Embed Size (px)
Citation preview

Restorative Dentistry
Occlusal caries: Diagnosis and noninvasive treatmentsRoberta Tarkany Basting'/Mônica Campos Serra, MS, ScD"
The diagnosis ot occiusai caries and the initiation of more effective treatment present a considerable chai-ienge. Caries not oniy has decreased in prevaience, but aiso has changed in pattern and in progressionbecause ot the increased use of fluorides. Correcf diagnosis is oruoiai. distinguishing iesions that can bearrested by noninvasive treatment from those ihat may justify restorative treatment. For incipient iesions, itis neoessary to improve the patient's home care preventive methods, lo apply tluoride or other prophyiac-tic agents, or even to seat fissures, preserving the maximum amount of sound tooth structure. This articlediscusses the diagnosis of oodusal caries and noninvasive treatments for the management of eariy caries.(Quintessence int 1999;30:174-178)
Key words: arrested iesicn. caries diagnosis, incipient lesion, noninvasive treatment, occlusai caries
CLINICAL RELEVANCE: Precise diagnostic methods areimportant for deciding whether to treat a parficuiar lesion.Noninvasive treatments are preferabie in early lesions.
The continued decrease in the prevalence of dentalcaries requires much greater caution on the part of
the clinician and a greater focus on accurate diagnosisof caries status and risk factors associated with theformation of new lesions and the progression of exist-ing lesions.' Furthermore, caries not only has de-creased in prevalence, but aiso has changed in patternand progression.- The increased use of fluorides isthought by many to be largely responsible for thischanging pattern of dental caries, an additional benefitbeing conferred on those who have had iifelong expo-sure to water fluoridation.'
The problems in caries diagnosis are usually notassociated with advanced lesions (Fig 1), but primarilyinvolve the eariy iesions (those confined to theenamel).'' It has heen suggested that the diagnosis offissure caries has become more difficult hecause thehigh remineralization capacity of fluorides tends tomask dentinai caries.^-'
"Questionable"' occlusal caries appears to be partic-ularly difficult to diagnose and to treat if the dentist'sgoal is conservative dentistry. For lesions in enamel,treatment consists of improvement in the patient'shome care preventive metbods, application of fluorideor other prophylactic agents, or seahng the fissures.Sometimes it is oniy necessary to practice "watchfuiwaiting."* These procedures are a part of the conserva-tive philosophy (noninvasive treatments), whichcontrasts with the invasive philosophy, which doesnot eliminate the disease and just treats the diseasesymptoms.'
The purpose of this article is to discuss the diag-nosis of occlusal caries and noninvasive treatments forthe management of early caries.
•Graduate Student, Ciinicai Denfal Science, Deparlmerit ot RestorativeOentisfry, School of Dentistry, University of Campinas-UNiCAMR Piraci-caha, Sao Pauio, Brazil.
"Professor, Departmenl of Restorative Dentistry, School cf Dentistry, Uni-versity of Campinas-UN iCAMP, Piracioaba, Sao Pauio, Brazii.
ReprinI requests: Ms Roberta Tarkany Basting, Facuidade de Odcnto-iogia ds Piracicaba-UNiCAMP, Departamento de Odontoiogia Restaura-do ra-Dent 1st ica. Avenida Limeira, 901-Areiào, CEP; 13414-900, Piracicaba,Sào Paulo, Brazil, Fax: 55-19-430-521B,
DIAGNOSIS OF OCCLUSAL CARIES
The diagnosis of occlusal caries presents a consider-able challenge. That is why it is important to diagnosecorrectly, distinguishing lesions that must he treatedrestoratively from those that can be treated in a nonin-vasive way. This procedure is difficult because of the
174 Voiume 30, Number 3, 1999

Basting/Serra •
Fig 1 Obvious cavitated iesion in an oeciusai surface The diag-nosis of caries is evident, and restorative treatment is neoessary.
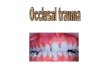
Fig 2 Early caries In an ocoiusal surface The white-apot iesionand the brown discoloration in the fissure indioate that demineral-izafion ot the enamei has occurred Bitewing radiography showedno radioiucenoy in dentin.
dynamic nature of dental caries, which includes peri-ods of demineralization and remineralization, mean-ing that the detection of small lesions is particularlyimportant. =
Visual inspection
Early caries in occlusal surfaces usually appears as awhite-spot lesion, with brown discoloration aroundthe fissure, suggesting tbat demineralization of theenamel has occurred (Fig 2). Compared to translucentsound enamel, white spots are opaque because theircrystals have changed physical properties and have adifferent chemical makeup. White spots can be seenaround the opening of an occlusal fissure, and tbeymay have a matte or dull appearance, indicafing activedisease.'" Alternatively, fissures may be stained, andthis appearance may or may not indicate a carious le-sion. Tbe area of enamel around the fissure may alsoappear opaque or may have a grayish tinge indicativeof stained dentinal caries.' Somefimes early stages ofthe lesion are hidden from the naked eye, with largedentinal lesions-beneath seemingly sound occlusalsurfaces'"''^-that may justify restorative treatment.
In arrested lesions, remineraiizing pbases have ex-ceeded demineralizing phases. Fluoride ions and otherminerals have been incorporated in the lesion as partof the consolidation process. A darker discolorationcan be seen in arrested lesions as a result of the extrin-sic organic material incorporated, and these areas aremore resistant to cariogenic challenge.""' This situa-tion can be addressed by noninvasive treatments thatean enhance this process.
Caries can be diagnosed by visual inspection. Aprobe sbould be used only for careful removal of debrisfrom the depths of the fissure.'" Probing may allow
transmission of cariogenic fiora from one infected siteto another. Ftirthermore, it can produce irreversibletraumatic defects in potentially remineralizableenamel, and probing is not more accurate in diagnosisthan visual inspection alone.' ' '•' '^ Because of the pos-sibility of introducing iatrogenic damage, there is rea-son to reconsider tbe probe as a classic invasivemetbod of diagnosis.'̂
Tben, tbe concept of "looking for" caries with theeyes is very important.' To allow reliable detecfion ofthe earliest, clinically visible, manifestation of dentalcaries-tbe wbite spot, teeth should be clean and dry.'Plaque and saliva can obscure these lesions,' and clin-icians working at the cavitation level are more likelyto make false negative diagnoses, missing active cariesthat could be arrested. In addition, the white spot ismore obvious when teeth are dry because of the differ-ent refractive indices of enamel, water, and air." Tberefractive index of enamel is 1.62. Wben demineral-ized, enamel becomes porous. If the teetb are wet,these pores are filled with a watery medium with arefractive index of 1.33; when the porosity is consider-able, this difference in refractive index will cause thetissue to lose its translucence and appear opaque. Ifthe enamel is dried, the water is replaced with air,which has a refractive index of 1.0; the difference inrefractive index between the air and the enamel isgreater than that between water and enamel, so tbelesion is more obvious.
When assessing a carious lesion, tbe dentist sbouldfirst ask, "Is there active caries?" instead of, "Is therecaries?"' Many times, lesions can be arrested if aconcept of treafing these diseases as infections ratherthan just treating the disease symptoms is adopted.*The concept of "lesion behavior" rather than "lesionprogression," now seems more logical because it
Quintessence Internatiorai 175

• Bastin g/s erra •
avoids any implication of unavoidable and unremittingactivity."^ Thus, dentists can apply more efficient andrealistic methods for better patient care and treatmentbased on the identification of caries risk or cariesactivity.'̂
Patient history
However, dentists continue, currently, to have diffi-culty in differentiating active from arrested lesions andusually base tbeir decision on "clinical judgment."Failure to diagnose caries may result in the continueddestruction of the dentition.'^ To help in their deci-sions, they should include in the patient's record anassessment of the past caries experience and cariesrisk. They should know the patient's dietary habits,salivary function, plaque localization and consistency,pit and fissure morpbology, and home care preventivemethods (exposure to fluoride, for example).' This sta-tus will identify the rate of caries progression and thenecessity of monitoring caries activity.'̂
Bitewing radiographs
Because no better method for determining the pres-ence and extent of occlusal caries has been developed,it is useful to include information obtained frombitewing radiographs in the diagnosis of occlusalcaries.̂ Radiographs are better than visual inspectionalone," because clinical scoring most frequently un-derestimates lesion depth.-"--' However, the anatomyof posterior teeth is such that large volumes of soundenamei cover the buccal and lingual cusps and, on aradiograph, conspire to mask any incipient demineral-ization in an occlusal fissure." There is a higher fre-quency of false-positive diagnosis in the occiusai areathan in the interproximal area, indicating that the bor-derline between enamel and dentin is difficult to inter-pret radiographically.^' The most dramatic clinicalconsequence is when restorations are placed in soundteeth.
An occlusal radiolucency in the bitewing radio-graph calls for attention, constituting a vaiuable sup-plement to the clinical examination,' and a restorativetechnique is considered necessary when a lesion ex-tends into dentin.̂ -̂̂ ^ However, it is not possible tocorrelate external characteristics, such as where thecaries occurred on the tooth surface, lesion color,presence of shadowing, or the fissure morphology,with the extent of the carious process.^' Radiographsare inaccurate in estimating the extent of the caries orin detecting minimal occlusal lesions but are useful formonitoring the preventive therapy.'^ This vigilance isnecessary to accomplish the ultimate goal of dentistry;to conserve as much tooth structure as possible. '̂'
In conclusion, the modern clinician's aim shouldbe to diagnose caries before cavitation has occurredso that noninvasive treatments may arrest it. To thisend, the clinician should examine clean, dry, andwell-lighted teeth by visual inspection and bitewingradiographs.
NONINVASIVE TREATMENT OF OCCLUSAL CARIES
For teeth with occlusal caries, there is a trertd forselecting the most conservative technique with respectto saving sound tooth substance, preferring nonin-vasive to invasive techniques. Clinicians now have amuch wider range of therapeutic options at their dis-posal for the management of occlusal caries.' Thechoice of treatment is based on the diagnosis,̂ '̂̂ ' andthe accuracy of that diagnosis is of major importance.
A restorative approach is justified when an occlusalcarious lesion has reached the dentin.̂ '•̂ '•̂ '' Because itseems to be a general opinion that dentinal cariesshould be treated operatively, it is important to knowthe amount of dentin involved in an occlusal cariouslesion without visible clinical cavitation.^'
When decisions arc made about restorative care,tbe generally slow average progression rates reportedbave to be weighed against the likely durability of anyrestoration.'" There is evidence that the longevity ofmany restorations may be short. Traditional restora-tive dentistry is the worst alternative for treating incip-ient occlusal caries, suffering from a large number offailures. Recurrent caries can occur at the tooth-restoration interface, indicating that disease is presentThe belief that dental caries can be treated effectivelyby restoring the lesion is an error. A decision to under-take invasive restorative treatment for a tooth may beappropriate only if, at the same time, noninvasive pre-ventive treasures are also applied.'-^'
Sound fissures or those with arrested lesions re-quire no specific treatment. As a matter of fact, ar-rested lesions exhibit a higher degree of resistance todemineralization than do uninvolved areas.'^'^However, where fissure morphology conceals progres-sive, active enamel lesions, preventive techniques arerequired to arrest lesion progression.^^ Noninvasivepreventive care is likely to be centered around coun-seling in oral hygiene, dietary matters, and the homeuse of topical agents such as fluoride toothpaste aswell as possibly the application of fissure sealants.^'
Occlusal surfaces of erupting permanent molars areparticularly susceptible to caries because conditions arefavorable for plaque accumulation. An individualized,nonoperative treatment program can reduce dentalplaque and caries on occlusal surfaces of newly eruptedmolars.^"' The treatment progratn must be based on
176 Voiume 30, Number 3, 1999

B asti ng/S erra •
the understanding of dental caries as a local diseaseand intensive training in home-based plaque control.
Special instructions about an appropriate techniquefor plaque control on the occlusal surfaces of partlyerupted permanent molars must be given to thepatient. He or she must be asked for intensive cooper-ation. The toothbrush is held in the buccolingualdirection, with the bristles toward the occlusal surface,and moved with rotary motions.'"
Fluoride toothpastes must be used in conjunctionwith the daily toothbrushing, constituting at-homepreventive care. At the dentist's office, the therapeuticuse of fluorides can be conducted. So. the cliniciancan also reinforce the plaque control of the patient,emphasizing the necessity of consistent use of a fluo-ride toothpaste. The effectiveness of fluoride againstcaries is known, and the frequency of fluoride pres-ence in the oral fluid is a strong factor in cariostasis.Improved methods of delivering low, but effective, lev-els of fluoride, either more frequently or over pro-longed periods, are beneficial for the increased effi-cacy of fluoride against earies.̂ ^
Another technique used by clinicians is "watchfulwaiting'' or réévaluation at the next appointment. Thistechnique may be combined with topical fluoridetreatment and dietary counseling that could providethe opportunity for arrest of the iesion and reminerai-ization and a return to a clinically sound state."
Sealant is usually placed when an active enamelcarious iesion shows signs of progression, when thepatient presents high caries risk and cannot controlthe dental plaque efficiently by toothbrushing, orwhen the patient does not cooperate with the pro-posed treatment. Sealant is considered interceptive,rather than preventive, because the carious process insmall lesions, and occasionally in larger lesions, mayhe arrested after sealing.^'"-'^ If the sealant is main-tained and the nutrients are prevented from enteringin the fissure, there is a continual reduction in the via-hility of the remaining bacteria.^*
There appears to be some evidence of the effectcaused by glass-ionomer cement on the consistencyof remaining carious dentin." However, it would bepremature to conclude that complete removal of cari-ous dentin need not be carried out when glass-ionomer cements are used. Although enamel cariesean be arrested by the use of sealant, means of diag-nosing occlusal caries are no less important,"Therefore, once the carious process has reached thepoint where bacteria have infected the dentin, removalof the infected tissue and its replacement with arestoration may be the treatment of choice.'*
In recent years, chlorhexidine has become availableas vamishes and has already been shown capable ofreducing Streptococcus mutans and demineralization
in several studies.'^ -"̂ Streptococcus mutans was sup-pressed in occlusal fissures for 2 months after oneapplication of 40% chlorhexidine varnish," The majoradvantages of its use seemed to be the lack of dis-coloration of teeth, the longer retention, and theabsence of bad taste for the patient because of thelocal application in occlusal surfaces.
The use of fluoride varnishes in conjunction withan antimicrobial solution, such as 0.2°!i) ehlorhexidinegluconate, may enhance the remineraiization of theaffected enamel in the fissure in vitro.-"-! Therefore, notonly would the infection be controlled by the reduc-tion of Streptococcus mutans, but also the structuralloss caused by the carious lesion would be repaired.
From this range of noninvasive treatments, the pro-fessional can choose the best for the patient, associat-ing compatible methods for specific cases, allied withhealth promotion.'' Once a noninvasive approach toone or more carious lesions in an individual has beenadopted, continued vigilance will be required so thatany progression of the caries can be monitored andmanaged accordingly.̂ Furthermore, clinicians shouldbe conscious of their diagnostic performance, adjust-ing their treatment philosophy to emphasize accuratediagnoses, resulting in fewer unnecessary restorations.Dentists who make the diagnosis and the treatment ofcaries fit the patient's risk will be rendering the bestprofessional service.
REFERENCES
1. Anusavice K). Protocol for conservative treatment deci-sions. I Am Dent Assoe 1995:126:740-743.
2. Newbrun E. Preventing dental caries: Current and prospec-tive strategies J Am Dent Assoc 1992;l23:68-73.
3 Elderton RI. Assessment and chnical management of earlycaries in young aduits: Invasive versus non-invasive meth-ods. Br Dent J 1985; 158:440-444.
4. Newbrun E. Problems in caries diagnosis. Int Dent J 1993;43:133-142.
5. Kidd EAM, Ricketts DNJ, Pitts NB. Occlusal caries diagno-sis: A changing challenge for clinician and epidemiologists.JDent 1993:21:323-331.
6. Sawlc RF, Andlaw RJ. Has ocelusal caries become more dif-ficult to diagnose? Br Dent J 1988:164:209-211.
7. Weerheijm KL, de Soct JJ, de Graaff J, van Amerongen WE.Occiusal hidden caries: A bacteriological profile. J DentChild 1990:57:428-432.
8. Meiers JC, Jensen ME. Management of the questionable ear-ious fissure: Invasive vs. noninvasive techniques. J Am DentAssoc 1984:108:64-68.
9. Anderson MH, Bales DJ, Omnell K. Modern managementof dentai caries: The cutting edge is not the dental bur. J AmDent Assoc 1993:124:37-44.
10. Carvaiho JC, Ekstrand KR, Thylstrup A. Dental plaque andearies on occlusal surfaces of first permanent moiars in rela-tion to stage of eruption. | Dent Res 1989;68:773-779.
Quintessence International177

• Basting/Serra •
l î . Pitts NB. The diagnosis of dental caries: Diagnostic meth-ods of assessing buccal, lingual and occlusal surfaces. DentUpdate 1991;18:393-396,
12. Shearer AC, Wilson NHF, Radiographie for the diagnosisof dental caries in posterior teeth. Clin Prev Dent 1989;11:24-28.
13. Barhakow F, Imfeld T, Lutz F. Enamel remineralization:How to explain it to patients. Quintessence Int 1991;22:341-347
14. Koulourides T, Cameron B. Enamel remineralization as afactor in the pathogenesis of dental caries. ] Oral Pathol1980;9:255-269,
15. Lussi A. Validity of diagnostic and treatment decisions offissure caries. Caries Res 1991;25:296-303.
16. Ekstrand K, Qvist V, Thylstrup A. Light microscope study ofthe effect of probing in occlusal surfaces. Caries Res 1987;21:368-374.
17. Thylstrup A, Fejerskov O. Textbook of Cariology. Copen-hagen: Munksgaard, 1986.
18. Pitts NB, Kidd EAM. Some of the factors to be consideredin the prescription and timing of bitewing radiography inthe diagnosis and management of dental caries. J Dent1992;20:74-S4.
19. Anusavice KJ. Treatment regimens in preventive andrestorative dentistry. J Am Dent Assoc 1995;126:727-743.
20. Lussi A. Comparison of different methods for the diagnosisof fissure caries without cavitation. Caries Res 1993:27:409-416.
21. Wenzel A, Fejerskov O, Kidd E, Joyston-Bechal S,Groenveld A. Depth of occlusal caries asserted clinically, byconventionai film radiographs, and by digitized, processedradiographs. Caries Res 1990;24:327-333.
22. Espelid I, Tveit AB, Fjelltveit A. Variations among dentistsin radiographie detection of occlusal caries. Caries Res1993 ;28:169-175,
23. Weerheijm KL, de Soet JJ, van Amerongen WE, de Graaff J.Sealing of occlusal hidden caries lesions: An alternative forcurative treatment. ] Dent Child 1992;59:263-268.
24. van Amerongen JP, Penning C, Kidd EAM. ten Cate JM Anin vitro assessment of the extent of caries under small oc-clusal cavities. Caries Res l992;26:89-93,
25. Weerheijm KL, Groen HJ, Bast AJ, Kieft JA, Eijman MA,van Amerongen WE. Clinically undetected occlusal dentinecaries: A radiographie comparison. Caries Res 1992;26:305-309.
26. Nytun RB, Raadal M, Espelid I. Diagnosis of dentin involve-ment in occlusal caries based on visual and radiographieexaminat ion of the teeth. Scand J Dent Res 1992;100:144-148.
27. Ricketts DNJ, Kidd EAM, Beighton D. Operative andmicrobiological validation of visual, radiographie and elec-tronic diagnosis of occlusal caries in noncavitated teethjudged to be in need of operative care. Br Dent J 1995;179:214-220,
28. Tveit AB, Espelid 1, Fjelltveit A. Clinical diagnosis of occlu-sal dentin caries. Caries Res 1994;28:368-372,
29. Elderton RJ. Overtreatment with restorative dentistry:When to intervene? Int Dent | 1993 ;43:17-24,
30. Carvalho JC, Ekstrand KR, Thylstrup A. Results after I yearof nonoperative occlusal caries treatment of erupting per-manent first molars. Community Dent Oral Epidemiol1991;19:23-28.
31. Carvaiho JC, Thylstrup A, Ekstrand KR. Results after 3years of nonoperative occlusal caries treatment of eruptingpermanent first molars. Community Dent Oral Epidemiol1992;20:187-192.
32. Koulour ides T Fluor ide and the caries process.) Dent Res 1990;69 558.
33. Handelman SL, Washburn F, Wopperer P, Two-year reportof sealant effect on bacteria in dental caries. J Am DentAssoc 1976;93.967-970.
34. Going RE, Loesche WJ, Grainger DA, Syed SA. The viabil-ity of microorganisms in carious lesions five years after cov-ering with a fissure sealant . J Am Dent Assoc1978;97:455-462.
35. Weerheijm KL, de Soet JJ, van Amerongen WE, de Graaff J.The effect of glass-ionomer cement on carious dentine: An invitro study. Caries Res 1993 ;27:417-423,
36. Mertz-Fairhurst EJ, Adair SM, Sams DR, Curtis JW Jr, ErgleJW, et al. Cariostatie and ultraconservative sealed restora-tions: Nine-year results among children and adults. J DentChild 1995;62:97-107
37. Weerheijm KL, van Amerogen WE, Eggink C, The clinicaldiagnosis of occlusal caries: A problem, J Dent Child 1989;56:196-200.
38. Fusayama T. Two layers of carious dentin: Diagnosis andtreatment. Oper Dent 1979;4:63-70.
39. Hmilson CG Potential efficacy of chlorhesidine against mu-tans streptococci and human dental caries, J Dent Res 1994;73:682-691.
40. Bratthall D, Serinirach R, Rapisuwon S. Kuratana M,Luangjar-Mekorn V, Luksila K, Chaipanich P. A study intothe prevention of fissure caries using an antimicrobial var-nisb. Int Dent J1995;45:245-254.
41. Sandham H), Brown J, Chan KH, Phillips HI, Burgess RC,Stokl AJ. Clinical trial in adults of an antimicrobial varnishfor reducing mutans streptococci. ] Dent Res 1991;7I]:1401-1408,
42. Emilson CG. Outlook for Hibitane in dental caries. [ CiinPeriodontol 1977,4.136-143.
43. Schaeken MJ. Effect of single and repeated application ofchlorhexidine varnish on mutans streptococci in plaquefrom fissures of premolar and molar teeth. Caries Res 1993;27 303-306.
44. Sorvari R, Spets-Happonen S, Luoma H. Efficacy of chlor-hexidine solution with fluoride varnishing in preventingenamel softening hy Streptococcus mutans in an artificialmouth, Scand J Dent Res 1994;102:206-209,
178 Volume 30. Numbers, 1999