported more health problems aiso reported lower quality of l i i this
relationship was not significant. In other words, the perceived impact of health problems
was a better indicator of quality oflife than the number of actual health problems. This
finding is consistent with other studies which have found selerated health to be a better
predictor of quality of life than actual health problems (Banon et al., 1992; Rodin &
McAvay, 1992; Osberg et al., 1987).
No relationships were found between cornparisons of current health to previous
health and quality of Iife. This result may be because most women rated their health as
unchanged. In cases where the women reported their health as better, temporary health
problems had resolved and their health had retumed to a previous status.
Perceptions of health contniute positively ancüor negatively to quaiity of life.
People often perceive their heaith to be excellent or good even when they have severai
chronic health problems or disabiüties. Since perceived health is a better predictor of
quality of Mie than actual health problems a better understanding is required of factors
which individuals consider when they rate theu heaith and quaiity of life. Knowing what
factors are taken into consideration when heaith is rated can provide important
uiformation about the relationship between hedth and quaiity of Ee.
interestingly, the relationship between heaith and dispositional optimism existed
for only one measure of health status, the number of health problems reported by the
women in this study. Women who reported a greater number ofhealth problems reported
lower levels of optimism This finding supports previous research findings, aithough most
of these studies addressed relationships between health and dispositional optimism in
younger populations (Scheier & Carver, 1987; Scheier et ai., 1989). Individuals who were
assessed to be more optllnistic have generdy reported fewer iliness syrnptoms or heaith
problems.
Heaith problems may signincantiy affect everyday Mie. In attemgting to deal with
heaith probIems, individuals ofken need to take decisive action towards improvirtg their

hedth or make adjustments in daily living to deal with these problems. In the conceptual
fiarnework used to guide this study, optimism was seen as an intemal resource which
influenced the expectancies of persons in goal attainment. Scheier and Carver (1987)
suggested that optimistic individuals strive for goal attainment even when faced with
adversity. However, even though individuais rnay have optimistic dispositions, those with
more heaith problems rnay have di.culty dealing with the impact that these problems have
on their everyday lives. Their sense of optimism rnay decline as it becomes more difficult
to make the necessary adjustments.
Perceptions of health in this study were not found to be related to perceived social
support. A relationship that approached statistical significance was found between social
support and both curent heaith status and number of reported heaith problems. Women
who reponed poorer health and more problems tended to report Iower perceived social
support. The women in this study reported several problems that specincally interfered
with their continued invohernent in various socid and church related activities: bowet
incontinence, pain, s h conditions, sensory deficits, and decreased mobiiity. These
findings support the conclusions by Bowling, Farquhar, Grundy, and Formby (1993) that
health problems rnay interfere with the ability to engage in desired social activities.
Social support is an important correlate of quality of Me. Health factors which
affect older persons' ability to maintain adequate social support rnay iduence their quality
of Ke. In Carver and Scheier's (1982) behavioural feedback system, changes in goal
achievement influence various internai and extemal resources which in mm affect
subsequent goal achievement. Early targeting of internai or extemal resources to deal
with the impact of heaith problems rnay prevent such negative consequences.
Research Question Eight
Severai relationships were found among personal characteristics and the major
study variables. Significant relationships were found between: (a) years of formal
education and quality of Mie, and @) age and perceived social support In addition, the
relationship between marital status and quality of life approached statistical significance.
Individuais in this study who had more years of formai education reported better
quality of Iife than indMduals who had fewer years offormal education Signincant

relationships between education and quaiity of life have not been reported in previous
studies ofolder persons. Relationships in this study rnay have occurred because a larger
proportion of this sample had higher levels of education than samples in most studies of
older persons. Although this sample is not representative ofthe educational status of the
older population, there is no reason to suggest that the relationship found between
education and quality of lXe is not plausible. This relationship between education and
quality of life may be secondary to the standard of living which those with more forma1
education generdy acquire. Socioeconomic status and standard of living have been
reported to be related to quality oflife (Ferrans, 1990; Medley, 1980; Stewart & King,
1994).
Although women in this study with more education reported higher quality of life,
16 individuals in this sample, in response to the single question in the Quality of Life Index
about satisfaction with education, expressed regrets about not having more education.
Although many of these women had a signincant number of years of formal education, the
regret expressed stemrned fiom not being able to do more or not having a choice in the
type of education which they had received. This regret about education is supportive of
several other studies which addressed regrets in older women (DeGenova, 1996).
The relationship found between age and social support is not surprising. Older
women reported lower levels of perceived social support than younger women in this
study. Changes in health and activity and changes in social network sue that are
associated with aging may explain the relationship between age and social support, in part.
Older wornen in this study reported a greater number of health problems and more often
reported worsening health than younger women Declinuig heaith may explain part of the
relationship found between age and social support.
in this study, ma"ed women reported lower overali quality of We t han non-
mamed women, although this relationship did not quite reach a Ievel of significance. The
relationship between marital statu and quaiity of We found in this study did not nippon
the relationship that has been found in most other studies (Girzadas et al., 1993; Larson,
1978). In most studies, mamed îndividuds tend to report higher weU-being and q u a 4 of
Ke. The proportion of unrnarrïed women in the current midy was not consistent with

many other samples in which the relationship between marital status and quality of life was
addressed. The low number of married women in the current study rnay have influenced
the results since several of these women expressed dissatisfaction with their marital status
and a few expressed signincant concern about the health of their spouse. The lower
quality of life for manied women rnay have resulted fiom issues related to their spouse
which had a negative impact on areas of importance for their quality of Iifie.
Limitations of the Study
Several limitations of the current study need to be addressed. Interpretation of the
study results should be done with consideration of (a) the sample, and @) measurement
issues.
The srnall sample ske and participation of only wornen in this study limit the
generalizability of the findings. Although there was enough power to detect significant
relationships among major study variables, the sample size rnay have resulted in some
clinically sipifIcant findings not achieving statistical significance.
nie education levels and marital status of this sample were not reflective of the
those in many other samples, especially for the older, Canadian, community-dweliing
population. As weli, the methods used for recruitment ofsubjeas rnay have limited the
diversity of the sample. Comunity-dweüing, older women who did not participate in
church and community activities were unlikely to be recmited for this study as the majority
of subjects were recmited through church, social, and recreationai involvement.
Individuals over the age of 65 years fom a more diverse group than those in any
other age-related population. This divenity stems fkom the number and variabüity of
experiences they have encountered over t h e as well as the wide range in age, health
status, and functionai abüity (Lawton & Herzog, 199 1; O'Brien & Gonger, 199 1;
Peterson, 1994; Wfiarns, 1990). Therefore, what is found to apply to one group of older
persons rnay not automaticdy translate to another group of older persons. Results Eom
this study rnay oniy be applicable to a d a r population of older women-
In this study, there were no relationships found between seKefficacy and the other
major variables. The conceptuai tiamework used to guide this study and resuits from
many other studies suggest that such reIationships should have been found. Severai issues

related to the questionnaire used to measure self-efficacy in this study may have influenced
the resdts.
The SelGEnicacy Scale (SES) used to measure generalized self-efficacy may not
have measured what it was proposed to measure. Validity has been reported by the
developers of the tool, but specincs regarding zttainment of this validity and specific
measures of validity have not been reponed.
For two questions on the SES, subjects' responses on the scale were not consistent
with their verbal comments about the statements. Subjects ofien disagreed with the
statements: "There are things 1 could do to make myself safer" and ' I I could make my
financial situation better if1 wanted to". With prompting, as suggested by the authors of
the SES, some subjects aitered their responses to indicate agreement but at least half of
the subjects scored disagreement with one or both of these statements. Their rationale for
disagreeing with these statements was primarily that they had aiready done everything they
felt needed to be done and they had chosen not to do anything more. These comments to
the researcher indicated that subjects beüeved in their ability to deal with their own safety
and financiai situations and had, in fact, aiready acted on their beliefs. Thus, their negative
responses on the SES to these statements were inconsistent with their actual self-efficacy
beliefs.
In addition, the attempt to measure self-efficacy tiom a global perspective
congruent with Scheier and Carver's conceptuai framework ofbehavioural self-regulation
may not have been appropriate. Scheier and Cmer (1987) suggest that self-efficacy is an
important component in specinc situations where specific outcornes are targeted. As a
concept, seLf-efficacy may not be meaurable nom a global perspective. As weli,
components that were measured by the SES rnay not have been related to quaihy of life or
perceived social support for subjects in this study.
Despite these limitations there are reasons to beiieve that many of the study results
are valid. Most of the significant findongs mpported sllniIar findïngs fkom O t her research
midies with diverse sarnples.
Implications of the Study
The findings of this study have implications for nursing practice, nursing

administration, and nursing education. Greater quaiity of life was assotiated with higher
levels of optimism, greater perceived adequacy of social support, and better overall health.
Optimism and social support were also found to be related. Levels of education were
associated with quality of life and social support diminished as individuais aged.
hplications of these findings are discussed in the following three sections.
Nursing Practice
Quality of life and factors which related to quality of life are important for
practicing nurses to understand. The findings of this study suggest that feelings of
opthïsm, perceived social support, and perceived health status are related to quality of
Iife of comrnunity-dwelling, older persons.
In this study a sense of optimism and greater adequacy of social support were
found to be related to quaiity of Iife. Individuals who were more optimistic enjoyed a
higher quality of üfe than less optimistic individuals. Individuals with greater perceived
social support also enjoyed a higher quality of Iife. Iffeelings of optimism and perceived
adequacy of social support are important correlates ofquality of iife then assessment of
optimism and perceived social support may assist nurses to identifjr persons whose quality
of life is at nsk of declining. Assessing these varîables will require finding reiiable
assessment tools and incorporating them into nursing practice. The questionnaires used in
this study provide tools to conduct such an issessment, although shorter measures may be
required in practice for ease of use.
Developing a better understanding of why individuals who are more optirnistic do
better than those who are less optimistic, is essential to determinhg appropriate nuning
care. Nurses are provided with reasons for developing interventions ifthey know that
individuais who are more optimistic are more iikely to: (a) continue to strive towards
goals in the face of adversity, @) accept the reaiity of situations, and (c) use a probiem-
solWig approach to deai with stressfui events. Since optunistic, oider persons are more
iikely to be able to ded with stressful events, additional nursing support may oniy be
needed by those who have Iittie optimism. This support rnay involve: (a) coachhg the
individual to use effective problem-so lving methods to deai with situations; (b) providing
additiond resources for a penod oftirne to reduce the effects of a stressfui situation,

a d o r (c) helping the individual to come to ternis with situations and to focus on dealing
with reality.
Consistent with other studies, the older women in this study whose health affected
theu ability to engage in daily activities reported a lower quality of life. As well, older
women reported a greater number of health problems than younger women and those with
more health problems reported less optimism. Since older persons are at greater risk for
health problems than younger persons and health problems are related to quality of life,
timely implementation of heaith maintenance strategies, such as exercise and wellness
programs, could prevent deterioration in both health and quality of We.
It is important for nurses to provide older persons with the oppominity to not only
descnbe their health problems but also to describe the impact that those problems have on
their daiiy Iives. Health problem which nurses may consider to be minor concems may in
fact, have a significant impact on older persons' daily We. For example, heaith problems
mentioned by the women in this shidy including psorasis, hearing loss, incontinence,
artluitis, pain, and aiterations in mobiiity, prevented many of them from engaging in social
activities and relationships which they once enjoyed.
The importance of socialization has been weli-documented. Diminished
socialization may place the older person at an even greater risk for senous negative health
consequences and diminished quality of Ke. When social support is found to be
hadequate, nurses need to work with older persons to determine the appropriate informai
or formai support requked to meet their needs. Older persons may not be able to obtain
adequate support on their own because of (a) deciïning health, (b) lack of awareness of
available support, (c) inability in access support, and/or (d) hesitancy to ask for help
because of perceived inability to reciprocate. Numerous intervention studies which outiine
both successfùI and unsuccessfùi social support programs are avdable in nursing
literature. They provide invaluable information for nurses to use in planning social
support programs,
Nursina Administration
Scarcity of heaIth care dollars, the increasing nurnbers ofpeopIe over 65, and the
high cost of the older person to heaith care are prompting reevaiuation ofthe ways in

which health care is provided to older persons. Traditionally, the majority of health care
dollars aiiocated to the care of the elderly have been spent providing for their physical care
needs. Supportkg quality of life of comrnunity-dwelling, older persons has not been the
focus of health care.
This study provides support for the need to reevaluate both the allocation of funds
and the focus of nursing care. The assessrnent of factors which support older individuals'
quality of life provides data which can be used to make better decisions regarding the
utilization of nursing care resources. Nursing administrators can use information about
the current quaüty of lie of older persons to design services that will rnaintain or promote
quality of life rather than planning prograrns which promote only longevity and
dependency (Gooding, et al., 1988).
In response to a question about their potential to Live a long time, many women in
this study expressed a desire not to live a long t h e and spoke about their fears of
becorning a "burden". Factors such as home, family, independence, and health were
important to quaiity of life.
Development of prograrns which will give older persons the opportunity to l em
more about their health and health promoting behaviour, can empower them. Not only
will such prograrns support maintainhg health, they will aiso support feelings of control
and seKworth. Restructuring health support for the older population is not a simple task.
This change in focus fiom *ülness driven care to health supportive care means that nursing
dollars wilI also need to be aiiocated to determinkg the effectiveness of new prograrns.
Nursing administrators need to understand what quality of life means to the older person
and have a vision of what nursing can do to support that quality of lXe*
Nursin~ Education
The majority ofolder persons requiring care have lived in institutional health care
settings. Gerontologicai nurshg education has focused mainly on acquiring nurskg skîIis
to deal with their physicai care and ttnctiond needs. With the ïncreasing number of order
persons living in the community and the move towards assisting older persons to iive
healthy, active, and productive lives within the community, gerontological nursing
education needs to continue to change fiom one ofcare provision to one which focuses on

prevention and support.
It is essential that nurses gain knowledge about what quality of Iife rneans to the
older persons and those factors which are important to their continuhg quality of life.
Studies, such as this one, provide information about the relationships of social support,
optimism, and heaith, to quality of life. Knowing that these factors are important to
quality of Ke, requires that gerontological nurses acquire new skills and knowledge.
Nursing support and interventions cm only be effective when they are appropriate
to the needs of individuais. This requires gathenng thorough and accurate information
about quaiity oflife issues. In general, gerontological nurses have had little experience
with assessing quality of life. Numerous assessment tools are available that can assist
nurses to gather appropriate information related to quality of Me. Nurses working with
older persons need to become familiar with these assessment tools and knowledgeable
about their strengths, weaknesses, and limitations.
Most of the women in this study rated their heaith as good or excellent, considered
themselves to have a high quality of life, felt optimistic, and perceived their social supports
to be adequate. From cornmunity-dweiing, older individuals, such as these women,
student nurses can lem a great deal about the resources and adaptations through which
older persons maintain their quality of life and their independence. Current nursing
programs offer students opportunities to gain nursing experience in a vaxiety of settings
including an increased focus on community-dweüing, older persons. Expansion of
cornmunity-based practke, to include greater opportunities to assess quality of Life and
those persond resources, such as optimism and social support, essentiai to that quality of
We, d help student nurses gain a better understanding of older persons and support the
provision of person-focused care.
Suggestions for Future Research
Several issues have emerged nom the current study which prompt suggestions for
fbture research. This study shouid be replicated in a larger study in which the sample
more accurately represents the population of cornrnunity-dweihg, older penons,
including diverse groups whose quality of life has been identaied to be at risk As weii,
use of a longitudinal design wodd capture changes in the major study variables and

provide data about the relationships between these variables over time that cannot be
obtained using a cross-sectional design.
A longitudinal design would also allow study of the effectiveness of interventions.
For example, since variables such as social support can be enhanced, observations of
changes in social support and its relationship to quality of life would provide information
that could lead to the development of effective nursing interventions to maintain quality of
life for older persons.
Longitudinal intervention studies could also provide better understanding of
optimism and its relationship to quality oflife, self-efficacy, and perceived social support.
If optimistic individuals are more able to face adversity and stnve for goal attainment,
knowledge about whether optimisrn cm be enhanced and about factors which can increase
optimism would be of particular benefit to the development of nuning interventions which
would indirectly support the quaIity of üfe for older persons.
As supported by testgretest results, dispositional optimism has been considered to
be a personaiity trait that is relatively stable over time. Yet, it is unknown why some
people are less optimistic than others. In addition, researchers who have questioned the
stability of optimism have reponed daily fluctuations in individuals' feelings of optimisrn in
response to various internai and extemal factors (Shinen, 1995; Shifien & Hooker, 1995).
Further research is needed to explore the stability of optimism and to determine factors
which would enhance individuals' optimism.
The current multitude of operationai definitions of quality of life and social support
that have resulted in the developrnent and use of dozens of instruments to measure these
constructs, presents a challenge to current research in that there are no standards for
measurernent (Ferrans, 1990; Grant et al., 1990; JaIowiec7 IWO). The use of such a wide
variety of definitions and instruments affects the vanCety and type of research results and
makes it very dicuit for research tuidùigs to be compared (Ferrans, 1990; Kahn, 1994).
It is oniy through the use of accmte and reliable measurements ofquality of life and
social support that appropriate care planning and interventions can be detemhed. If
maintairing qua& of life and adequacy of socid support is more important than s h p Iy
prolonghg Ke, then having a method of assessrnent that accuratety captures these

constnicts is imperative.
Surnmary
Quality of life must be considered to be one of the benchmarks when planning,
implementing, and assessing the adequacy of social policies and health care (Abeles et al.
1994; Ferrans & Powers, 1985). New technology Ieading to longer life span and change
in Canada's sociai structure will affect quality of Life, directly and induectly. It is
imperative that curent research on aging uncover the many detenninants of quality of life
so that the most important contniuton cm be targeted for programs and interventions
(Abeles et al.).
The purpose of health care should be to support people living longer and healthier
and to improve their quaiity of their Me during their last years (Kaplan, 1994). Longevity
cannot be used as the sole determinant of health care nor should it be used as the only
measure of effectiveness of quality of care. Developrnent and delivery ofquality care can
only occur through determining what older persons have defined as their quality oftife.
Although the results of this study are based on a smail convenience sample they
provide support for translating relationships which have been found in younger
populations to comrnunity-dweiiing, older populations. The positive relationships between
dispositional optimism and quality of life, and perceived social support and quality of life,
and the relationship between dispositional optimisrn and perceived sociai support have
been supported in this study. As well, relationships between quality of life and health,
dispositionai optirnism and number of health problems, and perceived social support and
number of health problems were found to be signincant or approach significance.
Ahhough this study does not support aii aspects of the conceptuai framework and
directions of relationships have not been fuUy explored, study resuits should provide a
basis for further research about the relationships between quality of life, dispositionai
O ptimism, self-efficacy, and perceived social support for CO rnmunity-dwelling, of der
persons,

APPENDICES Appendix A
Ferrans and Powers QUALiTY OF LIFE INDEX
For each of the following, please choose the answer that best descnibes how satisfied you are with that area of your Ise. Please mark your answer by circling the number. There are no right or wrong answers.
EOW SATISFIED ARE YOU WITH:
1- Your hedthii 1 2 3 4 5 6
2. The henlth cue you ;ire receiving? 1 2 3 4 5 6
3. The mount of pain thnt p u have7 1 2 3 4 5 6 -
4. The amount of energy you have h r evnydny activities? 1 2 3 4 5 6
5. Your physicd independence? 1 2 3 4 5 6
6. The amount of controt you have over your Me? 1 2 3 4 5 6
7. Your potemtid to live u long tirne'? 1 2 3 4 5 6
8. Your f d y ' s health? 1 2 3 4 5 6
9. Your children? 1 2 3 4 5 6
10, Your f d y 's hrippiness? 1 2 3 4 5 6
1 1. Y o m ~IationsEip with your spouse/signitTcant othd 1 2 3 4 5 6
1 2. Y0 w S ~ K life? 2 3 4 5 6
13, Your tnmds'? 1 2 3 4 5 6
14. The emotiond support you get h m others? 1 2 3 4 5 6
15. Your ability to m a t f d y responsibiliûes? 1 2 3 4 5 6
16. Your uset'uIness to otIIrnb? 1 2 3 4 5 6
88

KOW SATISFIED ARE YOU WTH:
17. The mount of stress or worries in your Me? 1 2 3 4 5 6
18. Your home'? 1 2 3 4 5 6
19. Your neighbourhood?
20. Yourstandard of living?
21. Yourjob? 1 2 3 4 5 6
22. Not h8viag a job?
23. Your ducat ion'? --
24. Your hanciai indepadmce? 1 2 3 4 5 6
25. Your leisure thne activitis? 1 2 3 4 5 6
26. Your ability to travel on vacations? i 2 3 4 5 6 - - - - - --
27. Your potentiai for a happy old agektirement? 1 2 3 4 5 6
28. Your peace of mind?
29. Your personai fiaith in God? 1 2 3 4 5 6 - - - -
30. Your achevernent of personai goals'? 1 2 3 4 5 6 - . .-
3 1 - Yom happiness in gnerd? 1 2 3 4 5 6
32- Your Me in gensrai? 1 2 3 4 5 6
33. Yom personai appamnce'? 1 2 3 4 5 6

For each of the following, please choose the answer that best describes hou important that area of life is to you. Please mark your answer by circling the number. There are no right or wrong answers.
EOW IMPORTANT TO YOU 1s:
- -- ..
3. Being completely tree of pain'? 1 2 3 4 5 6 - -
4- Having enough rnmgy for evqdny nctivities? 1 2 3 4 5 6 - - -
5. Your physical independence? 1 2 3 4 5 6
6. Havïng control over your l$e? 1 2 3 4 5 6
7. Living r i long tirne? 1 2 3 4 5 6 -- --
8. Your fruniIy's health? 1 2 3 4 5 6 - - - - - - -
9. Your children? 1 2 3 4 5 6
10. Your fomily 's happiness?
1 1. Your rehtionship with your spouse/si~crrnt other? 1 2 3 4 5 6
t 2. Your sex We? 1 2 3 4 5 6
13. Your fiiads?
14- The motionai ilpport you get h m others? 1 2 3 4 5 6
16. Being mehl to others?

HOW IMPORTANT TO YOU IS: -- --
17. Having a rasonable mount of stress or womes? 1 2 3 4 5 6 - -
18. Your home'? 1 2 3 4 5 6 -
1 9, Your neighbourhood? 1 2 3 4 5 6
20. Your standard of living? 1 2 3 4 5 6
21. Yourjob? 1 2 3 4 5 6
22- To have a job? 1 2 3 4 5 6
23. Your educption? 1 2 3 4 5 6
26. The abiiity to nvel on vocations? 1 2 3 4 5 6
29- Your personai f ~ t h in God? L 2 3 4 5 6
- - -.
3 1 - Your happiness in grnad? 1 2 3 4 5 6
- -- - --
33- Your personai applrarance? 1 2 3 4 5 6
34- Are you to yourself'? 1 2 3 4 5 6

Appendix B
Life Orientation Test (LOT)
Instructions: Please answer the following questions about yourself by indicating the extent of your agreement using the following scale.
(O) = strongiy disagree (1) = disagree (2) = neutral (3) = agree (4) = arongly agree
Be as honest as you can throughout, and try not to let your responses to one question influence your response to other questions. There are no nght or wrong answers.
1. In uncertain times, 1 usually expect the best.
2. It's easy for me to relax.
3. If something can go wrong for me, it wiIi.
4. 1 always look on the bright side of things.
5. i'm always optirnistic about my future.
6. 1 enjoy my fiiends a lot.
7. It's important for me to keep busy.
8- I hardy ever expect things to go my way.
9. Things never work out the way 1 want them to.
10. I don? get upset too easily.
1 1. I'm a bebever in the idea that " every cloud has a silver lining".
12. I rarely count on good things happening to me.

Appendix C
SELF-EFFICACY SCALE
Please teil me how strongly you agree or disagree with each of the statements 1 wiU read to you or show you. There is no right or wrong answer.
(1) = Strongly disagree (2) = Disagree (3) = Agree (4) = Strongly agree
L. Keeping healthy depends on things that I can do.
2. It's up to me to arrange transportation when I need it.
3. I am able to get what I want from my relationships with my family. I am able to rnake sure that my relationships with my family are as satisQing and rewarding as I would like. 1 2 3 4
4. t could make my financial situation better if1 wanted to. 1 2 3 4
5. There are things I could do to make myselfsafer. 1 2 3 4
- 6. 1 am able to get what I want from my relationships with my Wends. 1 am able to make sure that my relationships with my fnends are as sa t iang and rewarding as I would Sie. 1 2 3 4
7. I do not have enough control over how good my living arrangements are,
8. I cannot be as productive as I want to be.
Amer on& ifyozc me married, 9. I have been able to get what I want tiom my relationship
with my husband/wffee 1 am able to make sure that my relationship with my husbandlwife is as satisfluig and rewarding as 1 would like. 1 2 3 4

Appendix D Persona1 Resources Questionnaire
under how much you agree or disagree beside each statement.
2. 1 belong to a group in which I feel important
3. People let me know that 1 do well at my work (job, homemaking, school).
1. There is someone I feel close to who makes me feel secure,
4. I can't count on my relatives and 6iends to help me with problems.
Y cn
5. 1 have enough contact with the penon who makes me feel special.
6. I spend time with others who have the same interests as I do,
7. There is Little oppominity in rny life to be giWig and caring to another person.
9. There are people who are avdable if1 need thern 1 1 1
8. Others let me know that they enjoy working with me (iob, cornmittees, projects).
l
over an extended penod of üme.
10. There is no one to talk to about how 1 am feehg.
11. Among my group of fiiends, we do favours for each other-
3
12. 1 have the oppominity to encourage others to develop their hterests and skiiis.
I

13. My family lets me know that 1 am important for keeping the family running.
14. 1 have relatives or fiends who will help me out even if1 can't pay them back.
15. When 1 am upset there is someone I can be with who lets me be mvself.
16. 1 often feel no one has the same problems as 1.
17. 1 enjoy doing Little "extra" t hings that make another person's Iüe more oleasant.
18. I know that others appreciate me as a person-
19. There is someone who loves and cares about me,
20. i have people to share social events and fun activities with.
21. 1 am responsible for helping to provide for another peaon's needs.
22- If1 need advice there is someone who would assist me to work out a plan for deaiing with the situation.
23. 1 have a sense of being needed by another person.
24. People thînk that I'm not as good a fnend as 1 shotdd be.
25. If1 got sick there is someone to give me advice about carhg for myseK

Appendix E
BACKGROUND ïNFORMATIOW
1. Date of interview (d/rn/y) :
Sex? M F
Age on your last birthday?
What is your marital status? Divorced Married/Common law Single Widowed
How far did you go in school?
Are you married? (circle one)
6. Do you live alone? YES NO, if no who lives with you?
7 . 1s there a relative who lives within a 1-hour drive who could help you out i f you needed help?
NO YES If yes, who?
What kinds of things could he/she do?
8 . 1s there a friend who lives within a 1-hour drive who could help you out if you needed help?
NO YES If yes,
What kinds of things could he/she do?

Appendk F Health Status Questionnaire
A. Qverall Health (from General Health Survey - Statistics Canada, 1987)
1. How would you rate your overall health at the present t h e ? - Excellent - Good - Fair - Poor
2. 1s your heaith better, about the same, or worse than it was 6 months ago? - Better - About the same - Worse
3. How much do your health problems stand in the way of your doing daily activities or the things you want to do? - Not at al1 - A litt1e (some things) - A great dea1
4. Please Lia any health problem that you have. How much do your health problems interfere with your activities?
Health Problern N o t At Al1 A L i t t l e A Great Deal

THE UNIVERSITY OF WESTERN ONTARIO FACULTY OF NURSING
NEEDS SENIORS FOR A RESEARCH STUDY
ABOUT QUALITY OF LIFE OF SENIORS
If you are 65 years of age or older you are being asked to meet once with a researcher to talk about the quality
o f your life and your outlook on life
TDlE COMMITMENT: One meeting - 1 to 1 1 hours
PLACE OF INTERVIEW: Your home or a location of your choice
IF YOU ARE INTERESTED OR YOU WOULD LIKE MORE INFORMATION
PLEASE CALL LIS WHEABLE at 472-7282

Appendix H
Quality of Life of Community Dwelling Seniors: The Infiuence of Optimism, Self-Efficacy and Social Support
Researchers : Lis Wheable RN, BScN, MscN Candidate Janet Jeflrey RN, PhD, Faculty Advisor Elsie MacMaster RN, MscN Ed Kelmes PhD
Place ofResearch: Your home or a location ofyour choice
We are interested in talking with senior citizens, aged 65 or older, to leam about their quality of life and what impacts their quality of life. We would like you to take part in this research study.
To take part in this study you are being asked to meet with a researcher to answer questions about your quality of Me, your outlook on He, and your health. The researcher cm heIp you fili in the questionnaires ifyou like. The in te^-ew will take about one to one and a haif hours. Taking part in this study is voluntary . You may refuse to take part in the study, refuse to answer any question, or you rnay end the meeting at any time and your health care will not change. Everythhg you Say will be confidentid. What you Say will not be discussed wîth anyone but the researchers. Your name will not be used when ta lbg about what you said. The questionnaire forms will have a study number ody. Your name will not be used. No one will read the foms except the researchers. These foms will be kept in a Iocked nling cabinet in the researcher's home. After the meeting, your name, address and phone nurnber will be ripped up.

Appendix 1
etter of Consent
Quality of Life of Community Dwelling Seniors: The Influence of Optimism, Self-Efficacy and Support Support
I have read the information letter attached to this form, which explains the research study. I understand what I am being asked to do. 1 agree to take part in this study. Ail questions have been answered to my satisfaction.
Signaîure:
Date:

Appendix J
Combined Life Orientation Test
Please answer the following questions about yourselfby indicating the extent of your agreement using the following scale.
(0) = strongly disagree ( 1) = disagree (2) = neutral (3) = agree (4) = strongly agree
Be as honest as you can throughout, and try not to let your responses to one question Muence your response to other questions. There are no right or wrong answers.
1. In uncertain times, i usually expect the best.
2. It's easy for me to relax.
3. [fsomething can go wrong for me, it will.
4. 1 always look on the bright side of things.
5. [lm always optimistic about my future.
6. 1 enjoy my Eends a lot.
7. It's *mportant for me to keep busy.
8. 1 hardly ever expect things to go my way.
9. Things never work out the way I want them to.
10. 1 dont get upset too easiiy.
1 I . Pm a believer in the Ïdea that "every cIoud has a silver lining".
12. i rarely count on good things happening to me.
13. Overaü, I expect more good thuigs to happen to me than bad.

Appendix K
ALL HeALTH SCIENCES RESEàRCH INllOLVINI: HUMAN SUWBCTS AT THE UNIVERSITY OF WESTERN ONTARIO 1 S CARRIED OUT IN COWUANCE WIW THE MEDICAL RESBARCH COUNCIL OF CANADA "GUIDBLXNES ON RBSURCH WüOLVINC HWM SUBJECT.
Dr. a. aorwern, Ass f stant Dean-Raseuch - Medicine (Chairman) tAnatomy/Ophthalmoloqyl M5. S. Koddtnott, Aaoistant Director of Research Services (EpidemioLogyL Dr, t. NichoLson, Sc. Joaepb' 8 Hospital R~presanrativa {Nucleat Medicine) Dr. P. Rucledge, Victoria IIospital Representativa (Cricical Care - Medicine) Or- u- B0~k-g~ University Hospital Re~fesehtativo lPhysician - Lntarn.L Medicine1 Dr. 'P. tcuvlon, Office a€ the Prestdent Representatfve tPhilosophyl Hrs. B. Jones, Office O€ the Prestdent RepresentatLva (CwninUnftyl Mrs- J. BuckreLL, Office CE t h e President Representative (Legall Dr. D. Preemn, Faculty of Medxine Regresentatlve (Clinical Pharrnacology - Madlclne) Dr. J. Koval, Faculcy of Medicfne neprosantarive tBpidriniology/Biostatfsttw~ Or. D- Johnston, PacuLty of D~ntistry Ropresentatfve tcommunity Dentisuyl Dr, J. JeEErey, Faculty OZ Nursing Raptesantativo tlursing) Dr. J.R. MacKLnnon, ?acuky O€ AppLicci Heatth Sciences Representative Wccup. Therapy) Dr. S. H i l l , ?aculry of Kinesiology Representatfve tKlnesialoqyl D r . C. C. Ellrc , Research Institutas Representatlva (Medical Biophysics 1 Mrs. R- Yohicki. ildminrstiratlve O € f ice: Aïtemutes are appalnted for each memher,
THE REVLEW BOARD HAS EXAWZNED THE RESShRCH PRWECT EIJTfTLEDt "QuaLity oE LiEe of mmmuriity ciweLlinq seniors: The influenca of optimisia, ~alf-effic~~y and social supp~r:.~
APPROYAt D a E : 20 J n e 1995 :3 new strategxs €or recruiting subjects fata the atudy)
A W C Y c

Appendix L
The University of Minois UIC ,Chbg~
February 15, 1995
Ms. Elisabeth Wheable 38 Indian Road London, Ontario N6H 4A5 Canada
Oear Ms. Wheable:
Thank you for your interest i n the Ferrans and Powers Quality o f Life Index (PLI). I have enclosed the generic version o f the QLI and the cornputer progran for calculating scores. 1 also have included a list o f the welghted item that are used for each o f four subscales: health and functioning, social and economic, psychological~spirituaI+ and fanily, as uell as the camputer comands used to calculate the subscale scores. Rie same steps are used to calculate subscale scores and overall scores.
A t this tine there i s no charge for use o f the QU. You have #y permission ta use the QLI for your study. In return, 1 ask that you send me a photocopy o f al1 publications o f your flndings using the QLI. I then wi 11 add your publfcation(s) to the H s t that 1 send out to persans who request permission t o use the QLI.
If 1 can be of further assistance, please do not hesitate t o contact ne. I wish you much success with pur research.
Sincerely ,
(iutc*IaW Carol Estwing Ferrans, PhD, RN, FAAN Assistant Professar

Carnegie Mellon University or Cmtfiie Mdbn Uoirmity PiibPr@4 PennsyIvlpia 15213 Phoae: (412) 168-319 1 FAX (412) 268-7610 Intunet: mrû@mdnwmlLedu
Elisabeih Wheable 38 India0 Road London, Ontano CANADA N6H4A5
Ikar Ms. Wheable:
You have my pcnnission to npwdse aad use the Lifi Orientation Test (LOT) for rmmh purposes. 1 would apprcciate your leaing me how how your work tums out. 1 sbouid also tel you that tbe LOT has fecentiy been revised. h ewlobg acopy of the mimi LOT, almg with iht anicle describing it Our own plan is to use the rcvis#b KIT exclusinly in hture research. You my wan t io consider nshg it 100. IF you hPvc any questions, please feel fiee to caii my secretary Susan Kravia at 412-268-3'79l. Good luck
Michd F. Scheier, PhD. Professor of Psychotogy

Appendk N
Requat for Petmission to use the Self Emcacy QuestiollllPire
To : Dr. Teresa E. Seeman, PhD Deparnent of Epidemiology and Public Health School of Medicine, Yale University, 60 Coilege St., New Haven, CT 06510
From: Elisabeth Wheable 38 Indian Road London, Ontario N6H 4AS
Date: February 4, 1995
V Y I am wrîting to request your permission to use the Self Efficacy Questionnaire (Seeman, Rodin & Albert, 1993) for a research smdy which 1 hop to conduct in the next few months. I am a graduate snident in the Master of Science Program in Nursing at the University of Western Ontario. I wiii be researching the influence of dispositio~l optimism. social supports, and self efficacy on the quality of life of comrnunity dwelling seniors.
Along wiih your letter of approval, I am asking diat you send me a copy of the Sclf Efficacy Qucstiomaire anl ary zssociatd data thiii 1 iniglii ryuire. 1 will be happy to pay any related costs.
Thankyou for you assistance-

Appendix O
Eliaab.Uk Wheabla 38 Indian Road
Collcge o f Nurslng
London, ON H6K 4A5
2hank you for your request. 1 am ploasiod that you are interartad in the PRQ85 for inclusion in your: research projact. If you find it maatr your needs, you have my permission t o usa it and raproduce as aany copies as you will repuire. I n this packet you will find a copy o f the PRQBS, the directions for scoring, the suggested deiographic information, and some additional results fron the continued peychopetric evaluation of the PRQ, Much of our work is published, but if you bave spea i f i c questions please do contact me.
As wa continue to work with the refinepaent and developwnt of the PRQ we are likewise beginning t a coUect and t o collata data sets prwided by researchers vho have used the PRQ, One specific a h is t o have a systematized data base that uould provide a source of couparison aeross studies, populations, situations etc. If you are willing to share your data s e t we would be most happy to Lnolude it in this groving data base. I hava included the list of demographic variables that should be sent with tha data.
The PRQ has been designed with tuo distinct parts. P a r t 1 can address s m e aspects of the network structure and provides descriptive data regarding situational support. Part 2 ie a scale developed ta meaaura the level of perceived social support based on the vork of Robert Weisa. Whila Part 1 can be used without Part 2 or P a r t 2 without Part 1 we ask that no items or questions be changed/deleted, or the iten sequence altered in any way. If you feal yau need t o change specific items t o met the aims of your research, 1 would ask that you s u b û t tbei t o me for raviev. 1 would be happy to discuss any questions or concens you have in relation tu y o w specific research.
Pleasa send $3.00 to cover reproduction and aailing costs and if you decide to use the PRQ, please send us a brief letter describing your study. Students are t o include the name of theîr research advisor. mie toal mot be identified, in your quastiennaLre, as the Personal Resource Questionnaire and authorship of the tao1 acknovledged in any publication or coaununication regarding the tooL
Checks should be arade out to Clarann ifcinert. Thank you for your interest in the PRQ.

References
Abeles, R, Gift, H., & Ory, M. (1994). A& and puality of lif~. New York: Springer Publishing Company.
Abler, R. & Fretq B. (1988). SeKefficacy and cornpetence in independent h g among oldest old persons. Journal of GerontolQgy: 43, S 13 8 - S 143.
Adam, D. (1 969). Anaiysis of a life satisfaction index. Joum- 24 470-474, d
Allen, J., Becker, D., & Swank, R. (1990). Factors related to fiinctional status &ter coronary artery bypass surgery. Heart & L u n u 337-343.
Alloway, R, & Bebbhgton, P. (1987). The buffer theory of social support - a review of the literature. eSySologica1 Med 0 . rcing t 7,91408.
Andrews, F. & Withey, S. (1976). Social indicators O . * . f well being: A m e n c a - 7
perceptions of life auality. New York: Plenum Press.
Antonucci, T. (1990). Social supports and social relationships. In R Binstock & L. George (Eds.), mdbook of Am and the Social Science (3" ed., pp. 205-226), Orlando, FL: Academic Press.
Aspinwall, L. & Taylor, S. (1992). Modeling cognitive adaptation: A longitudinal investigation of the impact of individuai differences and coping on coiiege adjustment and
63, 989-1003,
Ausiander, G. & Litwin, K. (1991). Social networks, social support, and seK ratings of health among the elderly. Journal of A& and H M : 3,493-5 10.
Avom, I., & Langer, E. (1982). Induced disabiîity in nurshg home patients: A controiied trial. Journal of the American C w Soc . C iety? 3 O, 3 97-400-
Baltes, M (1994). Aging weii and institutional üving: A paradox? in R Abeles, EL Ga, & M. Ory (Eds.), Amne and Oualitv of Lifc @p. 185-201). New York: Springer.
Bandura, k (1977). Social Ieamin~ theory. Engiewood CWs, New Jersey: Prentice-Hall.
Bandura, A (1982). Self-efficacy mechanism in human agency. Arnerican &choI~&t. 37,122-147.
Bandura, A (1 995). Cornrnents on the crusade against the causal efficacy of human thought. Journal of B ehavioural Therapy & Experimental Psvchiatm- 26,
C
179-190.

Barlow, I., Williams, B., & Wright, C., (1996). The generalized self-efficacy scaie in people with arthritis. Mhritis Care and Research, 9,189-196.
Barron, C., FoxaII, M., Von Dolien, K., Shull, K., & Jones, P. (1992). Loneliness in low-vision older women. Issues in Mental Heaith N u r s m , 387-401.
Beck, A., Weissman, A, Lester, D., & Trexler, L. (1974). The measurement of a m l t i n ~ and C l i ~ a l . . pessimism: The hopelessness scale. Joun
861-865,
Belec, R. (1 992). Quality of Life: Perceptions of Long-Tenn Survivors of Bone Marrow Transplantation. Qncology Nursirlp Forum. l9(1), 3 1-37.
Berkman, L., Oman, T., & Seeman, T. (1992). Social networks and social support among the elderly: Assessment issues. In R. Waiiace & R. Woolson (Eds),
c Studv of the Elderly (pp. 196-212). New York Oxford University Press.
Billingsley, K., Waehler, C., & Hardin, S. (1993). Stability of optirnism and choice ofcoping strategy. Percentual and Motor Skills. 76,91-97.
Blazer, D. (1982). Social support and monality in an elderly community 1 of Eaidemiologv 1 1 & population. Amencan Jouma 684-694.
Bliley, A & Ferrans, C. (1993). Quality of life after coronary angioplasty. eart & Luw. 22,193- 199.
Bradbum, N. (1969). The structure O hological well-beirlp, Chicago: Aidine Pubiîshing Company.
Bradbum, N. & Caplovitz, D. (1965). - I f or related to mental healtk Chicago: Aldime.
Bradbury, V. & Catanzaro, M. (1989). The quality of life in a male population 1 sufGerhg fiom arthntis. Rehabiiitat'on Nursirg 14.187-f 90.
Brandt, P. & Weinert, C. (198 1). The PRQ: A social suppon measure. Nursiu 277-280.
Bromberger, J. & Matthews, K (1996). A longitudinal study ofthe eEects of pessûnism, trait anxiety, and life stress on depressive symptoms in middle-aged women P-holpgv and Aeine. 1 1,207-213.
B q , M & Hoime, A (1990). Quaiity of life and socid support in the very old. Journal of Agina Studies. 4,345-3 57.

Callaghan, P. & Momssey, 1. (1993). Social support and heaith: a review. Journal of Advanced Nursiqg 1 8.203-210.
C h a n , D. (1987). Definitions and dimensions of quality of life. In N. Aaronson & I. Beckman (Eds.), The qulity of life of cancer wtients (pp. 1-18). New York: Raven Press.
Campbell, A., Converse, P., & Rodgers, W. (1976). The aual-: Perceptions evaluations- and satisfactiong New York: Russell Sage Foundation.
Canadian Study on Health and Aging Working Group. (1994). Patterns of carhg for people with dementia in Canada. Canadianlouaal of-, 470487.
Carver, C. & Gaines, J. (1987). Optirnism, pessimism, and postpartum depression. &nitive Therap and Research. 1 1.449462.
Carver, C. & Scheier, M. (1982). Control theory: A usefil conceptual framework for personality-social, clinical, and health psychology. ~ c h o l w c a l Bulletin' 92. 11 1-135,
Carver, C. & Scheier, M. (1990). Principles of self-regdation: Action and . . * . emotion. In E. Higgins & R Sorrentino (Eds.), m o o k of Mot~vabon and Connition:
ounda*ons of Social Behavior (pp. 3-52). New York: Guilford Press.
Carver, C., Pozo, C., Harris, S., Noriega, V., Scheier, M., Robinson, D., Ketcham, A, Moffat, F., & Clark, K. (1993). How coping mediates the effect of optimisrn on distress: A study of women with early stage breast cancer. Journal of Persodity and Social Psy cholop- 65,375-390.
Cohen, J. ( 1988). tatistical power analysis for the behavioral sciences (2nd ed.). New Jersey: Lawrence Erlbaum Associates.
Cohen, S. & Willis, T. (1985). Stress, social support and the buffiering hypothesis. J%ycholokcal Bulletin. 93.3 10-357.
Columbo, S. (1 986). General weii-being in adolescents: Its nature and measurement (Doctoral dissertation, Saint Louis University, 1984). bsertation Ab- Jntemational. 46,2246R,
Cunningham, A, Lockwood, G., & Cunningham, 1, (199 1). A relationship between perceived self-eficacy and quality of He in cancer patients. Patient Educatio~ and Counselline 17,7 1-78.
DeGenova, M (1996). Regrets În Iater lifé. Journal of Wornen & -(2), 75-85,

Domelas, E., Swencionis, C., & Wylie-Rosett, J. (1994). Predicton of walking by sedentary older women. journal of Women's Health. 3.283-290.
Dunn, S., Lewis, S., Borner, P., and Meize-Grochowski, R (1994). Quality of life for spouses of CAPD patients. ANNA Journal. 2 1.237-246,257.
C . . C O . . Faden, R., & Gennan P. (1994). Quality of life. Clinics in Genatnc Medicine. 10,
54 1-55 1.
Ferrans, C. (1 99Oa). Development of a quality of life index for patients with cancer. Oncolo w Nurs ne Forum. 17(3), 15-19.
Ferrans, C. (1990b). Quaiity of me: Conceptual issues. Semin= in 0- N u r s i n a 642480254.
Ferrans, C. & Powers, M. (1985)- Quaiity of life index: development and inp Science. 8, psychometric pro perties. Advances in Nurs 1 5-24.
Ferrans, C. & Powers, M. (1992). Psychometric assessrnent of quality of life index. Resmch in Nursinn & Health. 1 5,29-38.
Fitzgerald, S. ( 199 1). Self-efficacy theory: Implications for the occupational health nurse. AAOHN Journal. 39.552-557.
Fitzgerald, T., Temen, H., Meck, G., Lk Pransky, G. (1993). The relative importance of dispositional optimism and control appraisais in quality of life after coronary . C artery bypass surgecy. Journal of Behavioral Medicine. 16.25-43.
Flanagan, 1. (L978). A research approach to împroving our quality oflife. mencan Psvcholoeia. 33,138-147.
Fontaine. K, Manstead, A., & Wagner, H. (1993). Optimism, perceived control over stress, and coping. European Journal of P e r s e . 7,267-28 1.
Foreman, M. & Kleinpeii, R (1990). Assessing the quality oflife of elderly persons. Seminars in Oncolow Nursine6,292-297.
Foxali, M., Barron, C., Von Doiien, K, Shuli, K, & Jones, P. (1994). Livhg 1 of C;erontolpgical Nun arrangements, loneliness, and social support- Jouma 20(8),
6-14-
Frank-Stromborg, M. (1988). Jnsmiments for c l i w nursinn research, I . Nomak,
Connecticut: Appleton & Lange

Friedman, L., Nelson, D., & Webb, 1. (1994). Dispositional optimism, self- efftcacy, and health beliefs as predicton of breast self-examination. Amen'can Journal O
* . f Preventive Medictne. 10(3), 130-135..
Funch, D., Marshall, J., & Gebhardt, G. (1986). Assessment of a short scale to ial Science Medrcine. 2 t . measure social support. Soc 3,337-344.
Gecas, V. (1 989). The social psychology of self-efficacy. b u a l Review of Sociologyt 1 5,29 1 -3 16.
. . George, L. & Bearon, L. (1 980). mity of life in older Denons: Me- and rneasurement, New York: Human Sciences Press.
Girzadas, P., Counte, M., Glandon, G., & Tancredi, D. (1993). An anaiysis of elderly health and life satisfaction. Behavior. H&h. and A u 103-1 17.
Gonzalez, V., Goeppinger, I., & Long, K. (1990). Four psychosocial theorîes and . . their application to patient education and clinical practice. Mhntis Care and esearch. 3, 132-143.
Gooding, B., Sloan, M., & Amsel, R. (1988). The well-being of older Canadians. e Canadian Journal O
. f Nurs iwearch. 20(2), 5-1 8.
Grant, M., Padilla, G., Ferreii, B., & M e r , M. (1990). Assessment of quality of life with a single instrument. Seminars in Oncology N u r s i e 260-270.
Grembowski, D., Patrick, D., Diehr, P., Durham, M., Beresford, S., Kay, E., & Hecht, J. ( L993). SeLf-efficacy and health behavior among older adults.
d Social Behavior. 34,89- 104.
Guarnera, S. & Wiliiams, R (1987). Optimism and locus ofcontrol for health and m a t i o n among elderly adults. m a l of GerontolQgy. 42,594-595.
Kamid, P. (1990). Optimism and the reporting offiu episodes. Social Behavioc d Personalitv. 18,225-234.
Harvey, C., Bond, I., & Greenwood, L. (1991). Satisfaction, happiness, and self-esteem of older rurd parents. Çanadian Journal o f Community Mental Heaith 10(2), 3 1-46.
Heaith and Weifàre Canada (1981). The health ofcan-: Rwort ofthe da Hdth Survev. Ottawa, Canada
Hicks, F., Larson, J., & Ferrans, C. (1992). Qu- of life after Iiver transplant. Research in Nursîng & Health. 1 5, L I L-I 19.

Hubbard, P., Muhlenkarnp, A*, & Brown, N. (1984). The relationship between social support and self-care practices. wursilig Research. 3 3.266-269.
Hughes, B. (1993). Gerontologicai approaches to quality of Mie. In J. Johnson & R Slater (Eds.), A~eing and Later Life (pp. 228-232). London: Sage Publications.
Jaiowiec, A (1990). Issues in using multiple measures of quality of Me. Semin- in Oncology Nursine. 6.27 1-277.
Jeffiey, 1. (L989). Predictors of qup lihr ' - of 1' tfe for adults who have rhe-toia mhàtis, Unpublished doctoral dissertation, Case Western Reserve University, Cleveland, O hio.
Jerusalem, M. & Schwarzer, R (1 992). Self-efficacy as a resource factor in stress appraisal processes. In R. Schwaner (Ed.), Selfiefficacy: Thwht Control of Action. Washington: Hemisphere.
* . Johnson, T. (1995). Aging well in contemporary society. Amencan Behavioral
cientm 39,120-130.
Kahn, R (1994). Social support: Content, causes, and consequences. In R Abeles, K. Gi & M. Ory (Eds.), &&g and Qw of Life (pp. 27-54). New York: Springer.
Kahn, R, Wethington, E., & Ingersoli-Dayton, B. (1987). Social support and sociai networks: Determinants, efects, and interactions. In R Abeles (Ed.), C m Pers~ectives and Social Psvchology (pp. 139465). New Jersey: Lawrence, Erlbaurn Associates,
Kaplan, R (1994). The Ziggy theorem: Toward an outcornes-focused health psychology. Health Psycholper: 13.451460.
Kaplin, R, Bush, S., & Berry, C. (L976). Health aatus: Types of vaiidity and the index of weil-being. Health Services Research. 1 1.478407-
Krause, N. (1987). Life stress, sociai support, and seLf-esteern in an elderly population. Psycholow and AGng-2- 349-356.
Korte, C. & Gupta, V. (199 1). A program of Eïendly visitors as network buildea. e GerontoIo&- 3 1.404407.
Larson, R (1978). Thirty years of research on the subjective weii-being ofolder Americans, Journal of Gerontolow. 33.109-125.

Lamb, L. (1996). Uncertainty, ootirrus t m. and oflife of adults following çoronarv arterv bypass mafi surgerv: Transition from al to home Unpublished mastefs thesis, University of Western Ontario, London, Ontario, Canada.
Lauver, D & Tak, Y. (1995). Optimisrn and coping with a breast cancer syrnptom. Vursine Research. 44,202-207.
Lee, R., Graydon, J., & Ross, E. (1991). Effects ofpsychological well-being, physical statu, and social support on oxygen-dependant COPD patients level of fiinctioning. Research in N u n i n e and Health. 14.323328.
Levitt, M., CIark, M., Rotton, S., & Finley, G. (1987). Social support, perceived control, and well-being: A study of an environrnentaliy stressed population. Jnternationd Journal of Asingand Human Development. 25,247-258.
Lindgren, A., Svardsudd, K., & Tibblin, G. (1994). Factors related to perceived health among elderly people: The Albertina project. &p and a 24.3289333.
Long, B., & Sangster, J. (1 993). Dispositional optirnism/pessimism and coping arategies: Predictors of psychosocial adjustment of rheumatoid and osteoarthritis patients. Journal of Applied Social Psyçholoqy. 23,1069-109 1.
Lubben, J. (1 98 8). Assessing social networks arnong elderly populations. Family Communitv Health. 1 1(3), 42-52.
Mahon, N. & Yarcheski, A (1988). Loneliness in early adolescents: An emperical test of altemate explanations. JVursi~ Researd? 37,330-33 5.
Mahoney, F. & Barthel, D. (1965). Functional evaluation of the Barthel index. Marvland State Medical louml. 14.61-65.
Maton, K (1989). Community settings as buffers of life stress? Hïghly supportive churches, rnutuai help groups, and senior centers. American J o u d of Cornmu& Psycholop. 17,203-232.
Matt, G. & Dean, A (1993). Social support fiom finends and psychological distress among elderly persons: Moderator effects of age. Journal of Hem and Social Behavior- 34,187-200-
McNair, D., Lorr, M., & Droppleman, L. (1971). prome of Mood States. San Diego, CaliforrÜa: Educational and Industriai TesMg Senice.
Medley, M (1 980). Life satisfaction across four stages of adult Hee International Journal of Amng and Human DeveIoornent. I 1,193-207.

Minkler, M. & Langhauser, C. (1988). Asseshg health diifferences in an elderly t .
population: A five-year follow-up. Journal of the Amencan ("i'inmcs Socie& 36, 113-1 18.
Moore, E. (1990). Using self-efficacy in teaching self-care to the elderly. Holistic rsinn Practice&Z), 22-29.
Muck, M. (1 996). Poetry. Journal of Women & -(1), 6 1.
. Munro, B. & Page, E. (1995). Dtistical methods for health care research.
Phiiadelp hia: Lippincott.
Neugarten, B., Havighurst, R., & Tobin, S. (196 1). The measurement of life satisfaction. Journal of Gerontologtlo. 134- 143.
Newsom, J. & Schuk, R (1996). Social support as a mediator in the relation berneen ttnctional status and quality of life in older adults. PqchoIgg~ and 1 1 (1), 34-44.
Novak, M. (1993). Aginp & Society: A Cadian Perspective, Scarborough: Nelson Canada.
OZeary, A. (1 985). SeKefficacy and health. j&&ivioral Research Therilp. 23, 43 7-45 1.
OZeary, A (1992). Self-efficacy and heaith: Behavioral and stress-physiological C C
mediation. W t 1 v e Thew and R-ch. 16, 229-245.
Oleson, M. (1 99Oa). Content validity of the Quality of Life Index. &lied Fur- Research. 3,126- 127.
Oleson, M. (1 99Ob). Subjectively perceived quality of Ke. JMAGE:Joumal of Nursing Scholanhip 22,187-NO.
Osberg, J. S., McGinnis, G., Ddong G., & Seward, M. (1987). Life satisfaction and quality of life among disabled elderly adults. Journal of G e r o n t w , 228-230.
Peariman, R & Uhlmann, R (1 99 1). Quaüty of We in elderly, chronicaüy ill outpatients. Journals of Gerontolog. 46(2), M3 1-M38.
Peplau, K (1994). Qualiq of LZe: An interpersonal perspective. fuuni0p Science uarterly. 7.10-15.

Piazza, D., Holcombe, J., Foote, A., Paul, P., Love, S., & Da@ P. (1991). Hope, social support and self-esteem of patients with spinal cord injuries. Journal of
eurosaence Nursina. 23,224-230.
Ploeg, J. & Faux, S. (1989). The relationship between social support, lifestyle behaviours, coping and health in the elderly. The Canadian Journal of Nursiqg Research. a(2), 53-65.
Po14 D. & Hungler, B. (1993). Essentials of nursine research: Methoh g9p"sal. and utilization, Philadelphia: I. B. Lippincott Co.
Preston, D. & Grimes, 1. (1987). A study of differences in social support. Journal gf Gerontol-(2), 36-40.
Rabinowî~ S. & Melamed, S. (L992). Personai determinants of leisure-time exercise activities. Percepnial and Motor Skills. 75,779-784.
Radloff, L. (1977). The CES-D Scale: A self-report depression scde for research in the general population. dpplied Psycholoj&al Mwrernent. 1.3 85-40 1.
Reker G. & Wong, P. (1985). Personai optUnism, physical and mental health: the . 0
tnumph of successtùl aging. in J. Birren & I. Livingston Pds.), ÇppOLtion? Stress a (pp. 134- 173). New York: Prentice Hall.
Revicki, D. & Mitchell, 1. (1986). Social support factor structure in the elderly. 8,232-348.
Rickelman, B., Gahan, L., & Pana, H. (1994). Attachent and quality of life in older, community-residing men. Nursirlg Research. 43.68-72.
Roberts, B., Anthony, M., Matejczyk, M., & Moore, D. (1994). The relationship of social support to tùnctional Limitations, pain, and weii being among men and women. Journal of Women & Aeiqg&(1/2), 3-19.
Rodin, J. & McAvay, G. (1 992). Detennlliants of change in perceived health in a 1 of Gerontology: P chological Sciences. longitudinal shidy of older adults. Journa 47,
Rowe, J. & Kahn, R (1987). Auman aging: Usual and successful. Scien& 237.143-149.
Ruchiin, H. & Morris, 1. (1991). Impact of work on the quality of Iife of cornmunity-residing young elderly. Amencm Journal of Public Hdth. 8 1,498-500.

Scheier, M. & Carver, C. (1985). Optîmism, coping, and health: Assessrnent and implications of generalized outcome expectancies. Heaith Psychologlt4.2 19-247.
Scheier, M. & Carver, C. (1 987). Dispositional optimism and physical well-being: The influence of generaiized outcome expectancies on health . Journal of Person Jïty and Social Psyc~ology. 55, 169-2 1 O.
Scheier, M. & Carver, C. (1992). Effects o f optirnism on psychologicai and * ,
physical well-being: Theoretical o v e ~ e w and empiricai update. Çpgnitive Therap~ Research. 1 6,20 1-228,
Scheier, M., & Carver, C. ( 1993). On the Power of Positive Thinking: The Benefits of Being Optimistic. Current Directions in P s y c i i o l ~ Science. XI), 26-28.
Scheier, M., Carver, C., & B tidges, M. (1 994). Disthguishing optllnism fiom neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation ofthe LXe
1 of Pe r sd i ty and Social P Orientation Test. Journa 67,1063-1078.
Scheier, M., Matthews, K, Owens, J., Magovem, G., Lefebvre, R., Abbott, R, & Carver, C. (1989). Dispositional optimism and recovery fkom coronary artery bypass surgery: The beneficial effects on physical and psychological weîi-being. Journal of Personalitv and Social Psychology 57,10244040.
Scheier, M., Weîntraub, J., & Carver, C. (1986). Coping with stress; Divergent strategies of optimists and pessimias. Journal of Perg0npli- and Social Psy&&gy. 51. 1257-1264.
Schipper, H., Chch, J., McMurray, A.., & Levitt, M. (1984). Measuring the quality of life of cancer patients: the Functional Living Index - Cancer: Developrnent and validation Journal of Cl
. C
inical O n c o l o ~ 472-483.
Schuiz, R, Tompkins, C., & Rau, M. (1988). A longitudinal snidy of the psychosocial impact of aroke on primary support persons. Psycha low&w 13 1-141,
Schulz, R, Bookwda, J., Scheier, M., Knapp, J., & Wiiamson, G. (1996). Pessimism, age, and cancer monality. Psycholog and A- 3 04-3 09.
Seeman, T. E., Rodin, J., & Albert, M. (1993). Self-efficacy and cognitive performance in high-tùnctionuig older individuak W d Hedth, 5. 455-474.
Sharpe, P., Kickey, T., & WoK F. (1994). Adaptation of a generai optimism scale for use with older women Psyhologicd Reports. 74.93 1-937.

ShifFen, K. & Hooker, K. (1995). Stability and change in optimism: A study among spouse caregivers. Experimental &&g Research. 2 1.59-76.
Solar, G. E., MacEntee, M. I., & Hü1, P. (1993). The elderly: Their perceived supports and reciprocal behaviors. Journal of îerontolpgical Social Work. 19.15-33.
Smilkstein, G. (1 978). The family APGAR: A proposai for a farnily tiinction test and its use by physicians. The Journal of Familv Pracbce. 6, L23 1-1239.
Spanier, G. (1976). Measunng dyadic adjustment: New scales for assessing the quaiity of marriage and famil y dyads. J o u d of u e and the Familv. 3 8.1 5-28.
Speake, D., Cowart, M., & Pettet, K. (1989). Heaith perceptions and lifestyles of the elderly. Research in Nursiqg and Health. 1 & 93-100.
Staab, A. & Hodges, L. (L995). JZssenUs of~rontological nursiu Adwtation process, Philadelphia: I. B. Lippincott Co.
Statistics Canada. (1987). General Social Surv-a Health and Social Support. Ottawa: Minister of Supply and Services.
Stewart, A & King, A. (1994). Conceptualinng and rneasuring quality of life in older populations. In R Abeles, K. G i & M. Ory (Eds.), m n d of Life @p. 27-54). New York: Springer.
Stoller, E. & Pugiiesi, K. (L99 1). Sue and effectiveness of uiformal helping networks: A panel study of older people in the cornrnunity. J o u d of Health and Socipl Behavior. 32.180-192.
Stone, A & Neale, L (1984). New measures of daüy coping: Development and preliminary results. Journal of Personal* and Social P hology. 46+ 892-906.
Strack, S., Carver, C., & Blaney, P. (1987). Predicting successfiil completion of an aflercare program fo ff owhg treatment for aicoholism: The role of dispositional optùnism. Journal of Personality and Social PsychoIop. 53.579-584.
Strecher, V., DeVeiiis, B., Becker, M., & Rosenstoclq 1. (1986). The role of self- efficacy in achieving health behavior change. flealth Ehcnb-erIv. 73-92.
Taai, E., Rasker, I., & Wiegman, 0. (1996). Patient education and self- .. management in the rheumatic diseases: A self-efficacy approach. Arthntis Care and esearch. 9,229-23 8,

Taylor, S., Kemeny, M., Aspinwall, L., Schneider, S., Rodnguez, R, & Herbert, M. (1 992). O ptirnism, CO ping, psychological distress and high-cisk sexual behavior among
f Persodity and men at risk for acquired immunodeficiency syndrome ( A I D S ) . Journal O
Social Psvchology. 63.460-473.
Telch, C. & Telch, M. (1986). Group coping skiiis instruction and supportive l of Consulting group therapy for cancer patients, a cornparison ofstrategies. Jouma
Clinical Psycholoq. 54.802-808.
Thompson, V. (1989). The elderly and their infiormal social networks. ÇPnadian Journal on &ne. 8.3 L 9-332.
Turner, R., Frankl, G., & Levin, D. (1983). Social support: Conceptuaiization, measurement, and implications for mental hedth. In I. Greenley (Ed.), Research in
ornmunity and Mental HeaItC (pp. 67 - 11 1). Greenwich, CT: IAI Press
Varricchio, C. (1990). Relevance of quality of life to clinical nursing practice. Seminars in Oncoioy N u r s i - 6,255-258.
Verbnigge, L. (L994). Disabiiity in late life. in R Abeles, H. Gift & M.Ory (Eds.), &&g and Ouality of Life (pp. 79-98). New York: Springer.
Watson, D., Clark, L., & Tellegen, A. (1988). Development and validation of bief measures of positive and negative affect: The PANAS d e . J o u d of Penonality
d Social Psvcholopv. 54,1063-1070.
Weinberger, M., Hiner, S., & Tiemey, W. (1987). Assessing social support in ial Science and Med . . elderly adults. Soc rcine. 25,1049-1055,
Weinert, C. (1987). A sociai support measure: PRQ85. Nur- Research. 3 6, 273-277.
Weinert, C. & Brandt, P. (1987). Measuring social support with the PRQ. stem Journal o f Nurs n~ - Research. 9,589-602.
Weinert, C. & Tilden, V. (1990). Measures of Social Support: Assessrnent of Vaiidity. Nuning Research. 3 9,2 12-2 16.
Weiss, R ( 1974). The provisions of sociai relationships. In 2. Rubin (Ed.), Doing ynto Ot her~ (p p. 17-26). Englewood CWs, NJ: Prentice-Raii.
White, N., Richter, I., & Fry, C. (1992). Coping, social support, and adaptation to chronic hess . Western Journal of Nursing Research. 14.21 1-224.

Wflcox, V., Kasl, S., & Berkman, L. (1994). Social support and physical disabEty in older people after hospitalization: A prospective study. Health Psychology. 13, 170-179.
Williams, T. (1990). Geriatncs: A perspective on quality of iife and care for older * * people. In B. Spilker (Ed.), Quality of Life Aswments in Clinical Trials (pp. 217-223).
New York: Raven Press Ltd.
Wood, V., Wylie, M., & Schafer, B. (1969). An analysis o f a short self-report measure of life satisfaction: Correlation with rater judgrnent. bumal of Gerontology. 24, 3 24-3 26.
Yarcheski, A., Mahon, N., & Yarcheski, T. (1 992). Validation of the PRQ8S social support measure for adolescents. FIursingPesearch. 4 1,3 32-3 37.
Yarcheski, A., Scoloveno, M., & Mahon, N. (1994). Social support and well- being in adolescents: The mediating role of hopetiilness. N u r s i m a r c h - 43.288-292.

IMAGE EVALUATlON TEST TARET (QA-3)