Embed Size (px)
Citation preview

NUTRITIONAL STRATEGIES: SATIETY, WEIGHT LOSS
AND SUPPLEMENTATION IN SPORTS
Scientific director: Enrico Arcelli


Calories: should we still count them? 2
Losing weight without losing lean body mass 4
Soy proteins in weight loss and sports 12
Beverages for athletes 20
Fatigue in football 37
Gastrointestinal disorders in long-distance runners 45
Sports anemia 51
table of contents

2
calories:
should we still count them?
The final conclusions of the round table of the 2nd
International Congress “Science in Nutrition”
(Rome, March 2010), organized by the Paolo
Sorbini Foundation for Nutritional Science, stated
that “calorie” is an "antiquated" term that is the
result of laboratory experience with calorimeters
and has no correspondence in physiology. The
calorie is the quantity of heat needed to increase
the temperature of one gram of water by 1°C, but
said quantity of heat depends on the initial tem-
perature and it is difficult to measure precisely.
Moreover, the International System of Units envi-
sages, instead of the calorie, the use of the joule,
the unit of measurement for thermal energy as a
function of temperature, which, in turn, is measu-
red in degrees. In general and in theory, the
quantity of heat can be expressed in units of
energy, but the human body does not behave like
a machine that burns calories.
It is a complex system of cells that regulates ther-
mal energy and hence body temperature by using
sophisticated metabolic mechanisms, the activity
of hormones (e.g., thyroid hormones) and other
body activities that do not simply depend on the
calories in food. For all these reasons, about 60%
of daily calorie intake is not used for metabolism.
In practice, when assessing different types of
food, you need to consider the glycemic index and
glycemic load. These physiological parameters -
which have been a part of scientific language for
a few decades now - refer to the quality and quan-
tity of food. The assessment of glycemic index and
load provides information to keep blood sugar
and carbohydrate metabolism under control. A
meal of foods with a high glycemic index and load
includes many carbohydrates that are quickly
assimilated. This entails a fast increase in blood

3
sugar and hence in insulinemia. This condition
stimulates the body to store energy as fat instead
of burning it to produce energy.
As underscored by Dr. Silvana Hrelia (Department
of Biochemistry at the University of Bologna) at
the round table, starting from the assumption
that lay people do not have a clear picture of the
scientific advances in the field of nutrition, it is
important to spread simple concepts and ideas to
reap positive results for well-being. It would
improve the chances of solving the obesity pande-
mic, also among children, and preventing chronic
pathologies (e.g., cardiovascular diseases, diabe-
tes and metabolic syndrome). Advertising messa-
ges that are harmful to the health of young peo-
ple must stop, and the language used must chan-
ge as well. It must be clear that it is not enough to
count calories without being aware of the real
meaning of the term, which 50% of Italians do not
know. Some use this unit of measurement for
mathematical calculations without knowing that a
diet low in calories is not enough to lose weight
and especially that such a diet is not enough to
lose weight well. The great majority of people do
not know that food with a low glycemic index
favors a feeling of fullness and is the first step
towards a healthy lifestyle. Prof. Enrico Arcelli
(Department of Sport, Nutrition and Health
Sciences at the University of Milan) added that
obesity is a risk factor for early mortality and that
two and a half hours of sports a week are not
enough to obtain optimal benefits (also in terms
of weight loss), but are enough to reduce the risk
of infarction and cardiovascular diseases by a
quarter.
In the field of nutrition, it is difficult to find an
agreement among all those involved, but there is
consensus on these rules: strike a balance
among the various types of nutrients; increase
the intake of vegetables and especially those with
a deep color - definitely not potatoes - and eat
seasonal fruits and extra-virgin olive oil regularly.
As for proteins, they are very important and you
should prefer leaner varieties, such as fish, poultry
and low-fat cheeses, ham (after removing fat) and
bresaola. In conclusion, it should be borne in
mind that 200 kcal derived from a certain food (for
instance, one rich in carbohydrates with a high
glycemic index) are not equivalent to those of
another food (for instance, one containing lean
proteins), as they have different effects on the
body, starting from blood sugar, insulinemia and
satiety.

4
- 1 -
losing weight without
losing lean body mass
This article discusses weight loss in sports,
namely the actual reduction in body fat without
reducing lean body mass. This objective can be
achieved by following those types of diets, such as
the Zone diet, that provide adequate quantities of
all nutrients, in a balanced relationship, and
ensure hormonal balance, while providing for
maximum physical efficiency, no feeling of hun-
ger and optimal training conditions. This way
there is a tangible loss of body fat while maintai-
ning muscle mass intact.
However, this article does not deal with those
practices, such as saunas and hypoglycemic
diets, that are carried out during the hours or
days before a competition and that do not affect
body fat but do cause dehydration or a reduction
in glycogen reserves.
LOSING WEIGHT IN SPORTS: WHY?
There are several reasons why athletes wish to
lose weight. Some athletes, like bodybuilders, do
it for aesthetic reasons; reducing subcutaneous
fat improves muscle definition. Other athletes do
it because competitions in their sports are divi-
ded into different classes based on body weight
(see Table 1); these sports include weight-lifting,
combat sports (boxing, judo, martial arts, etc.)
and rowing (lightweights and coxswains).
However, it also can be beneficial to lose weight
in sports with no classes with weight limits, since
lower body weight affords lower energy expendi-
ture (suffice it to mention here middle-distance
runners, mara thoners, race walkers, triathle-
tes…), or a better power-to-weight ratio (in parti-
cular, jumping competitions in athletics, the
open weight rowing class, artistic and rhythmic
gymnastics, and figure skating, etc.).

5
For instance, every kilo of extra weight leads to a
loss of about 1.5-2 cm in the high jump. If you
consider that the unit cost of running is equal to
about 200 ml/kg/km (Margaria, 1938), you can
calculate that in an athlete who initially weighs
65 kg, an extra kilo of fat leads to a worsening of
about 3-4 s in a 1500-meter runner who normal-
ly covers the distance in 3 min and 45 s; 12-14 s
in a 5000-meter runner whose regular time is
about 14 min and 30 s; and 25-30 s in a 10,000-
meter runner whose regular time is about 30 min
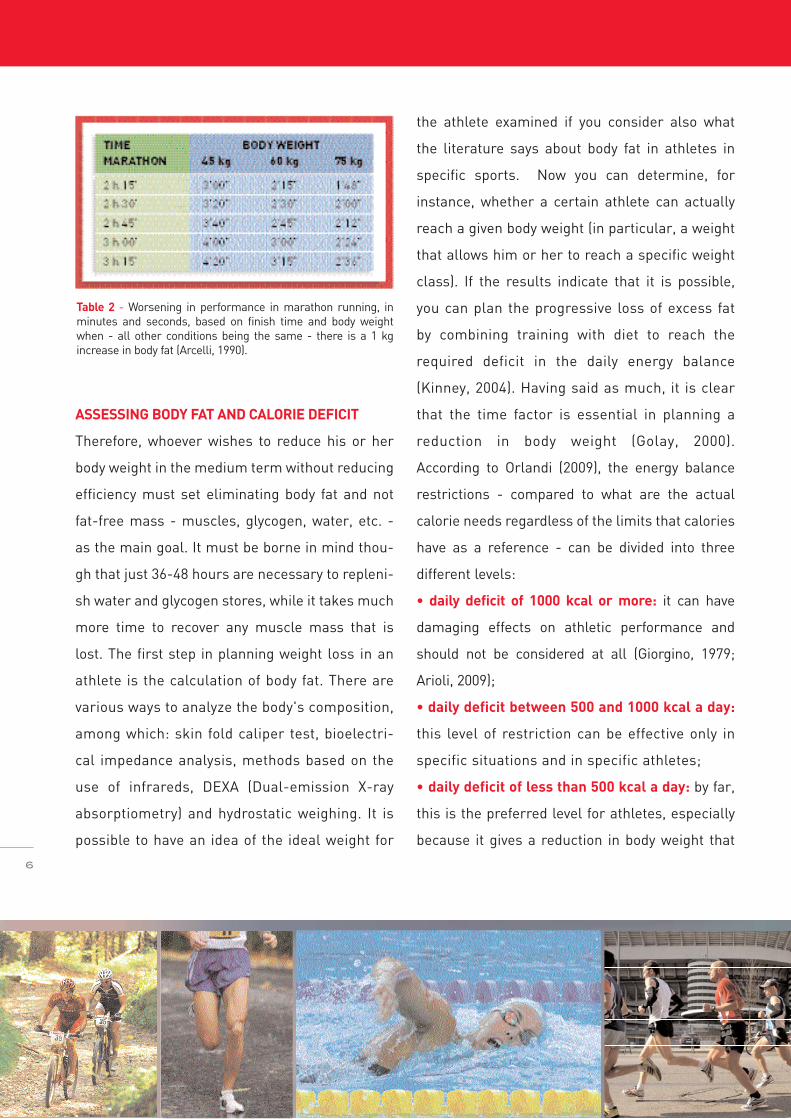
(Arcelli, 1990). In marathon racing the loss
amounts to 2-3 min (Table 2). Even in those
sports in which the movement is done by a hor-
se's muscles (showjumping, horse racing) or the
wind (sailing), a lower body weight is to be prefer-
red. On the contrary, in sumo, athletes focus their
efforts on increasing body weight (even reaching
extremely high levels of body fat), because the
technical characteristics of this sport do not
favor lighter athletes.
Table 1 - Weight classes and limits in rowing, weight-lifting and combat sports.
ROWINGMEN kg WOMEN kgLightweights 72,5 Lightweights 59Open weight > 72,5 Open weight > 59Coxswains 55 Coxswains 50
JUDOMEN kg WOMEN kgSeniors 55 Seniors 48“ 55-60 “ 48-52“ 60-66 “ 52-57“ 66-73 “ 57-63“ 73-81 “ 63-70“ 81-90 “ 70-78“ 90-100 “ > 78“ < 100
KARATEMEN kg WOMEN kgSeniors 55-60 Seniors 45-50“ 60-65 “ 50-55“ 70-76 “ 55-61“ 76-83 “ 61-68“ 83-90 “ > 68“ > 90
BOXINGMEN kg WOMEN kgLight flyweight 48 Light flyweight 44Flyweight 51 Flyweight 46Bantamweight 54 Bantamweight 48Featherweight 57 Featherweight 51Lightweight 60 Lightweight 54Junior welterweights 64 Junior welterweights 57Welters 69 Welters 60Middleweights 75 Middleweights 64Super middleweights 81 Super middleweights 69Heavyweights 91 Heavyweights 75Super heavyweights > 91 Super heavyweights > 81
WEIGHT LIFITINGMEN kg WOMEN kgSeniors 56 Seniors 48“ 62 “ 53“ 69 “ 58“ 77 “ 63“ 85 “ 69“ 94 “ 75“ 105 “ > 75“ > 105
ASSESSING BODY FAT AND CALORIE DEFICIT
Therefore, whoever wishes to reduce his or her
body weight in the medium term without reducing
efficiency must set eliminating body fat and not
fat-free mass - muscles, glycogen, water, etc. -
as the main goal. It must be borne in mind thou-
gh that just 36-48 hours are necessary to repleni-
sh water and glycogen stores, while it takes much
more time to recover any muscle mass that is
lost. The first step in planning weight loss in an
athlete is the calculation of body fat. There are
various ways to analyze the body's composition,
among which: skin fold caliper test, bioelectri-
cal impedance analysis, methods based on the
use of infrareds, DEXA (Dual-emission X-ray
absorptiometry) and hydrostatic weighing. It is
possible to have an idea of the ideal weight for
the athlete examined if you consider also what
the literature says about body fat in athletes in
specific sports. Now you can determine, for
instance, whether a certain athlete can actually
reach a given body weight (in particular, a weight
that allows him or her to reach a specific weight
class). If the results indicate that it is possible,
you can plan the progressive loss of excess fat
by combining training with diet to reach the
required deficit in the daily energy balance
(Kinney, 2004). Having said as much, it is clear
that the time factor is essential in planning a
reduction in body weight (Golay, 2000).
According to Orlandi (2009), the energy balance
restrictions - compared to what are the actual
calorie needs regardless of the limits that calories
have as a reference - can be divided into three
different levels:
• daily deficit of 1000 kcal or more: it can have
damaging effects on athletic performance and
should not be considered at all (Giorgino, 1979;
Arioli, 2009);
• daily deficit between 500 and 1000 kcal a day:
this level of restriction can be effective only in
specific situations and in specific athletes;
• daily deficit of less than 500 kcal a day: by far,
this is the preferred level for athletes, especially
because it gives a reduction in body weight that
6
Table 2 - Worsening in performance in marathon running, inminutes and seconds, based on finish time and body weightwhen - all other conditions being the same - there is a 1 kgincrease in body fat (Arcelli, 1990).

can be more easily achieved through the loss of
body fat alone (i.e., without altering the subject's
muscle mass).
QUALITY AND QUANTITY OF CARBOHYDRATES
Still, despite the calorie deficit, an athlete who
wishes to lose weight should never suffer a lack of
nutrients. In particular, the intake of proteins and
carbohydrates must never fall below certain daily
quantities. Athletes engaged in intense training
must have a protein intake of around 1.5-2
g/kg/day in order to avoid having a negative
protein balance (Tarnopolsky et al., 1988;
Chesley et al., 1992; Lemon et al., 1992.)
Protein breakdown can exceed protein synthe-
sis, which can lead to a loss of lean body mass,
even when there is a sharp drop in carbohydra-
tes in the diet. Therefore, athletes must always
rely on a minimum daily intake calculated as the
sum of:
• quantity of carbohydrates needed by the cen-
tral nervous system and other tissues and
organs that do not have their own energy reser-
ves (about 1 g every kg of body weight or slightly
more);
• quantity of carbohydrates consumed by
muscles during physical activity (to be calcula-
ted individually for each athlete).
If these quantities are not reached, the body must
produce glucose through gluconeogenesis, a pro-
cess that entails the breakdown of body proteins
and the use of the branched-chain amino acids
that they contain. The final result is a reduction in
lean body mass and especially in muscle proteins.
On the other hand, the choice of what types of car-
bohydrates should be eaten is also extremely
important. The weight loss phase can last several
months and the time during which the resulting
body weight needs to be maintained can be much
longer. Hence, you need to bear in mind that
during these periods there are two main factors
that counter diet maintenance: a drop in the
resting metabolic rate and an increase in appetite.
Generally speaking, there is no drop in resting
metabolic rate during weight loss - at least in
most athletes who regularly do a lot of training;
there can be, however, an increase in appetite
during diet restriction phases. When choosing
foods, you need to consider not only their calorie
content (the only element considered in the past),
but also the capacity of given foods to increase
appetite more or less quickly.
7
As for carbohydrates, you should especially
choose those with a low glycemic index (see
Sport Nutrition Report 1, 2010, pg. 6-12); the
quantities should always involve a moderate
glycemic load. A high glycemic load would make
the levels of insulin in the blood rise; hyperinsu-
linemia favors an increase in the fat contained in
adipocytes, but also leads to an early onset of
appetite (Sears, 2006) as a consequence of the
rapid drop in blood glucose to below baseline
levels, which takes the name of reactive hypo-
glycemia.
Among the foods that supply carbohydrates,
those with a low glycemic index often have a low
caloric density; that is to say they supply few
calories while having the same weight (and/or
volume). Being free to eat as much food as one
likes while having to eat mostly those with a low
caloric density, such as vegetables (and even
genuine whole-grain cereals) allows subjects to
lose weight more easily without any sort of defi-
ciency (Poppit and Prentice, 1996; Rolls and
Bell, 1999).
THE ROLE OF PROTEINS AND HORMONES
Proteins, unlike carbohydrates with a high
glycemic index, favor satiety. According to
Paddon-Jones et al. (2008), it is important for
anyone who wishes to lose weight to eat a reaso-
nable amount of proteins at every meal because
they: (a) promote maintenance of lean body mass,
(b) increase energy expenditure (thermal effect of
foods) and (c) increase the feeling of fullness.
As for fullness, first of all, it should be considered
(see box at pg. 10) that you have short-term full-
ness (or satiation) that occurs while you are still
eating (or immediately after) and long-term full-
ness (or satiety), which refers to a longer period
of time without appetite in the hours following
your last meal. Besides psychological factors or
other more complex factors, there are over
twenty peptide hormones that act on the various
centers in the hypothalamus that modulate hun-
ger and satiety. Among these hormones, suffice it
to mention the following four that favor satiation
or satiety, either indirectly (by acting on the
receptors of the vagus nerve, which, in turn, is
connected to the hypothalamus), or directly once
they reach the hypothalamus through circulation:
• PP (pancreatic polypeptide): gastric distension
leads to its production by the pancreas in the
cells arranged along the edges of the islets of
Langerhans; its levels remain high only for few
hours;
8
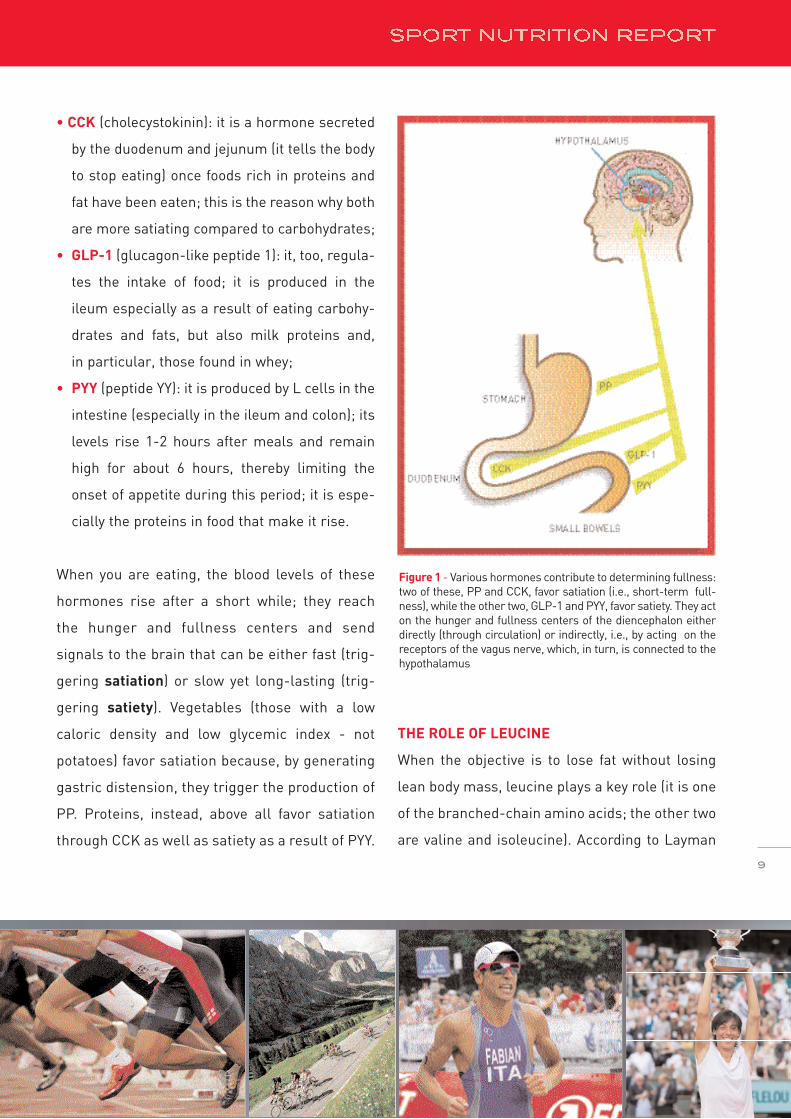
• CCK (cholecystokinin): it is a hormone secreted
by the duodenum and jejunum (it tells the body
to stop eating) once foods rich in proteins and
fat have been eaten; this is the reason why both
are more satiating compared to carbohydrates;
• GLP-1 (glucagon-like peptide 1): it, too, regula-
tes the intake of food; it is produced in the
ileum especially as a result of eating carbohy-
drates and fats, but also milk proteins and,
in particular, those found in whey;
• PYY (peptide YY): it is produced by L cells in the
intestine (especially in the ileum and colon); its
levels rise 1-2 hours after meals and remain
high for about 6 hours, thereby limiting the
onset of appetite during this period; it is espe-
cially the proteins in food that make it rise.
When you are eating, the blood levels of these
hormones rise after a short while; they reach
the hunger and fullness centers and send
signals to the brain that can be either fast (trig-
gering satiation) or slow yet long-lasting (trig-
gering satiety). Vegetables (those with a low
caloric density and low glycemic index - not
potatoes) favor satiation because, by generating
gastric distension, they trigger the production of
PP. Proteins, instead, above all favor satiation
through CCK as well as satiety as a result of PYY.
THE ROLE OF LEUCINE
When the objective is to lose fat without losing
lean body mass, leucine plays a key role (it is one
of the branched-chain amino acids; the other two
are valine and isoleucine). According to Layman
9
Figure 1 - Various hormones contribute to determining fullness:two of these, PP and CCK, favor satiation (i.e., short-term full-ness), while the other two, GLP-1 and PYY, favor satiety. They acton the hunger and fullness centers of the diencephalon eitherdirectly (through circulation) or indirectly, i.e., by acting on thereceptors of the vagus nerve, which, in turn, is connected to thehypothalamus

(2009), if a lot of carbohydrates are consumed,
especially those with a high glycemic index, the
fat accumulated in adipocytes tends to increase,
while the intake of a certain quantity of leucine
helps lose weight and maintain muscle mass.
Leucine has a double action: on the one hand, it
acts on the hypothalamus and triggers the
feeling of satiety (Cota et al., 2006; Zhang et al.
2007); on the other, it acts on muscles, thereby
favoring hypertrophy. In both cases, leucine's
action takes place thanks to the intervention of
m-TOR (Morrison et al., 2007). In order to lose
fatty tissue only and ensure total well-being,
according to Layman (2009), each main meal
should include a quantity of at least 30 g of
proteins, which is equal to about 2.5 g of leucine
if the proteins are of good quality.
This way, the concentration of leucine in blood
reaches the limits needed to stimulate weight
loss without losing muscle mass. On the con-
trary, carbohydrates should be less than 40 g
(Layman, 2009).
CONCLUSIONS
When an athlete wishes to lose weight, it is
important to determine - well outside the compe-
titive season - which weight loss targets can be
reasonably achieved and how long it will take to
reach these targets.
The choice of the diet to be followed must
undoubtedly be customized, considering the
principles discussed in this article. A regimen
such as the Zone diet seems to be very suitable to
reach these goals.
10
There are two forms of fullness wich are defined as
satiation and satiety.
Satiation is the short-term fullness that develops
during meals. When the stomach is full, the nerve
"sensors" on its walls send signals that stimulate
the secretion and circulation of PP, a hormone that
reduces appetite.
Satiety refers to long-term fullness, namely that
fullness that lasts several hours and keeps the fee-
ling of hunger from returning. If you reach the time
of the next meal without feeling too hungry, you eat
less. In general, foods rich in proteins - having the
same amount of calories - give longer satiety com-
pared to foods rich in carbohydrates.
SATIATION E SATIETY

REFERENCES
Arcelli E.: Che cos’è l’allenamento. Sperling & Kupfer Editori, Milan,1990.
Artioli G.G., Iglesias R.T., Franchini E., Gualano B., KashiwaguraD.B., Solis M.Y., Benatti F.B., Fuchs M., Lancia A.H. jr.: Rapid weight-loss followed by recovery time does not affect judo-related perfor-mance. J. Sports Sci., 23: 1-12, 2009.
Chesley A, MacDougall JD, Tarnopolsky MA, Atkinson SA, Smith K.Changes in human muscle protein synthesis after resistance exerci-se. J Appl Physiol., 73(4): 1383-1388, 1992.
Cota D., Proulx K., Smith K.A., Kozma S.C., Thomas G., Woods S.C.,Seeley R.J.: Hypothalamic mTOR signaling regulates food intake.Science, May, 12, 312 (5775): 927-930, 2006.
Equipe Enervit: Indice e carico glicemico. In “Sport Nutrition Report2010”, pg. 6-12, 2010.
Giorgino R., Scaldapane R., Lattanzi V., Cignarelli M., Various typesof reducing diets. Minerva Med., 70 (51): 3475-3491, 1979.
Kinney J.M.: Nutritional frailty, sarcopenia and falls in the elderly.Curr. Opin. Clin. Nutr. Metab. Care, 7 (1): 15-20, 2004.
Layman D.K. : Dietary Guidelines should reflect new understandingsabout adult protein needs. Nutr. Metab. (London).: Mar 13;6:12,2009.
Lemon PW, Tarnopolsky MA, MacDougall JD, Atkinson SA. Proteinrequirements and muscle mass/strength changes during intensivetraining in novice bodybuilders. J Appl Physiol., 73 (2): 767–775,1992.
Margaria R.: Sulla fisiologia e specialmente sul consumo energeticodella marcia e della corsa. Atti Accademia Nazionale dei Lincei,1938, serie VI, 72-99.
Morrison C.D., Xi X., White C.L., Ye J., Martin R.J..: Amino acids inhi-bit Agrp gene expression via an mTOR-dependent mechanism. Am JPhysiol Endocrinol Metab., Jul, 293(1): E165-171. 2007.
Orlandi C.: Gestione e controllo del peso e della muscolatura dell'a-tleta, Convegno Nazionale SIAS – Palermo, 13-14 novembre 2009.
Paddon-Jones D., Westman E., Mattes R.D., Wolfe R.R., Astrup A.,Westerterp-Plantenga M.: Protein, weight management, and satiety.Am. J. Clin Nutr., 87 (5): 1558S-1561S, 2008.
Poppitt S.D, Prentice A.M.: Energy density and its role in the controlof food intake: evidence from metabolic and community studies.Appetite, 26(2):153-174, 1996.
Rolls B.J., Bell E.A.: Intake of fat and carbohydrate: role of energydensity. Eur. J. Clin. Nutr., 53: S166-173, 1999.
Sears B.: Prevenire con la zona. Sperling & Kupfer editori, Milan,2006.
Tarnopolsky M.A., MacDougall J.D., Atkinson S.A.: Influence of pro-tein intake and training status on nitrogen balance and lean bodymass. J Appl Physiol., 64 (1): 187-193, 1988.
Zhang Y., Guo K., LeBlanc R.E., Loh D., Schwartz G.J., Yu Y.H.:Increasing dietary leucine intake reduces diet-induced obesity andimproves glucose and cholesterol metabolism in mice via multime-chanisms. Diabetes, Jun, 56 (6): 1647-1654, 2007.
11

Soy is a legume native to Asia; for many Asian
populations it has been a staple foodstuff for
over 5,000 years. Compared to other legumes, it
is easier to digest and richer in proteins: in soy-
beans, proteins account for over 35% of the dry
weight. They have a good amino acid profile with
a biological value near 75.
It should be borne in mind that the proteins iso-
lated from soy are much more effective compa-
red to the proteins ingested with the whole bean
or with soy-based foods. Thanks to the high con-
tent of glutamine, arginine and branched chain
amino acids as well as to new extraction and
processing methods, they have a higher protein
quality score in the new index (PDCAAS) develo-
ped by the World Health Organization (WHO).
The PDCAAS (Protein Digestibility Corrected
Amino Acid Score), adopted by the FDA - Food
and Drug Administration - and FAO, classifies
protein quality considering both the content of
amino acids and digestibility. The maximum
PDCAAS score is 1.0; it is given only to casein,
whey proteins, the proteins of whole eggs, albu-
men proteins and, indeed, the proteins isolated
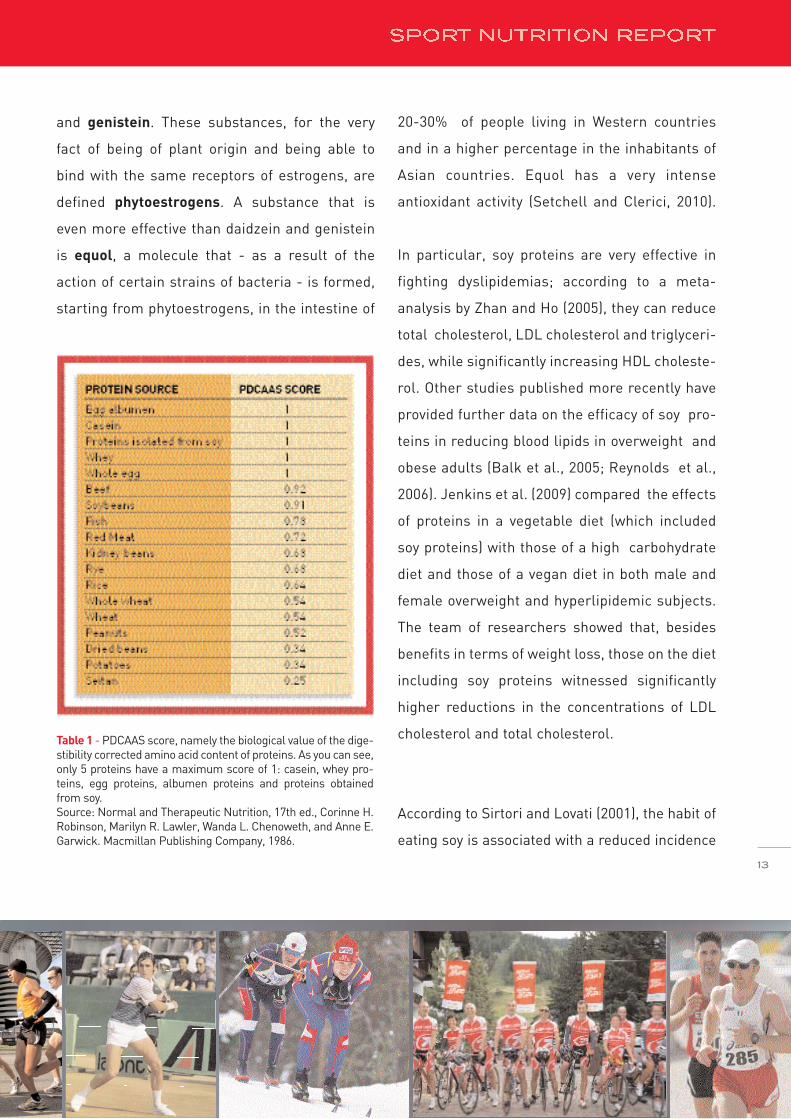
from soy (see Table 1). Beef has a score of 0.92,
followed by soybeans with 0.91; then come kid-
ney beans and rye (0.68), whole wheat (0.54),
lentils and peanuts (0.52); at the bottom of the
ranking you find seitan, which is composed of
wheat- derived proteins, with a score of 0.25.
Several epidemiological studies have shown that
people who regularly consume a higher quantity
of soy-based foods have a lower risk of develo-
ping some pathologies. The beneficial effects of
soy proteins are mainly associated with the pre-
sence of isoflavons and, in particular, daidzein
- 2 -
soy proteins
in weight loss and sports
12
and genistein. These substances, for the very
fact of being of plant origin and being able to
bind with the same receptors of estrogens, are
defined phytoestrogens. A substance that is
even more effective than daidzein and genistein
is equol, a molecule that - as a result of the
action of certain strains of bacteria - is formed,
starting from phytoestrogens, in the intestine of
20-30% of people living in Western countries
and in a higher percentage in the inhabitants of
Asian countries. Equol has a very intense
antioxidant activity (Setchell and Clerici, 2010).
In particular, soy proteins are very effective in
fighting dyslipidemias; according to a meta-
analysis by Zhan and Ho (2005), they can reduce
total cholesterol, LDL cholesterol and triglyceri-
des, while significantly increasing HDL choleste-
rol. Other studies published more recently have
provided further data on the efficacy of soy pro-
teins in reducing blood lipids in overweight and
obese adults (Balk et al., 2005; Reynolds et al.,
2006). Jenkins et al. (2009) compared the effects
of proteins in a vegetable diet (which included
soy proteins) with those of a high carbohydrate
diet and those of a vegan diet in both male and
female overweight and hyperlipidemic subjects.
The team of researchers showed that, besides
benefits in terms of weight loss, those on the diet
including soy proteins witnessed significantly
higher reductions in the concentrations of LDL
cholesterol and total cholesterol.
According to Sirtori and Lovati (2001), the habit of
eating soy is associated with a reduced incidence
13
Table 1 - PDCAAS score, namely the biological value of the dige-stibility corrected amino acid content of proteins. As you can see,only 5 proteins have a maximum score of 1: casein, whey pro-teins, egg proteins, albumen proteins and proteins obtainedfrom soy.Source: Normal and Therapeutic Nutrition, 17th ed., Corinne H.Robinson, Marilyn R. Lawler, Wanda L. Chenoweth, and Anne E.Garwick. Macmillan Publishing Company, 1986.

of cardiovascular diseases. Already back in 1999,
even the U.S. Food and Drug Administration
authorized that the following wording be put on
the labels of products containing soy proteins: “25
grams of soy protein a day, as part of a diet low in
unsaturated fat and cholesterol, may reduce the
risk of heart disease." Soy phytoestrogens are
similarly capable of influencing enzymes involved
in the regulation of cellular proliferation, thereby
inhibiting the increase in the number of neopla-
stic cells; for this reason, the regular consump-
tion of soy reduces the risk of some forms of can-
cer such as colon cancer (Bennink, 2001), prostate
cancer (Rowland, 2004; Hwang et al., 2009) and
breast cancer (Wu et al., 2008). Moreover, in
women, soy reduces the disorders associated
with menopause and the risk of osteoporosis
(Alekel et al., 2000; Scheiber et al., 2001;
Lydeking-Olsen et al., 2004). Soy proteins also
have antioxidant properties (Park et al., 2010) and
very beneficial effects on type-2 diabetes, espe-
cially in women in menopause (Jayagopal et al.,
2002). Another recent study (Pipe et al., 2009) on
men and women with type-2 diabetes has compa-
red the effects of the proteins isolated in milk and
the proteins isolated in soy and has shown that
with soy proteins the levels of LDL cholesterol are
significantly reduced.
SOY PROTEINS AND WEIGHT LOSS
Soy proteins have the ability to generate a greater
feeling of satiety compared with other widely
consumed high-quality proteins (Anderson et al.,
2004; Semon et al., 1987). Their main component
is beta-conglycinin, a peptone that, as proven by
studies on animals, is very effective in stimulating
the release of cholecystokinin (CCK), a hormone
that triggers satiety (Nishi et al., 2003). For this
reason, adding soy proteins to weight loss diets
aimed solely to reduce body fat is considered to be
an effective method to improve the feeling of
satiety, weight control and diet quality.
The role of soy proteins in weight loss has been
the subject of three recently published articles
(Westerterp-Plantenga et al., 2009; Cope et al.,
2008; Velasquez et al., 2007). These articles
argue that when hypocaloric diets - followed by
adults to reduce body fat and control weight - are
based mainly on the consumption of soy proteins,
the effects are equivalent to those of diets based
on the intake of other types of proteins. These
benefits are probably due in part to the metabo-
lic effects of soy on the metabolism of glucose
and lipids (Veldhorst et al., 2009). However, no
study has been carried out to investigate into the
effect of hypocaloric diets containing soy proteins
14

15
in children. It has been observed that soy proteins
can reduce weight and body fat even in rats and
mice (Nagasawa et al., 2002; Iritani et al., 1996).
There is also clear evidence that, in case of wei-
ght loss, diets with a high protein content and
particularly those containing high-quality pro-
teins help to preserve fat-free mass (FFM)
(Noakes, 2008; Layman, 2004). In turn, this
improves the metabolic profile of the diet and
increases the reduction in insulin levels and the
size of LDL particles (Westerterp-Plantenga et
al., 2007).
Several studies have proven that in adults, during
a period of planned weight loss, soy proteins pre-
serve fat-free mass just as well as dairy products
and mixed protein sources (Li et al., 2005;
Lukaszuk et al., 2007; Anderson et al., 2007; St-
Onge et al., 2007). While, on the one hand, the
mechanisms of this effect are not entirely clear
yet, on the other, it has been suggested that
these actions are the result of hormonal respon-
ses to an increased intake of proteins and/or a
reduced intake of carbohydrates (Westerterp-
Plantenga et al., 2007; Layman, 2003).
Table 2
THE BENEFITS OF SOY
Soy provides proteins in greater quantities and with
a better quality compared to other plants;
provides healthier lipids, such as monounsaturated
fats, polyunsaturated fats and phospholipids such as
lecithin;
provides less saturated fats and less cholesterol;
has a lower glycemic index: for a mixed composi-
tion, the glycemic index is 18 (as opposed to 100 for
glucose);
favors a balanced diet: the properties and compo-
nents of soy are beneficial to balanced nutrition;
is a good source of vitamins and minerals, and par-
ticularly vitamin E, iron and potassium;
helps bring down the level of cholesterol in blood,
thanks to the action of phytosterols as well as of
lecithin, a substance that also acts on circulation by
keeping cholesterol suspended and not allowing it to
build up on arterial walls;
regulates satiety, as proven by recent scientific
research;
acts on fat-free mass: many studies have documen-
ted the benefits of proteins obtained from soy on the
increase in fat-free mass;
mitigates the disorders associated with the men-
strual cycle and menopause in women: soy isofla-
vons rebalance both excess estrogens, which are the
cause of the premenstrual syndrome and the lack of
estrogens during menopause by restoring the cor-
rect hormonal levels;
lowers the incidence of colon, breast and prostate
cancer;
helps prevent osteoporosis.

SOY AND EXERCISE
Some data in scientific literature suggests that
soy proteins can be a useful nutritional supple-
ment to compensate the needs of a training pro-
gram (Brown et al, 2004; Candow et al., 2006;
Lukaszuk et al., 2007; Philips et al., 2009).
Soy proteins as a part of diet have the ability to
influence physical performance for a series of
reasons, particularly due to the high intake of
high-quality proteins and elements with a phyto-
chemical effect, such as isoflavons, and to the
action of some peptides that are formed during
digestion. A series of studies carried out by the
Ohio State University have shown that the con-
sumption of 40 g of soy proteins every day for
3-4 weeks can improve post-training recovery by
accelerating the recovery of muscle functions
that were involved in physical exercises and by
inhibiting muscle soreness (Rossi et al., 2000;
Hill et al., 2004; Box et al., 2006). Studies have
also assessed the inflammatory state, oxidative
stress and muscular damage in blood tests.
Another interesting finding regards the intake of
soy proteins, which after training have led to
a partial reduction in blood levels of cortisol,
a hormone correlated with stress (Disilvestro,
2005). Besides these effects, soy proteins favor
post-training recovery and increase muscle
mass and strength through stimulation during
training (Bazzoli, 2002). A study carried out on
women who regularly did aerobic exercise and
had an intake of 40 g of soy proteins over a
period of 4 weeks showed that oxidative stress
was sharply reduced, while this was not the case
in the control group, which had consumed only
whey proteins.
Many athletes tend to avoid soy proteins becau-
se they think that their biological value and effi-
cacy are lower than whey proteins when it comes
to increasing muscle mass. Research has shown
that, in actual fact, soy proteins and the associa-
ted antioxidants can contribute to increasing fat-
free mass (Kalman et al., 2007). Antioxidants are
agents that are either exogenous, namely absor-
bed through a correct diet, or endogenous, i.e.,
produced by the body (Rossi et al., 2000). They
act against the muscle damage caused by the
oxidant reactions of free radicals. The benefit of
the proteins isolated from soy is that they con-
tain a mix of antioxidants, among which isofla-
vons, saponins and copper. The latter is an
essential component in a number of antioxidant
enzymes (Box et al., 2006). The production of
free radicals by the body is especially intense
16

during exercise and the resulting oxidative
stress seems to contribute to muscle damage
and fatigue (Hill et al., 2004). Said damage and
sense of fatigue could slow down muscle reco-
very between training sessions thereby reducing
the progress made during physical training. As a
consequence the increase in fat-free mass
promoted by a specific training program could
be limited.
This has been confirmed in a research study to
assess the increase in lean body mass in two
groups of university students (Disilvestro, 2005).
They associated overload training with the con-
sumption of protein bars; in one group the bars
contained soy proteins, while in the other they
contained whey proteins. Both groups showed
an increase in fat-free mass, but the data collec-
ted in the phases following exercise demonstra-
ted that the group that consumed only whey pro-
teins showed the presence of perioxidative fac-
tors.
Table 3
THE BENEFITS OF SOY IN SPORTS
Soy proteins:
• favor the loss of body fat, without losing effi-
ciency, in athletes who need to lose weight;
• favor the increase of muscle mass and
strength;
• allow, in the same training conditions, the
reduction of inflammation and oxidative
stress; cortisol levels are also lower;
• favor recovery in the phase following trai-
ning; there are less muscle aches and less
fatigue.
17

REFERENCES
Alekel D.L., Germain A.S., Peterson C.T., Hanson K.B., Steward J.W.,Toda T.: Isoflavone-rich soy protein isolate attenuates bone loss inthe lumbar spine of perimenopausal women. Am J Clin Nutr, 72 (3):844-852, 2000.
Anderson J., Fuller J., Patterson K., Blair R., Tabor A.: Soy compa-red to casein meal replacement shakes with energy-restricted dietsfor obese women: randomized controlled trial. Metabolism, 56:280-8, 2007.
Anderson G., Moore S.: Dietary proteins in the regulation of foodintake and body weight in humans. J Nutr, 134:974S-9S, 2004.
Anthony T.G., McDaniel B.J., Knoll P., Bunpo P., Paul G.L., McNurlanM.A.: Feeding meals containing soy or whey protein after exercisestimulates protein synthesis and translation initiation in the skeletalmuscle of male rats. J Nutr137:357-362, 2007.
Astrup A.: The satiating power of protein - a key to obesity preven-tion? Am J Clin Nutr, 82:1-2, 2005.
Balk E., Chung M., Chew P., Ip S., Raman G., Kupelnick B., TatsioniA., Sun Y., Wolk B., Devine D., Lau J.: Effects of soy on health outco-mes. Agency for Healthcare Research and Quality: Evidence Report/Technical Assessment (Summary) 126:1-8, 2005.
Bazzoli D.L., Hill S., DiSilvestro R.A.: Soy Antioxidant Actions inActive, Young Adult Women. Nutr Res 22:807-815, 2002.
Bennink M.R.: Dietary soy reduces colon carcinogenesis in humanand rats. Soy and colon cancer. Adv Exp Med Biol, 492: 11-17, 2001.
Box W., Hill S., DiSilvestro R.A.: Soy intake plus moderate weightresistance exercise: effects on plasma concentrations of lipidperoxides in young adult women. J Sports Med Phys Fitness 45:524-528, 2006.
Candow D.G., Burke N.C., Smith-Palmer T., Burke D.G.: Effect ofwhey and soy protein supplementation combined with resistancetraining in young adults. Int J Sport Nutr Exerc Metab 16:233-244,2006.
DiSilvestro R.A., Brown E.C., Devor S.T.: Soy and whey effects on leanbody mass and plasma antioxidant status when combined with aweight training program. Nutr J 3:22-26, 2005.
DiSilvestro R.A., Goodman J., Dy E., Joseph E.: Soy extract increases erythrocyte superoxide dismutase activities in breast cancer
survivors. Br Cancer Treat Res 89:251-255, 2005.
Harland J.I. and Haffner T.A.: Systematic review, trials reporting anassociation between an intake of circa 25 g soya protein per day andblood cholesterol. Atherosclerosis 200:13-27, 2008.
Hill S., Box W., DiSilvestro R.A.: Moderate intensity resistance exer-cise, plus or minus soy intake: effects on serum lipid peroxides inyoung adult males. Int J Sport Nutr Exer Metab 14:125-132, 2004.
Hwang Y.W., Kim S.Y., Jee S.H., Kim Y.N., Nam C.M.: Soy food con-sumption and risk of prostate cancer: a meta-analysis of observatio-nal studies. Nutr Cancer, 61 (5): 598-606, 2009.
Iritani N., Hosomi H., Fukuda H., Tada K., Ikeda H.: Soybean proteinsuppresses hepatic lipogenic enzyme gene expression in Wistarfatty rats. J Nutr 1996;126:380-8, 1996.
Jayagopal V., Albertazzi P., Kilpatrick E.S., Howarth E.M., JenningsP.E., Hepburn D.A., Atkin S.L.: Beneficial effects of soy phytoestro-gen intake in postmenopausal women with type 2 diabetes.Diabetes Care, 25 (10): 1709-1714, 2002.
Jenkins D., Wong J., Kendall C., Esfahani A., Ng V., Leong T.,Faulkner D., Vidgen E., Greaves K., Paul G.: Singer W. The effect of aplant-based lowcarbohydrate (“Eco-Atkins”) diet on body weight andblood lipid concentrations in hyperlipidemic subjects. Arch Int Med169(11):1046-54, 2009.
Kalman D., Feldman S., Martinez M., Krieger D.R., Tallon M.J.: Effectof protein source and resistance training on body composition andsex hormones. J Int Soc Sports Nutr 4:4, 2007.
Layman D.K.: Protein quantity and quality at levels above the RDAimproves adult weight loss. J Am Coll Nutr, 23:631S-6S, 2004.
Layman D.K.: The role of leucine in weight loss diets and glucosehomeostasis. J Nutr, 133:261S-7S, 2003.
Li Z., Hong K., Saltsman P., Deshields S., Bellman M., Thames G.,Liu Y., Wang H.J., Elashoff R., Heber D.: Long-term efficacy of soy-based meal replacements vs an individualized diet plan in obesetype II DM patients: relative effects on weight loss, metabolic para-meters, and C-reactive protein. Eur J Clin Nutr, 59:411-8, 2005.
Lukaszuk, J.M., Luebbers, P. & Gordon B.A.: Preliminary study: soymilk as effective as skim milk in promoting weight loss. J Am DietAssoc, 107: 1811-14, 2007.
18

Lydeking-Olsen E., Beck-Jensen J.E., Setchell K.D., Holm-JensenT.: Soymilk or progesterone for prevention of bone loss-a 2 year ran-domized, placebo-controlled trial. Eur J Nutr, 43 (4): 246-257, 2004.
Nagasawa A., Fukui K., Funahashi T., Maeda N., Shmomura I.,Kihara S., Waki M., Takamatsu K., Matsuzawa Y.: Effects of soy pro-tein diet on the expression of adipose genes and plasma adiponec-tin. Horm Metab Res, 34:635-9, 2002.
Nishi T., Hara H., Tomita F.: Soybean beta-conglycinin peptone sup-presses food intake and gastric emptying by increasing plasma cho-lecystokinin levels in rats. J Nutr, 133:352-7, 2003.
Noakes M.: The role of protein in weight management. Asia Pac JClin Nutr, 17 Suppl 1:169-71, 2008.
Park C.E., Yun H., Lee E.B., Min B.I., Bae H., Choe W., Kang I., KimS.S., Ha J.: The antioxidant effects of genistein are associated withAMP-activated protein kinase activation and PTEN induction in pro-state cancer cells. J Med Food, 13 (4): 815-820, 2010.
Pipe E., Gobert C., Capes S., Darlington G., Lampe J., Duncan A.: Soyprotein reduces serum LDL cholesterol and the LDL choleste-rol:HDL cholesterol and apolipoprotein B:apolipoprotein A-1 ratiosin adults with type 2 diabetes. J Nutr, July 15, 2009.
Reynolds K., Chin A., Lees K.A., Nguyen A., Bujnowski D., He J.: Ameta-analysis of the effect of soy protein supplementation on serumlipids. Am J Cardiol 98:633-40, 2006.
Rossi A.L., Blostein-Fujii A., DiSilvestro R.A.: Soy beverage con-sumption by young men: increased plasma total antioxidant statusand decreased acute, exercise-induced muscle damage.J Nutraceuticals Funct Med Foods 3:33-44, 2000.
Rowland I.: Soy and prostate cancer. Atti del convegno “Soy andhealth 2004”, Bruges, 7-8 ottobre 2004.
Scheiber M.D., Liu J.H., Subbiah M.T., Rebar R.W., Setchell K.D.:Dietary inclusion of whole soy foods results in significant reductionsin clinical risk factors for osteoporosis and cardiovascular disease innormal postmenopausal women. Menopause, 8(5): 384-392, 2001.
Semon B.A., Leung P.M., Rogers Q.R., Gietzen D.W.: Effect of type ofprotein on food intake of rats fed high protein diets. Physiol Behav,41:451-8, 1987.
Setchell K.D., Clerici C.: Equol: history, chemistry, and formation.J Nutr, 140 (7): 1355S-13662S, 2010.
Sirtori C.R., Lovati MR.: Soy proteins and cardiovascular disease.Curr Atheroscler Rep, 3 (1): 47-53, 2001.
St-Onge M., Claps N., Wolper C., Heymsfield S.: Supplementationwith soy-protein-rich foods does not enhance weight loss. J Am DietAssoc, 107:500-5, 2007.
Velasquez M.T. & Bhathena. S.J.: Role of dietary soy protein in obe-sity. Int J Med Sci, 4:72-82, 2007.
Westerterp-Plantenga M.S., Nieuwenhuizen A., Tome D., Soenen S.,Westerterp K.R.: Dietary protein, weight loss, and weight mainte-nance. Ann Rev Nutr, 29:21-41, 2009.
Westerterp-Plantenga M., Smeets A., Nieuwenhuizen A.: Sustainedprotein intake for body weight management. Nutr Bull, 32:22-31,2007.
Wu A.H., Yu M.C., Tseng C.C., Pike M.C.: Epidemiology of soy expo-sures and breast cancer risk. Br J Cancer, 15, 98 (1): 9-14, 2008.
Zhan S., Ho S.C.: Meta-analysis of the effects of soy protein contai-ning isoflavones on the lipid profile. Am J Clin Nutr, 81:397-408,2005.
19
Water is very important in sports. In several
sports events and particularly in those that last
more than a few dozen minutes and/or that are
held in an environment that leads to abundant
sweating (i.e., with high air temperatures and
high humidity and irradiation levels), it is absolu-
tely essential that athletes reach the start of the
competition without any water deficiency and
that, during the competition, at least part of the
water lost through sweat (and if necessary,
minerals as well) is integrated. Even a moderate
loss of water by the body leads to a sensitive
worsening of performance and, if this loss is
even greater, it can be dangerous to health.
WATER LOSS BY THE BODY
Humans can survive without food for a few
weeks provided that they can drink fluids. They
cannot resist for more than a few days without
water: even when fasting in a cool environment,
humans need a daily intake of more than half a
liter of water. The human body is continuously
losing water, even though there are substantial
differences from one day to another. Save for
pathological cases, the routes through which
water is lost are the kidneys (the quantity of
urine increases when you drink more water than
needed), the digestive system (stools can be
more or less rich in water depending especially
on the food eaten; diarrhea and vomit can sub-
stantially increase the loss of water and mine-
rals), skin (through sweat and insensible perspi-
ration) and the lungs (a substantial amount of
water vapor can be eliminated through the
airway especially above a certain altitude). It
should also be borne in mind that every day the
glands of the stomach and intestine (especially
- 3 -
beverages for athletes
20

in the first section) secrete a large quantity of
fluids, on average between 7 and 10 liters; in
a normal individual, however, these liquids are
almost entirely reabsorbed by the large bowel.
Even in the glomeruli of the kidneys, an enor-
mous quantity of what is called first-intention
urine is produced every day, totaling almost
a few dozen liters. However, if the production of
adiuretin (anti diuretic hormone -ADH) by the
pituitary gland is normal, most of it is reabsor-
bed by renal tubules and only a small quantity
(even less than a liter) becomes urine and is eli-
minated as such by the body.
In order to have a correct (fluid balance), water
loss (output) must be compensated by the intake
of water (input). A substantial part of the input
(exogenous water) does not come from bevera-
ges, but foods. Very few foods are completely
dry, while some fresh foods (fruit, vegetables,
meat, fish…) contain percentages of water of
over 70% or even 90%. In the body, the combu-
stion of carbohydrates, fats and proteins produ-
ces other water called endogenous (or metabo-
lic). Every 100 g of carbohydrates used to produ-
ce energy yields 55 g of water; every 100 g of
lipids gives 107 g; and every 100 g of proteins 41
g. For an accurate calculation of the level of
dehydration in an individual who is engaged in a
prolonged effort that produces a lot of sweat, it
is necessary to take into account endo genous
water as well.
However, according to McArdle, Katch and Katch
(1998), its role is of scarce relevance in the fluid
balance of an athlete.
THIRST
The onset of the feeling of thirst depends on
several factors such as local factors (dryness of
the mucosa of the mouth and pharynx) or psy-
chological factors (watching others drink a beve-
rage, for instance, causes or worsens thirst).
Intense physical activity in an athlete during a
competition, on the contrary, can eliminate or
ease it. That's why when you are sweating inten-
sely during physical activity you need to drink
even if you are not thirsty. Anyhow, the feeling of
thirst depends on centers located in the hypotha-
lamus that regulate the intake of water. These
centers receive information from various recep-
tors such as the osmoreceptors, the volorecep-
tors and baroreceptors. Then there is a hormo-
ne called angiotensin that directly stimulates
thirst centers when there is a drop in the volume
of extracellular fluids. Most of the factors (osmo-
21

receptors, voloreceptors, baroreceptors, angio-
tensin) intervene and stimulate the thirst centers
when conditions in the body have already chan-
ged. In athletes, for instance, this happens when
they have already lost a substantial amount of
sweat that can even exceed 1% of body weight.
The interruption of the stimulus to the thirst cen-
ters by these factors takes place anyway with a
certain delay compared to the moment when,
following thirst, the individual has started to drink.
In some cases the stimulus is blocked only when
the fluids have passed the stomach, reached the
intestine, passed into blood, reached extracellular
fluids and thus redressed the imbalance that
triggered the stimulus in the first place. Dryness
of the oral mucosa, on the other hand, is usually
remedied at the very moment in which an indivi-
dual drinks. This avoids the intake of an excessive
quantity of water as would be the case if you con-
tinued to drink until all the other factors stopped
stimulating the thirst centers. The feeling of a full
stomach and tense stomach walls - such as the
feeling after rapidly drinking a large amount of
water - is another element that leads to the
inhibition of thirst centers.
The thirst stimulus is qualitatively non-specific;
that is to say, it does not provide information on
the type of beverage that an individual should
drink. When a primitive man felt thirst, he had
just one beverage to quench it: water. Nowadays,
however, people feel the same stimulus, but they
can choose from several beverages to quench
thirst and, at the same time, solve any issues of
restoring water and mineral levels.
In the case of an athlete, it is important that these
fluids are integrated as well as possible and,
in order to do so, you need certain knowledge and
experience. Once you have rationally chosen the
type of beverage, thirst can provide useful infor-
mation (though not always very accurate) on the
quantity that an individual should drink of said
beverage. Though there are substantial differen-
ces between one case and another, it can be
stated that the production of about 700 g of sweat
is all that is needed to trigger thirst. It should be
noted that in a sedentary person this is more or
less the quantity of fluid loss that can already lead
to a drop in efficiency, while in athletes the quan-
tity, according to some, is more than double.
THERMAL BALANCE
While performing any type of physical activity,
the muscles involved produce heat (metabolic
heat) and the quantity depends above all on the
22

energy consumed. The environment, too, gives
heat to an athlete's body (irradiated heat) and
particularly the sun, but also hot surfaces such
as tarmac previously warmed by the sun.
However, the increase in body temperature
above certain values reduces the body's perfor-
mance. Fortunately, the body has some mecha-
nisms by means of which - at least until environ-
mental conditions are not too unfavorable - its
temperature can be cooled down (Fig. 1).
Some of these mechanisms consist in the tran-
sformation of the water into vapor that leaves
the body in the form of sweat and, to a much
lesser extent, insensible perspiration (disper-
sion of vapor through skin without the interven-
tion of sweat glands) and also by means of to the
latent heat of vaporization (elimination of water
vapor through the respiratory system). Every
gram of water that leaves the body in the form
vapor burns almost 0.6 kcal. For the purpose of
thermoregulation, maximum efficacy of the three
mechanisms is achieved when air is dry. On the
contrary, when air is humid they are less useful
and, in particular, only a small percentage of
sweat produced can evaporate while the remai-
ning amount soaks clothing or falls to the ground
in drops.
Another two mechanisms (defined as convecti-
ve) are based on the heating of the air in contact
with skin and with the mucosa of the respiratory
system respectively. The film of air that is near
our skin and the air we inhale and exhale is hea-
ted. This way, a part of the body's heat is dispel-
led. The effectiveness of convection reaches its
maximum when there is a great difference (gra-
dient) between air temperature and the tempe-
rature of the skin (or mucosa).
If air temperature is higher than the temperatu-
re of the skin or mucosa (which happens if you
are playing a sport in an environment in which
air temperature is near or above 40°C), theseFig. 1 - Some of the main factors involved in the thermal balan-ce of an athlete engaged in physical activity.
23

mechanisms do not dispel heat from the body,
but actually add heat. Another way to dispel body
heat is what can be defined as conduction,
although the term is not very precise. It occurs
when there is contact between a fluid and the
body, as is the case when you are drenched in
fresh water (just think of sports in water or even
of athletes when they pour water over their
body), run a sponge soaked with water over your
skin, or even when you drink a cool liquid, which,
as it flows in the mouth, jaws, esophagus and
finally the stomach, comes into contact with the
mucosa, which has a temperature higher than
that of the liquid, and yields heat to the liquid
until it reaches the same temperature.
It should be borne in mind that athletes benefit
from a small rise in body temperature (e.g., the
internal temperature rise from the normal 37°C
to 38°C) that occurs during warm-up before trai-
ning or the competition. However, if the tempe-
rature rises even more, there are negative
effects on enzymatic systems and on the proces-
ses that are taking place inside the body (Åstrand
and Rodahl, 1970). An internal body temperature
of more than 40-41 °C can be tolerated for just a
few minutes (Åstrand and Rodahl, 1970) and is
hence incompatible with sports.
SWEAT
Sweat is a saline solution whose composition
varies from one individual to another and even
within the same individual in different situations
(see Table 2). These differences in the concentra-
tion of minerals are linked, among other things,
to the "training" characteristics of the small
organs that produce sweat, namely sweat glands
Fig. 2 - Schematic overview of the production of sweat by a sweatgland, composed of a gland proper and by a duct through whichsweat reaches skin surface. This duct is depicted with a straightline and minimum length, while it actually is not only very long,but it is also wrapped around the gland proper until it forms asort of ball. The sweat gland first produces sweat, which has aconcentration of minerals very similar to that of plasma. Alongthe gland duct, though, electrolytes, especially sodium andchloride, are reabsorbed. In sweat, therefore, these ions have aconcentration that is much lower than in the plasma. This sameconcentration in the sweat of an acclimatized athlete is lowerthan that of a non-acclimatized individual (see Table 2). In thegland duct, calcium and magnesium re-absorption is a bit lowercompared to that of sodium and chlorine; the re-absorption ofpotassium is minimal or none (Arcelli, 1989).
24
(Fig. 2). As soon as it is produced, sweat (which
can be defined as first-intention sweat) has a
concentration of electrolytes that is similar to
that of blood plasma, that is to say it is isotonic.
During the passage through the gland duct,
however, a great amount of electrolytes is reab-
sorbed, especially some of them. The sweat that
reaches the skin’s surface is hypotonic and
contains fewer ions compared to plasma and
extracellular fluids, even less than one-third or
one-fourth of chlorine, sodium, calcium and
magnesium. However, potassium often has a
concentration similar to (or slightly lower than)
its concentration in plasma. It should be borne
in mind that an athlete who trains for a few days
in an environment that causes intense sweating
undergoes a gradual adaptation in the produc-
tion of sweat from at least three points of view:
• the concentration of ions in sweat is lower (see
the values of the last and second-to-last
column in Table 2);
• there is an increase in the body surface wet
with sweat;
• there is an increase - even very significant - in
Main mechanisms by which heat is dispersed from an athlete's body.
• Heat lost through the evaporation of sweat on skin surface (60%).
• Heat lost through diffusion of vapor through skin or insensible perspiration (2%).
• Heat lost through the elimination of vapor through the airways or latent heat of vaporization (6%).
• Heat exchanged by convection between the body surface and ambient air (30%).
• Heat exchanged by convection between air inhaled and airway mucosa (2%).
The values in brackets refer to the percentage contribution of the various heat dispersion mechanisms
during a marathon (Arcelli, 1989). The evaporation of sweat from the skin surface becomes quantitati-
vely more important when air temperature is high (or rather, when the skin-air thermal gradient is
low). The heat exchanged by convection increases when high air humidity makes it more difficult for
sweat to evaporate (see Table 1).
HEAT DISPERSION DURING SPORTS
25
the quantity of sweat secreted by sweat glands
every minute.
The first two factors make it possible, in the
same environmental conditions, to transform a
higher percentage of sweat into water vapor and
to reduce the quantity of sweat that is wasted.
This is beneficial to an athlete because, in order
to dispel the same quantity of heat, a smaller
amount of heat is needed while losing less water
and minerals from the body. The percentage of
sweat that evaporates decreases with the rise in
air humidity (especially in cases in which it is
necessary to rapidly eliminate large quantities of
heat) through the evaporation of sweat (especially,
when air temperature is high and hence heat dis-
sipation through convection is reduced). The
third type of adaptation is also beneficial, it
allows sweat glands to produce a greater quan-
tity of sweat per unit of time. For an athlete who
needs to compete in a hot or hot and moist
climate, another extremely effective mechanism
is the body's ability to resist higher dehydration
rates.
Table 1 - Thermal balance of an athlete.
The thermal balance of an athlete doing physical exercise (B) is given by:
B = M + R - Es - Ep – Er ± Cv - P – Cd
In this formula the various symbols are:
M: metabolic heat, produced by muscles;R: irradiation heat that reaches the body especially with sunrays;Es: heat lost by the body through the evaporation of sweat;Ep: heat lost by the body through insensible perspiration, i.e., through the diffusion of vapor across theskin without the intervention of sweat glands;Er: heat lost through the elimination of water vapor through the airway (latent heat of vaporization);Cv: heat exchanged by convection between the surface of the skin and ambient air - the film of air in con-tact with the skin warms up if air has a temperature below that of the skin (this mechanismdispels heat from the body); if, on the contrary, the air has a very high temperature (near or above 40 °C),it warms the body;P: heat exchanged by convection between air inhaled and airway mucosa;Cd: heat exchanged by conduction, for instance, when the body comes into contact with cold water (eventhe water in a sponge) or when you drink a cool liquid.
26

This too happens after a few days (or few weeks)
of training in an environment that leads to the
production of large quantities of sweat. In this
period, the body's water (which is already greater
in a trained athlete) tends to further increase: in
a trained and acclimatized athlete the quantity
can even be over 5% more than that of a seden-
tary individual with the same percentage of body
fat. Anyhow, it should be stressed that even with
the same level of effort and environmental condi-
tions, the quantity of sweat lost by different ath-
letes differs: in situations in which some produce
less than a liter of sweat per hour, others can
even produce up to 3 liters (Murray, 2000).
Therefore, everyone needs to drink at a schedu-
led frequency according to their own needs
(Nadel, 1980).
DEHYDRATION AND ITS CONSEQUENCES
When an athlete competes in an environment
with high temperatures and high levels of humi-
dity and irradiation, there is a first phase (begin-
ning just a few minutes after the start of activity)
Table 2 - Electrolytes contained in plasma and sweat.
The following are the concentrations of the main electrolytes contained in plasma, in the sweat of an indi-vidual at rest, in the sweat of an athlete who is not used to physical exercise in an environment that leadsto intense sweating (“non-acclimatized athlete”) and, in the last column, in the sweat of a trained athletewho is used to practicing sports in a hot and moist environment (“acclimatized athlete”). It can be clearlyseen that the sweat produced in this last case has sodium and chlorine concentrations (and even calciumand magnesium concentrations) that are between three and four times lower compared to plasma levels.Only the concentration of potassium remains constant or is slightly reduced.
The values are expressed in grams per liter. Horta (1986).
Electrolyte Blood plasma Sweating at rest Non-acclimatized athlete Acclimatized
Sodium 3,25 1,85 1,38 0,92
Chlorine 3,70 3,10 1,50 1,00
Potassium 0,20 0,20 0,20 0,15
Calcium 0,10 0,04 0,04 0,03
Magnesium 0,04 0,01 0,01 0,01
Total 7,29 5,20 3,13 2,11
27

during which there is an increase in the quantity
of blood in the skin due to dilation of blood
vessels in the subcutaneous area and to the
increase in cardiac output. A greater quantity of
(metabolic) heat produced by muscles and possi-
bly of heat absorbed by the body due to irradia-
tion reaches the skin, whose temperature rises,
thereby favoring the dissipation of heat by
convection. As stated above, the greater the diffe-
rence between air temperature and skin surface
temperature, the more effective this heat disper-
sion mechanism is. At the same time, there is an
increase in the production of sweat, which is the
prerequisite for increased heat dispersion through
the evaporation of water in this saline solution at
skin level. However, when the body has lost a
large amount of sweat (depending on the degree
of acclimatization, there are differences between
one athlete and another in the level of dehydra-
tion that can be borne, as already mentioned
above) several changes occur in the body. First of
all, there is a rise in internal body temperature.
After 20-40 minutes (but even less in extreme
climatic conditions), the body's dehydration leads
to a reduction in total blood volume. As for blood,
since sweat is characterized by lower concentra-
tions of plasma electrolytes, it witnesses an
increase in the concentration of minerals and
some of them in particular. This imbalance can
lead to muscle cramps, especially in individuals
who have a predisposition and/or are less trained.
Still, if an athlete continues to maintain a high
intensity of effort and does not provide for
adequate rehydration, the consequences can
affect the entire body. At a certain point, the body
reduces the production of sweat; at the same
time, it reduces the quantity of blood that reaches
the skin. The possible purpose of these two adap-
tations is that the latter is an attempt to allow as
much circulating blood as possible to reach the
most important organs for the survival of the body
(central nervous system and heart). However,
both the reduction in sweat produced and the
decrease in the supply of blood to skin reduce the
body's ability to dispel heat. Body temperature
can rise to above 41°C. In this case, heatstroke
ensues. At the same time, there can be a drop in
blood pressure, especially due to a reduction in
blood volume. All this makes it extremely difficult
- and dangerous to health - to continue the effort.
In U.S. football (a sport in which, among other
things, players wear gear to protect them against
injuries but which makes heat dispersion more
difficult) there have been cases of death (even
among young children) during practice in hot and
28

moist climates - in most cases, the coach had
prohibited players from drinking.
In athletes who recover most of the water lost,
these negative effects do not occur and, if they do,
they are greatly mitigated: the temperature rises
less (if the beverage is cool, the conduction
mechanism can cool down the body's temperature
by a few tenths of a degree Celsius); the reduction
in blood volume is more limited; the reduction in
sweating is not as great; cardiac output is not
reduced to the same degree, while heart rate
increases by a lesser degree; the flow of blood to
the skin remains high; and so on. Acclimatization,
too, plays an important role in that the negative
effects discussed above occur later on.
RESTORING WATER AND MINERALS
The foregoing implies that when climate condi-
tions are such that there is a major production of
sweat it is absolutely necessary to drink before
and/or during and/or after a competition or trai-
ning session, depending on the characteristics of
the effort. It is important to choose the most
appropriate beverage, and this is especially true
for the beverage drunk just before or during the
physical effort: it must remain in the stomach for
as short a time as possible and it must be rapidly
absorbed in the intestine. If it is known before
starting physical exercise that it will last more
than a few dozen minutes and lead to intense
sweating (high levels of air temperature, humidity
and solar irradiation), it is important to drink
more than usual, especially in unfamiliar condi-
tions.
Some associations recommend drinking before
sports activities. The American College of Sports
Medicine (1996) recommends drinking about 500
mL of fluids two hours before physical activity to
favor adequate hydration and have enough time to
eliminate excess fluids. The recommendation of
the American Dietetics Association (2000) is very
similar: 400 to 600 mL of fluids two hours before
physical exercise. The National Athletic Training
Association (2000) states that, in order to ensure
adequate pre-exercise hydration, athletes should
drink about 500-600 mL of water or a sports
drink, 2-3 hours before exercise and 200-300 mL
of water or sports drink 10-20 min before the
start of the competition.
At any rate, the quantity of fluids that should be
drunk as soon as the warm-up is completed
and before the start of the effort depends on
29

30
the ability to support the presence of the beve-
rage in the stomach without feeling discomfort.
It also depends on the type of effort involved.
Running, for instance, implies vertical jolts at
every step and hence concentrated beverages
are not indicated, as, on the other hand, they are
for cycling.
As regards the quantities of fluids that can be
taken during exercise, the American Dietetics
Association (2000) recommends drinking
between 150 and 350 mL at intervals of 15-20
min, while the National Athletic Training
Association (2000) states that fluid replacement
must be equal to the quantity lost through urine
and sweat, thereby limiting weight loss to less
than 2%; in general, this can be achieved with
200 to 300 mL of fluids every 10-20 min.
It is impossible, though, to indicate precise
quantities for every athlete, because the volume
of fluids to be drunk depends on the volume of
Many years ago Jacobs (1980) had already stated
that dehydration does not seem to have a negative
impact on performances of less than 60 seconds;
there is no effect on results in sprints, throws,
weight-lifting and so on. It can actually be surmi-
sed that in trials having a very short duration,
during which it is advantageous to have a lower
body weight (for instance, high jump), being
slightly dehydrated can be an advantage. In conti-
nuous competitions lasting more than a minute or
in most cases over 10-15 min, be they cyclic (run-
ning, race walking, cycling…), or acyclic (tennis,
team sports…), the loss of water can have negati-
ve consequences on performance when it exceeds
certain quantities. For instance, every liter of
water lost corresponds to an increase in heart
rate (about 8 bpm), a drop in cardiac output and a
rise in internal temperature by about 0.3°C. These
elements help explain how a careful management
of hydration - before and during a competition -
can affect the performance of athletes in these
sports in climate conditions that cause abundant
sweating.
CONSEQUENCES OF WATER LOSS ON PERFORMANCE

31
fluids lost; the latter, in turn, is affected by
several factors. Moreover, it should be added
that the possibility of replacing lost fluids varies
during a competition depending on the sport.
In team sports, for instance, it can be done
during intervals and breaks in the match; in
marathons and race walking at refreshment
stations; and so on.
As regards the quantity of beverage needed each
time, it should not bloat the stomach too much.
The maximum quantity that does not cause any
disturbance varies from one individual to
another, also depending on the type of sport.
Therefore, every athlete should find the one
most fit to him/her. In more demanding climate
conditions, the production of sweat by the body
can amount to 20-40 grams per minute. This
clearly shows how high the intake of fluids
should be, although the intestine does not
absorb more than a certain quantity of water
per minute, not even when the beverage is the
most suitable one. It should always be borne in
mind that when clothing is soaked with sweat,
the quantity of beverage sipped should be grea-
ter than that needed to quench thirst.
During training sessions, an intake of fluids
might be needed that is even greater than that
needed during a competition. In some periods
of the year (for instance, during the pre-season
of some football and basketball teams), there
are often two daily training sessions and they
last quite a while, even more than a match. The
continuous production of sweat, which takes
place even outside of a training session if the
weather is hot or hot and humid, can lead to a
substantial loss not only of water, but also of
minerals in just a few days. It should be borne in
mind that a “casual” diet - that is to say one
based on the available foods and personal
tastes - does not necessarily restore the content
of minerals in the body to normal levels. Some
muscular problems (such as cramps) can be the
result of this imbalance between intake (with
food) and loss (through sweat). That's why it can
be useful to regularly replenish the body with
some of the electrolytes contained in sweat
especially during those times of the year when
loss is greater, namely when it is hotter.
THE "IDEAL" DRINK FOR ATHLETES
Drinks for athletes should have certain well-defi-
ned characteristics especially with regard to the
time of consumption.

32
Those who do sports lasting more than a few
minutes, if continuous, or for more than 20-40
minutes if these alternate moments of intense
activity with moments of rest (as is the case in
team sports and tennis), it is absolutely neces-
sary to know whether the intake of water during
exercise or during the day is enough to make up
for fluids lost during the day. In order to avoid
worsening performance, it is very important to
be well hydrated during practice (and even more
so during a competition), that is to say, to be in
a state of euhydration. If someone is dehydra-
ted, there is a worsening in performance. All
this applies in particular to the hottest periods
of the year and, above all, to professional athle-
tes during high load periods, when they train for
many hours every day.
The most important information on the state of
hydration can be obtained from bioelectrical
impedance analysis, but one's body weight can
be very useful provided it is always measured in
the same conditions, especially in the morning
on an empty stomach, before breakfast and
after voiding stools and urine.
A drop in weight by a few hectograms compared
to the day before must always be considered as
a possible state of poor hydration.
The first urine of the morning should be exami-
ned too: it must be abundant and, above all,
quite clear; its specific weight should be of 1020
or less. Watch out, though, for very abundant
and almost transparent urine: it could be a sign
of the difficulty to retain fluids due to a poor
intake of sodium and hence of a situation of
ineffective replacement, as signaled by the
American College of Sports Medicine (see the
article “Exercise and fluids replacement” in
issue #2 of 2007 of Medicine & Science in
Sports & Exercise, pg. 377-390). In order to
reduce the useless loss of sweat, avoid staying
too long in the sun and in the heat when it is not
necessary and also avoid physical exercise
when it is not required by the sports activity.
SOME TIPS FOR MAINTAINING PROPER HYDRATION IN THE HOTTEST PERIODS OF THE YEAR

33
Drinks to be taken before exercise
The drink should be consumed 20-40 minutes
before the competition or training session so that
it does not give rise to problems later on when the
physical effort has started. For instance, if it were
very rich in carbohydrates, which lead to a rise in
blood sugar and hence in insulinemia, it could
inhibit the use of fatty acids during exercise and
even cause what is known as reactive hypoglyce-
mia. Both problems occur when high quantities of
carbohydrates are ingested and rapidly assimila-
ted, as is the case of some drinks that contain
large quantities of glucose, sucrose or maltodex-
trins (at a high concentration). Consider that 300
mL of a sports drink containing 6% of carbohy-
drates with a high glycemic index (for instance
18 g glucose, maltodextrins, sucrose) can already
lead to significant insulin stimulation, thereby
having negative effects on the ability to oxidize
fats during exercise.
Drinks to be taken during exercise or right
before it
Like the one taken during exercise, the drink to
be taken right before a competition or training
must provide in the shortest time possible for
the replenishment of what has been lost in
sweat. Therefore, it must pass quickly through
the stomach and then be absorbed rapidly in the
intestine. If possible, it should also supply a
certain quantity of carbohydrates to the body.
The time a drink spends in the stomach depends
on its concentration of carbohydrates. A quick
passage through the stomach is possible when it
contains 5% or less and, at the same time, does
not contain too many minerals. At the same con-
centration (1 g of carbohydrate for every 100 g of
water), a drink containing fructose or maltodex-
trins passes more quickly compared to one
containing glucose or sucrose.
The drinks that should be preferred for fast
absorption of water are isotonic drinks - that is
to say, drinks with a concentration of substances
similar to that of blood - or, according to some,
hypotonic drinks - that is to say, with a lower
concentration.
Though limited, the presence of carbohydrates,
is nonetheless useful because when passing
through the intestine's walls, the monosacchari-
des already present in the drink (glucose and
fructose) or those formed after the digestion of
carbohydrates formed by two or more monosac-
charides "drag" along with them some molecu-

les of water. Sodium ions, too, bind, with water
and hence favor its absorption. Put otherwise,
pure water is absorbed more slowly compared to
some saline-energy drinks, even though a
person who has sweated intensely should drink
mineral water sold in bottles or tap water rather
than not drinking at all.
Drinks to be taken after exercise
Finally, the main purpose of the drink to be
ingested after a competition or training is that
of replenishing the body not only with water, but
also with the minerals lost during exercise and
of providing a certain quantity of carbohydrates.
Unless an athlete is in a condition of severe
dehydration, drinking water immediately is not
urgent. While, on the one hand, an intake of
carbohydrates, even in large quantities, slows
down the passage of fluids through the stomach,
on the other, together with carbohydrates in
food, it helps to re-synthesize the glycogen con-
sumed by muscles.
This is especially useful when there are training
sessions or competitions almost every day.
DRINK TEMPERATURE
Drinks ingested right before the competition or
training or during exercise should be cool, espe-
cially if the temperature and humidity are high.
Those drinks with a temperature below 15°C
spend less time in the stomach compared to
those that are warmer. If drinks are between
2.5°C and 9°C, the mucosa of the mouth, larynx,
esophagus and, above all, of the stomach can be
cooled even by several degrees. Gastric motility
increases, and the time spent by fluids in the
stomach is reduced. Moreover, heat is dissipated
from the body by conduction. All these are defi-
nitely advantageous effects. When the drink is
too cold, though, there is the risk of suffering
gastric or abdominal cramps and other even
more serious consequences.
MINERALS IN DRINKS
The lack of one - or more - of the minerals lost
through sweat gives rise to problems in the body.
If the absorption of ions is blocked, even the
absorption of water stops - save for situations of
dehydration (Curran et al., 1962). Therefore,
sports drinks should contain the main minerals
that are found in sweat, namely sodium, chlorine,
potassium and magnesium.
Sodium is definitely the most important from
34
this point of view, both because it is the positi-
vely charged ion that is most lost in sweat during
physical exercise and because hyponatremia is a
serious risk in athletes. If the drink contains
sodium, among other things, rehydration is
faster because sodium favors the absorption of
water in the intestine. It should be noted that, if
it is true that with the same amount of sweat
produced, as illustrated in Table 2, a well-trai-
ned athlete loses less sodium compared to
someone who exercises occasionally, it is also
true that - due to the very fact of being well-trai-
ned - an athlete can perform workloads that are
much greater than those of someone who is less
trained and hence risks a substantial depletion
of this ion. Among other things, it is not true
that, in an individual with no heart, circulation or
kidney problems an intake of sodium leads to a
rise in fluid retention. If this occurs, it is only a
temporary phenomenon. Still, rehydration velo-
city is fastest with isotonic drinks containing - in
addition to about 5% of carbohydrates - about 50
mmol/L of sodium (Murray, 2002).
Potassium plays a synergistic role with sodium;
these two electrolytes, taken together, accelerate
rehydration. After drinking water with sodium
and potassium, diuresis is lower compared to
water without these minerals. The assessment
of their concentration in plasma, however, provi-
des limited information only because the values
that really matter are the intracellular ones.
Replenishment of magnesium is also essential.
Even though sweat does not contain very much
magnesium (see Table 2), a lack of it is much
more frequent that one would expect.
35

36
REFERENCES
Arcelli E.: La maratona: allenamento e alimentazione. EdizioniCorrere. Milan, 1989.
Arcelli E.: Calcio: alimentazione e integrazioni. Edizioni Correre,Milano, 1996.
Arcelli E. e Molteni G.: Il bilancio termico del maratoneta. LaMedicina del Lavoro, 67, 2: 183-195, 1989.
Åstrand P.O. and Rodahl K.: Textbook of Work Physiology, McGraw-HillBook Compani, New York, 1970.
Curran P.F., Macintosh J.R.: A model system for biological watertransport. Nature, Jan 27; 193:347-8, 1962.
Horta L.: Alimentaçao no deporto. Xistarca, Lisboa, 1986, 1986.
Kleiner, S.M.: Workouts worth their salt: replacing what you sweataway. Physician Sportsmed. 21: 25-26, 1993.
Liu, L., Borowski, G. and Rose L.I.: Hypomagnesemia in a tennis player.Physician Sportsmed. 11: 79-80, 1983.
McArdle W.D., Katch F.I. and Katch V.L.: Fisiologia applicata allo sport.Casa Editrice Ambrosiana, 1998.
Murray B.: Preventing dehydration: sport drinks or water. GSSIProceedings-2002.
Noakes T.: Lore of running. Human Kinetics, Champaign, 2003.
O’Toole M.L., Douglas P.S., Laird R.H. and Hiller W.D.B.: Fluid andelec- trolyte status in athletes receiving medical care at an ultradi-stance triathlon. Clin. J. Sport Med. 5: 116-122, 1995.
O’Toole M.L., Douglas P.S., Lebrun C.M., Laird R.H., Miller T.K.,Miller G.C. and Hiller W.D.B.: Magnesium in the treatment of exertionalmuscle cramps (abstract). Med. Sci. Sports Exerc. 25: S19, 1993.
37
- 4 -
fatigue in football
According to Rampinini (2008), among the defi-
nitions of "fatigue" given by various researchers
who have dealt with the issue, the most appro-
priate to illustrate what happens to a football
player during a match is the one given by Enoka
and Duchateau (2008), who stated that fatigue is
“...the impossibility to produce force or power or
to support a given task due to an exercise
carried out before.” It can be said that these
four are the main types of fatigue that a football
player can experience during a match:
• temporary fatigue: it occurs after a player
has carried out a certain quantity of high-
intensity work (for instance, sprints at short
intervals); it is temporary, i.e., it goes away
after a certain period of time;
• fatigue at the beginning of the second half:
right after half-time, in the early phase of the
second half, players are not able to give their
maximum;
• fatigue in the last phase of the match: in the
last 15 minutes of a match players in any
position, even when the final score is still
uncertain, run less and especially with less
intensity;
• fatigue due to dehydration: it typically occurs
when the match is played in the presence of
high air temperatures and high levels of
humidity and irradiation, when you have an
intense production of sweat.
It is important here to understand what are the
causes of these types of fatigue and determine
whether it is possible to prevent them through a
correct diet and supplements, but also through
physical activity.

TEMPORARY FATIGUE
“Temporary fatigue" is the fatigue that leads to a
drop in the physical efficiency of a player. It can
occur both in the first and second half and it is
marked by the fact that it is temporary and short,
that is to say from a few to several minutes.
Mohr et al. (2003) have proven that a period of 5
min of high-intensity work (for instance, running
at a fast speed) is always followed by a phase
during which a player's intensity is below the
average of the entire match.
Krustrup et al. (2006) have carried out a study,
which focused, among other things, on under-
standing which factors during a match, after
intense phases of play, cause “temporary fatigue”
and thus a drop in a football player's performan-
ce. The research study saw the participation of 31
Danish semi-professional players in a number of
friendly matches. Besides monitoring their heart
rate, blood samples were collected and muscle
biopsies were performed not only before matches,
during half time and at the end, but also during
the matches.
Players also performed another test several
times: it consisted in covering a distance of 30
m, as fast as they could, 5 times, with an interval
of 25 s during which they had to jog back to the
starting point. Even during the tests carried out
on the players before the match, the time obtai-
ned over 30 m continued to worsen (it is normal
for this to happen, considering the short break
between one sprint and another) between the
first run and the fifth of each test. In the tests
carried out during the match, right after the
high-intensity phases of play, time worsened by
1.6% - compared to those before the match -
when the test was carried out during the first
half and 3.6% when it was done during the
second half. A "crisis" was documented, but it
was followed by a return to normal after a few
minutes.
The causes of this temporary fatigue have not
been entirely cleared up, though. According to
Mohr et al. (2003), they are not linked to the
drop in muscle glycogen, but to a disorder in the
homeostatis of ions in muscle fibers. According
to Krustrup el al. (2006), it is likely that this
temporary drop in efficiency is not determined
by a single factor, but by a set of factors, such as
a rise in the concentration of lactate, ammonia
or potassium, or a drop in the pH of muscle
fibers.
38
It is unlikely that diet can affect this type of fati-
gue in a positive manner, while types of training
consisting of intense loads for a short period of
time are definitely useful, those that football
physical trainers call “lactacid loads” and during
which the level of "perturbation" inside muscle
fibers is even greater than during the match.
FATIGUE AT THE BEGINNING
OF THE SECOND HALF
According to Mohr et al. (2005), at the beginning
of the second half, the ability of players to give
their maximum level of performance is inhibi-
ted. Probably, this occurs as a consequence of
the fact that during the interval between one
half and the other, there is a drop in the tempe-
rature of the players' muscles compared to the
temperature at the end of the first half.
These are some tips that players can use to
avoid this type of fatigue:
• do light exercises while in the locker room; if
a player does static stretching, he should stop
a few minutes before returning to the pitch
according to Alberti's recommendations
(Arcelli, 2008);
• once out of the locker room, players should
jog along the way to their position on the pitch
and, if possible add a few hundred meters of
running especially if the outside temperature
is very low.
FATIGUE IN THE LAST PHASE OF THE MATCH
Bangsbo et al. (1994) observed that in the
Danish first and second division championships,
players - regardless of the role on the pitch and
the progress of the match - run less at a high
intensity during the last 15 min of the match
especially if compared to the first 15 min. At the
same time, players who came on in place of
other players (and hence were less tired) ran
25% more than players who had been on the
pitch from the beginning.
Ferretti (2008) determined that there is a drop in
efficiency at the end of the match even in Italy's
Serie A championship. With regard to Serie A,
Arcelli et al. (2010) observed that there tends to
be an increase in the number of goals scored
that are almost double those of the first 15
minutes of the match and that players who
came on in the second half scored more than
those on the pitch from the beginning. It is very
likely that this happens because fatigue has a
greater impact on the ability of defenders to
39

prevent shots on goal by attackers rather than
the ability of the latter to score.
According to Reilly (1997), the cause of this type
of fatigue is the lack of glycogen in muscles.
Already over 40 years ago, Karlsson (1969) had
observed in muscle biopsies that players with
lower glycogen concentrations in muscles
during half-time were those who in the second
half ran less at a lower average speed. Saltin
(1973) then observed that those players who at
the start of the match already had little glycogen
in their muscles ran much less than the others.
According to Krustrup et al. (2006), glycogen
deficiency in muscles especially affects type-1
fibers. Training for aerobic strength (for instan-
ce, 4 series of 4 min each at 90% of maximum
heart rate, according to the recommendations of
Hel gerud et al., 2001) increa-
ses the content of glycogen in
muscles, but does not enti-
rely solve the problem becau-
se it also leads to an increase
in the velocity of the anaero-
bic threshold and hence the
tendency to run more during
the match with an increase in
glycogen consumption.
The nutritional aspects can
be very important. Saltin (1973), as mentioned
above, had proven that it is beneficial to try star-
ting the match with the greatest possible con-
centration of glycogen in muscles. Foster et al.
(1986) had observed that the intake of maltodex-
trins during half-time allowed players to run
more and faster during the second half compa-
red to the placebo group. Shephard and Leatt
(1987), in turn, administered 28 g of maltodex-
trins in 400 mL of water before the match and
during half-time; during the first half there were
no beneficial effects, while in the second half
the distance covered increased by 25% and the
Fig. 1 - Muscle glycogen concentration before, during half-timeand at the end of the match in 6 players. In all players the con-centration of glycogen after the match is very low. FromKarlsson (1986), modified.
40

speed by 40%. No effect was registered in the
placebo group. Leatt and Jacobs (1989) had
given players a placebo or 35 g of glucose poly-
mers in 500 mL of water both 10 min before the
start of the match and during half-time; the
drop of glycogen was greater in the placebo
group compared to the players replenished with
carbohydrates.
Based on the statements of the last three
papers (Foster et al., 1986; Shephard and Leatt,
1987; Leatt and Jacobs, 1989), the intake of car-
bohydrates before the match and during half-
time does give a certain boost to performance in
football players. Why don't the habits of football
players include the regular intake of carbohy-
drates at these two moments?
If they do so, why in minimum quantities? And
why so few players?
There are several reasons. If you play having
taken 400 or 500 mL of fluids just a few minutes
before, you have an unpleasant feeling of stoma-
ch fullness that is bothersome when running. On
the other hands, problems do not decrease if you
wish to obtain the same quantity of carbohydrates
in a smaller volume of a drink, because the
greater concentration determines, at least, a
longer dwell time in the stomach and a longer
intestinal absorption time (Maughan, 1991).
Putting off the moment of the drink intake is not
possible during half-time (which lasts about 15
min). Before the start of the match, though, an
earlier intake by 10-20 minutes can lead to a
condition of reactive hypoglycemia and also an
inhibition to use fats, which, as is quite likely,
contribute during the second half, to supplying
energy to muscles, though to a limited extent
(Bangsbo, 1994; Krustrup et al., 2006).
Recently, a solid gelatin (a new category of
energy supplements, not to be mistaken with
gel) made of carbohydrates such as fructose
and isomaltulose has become available, and it
has a minimal dwell time in the stomach
matched by slow absorption. It can be taken up
to a short time before the start of the match (in
some cases even 15 min before the start and at
the beginning of half-time) without any inconve-
nience. Slow assimilation, on the other hand,
allows these carbohydrates to be a sort of
energy supply that passes slowly into blood
during the match. Since, according to Stolen et
al. (2005), a player of 75 kg burns between 1500
and 1770 kcal to complete a match, each gelatin
41

- which supplies 26 g of fructose and isomaltu-
lose (equal to slightly over 100 kcal) - guaran-
tees, in theory, an extra 5-6 min of autonomy
during the match.
FATIGUE DUE TO DEHYDRATION
When a football match is played in environmen-
tal conditions (high levels of temperature, humi-
dity and irradiation) which lead to copious swea-
ting, there is a risk that the players experience
another type of fatigue, i.e., the one due to dehy-
dration and the rise in body temperature
(hyperthermia). During a football match, the
drop in the body weight of football players is
frequently 1-2 kg and can even reach 4-5 kg in
extremely hot environments (Shephard and
Leatt, 1987). According to Åstrand and Rodahl
(1970), already when water loss amounts to
2-3% of body weight (equal to about 1.5-2 L), the
body's efficiency worsens, while greater losses
can even cause very serious disorders; in these
cases, it is useful to drink in the run-up to the
match (see article on drinks, pg 20-36), imme-
diately after warm-up and during half-time as
well as to supply players with solutions of water
and minerals also during the match, during any
pause. It is also possible to assess the opportu-
nity of resorting to pre-hydration (Arcelli, 1996),
immediately after warm-up, so that the entire
intake of water (at least 0.4 L) is not eliminated
through urine before the start of the match due
Fig. 2 - During Italian Serie A footballmatches, if the 90 min are divided into 6spans of 15 min each, the percentage ofgoals scored rises from one span toanother, up to 23.9% of the total in thelast 15 minutes of the match. FromArcelli et al. (2010).
42

to a drop in blood levels of adiuretin. In extreme
climate conditions, you can also consider
drinking 1.5 L of water with glycerol (0.7-1 g per
kg of body weight) starting 90 min before the
match (Lyons et al., 1990).
At any rate, being used to physical activities in
environments that lead to the production of great
quantities of sweat allows the body to resist a
greater loss of sweat before witnessing a drop in
efficiency (Åstrand and Rodahl, 1970).
43
Even in sports with easily measurable perfor-
mance (for instance, running or swimming), it is
very difficult to assess fatigue, simply due to the
fact that motivation plays an important role.
Things become even more complicated in sports
like football in which the performance also
depends on skill and tactics.
It would be useful to be able to assess also other
parameters in football players during various
moments of the match, such as the number of
errors (passes, shots, position…). However,
relying on a parameter such as the mobility of an
athlete is anyhow correct because it is assumed
that when the athlete moves less, it is because of
tiredness.
It should be borne in mind that a football player,
especially at the start of the match, works at
around the intensity of the anaerobic threshold
with periods in which the effort is even greater
(thus accumulating an oxygen deficit), alternated
with others in which it is lower and the athlete
can partly recover and be more ready to perform
actions in which the correct movement can be
matched by the high intensity of the effort.
FATIGUE AND ITS ASSESSMENT

REFERENCES
Arcelli E.: La reidratazione, in “Calcio: alimentazione e integrazio-ne”. Edizioni Correre, Milan, pg. 89-92, 1996.
Arcelli E.: Stretching e dintorni. Intervista a Giampiero Alberti.Scienza&Sport, n. 0, pg. 56-58, 2008.
Arcelli E., Pugliese L., Borri D. and Alberti G.: L’importanza dei gio-catori entrati nel secondo tempo. I gol segnati nel finale di partita inserie A. Scienza & Sport, n. 6, pg. 46-50, 2010.
Åstrand P.-O. and Rodahl K.: Textbook of Work Physiology, McGraw-Hill Book Company, New York, 1970.
Bangsbo, J.: The physiology of soccer with special reference to inten-se intermittent exercise. Acta Physiol Scand Suppl, 619, 1-155, 1994.
Ekblom, B.: Applied physiology of soccer. Sports Medicine, 3 (1), pg.50-60, 1986.
Enoka R.M., Duchateau J.: Muscle fatigue: what, why and how itinfluence muscle function. J. Physiol., 586 (1): pg. 11-23, 2008.
Ferretti, F.: Calcio: allenamento aerobico di qualità e di quantità. Attidel XVI Congresso Isokinetic, Milano, Calzetti e Mariucci Editori, pg.149-156, 2008.
Foster C., Thompson N.N., Dean J. and Kirkendall D.T.:Carbohydrate supplementation and performance in soccer players.Medicine & Science in Sports & Exercise. 18, S12, 1986.
Helgerud J., Høydal K., Wang E., Karlsen T., Berg P., Bjerkaas M.,Simonsen T., Helgesen C., Hjorth N., Bach R. and Hoff J.: Aerobichigh-intensity intervals improve VO2max more than moderate trai-ning. Medicine & Science in Sports & Exercise, 39 (4), pg. 665-671,2007.
Karlsson, H.G.: Kohlhydratomsattning under footballsmatch. ReportDepartment of Physiology III, reference 6, Karolinska Institute,Stokholm, 1969. Cited by Ekblom, 1986.
Leatt P. and Jacobs I.: Effects of glucose polymer ingestion on glyco-gen depletion during a soccer match. Canadian Journal of SportsSciences, 14, pg. 112-116, 1989.
Krustrup P., Mohr M., Steensberg A., Bencke J., Kjaer M., BangsboJ.: Muscle and blood metabolites during a soccer game: implicationfor sprint performance. Med. Sci. Sports Exerc., 38 (6): pg.1165-1174, 2006.
Lyons T.P., Riedesel M.L., Meuli L.E. and Chick T.W.: Effects of glyce-rol-induced hyperhydration prior to exercise in the heat on sweatingand core temperature. Medicine & Science in Sports & Exercise, 22(4), pg. 477-483, 1990.
Maughan R.J.: Fluid and electrolyte loss and replacement in exercise.Journal of Sports Sciences. 9: pg. 117-142, 1991.
Mohr M., Krustrup P., Bangsbo J.: Match performance of high-stan-dard soccer players with special reference to development of fati-gue. J. Sport Science, 21 (7): pg. 519-528, 2003.
Mohr M., Krustrup P., Bangsbo J.: Fatigue in soccer: a brief review.J. Sport Science, 23 (6): pg. 593-599, 2005.
Railly T.: Energetics of high-intensity execise (soccer) with particularreference to fatigue. J. Sports Scie., 15, pagg. 257-263, 1997.
Rampinini E.: Il ruolo della fatica nel gioco del calcio.Scienza&Sport, n. 0, July, pg. 60-63, 2008.
Saltin B.: Metabolic fundamentals in exercise. Medicine & Sciencesin Sports & Exercise, 5, pg. 137-146, 1973.
Shephard R.J. and Leatt P.: Carbohydrate and fluid needs of thesoccer players. Sports Medicine, 4, pg. 164-176, 1987.
Stolen T., Chamari K., Castagna C. and Wisloff U.: Physiology ofsoccer. An update. Sports Medicine, 35 (5), pg. 501-536, 2005.
44

- 5 -
gastrointestinal disorders
in long-distance runners
Athletes of some endurance sports and particu-
larly runners often report gastrointestinal
disorders, which can particularly affect the
esophagus (retrosternal pain, gastroesophageal
reflux), stomach (heartburn, nausea, vomiting)
and intestine (abdominal pain and cramps, need
to urgently evacuate, diarrhea, blood in stools).
These (generally temporary) disorders lead ath-
letes at times to reduce the intensity of their
effort, to temporarily interrupt activity and, in
the worst cases, to quit a competition (Sullivan,
1984; Peters et al., 1995; Peters et al., 1999).
In endurance competitions, gastrointestinal
disorders are among the most frequent causes
for withdrawal from the race or lower perfor-
mance (Pfeiffer et al., 2009).
WHO IS MOST LIKELY TO SUFFER
GASTROINTESTINAL DISORDERS
The first studies on the prevalence of gastroin-
testinal (GI) disorders in athletes date back to
40 years ago. Sullivan (1981) studied 57 mem-
bers of a running club (of whom only one-third
ran in competitions) and observed that 30% of
them had to evacuate urgently after the compe-
tition, 25% suffered abdominal cramps, 10%
heartburn and 6% intense nausea or vomiting
during the competition. Keeffe et al. (1984) stu-
died 707 athletes who participated in the Oregon
marathon and observed that they had more fre-
quent bowel movements or diarrhea after the
competition in 36% of the cases, they had to
interrupt the competition to move their bowels
in 20% of cases, suffered abdominal cramps in
14% of cases and had blood in stools in 2.4 % of
cases. More or less similar data were recorded
45

by Riddoch and Trinic (1988) in 536 runners of
the Belfast marathon and by Halvorsen et al.
(1990) in 279 runners in a local marathon.
This and other studies have shown that GI
disorders
• are present both in competitive runners and in
amateur runners (Eichner, 1988)
• are more frequent in women than in men (Keeffe
et al., 1984; Riddoch e Trinick, 1988; Peters et
al., 1999)
• are more frequent in runners who abruptly
increase the quantity of training (Eichner,
1988), are younger (Moses, 1990; Riddoch and
Trinick, 1988), are rather new to the sport and
are less trained (Moses, 1990)
• are more frequent in those who have already had
(Riddoch and Trinick, 1988) and in those who
normally have (Eichner, 1988) issues of gastritis
or colitis
• are more frequent in competitions than in trai-
ning and in more challenging competitions com-
pared to easier ones (Eichner, 1988; Riddoch and
Trinick, 1988).
According to Brouns and Beckers (1993), in
sports in which the body remains in a more sta-
ble position (cycling, swimming, ice-skating or
cross-country skiing) the frequency of GI disor-
ders, at the same intensity of effort and same
intake of substances before or during the compe-
tition, is lower compared to running. Rehrer and
Meijer (1991) measured accelerations and dece-
lerations in the GI region both in runners and
cyclists and observed that in the former they
were double compared to the latter. At every step
while running, you have vertical oscillations of the
trunk, and when you land on the ground there is a
sudden deceleration of the body, while you have
an acceleration at the moment of the thrust.
In runners, endoabdominal organs experience a
sort of continuous shaking.
THE CAUSES OF GASTROINTESTINAL
DISORDERS
Many researchers have sought to understand
which factors cause GI disorders. Riddoch and
Trinick (1988) stated that usually the causes of
these problems are unknown. According to
Dawson et al. (1985), hypertrophy of the psoas
muscle, with its movement during running, pres-
ses a section of the intestine, leading it to eva-
cuate; this could be a first cause of runner's
diarrhea. Eichner (1988) stated that some GI
disorders are the result of the use of anti-inflam-
46

matory drugs that runners frequently use to fight
disorders of the locomotor system. Rehrer et al.
(1990) stated that dehydration (especially when
water loss is greater than 4% of body weight)
favors GI disorders. Moses (1990) suggested that,
if you drink pure water, there are fewer disorders
compared to when you drink solutions rich in
carbohydrates and that nausea and vomiting are
often a sign of dehydration and hyperthermia.
Among the causes for the onset of GI disorders,
Brouns and Beckers (1993) also included:
• level of training: whoever starts to run - or resu-
mes running after a pause - will more likely have
GI disorders
• intensity of exercise: whoever gives his/her
maximum has more problems
• what is eaten before the competition: most pro-
blems result from the intake before physical
activity of too much food rich in fats, proteins or
fibers
• food or drinks during the competition: disor-
ders can arise, for instance, due to the intake of
caffeine, proteins and drinks that are too rich in
carbohydrates.
As for runner's diarrhea, Brouns and Beckers
(1993) stated that it can also be caused by diffi-
culties in absorbing sugars; for instance, if a few
dozen grams of fructose (a sugar that is absorbed
slowly) are taken together, once they are in the
small bowel they draw water from the gut walls
and the presence in the bowels of a consistent
amount of water and fructose acts as a mechani-
cal stimulus that causes diarrhea. The tolerance
of athletes to large doses of drinks containing
carbohydrates and the likelihood of developing GI
disorders seem to vary greatly from one indivi-
dual to another.
As for blood in stools, there are two hypotheses:
• traumatic: the shaking of abdominal organs
typical of running leads to the so-called “cae-
cal slap syndrome” (Porter, 1982), i.e., the
continuous knocking of intestinal walls
against one another, especially in the cecum,
thereby causing lesions in the mucosa; this
could explain why blood is frequently found in
the stools of runners (whose endoabdominal
organs, as already stated, experience intense
vertical accelerations and decelerations), but
not in cyclists or swimmers whose efforts are
of the same duration and intensity of running;
• ischemic: during intense physical exercise -
as demonstrated by Rowell et al. (1964),
Clausen (1977) and Qamar and Reed (1987) -
47

intestinal blood flow greatly decreases since
the blood is diverted to muscles and skin to
favor thermal balance. This could explain why
GI disorders are more frequent when running
at a high temperature (and even more so
when even humidity is also high). Since a lot
of blood needs to be channeled to the skin to
favor the dispersion of heat, much less blood
reaches the bowels.
PREVENTION OF GASTROINTESTINAL
DISORDERS
Here are some tips on how to avoid the onset of GI
disorders during exercise or right after.
Pre-competition diet
If you suffer from diarrhea, abdominal pain or
cramps or you often feel the need to urgently
move your bowels during a competition or right
after, you should limit the intake of foods with a
high fiber content (e.g., legumes and whole
grains) during the two days before the competi-
tion and large amounts of fruit in the 24 hours
before the competition. You should also avoid
consuming milk, cream and ice-cream (even in
small quantities that normally do not cause any
problems) in the previous 24 hours if you suffer
from lactose intolerance. In the hours right
before the competition, limit the amount of cof-
fee. If you usually suffer from nausea, vomiting
or a heavy stomach while you are running, the
last meal should be eaten at least three hours
before in case of slow digestion. The total fats
should be few; avoid fried fats or fats that have
been cooked at length. Coffee with milk is espe-
cially slow to digest.
Drinks during the competition
If during the last part of previous competitions
you have suffered from nausea and vomiting or if
you have had the feeling of not being able to eat
or drink, try to avoid dehydration and hyperther-
mia by regularly drinking beverages with a low
concentration of carbohydrates, especially if the
climate makes you sweat a lot.
Training
When training at competition intensity, try the
drinks you plan on drinking during the competi-
tion. Usually, every runner tends to more easily
tolerate drinks with a certain maximum concen-
tration of carbohydrates and maximum volumes
of fluids in the stomach; each athlete should
precisely determine both of these before the
competition especially if he or she wishes to
48
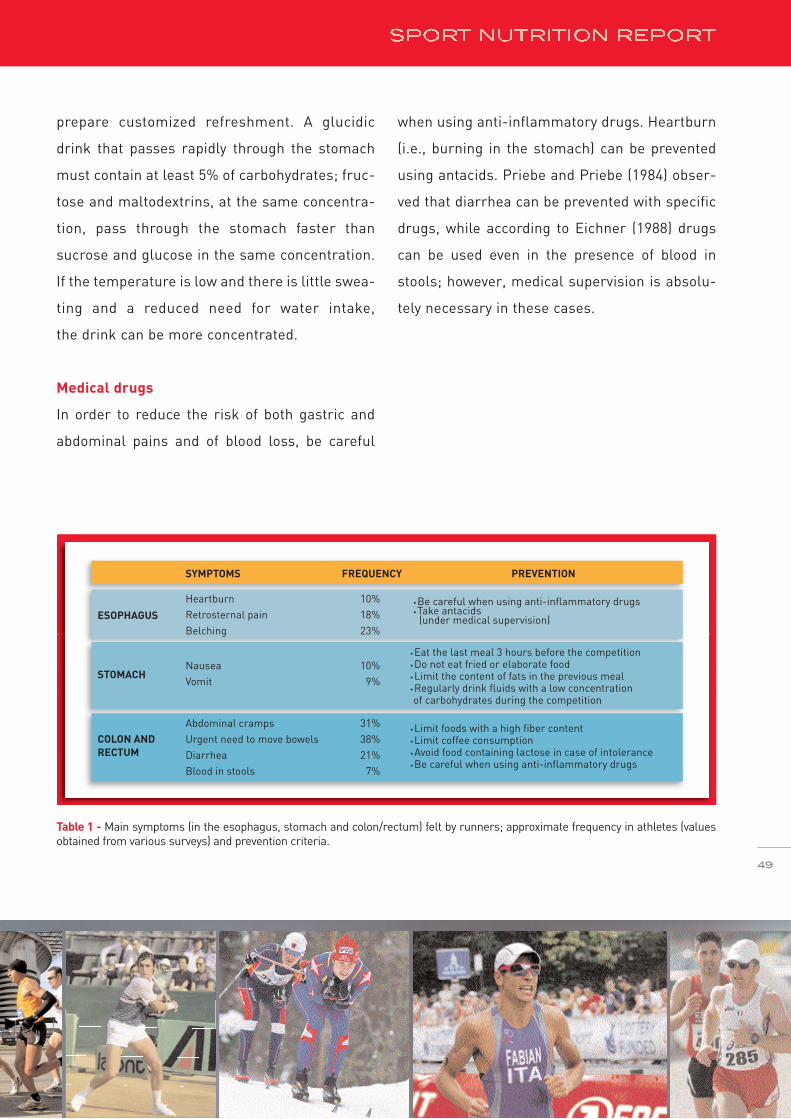
prepare customized refreshment. A glucidic
drink that passes rapidly through the stomach
must contain at least 5% of carbohydrates; fruc-
tose and maltodextrins, at the same concentra-
tion, pass through the stomach faster than
sucrose and glucose in the same concentration.
If the temperature is low and there is little swea-
ting and a reduced need for water intake,
the drink can be more concentrated.
Medical drugs
In order to reduce the risk of both gastric and
abdominal pains and of blood loss, be careful
when using anti-inflammatory drugs. Heartburn
(i.e., burning in the stomach) can be prevented
using antacids. Priebe and Priebe (1984) obser-
ved that diarrhea can be prevented with specific
drugs, while according to Eichner (1988) drugs
can be used even in the presence of blood in
stools; however, medical supervision is absolu-
tely necessary in these cases.
ESOPHAGUS
STOMACH
COLON AND RECTUM
SYMPTOMS FREQUENCY PREVENTION
HeartburnRetrosternal painBelching
● Be careful when using anti-inflammatory drugs● Take antacids (under medical supervision)
10%18%23%
NauseaVomit
● Eat the last meal 3 hours before the competition● Do not eat fried or elaborate food● Limit the content of fats in the previous meal● Regularly drink fluids with a low concentration of carbohydrates during the competition
● Limit foods with a high fiber content● Limit coffee consumption● Avoid food containing lactose in case of intolerance● Be careful when using anti-inflammatory drugs
10%9%
Abdominal crampsUrgent need to move bowelsDiarrheaBlood in stools
31%38%21%
7%
49
Table 1 - Main symptoms (in the esophagus, stomach and colon/rectum) felt by runners; approximate frequency in athletes (valuesobtained from various surveys) and prevention criteria.
REFERENCES
Brouns F., Beckers E.: Is the gut an athletic organ? Digestion,absorption and exercise. Sports Med., 15(4): 242-257, 199 Rowell etal. (1964), 3.
Clausen J.P.: Effect of physical training on cardiovascular adjust-ments to exercise in man. Physiol Rev, 57 (4):779-815, 1977. Cited byMoses F., 1990.
Dawson D.J., Khan A.N., Shreeve D.R.: Psoas muscle hypertrophy:medical cause for “jogger’s trot”? British Medical Journal, 391: 787-788, 1985. Cited by Eichner, 1988.
Eichner E.R.: Other medical consideration in prolonged exercise. In“Prolonged Exercise”, Lamb D.R. and Murray R., Benchmark PressInc., Indianapolis, Indiana (USA), 1988.
Halvorsen F.A., Lyng J., Glomsaker T., Ritland S.: Gastrointestinaldisturbances in marathon runners. British Journal of SportsMedicine, 24(4): pg. 266-268, 1990.
Keeffe EB, Lowe DK, Goss JR, Wayne R.: Gastrointestinal symptomsof marathon runners. West J Med., 141 (4): 481-484, 1984. Cited byMoses M., 1990.
Moses FM.: The effect of exercise on the gastrointestinal tract.Sports medicine 9(3): pg. 159-172, 1990.
Peters H.P., Bos M., Seebregts L., Akkermans L.M., van BergeHenegouwen G.P., Bol E., Mosterd W.L., de Vries W.R.:Gastrointestinal symptoms in long-distance runners, cyclists, andtriathletes: prevalence, medication, and etiology. Am JGastroenterol., 94 (6): pg. 1570-1581,1999.
Peters H.P., van Schelven F.W., Verstappen P.A., de Boer R.W., vander Togt C.R., de Vries W.R.: Gastrointestinal problems as a functionof carbohydrate supplements and mode of exercise. Med Sci SportsExerc., 25 (11): pg. 1211-1224, 1993.
Peters H.P., van Schelven W.F., Verstappen P.A., de Boer R.W., Bol E.,Erich W.B., van der Togt C.R., de Vries W.R.: Exercise performanceas a function of semi-solid and liquid carbohydrate feedings duringprolonged exercise. Int J Sports Med., 16 (2): pg. 105-113, 1995.
Pfeiffer B., Cotterill A., Grathwohl D., Stellingwerff T., JeukendrupA.E.: The effect of carbohydrate gels on gastrointestinal toleranceduring a 16-km run. Int J Sport Nutr Exerc Metab., 19 (5): pg. 485-503, 2009.
Priebe W.M., Priebe J.A.: Runners diarrhea: prevalence and clinicalsyntomatology American Journal of Gastroenterology., 79: pg. 827-828, 1984.
Qamar M.I., Read A.E.: Effects of exercise on mesenteric blood flowin man. Gut, 28 (5): pg. 583-587, 1987.
Porter A.M.: Marathon running and the caecal slap syndrome. Br JSports Med, 16 (3): pg. 178, 1982.
Rehrer N.J., Beckers E.J., Brouns F., ten Hoor F., Saris W.H.: Effectsof dehydration on gastric emptying and gastrointestinal distresswhile running. Med Sci Sports Exerc., 22 (6): pg. 790-795, 1990.
Rehrer NJ, Meijer GA.: Biomechanical vibration of the abdominalregion during running and bicycling. J Sports Med Phys Fitness,31(2): pg. 231-234, 1991.
Riddoch C, Trinick T.: Gastrointestinal disturbances in marathonrunners. Br J Sports Med., 22(2): pg. 71-74, 1988.
Rowell L.B., Blackmon J.R., Kenny M.A., Escourrou P.: Splanchnicvasomotor and metabolic adjustments to hypoxia and exercise inhumans. American Journal of Physiology, 247: H251-H258, 1964.Cited by Brouns and Beckers, 1993.
Sullivan S.N.: The gastointestinal symptoms of running (letter). NewEngland Journal of Medicine, pag. pg. 304: 915, 1981. Cited by MosesM., 1990.
Sullivan S.N.: The effect of running on the gastrointestinal tract. JClin Gastroenterol, 6 (5): pg. 461-465, 1984.
50

- 6 -
sports anemia
Sports anemia affects, above all, athletes who
train frequently and very intensely, starting with
those who do endurance sports such as
marathon, triathlon, cross-country skiing,
cycling and racewalking; but it also often affects
athletes who play individual or team sports.
Women athletes are affected more frequently
than men.
This article will discuss the most likely causes of
this disorder and the most effective treatments,
especially in light of recent discoveries (hepci-
din), which have shed new light on sports ane-
mia and, above all, have identified ways to cor-
rect it more easily.
SPORTS ANEMIA AND PSEUDOANEMIA
Hemoglobin is an iron-containing molecule that
is found in red blood cells; its task is to carry
oxygen. You have anemia when blood contains
scarce hemoglobin and/or when there are few
red blood cells and/or when the hematocrit is
low. Sports anemia is the result of iron defi-
ciency and is hence called sideropenic.
In sports that require a lot of oxigen in muscles
(typically aerobic continuous sports and those
with a substantial aerobic component, but also
intermittent sports - especially games - in which
fast recovery is needed between one intense
exercise and the next), performance is significan-
tly worse in athletes who become anemic. Often
times, there are even major problems to sustain
training sessions that were easily tolerated up to
a short time before.
It is often said that the ideal hemoglobin concen-
tration levels in blood should amount to at least
51

14.5 g/dL in men athletes and at least 13.5 g/dL in
women athletes. There have been though athletes
who have achieved extraordinary results (even
Olympic gold medals in the marathon) with levels
of hemoglobin much lower than these. Some
argue that you have anemia proper with levels
below 13 g/mL or, in women, below 11 g/L of
hemoglobin. In actual fact, an athlete can be con-
sidered anemic even if values fall within the nor-
mal range for the general population; the doubt
of an impending development of anemia must
arise when the values of an athlete’s last blood
exam are much lower than the values of the
exams when the athlete was in good condition.
Often times, though, low values of hemoglobin,
red blood cells and hematocrit in athletes are due
to pseudoanemia (i.e., false anemia). This can be
a consequence of training (e.g., of the sudden
rise in workloads, or work done at altitudes or in
conditions that cause copious sweating) and
involves a dilution of blood; there is no reduction
- rather an increase - in the total quantity of
hemoglobin or red blood cells in circulation, but
there is a significant increase in the volume of the
liquid portion. Therefore, the increase in plasma
volume is greater than the increase of the volume
of the red blood cells. In these cases, an athlete's
performance is not at risk.
In anemia proper - due to iron deficiency in bone
marrow (the organ that "makes" red blood cells) -
there is a drop in the total quantity of hemoglo-
bin in the blood, in the ability to carry oxygen and
in the availability of energy for muscles at every
second. The ability of muscles to work also
decreases because some very important mole-
cules for the use of oxygen (myoglobin, cytoch-
romes and various other enzymes involved in
producing energy through aerobic mechanisms)
contain iron and their production decreases
when there is an iron deficit.
Each time you have an anemic athlete, it is very
important to exclude the existence of other
pathologies that may have caused this condition.
It should also be borne in mind that celiac disea-
se too (which occurs in 1 out of every 150
Italians) can also cause anemia.
THE CAUSES OF SPORTS ANEMIA
Up to a few years ago, it was believed that the
only cause of sports anemia was that lost iron
amounted to more than the iron absorbed and
that the main reason for this imbalance consi-
sted solely in a low intake of iron with food or in
52

an increased loss of it especially through urine,
stools, sweat and, in women athletes, through
menstruation. Even today - although the role of
hepcidin has quite changed our view of things -
these aspects are nonetheless important and
should be known.
LOW IRON INTAKE
In Western countries an adult usually ingests a
few milligrams of iron through food. However, it
should be considered that only a small part of
this iron (often less than 10%) is usually absor-
bed. Heme iron, the one found in meat (inclu-
ding offal, cold cuts and fresh or frozen fish pro-
ducts), is more easily absorbed than non-heme
iron, i.e., that form of iron found in foods of plant
origin such as legumes, nuts (walnuts, hazel-
nuts, almonds, pineseeds, etc.), brewer's yeast,
parsley, spinach and so on.
Many of the athletes who tend to develop anemia
have a very low consumption of iron-rich food,
sometimes because they have totally eliminated
foods of animal origin from their diet without
having adopted, at the same time, those adjust-
ments that usually allow vegetarian athletes
with a good knowledge of dietetics to avoid
problems of iron deficiency.
INCREASE IN IRON LOSS
All individuals have a daily "physiological" loss
of iron through sweat, desquamation of the skin
and intestinal epithelium and so on. Some have
greater losses, for instance, due to blood losses
through the digestive tract (gastritis, duodenitis,
colitis, ulcers in various sites, hemorrhoidal
disorders, etc.), due to other hemorrhages (pro-
bably of minor extent yet continuous) and, in
women, gynecological disorders. The first goal
for anyone who has sideropenic anemia must be
to exclude these causes.
In athletes who train intensely and frequently,
there can be an increased loss of iron through
the following routes: stools, urine and sweat.
LOSS OF IRON THROUGH STOOLS
In runners' stools there are often traces of blood
especially after long training sessions or after
races over long distances (Stewart et al., 1984).
This can be due to various causes, such as “cae-
cal slap syndrome”, namely the shaking of the
cecum during running (Porter, 1982), or to inte-
stinal ischemia, i.e., a reduced supply of oxygen,
above all in the colon, with subsequent vasodila-
tion and the passage of red blood cells into the
53

intestine (Heer et al., 1987). In some cases blood
losses are due to lesions in the mucosa of the
bowels, stomach or esophagus or to full-blown
ulcers (Choi et al., 2001). These blood losses are
at times accompanied by GI disorders during
exercise and are often caused by the use of anti-
inflammatory drugs to treat problems in tendons
or joints, which are frequent in athletes (Baska et
al., 1990). See also the article on gastrointestinal
disorders, pg. 45-50.
LOSS OF IRON THROUGH URINE
The first researcher who spoke of “athletic
pseudonephritis” was Gardner over 50 years ago
(Gardner, 1956). He observed that after a match
the urine of American football players would
contain proteins and red blood cells, as if the
individuals had nephritis; but the urine would
return to normal after about ten hours of rest.
It is this very return to normal of urine that is
still considered today an important fact in deter-
mining whether it is a form of nephritis or a
condition linked to physical exercise. Hematuria
is caused by increased glomerular permeability
(in turn, favored by renal ischemia, which is
more likely if the hot climate draws blood to the
skin). The longer the duration and intensity of
physical exercise, the more common it is.
An important role is definitely played by catecho-
lamines and the increased production of free
radicals (Bellingheri et al., 2008).
In a runner's urine, blood can be found even in
large amounts due to lesions in the bladder cau-
sed by the continuous knocking between the
walls of the bladder (Blacklock, 1979). In cyclists
and in particular those riding mountain bikes,
hematuria can be caused by traumas to the peri-
neum (Albersen et al., 2006).
In urine, there can be hemoglobin when many
red blood cells break inside blood vessels; in
runners, this happens, above all, because of the
impact of feet on the ground, more specifically in
the tissue crushed between the ground and the
bones of the heel and forefoot (Telford et al.,
2003). Haptoglobin usually binds free hemoglo-
bin, which is released in blood and carried to the
spleen where iron is recovered. However, if trai-
ning is extended in time and if - due to the oxida-
tion of membranes as a result of the free radicals
formed during exercise - red blood cells tend to
break more easily, this molecule is no longer
available and a certain quantity of hemoglobin is
not “captured” eventually ending up in urine.
54

LOSS OF IRON THROUGH SWEAT
The sweat of an individual doing physical exerci-
se contains iron concentrations that tend to
decrease with the duration of the effort and the
degree of training in conditions that favor swea-
ting (DeRuisseau, 2002; Chinevere, 2008). Those
who train every day (or even twice a day) with
high temperatures, humidity and irradiation pro-
duce several liters of sweat every day. They can,
as a consequence, experience significant iron
losses. While in the past it was believed that
women athletes would lose more iron through
sweat compared to male athletes (Lamanca et
al., 1988), nowadays the tendency is to believe
that there is no significant difference between
genders especially in runners covering the same
number of kilometers (DeRuisseau, 2002).
EFFECTS OF A NEGATIVE IRON BALANCE
When the iron balance is negative (iron loss
greater than iron absorption), first there is just a
drop in total iron reserves in the body with the
blood level of ferritin dropping below normal
levels; this is a condition called pre-latent iron
deficiency and usually athletes do not feel any
symptoms (Fig. 1, pg. 57). Latent iron deficiency
occurs when even the values of transferrin are
also out of range (in this case high), while the
values of hemoglobin, red blood cells and hema-
tocrit are still or almost normal; the athlete
already feels much more tired than usual.
In manifest iron deficiency all values are alte-
red: ferritin, serum iron, hemoglobin, red blood
cells and hematocrit are low; transferrin is high;
the mean volume of red blood cells is small.
Besides generalized weakness, an athlete has
muscular pain and difficulty recovering between
one session and another and between one exer-
cise and another during training; the intensity
he/she can maintain (in running, cycling, swim-
ming, racewalking, etc.) is lower than usual.
HEPCIDIN AND THE ROLE OF INFLAMMATION
In recent years, the role that hepcidin plays in
the onset of sports anemia is becoming increa-
singly clearer. It is a hormone that is essential in
the regulation of iron in the body. Hepcidin grea-
tly influences the absorption of iron contained in
food: the greater its concentration in blood, the
less iron is absorbed in the duodenum.
Moreover, hepcidin regulates the release of iron
contained in reserves, especially in the liver and
spleen, in that the high levels of hepcidin
55

substantially reduces iron (Ganz, 2003; Leong
and Lönnerdal, 2004; Robson, 2004). As a conse-
quence of hepcidin’s double effect (inhibition of
both absorption of iron in the bowels and its
release from reserves), blood has a lower con-
centration of iron and bone marrow lacks enough
raw material, namely iron, which is absolutely
necessary for the synthesis of hemoglobin.
The rise in hepdicin levels is caused by the
increase in proinflammatory substances in the
body (Ganz and Nemeth, 2009), triggered by
some cytokines, in particular, interleukin-6 (or
IL-6); said increase is activated, in turn, by
intense and frequent training (Ostrowski et al.,
1998; Pedersen and Toft, 2000), although there
are significant differences between one indivi-
dual and another from this point of view.
RULES TO PREVENT SPORTS ANEMIA
The use of fish oil, thanks to its content of long-
chain omega-3 fatty acids and in particular EPA
and DHA, definitely makes it possible to reduce
the body's state of inflammation. In cell mem-
branes, these fatty acids replace in part arachi-
donic acid. This favors the production of both a
smaller quantity of pro-inflammatory cytokines
(starting from IL-6) and a greater quantity of
antiinflammatory series-1 prostaglandins (Bagga,
2003; Burns et al., 2007; Grimble, 1998).
Still, besides fish oil, supplements containing iron
can be taken in the case of anemia, but only until
blood levels indicating that the disorder is still in
progress normalize.
Anyone who has suffered sideropenic anemia in
the past tends to redevelop anemia.
Therefore, besides taking fish oil, an individual
should also follow some rules (Arcelli et al.,
1995):
• include a source of heme iron in main meals,
such as various types of meat at lunch and
dinner (white meat is better than red meat
because the latter is rich in arachidonic acid),
and a slice of trimmed ham or two slices of
bresaola at breakfast; iron absorption is favo-
red by the presence of vitamin C and other
organic acids, while it is hindered by tannins
found in tea, coffee and wine. Instead of these
beverages you should drink water or orange
juice at meals
• regularly follow an anti-inflammatory diet,
i.e., low in arachidonic acid (besides replacing
red meat with white meat, as mantioned
56

above, also reduce the intake of egg yolks to a
minimum). Limited amounts of plant seed oils
rich in omega-6 fatty acids should be consu-
med and very few foods containing them, such
as snacks, cookies and other packaged
products whose labels indicate the presence
of “vegetable fats”
• have regular blood tests, for instance, in win-
ter every 60 training sessions (every month
Fig. 1 - Situation of reserve iron, hemoglobin iron, blood tests and individual symptoms in normal conditions and conditions of pre-latent, latent and manifest iron deficiency.
57

and a half, if training 10 times a week and
every three months if training 5 times) and in
summer every 40 sessions
• keep a chart in a notebook or PC that summa-
rizes both the data of the main blood tests of
recent years (number of red blood cells,
concentration of hemoglobin, hematocrit,
ferritin, transferrin, MCV, and MCH) as well as
subjective feelings and objective results of
training and competitions at the time of the
blood tests.
Hepcidin is a peptide consisting of 25 amino acids, which, among other things, is also a regulator
of iron in the body. Individuals who do not have this hormone as a result of a genetic mutation accu-
mulate iron in the body and experience hemochromatosis. An abundance of hepcidin due to an
inflammation reduces the absorption of iron in the small bowel and makes macrophages (that build
iron reserves) release iron with difficulty. The name hepcidin was coined by Park et al. (2001) when
they discovered this peptide produced by the liver (hence the prefix hep-) in human urine and
realized that, in vitro, it had the power to kill bacteria (hence the suffix -cidin). Only some years later
was its role in iron metabolism fully understood.
HEPCIDIN
58

REFERENCES
Albersen M., Mortelmans L.J., Baert J.A.: Mountainbiker’s hematu-ria: a case report. Eur. J. Emerg. Med., 13: pg. 236-237, 2006.
Arcelli E., Fiorella P.L. and G. De Rocco: L’anemia dell’atleta: quelloche devono sapere i tecnici e gli atleti. Atleticastudi, 5: pg. 13-30,1995.
Bagga D.: Differential effects of prostaglandin derived from omega-6 and omega-3 polynsaturated fatty acids on COX-2 expression andIL-6 secretion. Proc. Natl. Acad. Sci. USA, 100: pg. 1751-1756, 2003.
Baska R.S., Moses F.M., Graeber G., Kearney G.: Gastrointestinalbleeding during an ultramarathon. Dig. Dis. Sci., 35 (2): pg. 276-279,1990.
Bellinghieri G., Savica V., Santoro D.: Renal alterations during exer-cise. J. Ren. Nutr., 18 (1): pg. 158-164, 2008.
Blacklock N.J.: Bladder trauma in the long-distance runner. Am. J.Sports Med., 7 (4): pg. 239-241, 1979.
Burns T., Maciejewski S.R., Hamilton W.R., Zheng M., Mooss A.N.,Hilleman D.E.: Effect of omega-3 fatty acid supplementation on thearachidonic acid:eicosapentaenoic acid ratio. Pharmacotherapy,27(5): pg. 633-638, 2007.
Chinevere T.D., Kenefick R.W., Cheuvront S.N., Lukaski H.C, SawkaM.N.: Effect of heat acclimation on sweat minerals. Med. Sci. SportsExerc.: 40: pg. 886-891, 2008.
Choi S.C., Choi S.J., Kim J.A., Kim T.H., Nah Y.H., Yazaki E., EvansD.F.: The role of gastrointestinal endoscopy in long-distance runnerswith gastrointestinal symptoms. Eur. J. Gastroenterol. Hepatol., 13(9): pg. 1089-1094, 2001.
DeRuisseau K.C., Cheuvront S.N., Haymes E.M., Sharp R.G.: Sweatiron and zinc losses during prolonged exercise. Int. J Sport Nutr.Exerc. Metab., 12 (4): pg. 428-437, 2002.
Ganz T.: Hepcidin, a key regulator of iron metabolism and mediatorof anemia of inflammation. Blood, 102 (3): pg. 783-788, 2003.
Ganz T., Nemeth E.; Iron sequestration and anemia of inflammation.Semin. Hematol., 46 (4): pg. 387-393, 2009.
Gardner K.D.: “Athletic pseudonephritis”, JAMA, 161: pg. 1616-1617,1974.
Grimble R.F. and Tappia P.S.: Modulation of pro-infiammatorycytokine biology by unsaturated fatty acids. Z. Emahrungswiss, 37suppl., 1: pg. 57-65, 1998.
Heer M., Repond F., Hany A., Sulser H., Kehl O., Jäger K.: Acuteischaemic colitis in a female long distance runner. Gut, 28 (7): pg.896-899, 1987.
Lamanca J.J., Haymes E.M., Daly J.A., Moffatt R.J., Waller M.F.:Sweat iron loss of male and female runners during exercise. Int. J.Sports Med.: 9(1): pg. 52-55, 1988.
Leong W.I., Lönnerdal B.: Hepcidin, the recently identified peptide thatappears to regulate iron absorption. J. Nutr., 134 (1): pg. 1-4, 2004.
Ostrowski K., Hermann C., Bangash A., Schjerling P., Nielesen J.N.and Pedersen B.K.: A trauma-like elevation of plasma cytokines inhuman in response to treadmill running. J. Physiol., 513: pg. 889-894, 1998.
Park C.H., Valore E.V., Waring A.J., Ganz T.: Hepcidin, a urinary anti-microbial peptide synthesized in the liver. J. Biol. Chem., 276: pg.7806-7810, 2001.
Pedersen B.K. and Toft A.D.: Effects of exercise on lynphocytes andcytokines. Br. J. Sports Med., 34: pg. 246-251, 2000.
Porter A.M.W.: Marathon running and the caecal slap syndrome. Br.Med. J., 287: pg. 1427, 1983.
Robson K.J.: Hepcidin and its role in iron absorption, Gut, 53 (6):pg. 617-619, 2004.
Stewart J.G., Ahlquist D.A., McGill D.B., Ilstrup D.M., Schwartz S.,Owen R.A.: Gastrointestinal blood loss and anemia in runners. Ann.Intern. Med., 100 (6): pg. 843-845, 1984.
Telford R.D., Sly G.J., Hahn A.G., Cunningham R.B., Bryant C., SmithJ.A.; Footstrike is the major cause of hemolysis during running. J.Appl. Physiol., 94 (1): pg. 38-42, 2003.
Waller M.F., Haymes E.M..: The effects of heat and exercise on sweatiron loss. Med. Sci. Sports Exerc.: 28 (2): pg. 197-203, 1996.
59

A publication of Equipe Enervit S.r.l. via Comm. Garavaglia, 2Loc. Pian del Tivano22020 Zelbio (CO)Taxpayer's code 02539160131
SPORT NUTRITION REPORT2 / 2011
Editor: Giuseppe SorbiniDirector: Enrico Arcelli
Editorial staff: Giancarlo Carli, Paolo Calabresi, Elena Casiraghi, Marco Cason, Paolo D’Iria, Marco Gambetti, Kristy Lynn Davis, Serena Martegani, Luca Mondazzi, Mauro Ostinelli, Paolo Petroni, Riccardo Pina, Monica Polgatti, Maurizia Sorbini, Chiara Trombetta
tel. 02 485631 – fax 02 4984727e-mail: [email protected]
Printed by: Grafiche Riunite Lito 4 – via Simone Martini, 3 20052 Monza
Registered at the Court of Milan n° 124, February 24, 2011
Copyright © Equipe Enervit 2011, MilanReproduction, either in part or in full, of the articles and illustrations of this volume,and the translation thereof, is reserved and requires the express authorization of the publisher.© Equipe Enervit - All rights reserved. Finished
Printing in September 2011


equipe enervit srl - piano del tivano - 22020 zelbio (co)
TM
Solae ™ is a trademark of Solae, LLC for its brand of soy protein products.
It is used under license by Enervit S.p.A. C
OD
. 623
17




























