Embed Size (px)
Citation preview

OCCUPATIONAL THERAPY PRESCRIBED MINIMUM BENEFITS
FINAL DOCUMENT
1 MARCH 2007

2
CONTENTS
TOPIC
AUTHOR
CONTACT DETAILS PAGE
Cover Document Romy iContents & Contact details of authors
2
Anxiety disorders Modise Mogotsi [email protected] 3Attention deficit hyperactivity disorder
Keri-Lee Roebert [email protected] 46
Dementia Michele Nye [email protected] 62
Eating disorders Anel Grobler [email protected] 89
Zonia Weideman [email protected]
Mood disorders Enos Ramano [email protected] 106Obsessive compulsive disorder
Rose Crouch [email protected] 136
Post traumatic stress disorder
Vivyan Alers [email protected] 144
Schizophrenia Rose Crouch [email protected] 163
Substance abuse Rose Crouch [email protected] 175
Document edited by Zonia Weideman.

3
ANXIETY DISORDERS Compiled by Modise J Mogotsi BSc (Occupational Therapy)-University of Cape Town, MSc (Public Health)-
Umeå Universitet, SWEDEN
1. INTRODUCTION
Occupational therapists “use scientifically chosen meaningful activities to assist diverse
clients with a range of problems to maximise their functioning. This empowers them to be
as independent as possible to experience dignity and quality of life at work, at home and
at play.”1
Throughout occupational therapy historical development has been associated with
people not being able to manage their anxiety and stress while recovering after an
injury/disease/illness/disorder/disability. Despite this anxiety being secondary to primary
condition, there has also been identified and recognised abnormal anxiety states and
stress levels. These were all addressed holistically in occupational therapy interventions.
The unique use of occupations (any activity a person performs on a daily basis)
therapeutically to achieve the desired results of improved health and well-being. This
underpins the philosophy in occupational therapy that human beings are occupational
beings, and therefore any occupation has potential to influence their state of health and
wellbeing1,2.
In anxiety disorders, the typical feature across the spectrum is that of irrational fear of
being out of control. Despite many psychiatric disorders and/or mental illnesses having
the control as the central core of their behavioural outcome, the emphasis here is on the
fear itself being irrational.
It has been widely acceptable that pharmacotherapy has become efficient and well as
psychotherapy in combination3,4. This has been observed in the recent evidence that has
come out of various empirical studies. Often this being the conventional approach,
occupational therapy has not been extensively studied in this context. There is however,
sparse evidence illustrating the contribution of occupational therapy either as a single
medium or in combination. The current occupational therapy evidence is gradually

4
approaching the gold standard of scientific rigour, nevertheless there have been
numerous successful clinical results from occupational therapy interventions.
To indicate further, consider the following occupational performance areas; (a) Work, (b)
Activities of Daily Living, (c) Leisure and (d) Social. If individual experiences: generalised
fear or constantly worrying, fear of imperfections, fear of dying, fear of interactions, and
re-experiencing previous fearful situation as though current. All of these being irrational,
occupational therapy will focus the individual on:
(a) Work
The nature of the task at hand, what needs to be accomplished, highlighting the skills
already mastered and providing a sense of competence for skills which require
improvement, i.e. setting achievable goals which could be measured at completion of
the task. For example having a roster to plan concisely the work duties such as
important and urgent deadlines.
(b) Activities of Daily Living
The ability to take care of oneself (as well as other/s), encouraging positive habits and
useful routines, as well as enhancing the satisfaction of enjoying ones end-products
of such tasks, e.g. grooming, cooking, shopping, etc
(c) Leisure
The ability to re-engage in hobbies and interest, as well as improve current/ introduce
new fun and creative activities, etc. The daily pre-occupations are often deterrent for
individuals to connect with their sources of contentment. Occupational therapy
inculcates this in an integral manner that an individual will perform automatically e.g.
smiling/ laughing, breathing, pauses, etc
(d) Social
The capacity to experience safety and support from various interpersonal interactions.
Assertiveness training, conflict resolution, stress management and many other coping
skills are a few examples.

5
As a general note, Occupational therapy contributes on different psychic (superego, ego and
unconscious), relational (self, other and environment), insight (intellectual and emotional),
spiritually (time-out, pampering, aloneness not loneliness, etc) and most crucially practical
(i.e. doing with the individual as opposed doing for the individual).
Referral sources usually range from individuals themselves (self-referral) or by family
member (parent, sibling or spouse) through organisations (educators or employers) to
professionals (General Practitioners, and/or Medical Specialists). Most commonly are from
professionals followed by organisations and lastly self.
2. DIAGNOSIS
According to Kaplan, Sadock and Grebb (1994) normal anxiety is a sensation that is
experienced by every human being, often accompanied by physiological changes in the
body. They expressed anxiety to be different from fear in that the threatening stimulus is
unknown in the one and known in the other, respectively.
Furthermore, stress is a state of response in either situation, i.e. anxiety, fear or both. Stress
itself does not lead to either, but often is a mechanism by which a balance is sought between
the internal (personal) and external (environmental) conditions, in order to restore or
minimize the effects of threatening stimulus.
They further explained pathological anxiety is the profound state where there is an intense
experience of such threatening stimulus and/or extreme response to this; that will lead to an
individual inability to sufficiently moderate these levels. Since an individual may not have a
clear understanding of such conditioned responses, this will fluctuate often in line with their
personality characteristics.
While the above may be the case, there are many theories e.g. psychological
(psychoanalytical, behavioural, existential), biological (autonomic nervous system,
neurotransmitters, genetic, brain-imaging, neuroanatomical) and arguably sensory (tactile
and vestibular modulation) around the causes of such abnormal or pathological
consequences. There is also a recent clinical observation that people with Anxiety Disorders

6
tend to also exhibit sensory modulation disturbance, particularly in children5. This experience
would warrant further research to establish the relationship between anxiety and sensory
states.
The Anxiety Disorders are a spectrum including Generalised Anxiety Disorder, Obsessive-
Compulsive Disorder, Panic Disorder, Social Anxiety Disorder and Post-Traumatic Stress
Disorder. This chapter on Anxiety Disorders will offer description and not the diagnostic
criteria6,7 for Generalised Anxiety Disorder, Panic Disorder and Social Anxiety Disorder. For
Obsessive-Compulsive Disorder, please refer to a chapter by Rosemary Crouch and for
Post-Traumatic Stress Disorder refer to a chapter by Vivyan Alers.
For tabulation, refer to Figure 8-2 Indicators of Anxiety Disorders in Bonder (1991).
(a) Generalized Anxiety Disorder
Generalised Anxiety Disorder is characterised by an “excessive anxiety and worry …
occurring more days than not for a period of at least 6 months …”7. The relevant code
300.02 (432).
“Anxiety is generalized and persistent but not restricted to, or even strongly predominating
in, any particular environmental circumstances.”6 The relevant code is F41.1.
(b) Panic Disorder
Panic Disorder is characterized by “a discrete period of intense fear or discomfort that is
accompanied by at least 4 or 13 somatic or cognitive symptoms. The attack has a sudden
onset and builds to a peak rapidly (usually in 10 minutes or less) and is often accompanied
by a sense of imminent danger or impeding doom and an urge to escape.”7. Code 300.01
(397) and 300.21 (397) with and without agoraphobia, respectively.
Panic Disorder is distinguished by “recurrent attacks of severe anxiety (panic), which are not
restricted to any particular situation or set of circumstances and are therefore
unpredictable.”6 (F41.0)
7
(c) Social Anxiety Disorder
Social Anxiety Disorder is characterized by “a marked and persistent fear of social or
performance situations in which embarrassement may occur (Criterion A). Exposure to the
social or performance situation almost invariably provokes an immediate anxiety response
(Criterion B).”7. Code 300.23 (411)
Social Anxiety Disorder is also associated with “Fear of scrutiny by other people leading to
avoidance of social situations. More pervasive social phobias are usually associated with low
self-esteem and fear of criticism.”6 (F40.1)
According to Kaplan, Sadock and Greb (1994), anxiety disorders are associated with alcohol
use disorders and other substance-related disorders as well as other general medical
conditions. Epidemiological studies reveal the following statistics Generalized Anxiety
Disorder 3-8%, Panic Disorder 1.5-3% and Social Anxiety Disorder 2-3%.
Predisposing factors
• Temperament: inherited traits
• Early psychological trauma, particularly disrupted mother-child relationship
• Stressful life events during maturation, particularly separation
• Exposure to unfavourable environment during maturation, e.g. poor housing, lack/
surfeit of stimulation, growing up in a deprived institutional environment or a war zone
• Basic physical needs unmet: hunger/ cold
• Faulty learning of maladaptive coping styles
Current Factors
• Stressful live events, e.g. bereavement, giving birth, relocation, unemployment, legal/
criminal activity
• Stressful lifestyles: conflicting roles, e.g. “working mother”, financial problems, study/
work-related pressure

8
• Social stress: role dissatisfaction/ ambiguity, poor social status, poverty, poor
accommodation
• Relationship/ family problems, e.g. divorce, caring for sick relatives or children
• Actual/ potential physical ill health, especially terminal/ progressive illness of self/
significant other
3. IMPACT ON OCCUPATION
Out of control feeling is generalisable to many psychiatric and mental illnesses, particularly
with anxiety states. This feeling is characterized by impending disaster or looming doom
resulting in individuals being left vulnerable and abandoned as they perceive it. In addition,
preoccupation about worries and bodily ailments is often present and lead to diminished
optimal performance in life. Occupational Therapists assist people who are anxious by
guiding their performance in valued occupations, tasks and roles9,10.
3.1 Work
Work as a distant environment for individuals (usually), will magnify the perceived and/or real
feelings as experienced where individual’s productivity or standard of performance set by the
workplace could be severely reduced. Some of the responsible factors are considered
below:
Generalised Anxiety Disorder
i. Restlessness
Individual may lack focus, become bored, deeply unhappy and could lack
motivation to initiate, implement and complete the tasks. They may thus require
stimulation.
ii. Fatigue
Individual may lack energy, focus, become emotionally heavy and could lack drive
to be occupationally present. They may thus require re-orientation or change of
duties/jobs.

9
iii. Poor concentration
Individual may lack attention to details and thus affect accuracy and precision,
which will in turn affect the quality of the work produced. They may require re-
strategizing the work layout and/or adjusting the speed of performance.
iv. Irritability
Individual may be generally unapproachable and in fowl mood, thus prevent
effective communication and work interrelations. They may require communication
skills to express themselves in terms of their own personal and work related
needs.
v. Muscle tension
Individual may be uptight and lack general humour and astuteness to the familiar
tasks, which could affect their productivity (both quality and quantity of work). They
may require relaxation techniques, stress and time management, etc.
vi. Sleep disturbance
Poor quality sleep may affect quality of the waking hours directly or indirectly
depending on the expected levels of performance on a task. Provision may be
made at work for slumber pause or period of non-work related activity. Individuals
would be encourage to utilise such time out (more) effectively e.g. leisure
management.
Panic Disorder
i. Palpitations, pounding heart, or accelerated heart rate
ii. Sweating
iii. Trembling or shaking
iv. Sensation of shortness of breath or smothering
v. Feeling of chocking
vi. Chest pain or discomfort
vii. Nausea or abdominal distress
viii. Feeling dizzy, unsteady, lightheaded, or faint

10
ix. Derealisation (feeling of unreality) or depersonalisation (being detached from
oneself)
x. Fear of losing control or going crazy
xi. Fear of dying
xii. Paresthesias (numbness or tangling sensations)
xiii. Chills or hot flushes
The above may be dealt with recognizing the triggers to such responses, failing which at the
time, handling techniques may become applicable. Experiencing the above may occur with
individual shutting the world out and perceiving no way out. They may require techniques to
counteract such negative experience, e.g. counting, breathing, panic padding, etc.
Social Anxiety Disorder
i. Avoidance
Usually works for individual since they do not have to be exposed to the perceived
threat. Where compelled to confront the stimulus, individuals may require
exposure technique (e.g. desensitisation), which would happen gradually and
systematically.
ii. Anxious anticipation
Individuals may believe they have premonition to certain effects which are usually
negative and a threat to themselves. Often times they find themselves in such
situation they have ‘predicted’. They may thus require a cognitive technique (e.g.
deconstruction and reconstruction), in which negatives are replaced with positive;
and hence actions would be guided as such.
iii. Distress
Individuals may be in general disarray and disorganised; they would often have no
plan or miss the target; they could also lack precept and apt to self-fulfilling
prophecy. They may require re-organization as well as re-building self concept.

11
3.2 Activities Of Daily Living
Activities of Daily Living predominantly manifest at home as an individual’s immediate
environment, could illustrate mild functional impairment due to the perceived and/or real
feelings as experienced; individual’s would thus remain fairly independent or rather becomes
more drawn to themselves than they usually are. Some of the responsible factors are
considered below:
3.3 Leisure
Leisure could be arguably the highest occupational satisfaction status where may
occupational factors integrate and consolidate. The perceived and/or real feelings as
experience could inhibit the individual’s occupational expression and a sense of integrity.
Since leisure would replenish energy stores and revitalise spiritually, individuals would be
expected to regularly engage in this occupational performance area. In fact, much of human
existence could be lived comprehensively in this regard, i.e. life being a leisure. Some of the
responsible factors are considered below:
3.4 Social
Society at large environment is an intermediate or interphase for individual’s private and
public self. The perceived and/or real feelings experienced by the individual may result in
moderate impairment (or emotional handicap) which will depend on the amount of available
or lack of social support and network connections. Some of the responsible factors are
considered below:
For detailed impact of Anxiety Disorders on occupation, please refer to Table 19.1 (The
occupational implication of disabling anxiety and stress)9.

12
4. IMPACT ON ROLES, HABITS AND ROUTINES
Roles
Roles refer to “set of behaviours that have some socially agreed-upon functions and for
which there is an accepted code of norms.”11,12
Across the Anxiety Disorders – individuals may not be able to accomplish the worker role
due to fear of inadequacy or poor standard of performance; withdraw from being a socialite
e.g. friend, colleague, family member (sibling/partner/spouse) and social club member
fearing to embarrass themselves or maintaining the environmental expectations;
underestimate their physical appearance by minimizing their unique individual attributes
either in both verbal and non-verbal presentations; as well as deep seated fear of failure in
any activities where they may be expected to perform according to the norms or socially
acceptable and unwritten rules.
Occupational therapy provides an opportunity to experience all roles in completion as
individuals may deem important and necessary for themselves. For example, demonstrating
the effects of task completion on ones occupational disposition; stemming from a negotiated
strategy between the doer, the demander and the demand of the activity itself.
Habits
Habit refers to a performance “on an automatic, preconscious level”11,12.
In most of Anxiety Disorders, the immediate rejection of a situation which impends doom or
imminent danger, individuals often automatically avoid the threatening stimulus or shut down
completely so by not responding or pretending it does not exist. Typically individuals not only
will they ignore a challenge at the time, but they may in fact do so for an extended period of
time. This is such any current or future resembles of such situation will also be automatically
overridden.
For example, never performing certain tasks because they invoke an extreme anxiety
response. Occupational therapy may provide a strategy to reframe the stimulus especially if
it falls within ones interest or obligatory function; or to re-adjust maladaptive patterns.

13
Routines
Refer to “occupations with established sequences.”11,12 .
Every occupational being has their own routines or deeply engraved ways of doing or
performing their activities and/or occupations. These take extremely long time to solidify and
even enormously difficult to undo. However, with easier methods of alteration or adaptation,
the routines can be successfully changed. In most instances, people with Anxiety Disorders
have certain rituals and unconventional practices which render them different from the rest of
the society.
These however are geared towards alleviate their debilitating experience due to their anxiety
and/or anticipation of such. While this may be temporarily useful, they also cause the extra
expense in time and effort of execution as well as the quest to master or improve on this
learned behaviour or skill. Practice does not make better, but for them practice makes
permanent and becomes extremely challenging to reverse. Occupational therapy provides
analysis and methods towards adopting ‘healthier’ routines.
5. HEALTH CARE STRUCTURES
5.1 Pillars Of Health Care:
A. Promotion/Prevention
Strategies of Health Care directed at promoting Health (physical, social mental
occupational (activities health) spiritual etc) and wellness and “coping” as an
individual and in groups. For example this may be directed at the public at large, at
“risk” groups or at individuals whom have illness / disabilities. It looks at developing a
healthy life style to support health. Strategies of Health aimed at preventing illness
(primary) or at preventing an existing illness from getting chronic (secondary) or the
client becoming disabled from an illness (tertiary)13.

14
Occupational therapy strategies of this nature for Anxiety Disorders will focus on
occupational practices that would promote healthy adaptation and demote destructive
patterns.
B. Curative/Remedial
Strategies used to help the client to recover from illness or a traumatic event so that
no disability results and that there are few or only minor long term consequences to
function13.
Occupational therapy strategies of this nature emphasis the increased sense of
occupational independence and optimal functioning while incorporating the lived
illness experience.
C. Habilitative/ Rehabilitative
Habilitation refers to a “process of giving a person the resources, including specialized
treatment and training, to promote improvements in activities of daily living, thereby
encouraging maximum independence”. Whereas, rehabilitation refers to “helping
individuals regain skills and abilities that have been lost as a result of illness, injury or
disease, disorder, or incarceration.”12
Occupational therapy strategies in this regard, will focus on expanding support
network as well as retraining personal skills to overcome the residual impact of the
illness experience.
D. Maintenance
Refers to “the process of maintaining or being maintained. The provision of the means
to support life.”14

15
Occupational therapy strategies considered here incorporates maintaining the current
functional levels and curbing any potential deterioration.
Occupational therapy intervention is commonly evidenced in the curative and remedial
levels, since the typical presentation of anxiety and stress states are masked by other
factors. Ones the plausible explanation of the behaviour has been unravelled, the target for
intervention is commonly direct and simple.
While current intervention may halter further deterioration, there are instances where the
contribution to recovery is extremely challenged by the nature/ severity of the Anxiety
Disorders where longer term and regular revision of plan is warranted10,15. This is usually in
the rehabilitative state where the chronicity affects the individual’s capacity to successfully
re-align to their environment, whether at home, work or in relationships.
The OT would also become involved with individuals whose condition shows no further
improvement and thus have to consolidate their occupational performance16,17.
Nevertheless, the current approach for many professions and discipline is to strategize the
health promotion and preventative programmes.
5.2 Level Of Health Care System:
I. Primary
At this level, occupational therapy is concerned with overall occupational performance
and optimal functioning for individuals to independent and productive. Minor factors
are often less emphasized, nevertheless the contribution assists in ‘quick-fix’ or
‘patch-and-go’ strategies. Despite the increased demand to regain control and
strength, often home programme are also issued at this level for further self-help tool.

16
II. Secondary
Occupational therapy at this level is involved with slightly more focus or specific areas
of difficulty. While highlighting occupational performance areas (home, work, activities
of daily living), performance components (cognitive, affective, psychomotor, etc) are
also considered to compliment the intervention strategy. This also affords slightly
more time for contact that in the primary level, however not nearly as much for
intensive contribution.
III. Tertiary
Occupational therapy often employs special or sophisticated techniques5 at this level.
Often a few performance components are pivotal to turning around the debilitating
experience, which in turn presents with severe occupational performance area
functional impact. Level of expertise both clinically and empirically affords the
occupational therapy intervention to offer a highly significant contribution. This is often
evidence by an individual making the necessary changes in their lives and
transforming their innate abilities into remarkable state of occupational performance.
6. ASSESSMENT
6.1 Baseline Assessments
6.1.1 Professional Interview
A professional interview is a structured, time limited and goal directed encounter between
a professional and a client in order to gather data or to discuss an intervention
procedure19.
Interviewing has also been defined as a verbal experience shared, jointly formulated by
the interviewer and the interviewee, or arranged about the asking and answering of
questions18.

17
In addition, an interview can be used as assessment initially, and as intervention during
the course of therapy18. Reasons for interviewing include (a) understanding the client’s
story, what may be referred to as narrative reasoning; (b) building the therapeutic alliance
referred to as cultural reasoning, (c) gathering information and developing the
occupational profile referred to as scientific reasoning, (d) observing behaviour referred to
as interactive reasoning, (e) identifying client strengths and potential problem areas
referred to as conditional reasoning, (f) clarifying your role in the setting referred to as
ethical reasoning, and (g) establishing priorities for intervention referred to as pragmatic/
procedural reasoning.
Interviewing techniques and tools19 may vary in their ranges between children through to
adolescents/youth and adults. Adolescent and adults interviewing tools may include but
not limited to;
(i) The Occupational Circumstances Assessment – Interviewing Rating
Scale or OCAIRS by Hanglund, Henriksson, Crisp, Fredhiem, and
Kielhofner (2001), represent a revision of the original OCAIRS
developed by Kaplan and Kielhofner (1989), provides a method for
gathering data on a client’s occupational adaptation;
(ii) The Occupational Performance History Interview – Second version or
(OPHI-II), a historical interview that gathers information about a client’s
occupational adaptation over time and can be used with adolescents
and adults in variety of settings (Kielhofner et al., 1997).
(iii) The Worker Role Interview or WRI, a semi-structured interview that
gathers data on psychosocial and environmental factors related to work.
It is appropriate to use with an individual whose disability has had an
impact on their participation in work (Handelsman, 1994, Velozo,
Kielhofner, & Fisher, 1998);
(iv) The Work Environment Impact Scale or WEIS, a semi-structured
interview and rating scale designed to examine how individuals with

18
disabilities experience the work environment (Corner, Kielhofner, &
Olson, 1998). The WEIS is intended for use with individuals who are
currently working or are actively anticipating returning to a specific job or
type of work; and
(v) The Canadian Occupational Performance Measure or COPM, a client-
centred semi-structured interview procedure designed to measure
clients’ perceptions of their occupational performance over time (Law,
Baptise, McColl, Opzoomer, Polatajko, & Pollock, 1998).
There are also adjuncts to interview, which may be administered before or after the
interview within the session. These are usually paper-and-pencil self-report measures,
which are differentiated for children and adolescents as well as for adults. These include;
Self-Report Measures for Children and Adolescents:
(i) The Pediatric Interest Profiles or PIPs, paper-and-pencil surveys of
plays and leisure interests designed to be used with children and
adolescents (Henry, 200). The three versions include the Kid Play
Profile or KPP, for children aged 6 to 9; the Preteen Play Profile or PPP,
for children aged 9 to 12; and the Adolescent Leisure Interest Profile or
ALIP, for adolescents aged 12 to 21.
(ii) Children’s Assessment of Participation and Enjoyment and the
Preferences for Activities of Children or CAPE, a two-part self-report
measure that gathers information on children’s participation in everyday
activities outside of mandated school activities (King, Law, King, et al.,
2001)

19
Self-Report Measures for Adults
(i) Interest Checklists – the Neuro Psychiatric Institute or NPI interest
checklist (Matsutsuyu, 1969), contains 80 activity items, grouped into
five categories of daily living, manual skills, cultural and educational
activities, physical sports, and social and recreational activities.
(ii) The Role Checklist or RC, a two-part, paper-and-pencil inventory or 10
occupational roles, including worker, student, family member,
homemaker, caregiver, volunteer, and hobbyist (Oakley, Kielhofner,
Barris, & Reicher, 1986). The first part of the RC examines the client’s
past, present, and future intentions related to performance of each role.
The second part examines the value the client assigns to each role.
(iii) Occupational Self-Assessment or OSA, a self-report measure designed
to gather data on clients’ perception of their occupational competence
(21 items) and the impact of the environment on their functioning (8
items) (Baron, Kielhofner, Iyenger, Goldhammer, & Wolenski, 2001). The
OSA also asks client to indicate the importance of specific areas of
functioning and to identify priorities for change, making it particularly
useful in conjunction with an interview.
(iv) The Occupational Questionnaire or OQ, a paper-and-pencil measure
that gathers data on time-use patterns and feeling about time use
(Smith, Kielhofner, & Watts, 1986). When completing the OQ, clients
indicate their main activity during each half hour of a typical day and
classify each activity as either school, work, ADL, recreation, or rest.
Clients then rate each activity, indicating how well they do the activity,
how important the activity is, and how enjoyable the activity is.

20
6.1.2 Clinical observation
There are four factors that could distort the observation process20, namely:
(a) Perceptual – how sensory stimuli (colour of clothing, perfume) affect the
way the other person is perceived.
(b) Conceptual – the knowledge base brought to the interaction
(c) Role – the way each person perceives the role he or she is to play in the in
the interaction
(d) Self-esteem – the way each person feels about himself or herself
6.1.3 Evaluation
The following are principles of uncovering needs9. This is also termed a collaborative
inquiry; empowerment; client-centred information gathering process.
1. Observation: attending to and interpreting the meaning and purpose of
verbal and non-verbal behaviour in structured and unstructured settings.
The identification of co-morbid psychiatric conditions in patients with
somatic complaints requires astute observation.
2. Measurement: use of standardized tools to provide objective data against
which to measure extent of problem; determine priority domains of
concern, outcomes of intervention and provide feedback on progress. For
example:
(a) Battery of Anxiety Questionnaire (Powell and Enright, 1991)
(b) Occupational Self-Assessment (Baron, Kielhofner et al., 2002)

21
3. Evaluation: use of multi-axial taxonomies to diagnose disorder or ascertain
level of functioning. For example:
(a) DSM-IV-TRTM multi-axial evaluation (American Psychiatric
Association, 2002)
(b) International Classification of Functioning (World Health
Organization, 2001a)
4. Interview: semi-structured information gathering. For example:
(a) Canadian Occupational Performance Measure (Law, Baptise et al.,
1998)
(b) Occupational Performance History Interview (Kielhofner, Mallinson
et al., 1998)
5. Narrative: occupational storytelling and story-making. For example:
Stories of ‘doing’, ‘being’, and ‘becoming’ through preferred occupational
choices across the life span (Clark, Ennevor et al., 1996; Wilcock, 1998a)
6. Consultation: gathering and sharing collateral information from and with
significant others (for example family, partner, employer, teacher); team
members and role players such as community and inter-sectoral
representatives. For example:
Surveys and community forums: participatory inquiry and action methods
to determine scope of need and expectations within a group/community
(Kniepmann, 1997).
Assessment areas21 (may include):
• postural control and balance
• posture during gross motor activities
• physical fitness and endurance
• fine motor skills, manipulation, dexterity, and bilateral coordination
• perceptual skills
• attending behaviour
• attention span and concentration

22
• understanding and following direction
• memory
• problem solving and decision making
• conceptualisation
• categorization
• organizational skills – time and materials
• ability to abstract
• mood or affect
• self-concept
• independence or dependence
• goals and values
• communication
• social roles
• daily living skills
• productivity history, skills, and interests
• leisure skills and interests
Assessment Instruments (refer Table 7-1: Sampling of tests used in evaluation, Hopkins
and Smith)
* Allen Cognitive Level Test (see C.K. Allen, ed. 1985. Occupational therapy for
psychiatric diseases: Measurement and management of cognitive disabilities,
ed. C.K. Allen, 108-113. Boston: Little, Brown & Co. See also C.K. Allen.
1988. Occupational therapy: Functional assessment of the severity of mental
disorders. Hospital and Community Psychiatry 39(3):140-2.)
* Riska Object Classification Test by L.R. Williams (See C.K. Allen. 1985.
Research with a non-disabled population. In Occupational therapy for
psychiatric diseases: Measurement and management of cognitive disabilities,
ed. C.K. Allen, 315-38. Boston: Little, Brown & Co.)

23
* Occupational Therapy Assessment for Older Adults with Depression (See
J.C. Rogers. 1986. Physical and Occupational Therapy in Geriatrics 5(1):13-
33.)
* Bay Area Functional Performance Evaluation, 2nd ed., by S.L. Williams and
J.S. Bloomer, Palo Alto, CA: Consulting Psychologists Press, 1987 (See also
R. Thibeault and E. Blackmer. 1987. Validating a test of functional
performance with psychiatric patients. American Journal of Occupational
Therapy 41(8):515-21; and S.L. Williams and D. Houston. 1986. Use of the
Bay Area Functional Performance Evaluation (BAFPE) with the depressed
patient: A preliminary impression. In Depression: Assessment and treatment
update: Proceedings, 22-25. Rockville, MD: American Occupational Therapy
Association.)
* Stress Management Questionnaire (See F. Stein and J. Smith. 1989. Short-
term stress management programme with acutely depressed in-patients.
Canadian Journal of Occupational Therapy 56(4): 185-92.
* Role Performance Assessment Scale (See M. Good-Ellis. 1986. Quantitative
role performance assessment: Implications and applications to treatment of
depression. In Depression: Assessment and treatment update: Proceedings,
36-48. Rockville, MD: American Occupational Therapy Association; and M.A.
Good-Ellis, S.B. Fine, J.H. Spencer, et al. 1987. Developing a role activity
performance scale. American Journal of Occupational Therapy 41(4): 232-
41.)
* Occupational History (See L.C. Moorhead. 1969. The Occupational history.
American Journal of Occupational Therapy 23:329-34.)
24
Possible problems:
Motor
• The person may exhibit psychomotor retardation (difficulty initiating the
action of moving the body or parts of the body).
• The person may have psychomotor agitation with restlessness and wringing
of the hands.
• The person may have lack physical endurance and fatigue easily
• They may also have idiosyncrasies (a mode of behaviour, peculiar to a
person e.g. tics)
Sensory
* The person may have hallucinations; auditory and visual hallucinations are
the most common but occasionally tactile or olfactory hallucinations occur as
well.
Cognitive
• The person may have difficulty in attending to a task
• The person may express recurrent thoughts of death and suicide
• The person may have difficulty making decisions and solving problems
• The person may have difficulty in finding activities of interest
• [The person may have difficulty in dealing with interactions]
Intrapersonal
• The person may have a poor self-concept or be self-denigrating
• The person may express feelings of helplessness and hopelessness
• The person may be preoccupied with feelings of guilt
• The person may be unable to feel or express emotions
• The person may express fear of going insane or losing his or her mind
• The person may be irritable
• The person may appear agitated
• The person may lack self-confidence
• The person may be dependent

25
• The person may express feelings of worthlessness
• The person may cry for no apparent reason
Interpersonal
• The person may become socially withdrawn
• The person may not speak or speaks with great effort
Self-Care
• The person is usually disinterested in most activities of daily living
• The person may refuse to eat, become anorexic, or lose weight
• The person may have insomnia and awaken early in the morning
Productivity
* The person may be unable to perform job tasks
Leisure
* The person may lose interest in leisure activities formerly enjoyed
6.1.4 Collateral information
This form of inquiry is usually accessed from the source of referral, client/patient’s
immediate relations e.g. family (partner/spouse, sibling, children), friends (peers in
regular contact) and colleagues (manager/supervisor, peers, subordinates).
6.1.5 Assessment report
The report usually varies depending on the purpose and the requestor. Generally
clinical/hospital records for occupational therapy are kept alongside with the medical
records. An occupational therapy clinician also keeps copy of records from which a full
report can be drawn.
A report which may be requested by relevant stakeholders would differ significantly both
in content and format, according to its intentions. The various types of records/ report

26
may include; doctor/specialist (comprehensive medical management), medical aid
(support further treatment/ rehabilitation), insurance (incapacity, disability), attorneys,
educators (school performance, remediation), employers (recruitment, training,
productivity, boarding), individuals (personal), etc.
6.2 Ongoing Assessment
Continuous evaluation is an automatic process that takes place following initial assessment.
While this may not be conducted deliberately, inquiry often requires repetition to construct
and deconstruct as the issues are systematically and gradually delineated22,23,24. The
purpose of interview as an intervention has already been mentioned. In most instances,
parameters considered/ measured at the baseline assessment would also require review by
re-assessing. Alternatively, re-assessment could also assist to clarify the condition from one
to the other, as the therapist builds rapport, observes behaviour and client becomes at ease
to divulge.
Therefore, reasons for subsequent assessment are:
a) For comparison with previous results;
b) To plan subsequent stages of treatment; and
c) To make recommendations for the future.
In essence, the assessment process seeks to:
i) provide accurate and comprehensive information about the problems and needs
presented
ii) assist both client and therapist in setting up realistic goals of treatment
iii) guide the selection of appropriate treatment techniques
iv) measure the extent of the problem before, during and after treatment so that
change can be identified
v) provide data for treatment outcome evaluation and research.

27
Thus it could also be summarized as follows:
A. Interview procedure using internally devised, structured schedules/ questionnaires.
B. Structured observation methods, e.g. behavioural observation, role play trials.
C. Physical examinations, e.g. skin temperature, pulse and respiration rates.
D. Standardized assessment tools/ psychometric tests, e.g. the State-Trait Anxiety
Inventory (Spielberger 1983).
7. INTERVENTION
7.1 Role Of O.T:
The general purpose of occupational therapy intervention would be directed toward enable
a person to become functionally independent and productive25.
7.1 .1 Work
Occupational therapist would assist an individual to become economically viable following
period of illness; in the light of returning to work; searching for job or starting income
generation project.
7.1.2 Activities of Daily Living
Occupational therapist would assist individual to resume autonomas life as prior to
illness, such as fully by performing all their activities or partially by exercising an
opportunity to be assisted.
7.1.3 Leisure
Occupational therapist would assist an individual to re-establish their engagement in
previously enjoyed activities and/or providing a creative environment to construct new
hobbies and interests.

28
7.1.4 Social
Occupational therapist would assist an individual to re-connect with existing support
and/or provide a strategy to network to expand the support.
7.2 Theoretical Framework
7.2.1 Models
A model “is a simplified representation of the structure and content of a system that
describes or explains the complex relationships between concepts within the system and
integrates elements of theory and practice2. In occupational therapy several conceptual
generic occupational performance models have been based on occupations / activities
theory.”
There are many model used in occupational therapy some of which are generic and
most are specific to occupational therapy. A few to note amongst many are (i) Model of
Creative Ability (du Toit, 1974); (ii) Model of Human Occupation (Kielhofner et al 1985,
1997, 2002); (iii) Activities Health (Cynkin and Robinson 1990); (iv) Canadian Model of
Occupational Performance; (v) Occupational Behaviour (Reilly); (vi) Person-
Environment-Occupational Performance Model (Christiansen and Baum, 1997); (vii)
Ecology of Human Performance Model (Dunn et al., 1994); (viii) Personal-Envronment-
Occupation Model (Law et al., 1996); and (ix) Occupational Adaptation Model
(Schkade and Schultz, 1992). It is important to note that models can be used either for
assessment, treatment or in combination.
7.2.2 Frame of References/ Approach
As with the models, approaches and/or frames of references are also numerous and help
discern the application of the model26,11. According to Texeira (2006), frame of reference
is an organized body of knowledge, principles and research findings that forms the
conceptual basis of a particular aspect of practice. An inter-linking of compatible ideas
29
and themes that may be used to direct the thinking for methods of intervention, once
goals and priorities have been established. Are not unique to occupational therapy and
have been developed and used outside the profession13.
Examples of FOR include, Client Centred, Developmental, Cognitive, Behavioural,
Psychodynamic (Object Relations), Sensori-Integration, Learning, Sensory Perceptual,
Cognitive.
For further details on frames of references please refer to Conceptual foundations for
practice in Hagedorn (1997) and Table 4-1: Frames of References used in Occupational
Therapy, page 63 in Hopkins and Smith (1993).
7.3 Treatment Programs
Models of treatment include occupational behaviour (Reilly) and human occupation
(Kielhofner).
Motor
• Increase the person’s energy through participation in energizing activities,
including recreation
• Decreasing the person’s anxiety through participation in relaxing activities
Sensory
* Maintain, decrease or increase sensory stimulation through participation in activities
Cognitive
• Provide opportunities to make choices, solve problems, and make decision in the
selection or colour, type of activity, or amount of time devoted to an activity.
• Provide instruction in time management and activity scheduling.
• Provide learning groups that discuss subjects, such as problems of anxiety

30
Intrapersonal
• Increase self-concept (self-mastery, sense of competence, self-confidence)
through creative activities, such as art, crafts, drama, dance, or music, that can
result in task accomplishment.
• Provide training in stress reduction, including discussion about life stresses,
assertion, and relaxation training.
• Relate present activities to immediate feelings and goals to increase concept of
purposeful activity and goal-directed behaviour.
Interpersonal
• Provide opportunities to develop social and participate in group activities through
structured task groups, discussion groups, or information work-related groups.
• Encourage interpersonal relationships through group activities. Encourage the
person to join a group in the community.
• Increase communication skills, verbal and nonverbal, through practice in group
situations, role playing, discussion, and review
Self-Care
• Express expectations that the person will perform activities of daily living.
• Provide instruction in daily living skills, such as money management, locating living
quarters, shopping, or preparing meals
Productivity
• Encourage the person to participate in home-management tasks. The family can
be encouraged to assign specific tasks for the person to perform
• If the person is working, explore career goals and interests
• If the person is retired, explore the possibility of volunteer activities.
Leisure
* Encourage the person to explore interests and develop enjoyable leisure activities
Precautions

31
• Watch the person to avoid self-inflicted injuries and suicide attempts
• Observe for signs of overmedication, such as tremor and loss of visual acuity.
Prognosis (Functional):
Between the anxiety episodes, there is full recovery of function.
• The person is able to resume his or her previous level of participation in the
community.
• The person is able to perform activities of daily living and functional skills
independently
• The person is able to test reality and control his or her anxiety and mood as well
as activity level independently
• The person is able to perform cognitive activities, including using judgement for
personal safety, decision making, problem solving, and time management.
• The person is able to perform productive activities while setting realistic goals,
conserving or expending energy, and setting limits
• The person assumes responsibility for performing leisure activities
• The person is able to function in one-to-one and group situations.
An anxiety management programme27,28,25
This may constitute, (i) Education, (ii) Skills rehearsal and (iii) Action.
i) Education
The educational element of the course may cover the following topics:
- Physical causes and effects of anxiety and relaxation
- Recognition of physiological cues of arousal
- The benefits of regular exercise
- Negative and irrational thinking and their effects on anxiety levels. (Includes
“catastrophizing”, unhelpful assumptions, unrealistic expectations of self/others)
- Avoidance and its reinforcing properties in relation to anxiety
- Realistic goal setting
- Problem-solving techniques

32
- Social skills and assertiveness as ways of improving confidence in dealing with
relationships and social situations.
ii) Skills
The rehearsal element of the course/ programme may cover arousal reduction skills
which are demonstrated during sessions:
(a) Physical relaxation methods
- Contrast relaxation
- Mitchell method/ Simple relaxation
- Correct breathing
- Emergency relaxation
- Differential relaxation
(b) Mental relaxation methods
- Meditative relaxation (Benson’s relaxation response)
- Visualization
(c) Cognitive control activities
- Imaginal desensitisation exercises
- Role play of stressful situations
- Recognition of faulty thinking, challenging and coping with the anxiety symptoms,
cognitive control exercises
iii) Action
The action element of the course/ programme refers to application of techniques
outside the sessions by individual clients, and may include:
(a) All relaxation methods as appropriate to the situation and individual client’s needs
(b) Self-help task assignments relevant to stage of course/ programme, to consolidate
material covered
(c) Completion of daily diaries and rating scales, e.g. recording stressful situations,
personal reactions and ways of coping, progress in developing relaxation skills

33
(d) Setting and tackling behavioural goals set during the course/ programme.
Anxiety management course: the Client Packs (1,2 & 3)
Pack 1:
This may focus primarily on (a) bodily feelings, (b) thoughts and emotions, and (c) life-
style
(a) Bodily feelings
- Breathing difficulties
- Shakiness
- Pounding heart
- Headaches
- Muscle aches and pains
- Excess sweating
- Bowel and urinary problems
- “Lumps” in the throat
- Persistent tiredness
(b) Thoughts and emotions
Fear of variety of things, people or situations due to anxiety
- Going out of doors
- Meeting people
- Travelling on public transportation
- Ill-health
(c) Life-style
Life-style may be seriously curtailed by a tendency to avoid stressful situations or
escaping them wherever possible. This might include:
- Not going out
- Not meeting people
- Not using public transport

34
- Not being able to do the shopping
- Not being able to stand up for oneself
Example of solution: Contrast Muscle Relaxation, which covers each major muscle
group. Parts of the body worked on include hands and forearm; upper arms; face;
neck; chest, shoulders and back; stomach and legs.
The rest of the packs will address the following (refer Keable, 1989 for further details
on all the packs):
2 = physical tension control
3 = how to apply relaxation skills in everyday life, respectively
4 = mental tension control
5 = the stress of modern living and how to cope with it
6 = goal-setting and problem-solving techniques
7 = improving your life-style and coping with people
7.4 Time-Span An average number of sessions required informed by clinical judgement and empirical
evidence.
Total number of sessions per year for both acute and chronic:
- Assessment: 486
- Treatment: 2003
8. TABLE OF THE EVIDENCE
(See appendix)

35
9. CONCLUSION
Anxiety Disorders are common in our modern society, however not a common place in
occupational therapy. There has been a considerable improvement in intervention of such
disorders in the recent years, particularly pharmacotherapy. While this is the case,
psychotherapy has also established its role especially as augmentation to pharmacotherapy.
The two therapies have thus subsequently being studied together and substantial evidence
has been well developed. The reality is that, occupational therapy has also formed an
integral part of such intervention, despite the lack of studies which demonstrate this as a
combination with the two conventional approaches.
Nevertheless, there is sufficient proof that occupational therapy on its own has showed its
effectiveness as a single measure of progress and improvements.
Arguably occupational therapy focuses more on the practical functional aspects than on
biological and psychological functioning respectively. Hence, occupational therapy not only
identifies the problem from an empirical/ scientific point of view, it also offers artistic/ creative
solution to everyday challenges.

10. REFERENCES
1. Occupational Therapy Association of South Africa (OTASA). Internet website.
www.otasa.org.za; 2001.
2. Creek J. Occupational Therapy and Mental Health. Edinburgh, London, New York, Oxford,
Philadelphia, St Louis, Sydney, Toronto, Churchill Livingstone; 2002.
3. Mogotsi M, Kaminer D, Stein DJ. "Quality Of Life In The Anxiety Disorders." Harvard Review of
Psychiatry. 2000; 8(6): 273-282.
4. Lochner C, Mogotsi M, du Toit PL, Kaminer D, Niehaus DJ, Stein DJ. Quality of life in anxiety
disorders: a comparison of obsessive-compulsive disorder, social anxiety disorder, and panic
disorder. Psychopathology. 2003 Sep-Oct;36(5):255-62.
5. Heuer L. "The Occupational Therapy Approach To The Management Of Children With Anxiety
Disorders." Institute For Occupational Therapy In Private Practice (INSTOPP). 2006; 3: 11-13.
6. World Health Organization. International Classification of Diseases (ICD) - 10th Version. (2006).
7. American Psychiatric Association. Diagnostic And Statistical Manual of Mental Disorders.
Washington, American Psychiatric Association. (1996).
8. Kaplan HI, Sadock BJ, Grebb JA. Kaplan And Sadock's Synopsis of Psychiatry: Behavioural
Sciences Clinical Psychiatry. Baltimore, Philadelphia, Hong Kong, London, Munich, Sydney
and Tokyo, Williams & Wilkins; 1994.
9. Crouch R, Alers V. Occupational Therapy In Psychiatry And Mental Health. London &
Philadelphia, Whurr; 2005.
10. Bonder BR. Psychopathology and Function. New Jersey, SLACK Inc. (1991).

37
11. Hagedorn R. Foundations for practice in Occupational Therapy. New York, Edinburgh, London,
Madrid, Melbourne, San Fransisco and Tokyo, Churchill Livingstone; 1997.
12. Jacobs K. Quick Reference Dictionary. New Jersey, SLACK Incorporated; 1997.
13. Texeira L. Definition and Terms in Occupational Therapy, University of the Witwatersrand.
Unpublished; 2006.
14. The Concise Oxford Dictionary, Oxford University Press. (1990).
15. Mountford SW. Orientation To Occupational Therapy: A fundamental approach to Principles
and Practicalities. Cape Town, College Tutorial Press; 1992.
16. Shader RI. Manual of Psychiatric Therapeutics. Philadephia, Baltimore, New York, London,
Buenos Aires, Hong Kong, Sydney and Tokyo, Lippincott Williams & Wilkins; 2003.
17. Willson M. Occupational Therapy In Long-Term Psychiatry. Edinburgh, London, Melbourne
and New York, Churchill Livingstone; 1987.
18. Crepeau Eb, Cohn SE, Boyt BA. Willard and Spackman’s Occupational Therapy. 10th Edition.
Lippincott Publishers. 2003
19. Mogotsi MJ. Skills Laboratory: Interviewing Skills, University of the Witwatersrand.
Unpublished; 2006.
20. Willson M. Occupational Therapy in Short-term Psychiatry. Malaysia, Churchill Livingstone;
1996.
21. Reed KL. Quick Reference To Occupational Therapy. Maryland, Aspen Publishers, Inc; 1991.

38
22. Hopkins HL, Smith HD. Willard And Spackman's Occupational Therapy. Philadelphia, J.B.
Lippincott Company; 1993.
23. Howe MC, Schwartzberg SL. A Functional Approach to Group Work in Occupational Therapy.
Philadelphia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney and Tokyo,
Lippincott Williams & Wilkins; 2001.
24. Paul S. "Culture and its influence on occupational therapy evaluation." Can J Occup Ther.
1995; 62(3): 154-61.
25. Gilkeson GE. Occupational Therapy Leadership: Marketing Yourself, Your Profession, and
Your Organization; 1997.
26. Bruce MA, Borg B. Psychosocial Occupational Therapy: Frames Of Reference For
Intervention. Thorofare, SLACK Inc. (1993).
27. Keable D. The Management of Anxiety: A Manual For Therapist. Edinburgh, London,
Melbourne and New York, Churchill Livingstone; 1989.
28. Prabst-Hunt W. Occupational Therapy Administration. Australia, Canada, Mexico, Singapore,
Spain, United Kingdom and United States, Delmar Thomson Learning; 2002.
29. Kielhofner G. Model of Human Occupation: Theory and Application. Maryland and
Pennsylvania, Lippincott Williams & Wilkins; 2002.
30. Henry AD. Introduction to Evaluation and Interviewing: The Interview Process in Occupational
Therapy; 2003.

39
APPENDIX - The Table of evidence
Author Title Source Study population
Type of design
Treatment group
Outcome variable
Findings
Larun L,
Nordheim LV,
Ekeland E,
Hagen KB,
Heian F
Exercise in
prevention
and
treatment of
anxiety and
depression
among
children and
young people
(Cochrane
review)
Cochrane
Database of
Systematic
Reviews
2006;Issue
3
systematic
review
Whilst there appears
to be a small effect in
favour of exercise in
reducing depression
and anxiety scores in
the general
population of children
and adolescents, the
small number of
studies included and
the clinical diversity
of participants,
interventions and
methods of
measurement limit
the ability to draw
conclusions. It makes
little difference
whether the exercise
is of high or low
intensity. The effect of
exercise for children
in treatment for
anxiety and
depression is
unknown as the
evidence base is
scarce.
Kirkwood G,
Rampes H,
Tuffrey V,
Richardson J,
Pilkington K
Yoga for
anxiety: a
systematic
review of the
research
evidence
British
Journal of
Sports
Medicine
2005
Dec;39(12):
884-891
systematic
review
Owing to the diversity
of conditions treated
and poor quality of
most of the studies, it
is not possible to say
that yoga is effective
in treating anxiety or

40
anxiety disorders in
general. However,
there are
encouraging results,
particularly with
obsessive
compulsive disorder.
Further well
conducted research
is necessary which
may be most
productive if focused
on specific anxiety
disorders.
Jorm AF,
Christensen
H, Griffiths
KM, Parslow
RA, Rodgers
B, Blewitt KA
Effectiveness
of
complementa
ry and self-
help
treatments
for anxiety
disorders
Medical
Journal of
Australia
2004;181(7
Suppl):S29-
S46
systematic
review
The treatments with
the best evidence of
effectiveness are
kava (for generalised
anxiety), exercise (for
generalised anxiety),
relaxation training (for
generalised anxiety,
panic disorder, dental
phobia and test
anxiety) and
bibliotherapy (for
specific phobias).
There is more limited
evidence to support
the effectiveness of
acupuncture, music,
autogenic training
and meditation for
generalised anxiety;
for inositol in the
treatment of panic
disorder and
obsessive-
compulsive disorder;
and for alcohol

41
avoidance by people
with alcohol-use
disorders to reduce a
range of anxiety
disorders.
Dunn AL,
Trivedi MH,
O'Neal HA
Physical
activity dose-
response
effects on
outcomes of
depression
and anxiety
Medicine
and Science
in Sports
and
Exercise
2001
Jun;33(6
Suppl):S587
-S597
systematic
review
All evidence for dose-
response effects of
physical activity and
exercise come from B
and C levels of
evidence. There is
little evidence for
dose-response
effects, though this is
largely because of a
lack of studies rather
than a lack of
evidence. A dose-
response relation
does, however,
remain plausible
Scaffa ME,
Gerardi S,
Herzberg G,
McColl MA.
The role of
occupational
therapy in
disaster
preparedness
, response,
and recovery.
Am J Occup
Ther. 2006
Nov-
Dec;60(6):6
42-9
Beutel ME,
Gerhard C,
Wagner S,
Bittner HR,
Bleicher F,
Schattenburg
L,
Knickenberg
R, Freiling T,
Kreher S,
Martin H.
Reduction of
technology
fears in
psychosomati
c
rehabilitation-
-concepts
and results
based on a
computer
training for
older
Z Gerontol
Geriatr.
2004
Jun;37(3):2
21-30

42
employees
Watanabe N,
Machleidt W.
Morita
therapy--a
Japanese
method for
treating
neurotic
anxiety
syndrome
Nervenarzt.
2003
Nov;74(11):
1020-4.
The treatment
consists of an initial
7-day period of strict
and isolated rest in
bed followed by step-
by-step occupational
therapy and final
reintegration into job
and family.
Simo-Algado
S,
Mehta N,
Kronenberg
F,
Cockburn L,
Kirsh B.
Occupational
therapy
intervention
with children
survivors of
war.
Can J
Occup Ther.
2002
Oct;69(4):2
05-17.
The
intervention
was based
on a
community-
centred
approach
with
spirituality as
a central
focus of the
intervention.
The Model of
Human
Occupational
and the
Occupational
Performance
Process
Model were
utilized to
guide the
identification
and
intervention
of
occupational
performance
issues.
With increasing
awareness of
populations facing
social and political
challenges, there is a
growing importance
of the concept of
occupational justice
and the need to work
against occupational
apartheid.
Lohman H,
Royeen C
Posttraumatic
stress
disorder and
traumatic
hand injuries:
a neuro-
occupational
view.
Am J Occup
Ther. 2002 Sep-
Oct;56(5):527-37
Neuro-
occupation is
an evolving
concept that
combines
knowledge
and
understandin
g of
occupation
with
knowledge
and
understandin
g of how the
human brain
functions in
environmenta
l context
a query about the
value of neuro-
occupation as a
developing
theoretical construct
is put forth.
Rosenheck
R,
Stolar M,
Fontana A.
Outcomes
monitoring
and the
testing of
new
psychiatric
treatments:
work therapy
in the
treatment of
chronic post-
traumatic
stress
disorder.
Health Serv
Res. 2000
Apr;35(1 Pt
1):133-51
Questionnair
es
documented
PTSD
symptoms,
violent
behavior,
alcohol and
drug use,
employment
status, and
medical
status at the
time of
program
entry and
four months
after
discharge
from the
hospital to
Substantively this
study suggests that
work therapy, as
currently practiced in
VA, is not an effective
intervention, at least
in the short term, for
chronic, war-related
PTSD

43
the
community.
Davis J,
Kutter CJ.
Independent
living skills
and
posttraumatic
stress
disorder in
women who
are
homeless:
implications
for future
practice.
Am J Occup
Ther. 1998
Jan;52(1):39-44.
Twenty-four
women
residing in a
supportive
housing
shelter in
Kansas City,
Missouri,
volunteered
to participate
in this study.
The
participants
were
evaluated for
independent
living skills
with the
Kohlman
Evaluation of
Living Skills.
Results suggest that
occupational
therapists have a
major role to play,
evaluating and
facilitating
independent living
skills, as members of
multidisciplinary
treatment teams in
supportive housing
programs for persons
who are homeless.
Phillips ME,
Bruehl S,
Harden RN.
Work-related
post-
traumatic
stress
disorder: use
of exposure
therapy in
work-
simulation
activities.
Am J Occup
Ther. 1997
Sep;51(8):696-
700.
Bavaro SM.
Occupational
therapy and
obsessive-
compulsive
disorder.
Am J Occup
Ther. 1991
May;45(5):456-8.
Menks F.
Behavioral
techniques in
Am J Occup
Ther. 1979
A case
history is
The results support
the effectiveness of

44
the treatment
of a writing
phobia.
Feb;33(2):102-7. presented in
which
progressive
muscle
relaxation,
diaphragmati
c breathing,
and flooding
were used to
extinguish
and
countercondit
ion a writing
phobia in a
junior-year
occupational
therapy
student.
these techniques
(systematic
desensitization and
the extinction
techniques of
implosion therapy
and flooding) in
modifying
maladaptive anxiety
or fear arising from a
situation that is not
objectively
dangerous.
Lambert RA,
Harvey I,
Poland F.
A pragmatic,
unblinded
randomised
controlled
trial
comparing an
occupational
therapy-led
lifestyle
approach and
routine GP
care for panic
disorder
treatment in
primary care.
J Affect
Disord. 2006
Sep 29
16 week
unblinded
pragmatic
randomised
controlled
trial in 15
East of
England
primary care
practices (2
Primary Care
Trusts).
Follow-up at
20 weeks
and 10
months.
Control arm,
unrestricted
routine GP
care. Trial
Arm,
Occupational
A lifestyle approach
may provide a
clinically effective
intervention at least
as effective as routine
GP care, with
significant
improvements in
anxiety compared
with routine GP care
at the end of
treatment.

45
therapy-led
lifestyle
treatment
comprising:
Beck Anxiety
Inventory.
46
ATTENTION DEFICIT HYPERACTIVITY DISORDER
Compiled by Keri-Lee Roebert BSc (Occupational Therapy) (Wits) Post-graduate Diploma in Group Activities (Pretoria)
1. INTRODUCTION
The occupational therapist has a vital role to play in the field of Psychiatry. She assists the
client to engage in more satisfying relationships and to display appropriate emotional
responses, treats specific problems, and aids in diagnosis. 1
She assesses and treats clients with visual perceptual and co-ordination difficulties. These
problems may occur in children with a variety of medical and psychiatric diagnoses. One
diagnosis in which these are frequently encountered is Attention Deficit Hyperactivity
Disorder (hereafter referred to as ADHD). 2
Referrals may come from a variety of settings and can include, but are not limited to:
• Hospitals,
• Schools and
• Private practice
2. THE DIAGNOSIS OF ADHD
According to the DSM-IV 3, ADHD can be predominantly inattentive type, or impulsive type,
or combined type. Symptoms need to cause impairment in two or more settings, e.g.
school/work and at home. There needs to be clinically significant impairment in social,
academic or occupational functioning.
There are a number of disorders associated with ADHD: 4, 5
• Specific Learning Disabilities
o Visual perceptual problems
o Auditory perceptual problems

47
o Delays in fine motor development
• Other disruptive behaviour disorders
o Oppositional Defiant Disorder
o Conduct Disorder
• Emotional difficulties
o Anxiety Disorder
o Depressive illness
• Tourette's Disorder/Syndrome
• Obsessive Compulsive Disorder
3. THE IMPACT OF ADHD ON OCCUPATION
Occupation refers to what a person "does". It refers to a person's work (or school for the
school-going child and adolescent), activities of daily living (ACTIVITIES OF DAILY LIVING),
and social and leisure activities.
Children with ADHD may experience significant functional problems, such as difficulties at
school with academic underachievement, problematic interpersonal relationships with family
members and peers, and a low self esteem. These symptoms may persist into adolescence
and adulthood. 5 As a result, the person's occupation could be negatively impacted upon at
all stages of their life, resulting in them not functioning optimally in any of the above
mentioned areas, i.e. work/school, activities of daily living, social activities and leisure
activities. 3.1 Work/School
A number of areas of academic difficulty have been identified for ADHD students: 6, 7
• Work rate

48
They do little or no independent work and must be reminded continuously to return to the
task at hand. They often procrastinate on academic tasks. Work is done extremely
rapidly, with little attention to instructions and careless errors. The work rate can also be
so slow that written work is rarely completed within the given time constraints.
• Reading
They often reverse letters, inverse the letter order in words, confuse or transpose relatively
common words, produce dysgraphic misspellings, and make frequent visual substitutions
in oral reading. They can be so inattentive and distracted while reading that their
comprehension of the material is significantly impaired, or they process the reading
material so slowly that they forget the initial part of a paragraph or even a single sentence
before coming to its end.
• Writing
They write rapidly and pay little attention to the quality and legibility of their work. The
rules of punctuation and capitalisation are often ignored. Some learners exhibit an
extremely slow handwriting rate and their work appears methodical and laborious.
• Spelling
They lack the attention and focus to memorise spelling rules and patterns.
• Mathematics
They exhibit difficulty in computational accuracy and organization. Mathematical problems
are frequently miscopied, sloppily written, and they make numerous errors due to lack of
attention.
• Oral instructions
Their inattention and distractibility play a significant role in their ability to follow oral
instructions.
• Thought processing
Amongst others, they have difficulty understanding, organising and prioritising their
thoughts.

49
• Attention focusing
They have difficulty sustaining attention, refocusing attention and blocking out distractions.
• Visual and auditory memory
Their inattentiveness affects their visual and auditory memory. They have difficulty
processing short-term memory to long-term memory.
• Prioritising
They battle to select the main idea in reading, listening or writing.
• Bridging
Remembering two or more instructions and linking one fact to another is problematic for
them.
• Decoding
They do not comprehend what is read, understand abstract concepts, or connect cause-
and-effect.
• Encoding
They have difficulty finding the correct word with which to express their ideas.
• Neatness
Their work is untidy and often full of smudges.
• Recalling
They forget to bring materials and completed work to school and have difficulty recalling
isolated facts such as names and dates.
• Organizing
They have difficulty ordering things into a logical sequence, selecting important information
and leaving out unnecessary aspects.

50
• Perceiving spatial relationships
They have poor left-right discrimination, form constancy figure-ground perception and
struggle with basic concepts, such as size, colour and shape.
• Eye-hand co-ordination
They struggle with visual tracking, do not keep their place while reading and have poor
handwriting.
• Content areas
They have difficulty with note taking and organisation, they fail to follow through on oral
instructions and do not complete homework. They have difficulty structuring and
organising their study time.
Children with perceptual-motor problems (such as perceiving spatial relationships and eye-
hand co-ordination, mentioned above) may also have some additional emotional problems.
These emotional difficulties may be precipitated by the stress they experience in dealing with
their perceptual-motor problems. In many other instances, a primary emotional stress
exacerbates an underlying perceptual-motor problem. The occupational therapist working
with children referred for visual perception or co-ordination problems needs to pay attention
to these emotional needs in therapy as treatment needs to be holistic. 2
Adolescents may be inattentive, withdrawn, impatient, intellectually dependent, have
negative feelings towards school, and poor relationships with peers and teachers. They may
also have secondary emotional problems which in turn, cause a drop in school performance.
A negative cycle develops, with poor academic performance causing low self-esteem which
contributes to further emotional problems and so on. 8 As with children, the occupational
therapist also needs to pay attention to the emotional problems as the adolescent is viewed,
and therefore treated, holistically.
Adults with ADHD experience difficulty in the sphere of work as they are unable to maintain a
job. They often change jobs frequently due to impulsivity. They are unable to form stable,
appropriate interpersonal relationships with work colleagues and superiors. They often have

51
unconsolidated pre-vocational skills. This will impact on their personal presentation, social
presentation and work competency skills in the work place.
3.2 Activities of Daily Living
The person with ADHD usually has the age appropriate skills to perform activities of daily
living activities. The quality of these activities, however, is usually poor. They show little
attention to detail and their impulsivity results in them completing tasks hastily and untidily.
3.3 Leisure Activities
A person with ADHD has difficulty organising and planning. As a result, they may not be
actively engaged in constructive leisure activities as they experience difficulty in planning
their time and organising appropriate activities.
They may also be involved in inappropriate leisure activities, such as those requiring high
risk, due to their risk-taking behaviour.
If they are involved in leisure activities, e.g. team sports, their behaviour is often
inappropriate and impulsive on the sports field resulting in them receiving disciplinary action,
e.g. a yellow card.
3.4 Social Activities
A person is required to function on a social level in all areas of their life. People with ADHD
have difficulty forming and maintaining appropriate relationships, whether they are with
subordinates, colleagues or authority figures at work, their friends on an informal level or
intimate relationships.

52
4. THE IMPACT OF ADHD ON ROLES, HABITS AND ROUTINES
A person with ADHD may not form appropriate interpersonal relationships. This impacts on
their ability to fulfil their roles; such as father/mother, son/daughter, worker/scholar/student,
friend, appropriately. Due to their impulsivity and poor planning, they may also experience
difficulty in balancing their roles appropriately; for example, they may spend an inappropriate
amount of time being a volunteer when they need to be involved in full-time paid
employment.
The risk-taking behaviour of people with ADHD, especially adolescents and adults, could
result in them engaging in risk-taking habits, such as drug use. They are also more inclined
to drive under the influence of alcohol.
They have difficulty planning and adhering to a routine due to poor planning and
organisational skills. They need firmly established boundaries so they know what is
expected of them. They cope better with changes in routine when prepared in advance for
this.
5. LEVELS OF HEALTHCARE AND PILLARS OF HEALTH IN RELATION TO ADHD
5.1 The Levels of Healthcare
The treatment of ADHD is largely at a primary level as clients are usually seen on an "out
patient" basis. A client is rarely seen in a hospital (secondary level) or academic hospital
(tertiary level) for the treatment of ADHD. If this is the case it is normally for the treatment of
a co-morbid condition, such as a behavioural or emotional disorder.
5.2 The Pillars of Health
Treatment at a preventive level involves educating educators and parents in the identification
of the symptoms of ADHD so that the child can be referred to the appropriate healthcare
professional.

53
Promotive care, in the case of ADHD, takes more of a consultative role, where the
occupational therapist can assist the educator in structuring the classroom, for example, so
that optimal learning can take place for the ADHD student. The occupational therapist can
also be involved in the work place where the employer is consulted with in terms of making
reasonable accommodations for the person with ADHD at work.
Treatment of ADHD takes place largely on a curative level where the occupational therapist
treats both the internal performance components, e.g. impulsivity, and the occupational
performance area, e.g. school/work, which have been impacted upon.
At a rehabilitative level, clients are given the necessary coping skills to function as optimally
as possible, within the limitations of their ADHD, and to maintain their quality of life.
6. ASSESSMENT OF ADHD
Assessment and evaluation is an ongoing process. It needs to precede treatment, be
repeated at least once during intervention, and conclude the therapy process. 1
6.1 Referral
A referral for an occupational therapy assessment may be made by a psychologist, doctor,
physiotherapist, speech therapist or teacher. It is recommended that if long-term therapy is
required the referral comes from a doctor. 2
6.2 Interview
An interview is conducted with the parent/guardian/caregiver in the case of a child or the
client himself if an adolescent or adult. During the interview detailed background information
is gathered. Information gained during the interview often clarifies or expands on the
assessment findings1, 2, 8. If a background questionnaire has been completed by the
parent/guardian/caregiver/client prior to the interview, the interview can be expected to take
half an hour. 2 If not, a longer time will be needed.

54
6.3 Evaluation
The occupational therapy assessment evaluates the client holistically.
During evaluation the occupational therapist observes the child's: 1
• Behaviour
• Conduct
• Motor behaviour
• Attention span
• Play
• Language
• Activities
• Habitual manipulations
• Sexual behaviour
• Mood
• Relationships towards peers and staff
The adolescent's environment and community (family, culture and peer group), basic abilities
(cognition, affect and conation), task performance (school, leisure time, ACTIVITIES OF
DAILY LIVING and interpersonal relationships) and aspects specific to adolescents
(developmental tasks and values) should all be assessed. 8
The occupational therapist makes use of standardised and non-standardised assessment
tasks.
The choice of tests used depend upon factors such as the age of the child, presenting
problems, the time available for assessment and the occupational therapist's qualifications
and experience. 2
Non-standardised assessment tasks are, for example, cutting with a pair of scissors, ball
throwing and catching, and handwriting samples. 2 With adolescents, for example, activities
are used, where they are required to produce an end product, which assess their internal

55
components and functional abilities. 8 Group sessions assist in assessing a client's
dysfunction in terms of interpersonal relationships. 8
Below is a table of some of the standardised tests available to occupational therapists to
assess a client diagnosed with ADHD: 1, 2, 8
Test Age Aspects assessed
The Test of Visual Motor
Integration (3rd revision)
(Beery, K.E.)
4 years 0 months to
17 years 11 months
Visual motor integration ability:
• Visual perception
• Transducing
• Motor reproduction
Developmental Test of
Visual Perception (2nd ed)
(DTVP-2)
(Hammill,et al)
4 years to 10 years
11 months
Eye-hand co-ordination
Motor reduced visual perception
Visual motor integration
Test of Visual Perceptual
Skills (TVPS non-motor)
(Gardner, M.F.)
4 years to 12 years
11 months Visual perception (no motor skills are required)
Test of Visual Perceptual
Skills (non-motor) Upper
Level (TVPS-UL)
(Gardner, M.F.)
12 years to 17 years
11 months Visual perception (no motor skills are required)
Test of Visual Motor Skills
(TVMS)
(Gardner, M.F.)
2 years to 12 years
11 months Visual motor integration ability
Test of Visual Motor Skills
Upper Level (TVMS-UL)
(Gardner, M.F.)
12 years to 39 years
11 months Visual motor integration ability
Motor-free Visual
Perceptual Test (MVPT)
(Colarusso and Hammill)
4 years to 8 years
11 months
Screening test of visual perception (no motor skills are
required)
Test of Motor Impairment
(Stott, Moyes Henderson) 5 years to 11 years Fine and gross motor co-ordination
Pre-School Test
(Geselle Institute of
Human Development)
2 years 6 months to
6 years
Fine and gross motor co-ordination
Visual perception
Visual motor integration
Language

56
Southern California
Sensory Integration Test
(Ayres, A.J.)
4 years to 10 years
11 months
Visual perception
Somatosensory perception
Fine and gross motor co-ordination
Clinical Observations
(Ayres, A.J.)
4 years to 10 years
11 months
Gross motor co-ordination
Neurological screening
Modular Arrangement for
Predetermined Time
Standards
Adolescents and
adults
Applied to assess school and work functioning in terms of
physical tasks
The evaluation varies from 1 ½ to 3 hours, depending on the client's tolerance, attention
span and age1, 2. Sometimes an evaluation needs to be divided into two or three sessions.
6.4 Assessment Report
The assessment report is a compilation of information obtained during the interview and
evaluation. The information contained in the report is used to:
• Plan a therapy programme
• Evaluate progress after a period of treatment
• Inform other professionals involved in the client's treatment
6.5 The Feedback Interview
Finally, feedback is given on the assessment findings. Feedback is usually given to parents
to discuss the findings of the assessment and to make recommendations based on the
findings. 2
7. APPROACHES, PRINCIPLES AND TECHNIQUES USED
The occupational therapist forms part of the multi-disciplinary team. The team decides on
the best therapeutic approach and handling strategies to use for a client and all involved in
the treatment of the client are expected to adhere to the decision. 1, 8
57
7.1 Approaches
The occupational therapist uses a variety of approaches during therapy. They may use one
approach or a combination of approaches for a single client to direct therapy.
7.1.1 Client centered approach
Occupational Therapists make use of a client centered approach whereby the client is
involved in the decision making process regarding the direction of their therapy. Their
interests, roles, needs and habits are taken into consideration during therapy.
7.1.2 Analytical approach Therapy is directed at improving the client's insight and understanding of himself and their
environment. The occupational therapist does not interpret, but assists the client to reflect
on the past and their feelings. 8
7.1.3 Interactive approach
This approach is used largely during occupational group therapy where focus is on the here
and now, and on the interaction between the group members and the insight the client gains
from this. 8
7.1.4 Cognitive-behavioural approach
The client learns to solve problems more effectively, and acquires new skills in interpersonal
relationships, e.g. assertiveness training. 8
7.1.5 Behavioural approach
Therapy aims at changing dysfunctional behaviour, and learning and reinforcing appropriate
behaviour.
58
7.2 Principles and Techniques
Based on assessment findings a detailed treatment programme is planned.
Therapy with children is usually through the medium of play, and they are usually treated
individually. 1
Occupational group therapy is the therapy of choice for adolescents and adults, particularly
where their interpersonal relationships are dysfunctional. 8
As clients are treated holistically, the occupational therapist will address concurrent
emotional and behavioural problems, as well as any perceptual and co-ordination problems
so that the treatment programme can be implemented effectively. 2
Once the treatment programme has been drawn up, the occupational therapist needs to
decide on the duration and frequency of the treatment sessions. Each individual session
usually lasts from half an hour to one hour and the client could be seen once or twice a
week. Two ½ hour sessions a week are often more beneficial for the young, preschool child
than one longer session once a week. 2
If the client is treated in a group, the treatment session is usually 1 ½ hours long.
Appropriate activities are selected for therapy taking, amongst others, the following into
account: 2
• The principles of therapy
• The client's level of motivation and action 9
While a child is receiving occupational therapy, the parents need to observe and discuss the
treatment programme with the occupational therapist. These appointments need to be
arranged regularly (monthly or once a quarter). The frequency of these appointments will
depend on the nature and severity of the child's problems. 2

59
Most clients requiring occupational therapy require it for an extended period of time, i.e. 12 to
18 months. 2
6. RESEARCH EVIDENCE
Author Study population
Type of design
Treatment group
Outcome variable
Findings
Abrahams,
Creighton,
Naidoo, Parker,
Pillay and
Wegner (1999)
Adolescents in
grade 10 at a
high school in a
low socio-
economic area
of the Western
Cape, South
Africa
Qualitative
research design
Life skills
programme with
16 grade 10
learners: 7 boys
and 9 girls
whose ages
ranged from 14
to 16 years
Reflective
worksheets and
journals after
life skills groups
Life skills have
a positive effect
on adolescents
in terms of
independent
adjustment
Arnold, Clark,
Sachs, Jakim
and Smithies
Primary school
children who
met the criteria
for ADHD with
hyperactivity
Controlled
clinical trial
30 primary
school children
who met the
criteria for
ADHD with
hyperactivity
Behaviour
ratings
Behaviour
ratings showed
significant
improvement at
the end of the
last treatment
and at follow-up
1 year later
Schilling,
Washington,
Billingsley and
Deitz (2003)
Children with
attention deficit
hyperactivity
disorder
A single subject,
A-B-A-B
interrupted time
series design
American 4th
grade children
(2 boys, 1 girl)
with ADHD
In-seat
behaviour and
legible word
productivity
The use of
therapy balls for
students with
ADHD may
facilitate in-seat
behaviour and
legible word
productivity
Shaffer,
Jacokes,
Cassily,
Greenspan,
Tuchman,
Stemmer
Boys, 6-12
years old, with
attention deficit
hyperactivity
disorder
Controlled
clinical trial
56 boys, 6-12
years old
previously
diagnosed with
ADHD
Cognitive and
motor skills
The Interactive
Metronome
training appears
to facilitate a
number of
capacities;

60
including
attention, motor
control, and
selected
academic skills
in boys with
ADHD
Van Den Berg
(2001)
Children with
attention deficit
hyperactivity
disorder
Qualitative
research design
4 American
students with
ADHD
On-task
behaviour
during fine
motor activities
in the classroom
Wearing a
weighted vest
increased on-
task behaviour
by 18-25%
7. CONCLUSION
Literature shows that occupational therapy intervention has a significant impact on the
performance capacity of people with ADHD in all spheres of life. It is, therefore, clear that
the occupational therapist has a vital roe to play in the assessment, treatment and
management of this disorder.

61
8. REFERENCES 1. Crouch, R.B. Occupational Therapy in Child Psychiatry in Crouch, R.B. and Alers,
V.M. Occupational Therapy in Psychiatry and Mental Health, 3rd ed. Maskew Millar
Longman: South Africa. 1997.
2. Kitchin, L.M. Occupational Therapy for Children with Perceptual, Motor and Emotional
Difficulties in Crouch, R.B. and Alers, V.M. Occupational Therapy in Psychiatry and
Mental Health, 3rd ed. Maskew Millar Longman: South Africa. 1997.
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
Disorders, 4th ed. American Psychiatric Association: Washington. 1994.
4. Attention Deficit Hyperactivity Booklet. Sponsored by Novartis.
5. Committee on Quality Improvement, Subcommittee on AD/HD. Clinical Practice
Guidelines: Diagnosis and Evaluation of the Child with Attention-Deficit/Hyperactivity
Disorder. American Academy of Paediatrics. Vol 105, No 5. May 2000.
6. Taylor, J.F. The ABC's of ADD and Related Conditions for Parents, Teachers,
Counsellors and Other Involved Caregivers. 2002 International Conference on
Attention Deficit Hyperactivity Disorder and Co-Morbid Disorders. Pretoria, 2002.
7. Copeland, E. Academic Problems of ADHD/ADD Students. 2002 International
Conference on Attention Deficit Hyperactivity Disorder and Co-Morbid Disorders.
Pretoria, 2002
8. Post, L. and van Antwerpen, T. Occupational Therapy with Adolescents in Crouch,
R.B. and Alers, V.M. Occupational Therapy in Psychiatry and Mental Health, 3rd ed.
Maskew Millar Longman: South Africa. 1997.
9. Du Toit, V. Patient Volition and Action in Occupational Therapy. Vona and Mariè du
Toit Foundation: South Africa. 1991.

62
DEMENTIA
Compiled by Michele Nye National Diploma Occupational Therapy(Pretoria) BSc (UNISA)
Post-graduate Diploma in Interpersonal Communication and Group Technique(Pretoria)
Post-graduate Diploma in Vocational Rehabilitation(Pretoria)
1. INTRODUCTION
Dementia has far reaching consequences for patients and their primary care givers and is
currently a major driver of costs in health care and social systems in developed countries.
Major problems are the losses in independence, initiative, and participation in social
activities, decreasing the quality of life of patients and putting pressure on both family
relationships and friendships. Care givers often experience feelings of helplessness, social
isolation, and loss of autonomy. Occupational therapy is found to be effective in treatment
and assessment of dementia. The primary focus of such a therapy is to improve patients'
ability to perform activities of daily living and hence promote independence and participation
in social activities and to reduce the burden on the care giver by increasing their sense of
competence and ability to handle the behavioural problems they encounter. These outcomes
are increasingly being considered equally or even more clinically relevant than measures of
cognitive outcome.1
Referrals may come from various sources and can include, but are not limited to:
• Other health professionals
• Hospitals
• Care givers
• Support groups
• Social workers
2. DIAGNOSIS
ICD10 Classification
F00 Dementia in Alzheimer's disease F00.0 Dementia in Alzheimer's disease with early onset

63
F00.1 Dementia in Alzheimer's disease with late onset
F00.2 Dementia in Alzheimer's disease, atypical or mixed type
F00.9 Dementia in Alzheimer's disease, unspecified
F01 Vascular dementia F01.0 Vascular dementia of acute onset
F01.1 Multi-infarct dementia
F01.2 Subcortical vascular dementia
F01.3 Mixed cortical and subcortical vascular dementia
F01.8 Other vascular dementia
F01.9 Vascular dementia, unspecified
F02 Dementia in other diseases classified elsewhere F02.0 Dementia in Pick's disease
F02.1 Dementia in Creutzfeldt-Jakob disease
F02.2 Dementia in Huntington's disease
F02.3 Dementia in Parkinson's disease
F02.4 Dementia in human immunodeficiency virus [HIV] disease
F02.8 Dementia in other specified diseases classified elsewhere
F03 Unspecified Dementia
DSM-IV Classification
290.0 Dementia of the Alzheimer’s Type, With Late Onset, Uncomplicated
290.10 Dementia due to Pick's Disease
290.10 Dementia due to Creutzfeld-Jacob disease
290.10 Dementia of the Alzheimer’s Type, With Early Onset, Uncomplicated
290.11 Dementia of the Alzheimer’s Type, With Early Onset, With Delirium
290.12 Dementia of the Alzheimer’s Type, With Early Onset, With Delusions
290.13 Dementia of the Alzheimer’s Type, With Early Onset, With Depressed Mood
290.20 Dementia of the Alzheimer’s Type, With Late Onset, With Delusions
64
290.21 Dementia of the Alzheimer’s Type, With Late Onset, With Depressed Mood
290.3 Dementia of the Alzheimer’s Type, With Late Onset, With Delirium
290.40 Vascular Dementia, Uncomplicated
290.41 Vascular Dementia, With Delirium
290.42 Vascular Dementia, With Delusions
290.43 Vascular Dementia, With Depressed Mood
3. THE IMPACT OF DEMENTIA ON OCCUPATION
Occupation refers to what a person "does". Kielhofner2 explains the "occupational
functioning of persons" as "how persons choose, order, and perform in everyday
occupational behaviour. Kielhofner focuses on both the individual's characteristics and the
environment as factors that influence choices and behaviour". Occupation, therefore, refers
to a person's work, activities of daily living, and social and leisure activities, within the
context of their environment.
The findings of the review of 23 studies indicated that occupation has an important influence
on health and well-being. Withdrawals or changes in occupation for a person have a
significant impact on a person’s self perceived and well-being. These performance
components that are experienced by clients with dementia will affect their occupation and or
performance areas as follows:4
3.1. Work
Due to the impairment of cognitive function, the person with dementia will have a decline in
their work abilities. The individual can work relatively well in familiar surroundings at routine
tasks but new tasks are difficult to execute. Colleagues will often be aware of the
deterioration. Studies show that persons with dementia who continued working in a repetitive
work environment showed less decline in daily living activities. Compared to traditional day
care activities, work activities involve sequencing skills and practice may translate to self-
care activities at home.4

65
3.2 Activities of daily living
The person with dementia shows a systematic decline in the ability to perform everyday
tasks such as self care tasks that include bathing and dressing, domestic activities such as
cooking, housework, or shopping, and community survival skills such as driving or using
public transport.5 6 8
3.3 Leisure activities
While the person may have the energy and desire to do things, they may lack the ability to
organise, plan, initiate and successfully complete even simple tasks. Sometimes it’s
impossible to get started. At other times they get into a muddle and are seen as negative and
uncooperative. They therefore have no way to express their talents and abilities5 6 8
3.4 Socialisation
Social problems occur due to decreased confidence, fear of failure, social isolation and low
self-esteem. Care givers may become less sympathetic and more intolerant. Such problems
by their very nature limit the individual’s level of independence.5 6
4. IMPACT OF DEMENTIA ON ROLES, HABITS AND ROUTINES With the deficits that occur with dementia, caregivers usually tend to concentrate on the
basic physiological needs of the individual. The roles, previous habits and routines are often
not considered and are lost. The occupational therapist may assist the patient with
identification of new roles, which will be satisfying to the individual. When established habits
and routines are not taken into consideration, the level of independence is likely to reduce at
a faster rate. There is a role reversal and the individual changes from being the caregiver to
becoming the dependant.5 6 8
66
5. HEALTH CARE STRUCTURES 5.1. Pillars of health care
5.1.1. Preventative/Promotive
Promotive care, in the case of Dementia, takes more of a consultative role, where the
occupational therapist can assist the caregiver in structuring the environment. In the case
of high-risk individuals, a healthy lifestyle, while not preventing dementia, appears to
delay the onset of dementia.
5.1.2. Rehabilitation
This is the process of giving the client the resources, including specialized treatment and
training, to promote improvements in activities of daily living, thereby encouraging
maximum independence and quality of life.
OT strategies in this regard, will focus on expanding the support network.
5.1.3. Maintenance
At a maintenance level, clients and their caregivers are given the necessary coping skills
to function as optimally as possible, within the limitations of the dementia, and to maintain
their quality of life.1 5 8
5.2. Levels of health care
5.2.1. Primary care1
The treatment of dementia is predominantly on a primary level as clients are usually seen
in the community.
67
Improvement in activities of daily living and sense of competence are associated with a
decrease in need for assistance and this could in the long term result in less need for
institutionalization.9
Mittleman reports a long term study showing that spouses of Alzheimer’s patients are less
likely to place their loved ones in a nursing home if the spouses receive enhanced
counselling and caregiver support.9
Training families to use adaptive techniques using familiar objects such as clocks and
calendars can help people in the early stages of dementia.
5.2.2. Secondary level
Initial contact is made with the patient and the caregiver and assessment is performed at
the secondary level. Based on the assessment, a care strategy is developed, with input
from the client as well as the caregiver. The client is introduced to therapeutic activities,
as an introduction to activity participation.
5.2.3. Tertiary level
Initial contact is made with the patient and the caregiver and assessment is performed at
the tertiary level. Based on the assessment, a care strategy is developed, with input from
the client as well as the caregiver.
The client is introduced to therapeutic activities, as an introduction to activity participation.
6. ASSESSMENT 6.1. Baseline assessment1
Each person has to be compared against their own previous abilities and behaviour hence
the importance of gathering information from people who have known the person prior to the
onset of deterioration and carrying out in depth baseline assessments to compare
functioning over time. 1

68
Since available assessment tools to diagnose dementia assume a previous intact level of
cognitive functioning, this poses difficulties in diagnosing people who have a learning
disability and cannot be compared against the general population.5
Research recommends that baseline assessments are carried out in all people who have
Down’s syndrome from the age of 35 years with reassessments every 5 years unless
changes in behaviour, skills or routines are noticed, when reassessment will be on an
ongoing basis.5
6.1.1. Professional Interview
An interview is conducted with the caregiver and the client. During the interview detailed
background information is gathered.
6.1.2. Clinical Observation
This is an ongoing process. During the interview the therapist will observe the client’s
non-verbal signs such as tone of voice, gestures, facial expression and personal
appearance.
The therapist will also observe the client’s performance and behaviour during
standardized and non-standardized tests and compare that with the assessment results.
The client will also be observed during participation in various activities and discussion
groups as part of on-going assessment.5 8
6.1.3. Evaluation
The following aspects should be covered during evaluation:5 8
• Core Identity
• Psychological Background
• Interests
• Cognition (level of consciousness, concept formation, memory, attention span and
concentration, judgement, planning and organisation, abstract thought, problem solving
and intellect)

69
• Emotional state (affect and mood)
• Visual perceptual skills (spatial relationship, etc)
• Senses/sensation (sensory deprivation/ sensory capacity)
• Motor skills (mobility/ambulation, motor coordination, visual motor coordination
• Social skills (lack of recollection of familiar individuals, level of interest in other people,
difficulty finding words during communication etc)
• Performance areas (activity of daily living, work, leisure, socialisation)
The following are examples of standardized tests that can be used1:
• Brief Cognitive Rating Scale (BCRS)
• Assessment of Motor and Process Skills (AMPS)
• Interview of Deterioration in Daily Activities in Dementia (IDDD)
• Canadian Occupational Performance Measurement (COPM)
• Dementia Quality of Life Instrument (DQOL)
• Sense of Competence Scale (SCQ)
• Mastery Scale.
• Interest checklist
• COTNAB
• Rivermead Behavioural Memory Test
• Role change assessment
• Cognitive Assessment of Minnesota (CAM)
Care should be taken that a client is not set up for failure.
6.1.4. Environmental Assessment 5 8
The once familiar and secure environment of home and/or day occupation can become
over stimulating and a confusing place for the person with dementia. The task of looking
at the environment from the person’s perspective and how aspects within it can be
threatening, confusing and difficult to predict is one which is crucial in assisting the
person to maintain daily routines and self esteem9.

70
6.1.5. Collateral Information5 8
Collateral information is obtained to confirm observations made and information gathered
during the assessment. Collateral information is essential from caregivers, healthcare
professionals, domestic staff, friends and other family members.
6.1.6 Assessment Report
Assessment reports are issued only to registered healthcare professionals unless
otherwise requested by permission of the caregiver. (Ethical Rules HPCSA 2006). 8
6.2. Ongoing assessment5 8
Assessment should be ongoing and formal assessment should be performed annually to
monitor progress. In cases where marked deterioration is clinically observed, assessment
should be repeated.
7. INTERVENTION 7.1 Role of Occupational therapy in the treatment of dementia9
Intervention by the occupational therapist is most effective as part of multi-disciplinary team
approach especially at secondary and tertiary level.
Key aim - To promote and maintain independence at home and in the community3
The use of environmental modifications is critical to task success and to satisfaction with
performance. Modification can be made in the client’s approach to the task, in the therapist’s
or caregiver’s approach, and in how the occupation, task, or exercise is set up or performed.
The following table lists specific modifications that may be made to the context in order to
promote occupational performance.9

71
Modifications by Therapist / Caregiver
Modifications in the Occupation, Task, & Exercise itself
Modifications by the Client
• Change verbal and body
language, concreteness of
instructions, physical cues
or reassurance
• Change tone of voice
• Change type of feedback
(verbal, written, pictures,
photos, physical)
• Change when and how
often feedback is given
• Change how feedback is
explained
• Change own expectations
biases (alter own value
judgments about ideal /
necessary performance)
• Change sensory modalities
challenged during a task
(i.e. decrease tactile,
auditory, or visual
distractions)
• Change amount of work
load (i.e. set up task to limit
number of steps, lay out
needed objects, label
cabinets and drawers)
• Change complexity of task
(i.e. simplify the number of
objects, the number of
steps, the number of
instructions, the form of
instructions, the type of
instructions or feedback)
• Change pace/speed of
task
• Change duration of task
• Change awareness levels
(arouse prior to task
performance)
• Change safety challenges
• Change need for error
detection & correction
• Change the social
environment
• Change postural readiness
prior to task performance
• Change organizational
strategies prior to task
performance
• Change medication or its
timing
Adapted from: Abreu, B. C. (1990). The quadraphonic approach: Evaluation and treatment of
the brain injured patient. New York: Therapeutic Service Systems.
Modification to the environment 8 9
Environments should be
• Predictable
• Calm
• Make sense
• Structured
• Suitably stimulating
• Familiar

72
In addition to looking at the aspects of the environment which would assist any person with
physical and/or sensory impairment – access, layout, aids to independence there are
specific aspects to consider for someone who is experiencing cognitive decline.
Consider should be given to the lighting, reflections and images which can be misinterpreted
or be a cause of fear and uncertainty.
• Mirrors and pictures should have non glare glass to avoid reflections being
misinterpreted
• It is suggested that turning the lights on 2 hours before dusk will lessen the agitation
and confusion which happens in the latter part of the day (Sundowning)
People with Dementia find it difficult to differentiate between colours, colours at the top end
of the spectrum such as red orange and yellow should be used to emphasize triggers
• Doors can be painted to aid with recognition e.g. bedroom, toilet etc.
• Conversely walls and doors can be painted the same colour to camouflage exit
routes.
Consideration should be given to the décor of rooms
• Patterned wallpapers can over stimulate and cause anxiety
• Matching carpets, suite and curtains can blend into one another which can cause
problems for people in finding somewhere to sit
• Carpets should ideally be self coloured and run throughout the house to avoid
problems in entering different rooms – perceived as a drop or a step (depth
perception). Conversely different coloured carpets in each room can aid with
recognition of that room
• Floors should have a dull non shiny finish. A shiny floor can be perceived as a pool of
water.
Pictorial information to aid with understanding should be used
• Pictures ,symbols or objects which have meaning for the person

73
Dementia friendly design
• Accommodate wandering by securing garden area, camouflaging gates and making a
path with areas for rest and which brings the person back round to the building
• Within the home, doors should be removed from the living area to allow the person to
hear and see others which can help if the person develops paranoia, they will know
where the sounds are coming from.
• Cupboard doors should be removed from the cupboards you want the person to
access
• Consider door handles, locks and opening mechanisms. A simple change can prevent
easy access.
Occupational therapists use a variety of approaches during intervention with clients who
have dementia. The goals of therapy include maintaining, restoring, and improving
occupational performance; promoting health and quality of life; and easing caregivers’
burden 4
7.1.1. Self care tasks and community survival skills
Self care is occupation that enables the individual to survive and that promotes and
maintains health.9
The occupational therapist aims to form a partnership with the individual to help identify
important areas of everyday life that may have been affected by the condition. For
example these areas may include everyday pursuits such as leisure activities, driving or
using public transport, domestic activities such as shopping, cooking, or housework, self-
care tasks such as bathing and personal matters such as intimate relations.6
The occupational therapist works with that individual to look at possible solutions that
may help maintain or improve independence in those areas. For example the OT will
provide discrete practical help in tackling memory problems, and help the individual to
engage successfully in the activities that they wish to pursue.6
Personal history should be used to develop these activities

74
7.1.2. Leisure and or Recreational activities
It’s important that the individual suffering from dementia should engage in a wide range of
leisure activities including sports, arts and crafts, attending concerts and participating in
activities that will bring meaning and fun into their life.
7.1.3. Socialisation
The occupational therapist actively assists the individual to cope with the social and
psychological problems, which may accompany the condition, such as decreased
confidence, fear of failure, social isolation, and low self-esteem. Such problems by their
very nature limit the individual’s level of independence. The OT will help the individual to
learn coping skills by using activities and treatment techniques in a carefully measured
and graded way.
Studies show the benefits of remaining active in later life. Furthermore, an exclusive
emphasis on exercise and fitness activity may be overly narrow. While it is recognized
that all social activity has the potential to include physical activity, as has been argued by
Yates,11 the physical actions in which humans engage are inherently social in nature as
well. Social and productive activities are seen as complements to exercise. On their own,
social and productive activities have independent health benefits.
A study by Glass reports on the impact of activity on risk of all cause mortality among
elderly people. More active elderly people were less likely to die than those who were less
active. Social and productive activities were observed to confer equivalent survival
advantages compared with fitness activities. This observation is important because it
suggests that activities that entail little or no physical exertion may also be beneficial. A
wider range of mechanisms, both physiological and psychosocial, may be involved in the
association between activity and mortality than had been previously thought11.
Structured Occupational Therapy groups, taking the individuals strengths and
weaknesses into consideration, allow for positive social interaction.
75
Maintaining identity5
The client’s likes, dislikes, personal habits and interests, strengths and weaknesses need
to be part of the profile of the individual. While this forms part of the assessment process,
it is necessary to constantly incorporate these aspects into activities to ensure that the
core identity is maintained for as long as possible. These include:
• How does client prefer to be addressed? Nickname?
• Sleeping patterns
• Bath time routine
• Eating patterns
• Method of dressing
• Bladder and bowl habits
• Hobbies and interests
• Profession
• Family details
• Personal history
• Religious beliefs
• Pre-morbid personality
Promotion of awareness and orientation5 8
Promote orientation and maximize awareness through environmental modification.
Sensory stimulation5 8
Optimal level of sensory stimulation should be provided avoiding under- and overload.
Rote learning5 8
Activities based on rote learning such as old songs, poems, dances etc. contribute
towards a sense of achievement and well-being

76
Reality Orientation5 8
The emphasis is on reality assurance and should not be for repetition or recall. Feelings
should be addressed rather than focussing on accuracy - especially when the individual is
paranoid.
Awareness of e.g. Seasons, Xmas, Easter.
Reminiscence therapy5 8
Reminiscence therapy focuses on long-term memory and past experiences.
Life story work5 8
This involves compiling a record of the person’s life through pulling together photographs,
objects, and mementos which hold meaning for the person and are significant to them in
remembering their past. The process of working closely with an individual to remember
their past and share it with significant others should be as therapeutic as the use of the
product.
Cognitive5 8
Ongoing cognitive stimulation includes participation in games and making use of familiar
phrases.
Exercise A study by Larson found a potentially important effect modification between exercise and
physical functioning in relation to incident dementia as well as Alzheimer disease. There
was a greater risk reduction of dementia by exercise among persons with lower levels of
physical functioning compared with those with higher levels of physical functioning. Low
levels of physical functioning were associated with an increased risk for dementia among
persons who exercised fewer than 3 times per week; however, this increased risk
diminished among persons who exercised 3 or more times per week. The finding
77
suggests that one of the ways that exercise might reduce the risk for dementia is through
modulating the relationship between physical functioning and dementia. It is suggested
that exercise does not prevent dementia but might be associated with a delay in onset 12
Support to care-giver reduces negative effects on care-giver.
The negative effects on the primary care-giver are reduced by improving daily
performance, communication, sense of competence and quality of life of a person with
dementia and his or her primary caregiver. A combination of education, setting feasible
goals, using adaptations in physical environment, training compensatory skills, training
supervision skills, and changing dysfunctional cognitions on patient behaviour and
caregiver role are considered to be beneficial.1
7.2. Theoretical framework
7.2.1 Models
Creative Ability Model (Vona du Toit)13
This is a South African approach that was elaborated in 1962 by Vona du Toit. This
approach is used to evaluate the client’s occupational performance according to the skills
he has attained in the personal, social, work and recreational occupational performance
area 3.
It also provides guidelines for treatment by:
• Identifying treatment priorities
• Proposing principles that guide treatment so that it is appropriate to the client’s
level
• Determine expectations for performance, as well as how and when to up or
downgrade the treatment.

78
This approach also helps the occupational therapist to categorise patients efficiently in
terms of their occupational performance needs and it enables the correct treatment to be
administered at the right time and in the most cost effective manner.3.
This approach does not represent the whole of occupational therapy for the client. It has
an assessment aspect, which determines the level on which the client functions and then
provides a stratified guide to increase the client’s level of performance.
This approach accommodates clients suffering from dementia, and it assists with proper
grouping and approach during the intervention. This theory postulates that creative ability
consist of two components:
• The inner drive towards action
• The externalisation of this motivation in action, which is seen through the
creation of concrete or abstract end-products in daily life.
More research is being done by South African occupational therapists to standardize this
approach, and to evaluate its reliability and validity.16
The occupational therapist can make use of a variety of models during the treatment of a
client with Dementia.
Model of Human Occupation (Kielhofner)2
• The model addresses a person’s occupational behaviour and occupational
dysfunction.
• Occupation is essential to human self-organization. Through occupations,
persons exercise their capacities and generate on-going experiences that
affirm and shape their psyches. Therefore the order or organization of humans
depends on occupational behaviour.
• Occupational therapy engages persons in occupational behaviour that helps
maintain, restore, reorganize, or develop their capacities, motives and
lifestyles.

79
• Specific subsystems contribute to occupational behaviour and needs to be
addressed i.e. volition, habituation and mind-brain-body performance.
7.2.2. Frames of Reference/Approaches for the treatment of Dementia
The occupational therapist uses a variety of frames of reference and approaches during
therapy. These may be used in combination for a single client to direct therapy.
Some of the approaches are summarized below as follows:
Humanistic approach/Client centered approach1 16
Occupational therapists make use of a client centered approach whereby the client and
the caregiver are involved in the decision making process regarding the direction of their
therapy. The client is given the opportunity to have the capacity for self awareness and to
make their own choices. Their interests, roles, needs and habits are taken into
consideration during therapy.
The therapeutic relationship is of great importance in order to facilitate the above,
therefore the therapist should be empathetic, congruent, warm, genuine and show
unconditional positive regard for the client.20
Physiological approach 1 16
The individuals is a biological ergonomist whose behaviour depends on genetically
determined factors, combined with selective action of nervous and endocrine systems
and the ability of the body to maintain homeostasis. Performance depends on the
integrity and the interactions of all body systems (e.g. cardiovascular, musculoskeletal
etc). Examples of activities that use the physiological approach are aerobics, ball games
etc.
80
Psychosocial Interactive approach13
This approach is used largely during occupational group therapy where focus is on the
here and now, and on the interaction between the group members and the insight the
client gains from this.10
Behavioural approach
Therapy aims at changing dysfunctional behaviour, and learning and reinforcing
appropriate behaviour.
Sensory integrative approach Sensory integration is the organisation of sensation for use. Sensory integrative approach
to the treatment of dementia may include controlled sensory stimulation as reduced
senses and reduced exposure to the environment may lead to sensory deprivation.5 8
Cognitive approach
This theory tries to understand the thought process such as memory, conceptualisation,
and perceptions, and also to provide theories about how the person forms relationships
between concepts, how he interprets structure and how he makes sense of the
surrounding environment. Therefore, the emphasis lies on each person’s perception and
interpretation.5 8
Logical reasoning (also seen in problem solving) and concept formation forms part of this
approach.
The learning process is an example of the cognitive approach.

81
7.3. Time Span
As Dementia is a progressive condition, assessment and intervention would be ongoing.
Primary level - Community/Outpatient basis 1
10 x 1hr sessions
• 4 x sessions of comprehensive assessment
• 6 x individual sessions
• Weekly Occupational group therapy sessions lasting 90min.
Secondary level
6 x 1hr sessions
• 4 x sessions of comprehensive assessment
• 2 x individual sessions
10 x Occupational group therapy sessions lasting 90min
Tertiary level
6 x 1hr sessions
• 4 x sessions of comprehensive assessment
• 2 x individual sessions
Daily Occupational group therapy sessions lasting 90min
8. TABLE OF EVIDENCE
Author Study population
Type of design
Treatment group Outcome variable
Findings
Graff, Vernooij-
Dassen, Thijssen,
Dekker,
135 patients
aged ≥65 with
mild to
moderate
dementia living
Single blind
randomised
controlled
trail.
Assessors
10 sessions of
OT over 5 weeks.
Cognitive and
behavioural
interventions,
Patients' daily
functioning
assessed with the
assessment of
motor and
Scores improved
significantly relative
to baseline in
patients and care
givers in the

82
Author Study population
Type of design
Treatment group Outcome variable
Findings
Hoefnagels
& Olde
Rikkert1
in the
community and
their primary
care givers.
blinded for
treatment
allocation
training patients
in use of aids to
compensate for
cognitive decline
and care givers in
coping
behaviours and
supervision.
process skills
(AMPS) and the
performance
scale of the
interview of
deterioration in
daily activities in
dementia (IDDD).
Care giver burden
assessed with the
sense of
competence
questionnaire
(SCQ).
Participants were
evaluated at
baseline, six
weeks, and three
months.
intervention group
compared with the
controls (differences
were 1.5 (95%
confidence interval
1.3 to 1.7) for the
process scale; –11.7
(–13.6 to –9.7) for the
performance scale;
and (11.0; 9.2 to
12.8) for the
competence scale).
This improvement
was still significant at
three months. The
number needed to
treat to reach a
clinically relevant
improvement in
motor and process
skills score was 1.3
(1.2 to 1.4) at six
weeks. Effect sizes
were 2.5, 2.3, and
1.2, respectively, at
six weeks and 2.7,
2.4, and 0.8,
respectively, at 12
weeks.
Conclusions
Occupational therapy
improved patients'
daily functioning and
reduced the burden
on the care giver,
despite the patients'

83
Author Study population
Type of design
Treatment group Outcome variable
Findings
limited learning
ability. Effects were
still present at 12
weeks, which justifies
implementation of this
intervention.
Clark, Azen,
Carlson,
Mandel,
LaBree,
Hay,
Zemke,
Jackson &
Lipson. 12
Independent-
living older
adults
Randomized
trial
9-month program
in preventive
occupational
therapy (OT).
Health, function,
and quality of life
benefits
Significant health,
function, and quality
of life benefits.
Followed for an
additional 6 months
without further
intervention and re-
evaluated.
Approximately 90%
of the therapeutic
gain observed
following OT
treatment was
retained in follow-up.
Bums ,
McCarten ,
Adler,
Bauer &
Kuskowski.4
Functioning
examined when
9 veterans
were moved
from a work
program to a
traditional adult
day care
program.
Subjects were
reassessed four
months after the
move with the
Mini-Mental State
Examination
(MMSE),
Cognitive
Performance Test
(CPT), and
Geriatric
Depression Scale
(GDS). Individual
slopes were
Observed scores at
reassessment were
significantly lower
than expected
scores. The MMSE
was on average 4.9
points lower, and the
CPT. 64 points lower
than expected. The
GDS did not change.
The spouses of all
nine patients reported
declines in daily living
activities.

84
Author Study population
Type of design
Treatment group Outcome variable
Findings
calculated for
seven subjects
who had
longitudinal
scores, and
expected scores
were predicted
based on the rate
of decline.
Observed scores
at reassessment
were significantly
lower than
expected scores.
Baldelli ,
Fabbo,
Costopulos,
Carbone,
Gatti &
Zucchl .14
Health care
staff of a
nursing home
Occupational
therapy and
cognitive
rehabilitation for
demented
patients
The Maslach
burnout inventory
(MBI)
1 Year Follow-
up.These treatments
seem to have
positive effects on
both the patients,
improving their
performances, and
the nursing staff, as
an aid to reduce the
job burnout.
Clark,
Azen ,
Zemke,
Jackson
Carlson,
Mandel,
Hay,
Josephson,
Cherry,
Hessel,
Palmer &
Lipson12.
Two
government
subsidized
apartment
complexes for
independent-
living older
adults. A total
of 361 culturally
diverse
volunteers
aged 60 years
Randomized
controlled trial
An OT group, a
social activity
control group,
and a non
treatment control
group. The period
of treatment was
9 months.
A battery of self-
administered
questionnaires
designed to
measure physical
and social
function, self-
rated health, life
satisfaction, and
depressive
symptoms
Significant benefits
for the OT preventive
treatment group were
found across various
health, function, and
quality-of-life
domains. Because
the control groups
tended to decline
over the study
interval, results
suggest that

85
Author Study population
Type of design
Treatment group Outcome variable
Findings
or older. preventive health
programs based on
OT may mitigate
against the health
risks of older
adulthood.
Dooley &
Hinojosa17 Two groups of
persons with
Alzheimer's
disease in their
own homes
Pretest-
posttest
control group
design
Caregiver burden
and three
components of
quality of life,
positive affect,
activity frequency
and self-care
status
Individualized
occupational therapy
intervention based on
the person-
environment fit model
appears effective for
both caregivers and
clients
Larson ,
Wang,
Bowename
s ,
McCormick
, Teri,
Crane &
Kukull11
Population-
based,
longitudinal
study
A reduced incidence
rate of dementia for
persons who
exercised 3 or more
times a week
compared with those
who exercised fewer
than 3 times per
week Exercise
seemed to be
associated with the
greatest risk
reduction in
participants who had
poor physical
functioning at
baseline.
86
9. CONCLUSION
Ten sessions of community occupational therapy over five weeks improved the daily
functioning of patients with dementia, despite their limited learning abilities, and reduced the
burden on their informal care givers.1
The effect sizes of all primary outcomes were higher than those found in trials of drugs or
other psychosocial interventions, and these effects were still present at three months1.
The advantage of occupational therapy is that it is client-centered practice since the client,
caregiver and the occupational therapist work together, as mutual partners in order to find
the best solution for the client.
It would be inappropriate for the client to be treated without the involvement of the
occupational therapist, due to their unique contribution to their well-being and health.

87
10. REFERENCES
1. Graff M, Vernooij-Dassen JM, Thijssen M, Dekker J, Hoefnagels WH, Olde Rikkert
MGM. Community based occupational therapy for patients with dementia and their
care givers: randomised controlled trial. Br Med J. 2006;333:1196
2. Kielhofner G. Conceptual Formations of Occupational Therapy 3rd ed Philadelphia;
F.A. Davis:2004.
3. Larson KB. Activity patterns and life changes in people with depression. American
Journal of Occupational Therapy. OCT 1990, Vol 44 number 10
4. Bums T, J. R McCarten, Adler G, Bauer M, Kuskowski M A. Effects of repetitive work
on maintaining function in Alzheimer's disease patients. Am J Alzheimers Dis Other
Demen.2004;19(1):39-44
5. Zgola JM. Doing Things: A Guide to Programming Activities for Persons With
Alzheimer's Disease and Related Disorders. Johns Hopkins Univ Pr; 1987.
6. Salmon N. Occupational Therapy in Dementia. Mental Health in later Life. Available
from:http://www.mhilli.org/index.html
7. Trombly CA. Historical and Social Foundation for practice. Occupational Therapy for
physical dysfunction, 4th ed. 196-197
8. Cruz ED. Tips for occupational Therapists working with clients Who Have Dementia.
Dementia Education. Available from: http://etgec.utmb.edu/dementia/index.html
9. American Occupational Therapy Association (1994). Statement: Occupational therapy
services for persons with Alzheimer’s disease and other dementias. Am J Occup
Ther.1994; 48, 1029-1031.

88
10. Glass TA, de Leon CM, Marottoli RA, Berkman L F . Population based study of social
and productive activities as predictors of survival among elderly Americans. Br Med
J.1999;319:478-483
11. Larson EB, Wang Li J. Bowenames D, McCormick WC., Teri L, Crane P, Kukull W.
Exercise Is Associated with Reduced Risk for Incident Dementia among Persons 65
Years of Age and Older 17. Ann Intern Med. 2006 Jan; 144(2):73-81
12. Clark F , Azen SP, Carlson M, Mandel D, LaBree L, Hay J, et al. Embedding Health-
Promoting Changes Into the Daily Lives of Independent-Living Older Adults. Long-
Term Follow-Up of Occupational Therapy Intervention. J Gerontol B Psychol Sci Soc
Sci.2001;56:60-63.
13. Crouch RB and Alers VM, editors. Occupational Therapy in Psychiatry and Mental
Health, 4th ed. South Africa: Maskew Millar Longman; 1997..
14. Baldelli MV, Fabbo A, Costopulos C, Carbone G, Gatti R, Zucchl P. Is it possible to
reduce job burnout of the health care staff working with demented patients? Arch
Gerontol Geriatr Suppl. 2004;(9):51-6
15. Graff M, Vernooij-Dassen JM, Thijssen M, Dekker J, Hoefnagels WH, Olde Rikkert
MGM. How can occupational therapy improve the daily performance and
communication of an older patient with dementia and his primary caregiver. Dementia.
2006;5(4);503-532.
16. Fouche L. Occupational Therapy in the community. Masters in psychiatry assignment.
Unpublished material. University of Pretoria.
17. Dooley NR, Hinojosa J. Improving quality of life for person’s with Alzheimer’s disease
and their family caregivers: brief occupational therapy intervention. Am J Occup
Ther.2004 Sep-Oct; 58(5), 561-9.
89
EATING DISORDERS Compiled by:
Anel Grobler, B.A. Occupational Therapy (Pretoria)
Zonia Weideman, B.A. Occupational Therapy (Pretoria) Post-graduate Diploma in Vocational Rehabilitation
(Pretoria)
1. INTRODUCTION
Eating disorders are a crippling and disabling condition and if it becomes chronic, the
emotional, physical and social effects are substantial1. It is a multi factorial condition that
poses many challenges to professional care givers. The efforts should be multidisciplinary
and an occupational therapist should be included in the team2.
The prognosis of this group of disorders is a great concern. Some patients with anorexia
recover completely but the majority remains under weight, with 10% meeting the diagnostic
criteria 10 years after treatment. Bulimia often persists for at least several years and could
be chronic or intermittent3.
Apart from the emotional and psychiatric problems and often disability, Anorexia is an illness
with multiple physical complications. Apart from the physical and emotional components 12 –
20% of patients with the illness die4. Although bulimia nervosa has a smaller amount of life
threatening cases (1%), the incidence of the illness is higher than anorexia4.
Henderson (1999) states that "occupational therapists' unique contribution towards the
treatment of individuals with eating disorders, is their combined knowledge of physical,
interpersonal and psychological functioning"5.
2. DIAGNOSIS
Eating disorders are seen as a group of disorders characterized by abnormal eating
behaviours and beliefs about eating, weight, and shape. The ICD 10 classification includes
the following:
1 Barnett et al, 2006 2 Garfinkel and Garner, 1982 3 Sue, 2003 4 Murphy RMN, Manning RMN. An Introduction to anorexia nervosa and bulimia nervosa. Nursing standard. 2003 Dec 17: Vol 18: 45-52. 5 Henderson

90
F50.0 Anorexia nervosa
F50.1 Atypical anorexia nervosa
F50.2 Bulimia nervosa
F50.3 Atypical bulimia nervosa
F50.4 Overeating associated with other psychological disturbances
3. IMPACT ON PERFORMANCE
3.1 Work / School Although these patients are often highly skilled and often perfectionists with obsessional
patterns of thinking and behaving4, their functioning at work / school are often affected by
rituals and manipulative behaviours. Commonly there will be significant depression and
isolation and performance in education or employment fall below the person with eating
disorders capabilities. Their belief of ineffectiveness also often hinders them to function
optimally.
3.2 Activities Of Daily Living The most problematic activity of a person with an eating disorder is eating and cooking. This
is the core pathology of this diagnostic group. As they struggle with issues of control – their
eating habits is an extreme measure to try and control their bodies6. This does not only
interrupt a balanced lifestyle and impair functioning in other areas, but can have adverse
physical affects.
3.3 Leisure These patients often do not have healthy leisure or social interests or the ability to pursue
them and would rather for example over exercise to loose weight. A great amount of their
free time will be spent on their preoccupation and rituals in relation to eating and cooking.
6 DeLaune

91
Although exercise is conducive to a healthier body and mind, it must be carefully monitored
in individuals with eating disorders as they tend to over exercise as they believe that a loss
of weight and change in body shape will lead to an improved life4.
3.4 Social A person with eating disorders struggles to form and maintain healthy relationship and hardly
engage in any form of social leisure. DeLaune describes this client group as manipulative,
and clients that avoid intimacy by maintaining a superficial relationship. She explains that
manipulation of the anorexic, bulimic and overeater reaches extreme proportions and
maladaptive behaviour6. Murphy and Manning explains that a person with bulimia is
“generally more impulsive in nature, a thrill- or excitement-seeker with extreme feelings, who
has a low tolerance of boredom and difficult interpersonal relationships”4
4. IMPACT ON ROLES, HABITS AND ROUTINES
A person with a eating disorder “strive for perfection and become increasingly obsessional,
sticking to routines and devising ever more complex sets of `rules` by which to live their
lives. They may lie and be very secretive to protect themselves and may withdraw from
situation, particularly those which involve food, both at home an in a wider social context.
These individuals may become hostile and angry if their routines are upset or interfered with,
obviously unhappy and in difficulty, they may refuse all offers of help and maintain that they
are `fine`, even in advanced stages of malnutrition and emaciation”7.
Thus individuals with eating disorders roles, habits and routines are severely affected by
their obsessional and manipulative ways. Such patients benefit from occupational Therapy
which does not focus on recovery but rather improving their quality of life.
7 Halek BA. Anorexia nervosa. Nursing Standard. 1997 Dec 10; pp 41-47.

92
5. HEALTH CARE STRUCTURES
5.1 Pillars Of Health Care Prevention can be attempted by strengthening a person’s natural defence against what are
assumed to be primary environmental causing agents such as unrealistic media
representation of body shapes or socially sanctioned inappropriate eating related
behaviours. Another form of prevention is to look for manifestations of disorders and
intervening as soon as possible (early intervention approach)8.
Remedial treatment comes into play if an individual with eating disorders resorts to using
food and eating behaviours as maladaptive coping mechanisms, therefore it is important to
learn them alternative methods for solving problems. Treatment is most likely to be
successful in collaboration with the patient and ranges from individual, group, family therapy
and psycho educational treatment.
5.2 Level Of Health Care System
Specialist treatment can result in a better outcome for patients than non-specialist treatment 9 (Tertiary health care), but access to specialist units remains problematic and most patients
are cared for in primary and secondary care settings6.
6. ASSESSMENT
6.1 Baseline Assessments
According to Bridges10 the seven areas of the assessment are: the patient's general status,
physical status, self-image, estimation of body size, time management, interests and
activities, and balance between internal/external controls.
8 Ben-Tovim DI. Eating disorders: outcome, prevention and treatment of eating disorders. Lippincott Williams & Wilkins, Inc. 2003 Jan; Vol 16(1): pp 65-69. 9 Crisp AH, Norton K, Gowers S et al. A controlled study of the effect of therapies aimed at adolescent and family psychopathology in anorexia nervosa. British Journal of Psychiatry. 1991. Vol 159; 325-329. 10 Bridges 1993

93
The occupational therapist plans treatment approaches for and with individual patients;
these are based on the findings of the assessment.
The baseline assessment is used to monitor progress and needs to be done
comprehensively. When progress is measured from a well documented baseline, it can be
used to motivate the client through realistic praise for her/his accomplishments.
6.1.1 During the Professional interview the following could be assessed11:
o Motivation to change
o Degree of insight
o Attention and concentration span
o Personal interests and talents
o Feelings about the family
o Work / school situations
o Social and family live
The difficulties of this diagnostic group are complex and special attention should be given
to adolescents that seem very high functioning because of perfectionist traits, especially
during clinical observation.
International Classification of Functioning gives the following definition of terms:
o Activity – is the execution of a task or action by an individual
o Participation – is involvement in a life situation
o Activity Limitations – are difficulties an individual may have executing activities12
o Participation Restrictions – are problems an individual may experience in
involvement in real life situations
In most conditions activity limitations results in participation restrictions which result in
disability. However in eating disorders it is not necessarily the difficulty with task execution
but involvement in a life situation that causes impairment and possible disability.
11 Stockwell R. Duncan S. Levens M. In Scott & Katz (Eds.) Occupational Therapy in Mental Health: Principles in practice. 1988. London: Taylor and Francis, Ltd. 12 ICF Int classification

94
6.1.2 Collateral information
Collateral information should be a large part of the assessment, as these patients often
struggle under relationship strain. Collateral is also needed for a complete picture of the
patient, as (as described above) their functioning are often not impaired by a problem with
performance components but a lack of personal effectiveness.
6.2 Ongoing Assessment Assessment is an ongoing process, which needs to continue throughout treatment to monitor
progress as well as to help identify specific needs of the patient.
7. INTERVENTION 7.1 Role of Occupational therapist
7.1 .1 Work
Various programs exist which occupational therapist facilitate that helps the person with
an eating disorder to begin or continue with their work, these include:
o Supported Employment
Supported Employment is defined as placing an individual with an eating disorder in a
full or part-time job and an employment consultant then supports the individual in
order to help the worker to succeed and retain the position indefinitely13.
According to Becker, Drake and Naughton there are six principles of supported
employment that improve employment outcomes; these are14;
i.Eligibility is based on the clients choice
ii. Supported employment is integrated with mental health treatment 13 Mechanic D. Cultural and Organizational Aspects of Application of the Americans with Disabilities Act to Persons with
Psychiatric Disabilities. The Milbank Quarterly. 1998; Vol.76 No. 1. 14 Becker DR, Drake RE, Naughton WJ. Supported Employment for People with Co-Occurring Disorders. Psychiatric
Rehabilitation Journal. Spring 2005; Volume 28 Number 4.
95
iii.Competitive employment is the goal
iv.The search for a job begins rapidly
v.Job finding is individualized
vi.Follow-along supports are continuous
o Job coaches
“A consultant serving as an agent of the employee, while also working cooperatively
with the employer, may be helpful in mediating some of the tensions involved. Such
interventions have been constructive in vocational programs when “job coaches” work
with both clients and employers to solve work problems as they arise”9.
7.1.2 Activities of Daily Living
Time Management is especially done to decrease the individual with an eating disorder’s
time spend on an overall pre-occupation with planning and preparing meals.
Healthy living is promoted by looking especially at healthy eating and sleeping habits,
this is usually done by psycho-education.
7.1.3 Leisure
The occupational therapist assess the client’s time spend on leisure and make sure the
client does not spend too much time on exercise. Treatment can be conducted through
leisure activity participation.
7.1.4 Social
Social skills training are imperative for clients with eating disorders, since social skills are
crucial in overall functioning. This is most effectively done by role-play; according to G
Moskowitz role-play is “a concrete way of transferring what one knows into what one
does”15. Role play is a tool where the client is given an opportunity to explore new
behaviour that would otherwise be foreign to him during group therapy 11.
15 Fouche L. Role Play. Class-notes: University of Pretoria, Occupational Therapy Department. Unpublished material. 2002
96
7.2 Theoretical Framework
7.2.1 Models
The following models can be applied by the occupational therapist in the treatment of
eating disorders:
o Creative Ability model,
o Model of Human Occupation,
o Canadian Occupational Performance Model,
o Model of Occupation through adaptation
7.2.2 Frame of References / Approach
Several treatment approaches are describe in literature and used in practice. A few of
these are discussed to illustrate the unique contribution the occupational therapist makes
as part of the team. (Please note: The approach is not explained or discussed in full.)
Behavioural:
Occupational Therapists do not often use the behavioural approaches in its pure form in
their treatment, but would as part of the multi disciplinary team. Patients may be allowed
to attend occupational therapy sessions of the ward and engage in craft activities, as part
of a reward or positive reinforcement behavioural programme.
This is by no means the focus of the occupational therapist's contribution. The
occupational therapist is in the excellent position to help patients recover with
engagement in 'doing'- or 'in-action' – therapy.
Cognitive behavioural approach:
Within this approach the contribution of the occupational therapist can be invaluable.
Psychotherapy alone might not help the patient with all their practical difficulties. During
activity the patient can start testing basic assumptions and practising the implications of
their insights gained in therapy16
16 Giles MG. Anorexia nervosa and Bulimia. An activity orientated approach. The American Journal of Occupational Therapy. 1985. 39(8). 510-517

97
“Despite the many advantages of the cognitive behavioural approach, practical activity is
inadequately stressed. Helping a patient work through his or her inappropriate thoughts
about cooking and eating a meal are best done while cooking and eating. ...... When
particularly negative thoughts arise, they are dealt with more spontaneously in the
relevant situation....Understanding and insight needs to be supported by activity... During
practical activities, basic assumptions may become apparent.”16
See evidence table.
Cognitive approach:
The occupational therapist helps patient to learn self-monitoring, cognitive restructuring,
measures to reduce risk of relapse as well as training in problem solving and other coping
skills11.
Activity orientated approach: Creative ability:
This approach aims to facilitate the highest creative response to increase a person’s
creative ability. It is important for eating disorder clients/patients to have a highly
individualised programme with their creative abilities as well as interests. This approach
allows for exploration and will emphasize the clients' effect on their environment to
improve the sense of personal effectiveness.
In practice it is often found that these patients has very little or no problems with
performance components. (Concentration, memory, following of instructions etc.) They
can engage in a task and produce end products of high quality. They do however struggle
with life skills such as time management and assertiveness. (Performance areas)17
In the article “When doing is not enough” the authors paint a similar picture18. Despite
excellent performance, a remark such as 'well done' after successful completion of a task
will be regarded as irrelevant or even be received with mistrust. They refer to
competencies not being the problem but a sense of effectiveness. For these
competencies (objective capacity for success) to be of value it must be accompanied by a
subjective belief. It is this belief that is lacking in the anorexic18.
17 Krasner Z. Consultation interview. 2006. Tara Hospital. 18 McColl MA, Friedland J, Kerr A (1986): When doing is not enough: The relationship between activity and effectiveness in Anorexia nervosa. Occupational Therapy in Mental Health: a journal of psychosocial practice and research, 6(1), 137-150.

98
During childhood it might be that everything is provided for these children (often from high
socio-economic backgrounds), but that they do not have sufficient opportunity to learn that
they have an effect on their environment. Therefore a sense of personal effectiveness
does not develop.
It is very important for the occupational therapist to help the patient recognise the effect
they have on the environment and so improve their sense of effectiveness. She must be
aware that she is exercising her own free will. This can only be done during activity
participation, with the skilled facilitation of carefully selected activities18.
Functional approach:
In this approach the occupational therapist helps the patient with practical learning of new
activities like cooking, shopping etc.
7.3 Treatment Programs Treatment programmes based on Stockwell11.
7.3.1 Anorexia nervosa
Multidisciplinary inpatient treatment is desirable for this diagnosis. After discharge follow-
up will happen on an outpatient basis, but outpatient treatment can also be considered
when admission is not suitable.
During the early stages (re-feeding) the occupational therapist's role would be limited as
the physical movement is discouraged and patients might be on bed rest. During this time
it is important to establish a good foundation for the therapeutic relationship.
During the middle stages treatment will work towards modifying body image, acceptance
of body shape, improving social and assertiveness skills and anxiety management. Useful
techniques include: relaxation (increase body awareness), assertiveness and social skills
training, psychodrama, movement therapy as well as crafts and creative activities
(writing)11.

99
In the latter stages the focus will move to planning and cooking meals, eating with others
as well as work or school related aims (perfectionism and effectiveness).
7.3.2 Bulimia nervosa
These patients can be treated on inpatient as well as outpatient basis11
In the early stages of treatment it is important to establish a secure therapeutic
relationship so that issues regarding control can be explore. The patient might be
ambivalent to engage as it might feel like giving up control, but have a great need to
control their emotions and behaviour. It is important to facilitate a greater sense of self.
During the middle stages the patient can be helped to address the binge-guilt-restrict
cycle and identify and addressing other needs. This can be done through drama groups,
assertion and social skills sessions and practical activities11.
During the latter stages the focus will be on consolidating experiences and preparing to
return to their lives with changed habits. Role play could be used to prepare for social
situations.
8. TIME-SPAN
8.1 Acute
• 2 sessions evaluation (including level of creative ability, collateral information and
possible family interview)
• 10 sessions individual treatment (Cognitive behavioural and activity orientated)
• 15 sessions Occupational Group Therapy (Cognitive behavioural and functional
approach.)

100
8.2 Chronic
• Ongoing evaluation
• 20 sessions individual treatment, two weekly over a year.
• 35 sessions Occupational Group Therapy, weekly over a year.
9. TABLE OF THE EVIDENCE
Author Study population
Type of design
Treatment group
Outcome variable
Findings
Garner DM,
Rockert W,
Davis R,
Garner MV,
Olmsted
MP, Eagle
M.19
60 clinical
referrals to
eating
disorder
programme.
(Bulimia
Nervosa)
Experimenta
l two group
design
Cognitive
behavioural
vs
Supportive-
Expressive
therapy
Bulimia
symptoms
(Eating
disorder
inventory)
Psychologic
al
functioning
Significant
improvement
s in both
groups with
results
moderately
in favour of
cognitive
behavioural
therapy.
Robinson A,
Kane M,
Leicht SB20
Surveys
were sent to
75 members
of the New
York State
Psychologic
al
Association
who had
self-
Self report
Questionnair
es
The results
of this study
show that
psychologist
s currently
use many of
the same
treatment
modalities
occupational
19 Garner DM, Rockert W, Davis R, Garner MV, Olmsted MP, Eagle M. (1993) Comparison of cognitive behavioural and supportive-expressive therapy for bulimia nervosa. American journal of Psychiatry, 150(1) 37-45. 20 Robinson A, Kane M Leicht SB (2005): Psychologists' perceptions of Occupational Therapy in the treatment of Eating Disorders. Occupational Therapy in Mental Health: a journal of psychosocial practice and research, 21(2) 39-53.

101
identified as
treating
eating
disorders.
therapist’s
use with
people with
eating
disorders
and view
those
techniques
as beneficial
for this
population
Kong s21 Volunteers
from an
outpatient
clinic for
eating
disorders
(n=43)
Pretest-
posttest
control
group
experimental
design
Treatment
group
(n = 21),
participating
in a modified
day
treatment
programme
Control
group
(n = 22)
receiving a
traditional
outpatient
programme
Participants
in the day
treatment
programme
showed
significantly
greater
improvement
s on most
psychologica
l symptoms
of the Eating
Disorder
Inventory-2,
frequency of
binging and
purging,
body mass
index,
depression
and self-
esteem
21 Kong S (2005): Day treatment programme for patients with eating disorders: randomized controlled trial. Journal of advanced nursing, 51 1) 5-14.

102
scores than
the control
group. They
also showed
significant
improvement
in
perfectionis
m, but the
group
difference
was not
significant.
10. CONCLUSION
In conclusion, the occupational therapist has a unique and crucial role in the rehabilitation
and care of people suffering from eating disorders. The 'doing' part of this process that is
achieved through activities facilitates the change needed.

103
11. REFERENCES
1. Barnett S, Buckroyd J, Windle K (2006): Using group therapy to support eating disordered
mothers with their children: the relevance for primary care. Primary Health Care Research
and Development, 7(1)39-49.
2. Garfinkel PE and Garner DM (1982): Anorexia Nervosa: A Multidimensional Perspective.
Brunner Mazel: New York.
3. Sue D, Sue DW, Sue S (2003): Understanding Abnormal Behaviour, 7th ed. Houghton
Mifflin.
4. Murphy RMN, Manning RMN. An Introduction to anorexia nervosa and bulimia nervosa.
Nursing standard. 2003 Dec 17: Vol 18: 45-52.
5. Henderson S (1999): Frames of reference utilized in the rehabilitation of individuals with
eating disorders. Canadian Journal of Occupational Therapy, 66(1), 43-51
6. DeLaune SC, (1991): Effective limit setting, How to avoid being manipulated. Nusing
Clinics of North America, 26(3) 757-763
7. Halek BA. Anorexia nervosa. Nursing Standard. 1997 Dec 10; pp 41-47.
8. Ben-Tovim DI. Eating disorders: outcome, prevention and treatment of eating disorders.
Lippincott Williams & Wilkins, Inc. 2003 Jan; Vol 16(1): pp 65-69.
9. Crisp AH, Norton K, Gowers S et al. A controlled study of the effect of therapies aimed at
adolescent and family psychopathology in anorexia nervosa. British Journal of Psychiatry.
1991. Vol 159; 325-329.
10. Bridges 1993

104
11. Stockwell R. Duncan S. Levens M. In Scott & Katz (Eds.) Occupational Therapy in Mental
Health: Principles in practice. 1988. London: Taylor and Francis, Ltd.
12. World Health Organisation, International statistical classification of diseases and related
health problems.10th revision. Volume 3. W.H.O. Geneva.1994.
13. Mechanic D. Cultural and Organizational Aspects of Application of the Americans with
Disabilities Act to Persons with Psychiatric Disabilities. The Milbank Quarterly. 1998;
Vol.76 No. 1.
14. Becker DR, Drake RE, Naughton WJ. Supported Employment for People with Co-
Occurring Disorders. Psychiatric Rehabilitation Journal. Spring 2005; Volume 28 Number
4.
15. Fouche L. Role Play. Class-notes: University of Pretoria, Occupational Therapy
Department. Unpublished material. 2002
16. Giles MG. Anorexia nervosa and Bulimia. An activity orientated approach. The American
Journal of Occupational Therapy. 1985. 39(8). 510-517
17. Krasner Z. Consultation interview. 2006. Tara Hospital.
18. McColl MA, Friedland J, Kerr A (1986): When doing is not enough: The relationship
between activity and effectiveness in Anorexia nervosa. Occupational Therapy in Mental
Health: a journal of psychosocial practice and research, 6(1), 137-150.
19. Garner DM, Rockert W, Davis R, Garner MV, Olmsted MP, Eagle M. (1993) Comparison
of cognitive behavioural and supportive-expressive therapy for bulimia nervosa. American
journal of Psychiatry, 150(1) 37-45.
20. Robinson A, Kane M Leicht SB (2005): Psychologists' perceptions of Occupational
Therapy in the treatment of Eating Disorders. Occupational Therapy in Mental Health: a
journal of psychosocial practice and research, 21(2) 39-53.

105
21. Kong S (2005): Day treatment programme for patients with eating disorders:
randomized controlled trial. Journal of advanced nursing, 51 1) 5-14.

106
MAJOR DEPRESSION Compiled by: Enos Ramano-Occupational Therapist
1. INTRODUCTION
The simplest and best way to explain occupational therapy is that it enables individuals of all
age groups to cope with their roles and tasks at home, social and at work, despite the
presence of some residual symptoms of their illness.
Occupation was understood narrowly as synonymous with activity.1 The use of activity as
therapy for mentally ill lay dormant for decades. Occupation in this sense denotes to
personal care activities, household activities, leisure activities, work activities and all kinds of
‘doing’ people engage in. Occupational science, the study of how people occupy their time
or as Law stated: “everything people do to occupy themselves” (Law 2002) is the theoretical
backdrop of occupational therapy. Therefore if a mental illness or any mental health problem
interferes with the normal way of how people occupy their time, occupational therapy is
indicated.
The Dunton creed of 1919 states:
“That occupation is as necessary to life as food and drink. That every human being should
have both physical and mental occupation… That sick minds, sick bodies, sick souls, may be
healed through occupation” (Creapeu, Cohn & Boyt Schell 2003: 17)
Referrals for occupational therapy service may come from various sources and can include,
but are not limited to:
• Other health professionals
• Hospitals
• Support groups
• Social workers
• Lawyers
• Insurance companies

107
2. DIAGNOSIS ACCORDING TO ICD-10 AND DSM IV Mood refers to the internal emotional state of an individual. Mood may be normal, elevated
and or depressed. Mood disorders are a group of clinical conditions characterized by a
disturbance of mood, a loss of that sense of control, and a subjective experience of great
distress,2 and it may be divided into two broad categories, namely the depressive and the
bipolar disorders.
Depressive disorder may be present and categorized in these ways: 2
• ICD10:F34.2 Adaptation disorder with depressed mood
• ICD10:F34.1 Dysthymic disorder
• ICD10:F32.2 Major depression without psychotic symptoms
• ICD10:F32.3 Major depression with psychosis
• ICD10:F32.1 Moderate depressive episode
• ICD10:F32.9 Depressive episode unspecified
• ICD10:F41.2 Mixed anxiety and depressive disorder
• Major depression with melancholia
3. THE IMPACT OF MAJOR DEPRESSION ON OCCUPATION By 2020, depressive disorders are expected to be the second biggest cause of disease
burden worldwide 3. This category of psychiatric illness is therefore of critical importance to
mental health practitioners and communities that need to collaborate in stemming the tide of
disease burden.
It is known that this feeling of depressed mood is accompanied by a loss of interest and
pleasure in life, its activities and responsibilities. Depressed patients show an inability to
perform even the simplest daily tasks. They are frequently pre-occupied with work, money,
family and their own health problems.
Childhood depression may occur in the absence of an overtly unhappy mood and manifest in
symptoms different from those seen in adult depression i.e. refusal to attend school, learning

108
difficulties, accident proneness, enuresis and encopresis, delinquency, aggressiveness and
obsessions.
The findings of the review of 23 studies indicated that occupation has an important influence
on health and well-being. Withdrawals or changes in occupation for a person have a
significant impact on a person’s self perceived and well-being. These performance
components that are experienced by depressed clients will affect their occupation and or
performance areas as follows:
3.1. Work/School
The depressed clients will show lack of energy and interest to go to work which will impact
their work habits such as poor personal presentation (untidy appearance, lack of self control,
high sick absenteeism or poor work attendance and unpunctuality at work) poor social
relationships and poor work competency (poor work planning and disorganisation, poor
concentration and poor memory, tiredness, difficulty handling a stressful job, poor frustration
tolerance and poor problem solving skills).
Depression causes impairment in work performance. Lack of drive, energy and motivation
have an adverse effect on productivity an cause an overall decline in the quantity and quality
of work; impairment of concentration is hazardous in employees responsible for driving or
operating machinery. In addition to loss of verbal fluency and impaired ability to maintain
attention, there is often a difficulty in making decisions and an increase in risk behaviours
which will have a negative impact to their relationship in the workplace. The depressed client
constantly complains of forgetfulness, tiredness, psychomotor retardation and headaches
which will affect their work speed and work endurance. A child who is attending school will
show deterioration in school performance and the dropping of his grades or marks.
3.2. Activities of daily living
A large percentage of depressed patients show loss of appetite and consequent weight loss,
increased appetite and consequent weight gain, sleep disturbances, psychomotor
disturbances (retardation and or agitation), low self esteem, lethargy and fatigue, poor

109
concentration and memory deficits, decreased libido and suicide thoughts.2,4 These will affect
their execution of activities of daily living.
Self care is completely neglected in some severe cases, and the patient shows little interest
in caring for himself and or his surroundings.
3.3. Leisure activities Most depressed client’s show lack of energy, loss of interest and poor motivation to execute
leisure activities. They experience lethargy and lack of energy to be actively involved in
leisure activities. Their activity profile is poor since they spend most of their time indoors and
or sleeping. They even show loss of interest in watching sport or listening to music.
3.4. Socialisation Most depressed clients show social withdrawal since they prefer to be alone most of the
time. A large percentage of depression suffers exhibit what is crudely called “poor social
skills” such as being less assertive, being less positive, displaying less interaction etc.
4. THE IMPACT OF DEPRESSION ON ROLES, HABITS AND ROUTINE In a large percentage of depressed clients, it is found that their work, play, friends and family
are neglected. They loose interest and or lack the motivation to perform their roles as
father/mother, son/daughter, worker/scholar and or friend appropriately.
Most of them show poor coping skills and they engage themselves in risk taking habits such
as excessive alcohol consumption and self medication as inappropriate means of handling
their issues.
Due to their lethargy, psychomotor disturbances, poor concentration and forgetfulness, lack
of energy and lack of interest, they find it difficult to engage themselves in a proper daily
routine.
110
5. HEALTH CARE STRUCTURES 5.1. Pillars of healthcare
5.1.1. Preventative/Promotive
Preventive health refers to tasks and efforts of the occupational therapist in limiting
health problems and the stress arising from them. 20 These may refer to life skills
training, as an example, either on an individual basis or within the community that can be
seen as preventative. These skills could include financial management, career planning,
social skills etc. All these skills enable the community member to deal with different
situations, which they found to be difficult to cope with previously. These will therefore
decrease the chances of developing depression. The occupational therapist can also
establish psycho-educational groups to try and improve the patient’s insight into their
depression and the importance of compliancy to medication, as a way of trying to reduce
chances of relapse and or non compliancy to treatment.
The definition of promotion reads as ‘the systematic efforts to enhance wellness through
education, behavioural change and cultural support’(20). The client’s capacity for coping is
increased and the client is encouraged and empowered to achieve well being.
In contrast to prevention that directly tries to prevent illness, promotion emphasizes
wellness. The occupational therapist can also address the environmental problems in a
work place, if needs be, as part of promotive role to help employees structure their work
areas and make use of work study principles and process charts in order to reduce
chances of a relapse.
5.1.2. Curative/Remedial programme
Occupational therapists are familiar with the curative role as this incorporates the more
traditional and known roles of occupational therapist within hospitals and institutions. The
therapist therefore strives to cure the client and place him back into his environment
without any further problems. This is also known as following a remedial programme.20

111
In this phase the occupational therapist will be strongly involved in the treatment of the
depressed patient to try and remediate or improve their specific performance
components (e.g. facilitate appropriate emotional response, improve concentration,
improve energy and physical fitness) that will in turn improve the clients occupational
performance areas (e.g. appropriate social interaction, improve proper work habits) to
the level that it was before the depression.
5.1.3. Rehabilitation
Rehabilitation implies that the patient has a remaining disability/impairment that he
needs to compensate for in order to function at his optimal level and to maintain quality
of life 20. The occupational therapists are mostly familiar and categorised with the
rehabilitation role, as it is their traditional role. This type of programme will be used
especially with patients suffering from chronic severe depression and their occupational
performance areas are permanently affected.
An example will be a patient who has developed depression after a divorce; she may
need temporary help concerning her children and her day programme to compensate for
the poor energy levels of her major depression. As soon as the mood improves, these
interim measures may no longer be necessary. Additionally, it may be the permanent
change in a work situation to prevent recurrent relapses of depression such as changing
to a new section or choosing a new job/career to try and compensate for a permanent
poor concentration and poor memory due to depression. The occupational therapist
might also need to liase with the employer of the depressed client so that they
reasonably accommodate his chronic depression by job restructuring (decreasing his
work load), flexible scheduling (allowing him to work slower, time off for consultations),
provision of job sharing/assistant etc.

112
5.1.4. Maintenance
During this phase the occupational therapist is trying to maintain the client’s impairment
or disability to try and prevent further deterioration.
This might include consolidation of life skills with the severely chronic depression
patients for their survival even though they will be showing poor prognosis for further
recovery. The occupational therapist will try and maintain their available skills in
executing performance areas. The occupational therapist might also include the family
during therapy with these patients to try and teach the family on how to cope with them.
5.2. Levels of healthcare
5.2.1. Primary care
The occupational therapists have a very important role to play at primary level of
healthcare with major depressive disorder patients. They could try to prevent depression
by helping people in the community to have a balanced life style in terms of their work,
leisure, personal management and relationships. The occupational therapist will be
involved in helping with bereavement counselling to prevent complications in
bereavement and the development of depression.
It may also include screening tests for depression in order to identify the disorder as
early as possible. They may also have insight sessions with patients suffering or in the
early stages of their depression.
Due to the hospitals limiting admissions time span, the occupational therapist will
continue with the patient’s treatment of depression in the rooms on an outpatient basis or
in their own homes to try and address their problems of the performance components
and occupational performance areas.
5.2.2. Secondary level

113
The prevention of illness on a secondary level occurs within a hospital setting. The
occupational therapist will try to prevent the client’s disorder from becoming chronic, by
engaging the client in therapeutic activities.
Life skill training could be seen as part of treatment on a secondary level, for example
assertiveness training or social skills training. Teaching the client specific work skills
could also assist the patient in coping with workload.
5.2.3. Tertiary level
The occupational therapist assists the client to compensate for the impairment in order to
function at his optimal level and to maintain quality of life. The treatment programmes
provided on this level are intense and may be very specialized. Therapy emphasises on
the occupational performance areas and helps clients to adjust and adapt their
environment in order to function optimally with their depressive illness.
Example: The occupational therapist can liase with the employer to reasonably
accommodate the client’s major depressive disorder and to assist with possible
adaptations.
6. ASSESSMENT The occupational therapy assessment evaluates the client holistically. The interview of the
client individually can last for sixty minutes. The comprehensive evaluation varies from one
to four hours, depending on the client’s psychological status, tolerance, attention span and
the reason for the assessment (4) and if whether it is for clinical intervention and or medico-
legal/insurance purposes. The compiling of the report may also last for two hours or more
depending on the information analysed and the purpose of the report.
6.1. Baseline assessment An objective assessment of the individual’s physical/mental abilities to perform a variety of
tasks related to the physical demands of work and to compare functioning over time.

114
6.1.1. Professional interview
The interview is conducted with the patient to gather detailed background information,
inquires about the patient’s feelings, previous illnesses and treatments, stressors at
home, work, financial and future are made. If the interview is too stressful for the patient,
the patient may be asked to write a story or an essay about himself.4
6.1.2. Clinical observation
During the interview the therapist will observe the client’s non-verbal signs such as tone
of voice, gestures, facial expression and personal appearance.
The therapist will also observe the client’s performance and behaviour during the use of
standardized and non-standardized tests and compare that with the assessment results.
The patient will also be observed during participation in various activities and discussion
groups as part of on-going assessment.4
6.1.3. Evaluation
The occupational therapist uses and chooses variety of standardized work samples,
questionnaires, inventories and pain scales to assess the client’s fitness to work and the
severity of the depression to the other performance areas. The occupational therapy
assessment with depressed patients will cover the following performance components
and occupational performance areas:
• Emotions (affect, mood, body image and self esteem)
• Conation/Motor behaviour (psychomotor disturbances, psychological endurance,
perseverance)
• Cognitive assessment (Orientation, Thought process, Memory, Attention and
Concentration, Decision making, Judgement, Insight and Intellect)
• Life skills (Reading, Writing and Money management)
115
• Self Management Skills (Occupational stressors/Coping skills, Time Management and
Self control)
• Occupational performance areas (Activity of daily living, Leisure, Work and
Socialisation)
The following are the examples of other tools (formal and informal) that are used for
evaluation to assess the above mentioned aspect by the occupational therapist working
with depressed clients:
• Hospital Anxiety and Depression Scale (HADS)
• Beck Depression Inventory (BDI)
• Wimbledon Self Report Scale (WSRS)
• Cognitive Assessment of Minnesota (CAM)
• Brief Cognitive Rating Scale (BCRS)
• General Health Questionnaire
• Rosenberg Self Esteem Scale
• Relevant pain Questionnaires (e.g. Borg numeric pain scale)
• Assessment of Motor and Process Skills (AMPS)
• Modular Arrangement of Pre-determined Time Standards (MODAPTS)
• Work Assessment Screening Program (WASP)
• Rivermead Behavioural Memory Test
• T/PAL
• Chessington OT Neurological Assessment Battery (COTNAB)
• Jamar hand dynamometer
It must be noted that if the evaluation tools are not suitable for the client, the
occupational therapist can perform on the job evaluation (work visit), where the client is
evaluated on site in a competitive work environment in order to determine job specific
functional capacity evaluation.

116
6.1.4. Collateral information
Each person has to be compared against their own previous abilities and behaviour,
hence the importance of gathering information from people who knew the person prior to
their depression such as close family members, the employer and colleagues and other
role players who will also be interviewed by the therapist. The occupational therapist
might also need to peruse previous medical documents and or available reports about
the patient as part of collateral information. The other treating specialists might need to
be interviewed as well to clarify the client’s condition.
6.1.5. Assessment report
During the completion of the assessment, the occupational therapist can assist with
comprehensive functional capacity evaluation reports for disability grants, medical
boarding, and recommendations for alternative occupations and to suggest possible
reasonable accommodations for major depressive disorder patients in a work place.14
6.2. Ongoing assessment Ongoing assessment is a process that needs to be repeated at least once during
intervention, and conclude the therapy process.4 .Ongoing assessment is particularly
important in the cases of patients suffering from depression due to the effect of their
medication and environmental stresses.
7. INTERVENTION
7.1. Role of Occupational therapy in the treatment of major depressive disorder
Intervention by the Occupational therapist is most effective as part of multi-disciplinary team
approach especially at secondary and tertiary level.
In 1990, a study by Karen Larson, with depressed patients, showed that activities can be
used to assess the activity level of a patient and for intervention.5 Verbal therapy and activity

117
therapy were also compared, and it was found that subjects who received activity therapy
experienced a greater reduction in symptomatology, (improvement in concentration and
memory, improvement in motivation and energy, improvement in decision making and self
esteem and improvement in social interaction abilities) than those who received verbal
therapy.
Some of the selected graded activity therapy, occupation or achievable tasks6 that are used
by occupational therapists in the treatment of depression are grouped according to our daily
performance areas as follows.7, 8
7.1.1. Self care task and community survival skills
Self care is occupation that enables the individual to survive and that promotes and
maintains health. This includes.9
• Caring for oneself to improve self-esteem.
• Cooking and baking activities to discuss the importance of balanced diet and meal
planning.
• Psycho-education to teach the patient about the effect of depression, symptoms, pre-
cursors to symptom exacerbation and the importance of compliancy to medication.
• Teach patient proper home management skills, parenting skills and money
management skills as an individual or in a group.
Each session that covers some of the above self-care activities may last for an hour (one
hour), on an individual basis and two hours during a group therapy session.
7.1.2. Leisure and or Recreational activities
• Sports and exercises (e.g. walking, aerobic exercise, volleyball, swimming or
hydrotherapy etc).
Literature shows that exercise sessions should take place at least three times a week if
both the physical and mental benefit is to be maintained. People suffering from mild to

118
moderate unipolar depression are more likely to benefit from exercise than those with
melancholia or bipolar disorders.8, 9
• Art and creative activities [e.g. flower arranging, candle making, painting, narrative or
writing therapy, collage etc]
Through these activities the depressed persons are able to express what they are
feeling towards themselves, express how they are feeling now and they also encourage
self- exploration.3,8 It must be noted that occupational group therapy focuses on the ‘here
and now’ approach.
The above mentioned leisure activities may be more effective and therapeutic when they
are performed in a group therapy session that lasts for one to two hours.
7.1.3. Socialisation
Extremely common in depression sufferers is the lack of satisfaction in various
relationships: family, work and social. Depression can cause the individual to loose
access to the skills and the desire to sustain these relationships successfully.
The occupational therapist will use occupational group therapy technique as an effective
brief and reliable method for assessing and treating depressed patients (10).
Occupational group therapy sessions are found to be effective and they teach and cover
the following3, 10,11,12,13:
• Social skills - Communication skills
- Assertiveness and conflict resolution skills
- Anger management skills
• Support group [support of one another, ventilation of feelings, imparting of information]
• Projective group therapy
• Coping skills training [time management, stress management, problem solving skills,
balanced lifestyle development, money management etc].

119
• Various group therapy activities which are client centered.
For effective results and quality of service, the patients will benefit from eight to ten
consecutive group therapy sessions that last for one hour thirty minutes to two hours a
session.10, 13
7.1.4 Work related activities [Vocational Rehabilitation]
Literature has shown that one does not get better in order to work, but one works in
order to get better. Work is seen as the critical element in the recovery of depressed
patients, since it boosts their self esteem and it provides a sense of purpose and
accomplishment. Different studies in occupational therapy predict better vocational
outcome for people with mood disorders3.
The Occupational therapist plays the following roles in the vocational rehabilitation of
major depressive disorder clients:
• Vocational counselling - advising the person with depression in the light of vocational
training and employment possibilities 3.
• Advocacy – The Occupational therapist acts as an advocate for the patient and this is
backed up by the present Labour Relation Act (LRA) and Employment Equity Act
(EEA) (15).
• Work preparation and training - this provides any necessary reconditioning and
training to the mood disorder client. These may be performed by means of: 3
o Work simulation
o Work hardening
o Role-play
o Job coaching
o On the job training
o Work trial

120
o Supportive employment
• Selective Placement – the occupational therapist ensures that the client returns to his
own or alternative occupation with or without reasonable accommodations.
• Follow up – until resettlement is achieved.
The Occupational Therapist who specializes in vocational rehabilitation may provide an
estimated eight to ten sessions of vocational rehabilitation, which lasts for two to four
hours a session, on an individual or group basis. The number of sessions is mostly
determined by the severity of the client’s depression, work motivation and compliancy to
multidisciplinary intervention, support system and medical and vocational prognosis.
7.2. Theoretical Framework
The activity therapy and/or occupations that are used in occupational therapy are utilized in
conjunction with certain therapeutic techniques, approaches and equipment to build up the
abilities and skills needed for the depressed patient to enable him/her to eventually execute
their daily tasks independently.9
7.2.1. Models
Creative Ability Model (Vona du Toit)
This is a South African approach that was elaborated in 1962 by Vona du Toit. This
approach is used to evaluate the client’s occupational performance according to the
skills he has attained in the personal, social, work and recreational occupational
performance area 3.
It also provides guidelines for treatment by:
• Identifying treatment priorities
• Proposing principles that guide treatment so that it is appropriate to the client’s level

121
• Determine expectations for performance, as well as how and when to up or
downgrade the treatment.
This approach also helps the occupational therapist to categorise patients efficiently in
terms of their occupational performance needs and it enables the correct treatment to be
administered at the right time and in the most cost effective manner.3.
This approach does not represent the whole of occupational therapy for the client. It has
an assessment aspect, which determines the level on which the client functions and then
provides a stratified guide to increase the client’s level of performance.
This approach accommodates clients suffering from depression and mania, and it
assists with proper grouping and approach during their intervention.
This theory postulates that creative ability consist of two components:
• The inner drive towards action
• The externalisation of this motivation into action, which is seen through the creation of
concrete or abstract end-products in daily life.
More research is being done by South African occupational therapists to standardize this
approach, and to evaluate its reliability and validity.16
Model of Human Occupation (Kielhofner) 20
• The model addresses a person’s occupational behaviour and occupational
dysfunction.
• Occupation is essential to human self-organization. Through occupations, persons
exercise their capacities and generate on-going experiences that affirm and shape
their psyches. Therefore the order or organization of humans depends on
occupational behaviour.
• Occupational therapy engages persons in occupational behaviour that helps maintain,
restore, reorganize, or develop their capacities, motives and lifestyles.

122
• Specific subsystems contribute to occupational behaviour and needs to be addressed
i.e. volition, habituation and mind-brain-body performance.
7.2.2. Frame of Reference/Approaches for the treatment of major depression
The Occupational therapist uses a variety of frames of reference and approaches during
therapy. These may be used in combination for a single client to direct therapy.
Some of the approaches are summarized below as follows:
Psychosocial analytical approach
Therapy is directed at improving the client’s insight and understanding of themselves
and their environment. The Occupational Therapist does not interpret, but assists the
client to reflect on the past and their feelings. 4
Psychosocial interactive approach This approach is mostly used during occupational group therapy where the focus is on
the here and now and on the interaction between the group members. The interaction
can be facilitated within the therapeutic, structured group where the clients are
encouraged to achieve personal growth, insight and develop social skills by means of
feedback from others.4
Cognitive approach
Some aspects of the treatment repertoire of cognitive therapy are very familiar to
occupational therapists and are consistent with the practice of occupational therapy.
They include: 3, 8, 9
• Educator/facilitator role - teach patients new skills, ways of interacting with others and
viewing the world.
• Use of activities to facilitate change
123
- Group activities
- Role-play
• Use of images in therapy
- Role-play
- Art
- Clay
Distraction technique is also used by engaging patients in constructive activities such as
crossword puzzles, listening to music etc.
Occupational therapists help the depressed client to become proficient at identifying and
countering cognitive distortions (irrational thought, negative self-evaluation, over-
generalisation of simple mistakes, negative self talk etc) - in that way depression looses
its strength.
Evidence suggest that cognitive therapy is valid in occupational therapy for patients with
mild to moderate depression and possibly for patients with more severe depression.8, 13
Cognitive behavioural approach The occupational therapist uses the following principles of the cognitive behavioural
approach:
• Training
• Repetition
• Modelling
• Practice and
• Association
This approach suits the occupational therapist because of its focus on functional problem
solving skills which help the patient identify and practice alternative behaviours to
problem situations.3, 8

124
It can be applied successfully to teaching, relaxation techniques, prevocational skills etc:
Social modelling may also be used, especially during role-play, to train social skills to the
depressed client. 3
The Cognitive behavioural approach is strongly considered as an initial therapy for
patients with severe or chronic depression.17 Literature also shows that 35% of patients
treated with the cognitive behavioural approach experienced a relapse.18 They also
experienced fewer depressive episodes during follow up periods than did those receiving
standard clinical management.18
Behavioural approach The Occupational therapist will select a new behaviour and break it up into smaller
components and sequence. It is then explained what is expected of the client and every
time the client displays the new behaviour, a reward is given. The reward can be positive
and/or negative. The reward must be given as soon as the new behaviour is displayed.20
• Monitoring activities
The client is requested to keep a record of his/her weekly activities.
• Scheduling activities
Activities are increased according to the pleasure the client derives from performing
them, as well as grading the activities that the client has mastered.
Humanistic approach/Client centered approach
Occupational therapists make use of a client centered approach whereby the client is
involved in the decision making process regarding the direction of their therapy. The
client is given the opportunity to have the capacity for self awareness and to make their

125
own choices. Their interests, roles, needs and habits are taken into consideration during
therapy.
The therapeutic relationship is of great importance in order to facilitate the above;
therefore the therapist should be empathetic, congruent, warm, genuine and show
unconditional positive regard for the client.20
Physiological approach 3, 4, 20 Individuals are a biological ergonomist whose behaviour depends on genetically
determined factors, combined with selective action of nervous and endocrine systems
and the ability of the body to maintain homeostasis. Performance depends on the
integrity and the interactions of all body systems (e.g. cardiovascular, musculoskeletal
etc). Examples of activities that use the physiological approach are aerobics, volleyball
etc.
7.3. Contra-indication for major depressive clients:
• Relaxation therapy and psychodrama are to be avoided in the severely depressed
states.
• Grouping too many depressed patients together may present a stifling atmosphere.
7.4. The most relevant techniques for the treatment of major depression are:
• Occupational group therapy.
• Role play.
• Projective therapy.
• Psychodrama [specialized technique which requires further training].
• Relaxation therapy [Jacobson]
• Counselling
• Music and Art therapy

126
7.5. A balanced weekly treatment programme for major depression patients A balanced weekly programme, at any stage of intervention, could consist of the following
activities, which can be undertaken individually or in groups.4
• Self care activities
• Domestic activities
• Sports and leisure time pursuits should be introduced gradually. Start off with walking
and activities with a low tempo and later introduce volleyball, hydrotherapy or
swimming etc.
• Work related activities.
• Occupational group therapy: psycho-educational, task orientated groups/creative
activities, expressive group and socio-emotional groups, stress management.
At primary level, the patient may need four individual sessions of occupational therapy (one
session per week), that lasts for one hour a session. They may benefit from six to eight
occupational group therapy sessions that lasts for ninety minutes. The occupational group
therapy session may be held once or twice a week for a period of two months and if there is
no progress, then the patient will be referred to the hospital for hospitalisation.
This weekly programme at secondary level may last for a period of two to four weeks while
the patient is hospitalised during an acute phase. The patient may have five to ten
occupational group therapy sessions per week that lasts for ninety to one hundred and
eighty minutes a session, on a daily basis. The patient may be seen for one to two hours on
an individual basis at least three times a week.
For a chronic phase at tertiary level, the patient may need to be seen for an extended period
of time once a week or twice a month for a period of six to twelve months. The patient may
benefit from individual sessions and group therapy sessions that last for one to two hours.

127
7.6. Time span/ Number of Occupational Therapy treatment sessions
7.6.1. Community/outpatient basis (Primary level)
• 1x session of comprehensive assessment that lasts for 1-2 hours a session (NHPR
code 66108 and 66209)
• 4x individual session that lasts for an hour (NHPR code 66315) a day for a month
• 6-8 x occupational group therapy sessions that lasts for 90 minutes a session (NHPR
code 66305) for a period of two months.
7.6.2. Acute phase (Secondary level)
• 1x session of comprehensive assessment that lasts for one to two hours (NHPR code
66108 and 66209)
• 1x collateral information or consultation (NHPR code 66108/66109)
• 3x session of individual treatment a week that lasts for one to two hours (NHPR code
66315/66317/66319)
• 5-10x occupational group therapy sessions per week that lasts for 90 minutes to 3
hours a session (NHPR code 66305)
• 3x sessions for vocational rehabilitation clients that lasts for an hour (NHPR code
66315)
• 2x follow up session that lasts for 30 minutes to an hour (NHPR code
66108/66311/66315)
7.6.3. Chronic phase (Tertiary level)
Patient in the chronic phase require long-term intervention. A patient may be part of the
occupational group therapy and individual occupational therapy sessions for ±6-12
months.

128
• 1x session of comprehensive assessment that lasts for two to four hours (NHPR code
66108 and 66211)
• 1x collateral information or consultation (NHPR code 66108/66109)
• 1x individual session per week or two individual session per month that lasts for an
hour for a period of six to twelve months (NHPR code 66315)
• 24-50 occupational group therapy sessions for a period of six months that lasts for
ninety minutes a session. (NHPR code 66305)
• 8-10x sessions of vocational rehabilitation on an individual or group therapy sessions
that lasts for two-four hours a session a day (NHPR code 66317/66319).
• 1x reassessment session after six months (NHPR code 66108 and 66209)
8. A TABLE OF EVIDENCE OF THE RESEARCH DONE
Author Study population
Type of design Treatment group Outcome
variable
Findings
Stein &
Smith
(1989)
Acutely
depressed
psychiatric
in-patient
(ages 20-45
years)
Single-group
pretest-posttest
design
Occupational
therapy based
management
training,
including
groups
discussion,
biofeedback,
relaxation
training,
behavioural
rehearsal, and
attention to
everyday
stressors and
activities
useful in
controlling
stress (n=7)
S-Anxiety
scale of the
state-Trait
Anxiety
Inventory
Subjects were
significantly less anxious
at the conclusion of the
program than they were
prior to its initiation
(+0,8)
Good-
Ellis, fine
Recently
admitted
Single-group
pretest-posttest
Occupational
therapy
Role
performance
Unipolar and bipolar
demonstrated different
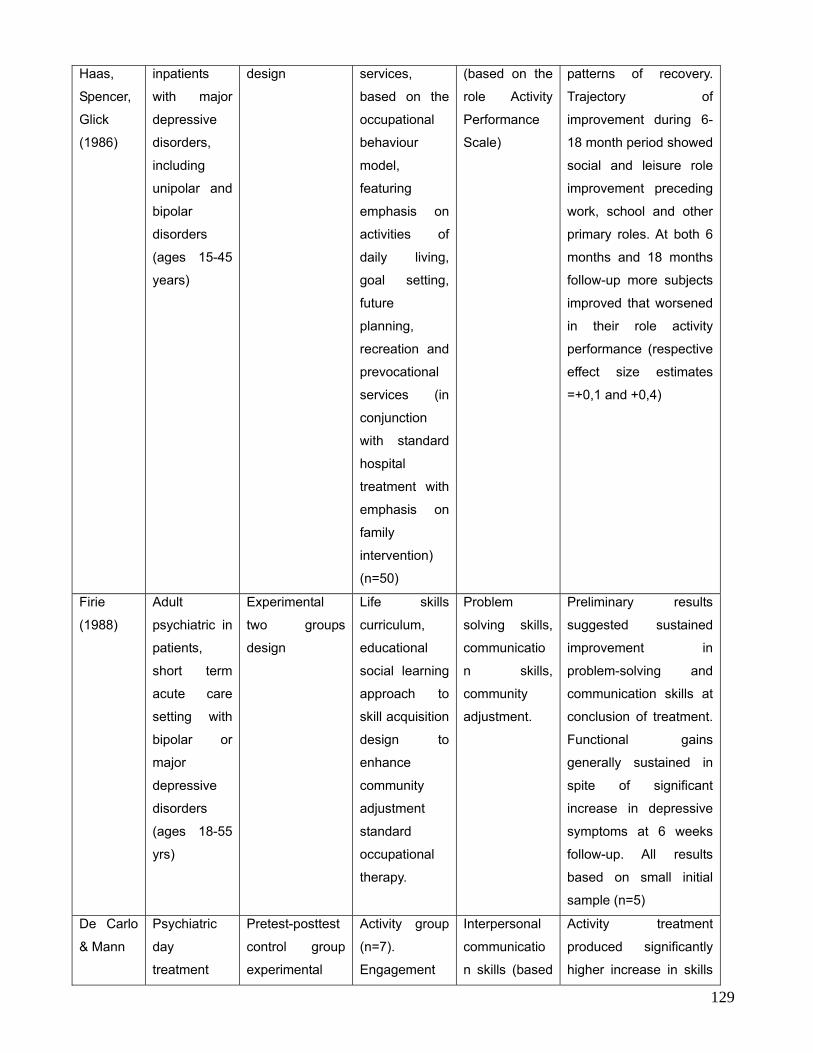
129
Haas,
Spencer,
Glick
(1986)
inpatients
with major
depressive
disorders,
including
unipolar and
bipolar
disorders
(ages 15-45
years)
design services,
based on the
occupational
behaviour
model,
featuring
emphasis on
activities of
daily living,
goal setting,
future
planning,
recreation and
prevocational
services (in
conjunction
with standard
hospital
treatment with
emphasis on
family
intervention)
(n=50)
(based on the
role Activity
Performance
Scale)
patterns of recovery.
Trajectory of
improvement during 6-
18 month period showed
social and leisure role
improvement preceding
work, school and other
primary roles. At both 6
months and 18 months
follow-up more subjects
improved that worsened
in their role activity
performance (respective
effect size estimates
=+0,1 and +0,4)
Firie
(1988)
Adult
psychiatric in
patients,
short term
acute care
setting with
bipolar or
major
depressive
disorders
(ages 18-55
yrs)
Experimental
two groups
design
Life skills
curriculum,
educational
social learning
approach to
skill acquisition
design to
enhance
community
adjustment
standard
occupational
therapy.
Problem
solving skills,
communicatio
n skills,
community
adjustment.
Preliminary results
suggested sustained
improvement in
problem-solving and
communication skills at
conclusion of treatment.
Functional gains
generally sustained in
spite of significant
increase in depressive
symptoms at 6 weeks
follow-up. All results
based on small initial
sample (n=5)
De Carlo
& Mann
Psychiatric
day
treatment
Pretest-posttest
control group
experimental
Activity group
(n=7).
Engagement
Interpersonal
communicatio
n skills (based
Activity treatment
produced significantly
higher increase in skills
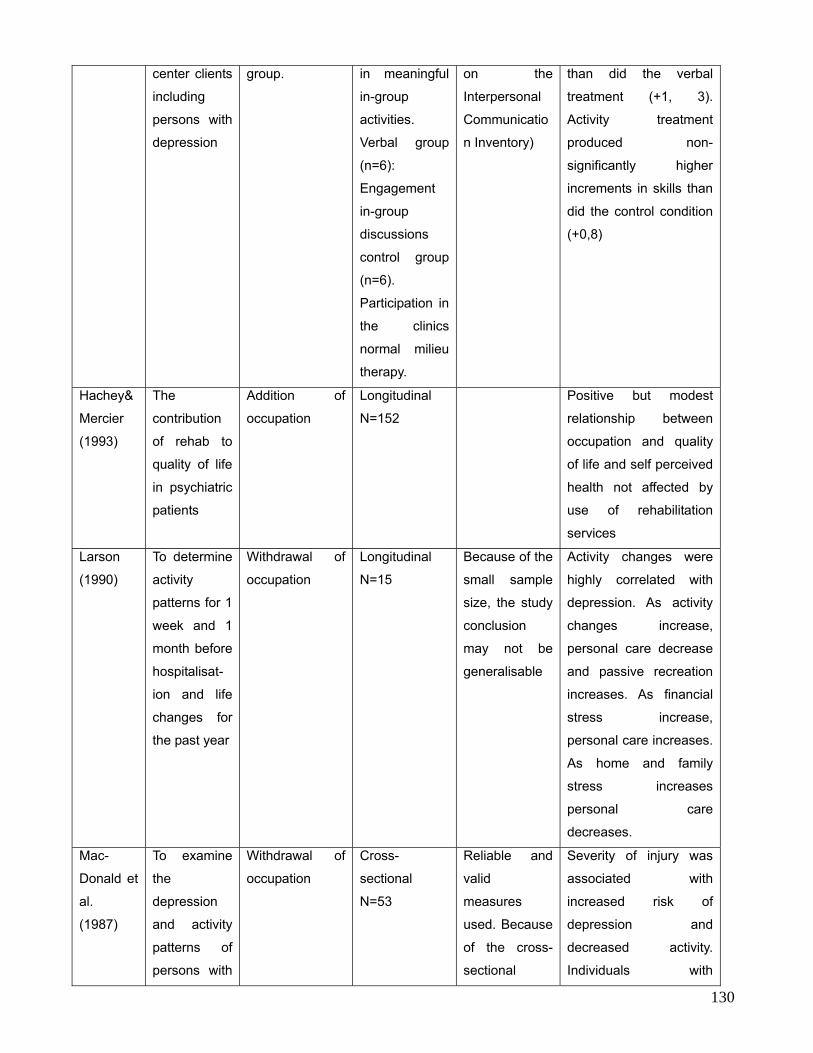
130
center clients
including
persons with
depression
group. in meaningful
in-group
activities.
Verbal group
(n=6):
Engagement
in-group
discussions
control group
(n=6).
Participation in
the clinics
normal milieu
therapy.
on the
Interpersonal
Communicatio
n Inventory)
than did the verbal
treatment (+1, 3).
Activity treatment
produced non-
significantly higher
increments in skills than
did the control condition
(+0,8)
Hachey&
Mercier
(1993)
The
contribution
of rehab to
quality of life
in psychiatric
patients
Addition of
occupation
Longitudinal
N=152
Positive but modest
relationship between
occupation and quality
of life and self perceived
health not affected by
use of rehabilitation
services
Larson
(1990)
To determine
activity
patterns for 1
week and 1
month before
hospitalisat-
ion and life
changes for
the past year
Withdrawal of
occupation
Longitudinal
N=15
Because of the
small sample
size, the study
conclusion
may not be
generalisable
Activity changes were
highly correlated with
depression. As activity
changes increase,
personal care decrease
and passive recreation
increases. As financial
stress increase,
personal care increases.
As home and family
stress increases
personal care
decreases.
Mac-
Donald et
al.
(1987)
To examine
the
depression
and activity
patterns of
persons with
Withdrawal of
occupation
Cross-
sectional
N=53
Reliable and
valid
measures
used. Because
of the cross-
sectional
Severity of injury was
associated with
increased risk of
depression and
decreased activity.
Individuals with

131
spinal cord
injury in the
community
design, it is not
possible to
know if
depression led
to decreased
activity or if
decreased
activity led to
depression.
Longitudinal
studies are
needed.
depression reported
engaging in less
personal activities.
9. CONCLUSION
It is found that major depressive disorders decrease a client’s functioning in all occupational
performance areas. Therefore occupational therapists have a unique role to play during the
treatment in the acute, chronic and intermittent phases of all major depressive disorder
patients.
A good deal of theoretical and empirical work supports the notion that occupational
engagement is associated with a reduction of symptoms in major depression patients.
Because of its explicit focus on roles, behaviours and adaptive skills, occupational therapy
can play a key role in the treatment of major depression.
The advantage of occupational therapy is that it is a client-centered practice since the client
and the occupational therapist work together as mutual partners in order to find the best
solution for the client.
It will be inappropriate for the client to be treated without the involvement of the occupational
therapist, due to their unique contribution to their well-being and health.

132
10. REFERENCES:
1. Trombly CA. Historical and Social Foundation for practice. Occupational Therapy for
physical dysfunction 4th ed. 3-13
2. Kaplan, HI; Sadock BJ & Grebb, JA. “Kaplan and Sadock’s synopsis of psychiatry”. 7th
ed. Williams & Wilkins. Baltimore. 1994.
3. Crouch R; Alers V. Occupational Therapy in psychiatry and mental health. 4th Ed
4. Crouch R; Alers V. Occupational Therapy in psychiatry and mental health. 3rd Ed
5. Larson KB. Activity patterns and life changes in people with depression. American
Journal of Occupational Therapy. OCT 1990, Vol 44 number 10.
6. Cracknell E.A small achievable Task. British Journal of Occupational Therapy. Aug
1995, 58 (8). 343-344.
7. Devereaux E, Carlson M. The Role of Occupational Therapy in the management of
depression. American Journal of Occupational Therapy. Feb 1992, Volume 46 number
2.175-905.
8. Creek J. The knowledge base of Occupational Therapy. Occupational Therapy and
mental health. 3rd Ed. 29-49.
9. Brollier C, Hamrick N, Jacobson B. Arobic exercises: A potential Occupational
Therapy Modality for Adolescents with depression. Occupational Therapy in mental
Health. Vol 12(4) 1994 19-27
10. Crouch R. A study of the effectiveness of certain occupational therapeutic group
techniques in the assessment of acutely disturbed adult psychiatric patients. 1983.
Masters thesis: University of Witwatersrand.

133
11. Kopecki. AAOHN Journal. 1986. 34 (7)’ 315-322.
12. Kuenstler G.A planning group for psychiatric outpatient. AJOT. 1976. 30(10)
13. Crouch R.B. The evaluation and development of a tool for community-based stress
management. 2002-Doctoral thesis. Medical University of South Africa.
14. Mancusso LL. Reasonable accommodations for workers with psychiatric disabilities.
Psychosocial rehabilitation Journal.1990. 14(2): 3-19.
15. Code of Good Practice on key aspects of the employment of people with disabilities
(this code is attached to the employment equity act (Act no 55 of 1998 of South Africa)
www.labour.gov.za/docs/legislation/eea/codegoodpractice.htm
16. Casteleijn.J. The Measurement of Properties of an instrument to assess the level of
creative participation. 2001. Masters thesis-University of Pretoria.
17. Stuart J; Rupke MD; Blecke D. Cognitive Therapy for depression. Journal of American
family Physicians. Jan 2006.
18. Rosebaun JF; Fredman SJ. Clinical Update on the treatment of depression.
www.medscape.com/view article 441270-441275
19. Cluster V.L; Wassink K.E. Occupational therapy intervention for an adult with
depression and suicidal tendencies. American Journal of Occupational therapy Sept
1991.45(9): 845-8
20. Fouche L. Occupational Therapy in the community. Masters in psychiatry assignment.
Unpublished material. University of Pretoria.
21. Alers V; Smits B. The development and evaluation of an experiential approach to
teaching occupational therapy group work. South African Journal of Occupational
Therapy 2002:32(3).

134
22. Finlay L. The practice of psychosocial occupational therapy.2nd Ed. United Kingdom
1997.
23. Harding C. Some things we’ve learned about vocational rehabilitation of the seriously
and persistently mentally ill.
www.akmhcweb.org/ncarticles/vocational%2520 Rehab.htm.1997.
24. Corey Ms; Corey G. Groups. Process and Practice.5th Ed. New York: Brooks/Cole
Publishing Company.1997.
25. Jacobs K. Work assessment and programming. In HL Hopkins and HD Smith (Ed).
Willard and Spackmans Occupational Therapy. Philadelphia. J.B Lippincott Company,
1993, pp.226-248.
26. Yalom ID; The theory and practice of Group psychotherapy 4th Ed 1985.
27. Cara, E. Mood disorders. In Case. In Cara E. & MacRae, A (Eds.) Psychosocial
Occupational Therapy: A Clinical Practice, 1998 pp: 285-311. Albany, NY: Delmar
Publisher
28. Cooper, N. Case management. In Cara, E & MacRae, A. (Eds) Psychosocial
Occupational Therapy: A Clinical Practice 1998, pp.577-606. Albany, NY: Delmar
Publisher.
29. Macrae, A. Occupational therapy models. In Cara, E. & Macrae, A. (Eds)
Psychosocial Occupational Therapy: A Clinical Practice, 1998, pp.97-136. Albany, NY:
Delamar Publisher.
30. Van Greunen, A. “Occupational therapy with mood disorders”. Chapter 15. Edited by
Crouch, RB & Alers, VM. “Occupational therapy in psychiatry and mental health”. 3rd
ed. Maskew Miller Longman. Cape Town. 1997.

135
31. Kusznir, A; Scott, ; Cooke, RG & Young, LT. “Functional consequences of Bipolar
Affective Disorder: An Occupational therapy perceptive”. Canadian Journal of
Occupational Therapy. Vol 63 (5).
Pp 313-322. December. 1996.
32. Gallagher MR; Cariati S. The pain-depression conundrum: Bridging the body and
Mind. www.medscape.com.
33. Franklin D. Cognitive therapy for depression.
34. Westermeyer R.W. The cognitive model of depression.
35. Pollock R; Korn M. Depression; Approaches to brain and body.
36. Blatner A. Foundatons of psychodrama. Therapy and practice.3rd Ed. New York:
Springer Publishing Co: 1992.
37. Checkly S. The management of depression. Oxford: Blackwell Science Ltd. 1998.
38. Shrey DE; Larcate M. (Eds). Principle and Practice of Disability management in
industry. 1997. pp.627/55-105 Winter Park; FL: Gr Press Inc.
39. Szabo CP. Adolescent depression; continuing medical education Journal.
1995.13(11): 1329-1333.
40. Tsang H; Lam P; Leung O. Predictors of employment outcome for people with
psychiatric disabilities: A review of literature since mid 80’s; Journal of rehabilitation.
2000.66(2)’19-31.
41. Katz, R, B.F, Vallis, T.M, & Kalser, A.S. The assessment of severity and symptom
patterns in depression. In Beckham, E.E. & Leber, W.R. (Eds) Handbook of
Depression (2nd ed.), 1995, pp.61-85.New York: The Gullford Press.

136
OBSESSIVE COMPULSIVE DISORDER
Compiled by Rosemary B Crouch PhD Occupational Therapy (MEDUNSA)
1. INTRODUCTION
Occupational therapists have for many years treated clients with anxiety disorders and obsessive-
compulsive disorders in South Africa. Unfortunately very little is documented.
Undergraduate training in all 8 Universities in South Africa teach about the illness of obsessive-
compulsive disorder (OCD) and the handling principles of a person with this disorder. However most
of the focus is on anxiety disorders as such.
The main objective of occupational therapy is towards helping the client with OCD to perform in, and
adapt to his/her environment. Since this disorder is extremely debilitating in terms of participating in
the major spheres of life, intervention is aimed at restoring functioning, or at least coming to terms
with the disability, so that the person may live a purposeful and meaningful life, despite the disability.
‘Functioning’ from an occupational therapy perspective is much broader than the absence of
symptoms. Optimal functioning is linked to well-being, quality of life and the person’s self-efficacy
and mastery in choosing, organizing and performing those occupations he or she finds useful and
meaningful in various living environments. Occupational therapists are concerned with encouraging
and enabling the person to live life fully by also addressing issues such as inclusion, reasonable
accommodations and equal opportunities in the contexts where they live, work and play, despite the
presence of some residual symptoms of the illness¹.
2. DIAGNOSES
Obsessive Compulsive Disorder, treated by an occupational therapist is usually under the following
categories of the ICD-10 and DSM. IV:
ICD-10 F42.9
F41.9
F41.8
F41.3
F60.6

137
DSM. IV 301.40 Obsessive Compulsive Personality Disorder
300.30 Obsessive Compulsive Disorder
300.00 Generalised Anxiety Disorder
3. IMPACT ON OCCUPATION
3.1 Work
Work is one of the areas of life that is most disrupted with the illness of OCD. Poor concentration and
the need to engage in compulsive, repetitive behaviours may significantly hamper work performance².
Most clients with mild symptoms maintain their work, but the number of hours they work is severely
disrupted as are relationships in the work-place and actual work ability. Time management is often a
serious problem. The OCD client has rituals to perform before actually arriving at work and is often
late.
3.2 Activities of Daily Living
Often the personal presentation of the client with OCD is poor and such aspects as personal hygiene
need to be addressed by the occupational therapist. Obsession with certain aspects of cleanliness, such
a washing hands, often brings about the neglect of other parts of the body such as the hair and feet.
The ability to attend to personal hygiene, eat, dress, perform household chores, manage money and
use the telephone is often compromised².
3.3 Leisure and social
Participation in social activities is often greatly reduced in the client with OCD and leisure pursuits
may be solitary and confining. Social relationships frequently suffer due to the overriding focus on the
completion of rituals².

138
4. IMPACT ON ROLES, HABITS AND ROUTINES
OCD is known as a sensory processing disorder. In other words the person struggles to form meaning
responses to sensory stimuli. As a result these individuals often exhibit problems with coordination,
sensory-seeking or sensory-avoiding behaviours and sensory modulation3. The disorder is also
characterized by distressing, intrusive thoughts and repetitive actions that interfere with the
individual’s daily functioning, normal routine, occupational or academic functioning and usual social
activities and relationship4.
5. HEALTH CARE STRUCTURES
Patients with OCD are usually first seen by the occupational therapist during initial hospitalisation
where there is a curative/remedial approach. Rehabilitation in a community-based setting or private
practice then takes place.
6. ASSESSMENT
6.1 Baseline Assessments
• Interview with client and significant others.
• Clinical Observation takes place continually.
• Evaluation takes place by both standardised and non-standardised tests.
Standardised tests include:
o Crouch Stress Assessment 2003¹
o Hospital Anxiety and Depression Scale
o The Canadian Occupational Performance Measure (COPM)
o Occupational Performance History Interview5
o Battery of Anxiety Questionnaires.
• Collateral information is often required form significant others.
• Assessment reports are furnished to the referral agent.

139
6.2. Ongoing Assessment
Ongoing assessment takes place throughout treatment and a final assessment on discharge when the
patient’s progress can be discussed and planning for the future takes place.
7. INTERVENTION
7.1 The Role of the Occupational therapist
Occupational therapists, throughout the world, are trained in the assessment and treatment of
obsessive-compulsive disorder, helping identify how major disruptions in habituation and volition can
affect a person’s ability to perform and adapt to everyday life6. A purposeful and meaningful
treatment plan is required containing the following aspects:
7.1.1 Work
Vocational rehabilitation is often necessary for the client with OCD and often reasonable
accommodation has to be discussed by the occupational therapist with the employer7.
7.1.2 ADL (Activities of Daily Living)
Personal hygiene has to be addressed very sensitively by the occupational therapist and individual
treatment is often required. Factors which must be addressed by the occupational therapist are
home management, including visits to the home and related issues such as child and adolescent
management are also important.
7.1.3. Social Participation and Leisure
OCD as an illness is based upon high levels of anxiety and one of the most important aims of
treatment in occupational therapy is to assist the client with a balance of activities that will release
stress and anxiety. Activities such as playing bridge, joining a book club or cinema club or learning
a new skill in a small group should be encouraged. Constructive use of leisure time often cuts down
OCD behaviour and rituals. Treatment can either be in a group or individually.

140
7.2 Theoretical Framework
7.2.1 Models
The Model of Human Occupation5 is often used as a frame of reference in the assessment and
treatment of obsessive-compulsive disorder. Careful application of this model promotes a more
holistic view of intervention by the occupational therapist.
7.2.2 Frame of Reference/Approaches
THE SENSORY-BASED TREATMENT APPROACH
The concept of sensory processing disorders comes from the work of occupational therapist
Jean Ayres, Ph.D (1983). Her work has launched a sensory-based treatment approach,
primarily practiced by occupational therapists3. The efficacy of treatment has been highly
researched. “It is a fact that pathology can interfere with the process of integrating sensory
information. If sensory information cannot be integrated or is integrated in a dysfunctional
way, it will contribute to the individual makes sense of their world and this could often be
disorganizing”8. An example is the person who is continually washing their hands, who is
receiving much tactile sensory stimulation and is obsessed with it, will shut out most other
sensory information such as sound.
7.3. Treatment Programmes
7.3.1 Occupational Group Therapy and Stress Management.
The use of group-work in occupational therapy has always been an integral part of intervention,
particularly in the psychiatric field, and constitutes a major part of any programme.
Occupational therapists in South Africa are highly trained in group-work and in stress
management (stress management does not have to take place in a group but is more effective in
this way).The teaching of relaxation is essential and how to cope with stress generally. In South
Africa occupational therapists are expert in the techniques of stress management and have a very
holistic approach. Research undertaken by Crouch (occupational therapist) in 2002 shows a
significant difference in the levels of stress of participants in stress management programmes
carried in the community in South Africa.

141
Groups for clients with OCD are extremely important and allow the client to share with other
people who have the same or similar problem. Groups focused on life skills and coping skills
are very important and support groups where four or more clients can safely discuss their
problems and let go of anxieties are very important. A number of excellent support groups are
also available in the community for clients with OCD and they should be encouraged to attend.
7.3.2 Sensory Integrative Therapy
Occupational therapist train at a post-graduate level in sensory integrative therapy and have to
be qualified to use these therapies. Therapy is carried out by diminishing the OCD behaviour by
providing the person with a sensory “diet” that will provide the sensory stimulation the client
requires. Activities will be used that are in keeping with the age and sex of the individual and
may include the use of the therapy ball, the trampoline, scooter boards, sport and swinging
activities.
7.3.3 Constructive Use of Leisure Time
As previously stated, the involvement of patients in a balanced programme which includes
constructive use of leisure time is essential. Exercising regularly, joining intellectual and support
groups and learning new skills such as computer skills, pottery and ceramics
7.4 Time Span
NUMBER OF OCCUPATIONAL THERAPY SESSIONS.
• Acute Phase:
1 x session of comprehensive assessment
1 x collateral information or consultation
2 x individual treatment
5 x occupational group therapy
2 x follow up

142
• Chronic Phase:
Patients in the chronic phase require long-term intervention. A patient may be part of
occupational group therapy for as long as a year, once a week.
1 x session of comprehensive assessment
1 x collateral information or consultation
2 x programming for daily activities
50 x occupational group therapy
1 x session reassessment
8. TABLE OF EVIDENCE
Author Study
population
Type of
design
Treatment
group
Outcome
variable
Findings
Crouch,R.B. 160 random
rural pop.
Quantitative
experimental
Impoverished
low soc/eco.
Alleviation
of stress
Significant
alleviation
of stress
9. CONCLUSION
Anxiety disorders appear to becoming more frequent amongst a broader South African population.
The profession of occupational therapy is in the process of addressing the need to become more
involved in the treatment of anxiety disorders generally and to produce more evidence in respect to
the success of treatment in this area
10. REFERENCES
1. Crouch, R.B. The Evaluation and Development of a tool for Community-based Stress
Management. Ph.D Thesis Medical University of South Africa (MEDUNSA) (2002)
2. Calvoconess, L., Libman, D., Vegso, S., McDougal, C. & Price, L. Global functioning of inpatients
with obsessive compulsive disorder, schizophrenia and major depression. Psychiatric Services 49:
379-38 March 1998. Arlington: American Psychiatric Publishing Inc. (1998)

143
3. Reisman, J. Sensory Processing Disorders. Minnesota Medicine. 85 (11): 48-51, Nov. (2002)
4. American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders. 4th
Edition. (DSM IV) Washington: American psychiatric Association. (2000)
5. Kielhofner,G. Model of Human Occupation. 3rd Edition. Baltimore: Lippincott Williams and
Wilkins. (2002)
6. Bavaro, S. M. Occupational Therapy and Obsessive-compulsive Disorder. American Journal of
Occupational Therapy 45 (5): 456-8, May. (1991)
7. Strong, S. Meaningful work in supportive environments: experiences with the recovery process.
American Journal of Occupational Therapy, 52, 31-38. (1998).
8. Crouch, R., & Alers, V. Eds. Occupational therapy in psychiatry and mental health. 4th ed. London
& Philadelphia: Whurr Publishers(2005)
9. Creek,J. Occupational Therapy and mental health. London: Churchill Livingstone. (2002)
10. Kaplan, H. I., & Sadock, B. J. Comprehensive textbook of psychiatry. 7th Ed. Philadelphia:
Lippincott Williams & Wilkins. (2000)

144
POST TRAUMATIC STRESS DISORDER (PTSD)
Compiled by Vivyan Alers (B.A. Social Work, M.Sc. Occupational Therapy)
10. INTRODUCTION
Post Traumatic Stress Disorder (PTSD) is a psychiatric disorder that can occur after the
experiencing or witnessing of life-threatening events which causes people to relive the
experience through nightmares and flashbacks, insomnia, detachment and impairment of
daily life.
The occupational therapist has an important role to play to get the trauma survivor to resume
their normal lifestyle again. The occupational therapist can make a profound impression on
the emotional, practical and functional aspects that are emphasized within the roles taken on
by the trauma survivor. PTSD can be complicated with other related disorders involving
depression, substance abuse, memory and cognition problems and physical and mental
health problems. There are clear biological changes and psychological symptoms which are
associated with the impairment of functioning in social and family life, occupational instability,
marital problems, divorce, family discord, difficulty in parenting. The effects of PTSD may be
pervasive and encompass the whole being of the person’s life which may immobilize them to
varying degrees. The effects of PTSD are long term and recurrent relapses may occur.
The potential contribution of Action Methods (sociometry and psychodrama) for addressing
healing the trauma and pain of victims and perpetrators of domestic violence is largely
untapped. “Psychodrama has been less used within the field of traumatic stress than other
therapeutic approaches”7. Many symptoms of Posttraumatic Stress Disorder (PTSD) “…
are unconscious, non-verbal, right-brained experiences that cannot in fact be accessed
through talk therapy”7. Psychodrama can be used “as a powerful method of restraint and
reintegration” as well as “expression and catharsis” 7. It can serve to address the very
symptoms of PTSD, to facilitate developmental repair, to provide structures for safe re-
enactment of the horror of core trauma scenes, and to promote control, containment, and
stability.

145
Referrals may come from a variety of sources, namely medical practitioners,
physiotherapists, work employers, teachers, parents, colleagues of the trauma survivor,
family members, community members, religious counsellors or the trauma survivors
themselves seeking help.
For the purposes of this document PTSD will be mainly described.
11. DIAGNOSIS
The diagnosis according to ICD – 101, 2 relevant to occupational therapy are the following as
they are all related to a perceived stressor / trauma.
F43 Acute stress reaction
F43.1 PTSD
F43.2 Adjustment disorders
F43.8 Other reactions to severe stress
F43.9 Reaction to severs stress unspecified
F93 Separation anxiety disorder of children
F93.1 Phobic anxiety disorder of children
F93.2 Social anxiety disorder of childhood
F94 Elective mutism
F94.1 Reactive attachment disorder of childhood
F94.2 Disinhibited attachment disorder of childhood
F94.8 Other childhood disorders of social functioning
The symptoms of PTSD according to the DSM IV3 fall into 4 categories;
A Person is exposed to a traumatic event , experienced, witnessed or confronted with an
event/s involving threatened death or serious injury, or threat to physical integrity of self

146
or others. Person’s response involved intense fear, helplessness, or horror. [In children
disorganised or agitated behaviour]
B The traumatic event is persistently re-experienced with intrusive distressing recollections
and recurrent distressing dreams. There is acting/feeling that traumatic event was
recurring with intense psychological distress to internal or external cues. There is
physiological reactivity on exposure
C Persistent avoidance of the stimuli associated with trauma [minimum 3 of the following]
Avoid thoughts feeling, conversations, Avoid activities, places or people, Inability to recall
important aspects of trauma, Diminished interest and participation, Detachment /
estrangement feeling, Restricted range of affect, Sense of foreshortened future
D Persistent symptoms of increased arousal with difficulty falling/staying asleep,
Irritability / anger, difficulty concentrating, hyper vigilance and an exaggerated startle
response
With all the above symptoms the duration of disturbance >1 month and the disturbance
causes clinically significant distress / impairment in social /occupational functioning.
12. IMPACT ON OCCUPATION PTSD has a pervasive effect on all the areas of functioning.
3.1 Work The impairment in the vocational environment may be clearly marked with a lack of
concentration, inability to focus on the tasks needed, inability to set and attain goals, a
decrease in accomplishments, a decrease in the quality of tasks done and a general
decrease in performance. Absenteeism is common, and the person becomes disorganised,
unpredictable and labile in the work setting. There is often an inconsistent employment

147
history, poor interpersonal relationships, and possible drug / alcohol abuse. Executive skills
become incapacitated.
With children in the school environment there is a lack of concentration, possible attention
deficit disorder symptoms, psychosomatic disorders, withdrawal and a decrease in academic
performance.
3.2 Activities of Daily Living Hygiene aspects do not carry the same importance as before, and the client shows a
decrease in their personal care of themselves. The inability to care for others makes
parenting a problem, relationships within the family deteriorate, and irritation, depression or /
and anxiety may be shown. Children may be disorganized in all their activities of daily life
and show an irritable attitude.
3.3 Leisure There is a definite decrease in the leisure pursuits of a trauma survivor as they may withdraw
or their concentration is not long enough to pursue a hobby. Sometimes they may immerse
themselves in work and totally forget about their leisure time.
Children withdraw from active play and seek passive play.
3.4 SOCIAL There is a definite decline in their interpersonal relationships within the family and within their
social environment. Withdrawal from social activities is common.
13. IMPACT ON ROLES, HABITS AND ROUTINES Trauma challenges a person’s belief in their safety, attachment, trust / betrayal, lifestyle,
sense of belonging and ego states. This is not a transient state of unbalance, as it can have
lasting emotional effects on a person, especially when experienced during childhood. In the
latter case there are often resultant interpersonal effects in adult life. The negative effects of

148
trauma can reoccur when triggered by a situation or flashback. This may happen years after
the incident. The more complex the trauma, and the repetition of trauma, can add to the
severity of the distress.
The occupational therapist needs to address all the roles and routines that were present and
fulfilled before the traumatic incident and slowly facilitate the person to return to these roles
and to become a member of the society again. Their beliefs and values need to be
addressed and normalized and social norms need to be encouraged.
14. HEALTH CARE STRUCTURES
5.1 Pillars of Health Care Preventative /promotive
Psycho-education is an important aspect in prevention. This is especially needed to prevent
further/repeated trauma, and risky behaviour.
Curative /remedial
Occupational therapy will be involved when children’s/ students academic performance
deteriorates to enhance their abilities and apply themselves to foster achievement.
Rehabilitative
This is the biggest role of the occupational therapist to help the client to return to normal life
and to be able to resume their roles, beliefs and routines. Safety and containment of
emotions and behaviour is important together with the expression of emotions and the
participation of meaningful tasks within their home and work contexts. Rehabilitation needs
to address the self, the environment, the context and the spirituality or meaning in life.
Maintenance
The occupational therapist puts structures and support systems in place that assist the client
to maintain their mental health. Relapse or flashbacks often occur and the client needs to
have practical and supportive ways to cope. The holistic philosophy of occupational therapy

149
addresses the personal, interpersonal and transpersonal (spiritual) aspects of a client’s life in
terms of maintenance.
5.2 Level of Health Care System
Occupational therapists can be involved with clients within the primary, secondary and
tertiary levels of the health care system.
Primary level – groups within the communities addressing prevention and promotion of
mental health. These would be psycho-education groups related to the formation of support
groups and lifestyle groups. These would be community based groups on an ongoing basis
as slow-open groups. Groups addressing the secondary traumatic stress factors for the
family members are also included here.
Secondary – these groups and individual treatment may be in the community, hospital or
practice rooms. These groups would be slow- open groups or closed groups depending on
the trauma survivors / clients. These groups may vary in length of time for each session from
2 hours to workshops that could be 1 or 2 days. Treatment also involves other family
members that need to be the support system for the trauma survivor.
Tertiary - these groups and individual treatment may be in the hospital or practice rooms.
These groups would be slow- open groups or closed groups depending on the trauma
survivors / clients. These groups may vary in length of time for each session from 2 hours to
workshops that could be 1 or 2 days. Treatment also involves other family members that
need to be the support system for the trauma survivor.
15. ASSESSMENT
6.1 Baseline Assessments The initial assessment is necessary to ascertain the previous and present functioning of the
client. This needs to be documented and may be used later in comparison when relapses
occur.

150
6.1.1 Professional interview
The professional interview is necessary to obtain background information, precipitating
and predisposing factors. During this interview time is needed to develop a rapport with
the client to build trust, confidentiality, and a contained arena to be able to discuss
emotional issues. This includes a narrative of the client’s life with any significant
occurrences during their life, and ascertaining whether the client has been a victim, a
perpetrator or both. It is also important to asses the client’s perception of how the
traumatic event has affected their functioning in all the spheres of daily living.
6.1.2 Clinical observation
Clinical observations relate to the nuances and body language, together of what is said
and omitted, especially regarding the incident / traumatic event. The attachment pattern
of children to their carers is also needed to be observed.
6.1.3 Evaluation
The evaluation includes the clinical reasoning of the therapist pertaining to narrative,
conditional, pragmatic, interactive, procedural, ethical, intuitive reasoning.
6.1.4 Collateral information
This is of utmost importance as often exaggeration, misconceptions or omissions are
portrayed in the client’s story due to their stress levels being high. The family and other
professionals need to be contacted and sometimes this may involve the justice system if
there is a statement necessary.
6.1.5 Assessment report
There are some ethical considerations to be noted when compiling the reports. Due to
the stigma attached to traumatic events (e.g. Rape, diagnosis of HIV, being a perpetrator
and then a victim) the assessment report needs to be formulated and the disclosure of
this report to other professionals needs to be discussed with the client. There is also an
ethical dilemma of whether the assessment is reliable after only one session, due to
omissions or misconceptions.

151
6.2 Ongoing Assessment The occupational therapist would monitor the frequency and consistency of symptoms and
level of motivation. Ongoing assessment is of utmost importance especially in the light of
malingering to claim from insurance policies. Ongoing assessment is also imperative as
PTSD is a long term illness and has an impact on all the spheres of daily life.
16. INTERVENTION
7.1 Role of O.T:
7.1.1 Work
The executive functions at work, motivation and productivity are key aspects addressed
by the occupational therapist. Coping skills, time management skills and stress
management / life skills are part of the role of the occupational therapist in the treatment
of PTSD.
The self esteem and self confidence together with meaning attribution in the workplace is
the aim of treatment. The outcome of this process is reduced absenteeism, improved
productivity due to the client feeling competent and confident in the workplace, together
with an improved motivation.
7.1.2 Activities of Daily Living
The occupational therapist addresses all the activities of daily living namely personal care
and personal presentation, management in the home including the executive functions to
assist the client to return back to their previous functioning and make their life
meaningful.
The self esteem and self confidence together with meaning attribution in the home is the
aim of treatment. When the home and personal environment is organised then the client
will feel more in control of their life and thus be able to maintain this control and be
motivated to be productive and return to work.

152
7.1.3 Leisure
The occupational therapist is able to assess and facilitate the client’s engagement in
meaningful leisure time pursuits.
Leisure time pursuits give meaning to the client’s life and assist to balance the stress
factors from the other spheres of life.
7.1.4 Social
Occupational group therapy is the best intervention addressing the social sphere for
PTSD as it addresses support systems, interpersonal relationships and socially
acceptable behaviour. The group dynamics and the occupational group therapy
techniques of action methods engage the client and encourage spontaneity and
involvement in the healing process.
The outcome of this process is that the client will re enter into meaningful relationships
which will in turn improve self esteem and self confidence and this has a motivating effect
which will improve productivity in the home and work environment.
7.2 Theoretical Framework
7.2.1 Models
The Therapeutic Spiral Model has shown to be an effective technique for children, youth
and adults, with histories of trauma because it specifically addresses self-growth,
containment, safety and conscious transformation in a therapeutic individual or group
setting4.
The Sinani / Kwazulu-Natal Programme for survival of Violence Model shows the cycle of
violence and the cycle of peace5.
The Trauma Debriefing Model / 4 leg Model can be used for debriefing. This includes
retelling the story, normalizing the symptoms, reframing and encouraging mastery6.
Vona du Toit Model of Creative Ability applied to Paediatrics6.

153
7.2.2 Frame of References / Approach
The different phases of trauma need to guide the treatment approach. The occupational
therapist may be involved in all the phases (impact phase, recoil phase, reorganisation /
recovery phase) and needs to know what the client’s needs are in each phase.
“Cognitive behavioural therapy has long proved useful in managing the disruptive
symptoms of PTSD, but it does not directly treat the core trauma that causes these very
symptoms “.4 Success within the cognitive-behavioural and psychodynamic approaches
depends on the following: individuality and personality, other past trauma or the build up
of trauma and its cumulative effect, the reliability of the support systems and the phase of
recovery.
“As an experiential method, the Therapeutic Spiral Model increases treatment
effectiveness while decreasing treatment time with PTSD. “Practitioners discover
techniques to provide containment and safety with action methods in educational,
community or therapeutic settings“4.
7.3 Treatment Programs The occupational therapy goal is to attain maximal functional independence and the
prerequisites for this are the following: good support systems, understanding of symptoms,
stress management, stay away from drugs and alcohol and a balanced lifestyle routine.
Sinani believes that a partnership with a community affected by violence should not be a
short term project, unless there is a very specific request. But usually the relationship with
any one partner community lasts for 3-5 years5.
Programmes for secondary traumatisation of the family (including the parents, spouse and
children) are also necessary.
Psychodrama has been developed further by Dr Hudgins to treat trauma survivors. The
Therapeutic Spiral Model ™ constitutes a treatment of choice for adults and youth at risk,
with histories of trauma because it specifically addresses self growth, containment, safety

154
and conscious transformation in a therapeutic group setting4. The model has proven to be
cross cultural. The Therapeutic Spiral Model™ is a clinically driven, structured system of
psychodrama for working with trauma survivors. This model was created specifically to
prevent the uncontrolled regression that has the potential to re-traumatize clients when
experiential methods are used without an integrated clinical framework. The constructs and
methods have been validated by self-report, therapist interviews, and current single case
research. The goal of The Therapeutic Spiral is to facilitate developmental repair at all levels
of healthy functioning. Occupational therapists need specific post graduate training in the
Therapeutic Spiral Model ™ or psychodrama techniques.
Occupational group therapy workshops using the Therapeutic Spiral Model™ over weekend
time is an effective program to address the complete program over this time which effectively
enables the client to process and use the constructs demonstrated in a safe and contained
environment. This intensive therapeutic time is effective in breaking the cycle of violence to
create healing and subsequent treatment sessions are shorter.
7.4 TIME-SPAN
“Working with traumatised people requires a sensitive touch, the right timing and the use of a
variety of effective techniques. …The length of time given for the session is another
important issue. A session that deals with trauma should not be abruptly ended because of
rigid rules of time, such as the exact “therapist hour”7
7.4.1 Acute
Psycho-educational approach [Debriefing] 6 – 8 sessions of 2 hours each
7.4.2 Chronic
Cognitive –Behavioural approach long term – 20 sessions of 2 hours each
Psychodynamic approach long term – 20 sessions of 2 hours each
Occupational group therapy long term – 20 sessions of 2 hours each

155
Occupational group therapy workshop 2 days of 8 hours at a time, preferably over a
weekend.
Secondary traumatisation programmes 4 sessions of 1 hour each
17. TABLE OF THE EVIDENCE Many medical studies (anatomical and drug related) have been carried out with PTSD but
very few empirical studies have been done in experiential action methods or occupational
group therapy. Bessel van der Kolk (Harvard University) is the leader in the development of
treatment for PTSD. (See bibliography)
Author Study population
Type of design
Treatment group
Outcome variable
Findings
Hudgins K. M.
Drucker K. Metcalf
K. The “containing
double”: A clinically
effective
psychodrama
intervention for
PTSD. British
Journal of
Psychodrama and
Sociometry. 20009
.
1 client
diagnosed
with PTSD
(complex
trauma)
experiencing
a block in
long term
psychothera
py
Single
case
subject
design
3 treatment
sessions of
psychodrama
using the
containing
double from
the
Therapeutic
Spiral Model
Use of the
containing
double in
social setting
outside
therapy.
Decrease of
dissociation
and other
trauma
symptoms.
Significant change in the
Dissociation Experience
Scale after 1 session.
Analyses of PTSD
symptoms were
significantly improved at
follow up time compared
to baseline
assessments.
Discussion: Client
attended a weekend
workshop on “Surviving
Spirits”
before
agreeing to participate in
the research.

156
Wright D. C.
Woo W. L.
Muller R. T.
Fernandes C. B.
Kraftcheck E. R.
An investigation
of trauma-
centered
inpatient
treatment for
adult survivors of
abuse
Department of
Psychology, La
Marsh Centre for
Research on
Violence and
Conflict
Resolution, York
University,
Toronto, Ont.,
Canada. 2002 10
One
hundred and
thirty-two
individuals
admitted to a
PTSD
inpatient
treatment
program for
adult
survivors of
childhood
trauma
consented to
participate in
this study.
Inter-
vention
study
design,
Long-
itudinal
design
of the
study
shows
main-
tenance
of treat-
ment
gains at
1-year
post
treat-
ment.
This study
examined
whether a 6-
week
Comprehen-
sive inpatient
treatment
program can
reduce PTSD
symptoms
among adult
survivors of
child abuse.
Evaluation of
PTSD
symptom-
atology data
at admission
and
discharge
This study is
an empirical
investigation
that
quantitatively
examines
change in
symptoms
following
treatment
occurring in
a group
therapy
modality.
The question
of whether a
brief,
inpatient
group
program is
effective in
reducing
Evaluation of PTSD
symptomatology
data at
admission and
discharge:
Analyses of the CAPS-2
data
were conducted for both
the
frequency and intensity
of the
three PTSD symptom
clusters
(re-experiencing,
avoidance / numbing,
and increased
arousal) as
well as on the overall
PTSD symptoms. All
paired t-tests
with Bonferroni
corrections
were statistically
significant.

157
Carbonell D. M.
Parteleno-
Barehmi C.
Psychodrama
groups for girls
coping with
trauma.
International
Journal of Group
Psychotherapy.
49 (3) 1999. 11
Twenty-eight
cross
cultural
sixth-grade
girls.
Ages were
between 11
and 13
years.
26
completed
the study.
They
identified
traumatic life
events and
chronic
stress.
These
experiences
Inter-
vention
study
design.
The girls
were
randomly
assigned to
the
treatment
and control
conditions in
equal
proportions.
Because two
of the girls
left the
school during
the early
stages of the
intervention,
the two
treatment
groups had a
total of 12
PTSD
symptoms
in adult
survivors of
abuse and
examining
one year
post-
treatment
symptoms.
A qualitative
component
was included
to evaluate
the impact of
the
group on the
participants.
In addition to
notes kept
by the group
leader
through the
course of the
20 weeks,
and exit
interviews
were
conducted.
Significant differences
were found between the
treatment and control
groups in their change
from the pre-test to post-
test scores in two of the
eight Youth Self-Report
(YSR) subscales:
“Withdrawn” and
“Anxious / Depressed.”
Although no other
differences in pre- and
post-test subscale
scores reached
statistical significance,
the scores were
consistently indicative of
a trend toward greater
improvement among the
treatment group.
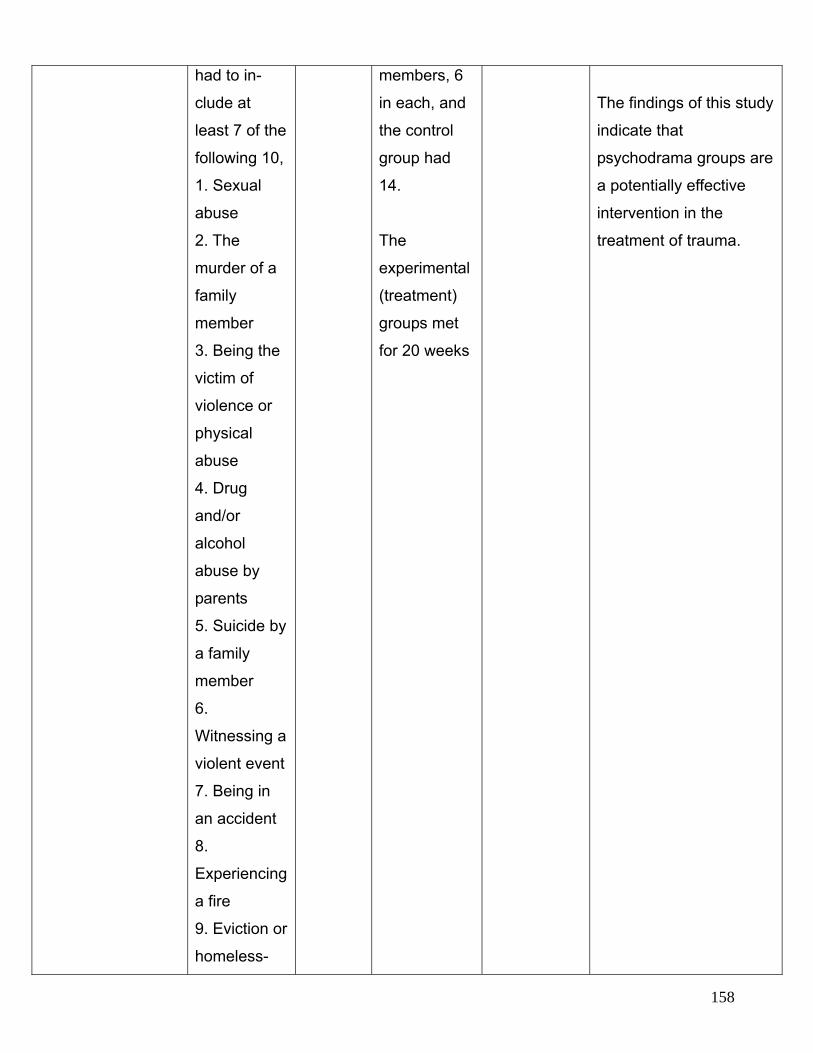
158
had to in-
clude at
least 7 of the
following 10,
1. Sexual
abuse
2. The
murder of a
family
member
3. Being the
victim of
violence or
physical
abuse
4. Drug
and/or
alcohol
abuse by
parents
5. Suicide by
a family
member
6.
Witnessing a
violent event
7. Being in
an accident
8.
Experiencing
a fire
9. Eviction or
homeless-
members, 6
in each, and
the control
group had
14.
The
experimental
(treatment)
groups met
for 20 weeks
The findings of this study
indicate that
psychodrama groups are
a potentially effective
intervention in the
treatment of trauma.

159
ness
10.
Immigration
under
hardship
conditions
(financial
and other)
18. CONCLUSION
Van der Kolk8 describes the value of experiential methods in the treatment of PTSD and
states that this is the ‘treatment of choice’ for people who have PTSD. From this premise,
occupational therapists have an invaluable contribution to make to the healing of trauma
survivors as their philosophy is holism and functionality. The occupational therapist is well
trained in individual and occupational group therapy at an undergraduate level, and other
projective techniques at a post graduate level (art therapy, psychodrama).
The impact of trauma on mental health is not to be underestimated. Many psychiatric
illnesses have a background of traumatic experiences which may influence resilience.
Resilience is dependant on personal, interpersonal and transpersonal (spiritual) strengths
and intrinsic meaning attribution of self.
Occupational therapists working in the trauma sector have described the Therapeutic Spiral
Model ™ as an invaluable tool to treat Post Traumatic Stress Disorder with individual and
occupational group therapy, and parts of the model are worthwhile in treating Compassion
Fatigue in healthcare workers4. The curative factors within the occupational group therapy
and the motivating factors within the psychodrama techniques give a unique treatment
modality for the treatment of PTSD.

160
19. REFERENCES
1. World Health Organisation, International statistical classification of diseases and
related health problems. 10th revision. Volume 1. W.H.O. Geneva. 1992.
2. World Health Organisation, International statistical classification of diseases and
related health problems.10th revision. Volume 3. W.H.O. Geneva.1994.
3. American Psychiatric Association. Diagnostic and statistical manual of mental
disorders. 4th ed. Washington, D.C.: The American Psychiatric Association. 1994.
4. Hudgins K.M. Experiential Treatment for P.T.S.D. The Therapeutic Spiral Model.
Springer Publishing Company. New York. 2002.
5. Sinani Kwazulu Natal Programmes for Survivors of Violence 2007 www.survivors.org (
cited 2007 February 22)
6. Crouch R. Alers V. eds. Occupational therapy in psychiatry and mental health. 4th ed.
London & Philadelphia: Whurr Publishers. 2005.
7. Kellerman P.F. Hudgins M. K. eds. Psychodrama with Trauma Survivors: Acting Out
Your Pain. London. Jessica Kingsley Publications. 2000.
8. van der Kolk B. The limits of talk therapy. Psychotherapy Networker. 2004
9. Hudgins K M. Drucker K. Metcalf K. The “containing double”: A clinically effective
psychodrama intervention for PTSD. British Journal of Psychodrama and Sociometry.
2000.
10. Wright D. C. Woo W. L. Muller R. T. Fernandes C. B. Kraftcheck E. R. An
investigation of trauma-centered inpatient treatment for adult survivors of abuse.
Department of Psychology, La Marsh Centre for Research on Violence and Conflict
Resolution. York University, Toronto, Ont., Canada. 2002.

161
11. Carbonell D. M. Parteleno-Barehmi C. Psychodrama groups for girls coping with
trauma. International Journal of Group Psychotherapy. 49 (3) 1999
BIBLIOGRAPHY
Kaplan H. I. Sadock B. J. Comprehensive textbook of psychiatry. 7th Ed. Philadelphia:
Lippincott Williams & Wilkins. 2000.
David Baldwin's Trauma Information Pages. Eugene, Oregon USA (cited 2007 February 25)
http://www.trauma-pages.com
Bannister A. Huntington B A. Communicating with children and adolescents. Action for
change. London. Jessica Kingsley Publishers. 2002.
Creek J. ed. Occupational therapy and mental health. 3rd Edition. Churchill Livingstone.
London 2002.
Hudnall – Stamm B. Secondary Traumatic Stress – Self Care Issues for Clinicians,
Researchers and Educators. Sidran Press. Maryland USA. 1999.
Lewis S. An adult’s guide to childhood trauma. Understanding traumatised children in South
Africa. David Philip. South Africa. 1999.
Wenar C. Cerig P. Developmental Psychopathology. From Infancy Through Adolescence.
McGraw-Hill companies Incorporated. International edition. 2000.
Western Cape Education Department. Abuse no more – Dealing effectively with child abuse.
WCED Western Cape, South Africa. 2000.
Hudgins M.K. Drucker K. The containing double as part of the Therapeutic Spiral Model for
treating trauma survivors. The International Journal of Action Methods 51, 2, 63-74. 1998

162
Hariri A.R. Bookheimer S.Y. Mazziotta J.C. Modulating emotional responses: Effects of a
neocortical network on the limbic system. Neuroreport 11:43-48. 2000.
Kipper D.A. Ritchie T.D. The effectiveness of psychodramatic techniques: A meta-analysis.
Group Dynamics 7:13-25. 2003
Teicher M.H. Scars that won't heal: The neurobiology of child abuse. Scientific American:68-
75. 2002.
van der Kolk B. McFarlane A. Weisaeth L. eds. Traumatic Stress. Guilford Press, New York.
1996.
van der Kolk B. Ogden P. et al. Movement and action in the transformation of trauma: The
role of somatic experience, purposeful action and theater in the treatment of trauma. Pre-
Conference Workshop at the annual Conference on Psychological Trauma, Boston, 29 May.
2003
Ogden P. Minton K. Pain C. Trauma and the body: A sensorimotor approach to
psychotherapy. W.W. Norton UK. 2006.

163
SCHIZOPHRENIA
Compiled by Rosemary B Crouch PhD Occupational Therapy (MEDUNSA)
1. INTRODUCTION Occupational therapists working in mental health care and rehabilitation have an important
task in supporting people with severe mental disorders such as schizophrenia, to as
satisfying a daily life as possible. The main focus of this support is the provision of
opportunities for meaningful daily occupations. Occupation in this sense denotes not only
work, but also leisure activities, household chores, and all kinds of “doing” people engage in.
It is widely recognized that people with severe mental disorders have a right to meaningful
daily occupations, and in some countries it is even stated in the legislation.
‘Functioning’ from an occupational therapy perspective is much broader than the absence of
symptoms. Optimal functioning is linked to well-being, quality of life and the person’s self-
efficacy and mastery in choosing, organising and performing those occupations he or she
finds useful and meaningful in various living environments. Occupational therapists are
concerned with encouraging and enabling the person to live life fully by also addressing
issues such as inclusion, reasonable accommodations and equal opportunities in the
contexts where they live, work and play, despite the presence of some residual symptoms of
the illness1.
Referrals to occupational therapists usually come from Psychiatrists and General
Practitioners, but also from Clinical and Educational Psychologists, Social Workers and very
occasionally Nurses. Referral is also by word of mouth.
2. DIAGNOSIS Schizophrenia treated by an occupational therapist is usually under the following categories
of the ICD-10:
• F 20
• F20.3

164
• F20.6
• F20.8
• F25.1
DSM.IV.:
• 295.1 Disorganised
• 295.3 Paranoid
• 295.9 Undifferentiated
• 295.6 Residual
3. IMPACT ON OCCUPATION 3.1 Work Most clients with schizophrenia wish to have a job, but very few have one. Having a job
brings a number of advantages, such as a better economic situation, more social contacts,
more structure to the day, and perceived better social status2.
3.2 Activities of Daily Living Often the personal presentation of the client with schizophrenia is poor and such as aspects
as personal hygiene, appropriate dress and self-awareness need to be addressed.
3.3 Leisure and social Meaningful and satisfying daily occupations are also associated with a richer social network,
with feelings of being in control of one’s own life situation, and with better self-esteem. Thus,
several links have been shown between meaningful occupations and positive and desired
aspects of people’s status. The direction of these relationships have not been solved,
however, and it might be that persons who perceive better well-being and quality of life have
more energy and motivation for participating in daily occupations and also tend to be more
satisfied with those occupations3.
165
4. IMPACT ON ROLES, HABITS AND ROUTINES Besides a hardship regarding meaningful daily occupations, people with severe mental
disorders have many other unmet needs. They often have poor life conditions, few and poor
social contacts, low self-esteem, and a bad quality of life. However, by addressing
meaningful daily occupations, some of these needs may be met as well.
5. HEALTH CARE STRUCTURES Patients with schizophrenia are usually seen initially by the occupational therapist in private
practice, on first admission or readmission to an acute clinic where there is a
curative/remedial approach. Rehabilitation and maintenance takes place after discharge and
this is where the occupational therapist has the prime responsibility and expertise.
Occupational therapists are involved in community-based projects for the treatment of the
person with schizophrenia and also in secondary and tertiary units.
6. ASSESSMENT 6.1 Baseline Assessments
6.1.1 Interview with client and care-givers, often separately.
6.1.2 Clinical observation takes place continually. Occupational therapists are experts in
clinical observations.
6.1.3. Evaluation takes place by both standardised and non-standardised tests.
Standardised tests include the Crouch Stress Assessment 2003, Hospital Anxiety and
Depression Scale (HADS1994), Canadian Occupational Performance Measure (COPM
1998)
6.1.4. Collateral information is essential from care-givers, child and adult-minders, nurses
and domestic staff, fellow health professional and sometimes teachers.

166
6.1.5. Assessment reports take time to be completed and are issued only to registered
healthcare professional unless otherwise requested by permission of the
parent/caregiver. (Ethical Rules HPCSA 2006).
6.2 Ongoing Assessment
There is often a slow recovery of the person with schizophrenia. Ongoing assessment is by
observation and formally at least once during the intervention, and on discharge.
7. INTERVENTION 7.1 The Role Of The Occupational Therapist Occupational therapists, throughout the world, are involved in the social support, prevention,
treatment and rehabilitation of the persons with schizophrenia at all levels of severity. The
intervention programmes may be implemented in psychiatric hospitals, life skills and day
centres, community clinics, in the home and in industry.
Intervention by occupational therapists is most effective as part of a multidisciplinary team
approach, but in developing countries where there is often a shortage of trained
professionals, occupational therapists are able, due to their versatile and intensive training in
the field of mental health, able to use those activities that are culturally accepted and
available in most occupations, in most conditions.
Early intervention and effective treatment of acute episodes of schizophrenia, with the
specific alleviation of symptoms, are very important for minimizing long-term disability. Short-
term or extended treatment programmes are focused on evaluating strengths, weaknesses,
skills and impairments at this early stage4.
The literature indicates that most occupational therapists base their intervention on the
following aspects of treatment:

167
7.1.1 Work
Open-market jobs and job-like daily occupations are an important target for occupational
therapists who work with people with schizophrenia. Often reasonable accommodation
has to be discussed with the occupational therapist and the employer. This makes work
rehabilitation an important area, including sheltered workshops and different types of job
training programmes.
Oka,M, Otsuka,K, et.al. in 2004 describe an excellent vocational rehabilitation
programme with 52 clients with schizophrenia which was followed up after 17 years in a
retrospective study5. The length of time spent out of hospital, social functioning improved
and the risk of hospitalisation diminished by 50%.
Since it seems unrealistic that all persons with schizophrenia will achieve working in the
open labour market, it is important to identify the rewards that having a job bring and try
to enrich other types of occupations with such rewards. For example, taking part in
planning, meetings, and customer contacts might be such job-like features that could be
implemented in day-care centres and other units that provide daily occupations that are
considered to be less job-like.
7.1.2 ADL (Activities of Daily Living)
Factors which are addressed with the person with schizophrenia, are improving the
quality of life including management of time, connecting and belonging and making
choices and maintaining control6.
Home management, including visits to the home, often needs to be addressed by the
occupational therapist. Related issues such as child and adolescent management are
also important.
7.1.3 Social Participation And Leisure
Providing opportunities for meaningful daily occupations, particularly in small groups,
where the issue of meaning can be addressed in terms of concrete, symbolic and/or self-
reward value, is extremely important. Counteracting the social isolation that occurs with
the illness is vital. Opportunities for social contact can be planned by the occupational
168
therapist and will include participation in social events such as sport, learning a new skill
in a group such a sculpture of pottery, outings to places of interest etc.
7.1.4. Occupational Group Therapy
The use of group-work in occupational therapy has always been an integral part of
intervention, particularly in the psychiatric field, and constitutes a major part of any
programme. Occupational therapists in South Africa are highly trained in group-work.
Groups specifically address the schizophrenic’s social participation and the training is
social and life skills. Focus in occupational group therapy is always on the client’s
functional problems and can also address symptoms of the illness. As can be seen in the
suggested programme below, most activities such as psycho-education, stress
management, personal care etc. take place in groups. Not only is this cost-effective
method of treatment for both client and therapist but it is has shown to be the most
effective type of treatment. Individual treatment with the schizophrenic client is only used
in aspects of a very personal nature or in the field of work.
7.2 Theoretical Framework
7.2.1. Models
Although some theorists in occupational therapy view dysfunction as a relationship
between emotion and action7, cognitive skills are the primary focus of treatment by
occupational therapists with the person with schizophrenia. The cognitive approach is
therefore employed.
An effective occupational therapy programme must contain “elements of practicality,
concrete problem-solving for everyday challenges, low-key socialisation and recreation,
engagement in attainable tasks and specific goal orientation”8
7.2.2 Frame of References/Approach
Recent research within occupational therapy internationally has shown that there is a
relationship between having meaningful and valued occupations and perceiving well-
being and a good quality of life9. Actual doing, such as being engaged in many activities

169
or having gainful employment has been found to be related to both self-ratings and
interviewer ratings of health and well-being. However, the way the doing was perceived,
in terms of satisfaction, value, and meaning, was even more consistently and strongly
related to health-related factors10.
Purposeful activity is the cornerstone and the major tool of intervention in occupational
therapy. Vona du Toit (1991) also ascribed to the belief, central to the profession’s
philosophy, that occupational therapy activity engages the mentally ill person in
meaningful occupation in order to maintain occupational performance and quality of life4.
It is therefore important that the occupational therapist can identify what kinds of
occupations are stimulating and engaging for a client. Moya Willson states that “Activities
are the major therapeutic measures used within occupational therapy11. Each activity
needs to be selected for its relevance to the functional and personal needs of the patient.’
Therefore, a client-centred practice is the current ideal for occupational therapists
working with persons with schizophrenia.
In client-centred practice the client and the occupational therapist work together as
mutual partners in order to find the best solutions for the client. However, it might be
difficult to establish communication and a relationship with persons with schizophrenia.
As a major symptom of the illness they may be unmotivated to participate in occupational
therapy and say they find most things meaningless. It is important to note also that the
illness of schizophrenia may have caused an impaired capacity and a loss of self-identity
which will affect the performance of purposeful activity. Especially in such cases, a
structure for how to identify meaning-making features of an occupation might be useful.
Persson and Colleagues proposed such a structure12, stating that for an occupation to be
perceived as meaningful, it must possess one or more of three identified value
dimensions: the concrete, the symbolic, and the self-rewarding. An occupation imprinted
with concrete value becomes meaningful because it brings tangible rewards, such as
payment, a product, or a new skill. Meaning can also spring from occupations that render
symbolic value at the personal, cultural or universal level. Occupations linked with self-
reward value are perceived as meaningful because they bring joy and excitement. These

170
types of values may serve as a checklist when communicating with a client in order to
find ways to a meaningful daily life. If none of these values can be identified for a certain
occupation, it should be abandoned.
7.3 Treatment Programmes A BALANCED WEEKLY PROGRAMME
A balanced weekly programme, at any stage of intervention, could consist of the following
activities which can be undertaken individually or in groups:
• Personal care/self independence and assistance in the family’s daily tasks
• Psycho-education
• Stress management and social skills training on a very basic level.
• Creative activity groups which can include hobby or leisure pursuits. Learning the skill
of using leisure time is very important.
• Simple exercise, walks and sport, all of which promote physical fitness.
• Sensory integrative programmes which are effective in treating the positive symptoms
of most severe mental illnesses.
• Sessions on subjects such as child and home management or budgeting where
appropriate.
• Vocational assessment and rehabilitation 7.4 Time Span NUMBER OF OCCUPATIONAL THERAPY HOURLY SESSIONS.
ACUTE PHASE:
1 x session of comprehensive assessment
1 x collateral information or consultation
2 x individual treatment
5 x occupational group therapy
2 x follow up

171
CHRONIC PHASE:
Patients in the chronic phase require long-term intervention. A patient may be part of
occupational group therapy for as long as a year, once a week.
1 x session of comprehensive assessment
1 x collateral information or consultation
2 x programming for daily activities
50 x occupational group therapy
1 x session reassessment
8. TABLE OF THE EVIDENCE
AUTHOR STUDY POPULATION
TYPE OF DESIGN
TREATMENT GROUP
OUTCOME VARIABLE
FINDINGS
Oka,
M.,Otsuka,K.
et.al. 2004
Schizophrenia Retrospective
study 52 clients
followed up
after 17
years
Vocational
rehabilitation
programme
50% drop in
risk of
hospitalisation
and
improvement
in social
functioning
9. CONCLUSION Advances in neuroleptic medication, as well as the move of the profession of occupational
therapy into the field of health sciences and psychosocial care, has provided a much more
scientifically-based, realistic, holistic and client-centred approach to the intervention of the
person with a severe mental disorder. At the same time the practical nature of the profession,
which provides expert knowledge of activities contained with our everyday occupations, has
not been lost. This is an essential part of the total rehabilitation and maintenance of the
person with schizophrenia.

172
10. REFERENCES 1. Duncan,M. (2005) Three approaches and processes in occupational therapy with mood
disorders, in Crouch & Alers Eds. Occupational therapy in psychiatry and mental health.
London & Philadelphia: Whurr Publishers. pp459-480.
2. Strong, S. (1998). Meaningful work in supportive environments: experiences with the
recovery process. American Journal of Occupational Therapy, 52, 31-38.
3. Crouch,R., & Eklund,M. (2006) Meaningful daily occupations – a central task in
occupational therapy with people with severe mental disorders. The World Association of
Psychosocial Rehabilitation (WAPR).
4. Crouch, R., & Alers, V. (2005) Eds. Occupational therapy in psychiatry and mental health.
4th ed. London & Philadelphia: Whurr Publishers.
5. Oka,M,Otsuka,K, et.al. (2004) An evaluation of hybrid occupational therapy and
supported employment progam in Japan for persons with schizophrenia. American
Journal of Occupational Therapy 58 (4) : 466-75,Jul-Aug.
6. Laliberta-Rudman,D,Yu,B. et.al. (2000) Exploration of the perspectives of persons with
schizophrenia regarding quality of life. American Journal of Occupational Therapy. 54 (2):
137-47. Mar,-Apr.
7. Chistiansen and Baum Creek,J. (2002) Occupational Therapy and mental health.
London: Churchill Livingstone.
8. Kaplan, H. I., & Sadock, B. J. (2000) Comprehensive textbook of psychiatry. 7th Ed.
Philadelphia: Lippincott Williams & Wilkins.

173
9. Aubin,G,Hachey,R & Mercier,C (1999) Meaning of daily activities and subjective quality of
life in people with severe mental illness. Scandinavian Journal of Occupational Therapy,
6,53-62
10. Eklund, M., & Leufstadius, C. (in press). Occupational factors and aspects of health and
wellbeing in individuals with persistent mental illness living in the community. Canadian
Journal of Occupational Therapy.
11. Willson,M. (1983) Occupational therapy in long-term psychiatry. Ediburgh:Churchill
Livingstone
12. Persson, D., Erlandsson, L-K, Eklund, M., & Iwarsson, S. (2001). Value dimensions,
meaning, and complexity in human occupation – A tentative structure for analysis.
Scandinavian Journal of Occupational Therapy, 8, 7-18.
13. Atkinson,JM. (1994) Schizophrenia at home: A guide to helping the family.
London:Croome Helm.
14. Boronow,JJ (1986) Rehabilitation of chronic schizophrenic patients in a long-term private
setting. Occupational Therapy in Mental Health. Vol. 6 pp 1-19.
15. Coviensky,M & Buckley,VC. (1986) Day activities programming: Serving the severely
impaired chronic client. Occupational Therapy in Mental Health. Vol. 6 pp. 21-30.
16. Evans, J.Salim, AA (1992) A cross-cultural test of the validity of occupational therapy
assessments with patients with schizophrenia. American Journal of Occupational
Therapy. 46 (8): 685-95, Aug.
17. Hachey,R,Boyer,G,& Mercier,C. (2001) perceived and valued roles of adults with severe
mental health problems. Canadian Journal of occupational Therapy 68 (2): 112-20. April.

174
18. Krupa,T&Thornton,J. (1986) The pleasure deficit in schizophrenia. Occupational Therapy
in Mental Health. V6. pp 65-77
19. Lesunyane,RA, (2005) Role performance of psychiatric clients in the community.
Research thesis for Master of Science in Occupational Therapy. University of Limpopo
(Medunsa Campus)
20. Straube,ER&Hahlweg,K. (1990) Schizophrenia: Concepts, vulnerability and intervention.
Springer-Verlag. Berlin
21. Stauffer,DL. (1986) predicting successful employment in the community for people with a
history of chronic mental illness. Occupational Therapy in mental health Vol. 6. pp 31-48.
22. Suto,M&Frank,G. (1994) Future time perspective and daily occupations of persons with
chronic schizophrenia in a board and care home. American Journal of Occupational
Therapy. 48 (1), Jan.
23. Vaccaro,JV,Young,AS,&Glynn,S. (1993) Community-based care of individuals with
schizophrenia. Psychiatric Clinics of North America. Vol. 16 (2) June.

175
SUBSTANCE USE DISORDERS.
Compiled by Rosemary B Crouch PhD Occupational Therapy (MEDUNSA)
1. INTRODUCTION
‘Alcoholism is the most treatable untreated disease’1.
Many occupational therapists in private practice are providing services to persons with
substance use disorders all over South Africa. It is unavoidable because of the high
percentages of dual diagnoses in the psychiatric field in South Africa. Occupational
therapists not only encounter these clients in specialised treatment settings, but in many
other incidences, for example in the orthopaedic or general medical unit. Here the client’s
substance use disorder may be complicated by other conditions such as multiple fractures
from a motor car accident, heart complaints, diabetes, anxiety or depression.
2. DIAGNOSIS One of the difficulties that a person with a substance use disorders has had in the past is the
attitude of the medical aids, which will not cover treatment of this disorder by an occupational
therapist or any other health professional. Consequently these patients have generally been
treated under an alternative or dual diagnosis e.g. depression, schizophrenia and bi-polar
disorder. For the sake of completeness, however, the diagnostic codes under which patients’
fall, which are treated by an occupational therapist, are usually as follows:
ICD 10 coding:
• F10.1 Mental and behaviour disorder due to use of alcohol: harmful use
• F23.9 Psychosis unspecified.
• Z 71.4 Alcohol abuse counselling and surveillance.
• T40 Poisoning cannabis
• X62 Intentional self-poisoning with narcotics.
• F32.2 Acute schizophrenia like psychotic disorder.

176
DSM IV: PSYCHOACTIVE SUBSTANCE USE DISORDERS:
• 303.90 + 305 Alcohol dependence and abuse
• 304.30 + 305.20 Cannabis dependence and abuse
• 304.20 + 305.60 Cocaine dependence and abuse
• 304.10 + 305.40 Sedative, hypnotic or anxiolytic dependence and abuse
• 304.90/305.90 Polysubstance dependence & abuse
• 298.80 Brief reactive psychosis
• 295.40 Schizophreniform disorder
• 297.30 Induced psychotic disorder
3. IMPACT ON OCCUPATION 3.1 Work
The effect of drugs and alcohol on the client’s performance at work is of major significance
and costs the country millions every year. The effects are usually on work performance,
absenteeism, accidents, excessive medical care, decreased productivity and faulty decision
making. Traditionally the alcoholic when not drinking is a hard worker but the greatest
problem is holding down the job down when he/she is drinking, denying the problem, and a
lack of understanding of most employers.
3.2 Activities Of Daily Living Often the client’s ability to cope with personal hygiene, self-care and care of the environment
is lacking in severe cases, particularly in the case of drug dependency.
Conversely female clients tend to overdress to try to disguise the fact that they have been
drinking. Their homes are often spotless and the physical needs of the family are well
attended to. However the emotional needs of the family is often sadly lacking.
Often clients have the inability to handle financial affairs and to budget adequately. This
would be a focus of treatment for the occupational therapist.

177
3.3 Leisure And Social
Most persons with substance abuse have no hobbies or pleasurable pastime activities other
than the use of the substance. Most past-times are associated with the use of alcohol or
drugs. Reintroducing, or in some cases introducing, the meaningful use of leisure time is a
primary aim for the occupational therapist.
The client’s ability to cope with the social sphere is often impaired i.e. in the area of social
awareness, communication with others and the formation of interpersonal relationships. This
is a stumbling block to the reintegration of the clients into the community after treatment. The
skills of the occupational therapist in carrying out occupational group therapy are of
importance here.
4. IMPACT ON ROLES, HABITS AND ROUTINES Substance use disorders result in a lack of balance between work, rest and play. The client
also does not use his capacities to the full, leading to an imbalance and failure to develop or
maintain normal functioning in most occupations. This leads to social withdrawal, less time at
work and with the family, breakdown of support systems and relationships2.
The possible consequences of both dependence and abuse of substances are:
• Failure to fulfil major role obligations
• Repeated situations which are physically hazardous
• Multiple legal problems
• Recurrent social and interpersonal problems e.g. divorce, physical and verbal abuse,
rape, child abuse
• Repeated absences at work/school and poor work/school performance
• Neglect of child-care and household duties
• Aggressive behaviour.

178
5. HEALTHCARE STRUCTURES Treatment of the person with substance-use disorders has long been the domain of the
social worker in South Africa to the exclusion of other disciplines such as occupational
therapy and clinical psychology. One of the reasons for this has been the legislation of the
country which dictated in the Social Services Act, that all rehabilitation centres for substance-
use disorders must have a social worker at the head. However experts in the field such as
the late Dr Sylvain de Miranda, head of the SANCA, introduced other disciplines into his
clinics, such as Phoenix House drug rehabilitation centre in Johannesburg. When he opened
Riverfield Lodge private rehabilitation centre, an occupational therapist and clinical
psychologist, with two social workers were the key staff at the centre. Although this clinic did
not survive financially, for three years it provided excellent treatment for alcoholics and drug
dependents. Today private clinics in Cape Town, Port Elizabeth, the Drakensberg and
Johannesburg all have occupational therapy services. Few SANCA clinics provide
occupational therapy services and generally the NGOs remain behind in providing services
other than social work.
6. ASSESSMENT 6.1 Base-Line Assessments
6.1.1 Interview with the client, family members and often employers. These interviews
can take place separately.
6.1.2 Clinical observations are essential from the time the client is first admitted to
treatment until he is discharged. It is an ongoing process.
6.1.3. Evaluation takes place by both standardised and non-standardised tests.
Standardized tests include the Crouch Stress Assessment 2003, Hospital Anxiety and
Depression Scale5, The Beck Depression Inventory3 and the Canadian Occupational
Performance Measure4.

179
6.1.4. Collateral information is essential from significant others, employers (where
available) and colleagues.
6.1.5. Assessment reports are issued only to the referring agent and to other health
professionals in the multidisciplinary team who are registered with the Health Professions
Council of South Africa (Ethical Rules 2006 HPCSA). This does not include unqualified
persons. In the field of rehabilitation of persons with substance use disorders there are
many volunteers and recovering addicts.
6.1.6. Ongoing assessment takes place during treatment and before discharge.
6.2 Theoretical Framework
6.2.1 Models It is important to look at the models of treatment of substance use disorders, used
throughout the world, in order to understand where occupational therapy is most
effective.
The most commonly used and fashionable model is the Minnesota Model which is used
by the AA worldwide. Chacksfield and Lancaster6 describe in detail the 12 steps to
recovery and how the occupational therapist has an important role to play in each. The
occupational therapy programme of skills fits in very well with this model.
Gorski7 describes six phases of treatment where the skills of the occupational therapist
with the cooperation of the team, are essential in each phase from pre-treatment to
maintenance8.
6.2.2 Frame Of Reference/Approach
The versatility of the training of occupational therapists worldwide makes them ideal for
taking part in the intervention within the client’s own environment, taking into
consideration the performance areas of their life i.e. the performance area, the
performance components and the performance contexts (American Occupational
Therapy Association, 1994).

180
A person engaging in substance abuse alienates him/herself from the usual activities
which he engages in. The results are frustration, boredom, unhappiness and stress.
Active, open, excessive drinking and drugging as well as solitary use of substances often
bring about these effects6.
7. INTERVENTION 7.1. The Role Of The Occupational Therapist The occupational therapist provides an invaluable service to the person with a substance
use disorder, in all clinical settings including private practice. The service today is often as an
aftercare service.
Intervention by the occupational therapist with a person with a substance use disorder is
usually on an individual level whilst he/she is still intensely ill and then group therapy is
introduced. It is recognized internationally that the dynamics of group-work are the most
successful factors in the rehabilitation of a person with these problems. Alcoholics
Anonymous (the AA) attributes its success to this fact.
7.1.1 Occupational Group Therapy
Occupational therapists all over the world have earned themselves a reputation for
excellent group work. In South Africa this is because of extensive training in occupational
group therapy at an undergraduate level and at post-graduate level.
Group therapy is the preferred method of intervention in a team approach to the
treatment of clients with substance use disorders. This is because the illness is basically
a social illness. All types of occupational group therapy are discussed below.
Of particular focus is:
• Stress management which is most effective in a group, and occupational therapists
are highly skilled in this discipline. Stress management is an integral part of the total
approach to the treatment of clients with substance use disorders.
• role-play, sociodrama and psychodrama (psychodrama is introduced to occupational
therapist at an undergraduate level and post-graduate training takes place by a

181
specialized group such as the GAPE Group(OTASA). These techniques are dynamic and
powerful in helping a client to gain insight into his problem and himself.
• Groups to encourage free time and leisure pursuits e.g. creative activities, gardening,
cooking and baking, physical fitness and sport. These pursuits are vital in introducing the
client to an alternative to his present lifestyle and providing a meaningful replacement to
drinking and drugging.
• Social skills training, in particular assertiveness training. Many clients use substances
to promote assertiveness.
• Psycho-education groups which provide information on the illness but are not the sole
domain of the occupational therapist.
7.1.2 Work
Vocational rehabilitation is a very important aspect of occupational therapy intervention
and is vitally important in rehabilitation of the client with a substance use disorder. After
rehabilitation it is important for the client to be involved in procuring his own employment
and that structures are in place where the occupational therapist is in contact with the
employers and the Employment Assistance Programmes in terms of the progress of the
client.
7.1.3. Activities Of Daily Living (ADL
It is often necessary to attend to activities of daily living (ADL) such as self-care, home
management, financial management/budgeting and childcare. These sessions can take
place individually or in small groups.
7.1.4 Physical Fitness
Physical fitness is an integral part of the occupational therapy programme. Walking,
jogging, physical training, relaxation and sport not only help to relieve stress but helps
with weight loss, tones up the body generally and provides another important facet to
living a balanced lifestyle e.g. encouraging a client to join a gym and to attend at the time
that he is most vulnerable to drinking, can be a valuable help to maintaining sobriety

182
7. 4 Time Span Number of Occupational Therapy Hourly Sessions
ACUTE PHASE:
1 x session of comprehensive assessment
1 x collateral information or consultation
2 x individual treatment for programming
6 x occupational group therapy
2 x follow up
CHRONIC PHASE:
Patients in the chronic phase require long-term intervention and support. A patient may be
part of occupational group therapy for as long as a year, once a week.
1 x session of comprehensive assessment
1 x collateral information or consultation
2 x programming for daily activities
50 x occupational group therapy (aftercare)
1 x session reassessment

183
8. TABLE OF EVIDENCE
AUTHOR STUDY POPULATION
TYPE OF DESIGN
TREATMENT GROUP
OUTCOME VARIABLE
FINDINGS
Stoffel, V C.&
Moyers, P A
2001
Occupational
therapists9,10.
Persons with
substance-
use disorders
in America
Interdisciplinary
evidence-based
review of
interventions
12 step
programme,
motivational
strategies
and cognitive
–behavioural
techniques
Outcome
primarily
related to
reduction
for alcohol;
and drug
use.
Significant
results
demonstrating
the effectiveness
of an
interdisciplinary
approach to the
problem.
9. IN CONCLUSION The move of the profession of occupational therapy into the field of health sciences and
psychosocial care, has provided a much more scientifically-based, realistic, holistic and
client-centred approach to the intervention of the person with a substance use disorder. At
the same time the practical nature of the profession, which provides expert knowledge of
activities contained within our everyday occupations, has not been lost. This is an essential
part of the total rehabilitation and maintenance of the person with a substance use disorder.
10. REFERENCES 1. Wicocks,L (1992) Alcohol Abuse. How to help someone you love. Johannesburg: Aspin Oaks
Associates.
2. Wilcock,A,A (1998) An occupational perspective of health. New Jersey: Slack Inc
3. Becks Depression Inventory (1990) Industrial Rehabilitation. American Therapeutics Inc.

184
4. Law,M.,Baptiste,S., Carswell,A., et.al. (1998) Canadian Occupational Performance Measure. 43rd
Ed. Ottawa: CAOT Publications ACE.
5. HADS. Hospital Anxiety and Depression Scale (1994)) Berkshire: The NFER-Nelson Publishing
Company Ltd.
6. Creek,J. (2002) Occupational Therapy and Mental Health. London: Churchill Livingstone.
7. Gorski,T (1989) Pages through recovery. An action plan for preventing relapse (Hazelden recovery
series). Iowa: Hazelden Information Series
8. Crouch, R., & Alers, V. (2005) Eds. Occupational therapy in psychiatry and mental health. 4th ed.
London & Philadelphia: Whurr Publishers.
9. Moyers,PA&Barrett,CA. (1992) Neurocognition and Alcoholism: Implications for Occupational
Therapy. Occupational Therapy and Psychosocial dysfunction. Pp. 87111.
10. Stoffel,VC&Moyers,PA (2004) An evidence-based and occupational perspective of interventions
for persons with substance-use disorders. American Journal of Occupational Therapy Sept-Oct: 58
(5): 570-96.
11. Kaplan, H. I., & Sadock, B. J. (2000) Comprehensive textbook of psychiatry. 7th Ed. Philadelphia:
Lippincott
12. Williams & Wilkins. In a board and care home. American Journal of Occupational Therapy. 48 (1),
Jan.
13. Miller,H. (1997) Prenatal cocaine exposure and mother –infant interaction: implications for
occupational therapy intervention. American Journal of occupational Therapy. Vol51(2). Pp119-
129. Feb.

185

186





























