Embed Size (px)
Citation preview

Nutritional care of pregnant women in South Asia:Policy environment and programme action
Acknowledgements
This report was prepared by UNICEF’s Nutrition Section, UNICEF Regional Office for South Asia. The study was designed and conducted by Sophie Goudet, and overall guidance and direction was provided by Harriet Torlesse and Zivai Murira. The authors are Sophie Goudet, Zivai Murira and Harriet Torlesse.
Suggested citation: UNICEF. Nutritional care of pregnant women in South Asia: Policy environment and programme action. UNICEF Regional Office for South Asia: Kathmandu, Nepal.
© United Nations Children’s Fund (UNICEF) Regional Office for South Asia, 2019
Photo credit, cover page: © UNICEF/2015/Zaidi
The study team is grateful to the technical contribution of Nutrition International to the design of this study, and to government staff, UNICEF nutrition staff and partners at country level for their enormous contributions to this study. The report was funded by contributions from the Bill & Melinda Gates Foundation through the Regional Initiatives for Sustained Improvements in Nutrition and Growth.
Nutritional care of pregnant women in South Asia:Policy environment and programme action
Table of Contents
2 Acknowledgements
7 Foreword
8 Executive summary
10 Introduction
12 Methods
16 Status of maternal nutrition in South Asia
21 Status of policy and programme action
23 Recommendation 1: Counselling on healthy eating and physical activity
27 Recommendation 2: Nutrition education to increase energy and protein intake
31 Recommendation 3: Balanced energy and protein dietary supplementation
35 Recommendation 4: Daily iron and folic acid supplementation
39 Recommendation 5: Intermittent iron and folic acid supplementation
41 Recommendation 6: Calcium supplementation
45 Recommendation 7: Vitamin A supplementation
49 Recommendation 8: Restricting caffeine intake
51 Summary
55 References
56 Annex 1: Country briefs
74 Annex2:Indicatordefinitions
76 Annex 3: Survey data on indicators of women’s and children’s health and nutrition
78 Annex 4: Sources of national survey data
81 Annex 5: Persons consulted


Nutritional care of pregnant women in South Asia: Policy environment and programme action 7
Foreword
I am pleased to share with you this review of the policy environment and programme action on the nutritional care of pregnant women during antenatal care in South Asia. Improving women’s nutrition is essential for the health and well-being of women and to break the intergenerational cycle of malnutrition in the region. Women who enter pregnancy with a good nutritional status and who have access to quality nutritional care are more likely to experience a healthy pregnancy and to give birth to well-nourished infants who thrive in childhood. But this is not a reality for women in South Asia, and there is abundant evidence that poor maternal nutrition is driving the persistently high burden of child stunting and wasting in the region.
The “World Health Organization recommendations on antenatal care for a positive pregnancy experience” were released in 2016. They include recommendations on the nutritional care of women during antenatal care and provide an opportunity to refocus attention to maternal nutrition. The UNICEF Regional Office for South Asia conducted this policy and programme landscape review to examine the extent to which national policies in South Asian countries are aligned with the
recommendations on maternal nutrition. The review also examined health system bottlenecks that are constraining the translation of these policies to the effective coverage of maternal nutrition interventions.
It is my sincere hope that all stakeholders concerned with the nutrition, health and well-being of women and their children in South Asia will utilize the findings and recommendations of this review to strengthen policies and programme actions to improve maternal nutrition in South Asia. Unlocking the power of maternal nutrition will transform the pace of progress in improving the growth and development of children in South Asia and the well-being of their mothers. It is encouraging that concerted efforts are already underway in countries across South Asia to implement multi-sector national nutrition plans to address malnutrition challenges. It is now time to ensure that these efforts give much greater attention to the resourcing and scaling-up of maternal nutrition interventions. In a few years’ time, we want to see much greater attention given to women’s nutrition, so they are not left behind as the region’s momentum to improve nutrition gathers pace.
Jean GoughRegional DirectorUNICEF Regional Office for South Asia

Nutritional care of pregnant women in South Asia: Policy environment and programme action 8
Executive Summary
Countries in South Asia may not reach the nutrition targets of the World Health Assembly and Sustainable Development Goals without the improved nutritional care of women. While progress has been made in reducing thinness (underweight) and increasing women’s height in South Asia, the status of women’s nutrition is a serious cause for concern. One in five women in the region are too thin (body mass index <18.5 kg/m2); one in ten women in the region have a short stature (<145 cm); overweight and obesity are rapidly rising; and anaemia is a severe or moderate public health problem in six countries, with no country on track to meet the World Health Assembly target to halve anaemia in women by 2025. The double burden of malnutrition – the coexistence of undernutrition with overweight and obesity – is well established in the region and poses a serious threat to the health and well-being of women and their infants.
The “World Health Organization recommendations on antenatal care for a positive pregnancy experience” (WHO, 2016) include recommendations on the nutritional care of women and provide an opportunity to refocus attention to maternal nutrition. This policy and programme landscape review examines the extent to which national policies in South Asian countries are in-line with the 2016 World Health Organization (WHO) recommendations on maternal nutrition and provides insights on the health system bottlenecks that are constraining the translation of these policies to programme action.
No country in the region has adopted all the recommended WHO maternal nutrition interventions and the number of recommendations covered by national policies or programme guidance ranges from one to six across countries. All countries except Pakistan have policy or programme guidance provisions for both the recommendations that apply in all contexts, daily iron and folic acid (IFA) supplementation and counselling of pregnant women on dietary intake and physical activity to prevent excessive intake. However, the number of countries with national policies or programme guidance that cover the context-specific recommendations is lower, particularly for intermittent IFA supplementation and
vitamin A supplementation. It is likely that countries have not fully considered the conditions under which these context-specific recommendations should be applied. There are also gaps in the alignment of policy and programme guidance with specific components of these recommendations, which may weaken their impact during implementation. Inconsistencies in policy and programme guidance provisions at multiple levels remains a challenge.
The extent to which countries in South Asia are implementing national level policies and programme guidance on maternal nutrition interventions was assessed qualitatively through a consultative process at country level to estimate geographic coverage (proportion of districts implementing a specific maternal nutrition intervention) and identify health system bottlenecks impeding implementation. The geographic coverage of maternal nutrition interventions is not at the level needed to transform the care of women during pregnancy and varies between countries and interventions. IFA supplementation is delivered in at least 75 per cent of districts in seven countries, but five or less countries are delivering the other interventions at this geographic scale. Data on the population coverage is only available for IFA supplements, indicating gaps in the capacity of national information systems to track coverage of maternal nutrition interventions. Bottlenecks to the implementation of maternal nutrition interventions vary by intervention and country. These bottlenecks persist at all levels of the health system; however, moderate and significant bottlenecks tend to be concentrated at the ‘downstream’ level (the demand for, supply of, and quality of services).
It is important to build on the tremendous political momentum on nutrition in the region in the past five years and ensure these national efforts give sufficient attention to the scale-up of maternal nutrition interventions.
In light of this evidence base, the following actions are recommended for countries in the region to accelerate action on maternal nutrition:
Nutritional care of pregnant women in South Asia: Policy environment and programme action 9
1. Undertake an evidence-based review and update of country maternal nutrition policies and programme guidance provisions in the context of the 2016 WHO nutrition recommendations for antenatal care.
2. Prioritize maternal nutrition in the national development agenda and sectoral plans and budgets, including national efforts to reduce maternal mortality, stunting and other forms of malnutrition.
3. Develop costed national and subnational plans for financing the sustainable scale-up of maternal nutrition interventions, with public sector and development partner support.
4. Develop programme implementation guidance and tools to support the implementation of the WHO recommendations, including practical guidance on subnational planning, budgeting, supply management, training packages and social and behaviour change communication materials.
5. Strengthen intra-sectoral (within health) and cross-sectoral coordination (across sectors) of the implementation of maternal nutrition policies and programme guidance through establishment and/or reinforcement of coordination structures within Ministry of Health and other cross sectoral platforms.
6. Strengthen the monitoring and tracking of maternal nutrition coverage indicators through household surveys, health information systems, and programme monitoring and reporting systems for all the recommended WHO maternal nutrition interventions.
7. Invest in implementation research to understand implementation bottlenecks and optimal approaches that drive improvements in the coverage, quality and equity of maternal nutrition interventions.
Recommended actions for countries in South Asia to accelerate action on maternal nutrition:
Nutritional care of pregnant women in South Asia: Policy environment and programme action 10
Introduction
Poor nutrition during pregnancy and postpartum is linked to adverse outcomes for both the mother and her baby. Maternal anaemia, especially in its severe form, elevates the risk of maternal mortality (Brabin et al., 2001) and accounts for 12 per cent of low birth weight, 19 per cent of preterm births, and 18 per cent of perinatal mortality (Rahman et al., 2016). Evidence demonstrates that maternal nutritional status is linked to child stunting in South Asia (Kim et al., 2017), the impacts of which can last generations (Christian et al., 2013). A recent four country analysis suggests that maternal prenatal care use is associated with both the height for age of children at 24 months and attained school grades later in life (Liu et al., 2017). Meanwhile, maternal overnutrition raises the risk of haemorrhage, hypertensive disorders, gestational diabetes and macrosomia, a high birth weight (Black et al., 2013).
Progress on improving maternal nutrition in South Asia has been slow. No country is on track to meet the World Health Assembly target to halve anaemia prevalence in women of reproductive age by 2025. South Asia carries the world’s highest burden of both anaemia and intrauterine growth restriction (Stevens et al., 2013; Lee et al., 2013), as well as the world’s highest burden of child stunting and wasting (UNICEF et al., 2018). Given the close links between maternal and child nutrition, efforts to improve maternal nutrition are critical to attaining the Sustainable Development Goals including the targets on ending hunger and all forms of malnutrition and reducing maternal and neonatal mortality.
In November 2016, WHO released new guidelines on “Recommendations on antenatal care for a positive pregnancy experience for women” (WHO, 2016). These guidelines include a comprehensive set of eight recommendations on nutrition interventions during pregnancy (Table 1). They present a renewed opportunity to focus attention on maternal nutrition and to assist countries in ensuring policies and programmes are designed to meet the nutritional needs of women during pregnancy.
In 2018, the UNICEF Regional Office for South Asia undertook a review of the policy and programme landscape on maternal nutrition in the South Asia region (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, Sri Lanka). The purpose of this review was to examine the status of policies and programme on maternal nutrition during pregnancy in the context of the 2016 WHO nutrition recommendations on antenatal care (ANC). The specific objectives of this review were to:
• Examine the extent to which national policies and programme guidance are in-line with the 2016 WHO recommendations on maternal nutrition
• Examine the geographic and population coverage of maternal nutrition interventions
• Identify bottlenecks in translating the national maternal nutrition policy or programme guidance to programme action
This report provides a synthesis of the status of maternal nutrition in South Asia and for each of the WHO maternal nutrition recommendations examines the alignment with national policies and programme guidance, geographic and population coverage, and bottlenecks impeding the implementation of each recommendation. It is intended that this review will provide an evidence-base to guide national governments and development partners in accelerating action on maternal nutrition in the region.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 11
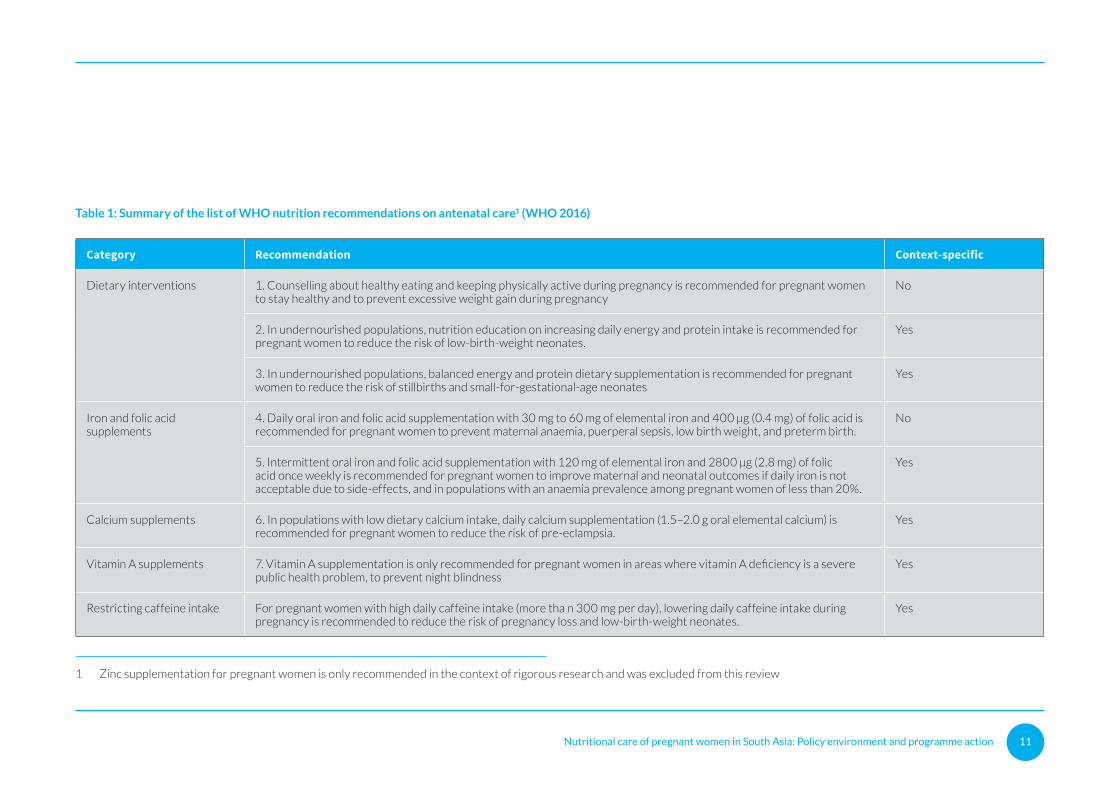
Table 1: Summary of the list of WHO nutrition recommendations on antenatal care1 (WHO 2016)
Category Recommendation Context-specific
Dietary interventions 1. Counselling about healthy eating and keeping physically active during pregnancy is recommended for pregnant women to stay healthy and to prevent excessive weight gain during pregnancy
No
2. In undernourished populations, nutrition education on increasing daily energy and protein intake is recommended for pregnant women to reduce the risk of low-birth-weight neonates.
Yes
3. In undernourished populations, balanced energy and protein dietary supplementation is recommended for pregnant women to reduce the risk of stillbirths and small-for-gestational-age neonates
Yes
Iron and folic acid supplements
4. Daily oral iron and folic acid supplementation with 30 mg to 60 mg of elemental iron and 400 μg (0.4 mg) of folic acid is recommended for pregnant women to prevent maternal anaemia, puerperal sepsis, low birth weight, and preterm birth.
No
5. Intermittent oral iron and folic acid supplementation with 120 mg of elemental iron and 2800 μg (2.8 mg) of folic acid once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects, and in populations with an anaemia prevalence among pregnant women of less than 20%.
Yes
Calcium supplements 6. In populations with low dietary calcium intake, daily calcium supplementation (1.5–2.0 g oral elemental calcium) is recommended for pregnant women to reduce the risk of pre-eclampsia.
Yes
Vitamin A supplements 7. Vitamin A supplementation is only recommended for pregnant women in areas where vitamin A deficiency is a severe public health problem, to prevent night blindness
Yes
Restricting caffeine intake For pregnant women with high daily caffeine intake (more tha n 300 mg per day), lowering daily caffeine intake during pregnancy is recommended to reduce the risk of pregnancy loss and low-birth-weight neonates.
Yes
1 Zinc supplementation for pregnant women is only recommended in the context of rigorous research and was excluded from this review

Nutritional care of pregnant women in South Asia: Policy environment and programme action 12
Methods
Synthesis of data on maternal nutrition status
Data on the nutritional status of women of reproductive age was compiled from the most recent nationally representative household survey. Where available, data form the most recent survey was compared with national survey data collected approximately 10 years previously to examine the direction of change in maternal nutrition. The indicators of maternal nutritional status examined included height, body mass index (BMI) and anaemia. A low maternal stature is defined as standing stature less than 145 cm. For non-pregnant women, underweight or thinness is defined as BMI less than 18.5 kg/m2, overweight as BMI greater or equal to 25 kg/m2, and obesity as BMI greater or equal to 30 kg/m2. Anaemia in non-pregnant women is defined as a haemoglobin concentration less than 12 g/dL, and in pregnant women as haemoglobin concentration less than 11 g/dL.
To provide the context for maternal nutrition in each country, data was also compiled on the dietary intake of women (dietary diversity and intake of iron-rich foods), socio-demographic indicators (maternal education and maternal decision-making) and maternal health (maternal mortality, adolescent pregnancy, and ANC from a skilled provider). In addition, data on neonatal mortality and child nutritional status (wasting, stunting and breastfeeding practices) was collated.
The indicator definitions, national survey data and sources of national survey data included in this report are provided in Annex 2, 3 and 4.
Qualitative assessment of policies and programmes to deliver maternal nutrition interventions
Qualitative methods were used to examine the status of maternal nutrition policies and programmes in South Asia.
Review of policy and programme documents
National policies, strategies, plans and programme guidance documents were sourced through country-level partners and on-line searches. The resultant repository of over 500 documents included
35 policy documents (e.g. national health policies, reproductive health policies, nutrition policies and food policies), 37 nutrition-related plans (e.g. health master plans, health promotion strategic plans, nutrition plans, and maternal, infant and child nutrition plans) and 43 strategy documents (e.g. national reproductive, maternal, newborn and child health strategies and micronutrient strategies).
The extent to which country policies and programme guidance documents are in-line with the 2016 WHO nutrition recommendations for ANC was assessed using a modified balanced scorecard approach to analyse policy content. The policy content of national policies, strategies, plans, and programme guidance documents (including training materials and communication documents) was reviewed manually and categorized (a policy/programme guidance exists or does not exist) for each of the assessed nutrition recommendations.
A qualitative assessment was also undertaken to review the extent of alignment of the national policies and programme guidance documents with components of each of the WHO recommendations. For example, in reviewing the policy content for daily IFA supplementation, the review assessed whether the dose of iron supplement, the dose of folic acid supplement, the frequency of supplementation, and the timing of initiation of supplementation were in-line (or not in-line) with WHO recommendations. For context-specific recommendations, a judgement was made on the applicability of the recommendation or components of the recommendation, based on the country context. The results of this qualitative review were validated by national partners, including government representatives.

Nutritional care of pregnant women in South Asia: Policy environment and programme action 13
Country questionnaire
An on-line country questionnaire was developed using Google Docs forms to gather data and information on geographic coverage of maternal nutrition interventions and the bottlenecks to implementation of these interventions.
Geographic coverage was defined as the percentage of districts that are delivering a specific maternal nutrition intervention and was categorized semi-quantitatively as ‘No programme’, ‘less than 25 per cent of districts’, ’25 to 49 per cent of districts’, ’50 to 74 per cent of districts’ and ’75-100 per cent of districts’.
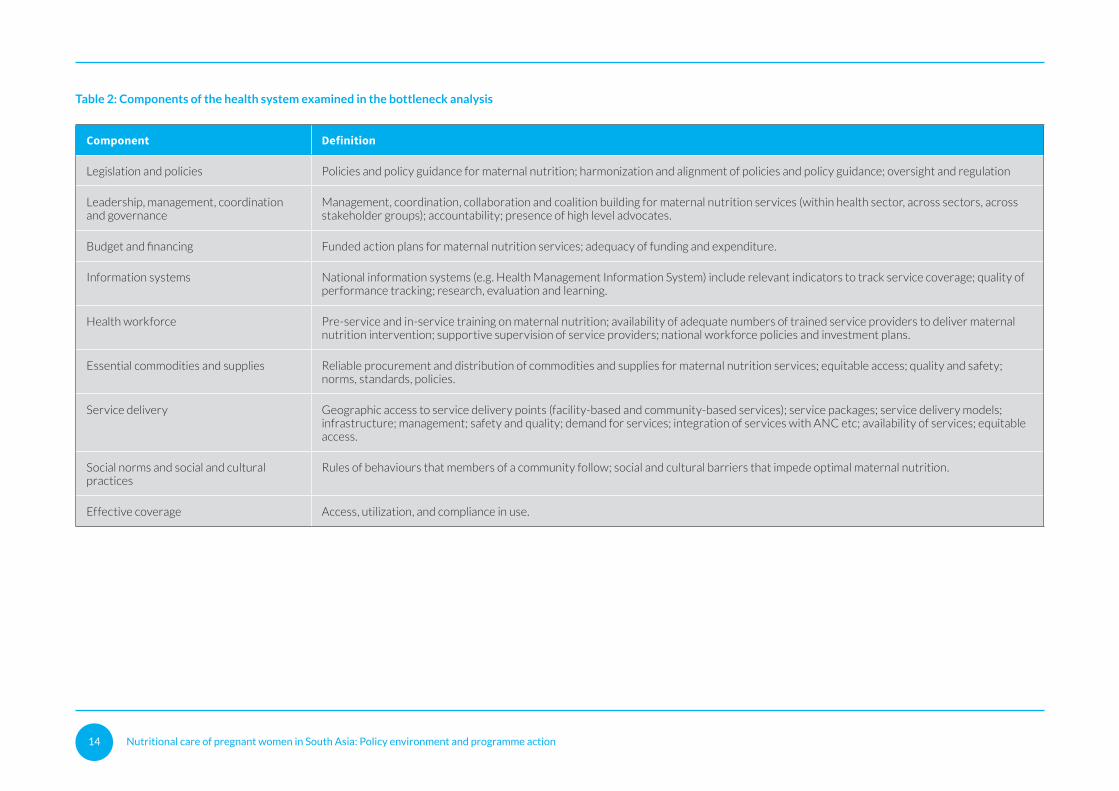
Bottlenecks in translating the national maternal nutrition policy or programme guidance for each WHO maternal nutrition intervention to programme action were examined for nine components of the health system, which were adapted from WHO’s health systems framework (Table 2). For each intervention, country respondents were asked to consensually assess whether bottlenecks existed for each of the nine components of the health system, and whether these bottlenecks were ‘mild’, ‘moderate’ or ‘significant’.
The consultative process to complete the on-line questionnaire was organized by UNICEF country offices in the eight countries between February and April 2018. The country teams ranged from two to seven individuals and comprised government representatives and partners (see Annex 5 for list of participants by country). Face to face interviews, workshop and phone interviews were used to gather information in the consultative process.
Development of country briefs
A set of eight country briefs were developed to summarize key data and information from the synthesis of data on maternal nutrition status, and the qualitative assessment of policies and programmes to deliver maternal nutrition interventions. These country briefs can be found in Annex 1.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 14
Table 2: Components of the health system examined in the bottleneck analysis
Component Definition
Legislation and policies Policies and policy guidance for maternal nutrition; harmonization and alignment of policies and policy guidance; oversight and regulation
Leadership, management, coordination and governance
Management, coordination, collaboration and coalition building for maternal nutrition services (within health sector, across sectors, across stakeholder groups); accountability; presence of high level advocates.
Budget and financing Funded action plans for maternal nutrition services; adequacy of funding and expenditure.
Information systems National information systems (e.g. Health Management Information System) include relevant indicators to track service coverage; quality of performance tracking; research, evaluation and learning.
Health workforce Pre-service and in-service training on maternal nutrition; availability of adequate numbers of trained service providers to deliver maternal nutrition intervention; supportive supervision of service providers; national workforce policies and investment plans.
Essential commodities and supplies Reliable procurement and distribution of commodities and supplies for maternal nutrition services; equitable access; quality and safety; norms, standards, policies.
Service delivery Geographic access to service delivery points (facility-based and community-based services); service packages; service delivery models; infrastructure; management; safety and quality; demand for services; integration of services with ANC etc; availability of services; equitable access.
Social norms and social and cultural practices
Rules of behaviours that members of a community follow; social and cultural barriers that impede optimal maternal nutrition.
Effective coverage Access, utilization, and compliance in use.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 15
Nutritional care of pregnant women in South Asia: Policy environment and programme action 16
Status of maternal nutrition in South Asia
This section of the report reviews the most recent national survey data on maternal nutrition in South Asia. It first describes the socio-demographic context for maternal nutrition and then examines data on the nutritional status of women, where possible comparing the most recent survey data with data from a survey conducted in the previous 10 years to determine the direction of change. A table summarizing the data on all key indicators can be found in Annex 3.
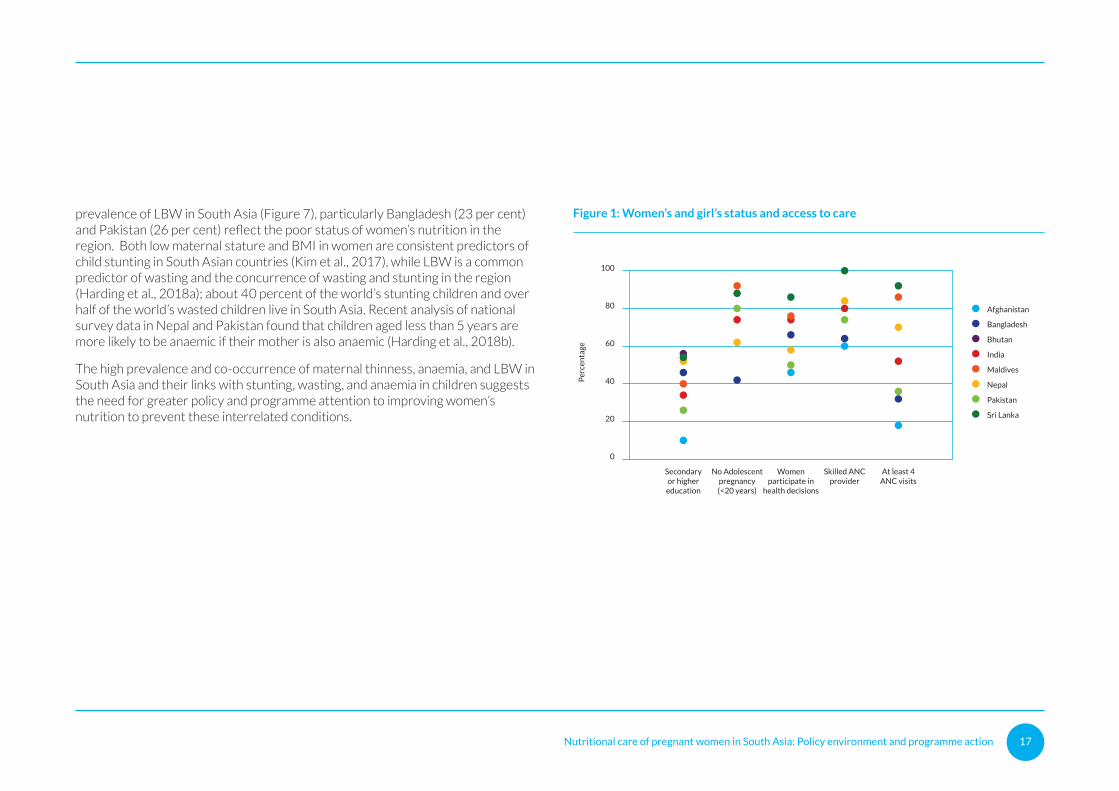
The underlying causes of maternal malnutrition include the suboptimal care of women, insufficient access to health care services, and household food insecurity, amongst others. Care, health services and food security are affected by social, economic and political factors, and the combination and relative importance of these factors differ from country to country (UNICEF, 2013). Figure 1 provides data on selected indicators of women’s and girl’s status and access to care in South Asian countries. The figure shows wide disparities between countries in the proportion of women who received secondary or higher education (9 to 55 per cent); did not experience a pregnancy in adolescence (42 to 92 per cent); are able to participate alone or jointly in decision concerning their own health care (48 to 86 per cent); received ANC from a skilled provider during their most recent pregnancy (59 to 99 per cent); and received at last 4 ANC check-ups during their most recent pregnancy (18 to 93 per cent). Multiple deprivations cluster in the same countries, with girls and women in Afghanistan, Bangladesh and Pakistan being at a significant disadvantage compared to those in Sri Lanka and the Maldives.
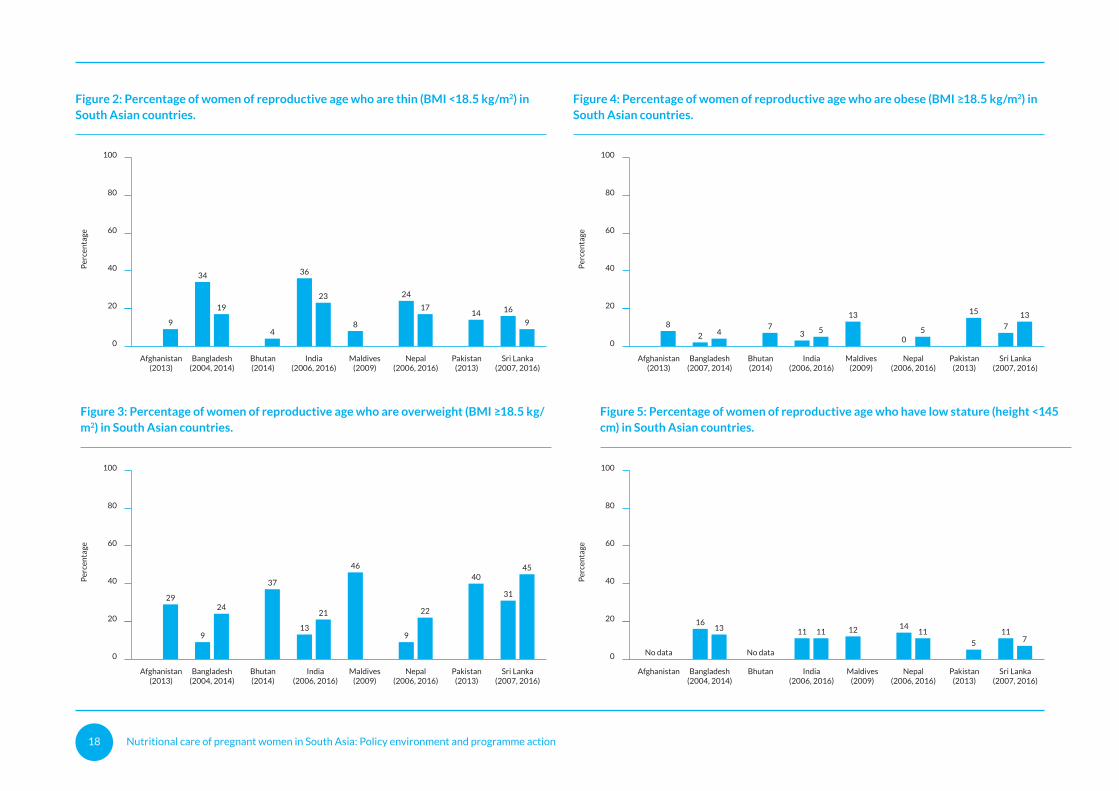
Body mass index provides a measure of thinness (or underweight), overweight and obesity for non-pregnant women. Figures 2, 3 and 4 show the prevalence of thinness, overweight and obesity in women of reproductive age in South Asian countries from the most recent national household survey. For Bangladesh, India, Nepal and Sri Lanka data are also available from a survey in the preceding 10-year period.
While substantial progress has been made, maternal thinness continues to be a public health concern in Bangladesh and India, where one in five women are affected, followed by Nepal and Pakistan where one in six women are affected. Elsewhere, the prevalence is below 10 per cent. Meanwhile the prevalence of overweight and obesity is rising at an alarming pace. In fact, the prevalence of overweight exceeds thinness in all countries except India and the prevalence of obesity exceeds thinness in four countries (Bhutan, the Maldives, Pakistan and Sri Lanka). More than one-third of women are overweight in Bhutan, the Maldives, Sri Lanka and Pakistan. This underlies why counselling on health diet and physical activity to prevent excessive weight gain in pregnancy needs to be a standard component of ANC in all countries.
Maternal height has increased in Bangladesh, Nepal and Sri Lanka over the last decade but there has been no change in the percentage of women with low height (<145 cm) in India (Figure 5). Overall, about one in ten women in the region have a low stature, which is a risk factor for obstructed labour as well as low birth weight, stunting and wasting. There is no data on maternal height in Afghanistan or Bhutan.
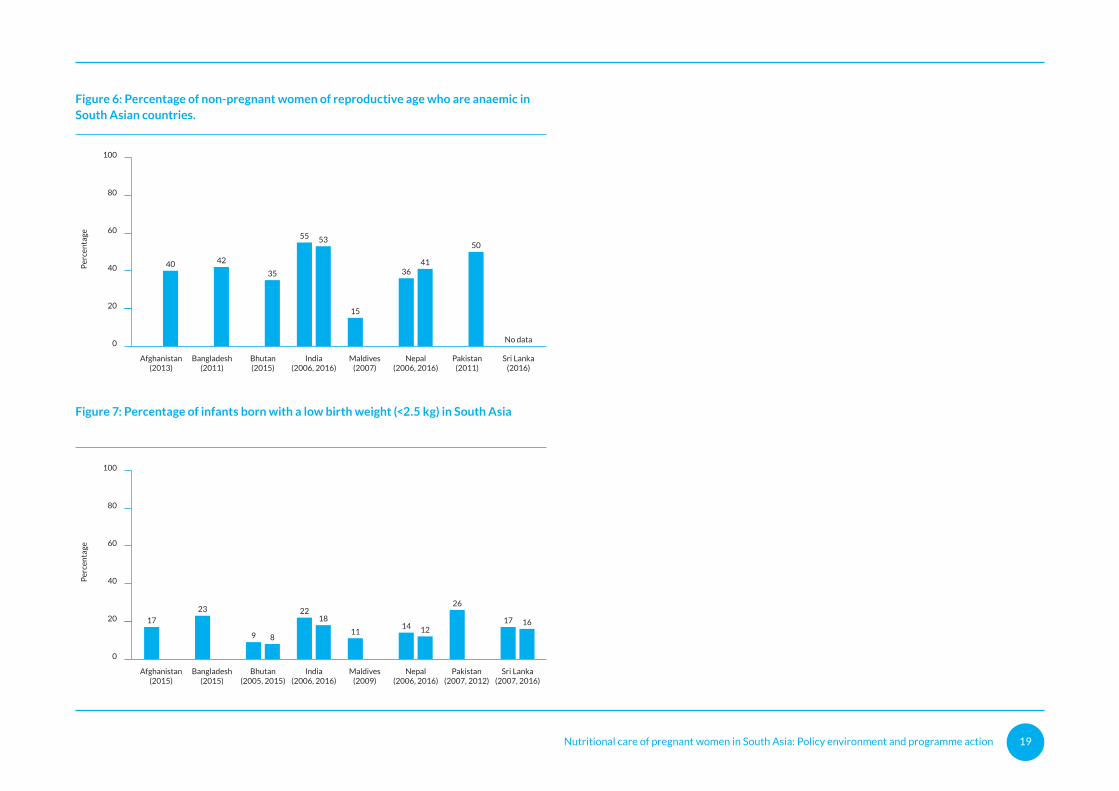
Anaemia is a severe public health problem (prevalence ≥40 percent) in Afghanistan, Bangladesh, India, Nepal and Pakistan, and a moderate public health problem (20-39 per cent) in Bhutan (Figure 6). In fact, only Maldives has brought the prevalence below 20 per cent. Only India and Nepal have data from two surveys in the last 10 years, and neither country has been successful in lowering the prevalence. It is not surprising, therefore, that no country in South Asia is on track to meet the World Health Assembly target to reduce anaemia in women of reproductive age by 50 per cent by 2025.
The nutritional status of women before and during pregnancy has a profound effect on foetal growth and development as well as the mother’s own health and well-being. A child whose pregnant mother is short, thin or anaemia is more likely to experience in utero growth restriction, preterm delivery and LBW. The high
Secondaryor higher
education
No Adolescentpregnancy(<20 years)
Womenparticipate in
health decisions
Skilled ANCprovider
At least 4ANC visits
0
20
40
60
80
100
Per
cen
tage
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 17
Secondaryor higher
education
No Adolescentpregnancy(<20 years)
Womenparticipate in
health decisions
Skilled ANCprovider
At least 4ANC visits
0
20
40
60
80
100
Per
cen
tage
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
prevalence of LBW in South Asia (Figure 7), particularly Bangladesh (23 per cent) and Pakistan (26 per cent) reflect the poor status of women’s nutrition in the region. Both low maternal stature and BMI in women are consistent predictors of child stunting in South Asian countries (Kim et al., 2017), while LBW is a common predictor of wasting and the concurrence of wasting and stunting in the region (Harding et al., 2018a); about 40 percent of the world’s stunting children and over half of the world’s wasted children live in South Asia. Recent analysis of national survey data in Nepal and Pakistan found that children aged less than 5 years are more likely to be anaemic if their mother is also anaemic (Harding et al., 2018b).
The high prevalence and co-occurrence of maternal thinness, anaemia, and LBW in South Asia and their links with stunting, wasting, and anaemia in children suggests the need for greater policy and programme attention to improving women’s nutrition to prevent these interrelated conditions.
Figure 1: Women’s and girl’s status and access to care
Nutritional care of pregnant women in South Asia: Policy environment and programme action 18
Afghanistan Bangladesh(2004, 2014)
Bhutan India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
Per
cen
tage
16
No dataNo data
11 12 141113 11 11
5 7
Afghanistan(2013)
Bangladesh(2004, 2014)
Bhutan(2014)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
Per
cen
tage
Afghanistan(2013)
Bangladesh(2004, 2014)
Bhutan(2014)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
Per
cen
tage
34 36
8
24
16
9
19
4
23
1714
9
Afghanistan(2013)
0
Bangladesh(2007, 2014)
Bhutan(2014)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
20
40
60
80
100
Per
cen
tage
2 3
13
0
784
7 5 5
15 13
913
46
9
312924
37
21 22
4045
Figure 4: Percentage of women of reproductive age who are obese (BMI ≥18.5 kg/m2) in South Asian countries.
Figure 5: Percentage of women of reproductive age who have low stature (height <145 cm) in South Asian countries.
Figure 2: Percentage of women of reproductive age who are thin (BMI <18.5 kg/m2) in South Asian countries.
Figure 3: Percentage of women of reproductive age who are overweight (BMI ≥18.5 kg/m2) in South Asian countries.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 19
Afghanistan Bangladesh(2004, 2014)
Bhutan India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
Per
cen
tage
16
No dataNo data
11 12 141113 11 11
5 7
Afghanistan(2013)
Bangladesh(2004, 2014)
Bhutan(2014)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
Per
cen
tage
Afghanistan(2013)
Bangladesh(2004, 2014)
Bhutan(2014)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
Per
cen
tage
34 36
8
24
16
9
19
4
23
1714
9
Afghanistan(2013)
0
Bangladesh(2007, 2014)
Bhutan(2014)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2013)
Sri Lanka(2007, 2016)
20
40
60
80
100
Per
cen
tage
2 3
13
0
784
7 5 5
15 13
913
46
9
312924
37
21 22
4045
Afghanistan(2013)
Bangladesh(2011)
Bhutan(2015)
India(2006, 2016)
Maldives(2007)
Nepal(2006, 2016)
Pakistan(2011)
Sri Lanka(2016)
Afghanistan(2015)
Bangladesh(2015)
Bhutan(2005, 2015)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2007, 2012)
Sri Lanka(2007, 2016)
0
20
40
60
80
100
0
20
40
60
80
100
Per
cen
tage
Per
cen
tage
55
15
36
No data
40 42
35
53
41
50
23
9
1722
1114
26
17
8
18
1216
Figure 6: Percentage of non-pregnant women of reproductive age who are anaemic in South Asian countries.
Figure 7: Percentage of infants born with a low birth weight (<2.5 kg) in South Asia
Nutritional care of pregnant women in South Asia: Policy environment and programme action 20
Nutritional care of pregnant women in South Asia: Policy environment and programme action 21
Status of policy and programme action
This section of the report provides the findings of the qualitative assessment of policies and programmes to deliver of maternal nutrition interventions.
Each of the eight WHO recommendations for the nutritional care of women during ANC is examined in turn. First, the recommendation is described, including the contexts in which the recommendation is relevant. Second, the alignment of national policy and/or programme guidance with the WHO recommendation is reviewed, and any gaps are identified. Third, data on the geographic coverage (proportion of districts that implement the intervention) and population coverage (proportion of women who received the intervention during pregnancy) is provided. Finally, bottlenecks in translating the national policy or programme guidance to programme action are described.

Nutritional care of pregnant women in South Asia: Policy environment and programme action 22
© Society for Health Education/2016/Milzero
Nutritional care of pregnant women in South Asia: Policy environment and programme action 23
Recommendation 1:Counselling on healthy eating and physical activity
Recommendation
Counselling about healthy eating and keeping physically active during pregnancy is recommended by WHO to help pregnant women stay healthy and to prevent excessive weight gain during pregnancy. This recommendation is applicable in all contexts.
A healthy diet contains adequate energy, protein, vitamins and minerals, and is obtained through the consumption of a variety of foods, including green and orange vegetables, meat, fish, beans, nuts, whole grains and fruit. A healthy lifestyle includes aerobic physical activity and strength-conditioning exercise aimed at maintaining an appropriate level of fitness throughout pregnancy.
Policy and programme guidance
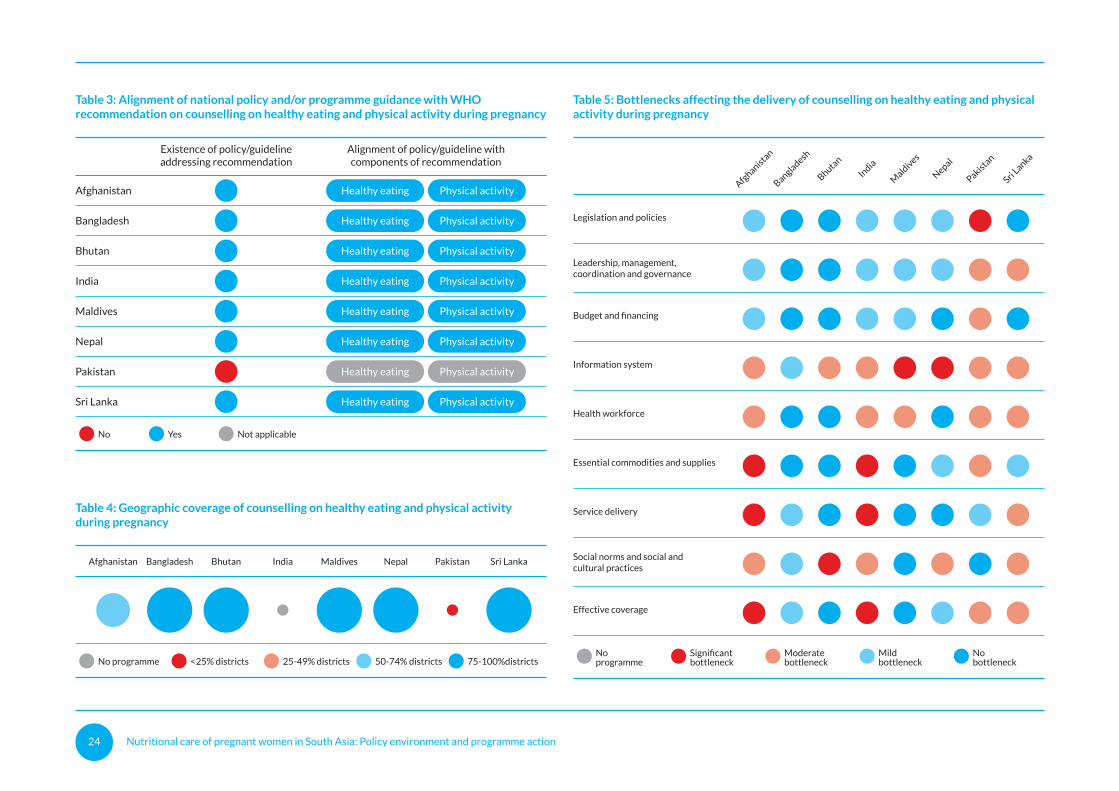
The recommendation to provide counselling about healthy eating and keeping physically active during pregnancy is included in national policy and/or programme guidance in all countries except Pakistan (Table 3). The recommendation is reflected in a range of national policy and programme documents including those that specifically focus on maternal and reproductive health and nutrition and those that are designed to improve feeding practices (maternal, infant and young child feeding and food-based dietary guidelines) and physical activity.
The policy and programme documents are broadly aligned with WHO recommendations for both components of healthy eating and keeping physically active. Provisions for culturally appropriate healthy eating have been included in communication and counselling materials in India, covering food taboos related to pregnancy and nutrition education on home augmented snacks recipes to prevent excessive weight gain in pregnancy. Weight gain recommendations are included in dietary guidelines in Bangladesh, in the Multi-Sector Nutrition Plan in Nepal and in the Sri Lanka National Health Policy (2016 – 2025).
Geographic and population coverage
Five countries estimate that between 75-100 per cent of districts deliver counselling support on healthy eating and physical activity to prevent excessive weight gain: Bangladesh, Bhutan, Maldives, Nepal and Sri Lanka (Table 4). Estimated coverage in Afghanistan is 50-74 percent, while coverage in Pakistan is less than 25 per cent of districts and there is no structured programmatic interventionin India, despite the existence of relevant policies or programme guidance. No data on population coverage of intervention was identified across all countries.
Bottlenecks
Whilst most countries in the region have policy and programme guidance provisions aligned with this recommendation, various bottlenecks are encountered in translating the provisions into programmatic action (Table 5). Afghanistan, India, Pakistan and Sri Lanka experience the greatest number of moderate and significant bottlenecks.
Moderate and significant bottleneck are most common for information systems (seven countries), followed by social norms and social and cultural practices (six countries) and the health workforce (five countries). Constraints in capture of coverage data are common because counselling services are rarely captured in information systems, and there is no agreed indicator on counselling on healthy eating and physical activity to prevent excessive weight gain. The health workforce is a common bottleneck because of the lack of a community health workforce to deliver counselling, and because this workforce does not have the knowledge and competencies to counsel mothers on healthy eating and physical activity; capacity building initiatives for health and community workers have tended to focus on improving dietary intake and limiting heavy physical activity to prevent undernutrition during pregnancy. The lack of focus of counselling services on the prevention of excessive weight gain may explain why social norms and social and cultural practices continue to be a bottleneck in a large number of countries.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 24
Table 3: Alignment of national policy and/or programme guidance with WHOrecommendation on counselling on healthy eating and physical activity during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Table 4: Geographic coverage of counselling on healthy eating and physical activityduring pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 5: Bottlenecks affecting the delivery of counselling on healthy eating and physicalactivity during pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 25
Table 3: Alignment of national policy and/or programme guidance with WHOrecommendation on counselling on healthy eating and physical activity during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Healthy eating Physical activity
Table 4: Geographic coverage of counselling on healthy eating and physical activityduring pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 5: Bottlenecks affecting the delivery of counselling on healthy eating and physicalactivity during pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka

Nutritional care of pregnant women in South Asia: Policy environment and programme action 26
© UNICEF/2016/Pirozzi
Nutritional care of pregnant women in South Asia: Policy environment and programme action 27
Recommendation 2:Nutrition education to increase energy and protein intake
Recommendation
In undernourished populations, nutrition education on increasing daily energy and protein intake is recommended for pregnant women to reduce the risk of low birth-weight neonates. While there is no specific definition of ‘undernourished populations’, a 20–39 per cent prevalence of underweight women (BMI <18.5 kg/m2) is considered a high prevalence of underweight and 40 per cent or higher is considered a very high prevalence. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider additional complementary interventions, such as distribution of balanced protein and energy supplements (see Recommendation 3).
Policy and programme guidance
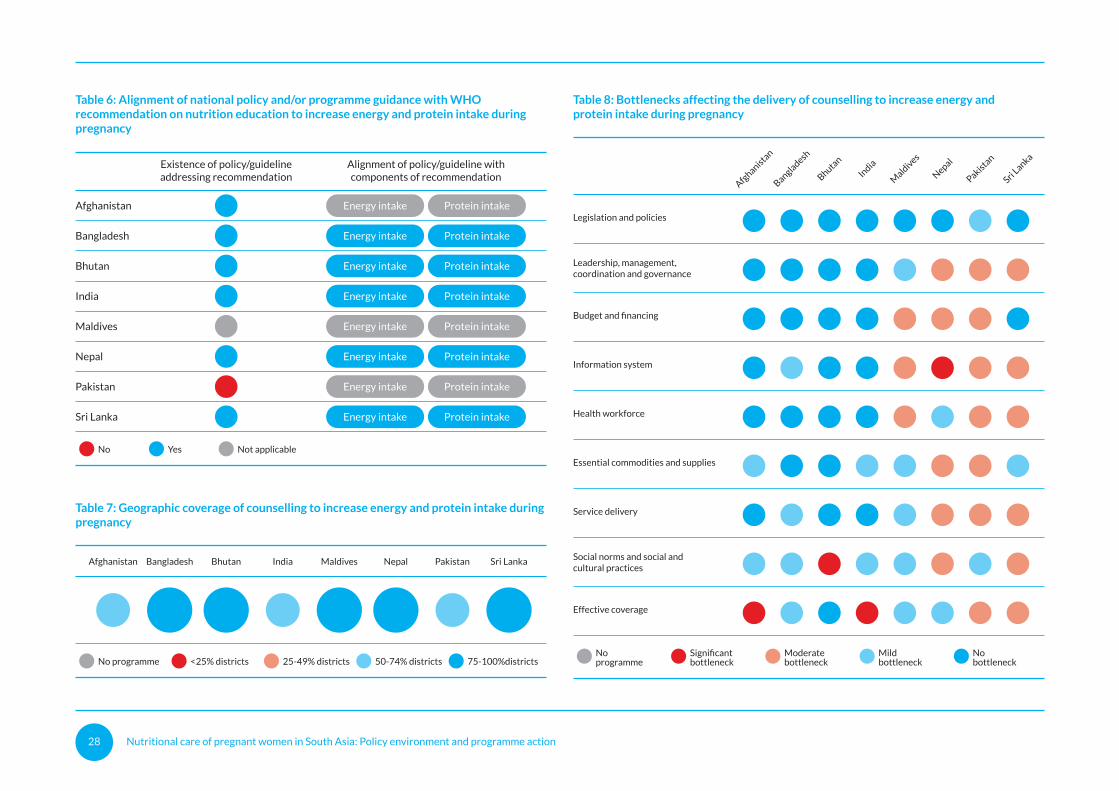
The recommendation to provide nutrition education on increasing daily energy and protein intake during pregnancy is included in national policy and/or programme guidance in all countries except Pakistan and the Maldives (Table 6). Where policies and programme guidance, exist they are aligned with WHO recommendations on energy and protein intake, except in Afghanistan, where information is lacking. This recommendation is considered not applicable in the Maldives, where the prevalence of underweight in women is low compared to overweight and obesity.
Most policies include specific conditions for providing support for pregnant women in undernourished populations. Some of the conditions identified are: pregnant women are undernourished or wasted; population living in food insecure areas; hard to reach populations groups; pregnant women in the lowest wealth quintile; pregnant women in underserved areas, including plantation communities; or urban poor population.
Geographic and population coverage
Nutrition education support on increasing daily energy and protein intake for pregnant women is delivered across all countries in the region with at least 50 per cent of districts delivering some form of counselling support (Table 7). The geographic coverage is 50-74 per cent of districts in Afghanistan, India and Pakistan, and 75-100 per cent of districts in Bangladesh, Bhutan, Maldives, Nepal, Sri Lanka. There is no data on population coverage.
Bottlenecks
Nepal, Pakistan and Sri Lanka experience the greatest number of moderate and significant bottlenecks to implementing this recommendation on nutrition education on increasing daily energy and protein intake during pregnancy (Table 8). Moderate and significant bottleneck are most common for information systems (four countries) and effective coverage (four countries), and three countries indicate bottlenecks in leadership management, coordination and governance; budget and financing; and the health workforce. Essential commodities and supplies, service delivery, and social norms and social and cultural practices are moderate or significant bottlenecks in two countries.
Several of these bottlenecks stem from the lack of priority given to nutrition education and counselling within all pillars of the health system, from the leadership to budgets, service delivery and programme monitoring, that collectively impact on effective coverage.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 28
Table 6: Alignment of national policy and/or programme guidance with WHOrecommendation on nutrition education to increase energy and protein intake duringpregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Table 7: Geographic coverage of counselling to increase energy and protein intake duringpregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 8: Bottlenecks affecting the delivery of counselling to increase energy andprotein intake during pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 29
Table 6: Alignment of national policy and/or programme guidance with WHOrecommendation on nutrition education to increase energy and protein intake duringpregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Energy intake Protein intake
Table 7: Geographic coverage of counselling to increase energy and protein intake duringpregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 8: Bottlenecks affecting the delivery of counselling to increase energy andprotein intake during pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka

Nutritional care of pregnant women in South Asia: Policy environment and programme action 30
© UNICEF/2014/Biswas
Nutritional care of pregnant women in South Asia: Policy environment and programme action 31
Recommendation 3:Balanced energy and protein dietary supplementation
Recommendation
In undernourished populations, balanced energy and protein dietary supplementation is recommended for pregnant women to reduce the risk of stillbirths and small-for-gestational-age neonates. While there is no specific definition of ‘undernourished populations’, a 20–39 per cent prevalence of underweight women (BMI <18.5 kg/m2) is considered a high prevalence of underweight and 40 per cent or higher is considered a very high prevalence.
Policy and programme guidance
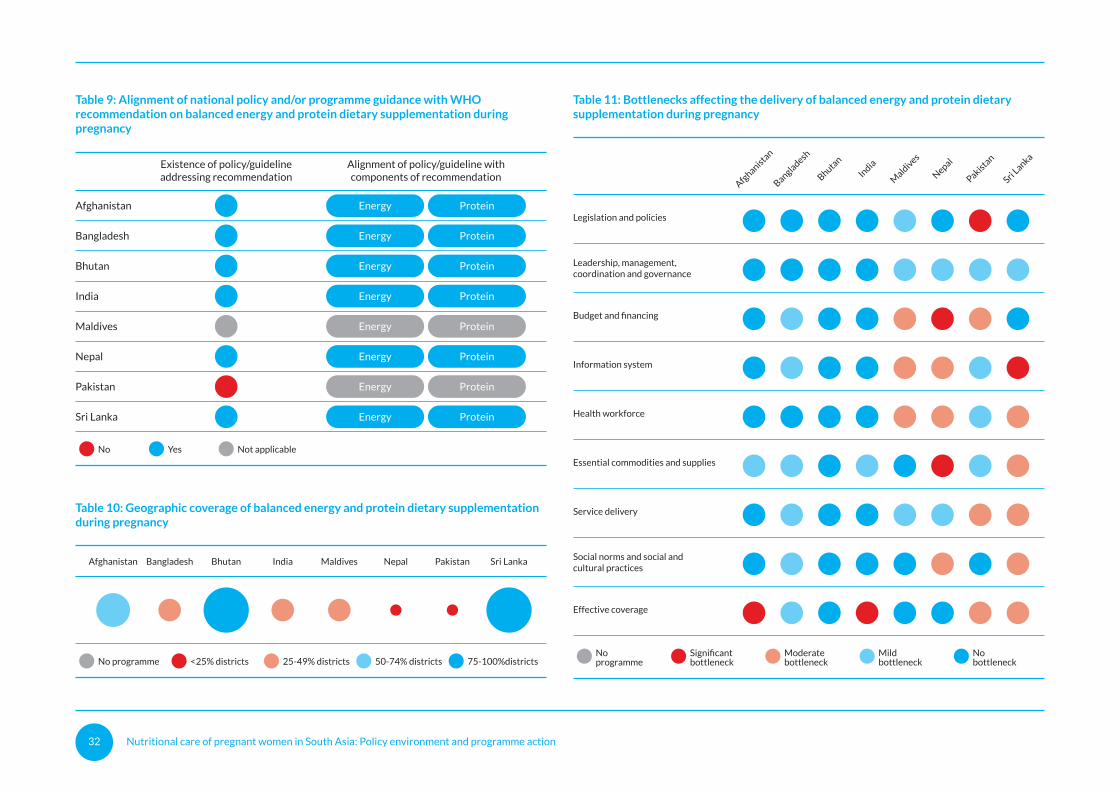
The recommendation to provide balanced protein and energy dietary supplementation during pregnancy in undernourished populations is included in national policy and/or programme guidance in all countries except Pakistan and the Maldives (Table 9). These are the same two countries that do not have a policy and/or programme guidance on nutrition education on increasing daily energy and protein intake during pregnancy. This recommendation is considered not applicable in the Maldives, where the prevalence of underweight in women is low compared to overweight and obesity. Where policies and programme guidance, exist they are aligned with WHO recommendations on energy and protein supplementation.
Geographic and population coverage
The geographic coverage of balanced protein and protein dietary supplementation during pregnancy is in general much lower than nutrition education to increase protein and energy intake in undernourished populations (Table 10). This intervention is delivered in 75-100 percent of districts in only Bhutan and Sri Lanka, 50-74 percent in Afghanistan, 24-49 per cent in Bangladesh, India and Maldives, and less than 25 per cent in Nepal and Pakistan. There is no data on population coverage.
Bottlenecks
Nepal, Pakistan and Sri Lanka experience the greatest number of moderate and significant bottlenecks to implementing this recommendation, similar to the recommendation on nutrition education on increasing daily energy and protein intake during pregnancy (Table 11). Moderate and significant bottleneck are most common for the health workforce (four countries), information systems (four countries) and effective coverage (four countries). Three countries indicate moderate or significant bottlenecks in budget and financing and essential commodities and supplies. Service delivery and social norms and social and cultural practices are moderate bottlenecks in two countries.
In undernourished populations,
balanced energy and protein dietary
supplementation is recommended for
pregnant women.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 32
Table 9: Alignment of national policy and/or programme guidance with WHOrecommendation on balanced energy and protein dietary supplementation duringpregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Table 10: Geographic coverage of balanced energy and protein dietary supplementationduring pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 11: Bottlenecks affecting the delivery of balanced energy and protein dietarysupplementation during pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 33
Table 9: Alignment of national policy and/or programme guidance with WHOrecommendation on balanced energy and protein dietary supplementation duringpregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Energy Protein
Table 10: Geographic coverage of balanced energy and protein dietary supplementationduring pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 11: Bottlenecks affecting the delivery of balanced energy and protein dietarysupplementation during pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka

Nutritional care of pregnant women in South Asia: Policy environment and programme action 34
© Nutrition International/Bangladesh/2017
Nutritional care of pregnant women in South Asia: Policy environment and programme action 35
Recommendation 4:Daily iron and folic acid supplementation
Recommendation
Daily oral IFA supplementation with 30 mg to 60 mg of elemental iron and 400 μg (0.4 mg) of folic acid is recommended for pregnant women to prevent maternal anaemia, puerperal sepsis, low birth weight, and preterm birth. Supplementation should begin as early as possible in pregnancy. This recommendation is applicable in all contexts.
Policy and programme guidance
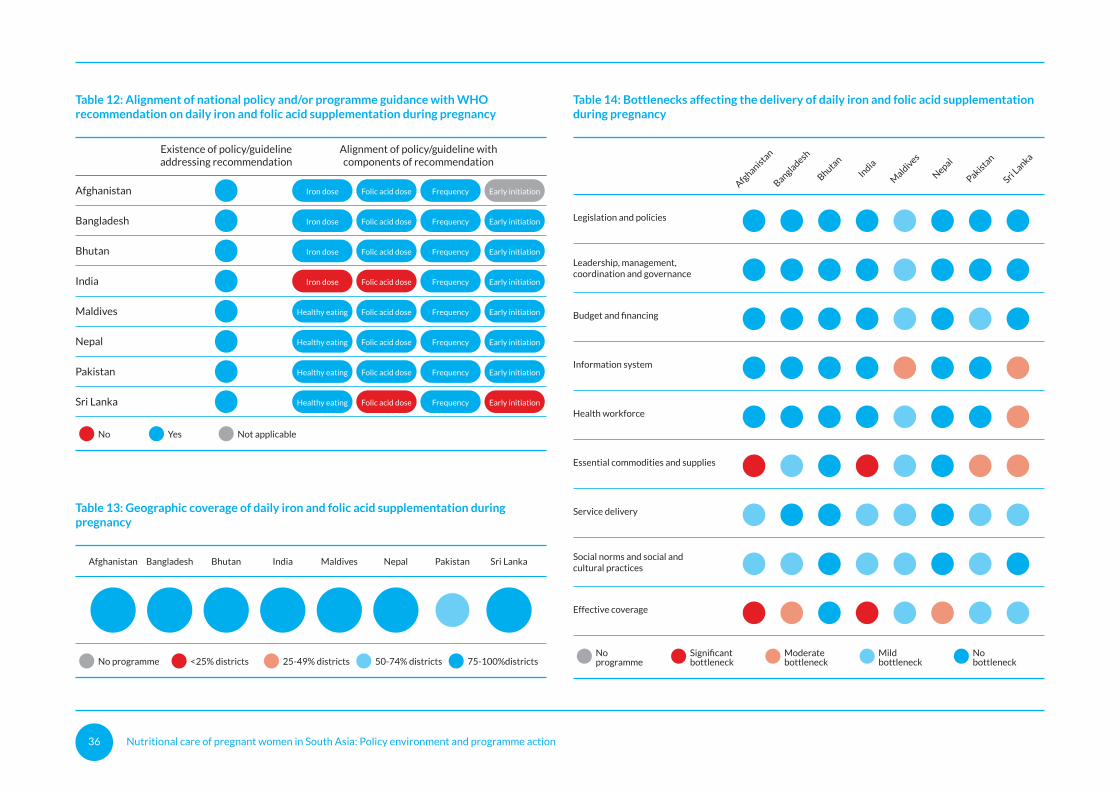
All countries in the region have policy/programme guidance provisions for daily IFA supplementation (Table 12). The dosage of IFA, the frequency of supplementation and early initiation are generally consistent with the WHO recommendation, but there are a few exceptions. India, the recommended dose of iron is 100 mg iron, higher than the 30-60 mg recommended by WHO. In both India and Sri Lanka, the recommended dose of folic acid is higher than the 400 μg recommended by WHO (500 μg and 1 mg respectively). There is no mention of the timing of commencement of supplementation in Afghanistan and Sri Lanka.
Geographic and population coverage
All countries reported that 75-100 per cent of districts deliver IFA supplements to pregnant women, except Pakistan, where the geographic coverage is lower (50-74 per cent) (Table 13).
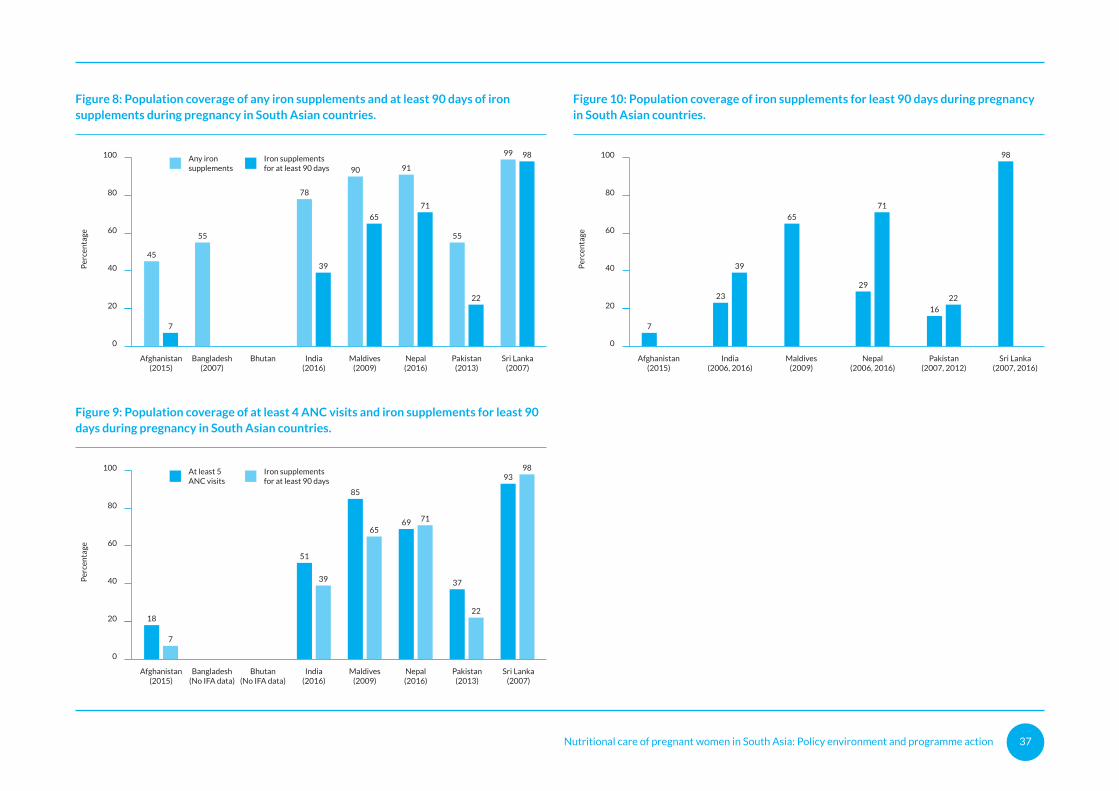
Population-level coverage of iron supplementation is available for all countries except Bhutan. Figure 8 shoes that coverage of any iron supplements during pregnancy exceeds 80 per cent in only Maldives, Nepal and Sri Lanka. Coverage of iron supplements for at least 90 days, the minimum duration considered necessary, is considerably lower, except in Sri Lanka. Figure 9 shows that the coverage of iron supplements for at least 90 days is similar to the coverage of at least four ANC check-ups, indicating that the access to ANC
may be a limiting factor for the effective coverage of iron supplementation. There are only three countries (India, Nepal and Pakistan) that have data from two surveys on the coverage of iron supplements for at least 90 days during pregnancy (Figure 10). While Nepal has achieved substantial success in increasing coverage between 2006 (29 per cent) and 2016 (71 per cent), the increase in coverage in India over the same period has only been 13 percentage points, while coverage increased by only 6 percentage points between 2007 and 2013 in Pakistan.
Bottlenecks
While daily IFA supplementation is one of the most commonly implemented maternal nutrition interventions across all the South Asian countries, the variation in population coverage both between and within countries points to uneven implementation of this recommendation. Moderate and significant bottleneck are most common for essential commodities and supplies (four countries) and effective coverage (four countries), followed by information systems (two countries) (Table 14).
Bottlenecks in the essential commodities and supplies health system pillar are a barrier to effective delivery of services in Afghanistan, India, Pakistan and Sri Lanka. Procurement constraints are a challenge in Afghanistan, where supplies are procured through development partners’ supply chains and poor quality is an issue. In Pakistan, there are supply breaks due to delays in procurement, while in Sri Lanka there is no quality assurance system to ensure that quality supplies are procured.
Effective coverage of IFA supplementation is problematic in Afghanistan, Bangladesh, India and Nepal. In Bangladesh, poor ANC coverage combined with inadequate counselling are the limiting factors. In India, negative publicity about IFA supplements, the taste of supplements and side effects contribute to low adherence. In Nepal, there is inadequate counselling and follow up by Female Community Health Workers, Auxiliary Nursing Midwife and health workers to counter the low demand for supplements.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 36
Table 12: Alignment of national policy and/or programme guidance with WHOrecommendation on daily iron and folic acid supplementation during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Healthy eating Folic acid dose
Healthy eating Folic acid dose
Healthy eating Folic acid dose
Healthy eating Folic acid dose
Table 13: Geographic coverage of daily iron and folic acid supplementation duringpregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districts
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Moderatebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 14: Bottlenecks affecting the delivery of daily iron and folic acid supplementationduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 37
Table 12: Alignment of national policy and/or programme guidance with WHOrecommendation on daily iron and folic acid supplementation during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Healthy eating Folic acid dose
Healthy eating Folic acid dose
Healthy eating Folic acid dose
Healthy eating Folic acid dose
Table 13: Geographic coverage of daily iron and folic acid supplementation duringpregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districts
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Frequency Early initiation
Moderatebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 14: Bottlenecks affecting the delivery of daily iron and folic acid supplementationduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Afghanistan(2015)
Bangladesh(No IFA data)
Bhutan(No IFA data)
At least 5ANC visits
India(2016)
Maldives(2009)
Nepal(2016)
Pakistan(2013)
Sri Lanka(2007)
Afghanistan(2015)
India(2006, 2016)
Maldives(2009)
Nepal(2006, 2016)
Pakistan(2007, 2012)
Sri Lanka(2007, 2016)
Afghanistan(2015)
Bangladesh(2007)
Bhutan India(2016)
Maldives(2009)
Nepal(2016)
Pakistan(2013)
Sri Lanka(2007)
0
20
40
60
80
100
0
20
40
60
80
100
0
20
40
60
80
100
Per
cen
tage
Per
cen
tage
Per
cen
tage
51
18
85
69
9893
7
39
65
71
22
37
7
65
29
98
23
39
71
16
22
55
78
90 91
99
55
45
7
39
71
65
22
98
Iron supplementsfor at least 90 days
Any ironsupplements
Iron supplementsfor at least 90 days
Figure 8: Population coverage of any iron supplements and at least 90 days of iron supplements during pregnancy in South Asian countries.
Figure 9: Population coverage of at least 4 ANC visits and iron supplements for least 90 days during pregnancy in South Asian countries.
Figure 10: Population coverage of iron supplements for least 90 days during pregnancy in South Asian countries.

Nutritional care of pregnant women in South Asia: Policy environment and programme action 38
© UNICEF/2015/Lemoyne
Nutritional care of pregnant women in South Asia: Policy environment and programme action 39
Table 15: Alignment of national policy and/or programme guidance with WHOrecommendation on intermittent iron and folic acid supplementation during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Iron dose Folic acid dose
Weekly frequency
Weekly frequency
Weekly frequency
Weekly frequency
Weekly frequency
Weekly frequency
Weekly frequency
Weekly frequency
Recommendation 5:Intermittent iron and folic acid supplementation
Recommendation
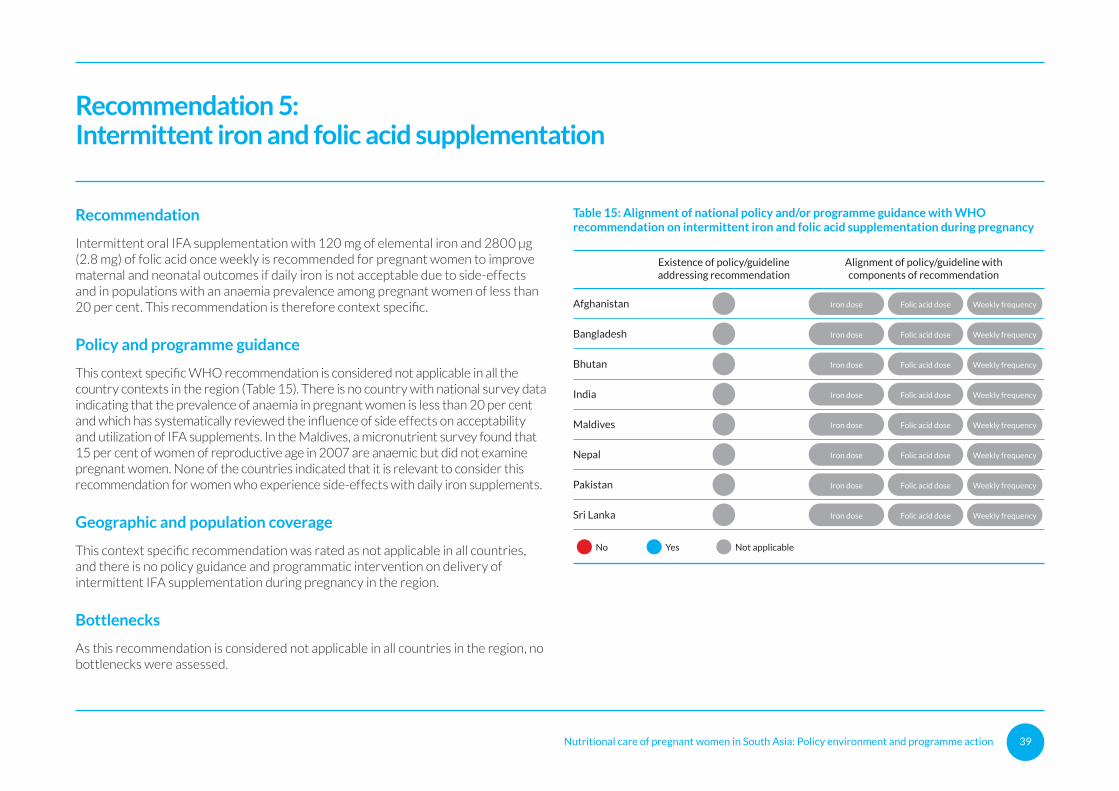
Intermittent oral IFA supplementation with 120 mg of elemental iron and 2800 μg (2.8 mg) of folic acid once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects and in populations with an anaemia prevalence among pregnant women of less than 20 per cent. This recommendation is therefore context specific.
Policy and programme guidance
This context specific WHO recommendation is considered not applicable in all the country contexts in the region (Table 15). There is no country with national survey data indicating that the prevalence of anaemia in pregnant women is less than 20 per cent and which has systematically reviewed the influence of side effects on acceptability and utilization of IFA supplements. In the Maldives, a micronutrient survey found that 15 per cent of women of reproductive age in 2007 are anaemic but did not examine pregnant women. None of the countries indicated that it is relevant to consider this recommendation for women who experience side-effects with daily iron supplements.
Geographic and population coverage
This context specific recommendation was rated as not applicable in all countries, and there is no policy guidance and programmatic intervention on delivery of intermittent IFA supplementation during pregnancy in the region.
Bottlenecks
As this recommendation is considered not applicable in all countries in the region, no bottlenecks were assessed.

Nutritional care of pregnant women in South Asia: Policy environment and programme action 40
© UNICEF/2016/Brown
Nutritional care of pregnant women in South Asia: Policy environment and programme action 41
Recommendation 6:Calcium supplementation
Recommendation
In populations with low dietary calcium intake, daily calcium supplementation (1.5–2.0 g oral elemental calcium) is recommended for pregnant women to reduce the risk of pre-eclampsia from 20 weeks of pregnancy.
Policy and programme guidance
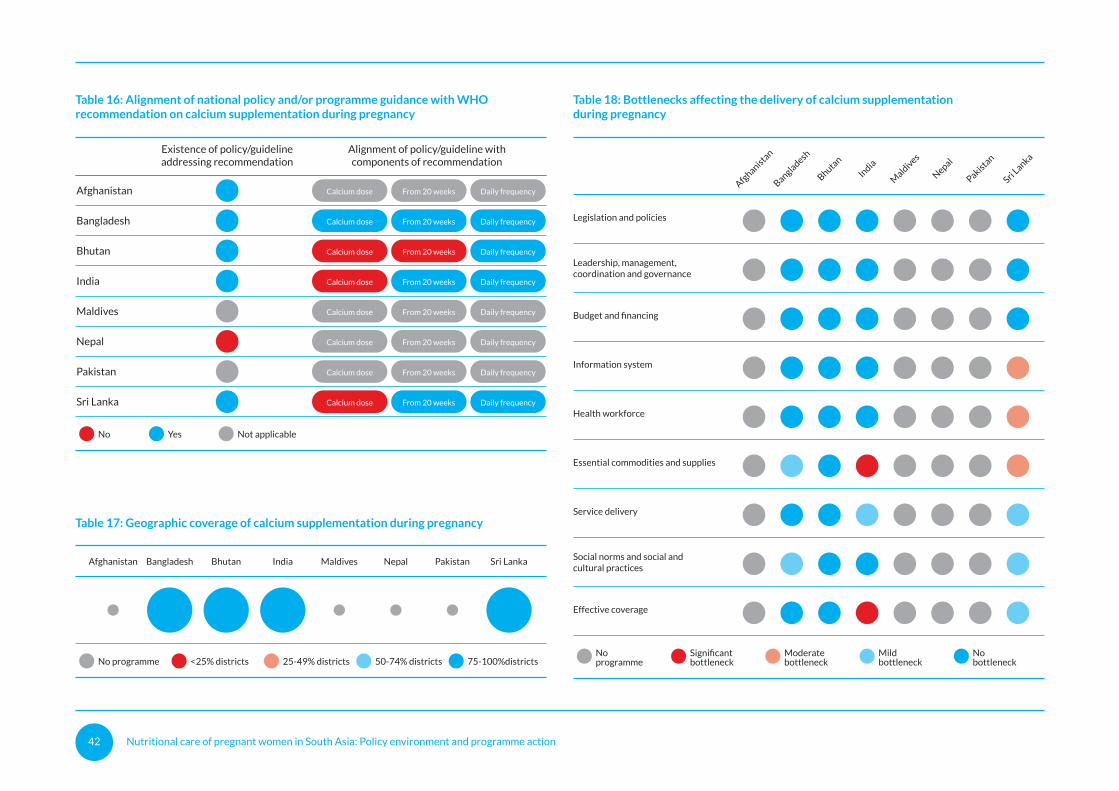
Five countries in the region have a policy and/or programme guidance provisions for daily calcium supplementation during pregnancy: Afghanistan, Bangladesh, Bhutan, India and Sri Lanka (Table 16). In Nepal, calcium supplementation has been delivered in small pilots but there is no national policy, programme guidance or programme. Calcium supplementation is considered not applicable in the Maldives and Pakistan. In Pakistan, only one province has a policy for calcium supplementation.
The dosage of daily calcium supplements is aligned with the WHO recommendation in Bangladesh only; elsewhere, the recommended dose is lower than the WHO recommendation (India and Sri Lanka) or is not specified. The frequency of provision of calcium supplements and timing of initiation of the supplementation is generally in line with WHO recommendations. However, there is no information on when to initiate calcium supplementation in the Bhutan policy/programme guidance.
Geographic and population coverage
Except for Afghanistan, all countries with policies/programme guidance on calcium supplementation are delivering programmes and report to reach 75-100 per cent of districts (Table 17). While policy provisions are in place in Afghanistan, calcium supplementation is still at a piloting phase. There is no data on population coverage in any country.
Bottlenecks
Only the four countries with active programmes (Bangladesh, Bhutan, India and Sri Lanka) examined bottlenecks to implementation of the WHO recommendation on calcium supplementation (Table 18). India and Sri Lanka reported moderate or significant bottlenecks, with constraints in supplies being a common issue in both countries. In India, a lack of adherence by pregnant women to daily supplementation is a bottleneck to the attainment of effective coverage. In Sri Lanka, calcium supplementation is not captured by the health information system, and the insufficient health workforce is also considered a bottleneck to the effective implementation of this WHO recommendation.
Five countries in the region have a policy
and/or programme guidance provisions
for daily calcium supplementation during
pregnancy.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 42
Table 17: Geographic coverage of calcium supplementation during pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districts
Table 16: Alignment of national policy and/or programme guidance with WHOrecommendation on calcium supplementation during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Moderatebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 18: Bottlenecks affecting the delivery of calcium supplementationduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 43
Table 17: Geographic coverage of calcium supplementation during pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districts
Table 16: Alignment of national policy and/or programme guidance with WHOrecommendation on calcium supplementation during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Calcium dose From 20 weeks
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Daily frequency
Moderatebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 18: Bottlenecks affecting the delivery of calcium supplementationduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka

Nutritional care of pregnant women in South Asia: Policy environment and programme action 44
© UNICEF/UNI47693/Khemka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 45
Recommendation 7:Vitamin A supplementation
Recommendation
Vitamin A supplementation is only recommended for pregnant women in areas where vitamin A deficiency is a severe public health problem to prevent night blindness. Vitamin A deficiency is considered a severe public health problem if 5 per cent or more of women in a population have a history of night blindness in their most recent pregnancy in the previous 3–5 years that ended in a live birth, or if 20 per cent or more of pregnant women have a serum retinol level below 0.70 μmol/L. In areas where supplementation is indicated for vitamin A deficiency, it can be given daily (up to 10,000 IU) or weekly (up to 25,000 IU).
Policy and programme guidance
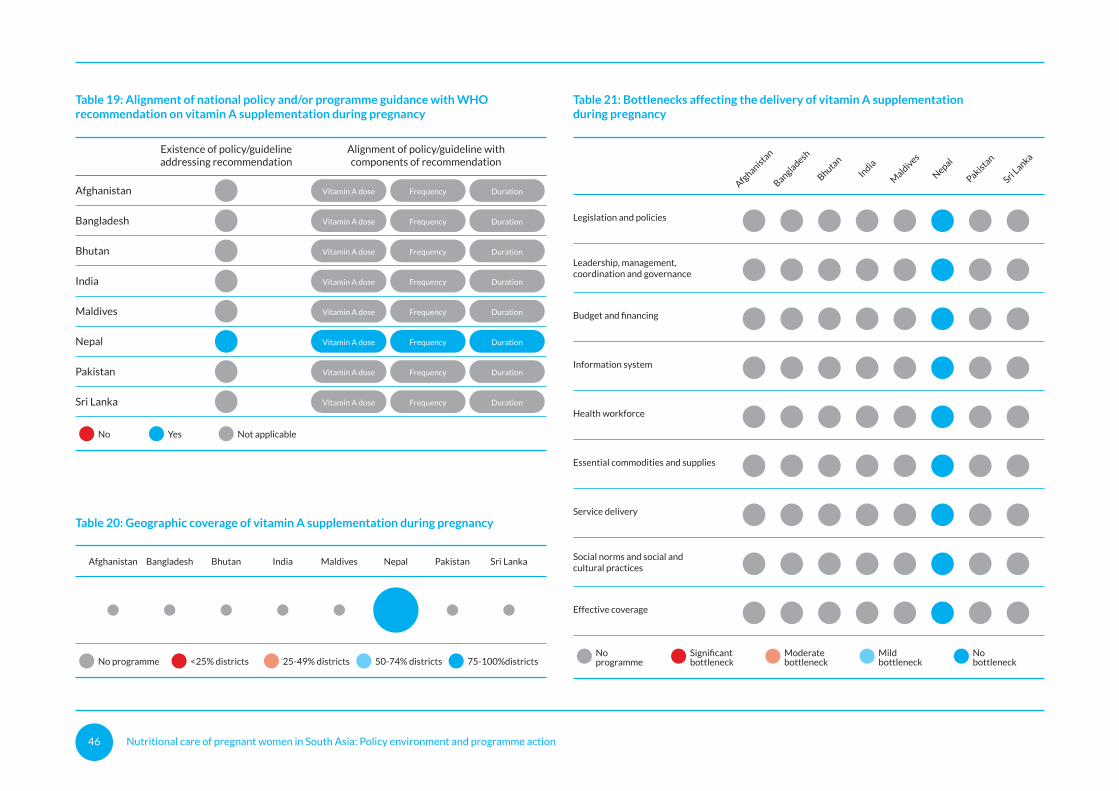
This context specific WHO recommendation for vitamin A supplementation during pregnancy was rated as not applicable in all countries except Nepal, where provisions exist in a national policy/programme guidance that align with the WHO recommendation (Table 19).
Geographic and population coverage
Nepal is the only country in the region with a policy/programme guidance provision for vitamin A supplementation for pregnant women. Other South Asian countries do not consider this recommendation to be applicable to their contexts and as a result there is no programmatic intervention (Table 20). In Nepal, the programme to deliver vitamin A supplementation to pregnant women is estimated to cover 75-100 per cent of districts (Table 20). There is no data on population coverage.
Bottlenecks
The country self-assessment process did not highlight any bottlenecks constraining implementation of recommendation on vitamin A supplementation in Nepal (Table 21).
Nepal is the only country in the region
with a policy/programme guidance
provision for vitamin A supplementation
for pregnant women.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 46
Table 19: Alignment of national policy and/or programme guidance with WHOrecommendation on vitamin A supplementation during pregnancy
Not applicableNo Yes
Table 20: Geographic coverage of vitamin A supplementation during pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districts
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Duration
Duration
Duration
Duration
Duration
Duration
Duration
Duration
Moderatebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 21: Bottlenecks affecting the delivery of vitamin A supplementationduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Nutritional care of pregnant women in South Asia: Policy environment and programme action 47
Table 19: Alignment of national policy and/or programme guidance with WHOrecommendation on vitamin A supplementation during pregnancy
Not applicableNo Yes
Table 20: Geographic coverage of vitamin A supplementation during pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districts
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Vitamin A dose Frequency
Duration
Duration
Duration
Duration
Duration
Duration
Duration
Duration
Moderatebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 21: Bottlenecks affecting the delivery of vitamin A supplementationduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka

Nutritional care of pregnant women in South Asia: Policy environment and programme action 48
© UNICEF/2016/Pirozzi
Nutritional care of pregnant women in South Asia: Policy environment and programme action 49
Recommendation 8:Restricting caffeine intake
Recommendation
For pregnant women with high daily caffeine intake (more than 300 mg per day), lowering daily caffeine intake during pregnancy is recommended to reduce the risk of pregnancy loss and low-birth-weight neonates. Pregnant women should be informed that a high daily caffeine intake (>300 mg per day) is probably associated with a higher risk of pregnancy loss and low birth weight.
Policy and programme guidance
The WHO recommendation on restricting caffeine intake during pregnancy was rated as not applicable in Afghanistan, India, Pakistan and Sri Lanka (Table 22). It is incorporated into policy and/or programme guidance documents in Bhutan, Maldives and Nepal and is missing in Bangladesh.
Geographic and population coverage
In the three countries that have incorporated this recommendation into policy and/or programme guidance (Bhutan, the Maldives and Nepal) the intervention is delivered in 75-100 per cent of districts (Table 23). There is no data on population coverage.
Bottlenecks
Among the three countries delivering interventions to restrict caffeine intake, only one bottleneck was identified: in the Maldives the information system is considered a moderate bottleneck to effective implementation of this recommendation (Table 24).
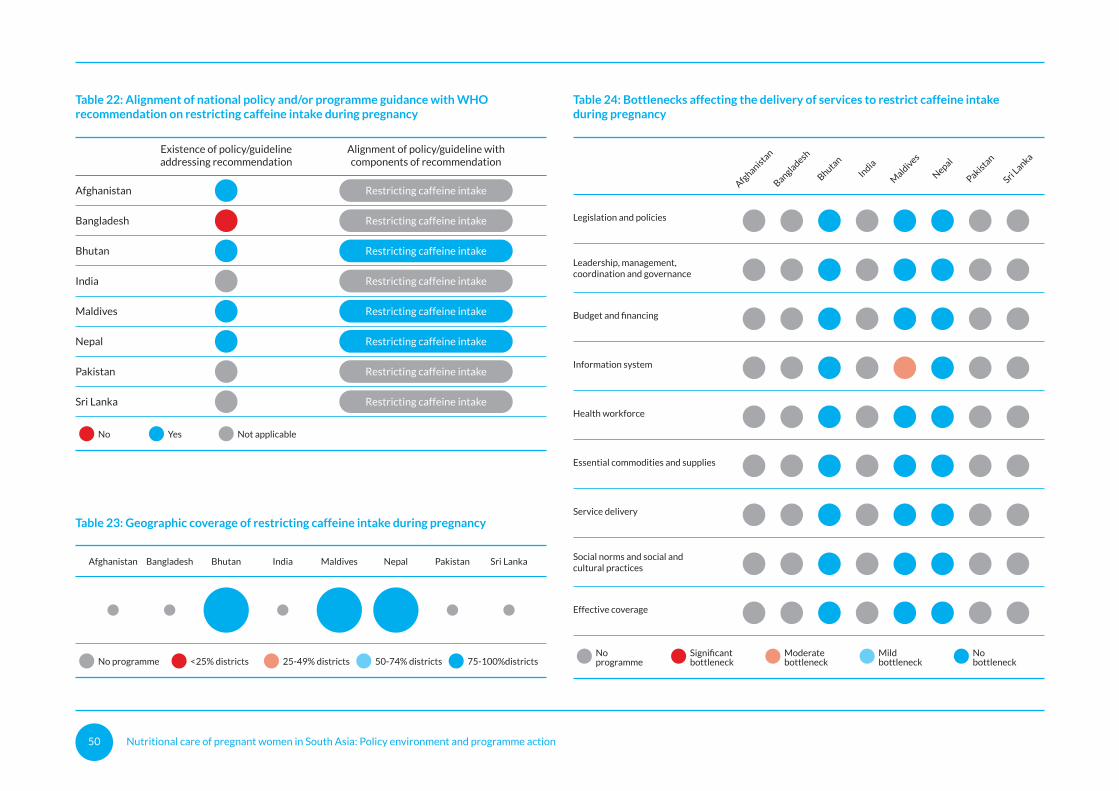
Nutritional care of pregnant women in South Asia: Policy environment and programme action 50
Table 22: Alignment of national policy and/or programme guidance with WHOrecommendation on restricting caffeine intake during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Table 23: Geographic coverage of restricting caffeine intake during pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 24: Bottlenecks affecting the delivery of services to restrict caffeine intakeduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka

Nutritional care of pregnant women in South Asia: Policy environment and programme action 51
Table 22: Alignment of national policy and/or programme guidance with WHOrecommendation on restricting caffeine intake during pregnancy
Not applicableNo Yes
Existence of policy/guidelineaddressing recommendation
Alignment of policy/guideline withcomponents of recommendation
Afghanistan
Bangladesh
Bhutan
India
Maldives
Nepal
Pakistan
Sri Lanka
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Restricting caffeine intake
Table 23: Geographic coverage of restricting caffeine intake during pregnancy
25-49% districtsNo programme <25% districts
Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
50-74% districts 75-100%districtsModeratebottleneck
Noprogramme
Significantbottleneck
Mildbottleneck
Nobottleneck
Legislation and policies
Leadership, management,coordination and governance
Budget and financing
Information system
Health workforce
Essential commodities and supplies
Service delivery
Social norms and social andcultural practices
Effective coverage
Table 24: Bottlenecks affecting the delivery of services to restrict caffeine intakeduring pregnancy
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Summary
Countries in South Asia may not reach the nutrition targets of the World Health Assembly and Sustainable Development Goals without the improved nutritional care of women. Maternal undernutrition has grave consequences for the mother and her infant, including increased risk of maternal mortality, low birth weight and small-for-gestational age infants, preterm delivery, neural tube defects, poor growth in early life and cognitive loss. Maternal overnutrition raises the risk of haemorrhage, hypertensive disorders, gestational diabetes and macrosomia (high birth weight).
While progress has been made in reducing thinness (underweight) and increasing women’s height in South Asia, the status of women’s nutrition remains a serious cause for concern. One in five women in the region are too thin (BMI <18.5 kg/m2); one in ten women in the region have a short stature (<145 cm); overweight and obesity are rapidly rising; and anaemia is a severe or moderate public health problem in six countries, with no country on track to meet the World Health Assembly target to halve anaemia in women by 2025. The double burden of malnutrition – the coexistence of undernutrition with overweight and obesity – presents policy and programming challenges for the region. The low levels of maternal education and women’s participation in household decisions, adolescent pregnancy, inadequate access to ANC and poor diets underpin the high prevalence of malnutrition in women of reproductive age in the region.
The “WHO recommendations on antenatal care for a positive pregnancy experience” (WHO, 2016) include recommendations on the nutritional care of women and provide an opportunity to refocus attention to maternal nutrition within the broader reproductive and maternal health landscape. This policy and programme landscape review examines the extent to which national policies in South Asian countries are in-line with the 2016 WHO recommendations on maternal nutrition and provides insights on the health system bottlenecks that are constraining the translation of these policies to programme action.
The policy intent to address maternal nutrition in the context of ANC is captured in various policy and programmatic guidance documents in all countries across the region. However, the review of national policies and programmes found that no country has adopted all maternal nutrition interventions that are recommended by WHO. The number of recommendations covered by national policies or programme guidance ranges from one to six across countries (Table 25). These provisions are found in a variety of policies, strategies, plans and programme guidance documents. There are two WHO recommendations that are applicable in all contexts: daily IFA supplementation and counselling on healthy eating and keeping physically active to prevent excessive weight gain during pregnancy. All countries have national policies or programme guidance on daily IFA supplementation, and all countries except Pakistan have national policies or programme guidance to counsel pregnant women on dietary intake and physical activity to prevent excessive intake.
However, the number of countries with national policies or programme guidance that cover the context-specific recommendations is lower, particularly for intermittent IFA supplementation and vitamin A supplementation, and these recommendations are considered not applicable in several countries. It is likely that countries in the region have not fully considered the conditions under which these context-specific recommendations should be applied. There are also gaps in the alignment of policy and programme guidance with specific components of these recommendations, which may weaken their impact during implementation. For example, the provisions on daily IFA supplementation are not always fully aligned with the corresponding WHO recommendation on the dose of IFA and on timing of initiation of supplementation. The review also highlighted gaps in consolidation of policy provisions under a unified common framework for addressing maternal nutrition. In a number of countries, the policy and program guidance provisions are scattered across many documents and frameworks, leaving countries without an overarching overview of policy interventions addressing maternal nutrition.
Nutritional care of pregnant women in South Asia: Policy environment and programme action 52
Periodic review of policy provisions and programme guidance is necessary to ensure consistency with global recommendations.
The extent to which countries in South Asia are implementing national level policies and programme guidance on maternal nutrition interventions was assessed qualitatively through a consultative process at country level to estimate geographic coverage (proportion of districts implementing a specific maternal nutrition intervention) and to identify health system bottlenecks impeding implementation.
The geographic coverage of maternal nutrition interventions in South Asia is not at the level needed to transform the care of women during pregnancy and varies between countries and interventions (Table 26). IFA supplementation is delivered in at least 75 per cent of districts in seven countries, but five or less countries are delivering the other interventions at this geographic scale. Balanced energy and protein dietary supplementation for pregnant women in undernourished populations has the least geographic coverage. Both Pakistan and Afghanistan are delivering interventions in less than half of districts, except for IFA supplements in Afghanistan.
Data on the population coverage is only available for IFA supplements, indicating gaps in the capacity of national information systems to the track coverage of maternal nutrition interventions. The proportion of women who received an iron supplement for at least 90 days during the previous pregnancy ranges from 7 per cent in Afghanistan to 98 per cent in Sri Lanka, and is less than 70 per cent in India, Maldives and Pakistan (there is no data for Bangladesh and Bhutan). This indicates that a high geographic coverage does not necessarily translate into good population level coverage. The proportion of women who take IFA supplements for at least 90 days during pregnancy is closely correlated with the coverage of at least four ANC visits, illustrating the importance of delivery platforms, including community-based services, in reaching women with supplements.
Bottlenecks to the implementation of maternal nutrition interventions vary by intervention type and country. The Maldives, Nepal, Pakistan and Sri Lanka reported a greater number of moderate and significant bottlenecks than other countries. The bottlenecks persist at all levels of the health system; however, moderate and significant bottlenecks tend to be concentrated at the ‘downstream’ level (the demand for, supply of, and quality of services). This means that even though policy environments may be conducive, there are implementation barriers that ultimately limit the population coverage and quality of interventions. However, there are
some exceptions such as Pakistan, where significant gaps at the policy level remain for interventions such as counselling on dietary intake and physical activity and balanced protein-energy supplementation.
It is important to build on the tremendous political momentum on nutrition in the region accrued in the past five years and ensure that these national efforts give sufficient attention to the scale-up of maternal nutrition interventions. While the health sector cannot solve all the underlying causes of poor maternal nutrition, it must ensure that women have access to quality nutrition and health care during ANC. An evidence-based review of epidemiological context, national policies and guidelines, together with a sound understanding of the implementation bottlenecks and barriers, can assist countries in identifying the actions needed to deliver maternal nutrition interventions through the ANC platform at scale and with equity.
In light of this evidence base, the following actions are recommended for countries in the region to accelerate action on maternal nutrition:
1. Undertake an evidence-based review and update of country maternal nutrition policies and programme guidance provisions in the context of the 2016 WHO nutrition recommendations for ANC. The review should pay attention to context and conditions under which the WHO recommendations apply.
2. Prioritize maternal nutrition in in national development agenda, and sectoral plans and budgets, including national efforts to reduce maternal mortality, stunting and other forms of malnutrition.
3. Develop costed national and subnational plans for financing the sustainable scale-up of maternal nutrition interventions, with public sector and development partner support. These plans should include actions that are informed by a comprehensive analysis of the bottlenecks to implementing maternal nutrition interventions at scale with quality and equity, and targets on the coverage of maternal nutrition interventions within health sector strategies and plans.
4. Develop programme implementation guidance and tools to support the implementation of the WHO recommendations, including practical guidance on subnational planning, budgeting, supply management, training packages and social and behaviour change communication materials.

Nutritional care of pregnant women in South Asia: Policy environment and programme action 53
5. Strengthen intra-sectoral (within health) and cross-sectoral coordination (across sectors) of the implementation of maternal nutrition policies and programme guidance through establishment and/or reinforcement of coordination structures within Ministry of Health and other cross sectoral platforms.
6. Strengthen the monitoring and tracking of maternal nutrition coverage indicators through household surveys, health information systems and programme monitoring and reporting systems for all the recommended WHO maternal nutrition interventions.
7. Invest in implementation research to understand implementation bottlenecks and optimal approaches that drive improvements in the coverage, quality and equity of maternal nutrition interventions.
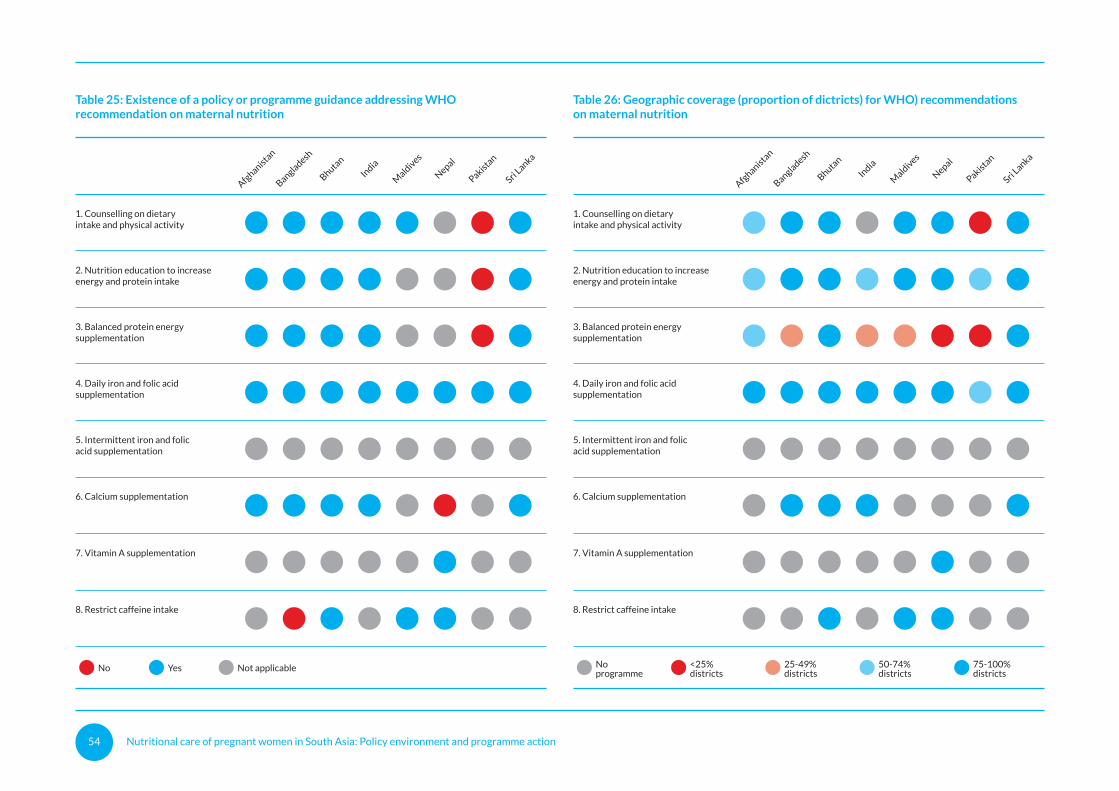
Nutritional care of pregnant women in South Asia: Policy environment and programme action 54
Table 25: Existence of a policy or programme guidance addressing WHOrecommendation on maternal nutrition
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Not applicableNo Yes
1. Counselling on dietaryintake and physical activity
2. Nutrition education to increaseenergy and protein intake
3. Balanced protein energysupplementation
4. Daily iron and folic acidsupplementation
5. Intermittent iron and folicacid supplementation
6. Calcium supplementation
7. Vitamin A supplementation
8. Restrict caffeine intake
Table 26: Geographic coverage (proportion of dictricts) for WHO) recommendationson maternal nutrition
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
1. Counselling on dietaryintake and physical activity
2. Nutrition education to increaseenergy and protein intake
3. Balanced protein energysupplementation
4. Daily iron and folic acidsupplementation
5. Intermittent iron and folicacid supplementation
6. Calcium supplementation
7. Vitamin A supplementation
8. Restrict caffeine intake
25-49%districts
Noprogramme
<25%districts
50-74%districts
75-100%districts

Nutritional care of pregnant women in South Asia: Policy environment and programme action 55
Table 25: Existence of a policy or programme guidance addressing WHOrecommendation on maternal nutrition
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
Not applicableNo Yes
1. Counselling on dietaryintake and physical activity
2. Nutrition education to increaseenergy and protein intake
3. Balanced protein energysupplementation
4. Daily iron and folic acidsupplementation
5. Intermittent iron and folicacid supplementation
6. Calcium supplementation
7. Vitamin A supplementation
8. Restrict caffeine intake
Table 26: Geographic coverage (proportion of dictricts) for WHO) recommendationson maternal nutrition
Afghanista
n
Bangladesh
Bhutan
India
Mald
ives
Nepal
Pakistan
Sri Lanka
1. Counselling on dietaryintake and physical activity
2. Nutrition education to increaseenergy and protein intake
3. Balanced protein energysupplementation
4. Daily iron and folic acidsupplementation
5. Intermittent iron and folicacid supplementation
6. Calcium supplementation
7. Vitamin A supplementation
8. Restrict caffeine intake
25-49%districts
Noprogramme
<25%districts
50-74%districts
75-100%districts
References
Black, R. E., Victora, C. G., Walker, S. P., Bhutta, Z. A., Christian, P., de Onis, M., et al. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet, 382(9890), 427-451.
Brabin, B. J., Hakimi, M., & Pelletier, D. (2001). An analysis of anemia and pregnancy-related maternal mortality. Journal of Nutrition, 131(2S-2), 604S-614S.
Christian, P., Lee, S. E., Donahue Angel, M., Adair, L. S., Arifeen, S. E., Ashorn, P., et al. (2013). Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. International Journal of Epidemiology, 42(5), 1340-55.
Harding, K. L., Aguayo, V. M., & Webb, P. (2018a). Birthweight and feeding practices are associated with child growth outcomes in South Asia. Maternal & Child Nutrition, 14(Suppl 4), e12650. https://doi.org/10.1111/mcn.12650
Harding, K. L., Aguayo, V. M., Namirembe, G., & Webb, P. (2018b). Determinants of anemia among women and children in Nepal and Pakistan: An analysis of recent national survey data. Maternal & Child Nutrition, 14(Suppl 4), e12478. https://doi.org/10.1111/mcn.12478
Kim, R., Mejia-Guevara, I., Corsi, D. J., Aguayo, V. M., & Subramanian, S. V. (2017). Relative importance of 13 correlates of child stunting in South Asia: Insights from nationally representative data from Afghanistan, Bangladesh, India, Nepal, and Pakistan. Social Science & Medicine, 187, 144-154.
Lee, A. C., Katz, J., Blencowe, H., Cousens, S., Kozuki, N., Vogel, J. P., et al. (2013). National and regional estimates of term and preterm babies born small for gestational age in 138 low-income and middle-income countries in 2010. Lancet Global Health, e26-36. https://doi.org/10.1016/S2214-109X(13)70006-8.
Liu, X., Behrman, J. R., Stein, A. D., Adair, L. S., Bhargava, S. K., Borja, J. B., et al. (2017). Prenatal care and child growth and schooling in four low- and medium-income countries. PLoS One, 12(2), e0171299.
Rahman, M. M., Abe, S. K., Rahman, M. S., Kanda, M., Narita, S., Bilano. V., et al. (2016). Maternal anemia and risk of adverse birth and health outcomes in low- and middle-income countries: systematic review and meta-analysis. American Journal of Clinical Nutrition, 103(2), 495-504.
Stevens, G. A., Finucane, M. M., De-Regil, L. M., Paciorek, C. J., Flaxman, S. R., Branca, F., et al. (2013). Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. The Lancet Global Health, 1(1), e16–e25.
UNICEF (2013). Improving Child Nutrition: the Achievable Imperative for Global Progress. New York: United Nations Children’s Fund.
UNICEF (2015). Stop Stunting in South Asia: A Common Narrative on Maternal and Child Nutrition. Kathmandu: UNICEF Regional Office for South Asia.
UNICEF, WHO, & World Bank Group (2018). Joint Child Malnutrition Estimates 2018 Edition. Available at http://www.who.int/nutgrowthdb/estimates2017/en/.
WHO (2016). WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Geneva: World Health Organization. https://doi.org/10.1186/1742-4755-10-19.5
Nutritional care of pregnant women in South Asia: Policy environment and programme action 56
Annex 1:Country briefs
Nutritional care of pregnant women in South Asia: Policy environment and programme action 57
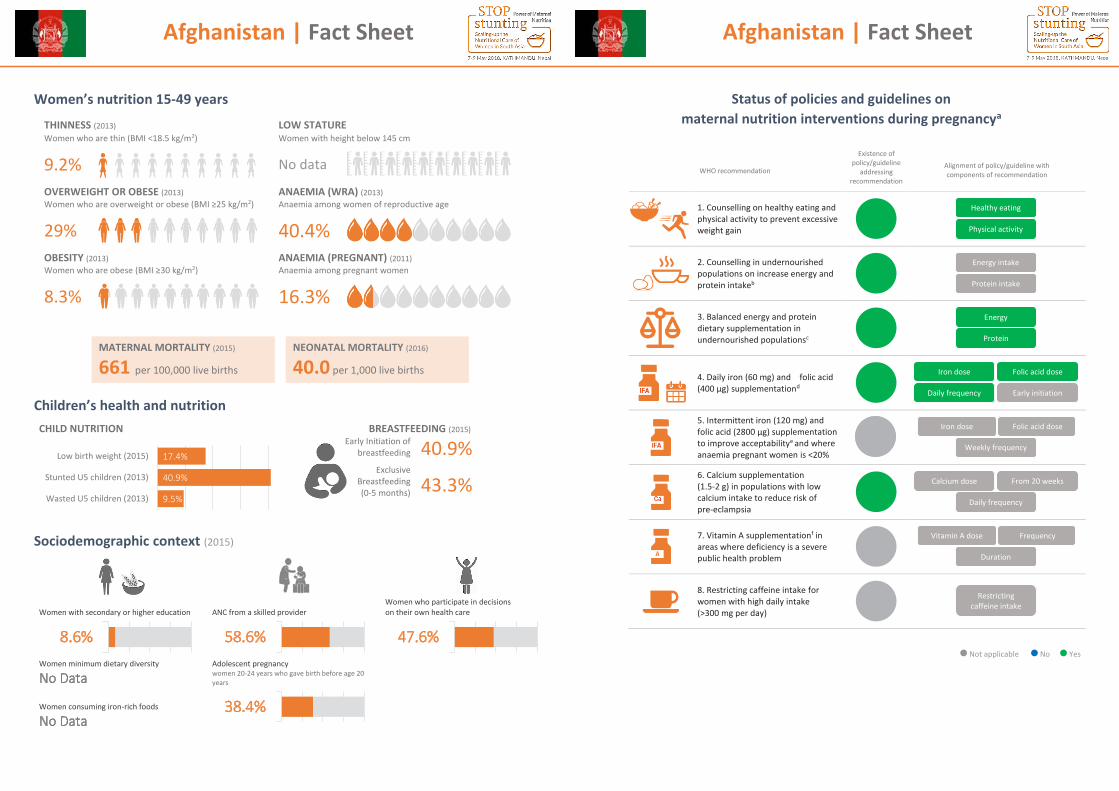
Afghanistan | Fact Sheet
1
Women’s nutrition 15-49 years
THINNESS (2013) LOW STATURE Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
9.2%
No data
OVERWEIGHT OR OBESE (2013) ANAEMIA (WRA) (2013) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age
29% 40.4% OBESITY (2013) ANAEMIA (PREGNANT) (2011) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
8.3% 16.3%
Children’s health and nutrition
CHILD NUTRITION BREASTFEEDING (2015)
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
40.9%
43.3%
Sociodemographic context (2015)
9.5%
40.9%
17.4%
Wasted U5 children (2013)
Stunted U5 children (2013)
Low birth weight (2015)
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods
No Data
8.6% 58.6% 47.6%
38.4%
MATERNAL MORTALITY (2015)
661 per 100,000 live births
NEONATAL MORTALITY (2016)
40.0 per 1,000 live births
Afghanistan | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
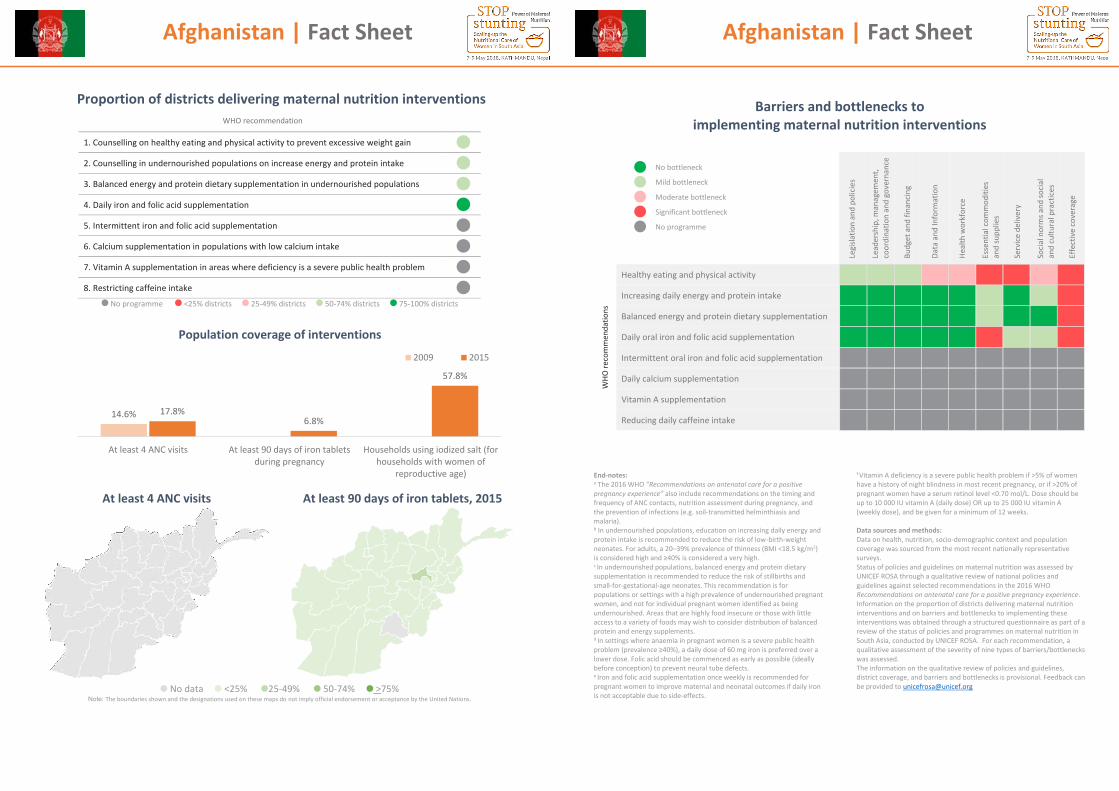
Afghanistan | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions
At least 4 ANC visits
At least 90 days of iron tablets, 2015
No data <25% 25-49% 50-74% >75%
Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
14.6% 17.8%6.8%
57.8%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt (forhouseholds with women of
reproductive age)
2009 2015
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
Afghanistan | Fact Sheet
4
Barriers and bottlenecks to implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects.
f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
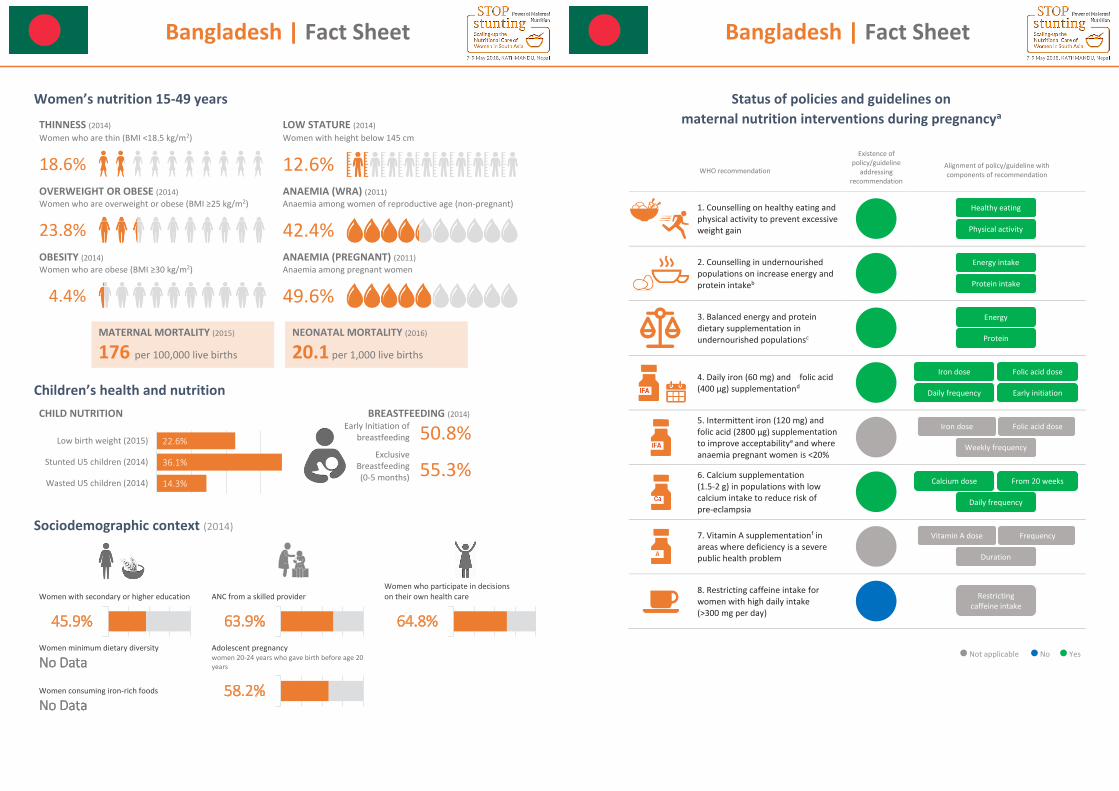
Bangladesh | Fact Sheet
1
Women’s nutrition 15-49 years
THINNESS (2014) LOW STATURE (2014) Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
18.6%
12.6% OVERWEIGHT OR OBESE (2014) ANAEMIA (WRA) (2011) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age (non-pregnant)
23.8% 42.4% OBESITY (2014) ANAEMIA (PREGNANT) (2011) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
4.4% 49.6%
Children’s health and nutrition CHILD NUTRITION BREASTFEEDING (2014)
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
50.8%
55.3%
Sociodemographic context (2014)
14.3%
36.1%
22.6%
Wasted U5 children (2014)
Stunted U5 children (2014)
Low birth weight (2015)
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods
No Data
45.9% 63.9% 64.8%
58.2%
MATERNAL MORTALITY (2015)
176 per 100,000 live births
NEONATAL MORTALITY (2016)
20.1 per 1,000 live births
Bangladesh | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
Bangladesh | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions
At least 4 ANC visits
At least 90 days of iron tablets
No data <25% 25-49% 50-74% >75%
Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
20.6%31.2%
80.3%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt(2012)
2007 2014
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
No Data

Bangladesh | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions
At least 4 ANC visits
At least 90 days of iron tablets
No data <25% 25-49% 50-74% >75%
Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
20.6%31.2%
80.3%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt(2012)
2007 2014
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
No Data
Bangladesh | Fact Sheet
4
Barriers and bottlenecks to
implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects.
f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
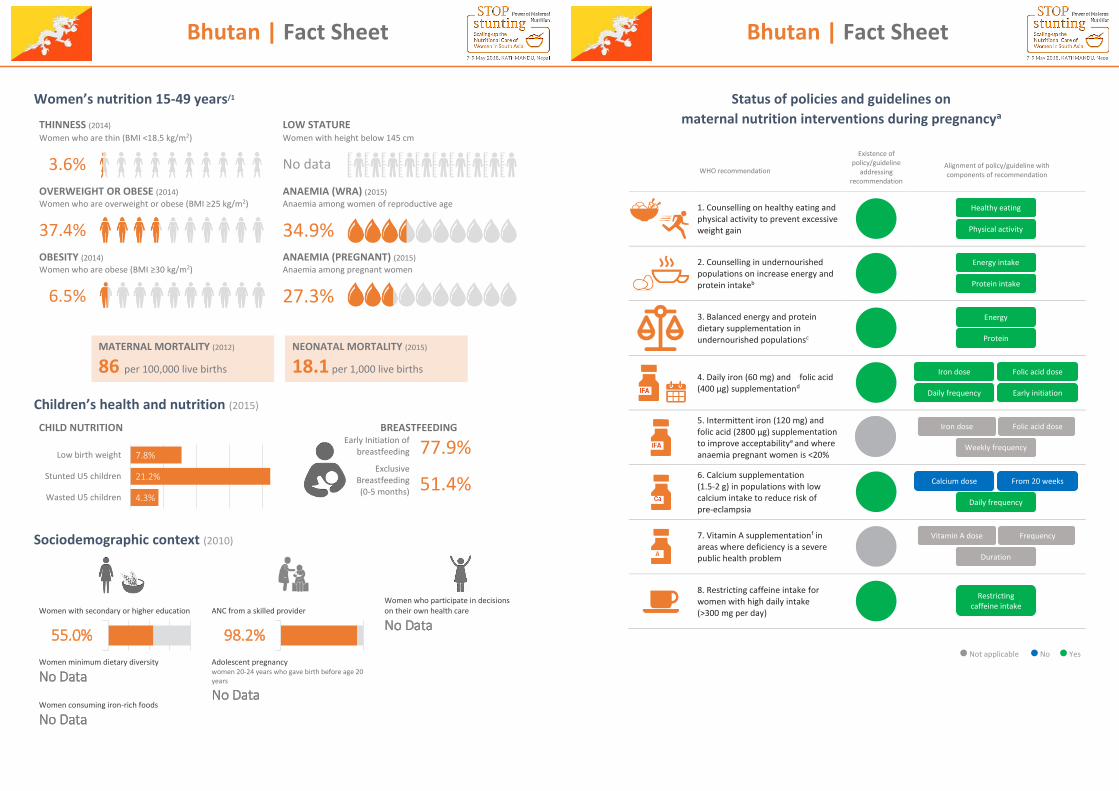
Bhutan | Fact Sheet
1
Women’s nutrition 15-49 years/1
THINNESS (2014) LOW STATURE Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
3.6%
No data
OVERWEIGHT OR OBESE (2014) ANAEMIA (WRA) (2015) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age
37.4% 34.9% OBESITY (2014) ANAEMIA (PREGNANT) (2015) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
6.5% 27.3%
Children’s health and nutrition (2015)
CHILD NUTRITION BREASTFEEDING
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
77.9%
51.4%
Sociodemographic context (2010)
4.3%
21.2%
7.8%
Wasted U5 children
Stunted U5 children
Low birth weight
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
No Data
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
No Data
Women consuming iron-rich foods
No Data
55.0% 98.2%
MATERNAL MORTALITY (2012)
86 per 100,000 live births
NEONATAL MORTALITY (2015)
18.1 per 1,000 live births
Bhutan | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
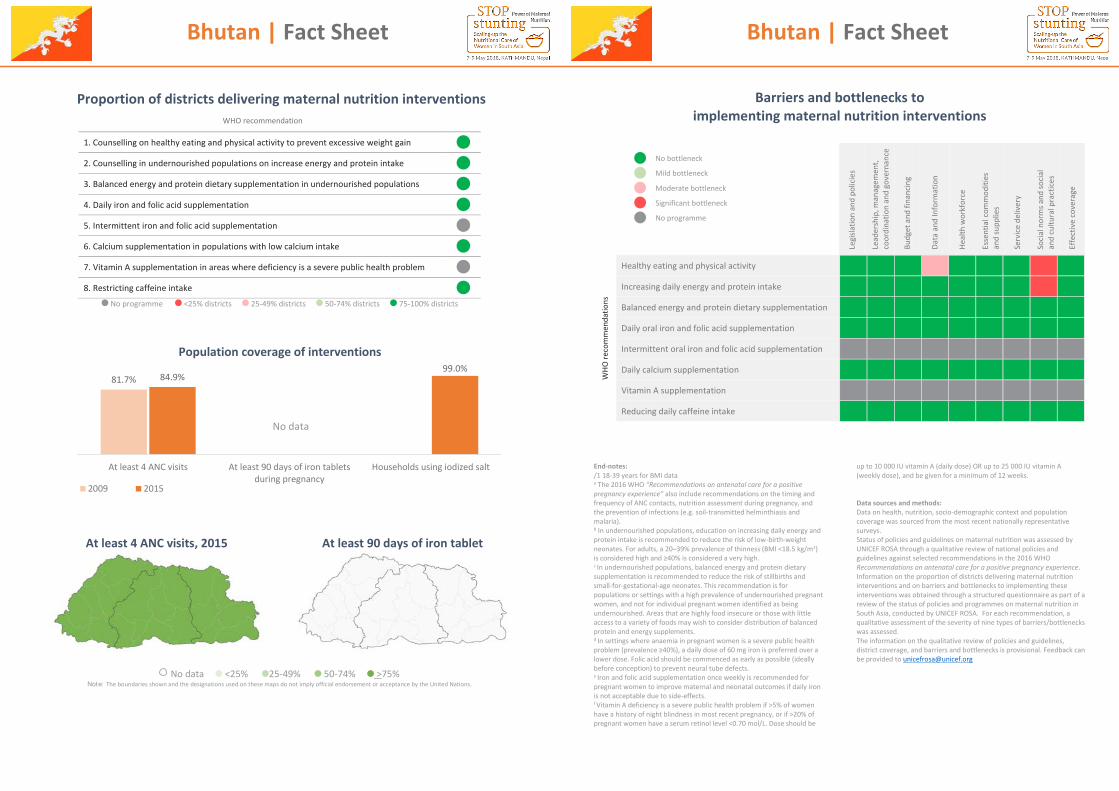
Bhutan | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions
At least 4 ANC visits, 2015 At least 90 days of iron tablet
No data <25% 25-49% 50-74% >75% Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
81.7% 84.9%99.0%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt
2009 2015
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
No data
Bhutan | Fact Sheet
4
Barriers and bottlenecks to
implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: /1 18-39 years for BMI data a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects. f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be
up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
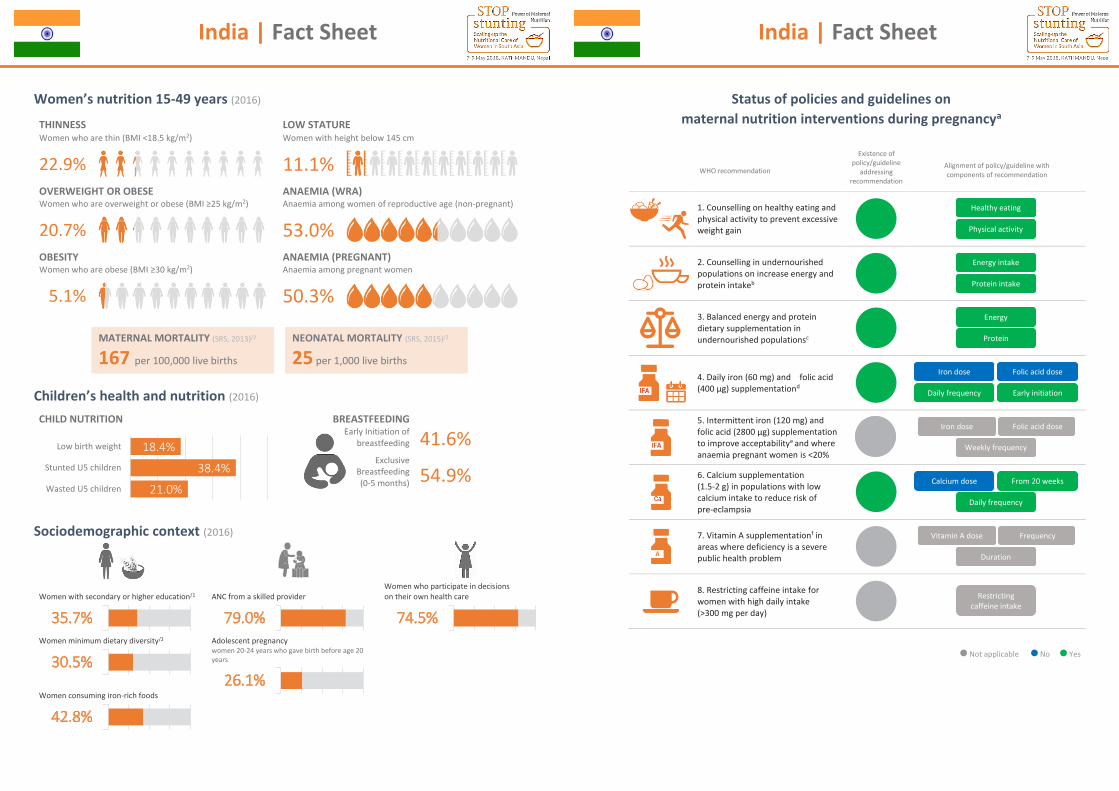
India | Fact Sheet
1
Women’s nutrition 15-49 years (2016)
THINNESS LOW STATURE Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
22.9%
11.1%
OVERWEIGHT OR OBESE ANAEMIA (WRA) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age (non-pregnant)
20.7% 53.0% OBESITY ANAEMIA (PREGNANT) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
5.1% 50.3%
Children’s health and nutrition (2016)
CHILD NUTRITION BREASTFEEDING
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
41.6%
54.9%
Sociodemographic context (2016)
21.0%
38.4%
18.4%
Wasted U5 children
Stunted U5 children
Low birth weight
Women with secondary or higher education/1
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity/2
Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods
35.7% 79.0% 74.5%
30.5%26.1%
42.8%
MATERNAL MORTALITY (SRS, 2013)/2
167 per 100,000 live births
NEONATAL MORTALITY (SRS, 2015)/2
25 per 1,000 live births
India | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
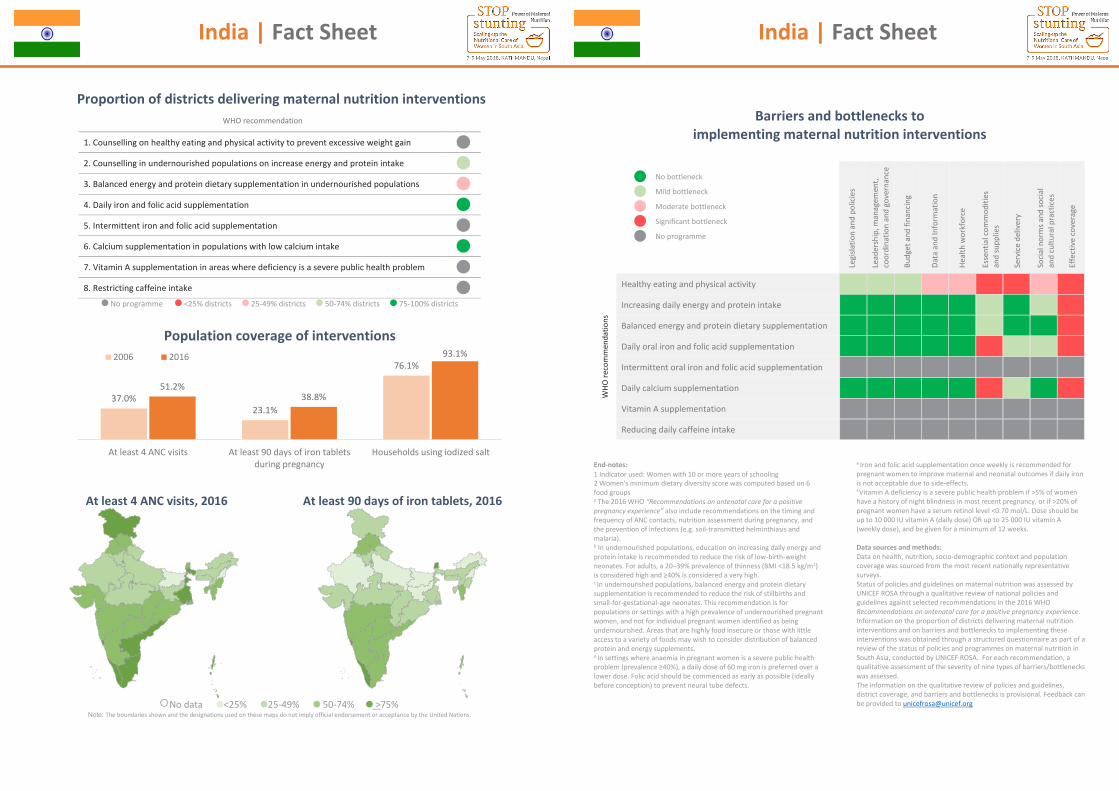
India | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions
At least 4 ANC visits, 2016
At least 90 days of iron tablets, 2016
No data <25% 25-49% 50-74% >75%
Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
37.0%23.1%
76.1%
51.2%38.8%
93.1%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt
2006 2016
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
India | Fact Sheet
4
Barriers and bottlenecks to implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: 1 Indicator used: Women with 10 or more years of schooling 2 Women's minimum dietary diversity score was computed based on 6 food groups a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects.
e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects. f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
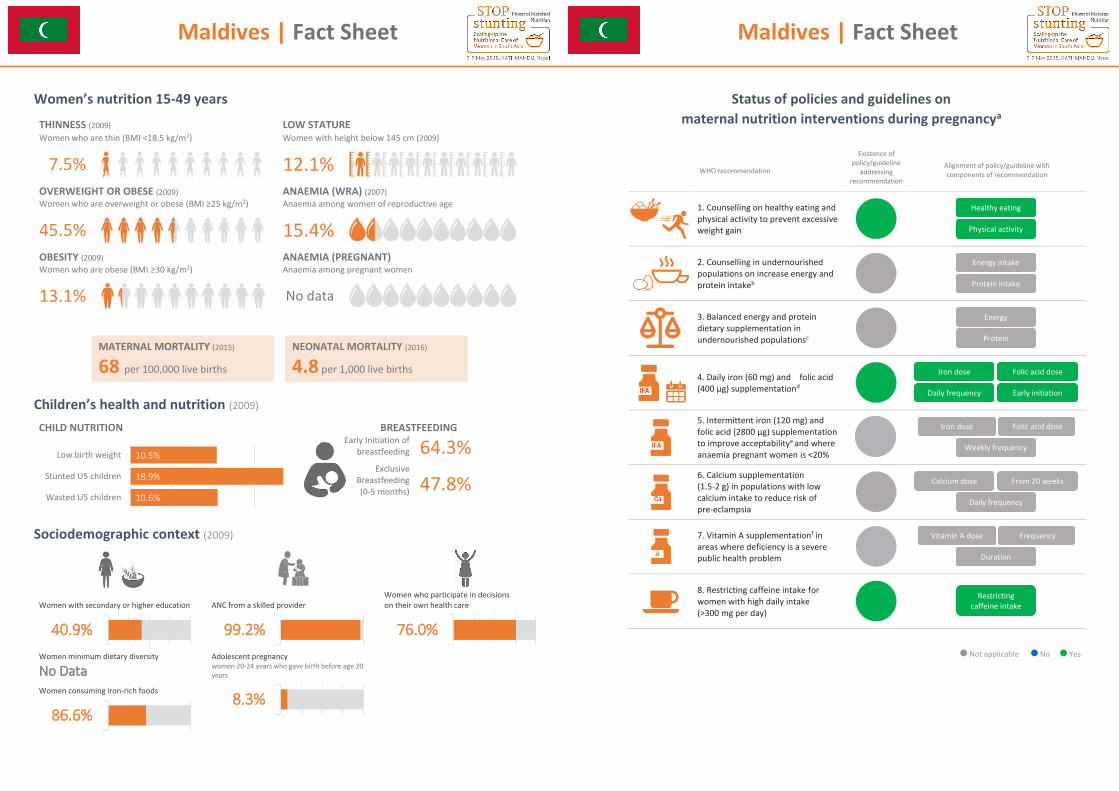
Maldives | Fact Sheet
1
Women’s nutrition 15-49 years
THINNESS (2009) LOW STATURE Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm (2009)
7.5%
12.1%
OVERWEIGHT OR OBESE (2009) ANAEMIA (WRA) (2007) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age
45.5% 15.4% OBESITY (2009) ANAEMIA (PREGNANT) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
13.1% No data
Children’s health and nutrition (2009)
CHILD NUTRITION BREASTFEEDING
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
64.3%
47.8%
Sociodemographic context (2009)
10.6%
18.9%
10.5%
Wasted U5 children
Stunted U5 children
Low birth weight
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods
40.9% 99.2% 76.0%
8.3%86.6%
MATERNAL MORTALITY (2015)
68 per 100,000 live births
NEONATAL MORTALITY (2016)
4.8 per 1,000 live births
Maldives | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
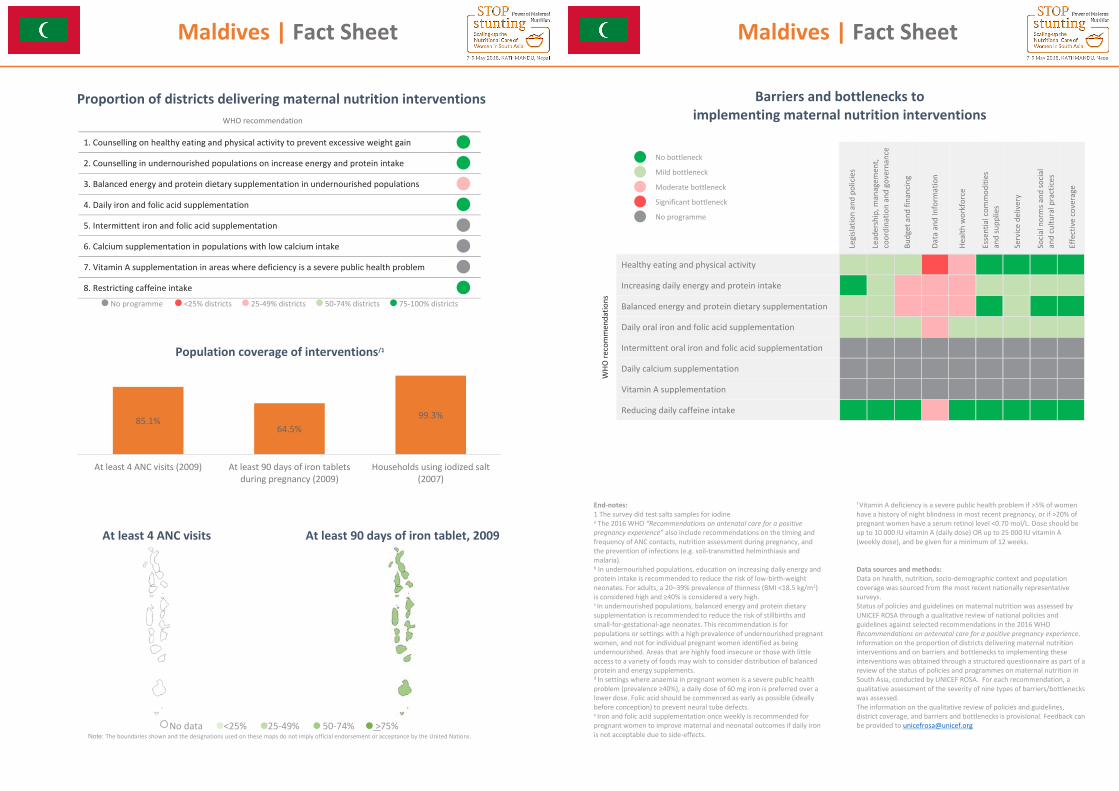
Maldives | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions/1
At least 4 ANC visits
At least 90 days of iron tablet, 2009
No data <25% 25-49% 50-74% >75%
Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
85.1%64.5%
99.3%
At least 4 ANC visits (2009) At least 90 days of iron tabletsduring pregnancy (2009)
Households using iodized salt(2007)
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
Maldives | Fact Sheet
4
Barriers and bottlenecks to
implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: 1 The survey did test salts samples for iodine a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects.
f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
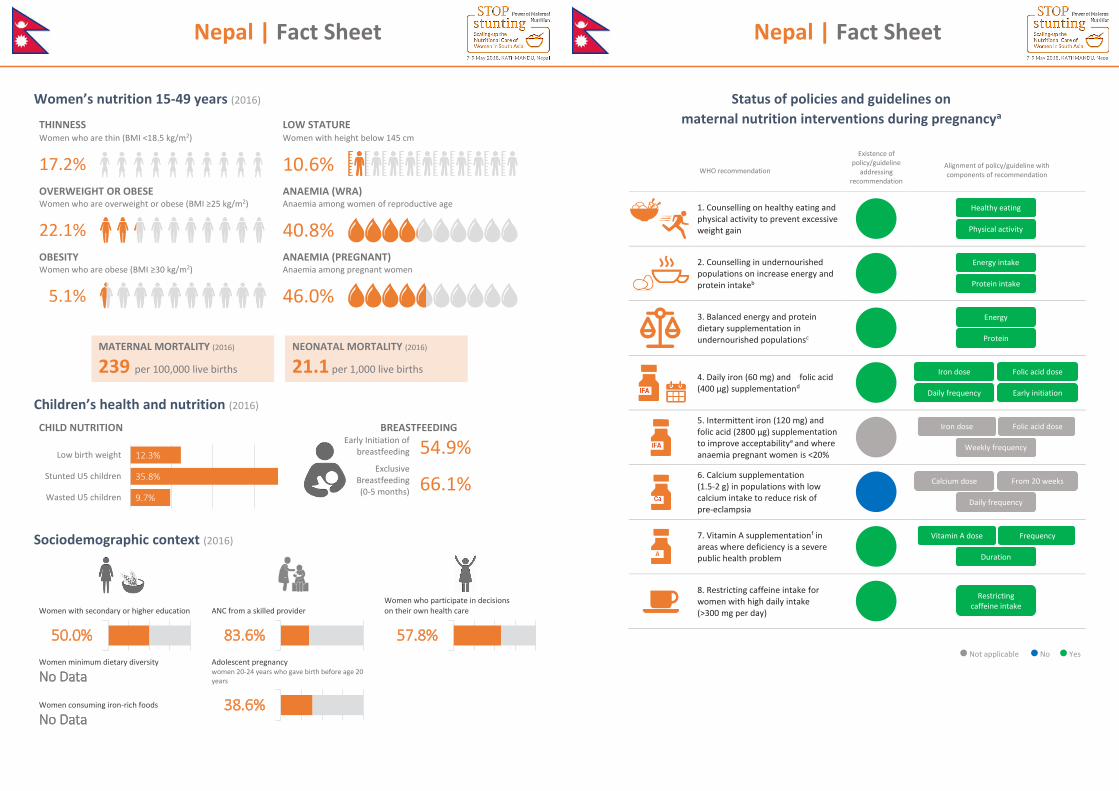
Nepal | Fact Sheet
1
Women’s nutrition 15-49 years (2016)
THINNESS LOW STATURE Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
17.2%
10.6%
OVERWEIGHT OR OBESE ANAEMIA (WRA) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age
22.1% 40.8% OBESITY ANAEMIA (PREGNANT) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
5.1% 46.0%
Children’s health and nutrition (2016)
CHILD NUTRITION BREASTFEEDING
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
54.9%
66.1%
Sociodemographic context (2016)
9.7%
35.8%
12.3%
Wasted U5 children
Stunted U5 children
Low birth weight
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods
No Data
50.0% 83.6% 57.8%
38.6%
MATERNAL MORTALITY (2016)
239 per 100,000 live births
NEONATAL MORTALITY (2016)
21.1 per 1,000 live births
Nepal | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
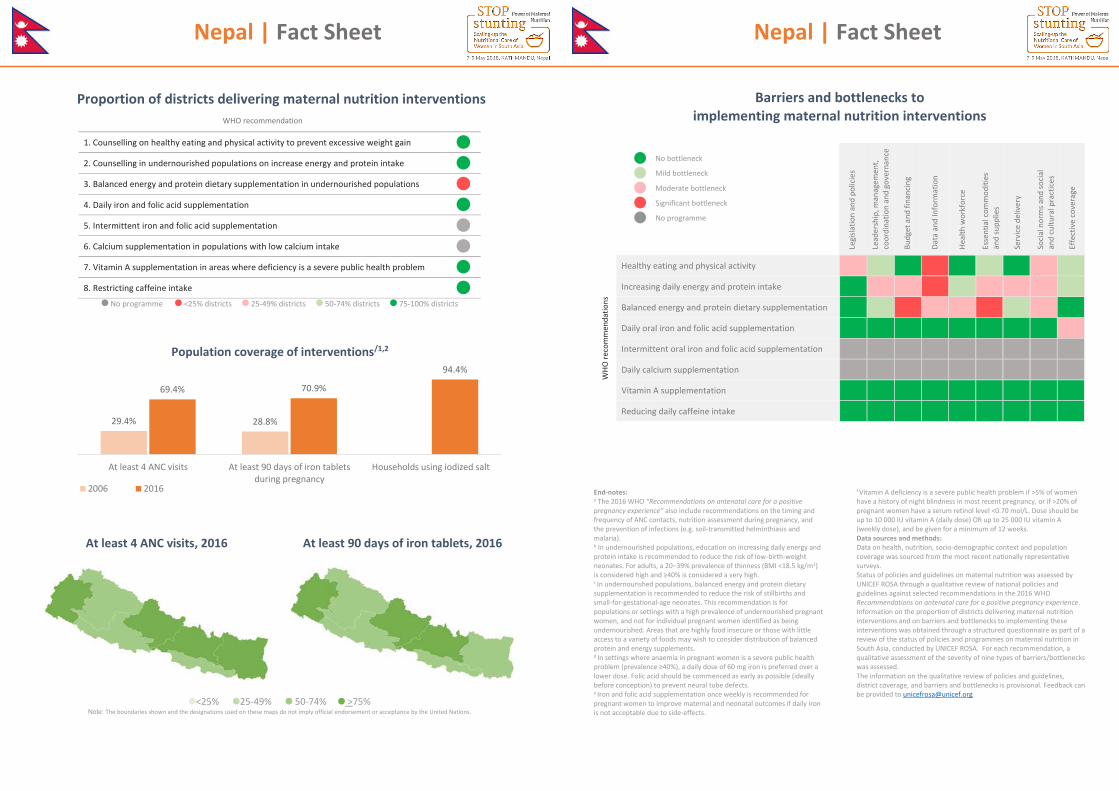
Nepal | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions/1,2
At least 4 ANC visits, 2016
At least 90 days of iron tablets, 2016
<25% 25-49% 50-74% >75% Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
29.4% 28.8%
69.4% 70.9%
94.4%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt
2006 2016
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
Nepal | Fact Sheet
4
Barriers and bottlenecks to
implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects.
f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
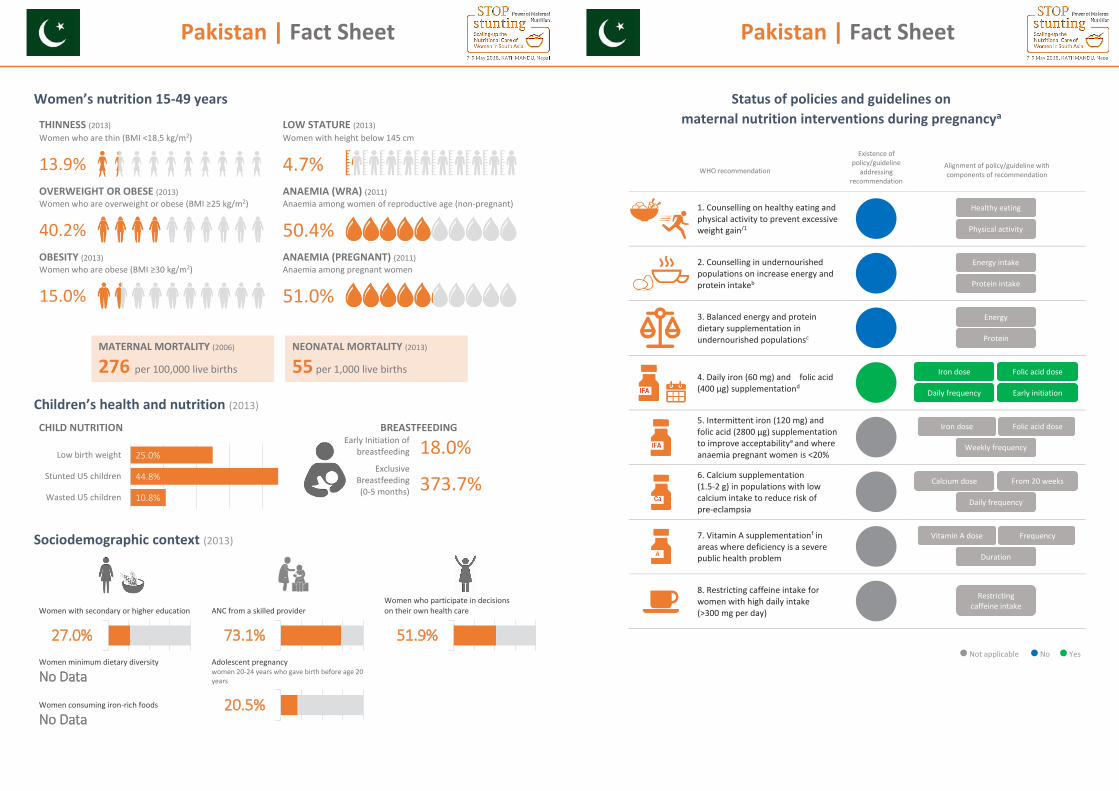
Pakistan | Fact Sheet
1
Women’s nutrition 15-49 years
THINNESS (2013) LOW STATURE (2013) Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
13.9%
4.7%
OVERWEIGHT OR OBESE (2013) ANAEMIA (WRA) (2011) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age (non-pregnant)
40.2% 50.4% OBESITY (2013) ANAEMIA (PREGNANT) (2011) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
15.0% 51.0%
Children’s health and nutrition (2013)
CHILD NUTRITION BREASTFEEDING
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
18.0%
373.7%
Sociodemographic context (2013)
10.8%
44.8%
25.0%
Wasted U5 children
Stunted U5 children
Low birth weight
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods
No Data
27.0% 73.1% 51.9%
20.5%
MATERNAL MORTALITY (2006)
276 per 100,000 live births
NEONATAL MORTALITY (2013)
55 per 1,000 live births
Pakistan | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain/1
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
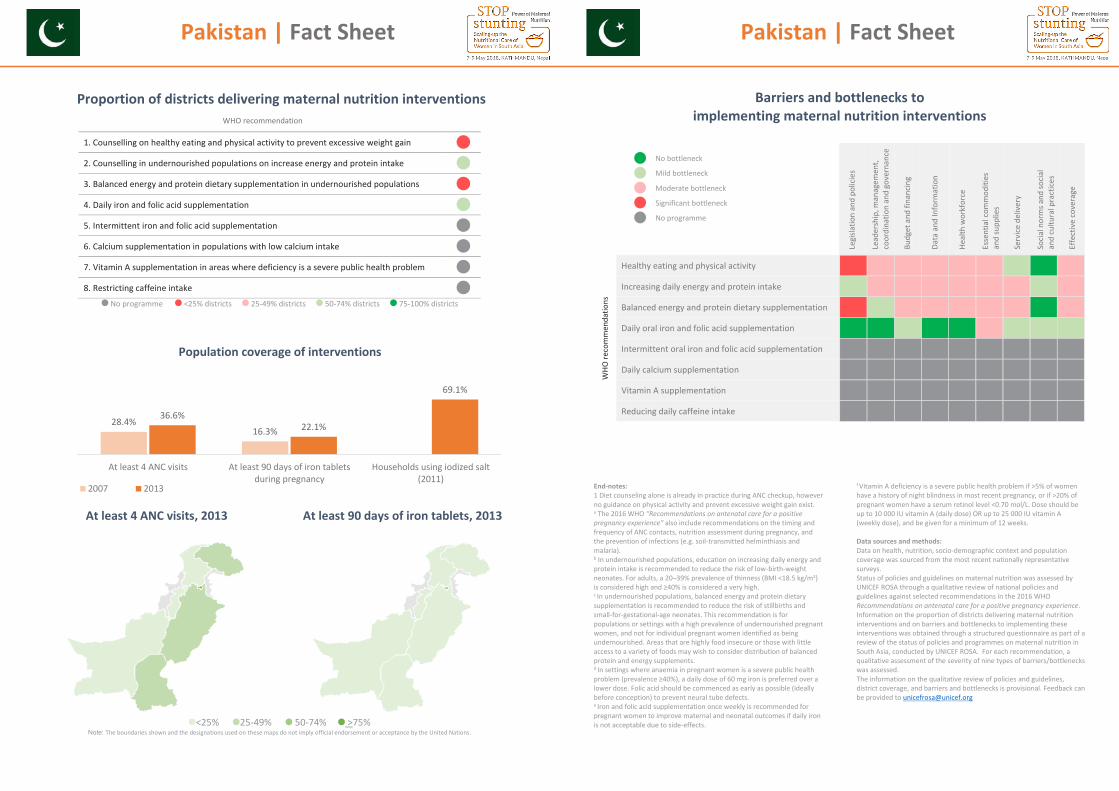
Pakistan | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions
At least 4 ANC visits, 2013
At least 90 days of iron tablets, 2013
<25% 25-49% 50-74% >75%
Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
28.4%16.3%
36.6%22.1%
69.1%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt(2011)
2007 2013
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
Pakistan | Fact Sheet
4
Barriers and bottlenecks to
implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: 1 Diet counseling alone is already in practice during ANC checkup, however no guidance on physical activity and prevent excessive weight gain exist. a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects.
f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
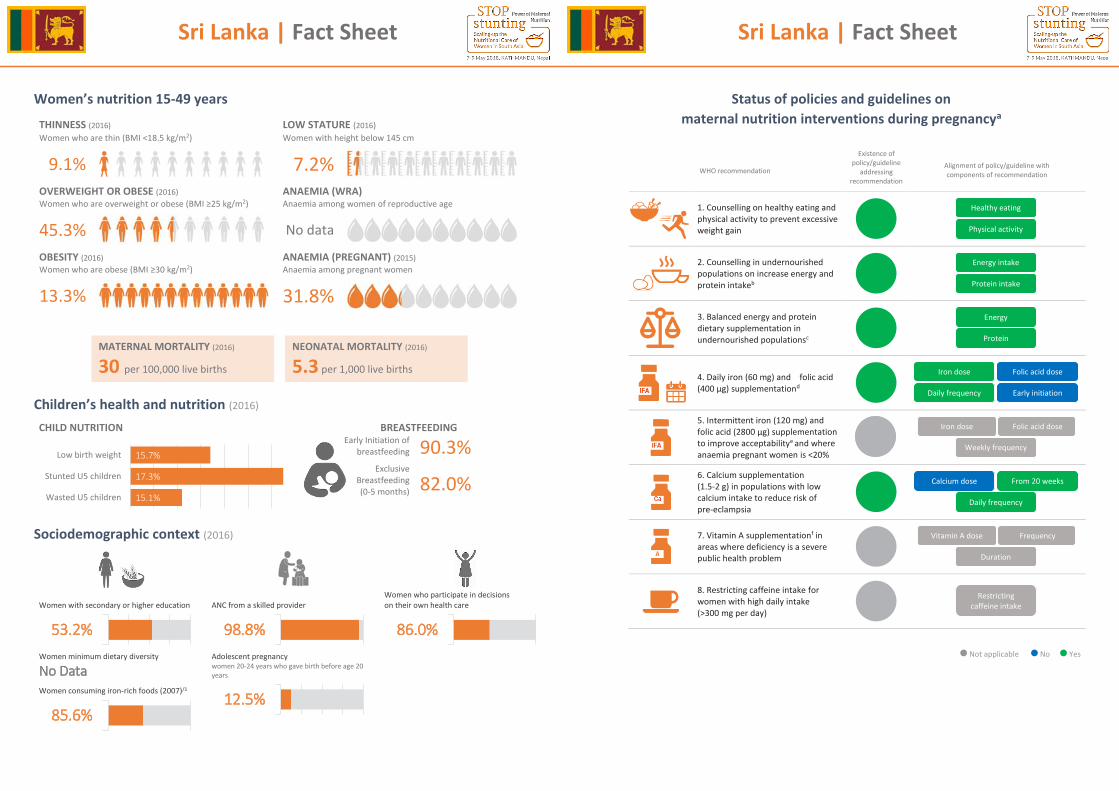
Sri Lanka | Fact Sheet
1
Women’s nutrition 15-49 years
THINNESS (2016) LOW STATURE (2016) Women who are thin (BMI <18.5 kg/m2) Women with height below 145 cm
9.1%
7.2%
OVERWEIGHT OR OBESE (2016) ANAEMIA (WRA) Women who are overweight or obese (BMI ≥25 kg/m2) Anaemia among women of reproductive age
45.3% No data
OBESITY (2016) ANAEMIA (PREGNANT) (2015) Women who are obese (BMI ≥30 kg/m2) Anaemia among pregnant women
13.3% 31.8%
Children’s health and nutrition (2016)
CHILD NUTRITION BREASTFEEDING
Early Initiation of breastfeeding
Exclusive Breastfeeding (0-5 months)
90.3%
82.0%
Sociodemographic context (2016)
15.1%
17.3%
15.7%
Wasted U5 children
Stunted U5 children
Low birth weight
Women with secondary or higher education
ANC from a skilled provider
Women who participate in decisions on their own health care
Women minimum dietary diversity
No Data Adolescent pregnancy women 20-24 years who gave birth before age 20 years
Women consuming iron-rich foods (2007)/1
53.2% 98.8% 86.0%
12.5%85.6%
MATERNAL MORTALITY (2016)
30 per 100,000 live births
NEONATAL MORTALITY (2016)
5.3 per 1,000 live births
Sri Lanka | Fact Sheet
2
Status of policies and guidelines on
maternal nutrition interventions during pregnancya
WHO recommendation
Existence of policy/guideline
addressing recommendation
Alignment of policy/guideline with components of recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intakeb
3. Balanced energy and protein dietary supplementation in undernourished populationsc
4. Daily iron (60 mg) and folic acid (400 μg) supplementationd
5. Intermittent iron (120 mg) and folic acid (2800 μg) supplementation to improve acceptabilitye and where anaemia pregnant women is <20%
6. Calcium supplementation (1.5-2 g) in populations with low calcium intake to reduce risk of pre-eclampsia
7. Vitamin A supplementationf in areas where deficiency is a severe public health problem
8. Restricting caffeine intake for women with high daily intake (>300 mg per day)
Not applicable No Yes
Physical activity
Healthy eating
Protein intake
Energy intake
Protein
Energy
Early initiation Daily frequency
Folic acid dose Iron dose
Weekly frequency
Folic acid dose Iron dose
Daily frequency
From 20 weeks Calcium dose
Duration
Frequency Vitamin A dose
Restricting caffeine intake
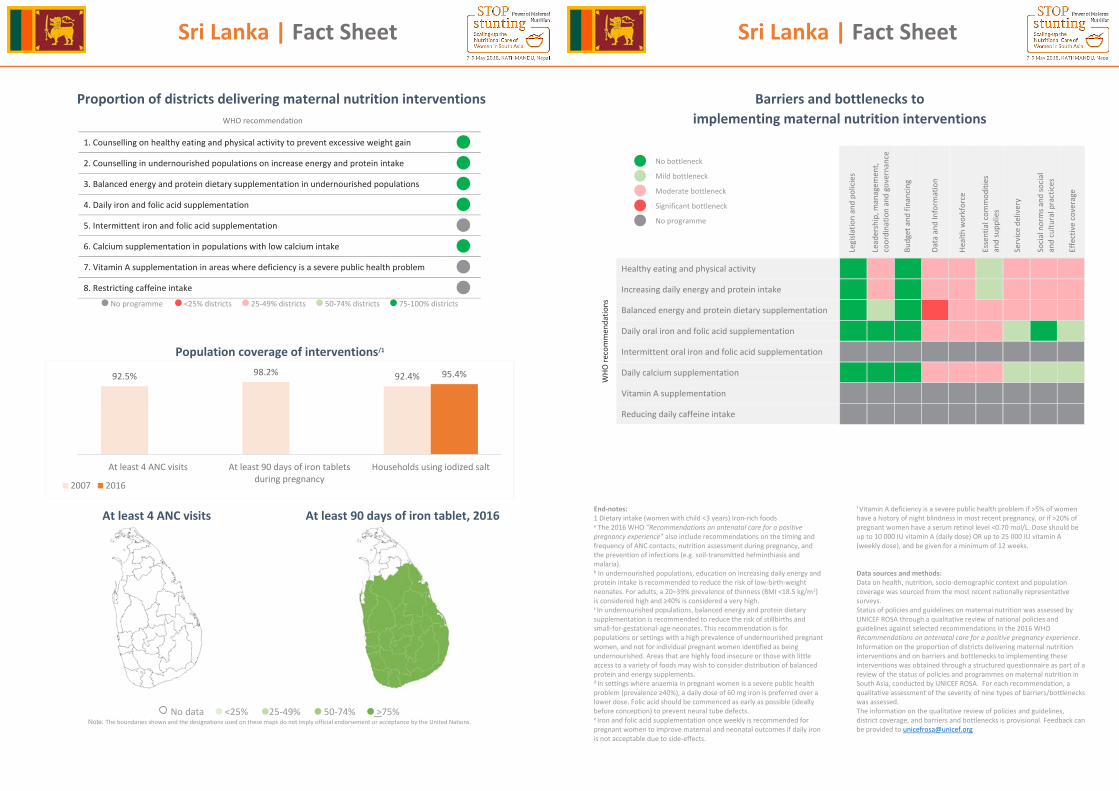
Sri Lanka | Fact Sheet
3
Proportion of districts delivering maternal nutrition interventions
No programme <25% districts 25-49% districts 50-74% districts 75-100% districts
Population coverage of interventions/1
At least 4 ANC visits
At least 90 days of iron tablet, 2016
No data <25% 25-49% 50-74% >75% Note: The boundaries shown and the designations used on these maps do not imply official endorsement or acceptance by the United Nations.
92.5% 98.2% 92.4% 95.4%
At least 4 ANC visits At least 90 days of iron tabletsduring pregnancy
Households using iodized salt
2007 2016
WHO recommendation
1. Counselling on healthy eating and physical activity to prevent excessive weight gain
2. Counselling in undernourished populations on increase energy and protein intake
3. Balanced energy and protein dietary supplementation in undernourished populations
4. Daily iron and folic acid supplementation
5. Intermittent iron and folic acid supplementation
6. Calcium supplementation in populations with low calcium intake
7. Vitamin A supplementation in areas where deficiency is a severe public health problem
8. Restricting caffeine intake
Sri Lanka | Fact Sheet
4
Barriers and bottlenecks to
implementing maternal nutrition interventions
Legi
slatio
n an
d po
licie
s
Lead
ersh
ip, m
anag
emen
t, co
ordi
natio
n an
d go
vern
ance
Budg
et a
nd fi
nanc
ing
Data
and
Info
rmat
ion
Heal
th w
orkf
orce
Esse
ntia
l com
mod
ities
an
d su
pplie
s
Serv
ice d
eliv
ery
Socia
l nor
ms a
nd so
cial
and
cultu
ral p
ract
ices
Effe
ctiv
e co
vera
ge
WHO
reco
mm
enda
tions
Healthy eating and physical activity
Increasing daily energy and protein intake
Balanced energy and protein dietary supplementation
Daily oral iron and folic acid supplementation
Intermittent oral iron and folic acid supplementation
Daily calcium supplementation
Vitamin A supplementation
Reducing daily caffeine intake
End-notes: 1 Dietary intake (women with child <3 years) Iron-rich foods a The 2016 WHO “Recommendations on antenatal care for a positive pregnancy experience” also include recommendations on the timing and frequency of ANC contacts, nutrition assessment during pregnancy, and the prevention of infections (e.g. soil-transmitted helminthiasis and malaria).
b In undernourished populations, education on increasing daily energy and protein intake is recommended to reduce the risk of low-birth-weight neonates. For adults, a 20–39% prevalence of thinness (BMI <18.5 kg/m2) is considered high and ≥40% is considered a very high. c In undernourished populations, balanced energy and protein dietary supplementation is recommended to reduce the risk of stillbirths and small-for-gestational-age neonates. This recommendation is for populations or settings with a high prevalence of undernourished pregnant women, and not for individual pregnant women identified as being undernourished. Areas that are highly food insecure or those with little access to a variety of foods may wish to consider distribution of balanced protein and energy supplements. d In settings where anaemia in pregnant women is a severe public health problem (prevalence ≥40%), a daily dose of 60 mg iron is preferred over a lower dose. Folic acid should be commenced as early as possible (ideally before conception) to prevent neural tube defects. e Iron and folic acid supplementation once weekly is recommended for pregnant women to improve maternal and neonatal outcomes if daily iron is not acceptable due to side-effects.
f Vitamin A deficiency is a severe public health problem if >5% of women have a history of night blindness in most recent pregnancy, or if >20% of pregnant women have a serum retinol level <0.70 mol/L. Dose should be up to 10 000 IU vitamin A (daily dose) OR up to 25 000 IU vitamin A (weekly dose), and be given for a minimum of 12 weeks. Data sources and methods: Data on health, nutrition, socio-demographic context and population coverage was sourced from the most recent nationally representative surveys. Status of policies and guidelines on maternal nutrition was assessed by UNICEF ROSA through a qualitative review of national policies and guidelines against selected recommendations in the 2016 WHO Recommendations on antenatal care for a positive pregnancy experience. Information on the proportion of districts delivering maternal nutrition interventions and on barriers and bottlenecks to implementing these interventions was obtained through a structured questionnaire as part of a review of the status of policies and programmes on maternal nutrition in South Asia, conducted by UNICEF ROSA. For each recommendation, a qualitative assessment of the severity of nine types of barriers/bottlenecks was assessed. The information on the qualitative review of policies and guidelines, district coverage, and barriers and bottlenecks is provisional. Feedback can be provided to [email protected]
No bottleneck
Mild bottleneck
Moderate bottleneck
Significant bottleneck
No programme
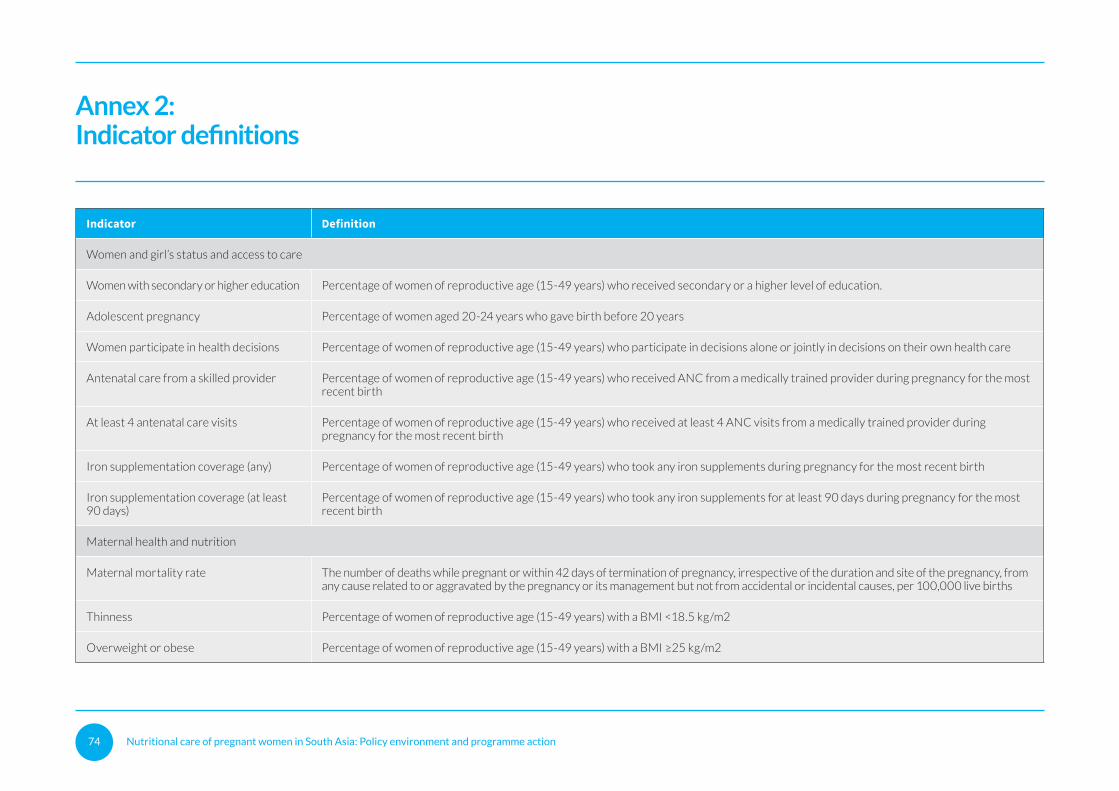
Nutritional care of pregnant women in South Asia: Policy environment and programme action 74
Annex 2:Indicator definitions
Indicator Definition
Women and girl’s status and access to care
Women with secondary or higher education Percentage of women of reproductive age (15-49 years) who received secondary or a higher level of education.
Adolescent pregnancy Percentage of women aged 20-24 years who gave birth before 20 years
Women participate in health decisions Percentage of women of reproductive age (15-49 years) who participate in decisions alone or jointly in decisions on their own health care
Antenatal care from a skilled provider Percentage of women of reproductive age (15-49 years) who received ANC from a medically trained provider during pregnancy for the most recent birth
At least 4 antenatal care visits Percentage of women of reproductive age (15-49 years) who received at least 4 ANC visits from a medically trained provider during pregnancy for the most recent birth
Iron supplementation coverage (any) Percentage of women of reproductive age (15-49 years) who took any iron supplements during pregnancy for the most recent birth
Iron supplementation coverage (at least 90 days)
Percentage of women of reproductive age (15-49 years) who took any iron supplements for at least 90 days during pregnancy for the most recent birth
Maternal health and nutrition
Maternal mortality rate The number of deaths while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes, per 100,000 live births
Thinness Percentage of women of reproductive age (15-49 years) with a BMI <18.5 kg/m2
Overweight or obese Percentage of women of reproductive age (15-49 years) with a BMI ≥25 kg/m2
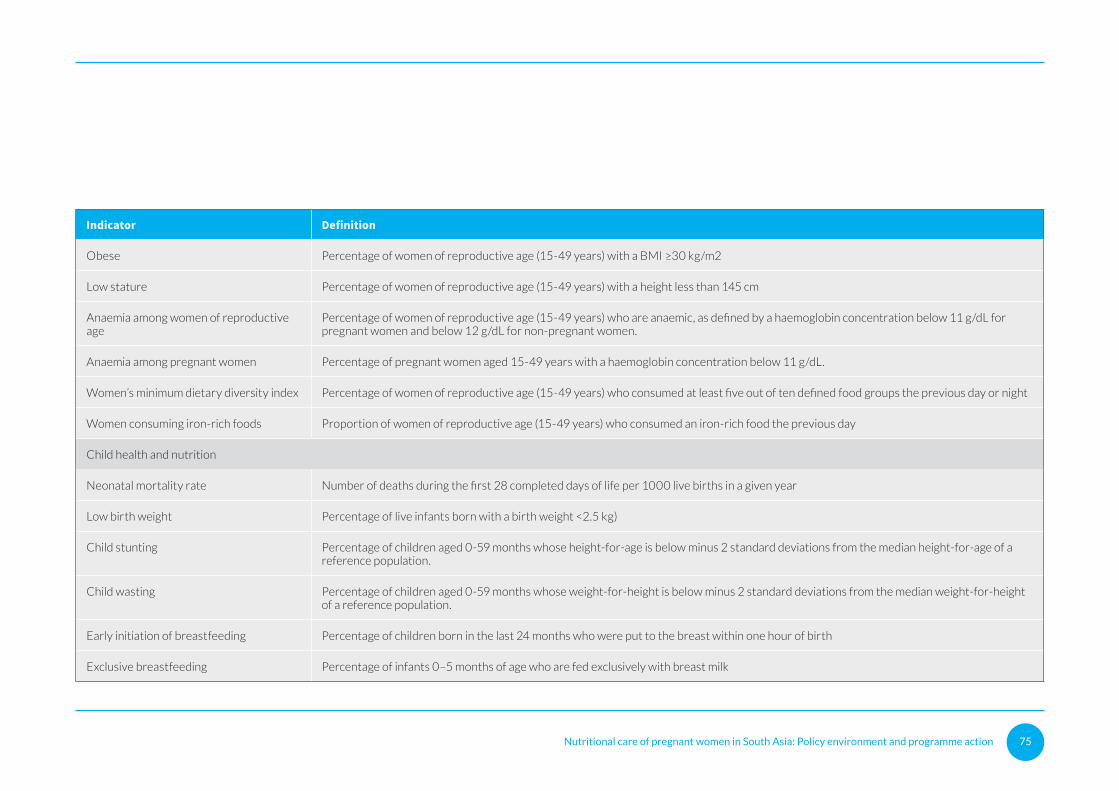
Nutritional care of pregnant women in South Asia: Policy environment and programme action 75
Indicator Definition
Obese Percentage of women of reproductive age (15-49 years) with a BMI ≥30 kg/m2
Low stature Percentage of women of reproductive age (15-49 years) with a height less than 145 cm
Anaemia among women of reproductive age
Percentage of women of reproductive age (15-49 years) who are anaemic, as defined by a haemoglobin concentration below 11 g/dL for pregnant women and below 12 g/dL for non-pregnant women.
Anaemia among pregnant women Percentage of pregnant women aged 15-49 years with a haemoglobin concentration below 11 g/dL.
Women’s minimum dietary diversity index Percentage of women of reproductive age (15-49 years) who consumed at least five out of ten defined food groups the previous day or night
Women consuming iron-rich foods Proportion of women of reproductive age (15-49 years) who consumed an iron-rich food the previous day
Child health and nutrition
Neonatal mortality rate Number of deaths during the first 28 completed days of life per 1000 live births in a given year
Low birth weight Percentage of live infants born with a birth weight <2.5 kg)
Child stunting Percentage of children aged 0-59 months whose height-for-age is below minus 2 standard deviations from the median height-for-age of a reference population.
Child wasting Percentage of children aged 0-59 months whose weight-for-height is below minus 2 standard deviations from the median weight-for-height of a reference population.
Early initiation of breastfeeding Percentage of children born in the last 24 months who were put to the breast within one hour of birth
Exclusive breastfeeding Percentage of infants 0–5 months of age who are fed exclusively with breast milk
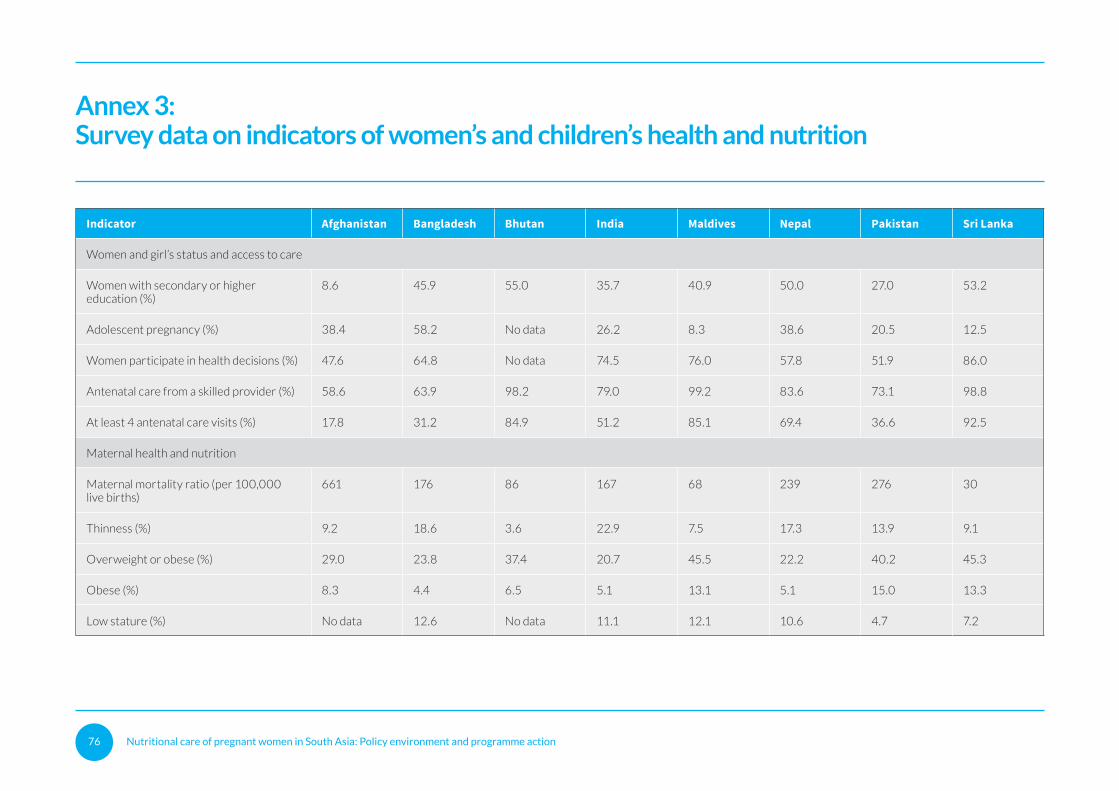
Nutritional care of pregnant women in South Asia: Policy environment and programme action 76
Annex 3:Survey data on indicators of women’s and children’s health and nutrition
Indicator Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
Women and girl’s status and access to care
Women with secondary or higher education (%)
8.6 45.9 55.0 35.7 40.9 50.0 27.0 53.2
Adolescent pregnancy (%) 38.4 58.2 No data 26.2 8.3 38.6 20.5 12.5
Women participate in health decisions (%) 47.6 64.8 No data 74.5 76.0 57.8 51.9 86.0
Antenatal care from a skilled provider (%) 58.6 63.9 98.2 79.0 99.2 83.6 73.1 98.8
At least 4 antenatal care visits (%) 17.8 31.2 84.9 51.2 85.1 69.4 36.6 92.5
Maternal health and nutrition
Maternal mortality ratio (per 100,000 live births)
661 176 86 167 68 239 276 30
Thinness (%) 9.2 18.6 3.6 22.9 7.5 17.3 13.9 9.1
Overweight or obese (%) 29.0 23.8 37.4 20.7 45.5 22.2 40.2 45.3
Obese (%) 8.3 4.4 6.5 5.1 13.1 5.1 15.0 13.3
Low stature (%) No data 12.6 No data 11.1 12.1 10.6 4.7 7.2
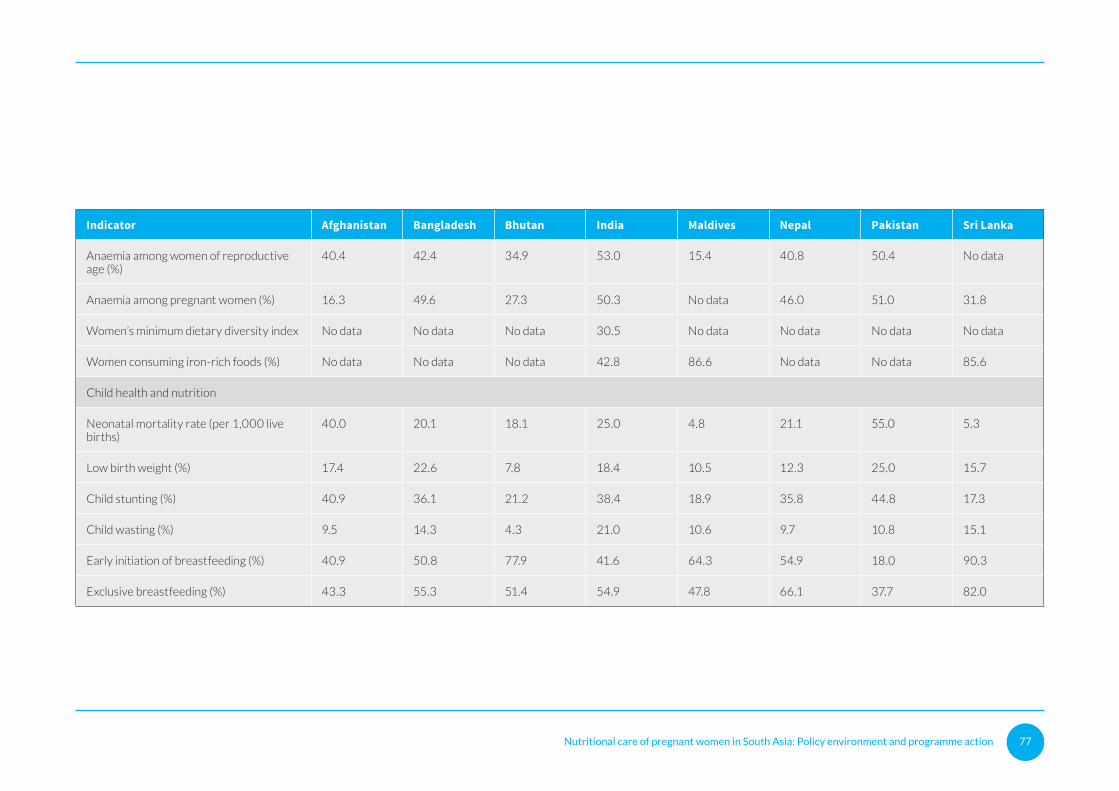
Nutritional care of pregnant women in South Asia: Policy environment and programme action 77
Indicator Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
Anaemia among women of reproductive age (%)
40.4 42.4 34.9 53.0 15.4 40.8 50.4 No data
Anaemia among pregnant women (%) 16.3 49.6 27.3 50.3 No data 46.0 51.0 31.8
Women’s minimum dietary diversity index No data No data No data 30.5 No data No data No data No data
Women consuming iron-rich foods (%) No data No data No data 42.8 86.6 No data No data 85.6
Child health and nutrition
Neonatal mortality rate (per 1,000 live births)
40.0 20.1 18.1 25.0 4.8 21.1 55.0 5.3
Low birth weight (%) 17.4 22.6 7.8 18.4 10.5 12.3 25.0 15.7
Child stunting (%) 40.9 36.1 21.2 38.4 18.9 35.8 44.8 17.3
Child wasting (%) 9.5 14.3 4.3 21.0 10.6 9.7 10.8 15.1
Early initiation of breastfeeding (%) 40.9 50.8 77.9 41.6 64.3 54.9 18.0 90.3
Exclusive breastfeeding (%) 43.3 55.3 51.4 54.9 47.8 66.1 37.7 82.0
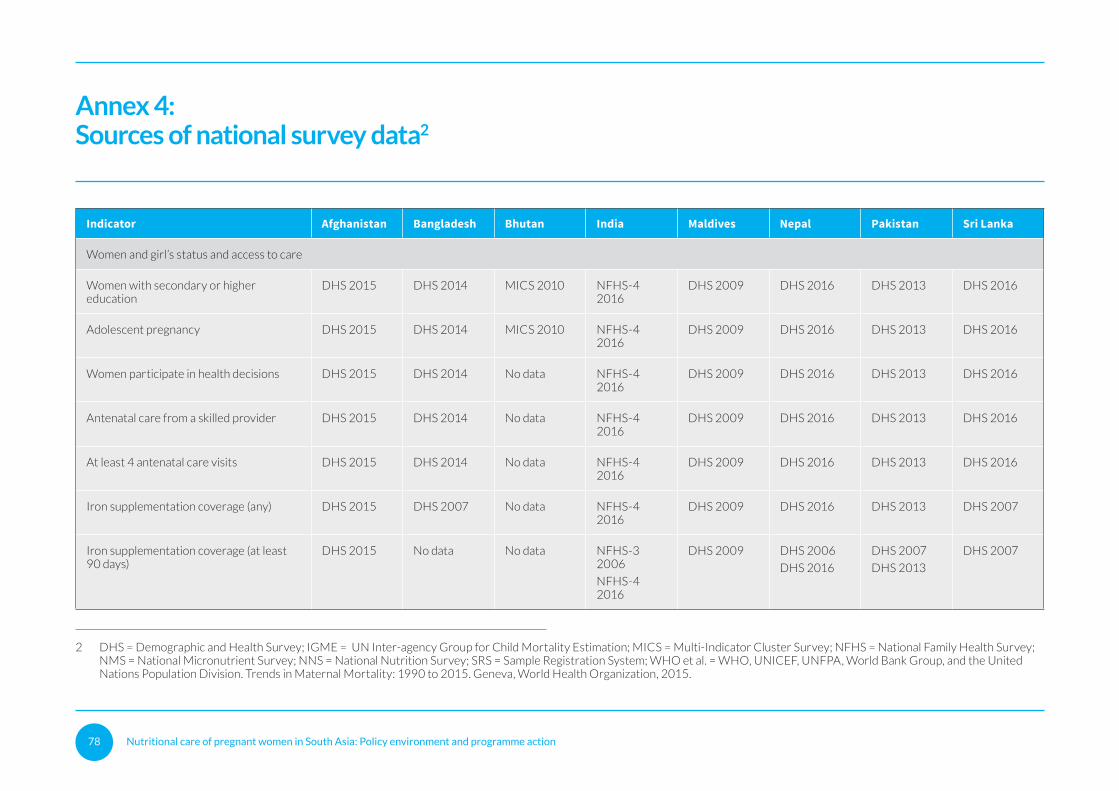
Nutritional care of pregnant women in South Asia: Policy environment and programme action 78
Annex 4:Sources of national survey data2
Indicator Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
Women and girl’s status and access to care
Women with secondary or higher education
DHS 2015 DHS 2014 MICS 2010 NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Adolescent pregnancy DHS 2015 DHS 2014 MICS 2010 NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Women participate in health decisions DHS 2015 DHS 2014 No data NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Antenatal care from a skilled provider DHS 2015 DHS 2014 No data NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
At least 4 antenatal care visits DHS 2015 DHS 2014 No data NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Iron supplementation coverage (any) DHS 2015 DHS 2007 No data NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2007
Iron supplementation coverage (at least 90 days)
DHS 2015 No data No data NFHS-3 2006
NFHS-4 2016
DHS 2009 DHS 2006
DHS 2016
DHS 2007
DHS 2013
DHS 2007
2 DHS = Demographic and Health Survey; IGME = UN Inter-agency Group for Child Mortality Estimation; MICS = Multi-Indicator Cluster Survey; NFHS = National Family Health Survey; NMS = National Micronutrient Survey; NNS = National Nutrition Survey; SRS = Sample Registration System; WHO et al. = WHO, UNICEF, UNFPA, World Bank Group, and the United Nations Population Division. Trends in Maternal Mortality: 1990 to 2015. Geneva, World Health Organization, 2015.
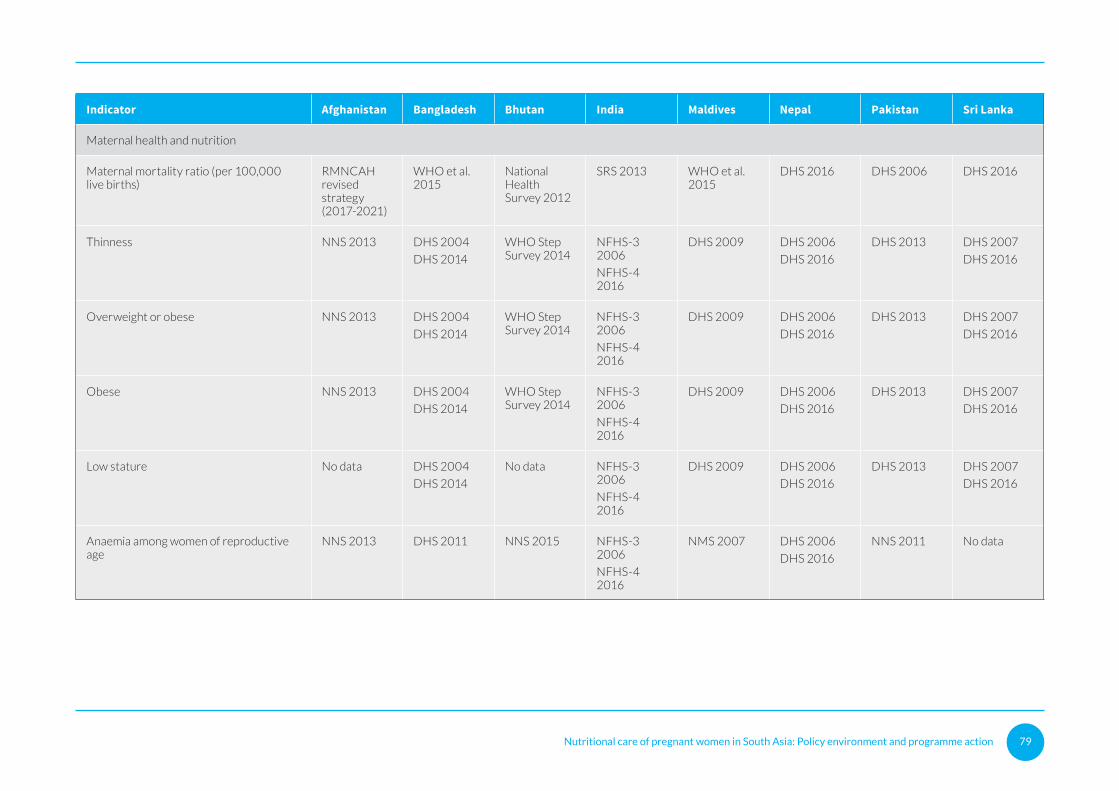
Nutritional care of pregnant women in South Asia: Policy environment and programme action 79
Indicator Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
Maternal health and nutrition
Maternal mortality ratio (per 100,000 live births)
RMNCAH revised strategy (2017-2021)
WHO et al. 2015
National Health Survey 2012
SRS 2013 WHO et al. 2015
DHS 2016 DHS 2006 DHS 2016
Thinness NNS 2013 DHS 2004
DHS 2014
WHO Step Survey 2014
NFHS-3 2006
NFHS-4 2016
DHS 2009 DHS 2006
DHS 2016
DHS 2013 DHS 2007
DHS 2016
Overweight or obese NNS 2013 DHS 2004
DHS 2014
WHO Step Survey 2014
NFHS-3 2006
NFHS-4 2016
DHS 2009 DHS 2006
DHS 2016
DHS 2013 DHS 2007
DHS 2016
Obese NNS 2013 DHS 2004
DHS 2014
WHO Step Survey 2014
NFHS-3 2006
NFHS-4 2016
DHS 2009 DHS 2006
DHS 2016
DHS 2013 DHS 2007
DHS 2016
Low stature No data DHS 2004
DHS 2014
No data NFHS-3 2006
NFHS-4 2016
DHS 2009 DHS 2006
DHS 2016
DHS 2013 DHS 2007
DHS 2016
Anaemia among women of reproductive age
NNS 2013 DHS 2011 NNS 2015 NFHS-3 2006
NFHS-4 2016
NMS 2007 DHS 2006
DHS 2016
NNS 2011 No data
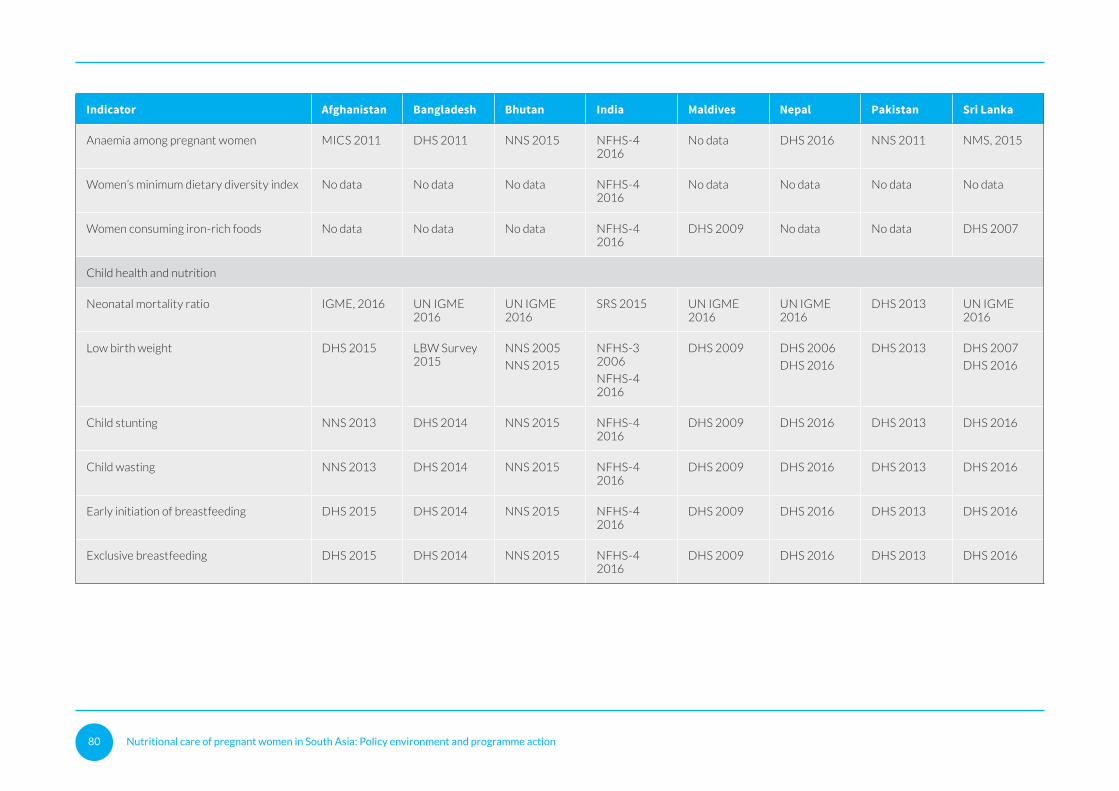
Nutritional care of pregnant women in South Asia: Policy environment and programme action 80
Indicator Afghanistan Bangladesh Bhutan India Maldives Nepal Pakistan Sri Lanka
Anaemia among pregnant women MICS 2011 DHS 2011 NNS 2015 NFHS-4 2016
No data DHS 2016 NNS 2011 NMS, 2015
Women’s minimum dietary diversity index No data No data No data NFHS-4 2016
No data No data No data No data
Women consuming iron-rich foods No data No data No data NFHS-4 2016
DHS 2009 No data No data DHS 2007
Child health and nutrition
Neonatal mortality ratio IGME, 2016 UN IGME 2016
UN IGME 2016
SRS 2015 UN IGME 2016
UN IGME 2016
DHS 2013 UN IGME 2016
Low birth weight DHS 2015 LBW Survey 2015
NNS 2005
NNS 2015
NFHS-3 2006
NFHS-4 2016
DHS 2009 DHS 2006
DHS 2016
DHS 2013 DHS 2007
DHS 2016
Child stunting NNS 2013 DHS 2014 NNS 2015 NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Child wasting NNS 2013 DHS 2014 NNS 2015 NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Early initiation of breastfeeding DHS 2015 DHS 2014 NNS 2015 NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016
Exclusive breastfeeding DHS 2015 DHS 2014 NNS 2015 NFHS-4 2016
DHS 2009 DHS 2016 DHS 2013 DHS 2016

Nutritional care of pregnant women in South Asia: Policy environment and programme action 81
Annex 5:Persons consulted
Country Persons consulted
Afghanistan Zohra Shamszai, Maternal and Neonatal Healthcare Manager, Ministry of Public Health
Homayoun Ludin, Public Nutrition Director, Ministry of Public Health
M. A. Nawabzai, WIFS officer, Ministry of Public Health
Zarmina Sidiq, Maternal Nutrition Officer, Ministry of Public Health
Bangladesh Dr. Zaba Mahmud, Programme Director Alive &Thrive
Dr. Fatema Nawaz, Deputy Programme Manager, Institute of Public Health and Nutrition
Dr. Mahfuza Rifat, Programme Director, Health, Nutrition and Population BRAC
Bhutan Laigden Dzed, Senior Programme Officer, Ministry of Health
Loday Zangpo, Programme Officer, Ministry of Health
Pema Lethro, Senior Programme Officer, Ministry of Health
Dr. Chandralal Mongar, Health and Nutrition Officer, UNICEF
Sonam Gyaltshen, WASH Officer, UNICEF
India Dr. Dinesh Baswal, Deputy Commissioner Maternal Health, Ministry of Health and Family Welfare
Dr. Sucharita Dutta, Country Lead, Nutrition International
Dr. Neena Bhatia, Lead, National Centre for Diets and HOD, Department of Nutrition, Lady Irwin College
Dr. Hari, Lead Consultant, Maternal Health Division, Ministry of Health and Family Welfare
Dr. Salima Bhatia, Lead Consultant, Maternal Health Division, Ministry of Health and Family Welfare
Dr. Nishtha Kathuria, Lead Consultant (Nutrition), Maternal Health Division, Ministry of Health and Family Welfare
Dr. Rasmi Avula, Research analyst, IFPRI
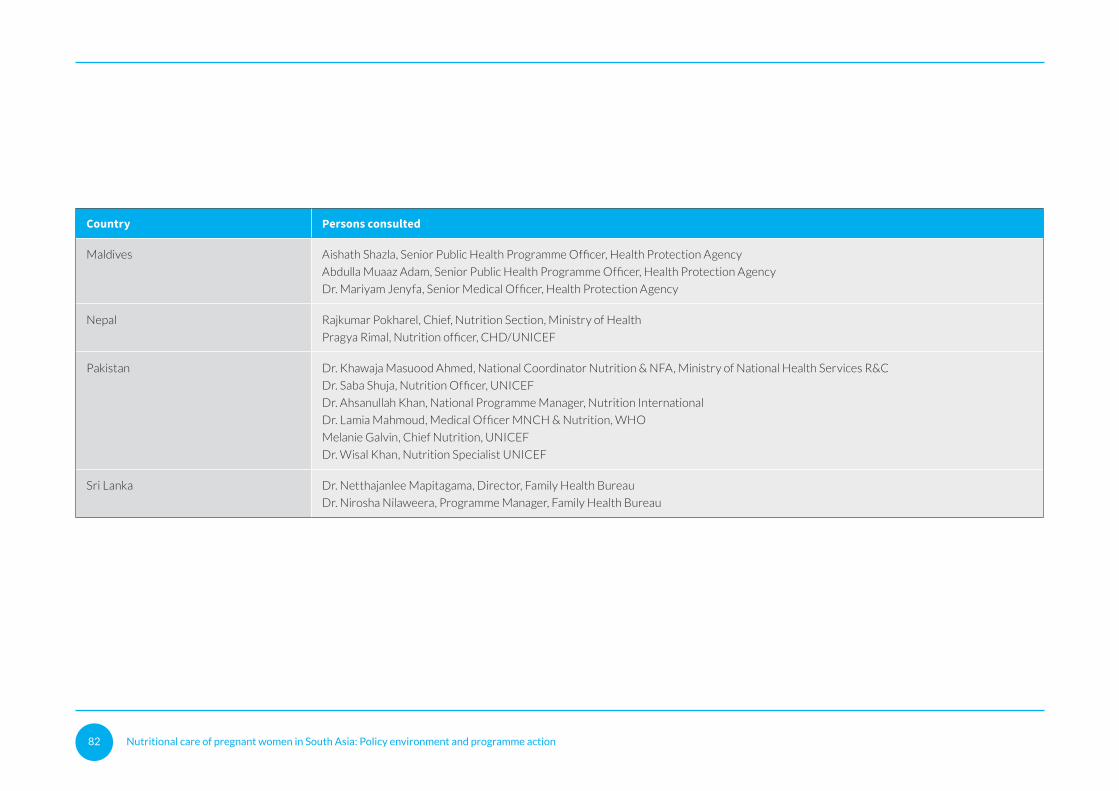
Nutritional care of pregnant women in South Asia: Policy environment and programme action 82
Country Persons consulted
Maldives Aishath Shazla, Senior Public Health Programme Officer, Health Protection Agency
Abdulla Muaaz Adam, Senior Public Health Programme Officer, Health Protection Agency
Dr. Mariyam Jenyfa, Senior Medical Officer, Health Protection Agency
Nepal Rajkumar Pokharel, Chief, Nutrition Section, Ministry of Health
Pragya Rimal, Nutrition officer, CHD/UNICEF
Pakistan Dr. Khawaja Masuood Ahmed, National Coordinator Nutrition & NFA, Ministry of National Health Services R&C
Dr. Saba Shuja, Nutrition Officer, UNICEF
Dr. Ahsanullah Khan, National Programme Manager, Nutrition International
Dr. Lamia Mahmoud, Medical Officer MNCH & Nutrition, WHO
Melanie Galvin, Chief Nutrition, UNICEF
Dr. Wisal Khan, Nutrition Specialist UNICEF
Sri Lanka Dr. Netthajanlee Mapitagama, Director, Family Health Bureau
Dr. Nirosha Nilaweera, Programme Manager, Family Health Bureau
Nutritional care of pregnant women in South Asia: Policy environment and programme action 83
Nutritional care of pregnant women in South Asia: Policy environment and programme action 84
United Nations Children’s FundRegional Office for South Asia
P.O. Box 5815Lekhnath Marg,Kathmandu, Nepal
Tel: +977 1-4417082Email: [email protected]
Websites:www.unicef.org/rosawww.facebook.com/unicefsouthasia





























